Embed Size (px)
Citation preview

THERAPEUTIC RECREATION JOURNAL Vol. 38, No. 2, 133-147, 2004
Aromatherapy and Hand Massage:Therapeutic Recreation Interventionsfor Pain Management
Robin Kunstler, Re.D., CTRS, Fred Greenblatt, M.S., MPA, CTRS, andNereida Moreno, CTRS
Chronic pain is a major health problem among the elderly. Therapeutic recreation, with itsemphasis on quality of life and its utilization of a range of relaxation interventions, can be animportant component of a multidisciplinary pain management program. An investigation wasconducted of four older women residing in a skilled nursing facility, with histories of multiplehealth problems and chronic pain. They received one-to-one sessions of aromatherapy and handmassage from a therapeutic recreation specialist. The design of the study was a multiplesingle-subject withdrawal design. Pain was self-assessed on a modified Wong-Baker FacesRating Scale and participants' comments were recorded. A significant difference between pre-and post-sessions pain scores was found using an unbalanced randomized block design.Participants reported benefits of relaxation, pain relief, and improved sleep. The results of thestudy support the role of therapeutic recreation in providing pain management interventions.Implications for professional practice and research are examined.
KEY WORDS: Nursing Homes, Long-Term Care, Pain, Massage, Aromatherapy, Non-Phar-maceutical Pain Management
Robin Kunstler is Professor and Recreation Education Program Director, Department ofHealth Services at Lehman College of the City University of New York. Fred Greenblatt isDirector of Therapeutic Recreation and Nereida Moreno is a Therapeutic RecreationSpecialist at the Jewish Home and Hospital in the Bronx, NY.
This project was funded by the National Therapeutic Recreation Society Research Support funds and theLehman College Shuster Fellowship Award Committee. The authors gratefully acknowledge their support,without which this project would not have been possible.
Second Quarter 2004 133

Pain management is one element of qualityof life that has been identified as most impor-tant to people as they age (Levine, 2000).Although people over sixty-five are morelikely to experience chronic pain than youngeradults, pain relief is more elusive for the el-derly (Gloth, 2000). Due to the misconceptionon the parts of both the elderly and theirhealthcare providers that chronic pain is anormal, unavoidable part of aging (AmericanGeriatrics Society, 1998; Young, 2003), peo-ple have been forced to suffer its enormousphysiological and psychological effects (Platt& Reed, 2001). Chronic pain, commonly de-fined as pain that persists longer than theexpected time frame for healing, or pain asso-ciated with progressive, nonmalignant disease,cannot be eradicated or cured in most cases(Ashburn & Staats, 1999). Chronic pain leadsto decreased movement resulting in passivityand dependence; decreased bodily contact thatalters relationships; and poor sleep and fatiguethat causes decreased concentration and socialinteraction (Varela-Burstein & Miller, 2003).Other effects include depression, moodswings, social isolation, sleep problems, anddifficulty in performing daily activities(Young). Estimates of pain problems in com-munity-dwelling elderly are 25 to 50%, and 45to 80% among nursing home residents (Gloth).In an extensive study, on pain in nursinghomes, Teno (2002) found a "high rate ofpersistent severe pain in all U.S. nursinghomes" (p. 1) with about one-sixth of nursinghome residents reporting experiencing dailypain.
Challenges of Pain ManagementAs improving the quality of life in long-
term care becomes the focus of regulatorybodies (Levine, 2000), pain management hasreceived increased attention and emphasis.Recognizing the extent and seriousness ofchronic pain in nursing home residents, theCenter for Medicare and Medicaid Services(CMS) launched a Nursing Home Quality Ini-tiative in the fall of 2002 to assess all medi-
care-certified nursing homes in the UnitedStates on ten quality indicators. One of thoseindicators is pain management, measured asthe percentage of residents with moderatedaily pain or excruciating pain at any time. In2001, the Joint Commission on Accreditationof Healthcare Organizations (JCAHO) issuedstandards for assessing and managing pain inlong-term care facilities, hospitals, homehealth agencies, and outpatient clinics (Acello,2000; Platt & Reed, 2001). Under the JCAHOstandards, all patients have the right to appro-priate pain assessment and management usinga pain assessment tool that is appropriate totheir age, culture, and medical conditions.Since, in most patients, chronic pain cannot beeliminated or cured, the goal of pain manage-ment is to alleviate or reduce pain to a levelthat is comfortable and acceptable to the pa-tient (Mosby, 1998).
Despite this attention to chronic pain, olderadults in nursing homes experience many bar-riers to pain management, both internal andexternal. Internal barriers include concernabout side effects of treatment, belief thatnurses are too busy to help, and fear of beingseen as a "complainer," a malingerer, or aburden to others. External barriers to painmanagement include lack of good relation-ships with healthcare providers; and staff'slack of knowledge about the characteristics ofchronic pain, lack of open-mindedness abouttreatment approaches, and lack of understand-ing of pain as a treatment priority (Davis,Hiemenz, & White, 2003). Pain treatment isalso complicated by the fact that many eldersin nursing homes have multiple medical con-ditions with depression in particular having atremendous impact on pain management(Gloth, 2000).
Role of Therapeutic Recreation inPain Management
Along with JCAHO and CMS, the Ameri-can Geriatrics Society (1998) has also issuedguidelines on managing chronic pain in theelderly, emphasizing the importance of an in-
134 Therapeutic Recreation Journal

