Embed Size (px)
Citation preview

Acta Nedica Scandinavica. Vol. CXXVIII, fasc. 11, 1947.
From the Medical Department of the Frederiksborg County Hospital, Hillererd, Denmark.
Chief: Torben Andersen. M. D.
Arteritis Temporalis (Horton). (a Symptoni of a Benerslized Vascular Disease.)
A Survey and a Case with Glaucoma.
BY
TORBEN ANDERSEN.
(Snbmitted for publication October 21, 1946.)
On November 15th 1945 a manufacturer, aged 54 years, was admitted to the ward for observation for cerebral tumour (Case record No. 1520/45).
18 months before admission he was treated with massage and applic- ation of heat owing to rheumatic pain in the trunk and the extre- mities. The pain subsided, though not completely, until, at the end of September 1945, he suddenly got violent pain in the right side of his occiput without any known causation (infection, trauma, overwork). Later, the pain spread to the right temporal region, the right eye, right ear and right side of the upper part of the neck. The pain was partly constant, dull, throbbing, increasing when the patient strained a t stool, partly lancinating, convulsive. It was extremely violent, he often bumped his head against the bedside, she was on the point of being mad with pain)), still without any thoughts of suicide. He be- lieved that during a period he now and again had had a transient swelling of the right temporal region. He was treated with massage of the nuchal musculature for about 5 weeks, during which the pain was constantly increasing. Now there was also periodical misty vision and iridescent vision, and the patient felt a tension in his right eye. At this time his doctors got the suspicion that he might suffer from a cerebral tumour and, therefore, he was admitted to this hospital for examination. There had been no other cerebral symptoms. He had not had any subjective signs of fever (his temperature had not been measured). During the whole period of his disease he felt extremely exhausted, with a poor appetite and a loss of weight of about 10 kilos.
ll--’t71585. Acta wed. scund inav . Vol. C X X V I I I

152 TORBEN ANDERSEN.
In addition to the physical therapy he had been treated with vitamin B injections and large doses of anodynes, including scopolamine and morphine. Thus, on the day of admission, he had got an injection of 5 cg of morphine hydrochloride.
On admission he felt very distressed and somewhat confused owing to the large doses of narcotic he had been given; he was otherwise physically and mentally well-preserved, still, during the entire course of the disease, he had a tendency to weeping and was on the whole psychically unstable, in contrast with his previous habitus. The exami- nation (apart from that of the eyes) showed nothing abnormal, especi- ally no abnormal neurological signs, and no observations were made about the state of the temporal arteries despite palpation of the skull. When questioned later on, the patient believed that he could confirm that on this admission the temporal arteries were unaffected. The ophthalmologist, who was called in, a t once ascertained the presence of a bilateral glaucoma, most marked in the right eye.
The patient was then treated with instillation of pilocarpine into the eyes, sweating mantle and acetylsalicylic acid, 5 g in the 24 hours. The pain soon subsided and, after 12 days’ stay in hospital, the patient was discharged on Nov. 27th for continued treatment of the glaucoma a t home. When discharged, the patient only felt a slight grumbling in his right temporal region.
At that time our diagnosis was glaucoma essentialis. Still, we were well aware that this diagnosis did not satisfactorily explain why the sedimentation rate of the patient was highly increased, since the examination of the eyes was not suggestive of the presence of rheumatic iridocyclitis with a secondary glaucoma.
Two days after his discharge the patient did get renewed attacks of pain, now in both temporal regions, and of the same character as previously, however without any ocular pain. The patient also noticed that the pain increased synchronously with his pulse, and he observed that the vessels in both temporal regions (but especially on the right side) became highly swollen and tender. He was treated again with antineuralgics and massage in the nuchal region. The pain subsided gradually in the course of this treatment, but as he was anxious and depressed owing to his disease and felt alarmed because his sedimenta- tion rate was a t a very high level, the patient asked to be readmitted to the ward and was so on Jan. 5th 1946.
On his second admission he complained of intense pain in the right side of his head, localized to the parietal and temporal regions. Without any other treatment than rest in bed and the administration of acetyl- salicylic aci& according to requirement the pain gradually subsided in the course of 3 to 4 days, leaving only a slight sensation in the right temporal region, which also subsided in the course of the next 12 to 14 days.
The ophthalmologist, however, still maintained that neither the present pain nor the highly increased sedimentation rate of the patient could be explained as sequelae of the glaucoma, which had been satisfactorily treated with pilocarpine. It had been noticed on admission that both

ARTERITIS TEMPORALIS (HORTON). 153
of the temporal arteries were swollen, hard and pulseless (but not tender now), and the patient’s pain was now supposed to be due to arteritis. For diagnostic purposes a resection of the ramus frontalis of the superficial temporal artery was therefore made, the patient, who had then been free from pain for a long time, not being affected a t all by this interference. On the resection the artery was found to be ofirmly thickened, and the tissue surrounding the artery somewhat indurate&) (signed Aaberg). A histological examination of a portion of the removed artery gave the following result:
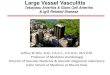
))In the place of the intima and almost the entire lumen there are dense, uniform, connective tissue masses with a moderate content of cells and without any accumulation of blood pigment or lipoids, necrosis or sclerosis. Excentrically in this connective tissue there is a single medium-sized and a few smaller endothelium-covered, blood-filled, but not thrombosed, tubular, longitudinal canals. The lamina elastica displays a wavy surface, and is thickened, either dense or frayed, in parts completely absent. Corresponding to the peripheral part of the intima, close to the lamina elastica, but only seldom passing the latter in the direction of the periphery, there is a number of greater, pale elongated mesodermal elements with smooth or slightly rugged edges, lying close to each other. These cells appear, now as a new zone interposed in the wall of the vessel, now as ill-defined nodules. There is some exudation within the latter granulomatous proliferations, and there is a tendency to the occurrence of capillaries and giant cells. In the portion of the said zone there is a couple of rows of comparatively large calcium deposits. In the parts where the granulomata interfere with the lamina elastica, the latter has been destroyed in a small tract, whereas the adjoining portion of elastic tissue is diffusely or slightly sclerosed. The granulomata occur in a number of 1 or 2 in each cross section of the vessel. No necrosis or processes of capsulation around the granulomata. In the peripheral part of the intima proliferation there is one small, slit-like, fresh hemorrhage (artificial?). The tunica media is narrowed moderately or great- ly, in parts almost completely lacking. No granuloma formation is seen in most of the narrower parts of the media. The structure is dense, without any cicatricial alterations or sclerosis. The ad- ventitia is partly dense, staining abnormally owing to shrivelling, partly of normal structure, apparently not thickened. Whereas the dense connective tissue masses in the lumen and the intima apparently display no signs of inflammatory infiltration, there is a scattered moderate, inflammatory infiltration (few leucocytes and plafima cells, a number of lymphocytes) in the cellular, granu- lomatous, proliferating zone of tissue in the peripheral parts of the tunica intima and media. The muscular conncetive and fatty tissue surrounding the vessel displays rather marked, chiefly perivascular infiltration with lymphocytes. The smaller vessels in this part of the tissue are apparently normal.

