Embed Size (px)
Citation preview

22
LEAVES FROM THE ARMY TUMOUR REGISTRY
I-TUMOURS OF LYMPHOID TISSUE
Lieutenant-Colonel P. D. STEWART M.D., Ch.B., D.T.M. & H., R.A.M.C. (Retired)·
Vale of Leven Hospital, Alexandria, Dunbartonshire
Introduction ONE of the functions of the Army Tumour Registry is to build -up as complete a record as possible of tumours in military personnel by collecting biopsy and autopsy material from cases of benign and, malignant neoplasms treated in military hospitals. The first report of the Registry covering the years 1948-52 was published by Neal in 1954; the statistical tables in that report show that tumours of lymphoid tissue form the largest group of malignant neoplasms in soldiers and provide support for Ogilvie's (1954) statement that "Hodgkin's disease, with the other reticuloses, is the commonest manifestation of malignancy in young ServiCe people."
The present paper is base,d on a review of a series of cases of lymphoid tumours in British military personnel. The principal aims -are to record the more important pathological findings, to discuss the histological diagnosis and to study the correlation of histology with the clinical course of the disease. The descriptions of the pathological changes are necessarily curtailed and for fuller accounts the reader is referred to the
, works of Robb-Smith (1938), Gall and Mallory (1942), lackson and Parker (1947), Lumb (1954), MarshaIl (1956) and Harrison (1960), and to the papers on the individual tumours quoted later.
Material and Methods The material of this study comprises all the histologically proved cases of lymphoid
tumours occurring in serving British military personnel in the years 1948-58. During this period there were 150 cases of whom 147 were males and three were females. Most of the cases were registered in the Army Tumour Registry; the remainder, mainly patients admitted direct to civilian hospitals, were traced with the aid of A.M.D. (Stats.).
This review does not cover the total lymphoid tumour material available in the Army Tumour' Registry, as the Registry receives specimens from sources other than serving army personnel.
Histological pxeparations from each patient were personally examined either during a tour of duty at Eastern Command Laboratory or later at the Army Tumour Registry. The material available consisted of slides, blocks or tissue from biopsies or
* This paper is based on an M.D. thesis submitted to the University of Edinburgh.
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Stewart 23
necropsies and in many cases from both. Sections were stained with hremotoxylin and eosin in all instances and for reticulin in most. Other stains used included Van Gieson and P.A.S. Preparations from conditions which require to be differentiated histologically from primary tumours of lymphoid tissue were also studied. The majority of patients have been followed up to date, but a few have been lost sight of.
Classification of Lymphoid Tumours
It is perhaps begging the question to refer to the group of conditions described in this paper as "tumours" since there is still some doubt concerning the nature of the commonest histological variety, namely Hodgkin's disease. Nevertheless, the present consensus of opinion accepts them as neoplasms.
Many classifications of tumours of lymphoid tissue have been published and many different names have been applied to the same histological picture. In probably no other field of oncology is the subject of classification so complicated and confused by the many names employed, and it would be the greatest help to both clinicians and pathologists if a standard nomenclature could be agreed upon.
While recognizing the value of Classification especially for prognostic use, we must remember that· all tumours of lymphoid tissue are probably genetically related through the primitive reticular cell. it is, therefore, not surprising to find that some of the histological pictures are intermediate between the various types described; and that not only have alterations in the type of tumour from one biopsy to another been noted but varying histological appearances have been found in different areas of one tumour (Custer and Bernhard 1948; Lumb 1954; Evans 1956); .
The nomenclature used in this paper (Table I) is based on the simple and practical classifications of Lumb (1954) and Harrison (1960).