terdisciplinary approach. The society recom-mended both pharmacological and nonphar-macological strategies. These strategies includebehavioral approaches, such as cognitive-behavioral therapy, patient education, exer-cise, biofeedback, and relaxation techniques,which can foster healthy actions on the part ofthe patient. Austin (2004) states that the mis-sion of therapeutic recreation (TR) is to useactivity, recreation, and leisure to help peopleovercome barriers to health and achieve theiroptimal level of well being. As vital membersof the interdisciplinary teams in nursing homes(Saul, 1993), recreation therapists activelyengage individuals in meaningful activitiesthat give them a sense of control and purpose,with emphasis on the individual's well-being(McGuire, Boyd, & Tedrick, 1999). Recre-ation therapists provide interventions such asmusic, meditation, breathing exercises, guidedimagery, aromatherapy, and simple massageactivities that promote relaxation and feelingsof well-being, as well as relieve pain andtension (Bartalos, 1993).
With increased attention to quality of lifeas a legitimate healthcare goal (Van Andel,1998), and promoting personal responsibilityfor one's health by exercising choice and con-trol in the healthcare environment (Austin,2004), recreation therapists assist clients inchoosing treatment that will meet their needs.As pain is always subjective (Darr, 2001), theclients' role in determining effective painmanagement techniques is crucial. Patient sat-isfaction and well-being are important out-comes in healthcare settings today (LaTorre,2003) and should not be overlooked in plan-ning and implementing pain management pro-grams. One study (Wittink, 2000) found thatelderly people themselves preferred massageand informal coping techniques for pain man-agement, such as distraction rather than med-ication and exercise. Informal techniques, suchas massage and distraction, are highly rated bypain specialists because they are inexpensiveto offer, easy to teach (Pinkowish, 2000) andare favorably regarded by patients (LaTorre).Although these techniques are not the exclu-
sive domain of recreation therapists, programsrelated to stress, coping, anxiety, and relax-ation are designated within the scope of prac-tice for recreation therapists as denoted bytheir inclusion in the content areas for thenational certification exam as a certified ther-apeutic recreation specialist (CTRS) (NationalCouncil for Therapeutic Recreation Certifica-tion, 1999). As quality of life may be thehealthcare outcome that recreation therapistshave the most potential to influence (Van An-del), TR could play an important role in aninterdisciplinary pain management program byoffering clients a choice of relaxation tech-niques to clients to address pain and discom-fort.
Relaxation TechniquesRelaxation techniques comprise a group of
therapeutic approaches that may be effectivein the treatment of chronic pain (Ashburn &Staats, 1999). Relaxation has been describedas a process that assists individuals to retreatmentally from their surroundings, while quiet-ing their thoughts, relaxing their muscles, andmaintaining a relaxed state for a sufficientperiod of time to decrease anxiety, tension,and pain (DeMarco-Sinatra, 2000). Relaxationtechniques have been found to bring heart rate,blood pressure, and respiration under control(DeMarco-Sinatra).
One relaxation technique that may haveboth emotional and physical benefits for nurs-ing home residents is aromatherapy (Cerrato,1998). Aromatherapy is the therapeutic use ofessential oils to enhance relaxation, stimula-tion, and immune response (Jones, 1999).Most current studies show that essential oilsare safe and that clients respond to them in apositive, favorable manner (LaTorre, 2003).Elderly patients may benefit from aroma-therapy (Brett, 1999) as it eases or reduces theuse of sleeping pills and increases patients'ability to care for themselves (Robinson,2003). Studies have shown that use of essen-tial oils reduced anxiety and improved qualityof life in cancer patients (Cerrato); relievedsigns of distress, anxiety, and agitation in nurs-
Second Quarter 2004 135

ing home residents with Alzheimer's disease(Brown University, 1998); significantly re-duced agitation, without producing the sideeffects that may come with the use of drugs, inpeople with dementia (Futurist, 2003); andhelped one very anxious nursing home resi-dent who could not sleep to develop goodsleep patterns (Healthcare Review, 2001).Buckle (1999), in her review of nine studiesutilizing aromatherapy to address pain in arange of patients, found that subjects reportedpositive effects including perceptions of re-duction in pain, improved sleep patterns, andimproved ability to cope. She suggests there issufficient evidence to demonstrate that aroma-therapy can play a complementary role in painmanagement (Buckle). Within the aroma-therapy literature, lavender is considered agood general essential oil to use. Research onlavender has shown some promise in its effi-cacy in reducing analgesia and heart rate andincreasing ability to cope (Buckle). It has alsobeen found to promote an overall sense ofwell-being (LaTorre).
Massage is another relaxation techniquethat can address chronic pain, improve sleep,reduce fatigue, and enhance a state of relax-ation (Pinkowish, 2000). In a quasi-experi-mental study of 41 cancer patients, it wasfound that massage led to significant decreasesin pain and symptom distress and improve-ments in sleep (Smith, Kemp, Hemphill, &Vojir, 2002). Brett (1999) found that handmassage was very therapeutic and beneficialfor muscles and joints in the care of olderpeople. Massage has been noted to foster com-munication among recipient and provider andproduce a sense of well-being. This could beparticularly valuable for individuals with lim-ited opportunities for physical contact, such asnursing home residents (Vickers, Zollman, &Reinish, 2001). Massage provides the benefitsof one-on-one attention and a relaxing andcalming effect that produces lessened anxietyand confusion (Healthcare Review, 2001).Brownlee and Dattilo (2002), based on theirreview of current research on the use of mas-sage, concluded that massage is effective in
reducing pain, anxiety, and muscle tension;and that some basic Swedish massage tech-niques can be learned and easily performed byrecreation therapists in order to assist individ-uals in reducing anxiety, relieving pain, andovercoming barriers to leisure participation.
Combining two or more relaxation tech-niques has been found to be very beneficial inpain management. "Often it is the blend ofsmell, touch, and human interchange thatappear to create the best outcome" in thetreatment of pain (Buckle, 1999, p. 44). Forinstance, Jones (1999) reported that aroma-therapy can be combined with massage toreduce anxiety, depression and stress, and alterpain perceptions. Likewise, a relaxation groupthat used combined modalities (i.e., aroma-therapy, exercise, music, and stretching) andwhich was co-led by a recreation therapist anda social worker led to reduced confusion andfrustration in elderly nursing home residentswith Alzheimer's disease (Brown University,1998).
While research has validated the use ofrelaxation techniques in addressing chronicpain and related problems, there is a need forfurther research to validate the effectiveness ofvarious techniques (DeMarco-Sinatra, 2000),especially with the elderly in whom chronicpain is excessive. Little has been reported inthe therapeutic recreation literature on painmanagement in nursing home residents or onthe use of aromatherapy and hand massage.The purpose of this study, therefore, was toinvestigate the use of the relaxation techniquesof aromatherapy and hand massage as painmanagement interventions for nursing homeresidents with chronic pain.
Methodology
Research DesignThe design of the study was a multiple
single-subject ABABA research design. Ac-cording to Dattilo, Gast, and Schleien (1993),potential benefits of single-subject research areproviding data that can result in the develop-ment of more effective treatment and in-
136 Therapeutic Recreation Journal