154 TORBEN ANDERBEN.
Fig. 1. Section of artery showing larger central part, representing severe, dense, uniform proliferation of the intima with remnants of lumen of the vessel. I n circular arrangement round the latter, an uneven, thick cellular inflammatory zone con- taining a larger, fully developed granuloma (immediately to the left of the greatest lumen). I n the peripheral part the atrophic media, respectively adventitia; com-
paratively narrow here, almost without any round-cells.
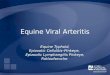
Fig. 2. High-power view of the granuloma with its chiefly lymphocytic inflammatory cells, proliferating stroma cells and capillaries; to the right upwards the ill-defined border at the media. In the centre of the picture two large, dark, angular chalky particles of unequal size; t o the left upwards two polynnclesr giant cells, viewed
in part tangentially.

ARTERITIS TEMPORALIS (HORTON). 155
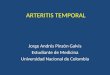
Pig. 3. High-power view of the granuloma, especially showing several fairly large capillaries; to the right downwards the border a t the media.
The jilrzdings are then as jollows 1) An exudative and especially proliferative, partly granulo-
niatous alteration of the wall of the artery with a small number of giant cells, the alteration being unevenly distributed and of varying intensity, but marked in most parts. The process is localized to the peripheral part of the tunica intima, penetrating the lamina elastica in parts and on the whole appearing as an additional zone of the wall of the vessel of varying thickness.
2) A more marked chronic, exudative (but not proliferative) inflammation of the adventitia and especially of the adjoining fatty tissue.
3) A marked, uniform proliferation of the connective tissue of the intima with a moderate content of cells and in parts also of the lamina elastica, hardly displaying any connective tissue infiltration and without any degeneration. The connective tissue infiltration has replaced the lumen of the vessel almost completely. The scanty remains of the lumen are not thrombosed. 4) A medium to marked atrophy of the media and 5) diffuse, moderate sclerosis in spots in the interposed
proliferating granulomatous zone, respectively in the adjoining lamina e1astica.o
(signed Svend Petri).
-1 portion of the artery was sent to the State Serum Institute for bacteriological examination: In attempts a t cultivation no growth was produced. In addition, the following examinations were made, as far as most of them are concerned before the diagnosis was finally established:

13; TORBEN ANDERPEN.
Ophthalmoscopy: Normal conditions of disks and vessels. No stasis phenomena. Spinal fluid: Normal. X-raying of the skull: Normal. Encephalography: Moderate internal hydrocephalus. X-raying of heart, lungs, urinary tract (intravenous pyelography), vertebral col- umn, pelvis, right crus, and teeth: Nothing abnormal. Electrocardio- gram: Normal (left-sided axis deviation). Blood-pressure (repeated examinations): About 150190. T h e temperature of the patient was normal during both of his stays in hospital. Wassermann’s, Kahn’s and Meinicke’s tests negative in blood and spinal fluid; antjstreptolysin titer: 32-25 and 40 (normal); staphylococcus antitoxin titer: < 2 (normal); Vidals and Weil’s reactions negative; Ewald’s test meal normal; the stools did not contain blood; the urine did not contain protein or sugar, and urine sediment count (a. m. Addis) showed normal conditions; hemo- globin percentage (Haldane) about 85; leucocyte count 7,320; differ- ential count normal (4 per cent eosinophilic leucocytes); sternal marrow normal; plasma fibrinogen (a. m. Gram) 0 . 7 2 per cent. Blood sedimen- tation rate (Westergren): Greatly increased durilzg both of the patient’s stays in hospital, the maximum being 105 mm/l hour, and still in August 1946 it was 41 mm per hour.
The symptoms subsided gradually during the patient’s stay in hospital and on Peb. 2nd 1946 he was discharged. He still felt somewhat fatigued when discharged, and the glaucoma persisted, still requiring treatment in August 1946. During his convalescence the patient still felt tired and was psychically unstable with a tendency to depression, and though he was still improved, the patient did not feel quite well in August 1946, thus he still had slight rheumatoid pain in the lower extremities. About April 1946 he began t o complain of ))humming as that of a tele- graph poler in his left ear, especially when he felt congested in his head, possibly suggestive of an intracranial aneurysm.
Epicrisis: A 54-year-old well-preserved business man devel- oped violent pain in the right nuchal region and in both temporal regions. Symptoms of glaucoma developed. While t h e latter was being treated, the pain subsided almost completely. In spite of continued treatment of the glaucoma he got renewed pain in the temporal region, observing at t h e same time tha t the vessels, especially those of t h e right side, became highly swollen and tender. I n the histological examination of an excised portion of the artery the latter was found t o be the seat of violent and characteristic inflammatory alterations, 9 months after the onset of the arteritis, though his condition has improved and he is completely fi t for work, he still suffers from some fatigue orheu- matic)) pain in the extremities, and symptoms t h a t may suggest the presence of a n intracranial aneurysm, the glaucoma still being treated too.