TABLE I
CLASSIFICATION OF 150 CASES BY ORIGINAL HISTOLOGY
Type Male Female Total
HODGKIN'S GROUP 'Reticular lymphoma ...... ...... ...... . ..... . ..... 16 - 16 Hodgkin's disease ...... .... , . ...... ...... ...... 86* 1 87* Hodgkin's sarcoma •.... ...... ...... ...... . ..... 9 - 9
FOLLICULAR LYMPHOMA ..... ...... . ..... 8 - 8 LYMPHOSARCOMA ..... ...... ...... ...... . ..... 12 2 14 RETICULUM CELL SARCOMA ...... . ..... .."., 11 - 11 HISTIOCYTIC MEDULLARY RETICULOSIS ...... 3 - 3 UNCLASSIFIED (MIXED) ...... ...... ...... .", .. 2 - 2
Total ...... 147 3 150
* Includes one case where histology at necropsy showed histiocytic meaullary reticulosis.
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

24 Leaves from the Army Tumour Registry
Aetiology Age
The age on first admission of the 150 patients is given in Table H.
TABLE 11
AGE ON FIRST ADMISSION
10-19 20-29 30-39 40-49 50-59 Not stated Total ----------
RETICULAR LYMPHOMA ..... 7 7 1 . 1 - - 16 HODGKIN'S DISEASE ..... 27 45' 10 3 - 2 87* HODGKIN'S SARCOMA ...... - 7 2 - - -, 9 FOLLICULAR LYMPHOMA 5 2 1 - - - 8 LYMPHOSARCOMA ...... ... 7 6 - 1 - - 14 RETICULUM CELL SARCOMA .. 4 5 - 1 1 - 11 HISTIOCYTIC MEDULLARY
RETICULOSIS ...... - 3 - -. - - 3 UNCLASSIFIED ...... 1 - 1 - - - 2
---------------Total ...... 51 75 15 6 1 2 150
* Includes one case where histology at necropsy showed histiocytic medullary reticulosis.
It is not surprising that most of the patients were under 30 years of age, because the selected population from which they were drawn is predominantly a young one and Hodgkin's disease, which is the most common tumour in the series, is recognized as having a high instance in the third-decade (Jacks on and Parker 1947; Lumb 1954; Jelliffe and'Thomson 1955).
Other Factors The patients admitteq to hospital in 1948-55 were analysed by corps, rank, sex,
service and service overseas, but no significant retiological factor was found. Taking into account the selected population dealt with, there would appear to be no difference between the incidence of these tumours in military personnel and that in the general population.
The Hodgkin's Group This group has been sub-divided into three histological types, but there is, in fact,
no definite line of distinction between the three, Hodgkin's disease merging imperceptibly into reticular lymphoma on the one hand and Hodgkin's sarcoma on the other. Of the types recognized Hodgkin's sarcoma is the least clearly defined, but the term has been retained for those cases at the more malignant end of the histological spectrum.
Reticular Lymphoma Reticular lymphoma is the name given by Lumb (1954) to the most benign member ..
of the Hodgkin's group. The other designations which have been used include
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Slewarf 25
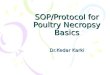
Figure I . Reticular lymphoma. Lymph node. Lymphocytes with scorrered reticulum cells. (H . alld E. x 110)
Figure 2. Hudgkin's dh'e(lse. Lymph nude. Typical giallll.'el/s. (H . al/d E. x 330)
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

26 Leavesfrom the Army Tumour Registry
Figure 3. Follicular lymphoma. Ly mph node. Iltrollgholll 'he node.
FI/?lIre 4. Follicular lymphoma, Lymph "ode. !ollicleJ.
Numerous follicles of I'Drying size (H. a/ld E. X 5.5)
Compressioll of re/iell/ill arOUlld (Gorcloll alld Sweet X 55)
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

;./
<" ,\
P. D. Stewart 27
Hodgkin's paragranuloma (Jackson and Parker 1944), lympho-reticular medullary reticulosis (Robb-S,lUith 1947) and benign Hodgkin's disease (Harris'on 1952; Dawson ' and Harrison 1961). . '
There were 16 pati~nts in respect of whom the original lymph node biopsy showed' the typical histological features of reticular lymphoma. .