creased accountability of TR service provi-sion. A single-subject design allow theresearcher to examine the impact of an inter-vention on one person's behavior and is auseful alternative to experimental design inclinical settings where it is difficult to formexperimental and control groups (Voelkl &Negley, 2001). Single-subject design "comple-ments the ability of TR specialists to meet theindividual needs of participants" (Dattilo,Gast, Loy, & Malley, 2000, p. 254).
Participant Selection and InformedConsent Procedures
The current study was conducted at an816-bed, not-for-profit, long-term care facilitythat provides a continuum of comprehensivecare including skilled nursing, sub-acute care,and community outreach services in NewYork City. Selection criteria for participationlimited involvement in this study to the clientswho had the following characteristics: (a) res-ident of one of the skilled nursing units at thefacility, (b) a report of chronic pain on theirmost recent pain assessment conducted by thenursing staff, and (c) a minimum score of 24out of 30 on the Mini-Mental Status Exam(MMSE). The MMSE is a quick screening toolused to evaluate cognitive functioning andevidence of dementia in people over sixtyyears of age. A score of 24 out of 30 isconsidered normal on the MMSE and was thequalifying score mandated by the facility'sInstitutional Review Board for participation inthis study. This score was mandated to assurethat those who expressed interest in participat-ing were "legally" capable of understandingand providing informed consent to participatein a research study.
Participant RecruitmentFlyers that clearly outlined the purpose,
procedures, benefits, and risks associated withthe study were posted and distributed through-out the skilled nursing units. The flyer wasdesigned to be both culturally appropriate andaccommodating to the participants based on
their disability (e.g., large print flyers, Spanishversions). Those interested in participatingwere directed to contact the Director of Ther-apeutic Recreation. Upon expressing their in-terest in participating, they were given theMMSE to verify their eligibility. Informedconsent was obtained from those who scored24 or higher.
Pain Assessment ProceduresPatient self-reports of pain is considered
the single most reliable assessment tool avail-able to quantify the existence and intensity ofpain (Platt & Reed, 2001). The facility's painassessment includes a modified Wong-BakerFaces Rating Scale (Mayer, Torma, Byock, &Norris, 2001). This scale features a series offacial expressions, accompanied by a four-point numeric rating, and serves as a basicmethod of communication about pain. Elderlynursing home residents indicated that a painrating scale allowed them to more effectivelydescribe their pain to nursing staff and that theFaces Scale was easier to use than other scales(Carey et al, 1997). The Faces Scale has beenfound to be an effective measure of pain incognitively intact elderly (Agarwal, 2002) ashas the use of a four-point pain scale (Smith etal., 2002). Wong (2002) demonstrated initialconstruct validity of the scale with an adultpopulation, ages 21 to 67, as compared to awell established numeric pain rating scale.
General Description of ParticipantsFour residents, who met the eligibility cri-
teria, agreed to participate in the research. Allparticipants were female, reflecting the com-position of the residents of the facility. Thepredominance of females in the intervention isalso consistent with the fact that older womenare more likely than older men to report pain(Varela-Burstein & Miller, 2003). Their ageswere 60, 63, 63, and 90. All four were activeparticipants in a wide range of recreation pro-grams in the facility, both on and off unit. Twoparticipated off-unit on a daily basis, and twoapproximately every other day. Although three
Second Quarter 2004 137