ARTERITIS TEMPORALIS (HORTON). 1 5 i
History. It has been believed hitherto that the syndrome of arteritis
temporalis was first described in 1932 by Horton, Magath & Brown. This is not so, however. As far as I knowl, the first publication on this syndrome should be credited to Max Schmidt. However, he has to share the credit with Erik Warburg, who observed a case and reported it to Schmidt. The case was described in detail in Bibliot. f. LEeger 1930, 122, page 320 and in Brain 1930, 53, page 532 in an article dealing with intracranial aneurysms. On the whole it corresponds closely to the cases that have been described later on and will, therefore, not be mentioned in detail here. There is, however, an interesting feature of this case, namely that is was associated with a paracentral scotoma of the right eye and that an intracranial aneurysm ())presumably of the right internal carotid artery))) developed in connection with the ar- teritis. The author of this first publication thus realized, what was only finally established in subsequent publications, that the disease is not an affection that is confined t o the temporal artery but that the temporal arteritis only forms part of a more wide- spread vascular disorder.
Horton. Magath & Brown, however, are to be credited for having established the syndrome as a nosological entity and for the increasingly thorough investigations into the disorder in the course of time. Therefore the disease has not injustly been termed Horton’s disease. Apparently without any knowledge of this American work Paviot, Chevallier, Guichard & Damez described the disease in 1934 (as pointed out by Oldberg), and in 1939 ThBvenard (pointed out by Sprague & MacKenzie) and Lucien, Mathieu & Verain, also in 1939 (pointed out by Sjovall & Win- blad) published apparently independent descriptions of the disease. The publications by other authors have all been made with a knowledge of Horton, Magath & Brown’s work. As regards these publications, I may refer to Table I . I would, however, mention that, apart from Schmidt’s and Warburg’s observation, the syndrome was first described in Scandinavia by Oldberg in 1942. I n 1944 Sjovall & Winblad reported two cases with biopsy. Broch & Ytrehus observed 4 cases in Norway. The knowledge of this disorder now forms part of the teaching of medical students
Akklitional note a t the proof-reading: Is Allen, E. V., Barker, N. W. & Hines, E. A.: Peripheral Vascular Diseases. W. B. Gaunders Comp., Philadelphia - London, 1940, Pg. 479 it is stated by W. F. Iivale that the first publicatios cosreroing temporal arteritis was given by Jonathan Hutchisson in Arch. Rurg. (London) 1:323, 1890.

158 TORBEN ANDEREEX.
Table Surrey of Cases
I Rl L 5
1
0
3 4
5
6 rJ
8
9 10
i 11 ~ 12 1
13 14
15
16
Authors
Schmidt & Warborg
Horton, Magath &
D:o l'aviot & nl.
Brown
MacDonald & Moser
Horton & Magath D:o D:0 D:0 D:0 D:o Jennings
D:o Bain
Thkvenard . . . . . . . . .
Lucien & al. . . . . . . . ,
17 Dick & Freeman . , . ,
18 ~ D:o
! I Ill: '69' a few weeks 6 months lboth
1 1
I I F ~ 5 5 6 weeks
31 1681 4 0
P 75 6g~ 111 172'
i i 31 65' K 68 4 weeks III 57 F 66 7 months
F ,72 a few weeks P 71 2 days
I
M '66' I
I
P 65 afewdays
F 76 5 months
22 0 >
, 1 year >
6 months 2 B
11 9
i 6 weeks
more than 18 months
3 months
1 year

ARTERITIS TEMPORALIS (IIOKTON).
~ Paracentral scotoma I
Actinomyces
159
- Intracranial aneurysm.
occlusio coronariae. Died 13 years later of
1.
hitherto published.
, 60 l20/60
1 1
1 1
' 46' 230/125 I 1
1 87 I 120175
71 148/90 ~
I
220/140 781 165,'lOO
1
I
IStaphylococ- 1 cus aureus
I 48 160/90 ' 76 136/80 ,
I
+ Staphylococ- I cil
70
I
74 172,'80
6 years later Post & San-IUied G years later of ce- ders found peculiar ar- rebro-vascular disor- terial alterations in der (Post 8: Sander's patient's retina communication) I
Observed by ,J. A. ltiegel
phlebitis in retinal vein with hemorrhage and Observed by 11. c. Riddle/
I eisudates
Observed by Articio & al.
In two of these cases~ in 1934.
Thrombosis a. centralis retinae of both eyes, left eye blind,restricted field of vision in right eye. I
i Photophobia. sensorium
I eyes
~Lilne corrosions of both l corneae immediately ~ before onset 1 From a similarly affec-
ted artery in front of patient's strnma
I
-4 Streptococcus Constricted retinal veins.1 viridans Papilla enlarged; blur-l
ring of vision with^ greatly reduced field of vision in left eye. 1
Tenderness of eyes, blur-1 ring of vision, sient diplopia --I

W
at
-
z2
3 I
3
m
Qi
m
61
E
l B
lood sedimen
tation rate ~
~~
__
__
_
or anorexia
Side
m
f 2 Q
i 3
Duration of disorder
m
t-
Duration of
3isorder before onset. of tem
poral arteritis
__
__
_
-
Age
__
__
-
Sex
w
01
m
mn
&
3
3
Year w
hen published
m
2 c
~-
..
.
2 .
..
.
..
G
: ::
. .
-
=-3 :
:g
..
.
..
.
.
..
.
*.
.
4.
.
.
..
.
..
.
.
:$
::
.
..
.
.
:s
:.
.
- .
.
.m
. .
a
..
.
..
.
.
e
e r, u2 C
ase Pir

ARTERITIS TEMPORALIS (HORTON). 161
1 I Cultivation Ocular symptoms Comment
I
ted field of vision. Blind in both eyes. Blind in one eye.
80 220/110 ~ A- lgrampositive rocci in clusters
I I ' I I I
acuity and retinal al-
Observed by R. A. John-
I t e ~ ~ A o n s .
son
85l 145/95 I J -
I llSj62 + 130/80 -r
I 195'100 59 110!70 -t
t 89, 155/8O 761 130185
no growth
Transient cerebral coma (possibly owing to hy- pertensive cncephalo-
~IReported to Bowers by
pathy)
Horton Confused sensorium
Radial artery also affec- ted (biopsy)
{lind in right eye. Re- Diabetes. Arteries of duced vision in left eye arms and hands pre- (retinal changes dia- sumably also affected betogeuic?)
Diabetic. Died of coro- nary sclerosis. First CUM with post-mortem exam. : Typical altera- tions in aorta, carotid, anonymous, subcla- vian, pulmonal, coe- liac, mesenteric, renal and iliac arteries. His- tological examinations of coronary or tempo- ral arteries not stated.
t tl
I ~
i Blind in right eye, great- ly reduced visual acu-
~ ity in left eye.
See Comment to Nos. 34 and 35.