Macroscopically the lymph nodes were found to be moderately enlarged (up t"o 4.5.cm. in length) smooth, firm, often slightly lobulated and presented a homogeneous, greyish-white cut surface. .
Microscopically the capsule of the lymph node was intact, but in part or. in the whole of the node the normal architecture was destroyed., Division of the node into lobules by bands of collagen or' reticulin was sometimes seen. The neoplastic tissue consisted of lymphocytes with .scattered abnormal retic~lllm cells. and multi-nucleated Hodgkin-type giant cells (Figure 1). The infiltration lacked the cellular Bleomorphism and fibrosis of classical Hodgkin's disease although ina few nodes occasjonal eosinophils and plasma cells were noted.
In. two of the fatal cases, repeat biopsies showed that Hie histQl9gical picture had progressed to that of Hodgkin's disease. One patiel)t suffered a rapid downhill ~o~rse
~ and died within one year yet the lymph node biopsy taken soon after first admissio)1 to hospital can only be classified histologically as reticular lymphoma. It is possible thatthis patient had already progressed to Hodgkin's disease when first seen and tha~ the gland removed at biopsy did not represent the most advanced lesion; unfortunately, no post-mortem examination was carried out..
Hodgkin's Disease , In 1832 Hodgkin published the first description of the disease now named after
him. Many different names have since been applied to Hodgkin's disease, lymphaden- . oma being one of the most common, but none is better tha)1 the eponymous one. It was some time after Hodgkin's paper before the characteristic histological features of the disease were defined by Greenfield(1878), Andrewes (1902), Reed (1902) and
· Lon,gcQpe (1903). Since then, many accounts of the pathological findings have been. published including a full and detailed monograph by Pullinger (1932). .
In the present series there were 87' patie~ts diagnosed on biopsy as suffering from · Hodgkin's disease.The biopsy material was usually from acervicallymph node, but was sO:qletimes from lymph nodes in other sites including the mediastinum; in one case, the biopsy was taken from lung,
,,,-'/' \
Macroscopically biopsy lymph nodes were moderately enlarged, encapsulated and · easily separated from each other. They were. usually firm, but not hard, and presented' a homogeneous greyish-white cut surface except in a few cases where . the surface
· was intersected by slightly depressed denser bands of fibrous tissue;
Microscopically there was complete or partial destruction of the normal lymph node architecture which was replaced by the characteristic! pleomorphic cellular infiltration. This infiltration always included lymphocytes and abnormal reticulum cells. The abnormal reticulum cells were large with irregular outlines and, large
\
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

(
, ,
28 Leaves from the AmlY Tumour Registry
vesicular nuclei containing a prominent eosinophilic nucleolus. In addition, multilobed and multi-nucleated' f9rms~the sQ-called, Sternberg-Reed giant cells*-were always found (Figure 2). Eosinophits were usually seen and were sometimes a pro-' rninent feature~ PolymorphOliuclear -le~cocytes' were frequently, present and plasma
/ cells were found in approximately half of the biopsies. Areas of necrosis infiltrated hypolymot:phs were noted in several lymph nodes. Fibrosis in varying degrees was common and .reticulin fibrils were usually increased in number.
In 'respect of a number of patients. more than .one biopsy was perforrned, and in some instances the second or subsequent biopsies showed a progression of the disease towards Hodgkin's sarcoma.
, Two biopsies showed the co-existence of tuberculosis and Hodgkin?s disease and one sarcoid and HodgKin's disease in the same lymph node. '
Post-mortem mah~rialfrom 15 ofthe patients with Hodgkin's disease was available for study. Examples of involvement of most internal organs were fOl.lnd, but the lymphnoaes, spleen and liver were the most commonly affeCted. Histologkally, there was a tendency for the'microscopical picture to approach that see~ in Hodgkin's sarcoma. One further example of co-existing tuberculosis was found' at necropsy, but no examples of torulosis were detected. In Olle case, the, origimll biopsy showed Hodgkin's disease but the post-mortem histology was that of histiocytic medullary reticulosis.