of the women were under 65 years of age, theywere typical of most older nursing home res-idents, in having at least one chronic condi-tion, such as arthritis, hypertension, heartdisease, visual difficulties, cerebrovasculardisease, and diabetes (Gloth, 2000). Two ofthe participants reported chronic pain, one re-ported acute head and back pain and sinusproblems, and one participant complained ofpain that made her body ache all over. All fourparticipants were routinely taking medicationfor pain (e.g., approximately 75% of the time).They were reported by nursing to have "fair"sleep patterns. Two participants had additionaldiagnoses of depression, another participantwas described by nursing as anxious and thefinal participant was described as irritable.
Data CollectionPain data were collected by the CTRS im-
plementing the study. Participants were pre-tested and post-tested on the Faces Scale dur-ing each session in the baseline andintervention phases. Prior to and at the conclu-sion of each session, participants indicated theface that corresponded to their self-assessmentof pain, scored as 0 (no pain), 1 (mild), 2(moderate), and 3 (severe). When a participantdescribed her pain as between two ratings, itwas recorded with a .5 interval.
Baseline data was collected twice in theweek prior to the onset of the intervention.Following the baseline phase (Al), the four-week treatment condition was initiated. A self-assessment of pain was collected before andafter each of the 12 treatment sessions (threetimes a week for four weeks) during thisphase, labeled the first intervention phase(Bl). Self-assessment of pain was again col-lected on two separate occasions during thewithdrawal phase (A2). This pattern of datacollection was again followed during the sec-ond intervention phase (B2) and the secondwithdrawal phase (A3). In addition, the CTRSrecorded her observations of the participantsand their comments to her regarding theirresponses to the treatment.
Intervention ProceduresThe CTRS designed and implemented the
intervention, based on her training. She hadcompleted a 100-hour certificate program inaromatherapy and was certified in refiexology.Reflexology uses finger pressure on the handsand/or the feet to affect change in other partsof the body (Brownlee & Dattilo, 2002) andmay incorporate hand massage techniques.During the intervention phases, each partici-pant received an individualized, fifteen minutehand massage and aromatherapy sessionthree times a week for four weeks in the lateafternoon or early evening hours. Each indi-vidual's contact with the CTRS was approx-imately thirty minutes. The sessions wereheld in the resident's own room and theCTRS took time to assure a soothing envi-ronment was created (e.g., lights lowered,the door closed to minimize interruptions,materials like massage cream and diffuserwithin easy reach, resident and CTRS incomfortable sitting positions).
In the conventional healthcare setting, mas-sage can be limited to the hands, head, or back,with the patient sitting in a chair fully clothed(Vickers, Zollman, & Reinish, 2001). This wasthe massage procedure followed in this study.For the massage, the CTRS used the resident'sown brand of hand cream to avoid allergicreactions. Latex gloves were worn by theCTRS, in accordance with the facility's uni-versal precautions procedures. After ratingtheir pain levels on the Faces Scale, residentstold that they could close their eyes if theywished, reinforcing the principles of partici-pant control and choice in the process. TheCTRS then used the verbal cue "relax" andencouraged residents to breathe deeply andsteadily. She began the massage by holdingeach resident's hand, palm down, in both ofher own hands and stroking outward in acirculation motion. The massage then ad-vanced to each resident's wrist and continuedwith a deep stroking pattern up to their elbow.The CTRS also used her fingertips to massageeach resident's fingers. Toward the end of the
138 Therapeutic Recreation Journal

massage intervention, the CTRS gave eachresident a two-minute notice prior to ending ofthe session. At the session's end, each residentrested without speaking for five minutes, thenthe CTRS asked how they felt and to againindicate their pain level using the Faces Scale.Preparation and procedures for the interven-tion are presented in Table 1.
Data AnalysesAnalysis of single-subject research relies
on graphic displays to allow for visual inspec-tion of data. Changes in magnitude and levelof the dependent variable are readily observ-able when data is graphed. A magnitudechange refers to the difference between theaverage value of the dependent variable in onephase compared to the average value of thedependent variable in the following phase(e.g., mean value during baseline compared tomean value during intervention phase). In con-trast, a level change refers to the immediateshift in the value of the dependent variable atthe end of one phase compared to the value ofthe dependent variable at the beginning of thenext phase. Level changes examine differ-ences occurring immediately at the start orstopping of an intervention; while magnitudechanges examine differences in the averagescore between two phases. Post-session paindata from the four cases in this study weregraphed and examined for changes in magni-tude and level of the pain ratings. In addition,statistical analysis comparing the pre-sessionand post-session pain ratings of the four sub-jects utilizing an unbalanced randomizedblock design (unbalanced due to missing datafor one participant who chose to not partici-pate in the second intervention phase) wereconducted.
ResultsBecause of the single-subject design em-
ployed, results are presented via a brief casestudy of each participant. Each case includesdiscussion of the client's pain rating duringbaseline, intervention, and withdrawal phases,
as well as their qualitative comments regard-ing the intervention's effectiveness, providedby participants at the end of their sessions.This presentation is then followed with a sta-tistical analysis of changes in pre- to post-session pain ratings during the two interven-tion phases.
Case ofMCMC was a 60-year old nurse who was
admitted to the nursing home after 2 weeks incoma, with a history of low blood pressure,anemia, a ruptured disc, cervical arthritis, os-teoporosis, spastic bladder, and chronic pain.MC had had 10 major surgeries. Her majorpain complaint was chronic back pain due toarthritis and the ruptured disk. She was re-ported by nursing to have an irritable mood, befearful and to have a fair sleeping pattern. Shewas prescribed Ultram for pain and took itroutinely.
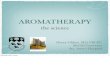
As can be seen in Figure 1, her averagebaseline (Al) pain rating was 1.75 on theFaces scale. With the onset of the first inter-vention phase (B1), an immediate level changeis observed indicating an increase in MC'sperception of pain. This increase is observedthroughout the first intervention phase with anaverage mean pain score of 2.5 during thisphase.
Contradictory findings in terms of level andmagnitude of change are observed in the painratings during the withdrawal phase. MC'sinitial pain rating during the withdrawal phasewas higher than her last pain rating during theintervention phase suggesting that an increasein pain perception occurred when the interven-tion was withdrawn. However, MC's pain rat-ing decline during the following week, despitethe absence of the intervention and no levelchange in pain perception occurred with theonset of second intervention phase.
Visual inspection of the data set as a wholesuggest that MC's level of pain was fairlyconsistent (i.e., at the moderate to high level)across all phases. Although MC said she stillfelt pain, she reported feeling relaxed at the
Second Quarter 2004 139