40, l'rofant . . . . . . . . . . . . . > 1 F , 76 5 weeks
2 0
3 months
1 L
2 weeks
1 year 'right
41
I 42
43 44 4.5
I 46
D:o . . . . . . . . . . . . . . . . 3) I." GI more than 2 months
18 0
8 D
G weeks 6 months
I Sjdvall & Winblatl . . R
D:o . . . . . . . . . . :... . . u
Shannon &Solomon . 194: Cooke 8: al. . . . . . . . .1194(
M
M
62
63 73 6G
} 11; - 10:
t
t
-
-
D:o . . . . . . . . . . . . . . . . n 66 5 months 10
D:o . . . . . . . . . . . . . . . i 69 7 v 30 D ~ n I
I I
4 8 ' D:o . . . . . . . . . . . . . . . . L
I49 n:o . . . . . . . . . . . . . . . . >j
more than 30 months more than 12 months
>
D +
71
39
5 n
5 S)
' In their publication Sjovall & Winblad by erratum has stated the ngc of this

ARTERITIS TEMPORALIS (HORTON). 163
150 50
76 l5OjS0 +
79 130 7.5 + 90 130,'90 + 96 130,W 1-
60 130195 + 98 180/90 +
, I
I
patient a> 1 3 year\
Blind in both eyes. Transient ptosis. Blind
in one eye.
Transient diplopia
1 Transient diplopia. Blind in both eyes.
Blind in both eyes.
Transient blurring of vi- ~ sion.Permanent restric-
tion offield of vision.
Comment I I
45 minutes. Died in stupor. Result of
post-mortem not sta- ted, only tha t altera- tions were found in other vessels than tem- poral artery and that post-mortem findings will be published by Mahoney & Hall (Bel- levue Hospital).
Extraction of three in- fected teeth was imme- diately followed hy a severe, acute exacerba- tion of the temporal arteritis.
Articular symptoms.
Articular symptoms. Psychically unstable.
Died a t home 6 weeks' after discharge, pre- 1 sumably of ))a cerebral vascular accident,).
Died with symptoms of emollitio cerebri. Post mortem: (Besides af- ~
fection of temporal ar- teries) affection 1 of aorta, renal, femoral, mesenteric and sub- clavian arteries. In cer- ebral arteries both small emboli and aut- ochthonous thrombi with emollition of cere- , bra1 tissue.
irticular symptoms.

164 TORBEN ANDERSEN.
__
Cooke & al. ( c t . ) . . . . . 11941
D:o . . . . . . . . . . . . . . . .
Kilbourne & Wolff . ,
Broth & Ytrehus, . . . , u
D:o . . . . . . . . . . . . . . . . 9
D:o . . . . . . . . . . . . . . . . i
D:o . . . . . . . . . . . . . . . . R
Torbcn Andersen . . . .I194 I
h L year i 14 months 'both ~ -1 ~-
I
b 18 months more than , 1 )) -1 ~ i
8 about 1 week
1
191 1 month I
6
17 4 3-4 months
I4 18 1,
2 years ~
P/,months o I + l i
I , i j
1 year 1 106 6 months 1 ': c 101 about '
1 year I morethan 1 !>
3 years
In a personal communication in July 1946 Horton states that he has now observed
in Scandinavia (Warburg), so that the number of observed Scandinavian cases must be supposed to increase rapidly. (Apart from the 57 cases stated in the table Chavany has described a ))syndrome algique du territoire de l'art6re temporale superficielleo with a ))douleur discontinue survenant par crises paroxystiquem, which occurred with increasing frequency (at intervals from some months to 1 week) throughout 5 years in a woman aged 63 years. This is apparently a case of another disorder (arteriospasm) localized to the same arterial branch as arteritis temporalis).

ARTERITIS TEMPORALIS (HORTON). 165
7 4 i 145170 +
I i I
I 80 l40j80 -1
I I
‘ I I 69‘ l60/90 1 I 681 120jSO G61 135,llOO GOl 175/95 + 85 l50/90 1- INo growth
Transient diplopia. Articular symptoms. Blind in both eyes. Died with symptoms ’ of emollitio cerebri.
1 Post-mortem: (Besides I affection of temporal I artery) affection of
aorta, coronary, mes- 1 enteric, femoral, ra-
dial, central retinal ar- 1 teries. I n cerebral ar-
Slight reduction of vision.
I
I
1 Ptosis, diplopia, strabis- mus.
!
Bilateral glaucoma
teries thrombi and emollition of cerebral tissue.
Aneurysm on basilar ar- tery or circulus arterio- SUB Willisii (X-ray). Died 2l/, m o n t h after arteritis had ceased of coronary occlusion. No post-mortem.
Died 2 months after dis- charge of hematemcsis (hemoptysis? )
Psychically unstable.
Psychically unstable. In- tracranial aneurysm? DRheumatismr
33 cases in all. The total of observed cases is then 73 .
Except Schmidt & Warburg the authors of the first years are of opinion that temporal arteritis is a disease that is confined to the temporal artery. Communications about complications from the eyes (26, 13, 17) were published rather soon, suggesting that the delimitation of the disease is not so easy. In a publica- tion, which apparently remained unnoticed till 1944, Lucien, Xathieu & Verain, in 1939, gave the first indefeasible proof that other arteries than the temporal artery might also be affected; in their patient suffering from arteritis temporalis they made a

16(i TORBEN ASDEHSEN.
biopsy of an artery passing across the patient’s struma, and this artery proved to be the seat of the characteristic histological alterations. I n 1941 Hines found similar alterations of the radial artery of his patient suffering from arteritis temporalis and, on the basis of clinical observations, several authors of that time realized the more widespread character of the disorder. I n 1942 Sproul reported the first fatal case. He gave a brief communication about a 68-year-old diabetic who died of cardiac insufficiency on the basis of a coronary sclerosis a few months after the mani- festation of his arteritis temporalis. In the post-mortem examina- tion typical alterations of the aorta, the carotid, anonymous, subclavian, pulmonal, coeliac, mesenteric, renal and iliac arteries were ascertained. Unfortunately nothing was stated about the histological examination of the coronary arteries, but simply that there was aadvanced coronary stenosiso with infarcts in the myocardium. This publication, too, seems to be slightly noticed, even though it changes decisively our view of the disorder. Another case with post-mortem examination was briefly com- municated by Chasnoff & Vorzimer in 1944 until, in 1946, Cooke, Cloake, Govan & Colbeck, in a fine work (Temporal Arteritis: A Generalized Vascular Disease), in which, among others, two cases with post-mortem examination are reported, clearly prove the disorder to be a generalized vascular disorder, which does not only affect arteries anywhere in the organism, but also affect the veins, for in their summary the said authors state ))involve- ment of the femoral vein in one case)), out of two cases with post-mortem examination. It does not appear from the case records in question that the femoral vein has been examined histologically in any of these cases. But on the other hand it is stated that in their case No. 3 both axillary veins proved t o be transiently affected in the clinical examination. This finding elucidates in an interesting manner two works by Eckerstroni on phlebitis temporalis observed by him in three patients. The case records reported by him bear so striking a resemblance to those that are most characteristic of Horton’s disease that, having read his first publication dealing with two patients, I believed that he had established the diagnosis of phlebitis by mistake instead of arteritis, the more so as the diagnosis had been established solely on the clinical examination without any biopsy. I n his second publication, however, he reported a third case with biopsy, which does not leave any doubt about the cor-