Hodgkin's Sarcoma The distrinction between Hodgkin's disease and Hodgkin's sarcoma is one of
degree dirly. Nine cases were classified as Hodgkin's sarcoma. The histological diagnosis was made on lymph,node biopsy in seven cases and on a surgically remoyed spleen in one case. The diagnosis in the nInth case was only made post-mortem. Post-mortem material was also available from five cases diagnosed by biopsy. The general histological changes ,in Hodgkin's· sarcoma were the same as those 'seen in Hodgkin's disease,but the degree of activity was greater. The cdls were llQi"e b~a~r~, multi-nucleated cells more frequent, mitotic activity greater,' necrosis more frequent and fibrosi~ less commoQ.
Follicular Lymphoma The .diseasenow 'often referred to as ,iFol1kular Lymphoma" (Gall and Mallory
1942; Lumb 1954; Harrison 1960) was first· fully described by Brill, Baehr and Ros'tmthalin 1925: Other names ~hich have been used t6 design~te this condition include lymphoid follicular reticulosis (Roob-Smith 1938), giant follicle lymphoma (Jackson and Parker 1947), inacrofollicular lymphoma (Wright J956), giant follicula:r-lymphoblastoma (Hurst and Mey~r 1961) and Brill-Symmers disease. '
In the present series there were eight patientsin1respe.et of whom the histological diagnosis of follieular lymphoma was reasonably certain. The diagnosis was made on lymph node biOpSies in seven cases· and on a lymph node biopsy· and splenectomy speCimen in the eighth.
* These giant cells were first described by Greenf1eld in 1878.
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Slewarl
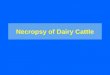
Figure 5. Lymphosarcoma. Lymph 1/ot/e. Sheet of small Lyn/plwc)'Jes. (H. and E. x 55)
Figure 6. Reticulum cell sarCQma. Lymph lIode. Sheet of re/;culum cells fel1dillg tu form a syncytium. (H. allll E. x 330)
29
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

\ /
-'\' ",
30 Leaves from the Army Tumour Registry \. .
Macroscopically it was sometimes p6ssibleto see an obvious follicular pattern on the cut. surfaces· of the lymph nodes. The surgically removed spleen weighed 365 g. and the cut surface displayed numerous enlarged malpighian bodies. -
" .. Microscopically the most obvious change' in \ the lymph nodes was a numerical and dimensionaJ increase in follic~es which were found. throughout the whole node in all cases (Figure 3). The foUicular pattern was well demonstrated in sections stained t.o show reticulum, ~he enlarged fDllicles being surrounded by compressed reticulum fibres (Figure 4). Reticulum was almost absent from the follicles themselves.
The centres of the follicles were composed of primitive reticular cells with largelymphocytes (lymphoblasts) in varying proportions while macrophage cells . with phagocytised particles wer~ either absent or present in ollly .small llUmbers. Mitotic activity in the centre of the follicles was usually slight. The paler staining centre .of each follicle was surrounded by a darker staining zone 'of small lymphDcytes.
In the spleen, the changes were fconfinedtD the white. pulp where fDllicles similar to those described above were nUl1lerDUS.
LymphosarcOlha, Reticulum Cell Sarcoma and MixedTu';;ours/
. It is cDnvenient to discuss these tumDurs together as they have many features in CDmmDn. The present series includes 14 patients with lymphosarcDma, '11 with reti~ culum cell sarcoma and tWD with mixed sarcomas. Reticulum cell sarCDmata of bone have not been included. . .
. The surgically r~m.oved specimens included lymph n.odes (15), skin (1), S.oft tissue (1), .ovary (1), tDnsil (1), st.omach (1) and, intestine (4). For .one patient a tentative diagnDsis .of lymphDsarcoma was made .on cytDIDgical examination of pleural fluid, and this diagnosis was confirmed at autopsy. In seven cases the diagnosis was not finally established until autopsy. ( . ' , .