Table 1.
Preparation and Procedures for Aromatherapy and Hand Massage
Preparation for the recreation therapist
• Recreation therapists should be suitably dressed in comfortable, but professional-looking,clothing such as slacks and lightweight top that are not revealing. Tops with tight or full-length sleeves are preferred.
• Recreation therapist's hands should be groomed with nails trimmed, short, andunpainted. They must be washed prior to treatment and the use of hand cream to softenthem is advised. All jewelry should be removed from the hands and wrists, as well aslong necklaces and dangling earrings. Long hair should be tied back to avoid inadvertentcontact with the resident.
• Recreation therapist should bring clean towels, large and small pillows for wrist, arm,back positioning and support, essential oils and diffuser, latex gloves, and othernecessary supplies to create a soothing environment for the intervention.
Preparation of the environment
• Room should be warm, airy, and have good ventilation.• The door should be closed to ensure privacy, provided this is consistent with facility
guidelines.• Televisions, radios, and telephones should be turned off to avoid interruptions.• The room should be large enough to arrange so that client and recreation therapist do not
feel crowded while conducting the intervention.• Lights should be dimmed.• Do not disturb, session in progress sign should be posted to prevent interruptions.
Procedures
• Make sure the client is comfortable (i.e., warm enough, in a comfortable position,pillows placed wrists, arms, back for support, if needed)
• Make sure the you (recreation therapist) are positioned comfortably so to effectivelyprovide intervention:• Position yourself comfortably in your chair with good posture to avoid backache and
fatigue.• Sit facing the client with your chair on the left side of the client.• Avoid any contact with the resident's body except his/her hands and arms.• Perform hand exercises for flexibility, strength, relaxation, and sensitivity.• Put on latex gloves, if needed, for universal precautions.• Take a minute to breathe deeply and slowly.
• Use client's own brand of hand lotion or cream to avoid allergic reactions.• Support client's wrist at all times; may use a pillow.• Administer massage.• Give client two-minute notice of conclusion of massage.• Allow client to rest for several minutes before restoring original environment.
end of sessions, especially because she liked 24 interventions sessions that occurred in boththe smell of lavender. MC did not complain of phases. MC reported that the interventionpain and actually fell asleep during 11 of the helped her sleeping and she also believed it
140 Therapeutic Recreation Journal

3.5 -
3 •
2.5 -
= 2 •
°- 1.5 •
1 •
0.5 •
0 •
Al
/
/
I
Bl
Y \ . . / v v
A2 B2
A,/\.../\J..\
Al
7 9 11 13 15 17 19 21 23 25 27 29
Sessions
Key: . . . - Mean, Al= baseline, Bl = first intervention phase, A2 = first withdrawal phase, B2= second intervention phase, A3=second withdrawal phase
FIGURE 1. MC'S PAIN RATINGS.
improved her circulation because her handsfelt warm.
Case of TS
TS was a 63-year-old office supervisor whohad a right cerebral vascular accident at theage of 54. She had left-side hemiparesis, worea brace on her left leg, and used a motorizedwheelchair for mobility. She also had a historyof diabetes and hypertension. She was re-ported to have moderate chronic pain anddepression. Her chronic pain was due to arthri-tis and left hemiparesis that resulted in saggingand pinching of her left arm and neck muscles.TS also had a chipped tail bone that preventedher from shifting her position. She was pre-scribed Neurotin for pain and used it routinely.
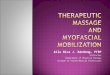
Her mean pain rating at baseline (Al) was1 on the Faces scale (Figure 2). As can be seenin Figure 2, TS displayed significant levelchange in her pain score with the onset of thefirst intervention phase (Bl) reflecting a de-cline in her pain score. She also had a declinein magnitude during this phase with a meanpain score of .7 during this phase. A levelchange increase in pain rating is seen duringthe withdrawal phase (A2), with a subsequentdecline in pain rating with the onset of thesecond intervention phase (B2). Magnitude
changes indicative of the intervention's effec-tiveness in decreasing pain perceptions for TSare also observed during each interventionphase.
Visual inspection of the data set as a wholesuggests that the intervention was effective inreducing pain perceptions for TS. Her painratings were slightly lower during the inter-vention phases as compared to the baselineand withdrawal phases. These findings areconsistent with TS's qualitative comments. TSstated that she felt "great" after the interven-tion sessions, with a feeling of relaxation last-ing the rest of the day and through the night.She also reported sleeping better and longer atnight. TS also stated that she felt the interven-tion was effective in improving her breathing(sinuses were clearer) and her neck pain de-creased. Like MC, TS enjoyed the smell oflavender and reported looking forward to eachsession as they diverted her attention from herpain.
Case ofDFDF was a 63-year old factory worker who
had a right cerebral vascular accident one yearprior to her admission to the nursing home.She had a history of high blood pressure,depression, anxiety, anemia, and gastritis. Due
Second Quarter 2004 141

9 11 13 15 17 19 21 23 25 27 29
Key: •" • = Mean, Al= baseline, Bl = first intervention phase, A2 = first withdrawal phase,B2 = second intervention phase, A3=second withdrawal phase
FIGURE 2. TS'S PAIN RA TINGS.
to her left-side paralysis, DF used a wheelchairfor mobility. DF developed carpal tunnel syn-drome from using her wheelchair affecting herfingers, wrist, and shoulder. She also was re-ported to have head and back pain and sinusproblems. Her chief pain complaint was thecarpal tunnel syndrome. DF was prescribedCelebrex and Neurotin for pain and used itroutinely.
As can be seen in Figure 3, DF reportedlevel change declines in her pain score duringthe first intervention phase (Bl) and levelchange increases in her pain score during bothwithdrawal phases (A2 and A3). DF also hadconsistent changes in the magnitude of herpain scores during each phase with notabledeclines in average pain scores occurring dur-ing the first (Bl) and second (B2) intervention
Key: • • • • = Mean, Al= baseline, Bl = first intervention phase, A2 = first withdrawal phase,B2 = second intervention phase, A3=second withdrawal phase
FIG URE 3. DF'S PAINRA TINGS.
142 Therapeutic Recreation Journal