AETERITIS TEMPORALIS (HOBTON). l ( i 7
rectness of the diagnosis of phlebitis, and the histological picture of which shows a fine conformity with the numerous examinations of arteries that have been made.
It may be mentioned that in 1937 Sproul & Hawthorne de- scribed similar alterations in the aorta and the iliac arteries and that. in a much quoted work of 1941, which, unfortunately, has not heen available to me, Gilmour described a ))chronic giant-cell arteritis)) localized to the aorta and its branches, which he iden- tified with arteritis temporalis, without any affection of the temporal artery in these cases as far as I can gather. The present perception of arteritis temporalis is thus that it is a frequent manifestation of a generalized vascular disorder.
Etiology.
The etiology is unknown. The disorder is often preceded by various diseases and debility, such as bronchopeumonia, ))in- fluenza)), sinusitis, dental disorders and ))rheumatism)). I n cul- tivatioii from the excised artery actinomyces (14, 15), staphy‘o- coccus (23, 2 2 ) , streptococcus viridans (8) and gram-positive cocci in clusters ( 2 ) have been demonstrated.
(Dick & Freeman believe that streptococcus viridans has been culti- vated iii two cases (one case besides their own). This is doubtless due t o a mistake, since MacDonald & Moser have reported the finding of streptococcus viridans in cultivation from a periodontal pouch, whilst in cultivation from the artery they found staphylococcus aureus.)
Cultivation with a negative result has been made a t anyrate in another two cases. It cannpt yet be ascertained whether the bacteria mentioned above represent the etiologic factor, which would then be varying. The respective authors do not seem to attach special importance to these findings, and I would be most inclined to believe that they are due to contamination. The disease occurs almost exclusively in elderly individuals and, therefore, arteriosclerosis is believed to be a concurrent factor. The fact that the disease is often associated with fever and a highly increased blood sedimentation rate is indicative of an infection, and the not infrequent rheumatoid muscular and articular symptoms have been considered proof of the ))rheumatoid)) etiology, especially by Swedish authors (34, 9, 10). Profant has, after having extracted some infected teeth, observed severe exacerbation of the temporal arteritis.
12--’t71585. d e f o m e d . scnndinnv. Vol. CXXT’ I I I .

168 TORBER ANDERSEN.
Pathology.
Biopsy has been made on 30 patients a t any rate, and the histological examinations gave identical results, even though in the individual cases the alterations have been observed a t different stages. On excision the artery proved to be hard like cartilage, with little or no lumen, of unequal calibre. As to the histological picture, reference may be made to the description of the prepara- tion originating from my patient and given above; as especially characteristic features the occurrence of giant-cells in the media and of round-cell infiltration around the vasa vasorum of the adventitia must, however, be pointed out. Otherwise, particularly good descriptions of the histological picture are to be found in the said article by Cooke, Cloake, Govan & Colbeck. Post-mortem examination has been made in four cases, by means of which the generalized nature of the disorder was ascertained. Charac- teristic histological alterations thus has been found in the aorta, ihe coronary, carotid, anonymous, subclavian arteries, superficial artery of the neck, the temporal, central retinal, radial, pultjLona1, coeliac, mesenteric, renal, iliac and femoral arteries; further, in the femoral vein ( 7 ) and the temporal vein (lo), as well as in the axillary veins, which were seen to be clinically affected in one case (7).
Sex and Age Incidence. There were 30 females and 24 males out of 54 patients, about
whom information as to sex and age is obtainable. The youngest patient was 54 years, but only five were under 60 years, and the average age of these 54 patients was 67 years.
Symptom at01 ogy.
In most cases the onset is insidious with vague uncharacteristic symptoms: Fatigue, anorexia, loss of weight, slight fever, night- sweat, often also ))rheumatic)) pain (8, 34, 7) of varying locali- zation in the trunk, the neck or the extremities. This prodromal stage may last many weeks or months (17, 5, 7), as it did in my case too. Gradually or suddenly, headache occurs. Sometimes it is localized to the temporal region itself; but it is frequently localized, first or simultaneously, to the nuchal region, denoting

ARTERITIS TEMPORALIS (HORTON). 169
an involvement of the occipital arteries (13, 1, 22, 8, 32, 25, 4, 33, 7), as was seen in my case. The pain may also begin in the jaws (33, 16, 7, 21). Gradually the pain is localized to an increasing extent to the temporal region and, from a couple of days t,ill a few months after the pain in the head began, the superficial temporal artery, and especially its ramus frontalis, becomes swollen and tender. In contrast with this slow development of the symptoms, cases may also be seen in which the temporal itrteritis manifests itself in the course of quite a few days (1, 8), or other cases may be observed in which the disease is ushered in by one of its most serious complications, namely affection of the vessels of the eyes (Cooke et al.: 2nd and 6th cases). As u rule (in 43 out of 47 cases) both temporal arteries are affected but it is very common that the pain is not equally intense on both sides. The pain is dull, continuous, alternating, with violent paroxysmat'c attacks of shooting pain, so that the patients may cry out with pain. Straining a t stool sometimes increases the pain (13, 3), as was the case with my patient. The pain often radiates to the ear, the neck or the jaws, rendering i t difficult for the patient to chew, and as there is often pain in the tongue, too, the ingestion of food of these patients, who often have a poor appetite in advance, is further impeded. Profant states that 50 per cent out of 19 patients felt pain while chewing. The temperature is stated to be increased in 36 out of 41 cases; i t is only greatly increased in rare cases. Night-sweat is of frequent occurrence. The general health is often greatly influenced. The patients are often depressed, but there are no reports of suicidal intentions.
If the patient is seen before the temporal arteries have be- come swollen and tender, it will hardly be possible to establish the diagnosis, unless complications have already occurred a t an early stage, arousing suspicion as to the nature of the disorder. Otherwise the temporal arteries (or one of them) are found to be swollen, and are often felt to be to cm thick, twisted, in many cases irregularly swollen, hard like cartilage, with little or on pulsation, and tender. At the beginning or during exacerba- tions of the disease the skin covering the artery may be found to be hyperemic and oedematous. If other palpable arteries are involved, the following may be the seat of similar changes: the occipital artery (8, 7, 3) and the radial artery (12, 7). The tongue may be red and burning (2, 7), regional glands swollen and tender