MacroscopicallY the affected lymph nodes were enlarged and usually presented a unif.orm greyish-white appearance onthe cut surface.
Microscopically in lymphosarcoma, the architecture .of the lymph nodes was destroyed and replaced by sheets of lymphocytes -which vaded from small'tD large in different 'cases although they were usually of uniform size' in anyone biopsy (Figure 5). In a few instances a follicular pattern could be discerned suggesting that in these cases the. disease might have begun as a f.ollicular lymph.oma.
'In reticulum cell sarc.oma, the lymph.oid tissue was replaced by masses .of abn.ormal reticulum cells similar to those seen in Hodgkin's disease (Figure 6). In several tumours the cell boundaries merged to fDrm a distinct syncytium. Multi-nucleated reticul-iImcells were present in about half the biopsies. Reticulin was usually but
'not always, increased. Mitotic activity was obvious in most cases. The tw.o mixed tum.ours were c.omposed of mixtures of lymphocytes and reticulum
cells in approximately equal pr.oP.orti.ons. Post~mortem examinations were carried .out in respect of ten of the patients.
The lymph nDdes,- spleen, livyr, gastro-intesti'nal tract and kidneys were frequently found to be involved and examples were also seen of invasion of the lungs, bones,! supra-renals, pituitary., dura,- spinal cord and healt. \
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Stewart 31
It is interesting to note that lesions were found in the gastro-intestinal tract in no less than nine cases of the total of 27. In seven of the nine patients the operation or autopsy findings suggested that the tumours began as primary lesions in the gastrointestinal tract. Two of these cases involving the stomach have been fully described elsewhere (Stewart and Holman, 1959). The occurrence of primary lymphoid tumours in the gastro-intestinal tract has recently received renewed attention (e.g. Skrimshire 1955; Irvine and Johnson 1955; Azzopardi and Menzies 1960; Dawson et al. 1961).
Histiocytic Medullary Reticulosis
In 1939 Bodley-Scott and Robb-Smith described ten patients comprising four of their own and six from the literature, with a rapidly fatal disease characterized by fever, generalized lyn'lphadenopathy, splenomegaly and hepatomegaly. Anremia, leucopenia, purpura and jaundice were common in these patients. The principal pathological finding was aproliferation in the reticular tissue of histiocytic cells with much erythrophagocytosis.
Four patients with features. similar to those described by Bodley-Scott and RobbSmith -occurred among British military personnel during the period under review. One of these patients was diagnosed as Hodgkin's disease on the original lymph node biopsy, but the appearances at autopsy were those of histiocytic medullary reticulosis.
These cases will be described more fully elsewhere.
Histological Diagnosis
The first essential in the histological examination of a lymph node is the preparation of a good section. To achieve this, the biopsy must be performed without damage to the specimen; the gland must be cut longitudinally through the hilum; fixation must be adequate; the block must be properly prepared and a thin section cut and expertly stained.
There are many conditions in which lymphadenopathy is found and these must be distinguished microscopically from primary tumours of lymphoid tissue.
The commonest lesion in lymph nodes which must be distinguished from tumour are the non-specific reactions referred to as sinus catarrh and reactive hyperplasia. Reactive hyperplasia may closely simulate follicular lymphoma and it is sometimes extremely difficult, if not impossible, to distinguish between these two conditions. In attempting to come to a decision on a lymph node showing many follicles, the following histological changes would suggest a diagnosis of follicular lymphomaobliteration of the sinuses; condensation of reticulin fibres around the follicles; scarcity of mitoses and lack of macrophages with ingested nuclear material in the centre of the follicles.
Chronic lymphadenitis, especially if fibrosis is present, may closely resemble Hodgkin's disease and it is important to remember that a diagnosis of Hodgkin's disease should not be made unless the typical multi-nucleated cells are found.