phases. DF's pain ratings changed from anaverage pain rating of 2 during baseline to 1during the first intervention phase. During thefirst withdrawal phase, there was no change inthe magnitude of DF's pain rating (it remainedat 1); however, further declines in the averagepain rating occurred during the second inter-vention phase (it declined to .7). This declinewas followed by a dramatic increase (to 2) inaverage pain ratings during the second with-drawal phase (A3).
Visual inspection of DF's data set as awhole suggests that the aromatherapy andmassage intervention was effective in decreas-ing her perceptions of pain. Qualitative com-ments support this conclusion. DF reportedthat she felt more relaxed and had less painafter interventions. She noted that during theintervention sessions her mind wandered—asign to her that she was not focused on herpain. She also fell asleep in two of the ses-sions. She also stated that she felt her breath-ing and sleep improved. She believed that theintervention was more effective in relievingher pain than other interventions she had re-ceived in physical therapy (i.e., hot com-
presses). Like the other participants, DF re-ported enjoying the smell of lavender.
Case of ATAT was a 90-year old retired nurse's aide
with a history of diabetes, hypertension, cer-vical cancer, and neuropathy. She experiencedchronic pain in her legs, knees, and hands dueto arthritis, and more recently in her eyes dueto glaucoma. She was reported to have a de-pressed mood and described her body as ach-ing all over—"nothing helps." She routinelytook Neurotin and Tylenol for pain.
AT only participated in the research upuntil the beginning of the second phase of theintervention. At this point, AT declined toparticipate any further due to the fact that shehad recently received a diagnosis of glaucomaand did not "feel up to it." Despite AT'sdecline, her data from the baseline through thefirst withdrawal phase, suggested that the in-tervention was effective in reducing AT's per-ceptions of pain (Figure 4). A significantchange in level is observed in the transitionfrom baseline (Al) to the first phase of the
Key: • • • • = Mean, Al= baseline, Bl = first intervention phase, A2 = first withdrawal phase
FIGURE 4. AT'S PAIN RATINGS.
Second Quarter 2004 143

intervention (B), with an associated decline inmagnitude in each phase (i.e., from 1.5 inbaseline to 1.0 in the first intervention phase).
AT stated that following intervention ses-sions, she felt good, relaxed, and sleepy. Shestated her pain had either decreased or disap-peared. She found the sessions to be helpful indistracting her attention from the pain andimproving her breathing.
Summary of CasesThree of the 4 participants (TS, DF, and
AT) showed an immediate response at theinitiation of the first intervention phase asindicated by level changes in between thesephases (Figures 2-4). These same participantsalso had magnitude declines during the inter-vention phases suggesting that aromatherapyand massage was an effective pain manage-ment intervention for these participants. Table2 contains the mean scores for each participantduring each phase of the study.
The only participant for whom the inter-vention did not appear effective was MC.Interestingly, unlike TS, DF, and AT, she wasnot hypertensive; rather, she had a history oflow blood pressure. She was also unlike theother participants in that her major pain com-plaint centered on back pain. The other partic-ipants may have had back pain, but they alsoreported hand, arm, neck, and shoulder pain.These differences may partly explain the dif-ferences in MC's response to the intervention.
Table 2.
Mean Pain Ratings of Participants in AllPhases
Case
MCTSDFAT
Al
1.75121.5
Bl
2.5.7
1.11
A2
2.0111
B2
2.1.7.9
A3
212
Al = Baseline; A2, A3 = Withdrawal; Bl,B2 = Intervention.
Summative evaluation of the qualitativedata also supports the effectiveness of theintervention. Regardless of how participantsnumerically rated their pain after each session,they all reported feeling more relaxed andsleeping better following the interventions.They described their sleep as deeper, moresound, less restless, and longer. Their reportsof sleep patterns were verified by nursing staff.Three of the participants said their pain wasrelieved or decreased, 3 said their mind wasdiverted from the pain, and 3 said they likedthe aroma.
Statistical Analysis of the Pre-PostSession Pain Scores
While the graphic analysis of the data pro-vided some support for the effectiveness ofthis TR intervention, statistical analysis of thepre-post session pain scores would providefurther support. A 2 (time) by 2 (interventionphase) unbalanced randomized block designwas computed using the average pain ratingscores from the 83 intervention sessions thatwere conducted with the 4 subjects. Diagnos-tic checks of the underlying assumptions asso-ciated with this statistical analysis included anexamination of the variance distribution of thescores (i.e., homescedaciticty) and the normal-ity of the residuals. No significant violations ofthe underlying assumptions for this analysiswere found.
A significant main effect for time, F (1,10.1) = 8.68, p < .01, was observed but nostatistical difference in average pre- and post-pain scores were observed for the interventionphase, F (1, 10.5) = 0.32, p > .57. Likewise,no statistically significant interaction effectswere found, F (1, 10.1) = 0.11, p > .74. Thesefindings indicated that clients reported statisti-cally significant declines in pain ratings frompre- to post-session, regardless of interventionphase. It can therefore be concluded that thearomatherapy and hand massage interventionwas effective in reducing participant's percep-tions of pain following a treatment session.
144 Therapeutic Recreation Journal