170 I‘ORBHK ANDERPEN.
(14, 15, 23, 8, 16, 32, 25). The remaining somatic examination shows nothing in particular. Some patients, however, displayed objective articular symptoms (34, 7). The fact that others had symptoms of arteriosclerosis (25) is hardly to be wondered a t in patients a t this age. The following laboratory examinations may be mentioned: As a rule there is a slight hypochromic anemia. In 22 out of 31 cases the hemoglobin percentage (which I have recalculated according to Haldane’s standard as far as possible) was below 80. In many cases there is a neutrophilic leucocytosis. The blood sedimentation rate was only examined in 19 cases. It was found to be ))normal)) in one case only, in all other cases i t was most frequently considerably increased, in 13 cases even 100 or more; and i t is stated to remain increased for a very long time (months) after the local symptoms have subsided. The blood-pressure was found to be over 200 in 3 out of 38 cases. In 8 cases, a t any rate, the spinal fluid showed normal conditions (13, 16, 34, a l ) , as in my case, whilst in 4 cases an increased pro- tein content was found without increase of cells (30, 7). Wasser- mann’s test was negative in all cases where it has been stated.
1 have tried above to describe the symptomatology as i t appears in its classical form, i. e. the form which has its actual climax in the temporal arteritis and which, just for that reason, has lend its name t o the disease and led t o the perception of the diseast. as a disorder that is especially characteristic of the temporal artery. As has already been suggested above, the latter is, however not the case. The disorder is a generalized vascular disease and, therefore, it cannot always be expected to affect the temporal artery in particular. With a few exceptions (11, 9) the literature only deals with cases with involvement of the temporal artery, and the various other symptoms that have been observed have been considered complications of the temporal arteritis, but the latter should rightly be considered a fairly indifferent, easily observable external manifestation of the generalized disorder. From this point of view the symptomatology of this diyorder. of course, displays a very complex picture, the predominant feature of which depends, in the individual case, upon the vessels or the vasculature that are most severely affected or perhaps rather upon the vital importance of the organ supplied by the affected vessels.
Ocular symptoms: The vessels which, next to the temporal artery, are most frequently affected are, according to the lit-

ARTERITIS TENPORALIS (HORTON). 171
erature, those of the eyes. This applies both to the vessels supplying the sensitive apparatus of the eyes and to those supplying their motor apparatus. As will appear from the survey given in the table, ocular symptoms were found in 24 out of 57 patients (40 per cent) dealt with in the literature. Still considering the tem- poral arteritis as the primary feature of the disease, Johnson et al. give the following description of the route by which the affection may be imagined to spread: aThe a. teniporalis profunda anterior has an anastomosis with the a. lacrymalis arising from the a. ophthalmica. The latter gives off the a. centralis retinae, which sends an anterior and a posterior branch to the optic nerve (Kerschner). It can be understood that in this case the in- flammatory process has spread by these routes.)) Cooke et ul. make similar reflections, also pointing out that, no doubt, the disorder may affect the arterial supply to the oculomotor nerve (ptosis, diplopia etc.). That the retinal vessels are actually affected has been shown by Cooke et al. by means of histological examina- tion of their 6th case. The subjective ocular symptoms vary from slight tenderness of the eyes, transient diplopia, photo- phobia, transitory blurring of vision, from a varying degree of decreased visual acuity with reduced field of vision to complete blindness in one or both eyes. Of special interest is the fact ascer- tained by Johnson et al. that sometimes there is a striking dis- proportionality between the visual defect and the retinal changes, which they explain in the manner that the retinal changes are the more marked the more the vascular disorder is in the peripheral direction (of the retina). If the arterial occlusion takes place in the arterial branches supplying the optic nerve far behind the retina, the patient may become totally blind without dis- playing any changes of the retina. These considerations are doubtless of importance to the understanding of other visual disturbances than those referred to here. Further, it is important to note that in two patients Cooke et al. (2nd and 6th cases) observed the visual disturbances before the temporal arteritis manifested itself. It must be possible for visual disturbances of this nature and origin to occur without affection of the temporal arteries. And Cooke et al. briefly mention that they have such cases under observation. It should be noted that, when the ocular symptoms occur with so extreme a frequency in this generalized disorder, the fact should always be borne in mind that all the ocular complications reported have been observed

172 TORBEN ANDERSEN.
in patients with involvement of the temporal artery, i. e. in cases where the arteries of the skull are especially affected. Therefore, t o arrive a t a quite correct estimation of the frequency of ocular complications, i t must be established that when patients suffering f rom this generalized vascular disorder develop subjective or objective syrnptorris frorn the temporal artery, they have a PO per cent chance of getting ocular symptoms.
Glaucoma has not been previously described as a ocomplica- tion)) in temporal arteritis. As i t is known now that the generalized vascular disorder also affects the venous system (9, 10, 7), the explanation suggests itself that in my patient the glaucoma was due to involvement of the venous apparatus. (Dr. Henning Skyds- gaard will account for the ocular symptoms in the ))Acts ophthal- mologica)). )
Cerebral symptoms: Already in the first published case (31, 39) an affection of the cerebral vessels was ascertained, clinical signs of intracranial aneurysm being found. Kilbourne & Wolff made similar findings in X-raying of the skull, and my patient displays clinical symptoms of this disorder. The patients have been stated to be mentally confused in several cases (1, 35)) psych- ical instability (34, 3) was also observed in my patient. Emol- litio cerebri (7 ) was found in two patients on post-mortem exami- nation, one patient died of ))a cerebral vascular accident)), one died in stupor, whilst another patient died of a cerebrovascular disorder (28) 6 years after the onset of the disease.
Cardiac symptoms: Schmidt’s and Warburg’s patient died 13 years after the onset of the disease of a coronary occlusion, which, no doubt, cannot be associated with the disease. Sproul’s patient died of cardiac insufficiency. I n the post-mortem exani- ination coronary sclerosis with infarcts in the myocardium was found, but it seems as if the coronary arteries have not been examined histologically. Kilbourne & Wolff’s patient had a coronary occlusion about 3 weeks after the arteritis had ceased. and about 7 weeks later he got another occlusion ending in death. Post-mortem examination was not made. The patient had suf- fered from stenocardiac attacks for 3 years before he developed temporal arteritis, and the authors believe that there is no con- nection between the two disorders. In post-mortem examination of one case (Cooke et al., 6th case) characteristic alterations of the coronary arteries and fibroses in the myocardium were found, but nothing is stated about cardiac symptoms.