Of the specific inflammatory diseases of lymph nodes, tuberculosis is the commonest. Caseating tuberculosis can be readily recognized and even the tubercles of non-caseating tuberculosis and the somewhat similar follicles of sarcoid are unlikely
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

32 Leaves from the Ar11'lY Tumour Registry
.to be diagnosed as neoplasms. The possibility that Hodgkin's disease and tuberculosis may co-exist in a lymph node must not be overlooked.
Protozoal diseases may mimic tumour. One of the ~ases of Leishmaniasis involving superficial ly~ph nodes described by Bell et al. (1958) was originally diagnosed histologically as "generalized reticulosis." The proliferating cells were, however, endothelioid in type and Leishman-Dqnovan bodies could be seen in some of the cells. The diagnosis was confirmed by lymph node aspiration and by the demonstration of the parasites in smears prepared from the freshly aspirated material
Certain fungal diseases may cause lymphadenopathy and if such a possibility is suggested sections should be stained by the P.A.S. method to reveal the microorganisms.
Sometimes difficulty may be experienced in distinguishing. between the various types ,of lymphoid tumours.
Before arriving at a diagnosis of reticular lymphoma, it may sometimes be necessary to consider the possibility of lymphosarcoma, follicular lymphoma or Hodgkin's disease. In reticular lymphoma and lymphosarcoma the nodes are diffusely infiltrated by lymphocytes but abnormal reticulum cells and Sternberg-Reed cells are not found in lymphosarcoma. Similarly, Sternberg-Reed cells are not seen in follicular lymphoma which may superficially resemble those reticular lymphomas which show a pseudo-
, follicular pattern. The distinction between reticular lymphoma and Hodgkin's disease is not clear-cut, as histologically the two conditions merge. Follicular lymphoma and lymphosarcoma can usually be distinguished, but it should be remembered that follicular lymphoma may progress to lymphosarcoma; rupture of the follicles and capsular invasion being evidence that such a change is taking place.
Many neoplasms metastasise to lymph nodes. In most instances the recognition of metastatic tumour will present no diagnostic problem, but anaplastic c.arcinoma may resemble reticulum cell sarcoma. Several cases were excluded from this series because the distinction between these two tumours could not be made with any degree of certainty, and more thim one case was rejected because the biopsy diagnosis of reticulum cell sarcoma was proved wrong by the finding of a bronchial carcinoma at autopsy.
Neuroblastoma may similate lymphosarcoma and reticulum cell sarcoma especially if rosette formation is scanty.
Finally, the leukremias may be confused with lymphoid tumours. This is not surprising as both are malignant proliferations of reticular tissue and there is some overlap between the two groups. Routine blood examination will generally suffice -to distinguish between leukremias and lymphoid tumours but occasionally in borderline cases even bone marrow biopsy does not completely resolve the problem.
Results and Prognosis
One of the main practical uses for any histological classification of lymphoid tumours, namely in prediction of the probable course of the disease, has already been mentioned. The results of the follow-up to mid-1962 of the 150 cases analysed by histological type are given in Table Ill.
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Stewart 33
TABLE IJI
RESULTS OF 150 CASES
Lost trace of Alive Dead Total
HODGKIN'S GROUP Reticular lymphoma ...... .. .. . ..... - 12 4 16 Hodgkin's disea~e ...... ..... 4 14 69 87 • Hodgkin's sarcoma ..... ...... . ..... - - 9 .9
FOLLICULAR LYMPHOMA 2 5 1 8 LYMPHOSARCOMA ..... ... - 3 11 14 RETICUl.,UM CELL SARCOMA ...... . ..... - 1 ,10 il HISTIOCYTIC MEDULLARY RETICULOSIS - - 3 3 UNCLASSIFIED ...... ~ ..... .....• . ..... . ..... - - 2 2
------Total 6 35 109 150
The Hodgkin's Group Of the 16 patients with reticular lymphoma 12 are still alive and four have died.