DiscussionThe purpose of the study was to investigate
the use of aromatherapy and hand massage astherapeutic recreation interventions for painmanagement. Limitations of the study in mea-suring pain are noted. One limitation may havebeen the use of the modified Faces Scale. Thefour-point scale did not produce much varia-tion in the ratings. Most ratings were 1 (mild)or 2 (moderate) and with a rating of 3 (severe)given only four times. Use of other scales infuture studies may be warranted. Another lim-itation was the number of times pain levelswere measured during the baseline and with-drawal phases. In future research, more thantwo baseline ratings should be taken so that amore stable measure of pain prior to treatmentis obtained.
Another limitation of the study is the factthat all participants were receiving pain med-ications prior to, during, and subsequent to theinterventions. While the study's single subjectdesign would control for the effects of medi-cation as each participant serves as their owncontrol, the researchers did not assess ifchanges in the patterns of types of pain med-ications used occurred throughout the study.Future research should more carefully controlfor this variable.
All participants expressed satisfaction withthe techniques and the effects of relaxation,including improved sleep and the diversion oftheir thoughts from the pain. This supportsother studies that reported the effects of mas-sage on improving sleep and promoting asense of well-being (Brownlee & Dattilo,2002; Healthcare Review, 2001; Smith et al.,2002).
In some respects these four participantswere atypical of the current nursing homepopulation. Three of the four participants werein their early sixties. The average age of theresidents of this facility was 86 years. How-ever, they had the multiple health problemstypical of elderly nursing home residents andpain in nursing homes affects residents of allages. Another difference was that while an
estimated 85% of the residents of the facilityhad some evidence of dementia, these partic-ipants did not. Future research with older res-idents and those with dementia is recom-mended. When working with adults withdementia it is important to observe and docu-ment nonverbal indicators, such as behaviorchanges, facial expressions, and body lan-guage (Acello, 2000). In the present study,nonverbal indicators presented powerful evi-dence of pain relief (i.e., falling asleep, morerelaxed posture), and could be an interestingarea for future research.
An unexpected outcome of this study thatalso warrants further research was the effect ofthe intervention on improving sleep patterns.Falling asleep in a nursing home during theday may be attributed to overmedication orboredom. However, this day-time sleepingpattern was not typical for the study's partic-ipants. Rather, their high and consistent activ-ity level would suggest they were not bored orconstrained in their activities due to overmedi-cation. MC was a member of the resident'scouncil; she and TS were also active as vol-unteers in the nursing home, and AT spentmuch of her time socializing in the nursinghome cafe, so it is interesting to note that theseparticipants often fell asleep during the inter-vention, a behavior that was atypical for them.
Additional research could be done on theuse of relaxation techniques in therapeutic rec-reation with diverse groups. Other populationsof all ages and in all settings have been shownto benefit from relaxation techniques in theareas of pain management and anxiety reduc-tion (Brownlee & Dattilo, 2002). Combiningaromatherapy and hand massage with music,guided imagery, and/or relaxation breathingtechniques, established methods of TR prac-tice, are other areas of potential study. Animportant consideration to explore would bedelivering the intervention in groups. Practi-cally speaking, one-to-one intervention is la-bor-intensive. Could participants themselves,and/or their family members, be trained inbasic techniques and a group be held understaff supervision? Another consideration is
Second Quarter 2004 145

length of sessions. Although short sessions doprovide some benefits, longer and more fre-quent sessions may produce more intense andmore lasting outcomes (Smith et al., 2002).
Successful delivery of programs such asmassage and aromatherapy depend on supportfrom upper management and the unit level intheir willingness to try out new ideas (Austra-lian Nursing Federation, 2003). It is the man-ager's role to establish an organizational cul-ture that recognizes the importance of painmanagement (Darr, 2001). The JCAHO painmanagement standards also require a pain au-dit, which is an assessment of pain manage-ment methods and tools. A range of painmanagement approaches should be offered.Multidisciplinary collaboration and communi-cation are essential if complementary and al-ternative techniques are to play a more signif-icant role in symptom control and painmanagement (Scrace, 2003). The successfuluse of relaxation techniques by the CTRS inthis study lends support to the inclusion oftherapeutic recreation as part of a comprehen-sive pain management program.
TR can offer participants a choice of relax-ation techniques that are carefully planned toincrease their level of comfort and sense ofcontrol over their pain. The significant de-clines in pain ratings from before to after thesessions that were found in this preliminarystudy support aromatherapy and hand massageas contributors to feelings of well-being. Out-comes of relaxation, improved sleep, reducedanxiety, and mental distraction are not onlyquantifiable, but are also subjective indicatorsof quality of life. The comments of the partic-ipants indicated they experienced the benefitsof the intervention into the following day andwere eager to resume the treatment long afterthe study ended.
Hand massage has physical and emotionalbenefits, allowing a participant to experiencephysical contact in an atmosphere of respectand dignity. "Aromatherapy allows the patientand carer to 'be' with one another and perhapsis one of the 'kindest' therapies we can offer"(Buckle, 1999, p. 50). Respect, dignity, and
kindness are values of therapeutic recreationevident in our goal of providing holistic ap-proaches that are accessible to all. An impor-tant finding of this study may be to remind usto focus on the quality of the TR experience,the joy and meaning that comes from partici-pation, as well as the quantitive outcomes wedocument after the activity is over.
References
Acello, B. (2000). Meeting JCAHO standardsfor pain control. Nursing, 30, 52.
Agarwal, K. (2002). Assessment of pain in pa-tients with dementia. Pain Relief Connection, 1(9).
American Geriatrics Society. (1998). Combatingpain in older persons: New recommendations. Con-sultant, 38, 1925-1928.
Ashburn, M., & Staats, P. (1999). Managementof chronic pain. The Lancet, 353, 1865-1875.
Austin, D. (2004). Therapeutic recreation: Pro-cesses and techniques (5th ed.). Champaign: Saga-more Publishing, Inc.
Australian Nursing Federation. (2003). Thesweet smell of The Birches. Australian NursingJournal, 10(9), 31-32.
Bartalos, M. (1993). Work, health and creation:Aspects of the total person. Loss, Grief and Care, 6,7-14.
Brett, H. (1999). Aromatherapy in the care ofolder people. Nursing Times, 95(33), 56-58.
Brown University (1998). Relaxation techniquesbenefit AD residents. The Brown University Long-Term Care Quality Advisor, 70(10), 5-7.
Brownlee, S., & Dattilo, J. (2002). Therapeuticmassage as a therapeutic recreation facilitation tech-nique. Therapeutic Recreation Journal, 36, 369-381.
Buckle, J. (1999). Use of aromatherapy as acomplementary treatment for chronic pain. Alterna-tive Therapies, 5(5), 42-50.
Carey, S., Turpin, C , Smith, J., Whatley, J.,Haddox, D., & Hunt, A. (1997). Improving painmanagement in an acute care setting: The CrawfordLong Hospital of Emory University. OrthopaedicNursing, 16(4), 29-37.
Cerrato, P. (1998). Aromatherapy: Is it for real?RN, 61(6), 2-4.
146 Therapeutic Recreation Journal