ARTERITIS TEMPORALIS (HORTON). 173
Abdominal symptom: Broch & Ytrehus state that their first patient died 2 months after discharge of a sviolent hemorrhage)), presumably a hematemesis. The patient died while he was a t home. post-mortem examination was not made, and in personal communication to me dr. Broch states that he cannot come any nearer to the cause of desth. As an affection both of the pulmonal artery and the coeliac artery has been observed in post-mortem examination of other cases, as was mentioned earlier, the cause of death may presumably also be a hemoptysis. J’ersild has re- cently mentioned the simultaneous occurrence of blindness and hematemesis. In such cases a simultaneous occurrence of throm- bosing of the branches of the coeliac artery and of the arteries of the eye must doubtless be imagined, even if such thrombosing of course need not arise on the basis of the disorder dealt with here. In the present period, when a special interest is taken into the vascular pathogenesis of the ulcer disease, it would perhaps be reasonable to draw the attention to the possibility that a few cases of stomach bleeding may occur on the basis of pathologic- anatomical vascular alterations of the nature dealt with here. Cooke et al. mentioned that their second patient (a woman, aged 66 years) had a severe uterine hemorrhage of unknown causation. In this connection I would remind of the fact that in post- mortem examination of other cases the iliac artery has been seen to be involved.
As pointed out already, the publications referred to always stress the affection of the temporal artery, for which reason the above ))complications)) are most frequently dealt with only to the strictly necessary extent. In addition to the vessels men- tioned, an affection has been found in several superficial vessels, as already referred to: The occipital, radial and femoral arteries, and the temporal, axillary and femoral veins.
Diagnosis.
We may thus expect to see the disorder manifest itself with highly varying pictures. The symptoms which, besides the histo- logical findings, are required to establish the clinical entity may be summarized as follows: Occurrence in elderly patients, insidious onset, exhausted general health, fatigue, anorexia, loss of weight, slight fever, night-sweat, ))rheumatic)) pain; in many cases greatly increased blood sedimentation rate, hypochromic anemia, neutro-

174 TORBEN ANDERSEN.
philic leukocytosis -- and then we have to wait patiently for the appearance of affection of vessels which are accessible to biopsy or for the occurrence of others of the ))complications)) mentioned above which may confirm the diagnosis.
ritis 10. l’eriphcral
Differential Diagnosis. It has been discussed whether arteritis temporalis is an inde-
pendent disorder, or a special manifestation of known vascular
Table 11. Comparison of Clinical Features in Temporal Ar ter i t i s , I’hromboangeitis
Obliterans, and Periarteritis Nodosa (modi f ied a f t e r Cooke et a1 1. 1 I Temporal arteritis
1. sex Equally frequent in men and women.
2 . Age Over 54 years (aver- age 67 years)
3 . Myaigia Frequent. and joint symptoms.
tion 4. Localiza-
11. dlbumin-
12. Ocular and 1 uria
, oculomotor symptoms
~ 13. Prognosis
Generalized vascular disorder.
Observed.
Not observed. Common and sevcre. Common (slight). Not observed.
Arterial thrombosis common. Aneu- rysm observed clin- ically.
Not observed.
Frequent.
TJsually rec’jirery (sometimes with loss of sight) in the course of 6 to 12 months
, Thromboangcitis Periarteritis ,
obliterans nodosa --- Almost entirely
confined to men. Between 25 and 45 years.
Uncommon.
Especially the ves- sels of the ex- tremities.
Frequent.
Frequent. Not prominent. Common. Not observed.
Superficial and deep thrombosis of vein and art- eries of legs.
Occasionally.
Rarely.
Loss of extremitv and sometimes life.
Much commoncr in men.
Usually young adults.
Frequent.
Small arteries (3 to 5 nim) in many organs.
Observed.
Occasionally. Not prominent. Prominent. Frequent.
Nodular swellings with occasional formation of aneurysm.
Frequent.
Rarely.
&Iost frequently, fatal vithin a 1 year.

ARTERITIS TEMPORALIS (HORTON). 175
disorders. It has been maintained in this connection that the histological picture differs from the disorders of the vascular system previously known (especially thromboangeitis obliterans and periarteritis nodosa). Moreover these disorders differ clinic- ally from each other in several important respects, as will appear from Table I1 (modified after Cooke et d). During the first stage of the disease, which may vary from a few days till several months, the diagnosis is difficult, which will appear from the fact that it has been mistaken for the following disorders: Hemicrania, si- nusitis, cerebral tumour, meningitis, fibrositis of the neck, osteo- arthrosis columnae, hypertensive encephalopathy, mandibular arthritis, odontic neuralgia, and temporal neuralgia. If ocular symptoms have occurred in the first stage, they may induce us to be content with a symptomatologic diagnosis on an eye disease in such cases.
Prognosis.
This disorder hitherto has been believed to have a good pro- gnosis. It was realized that it took a very prolonged course, often up to a year or more (Table I ) , but i t was believed that the patients always recovered. Now the prognosis is known to be uncertain. 7 out 57 cases have been reported as fatal in con- nection with the acute stage. In 4 cases the death was due to cerebral vascular complications, in 2 cases to coronary sclerosis or coronary occlusion, and in 1 case to ))violent hemorrhage)) (hematemesis or hemoptysis) . The various com- plications ( e . g. from the eyes), like the causes of death, depend on the vasculatures that are affected.
Treatment.
As a rule, the treatment has been merely palliative. Paviot et al. observed a good effect of salicyl, whereas Eckerstrom found the latter to be without any effect. Sulfanilamide (8, 16), sulfa- pyridine (16) and sulfathiazole (10) have been administered, without any effect. Further, treatment has been tried with short waves, iodides, nicotinic acid, and of course vitamin B,. In illustration of the therapeutical escapades that have been made, it may be mentioned that Schaefer 85 Sander's patient in ))Sander's oscillating bed cleared up completely)). A number of authors have observed a considerable improvement, indeed in