The high five- and ten-year survival rates for reticular lymphoma compare very ,favourably with the low rates for Hodgkin's disease and the even worse figures for Hodgkin's sarcoma (Table IV).
TABLE IV
. FIVE- AND TEN-YEAR SURVIVAL RATES-HODGKIN'S GROUP (calculated from firsLadmissidn to hospital)
5-year 10-year Histological Type
No. available Alive No. available Alive ..
RETICULAR LYMPHOMA 14 13 (93%) 8 5 (62%) HODGKIN'S DISEASE ...... 68 14 (21 %) 33 4 (12%) HODGKIN'S SARCOMA ...... - - - -
The average duration of the disease in the fatal cases was, reticular lymphoma 5!years (range 10 months to 11 years 4 months), Hodgkin's disease 21 years (range 3 months to 10 years 2 months) and Hodgkin's sarcoma 1 t years (range I month to 2 years).
Reference has already been made to the .. histological progression from reticular lymphoma to Hodgkin's disease in at least two of the cases. It is probable that such a change is part of the natural' history of the disease although it may not occur for many years during which the patient remains symptom free. Lumb and Newton (1957) drew attention to the fact that when eventually generalization of the disease
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

34 Leaves from the Army Tumour Registry
occurs the terminal phase is often short and mention has been made earlier of· one patient in this series who died within a year of first admission to hospital. It is not yet known whether treatment can ever prevent eventual deterioration in reticular lymphoma, but both Wright (1960) and Dawson and Harrison (1961) believe permanent cure is possible.
Although most of the army patients with Hodgkin's disease died in under five years from first admission to hospital, four survived for ten years and one is alive and well after 12 years.
Follicular Lymphoma The course of follicular lymphoma is slow. Only one patient of the eight is known
tobe dead and this patient died four years after his first admission; autopsy showed that the disease had progressed to lymphosarcoma. Several patients have· survived for five or more years (see Table V) and one for over 13 years. .
Lymphosarcoma, Reticulum Cell Sarcoma.and Mixed Cell Sarcoma The poor prognosis of these tumours is shown by the low survival figures (Table V).
The two patients with mixed cell sarcoma have been omitted from the Table; both died shortly after admission to hospitaL .
TABLE V
FIVE- AND TEN-YEAR SURVIVAL FIGURES-FOLLICULAR LYMPHOMA AND THE SARCOMATA
5-year I IO-year Histological Type -----
No. available Alive No. available Alive
FOLLICULAR LYMPHOMA 7 6 (86%) 2 I (50%) LYMPHOSARCOMA 12 2 (16%) 6 -RETICULUM CELL SARCOMA 10 - - -
Conclusion The results of the follow-up of the cases reviewed in this paper can be briefly
summarized. Most of the patients with lymph node biopsies showing the histological picture of reticular lymphoma remained fit for many years although· a proportion progressed to Hodgkin's disease. Follicular lymphoma behaved similarly except that progression, when it occurred, was to lymphosarcoma. Cases diagnosed on biopsy as Hodgkin's disease usually ran a progressive course over a period of about two years but a proportion were dead within a shorter time while others remained fit for several years. A histological diagnosis of Hodgkin's sarcoma, lymphosarcoma and reticulum cell sarcoma was usually associated with fairly rapid clinical deterioration.
These results show that the prognosis in the different types of lymphoid tumours varies considerably. It is, therefore, worth while attempting to classify these tumours
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from

P. D. Stewart' 35
on a histological basis as this gives some indication of the likely course of the diseas.e. Because exceptions to the. general pattern outlined above are by no means ,rare, a prediction based on histologiCal appearances may prove unreliable in any particular case.