Darr, K. (2001). The manager and pain controlfor patients. Hospital Topics, 79(4), 27-30.
Dattilo, J., Gast, D., & Schleien, S. (1993).Implementation of single-subject designs in thera-peutic recreation research. In M. Malkin & C. Howe(Eds.), Research in therapeutic recreation: Con-cepts and methods (pp. 181-206). State College:Venture Publishing, Inc.
Dattilo, J., Gast, D., Loy, D., & Malley, S.(2000). Use of single-subject research designs intherapeutic recreation. Therapeutic Recreation Jour-nal, 34, 253-270.
Davis, G., Hiemenz, M., & White, T. (2003).Barriers to managing chronic pain of older adultswith arthritis. Orthopaedic Nursing, 22, 149-150.
DeMarco-Sinatra, J. (2000). Relaxation trainingas a holistic nursing intervention. Holistic NursingPractice, 14(3), 30-45.
Futurist, (2003). Aromatherapy fights dementia.37(3), 2.
Gloth III, F. (2000). Geriatric pain: Factors thatlimit pain relief and increase complications. Geriat-rics, 55(10), 46-56.
Healthcare Review (2001). Therapies and posi-tive results: Evaluation of the use of touch, music,massage and aromatherapies in nursing homes.14(3), 24.
Jones, K. (1999). Clinical aromatherapy andtouch: Complementary therapies for nursing prac-tice. ANNA Journal, 26, 527.
LaTorre, M. (2003). Aromatherapy and the useof scents in psychotherapy. Perspectives in Psychi-atric Care, 39(1), 35-38.
Levine, K. (2000). The shift to palliative care.Contemporary Long-Term Care, 23(2), 27-29.
Mayer, D., Torma, L., Byock, I., & Norris, K.(2001). Speaking the language of pain. AmericanJournal of Nursing, 101(2), 44.
McGuire, F., Boyd, R., & Tedrick, R. (1999).Leisure and aging: Ulyssean living in later life (2nded.). Champaign: Sagamore Publishing.
Mosby's Medical, Nursing and Allied HealthDictionary (Edition 5). (1998). Mosby-Year Book,Inc.
National Council for Therapeutic RecreationCertification. (1999). Certification standards. NewCity: Author.
Pinkowish, M. (2000). Management of pain andother discomfort. Patient Care, 34(2\), 38-54.
Platt, A., & Reed, P. (2001). Meet new painstandards with new technology. Nursing Manage-ment, 32(13), 40-48.
Robinson, F. (2003). Complementary therapiesin primary care. Practice Nurse, 25(4), 14-16.
Saul, S. (1993). Meaningful life activities forelderly residents of residential healthcare facilities.Loss, Grief and Care, 6(4), 79-86.
Scrace, J. (2003). Complementary therapies inpalliative care: A literature review. Pediatric Nurs-ing, 15(3), 36-40.
Smith, M., Kemp, J., Hemphill, L., & Vojir, C.(2002). Outcomes of therapeutic massage for hospi-talized cancer patients. Journal of Nursing Scholar-ship, 34, 257-263.
Teague, M., McGhee, V., & Hawkins, B. (2001).Geriatric practice. In D. Austin & M. Crawford(Eds.), Therapeutic Recreation: An Introduction(3rd ed.) (pp. 2333-254). Needham Heights: Allyn& Bacon.
Teno, J. (2002). Now is the time to embracenursing homes as a place of care for dying persons.Innovations in End of Life Care, 4(2) www.edc.org/lastacts.
Van Andel, G. (1998). TR service delivery andTR outcome models. Therapeutic Recreation Jour-nal, 32, 180-193.
Varela-Burstein, E., & Miller, P. (2003). Ischronic pain a risk factor for falls among communitydwelling elders? Topics in Geriatric Rehabilitation,19, 145-160.
Vickers, A., Zollman, C , & Reinish, J. (2001).Massage therapies: Overview of techniques and ben-efits. The Western Journal of Medicine, 175, 202-213.
Voelkl, J., & Negley, S. (2001). Management,consultation and research. In D. Austin & M. Craw-ford (Eds.), Therapeutic recreation: An introduction(3rded.) (pp. 318-332). Needham Heights: Allyn &Bacon.
Wittink, H. (2000). Chronic pain management:A qualitative study of elderly people's preferredcoping strategies and barriers to management. Phys-ical Therapy, 80, 1049-1055.
Wong, D. (2002). Validity of a FACES painrating scale with an adult population. Wong on Web.www3.us.elsevierhealth.com/WOW/facesll.html.
Young, M. (2003). Chronic pain management inthe elderly. Patient Care, 34, 31-50.
Second Quarter 2004 147