l 7 ( i TORBEN ANDERSEN
some cases a complete subsidence of the pain, after resection of a portion of the affected artery, generally for diagnostic purposes (13, 38, 23, 2 , 16, 32, 5 , 34, 33, 7) . Scott & Maxwell state tha t the pain subsided, but the poor general health remained unin- fluenced by the resection, whereas MacDonald & Moser observed that both pain and fever subsided immediately after the resection. The favourable influence of this interference is presumably due to the fact that, when the artery is cut through, the peri- arterial sympathetic fibers are cut simultaneously. It may be mentioned that Sprague & MacKenzie saw no improvement of the pain in the head after the resection, which is attributed to the possibility that intracranial arteries may have been affected.
Considering the serious complications, especially those of the eyes, I believe I ought to recommend experiments with heparin- dicoumarol treatment as soon as the diagnosis has been established, and continued treatment as long as the danger of renewed throm- bus formation is believed to persist.
Comment. Temporal arteritis is merely a frequent manifestation of a
generalized vascular disorder that is easily diagnosed. The latter may occur without any affection of the temporal artery. It is difficult to establish the diagnosis in cases in which the super- ficial vessels are not affected. With our present knowledge of the disorder it should probably be more frequently diagnosed by means of post-mortem examination than has hitherto been the case. For this purpose the macroscopical post-mortem examina- tion of the organs of circulation should be supplemented with histological examinations of these organs to a greater extent than previously. This applies, of course, especially to the examination of patients with circulatory symptoms (thrombosis, hemorrhage in various organs).
Summary. 1. A case of temporal arteritis in a man, aged 54 years, is
reported. 2 . A survey is given of the history of the disease, its etiology,
pathology, symptomatology, diagnosis, differential diagnosis, prognosis, and treatment, and also, in a table, a survey of the cases hitherto published.

ARTERITIS TEMPORALIS (HORTOR). 177
3. It is emphasized tha t temporal arteritis is looked upon as a frequent manifestation of a generalized vascular disorder tha t is easy to diagnose. 4. The writer’s case complicated with glaucoma. It is considered
a consequence of involvement of the ocular veins. 5. The uncertain prognosis of the disorder is stressed in contrast
with the previous prognostic view. 7 out of 56 patients died in connection with the disease, 24 developing more or less severe ocular symptoms.
6. It is recommended t o t r y heparin-dicoumarol treatment at a n early stage of the disorder.
References.
1. Bain, C. W. C.: Lancet 1: 517, 1938. - 2. Bowers, J. M.: Arch. Int. Med. 66: 384, 1940. - 3. Broch, 0. J. & Ytrehus, 8.: Nord. Med. 30: 1251, 1946. - 4. Brown, J. W. & Hampson, I?.: Brit. Heart J. 6: 154, 1944. - - 5. Chasnoff, J. & Vorzimer, J. J.: Ann. Int. Med. 20: 327, 1944. - 6. Chavany, J.-A.: Presse m6d. 44. I : 347, 1936. - 7 . Cooke, W. T., Cloake, P. C. P:, Govan, A. D. T. & Colbeck, J. C.: Quart. J. Med. 15: 47, 1946. - 8. Dick, G. F. & Freeman, G.: J. A. M. A. 114: 645, 1940. - 9. Eckerstrom, S.: Nord. Med. 25: 585, 1945. -- 10. Eckerstrom, S.: Acta med. Scandinav.: Xuppl . 170: 169, 1946. - 11. Gilmour, J. R.: J. Path. Bact. 53: 263, 1941. - 12. Hines, E. A.: Arteritis temporalis. In: Stroud, W. D. (edit.): Diagnosis and Treatment of cardiovascular Disease. Fasc. 2, sec. edition, F. A. Davis Comp., Philadelphia, 1941, P. 1681. - 13. Horton, B. T. & Magath, T. B.: Proc. Staff Meet., Mayo Clin. 12: 548, 1937. - 14. Horton, B. T., Magath, T. B. & Brown, G. E.: Proc. Staff Meet., Mayo Cliii. 7 : 700, 1932. - 15. Horton, B. T., Magath, T. B. & Brown, G. E.: ilrch. Int. Med. 53: 400, 1934. - 16. Hoyt, L. H., Perera, G. A. & Kauvar, A. J.: New England J. Med. 225: 283, 1941. -- 17. Jennings, G. H., Lancet 1: 424, 1938. - 18. Jersild, P. M. ,Acut Blindhed efter Hzematemese)). To be published in Ugeskr. f. Laeger. - 19. Johnson, R. H., Harley, R. D. & Horton, B. T.: Am. J. Ophth. 26: 147, 1943. - 20. Kershner, C. M.: Blood supply of the visual pathway. Thesis, University of Minnesota, 1940 (cit. Johnson et al.). - 21. Kilbourne, E. D. & Wolff, H. G.: Ann. Int. Med. 24: 1, 1946. -- 22. Lucien, M., Mathieu & Verain, M.: Arch. d. mal. du coeur 32: 603, 1939. -- 23. MacDonald, J. A. & Moser, R. H.: Ann. Int. Med. 10: 1721, 1937. - 24. Murphy, J. R.: New York State J. Med. 42: 2236, 1942. - 25. Oldberg, S.: Nord. Med. 16: 3213, 1942. -- 26. Paviot, J., Chevallier, R., Guichard, A. & Damez, M.: Lyori med. 154: 45, 1934. - 27. Plaut, A.: New York State J. Med. 42: 346, 1942. - 28. Post, L. T. & Sanders, T. E.: Tr. Am. Ophth. SOC. 41: 241, 1943. - 29. Profant, H. J.: Ann. Otol., Rhin. & Laryng.

178 TORBEN ANDLRShN.
53: 308, 1944. - 30. Schaefer, C. L. & Sanders, C. E.: Am. Heart J . 84: 410, 1942. - 31. Schmidt, M.: Bibliot. f. L=ger 122: 269, 1930. (Case 24, Pg. 320). Brain 53: 489, 1930. (Case 24, Pg. 532). -
32. Scott, T. & Maxwell, E. S.: New Internat. Clin. 2: 220, 1941. --- 33. Shannon, E. W. & Solomon, J.: J. A. M. A. 127: 647, 1945. - 34. Sjovall, B. & U'inblad, S.: Acta path. e t microbiol. Scandinav. SuppZ. 54: 385, 1944. ~- 35. Sprague, P. H. &. MacKenzie, W. C.: Canad. M. A. J . 43: 562, 1940. - 36. Sproul, E. E.: New York State J. Med. 42: 345, 1942. - 37. Sproul, E. E. 8: Hawthorne, J. J.: Ani. J. Path. 13: 311, 1937. - 38. Thhenard, M.: Bull. e t mkm. SOC. d. chirurgiens de Paris, 31: 136, 1939. - 39. Warburg, E.: Kredslobssyg- tlommcnc. In: Paber, Knud (edit.): Nordisk Lsrebog i Intern Mcdicin. P a x . IV, 2nd edit., Copenhagen: Gyldendal 1946. P. 343.