ACKNOWLEDGMENTS
I am grateful to Sir Stanford Cade, Mr. T. M. Prossor, Dr. K. A. Newton, Miss P. Wheatley, Dr. G. Lumb and Dr. D. H. McKenzie, for assistance in many ways; to the civilian pathologists who kindly sent me slides; to the radiotherapists, clinicians, general practitioners and others who gave me follow-up information, and to the technicians who assisted me. I am indebted to Miss M. Scott for much secretarial assistance.
(The author also wishes to acknowledge the assistance of several serving officers and civilians employed by the War Department. It is regretted that we are not permitted to publish their names.Editor.)
REFERENCES
ANDREwEs, F. W. (1902). Trans. Path. Soc. London, 53, 305. AZZOPARDI, J. G., and MENZIES, T. (1960). Brit. J. Surg., 47, 359. BELL, D. W., CARMICHAFL, J. A. G., WILLIAMS, R. S., HOLMAN, R. L., and STEWART, P. D. (1958),
Brit. med. J., 1, 740. BODLEY-SCOTT, R., and ROBB-SMITH, A. H. T. (1939). Lancet, 2, 194. BRILL, N. E., BAEHR, G., and ROSENTHAL, N. (1925). J. Amer. med. Ass., 84, 668: CUSTER, R. P., and BERNHARD, W. G. (1948). Amer. J. med. Sci., 216, 625. DAWSON, I. M. P., CORNES, J. S., and MORSON, B. C. (1961). Brit. J. Surg., 49, 213. DAWSON, P. J., and HARRISON, C. V. (1961), J .. clin. Path., 14,219. EVANs, R. W. (1956). Histological Appearances of Tumours, Edinburgh. GALL, E. A., and MALLORY, T. B. (1942). Amer. J. Path., 18, 381. GREENFIELD, W. S. (1878). Trans. Path. Soc. London, 29, 272. HARRISON, C. V; (1952). J.Path. Bact., 64, 513. HARRISON, C. V. (1960). Recent Advances in Pathology, 7th Edition, London. HODGKIN, T. (1832). Med. Chir. Trans., 17, 68. HURST, D. W., and MEYER, O. O. (1961). Cancer, 14. 753. IRVlNE, W. T., and JOHNSTONE, J. M. (1955). Brit. J. Surg., 42, 611. JACKSON, H., and PARKER, F. (1944). New Engl. J. Med., 230, 1. JACKSON, H., and PARKER, F. (1947). llodgkin's Disease and Allied Disorders, New York. JELLIFFE, A. M., and THOMSON, A. D. (1955). Brit. J. Cancer, 9, 21. LONGCOPE, W. T. (1903). Bull. Ayer. Clin. Lab., I, 4. LUMB, G. (1954). Tumours of Lymphoid Tissue, Edinburgh. LUMB, G., and NEWTON, K. A. (1957), Cancer, 10,976. MARSHALL, A. H. E. (1956). Cytology and Pathology of the Reticular Tissue, Edinburgh. NEAL, J. B. (1954). Report on the First Five Years' Work of the Army Tumour Registry, 1948-1952,
The War Office, London. OGILVlE; H. (1954). Lancet, 2, 395. PuLLINGER, B. D. (1932). Rose Research on Lymphadenoma, Bristol. REED, DOROTHY, M. (1902). Johns Hopk. Hosp. Rep.', 10, 133. ROBB-SMlTH, A. H. T. (1938). J. Path. Bact., 47, 457. ROBB-SMlTH, A. H. T. (1947). Dyke's Recent Advances in Clinical Pathology, 1st Edition, London. SKRIMSHIRE, J. F. P. (1955). Quart. J. Med., 24, 203. STEWART, P. D., and HOLMAN, R. L. (1959). Brit. J. Surg., 46, 397. WRIGHT, C. J. E. (1956). Amer. J. Path., 32, 201. WRIGHT. C. J. E. (1960). J. Path. Bact., 80, 157.
guest. Protected by copyright.
on July 30, 2021 byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-109-01-05 on 1 January 1963. D
ownloaded from