Embed Size (px)
Citation preview
Arthroscopic Findings and Treatment of Shoulder Instability
Emmanuel Antonogiannakis,M.D.
Center For Shoulder arthroscopy
IASO gen. hospital
Athens Greece
The Shoulder
Greatest Range of Motion in the Body
Motion in all 3 planes of movement
Prone to injuries
8-20% of all sports injuries
How common is shoulder dislocation;
2% of the general population
90% anterior
Classification SchemesClassification Schemes
• Mechanism– Traumatic– Atraumatic– Congenital– Neuromuscular
• Frequency– Acute– Chronic– Recurrent– Involuntary– Voluntary
• Mechanism– Traumatic– Atraumatic– Congenital– Neuromuscular
• Frequency– Acute– Chronic– Recurrent– Involuntary– Voluntary
• Direction– Anterior (and inferior)– Posterior (and inferior)– Superior?– Multidirectional
• Extent– Subluxation– Dislocation
• Direction– Anterior (and inferior)– Posterior (and inferior)– Superior?– Multidirectional
• Extent– Subluxation– Dislocation
TRAUMA
What is Traumatic Shoulder Instability ?
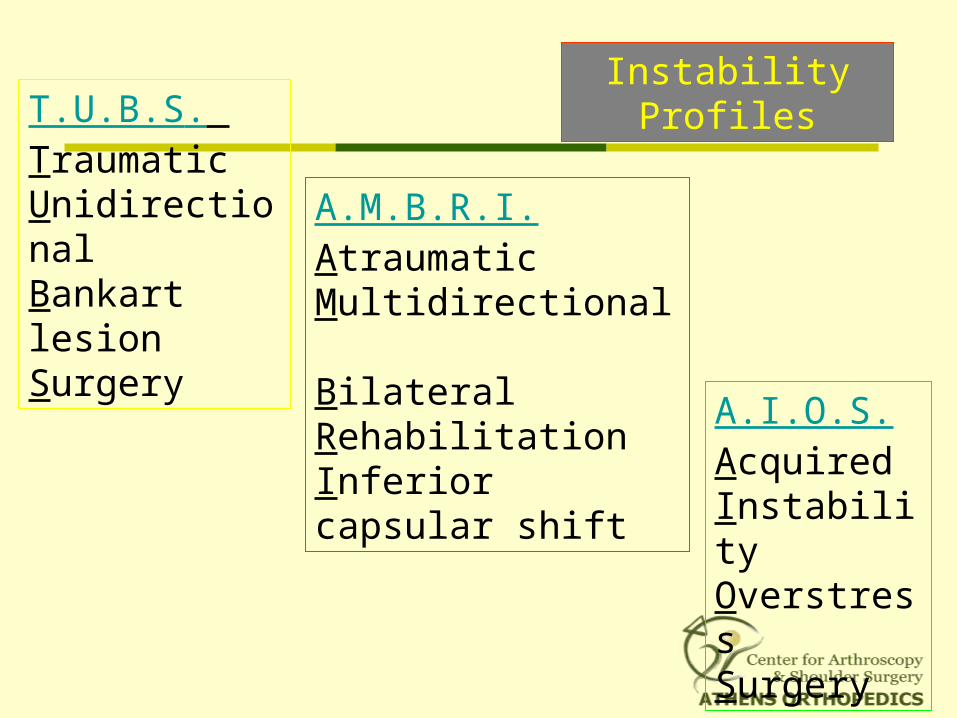
T.U.B.S. Traumatic Unidirectional Bankart lesion Surgery
A.M.B.R.I. Atraumatic Multidirectional Bilateral Rehabilitation Inferior capsular shift A.I.O.S.
Acquired Instability Overstress Surgery
Instability Profiles
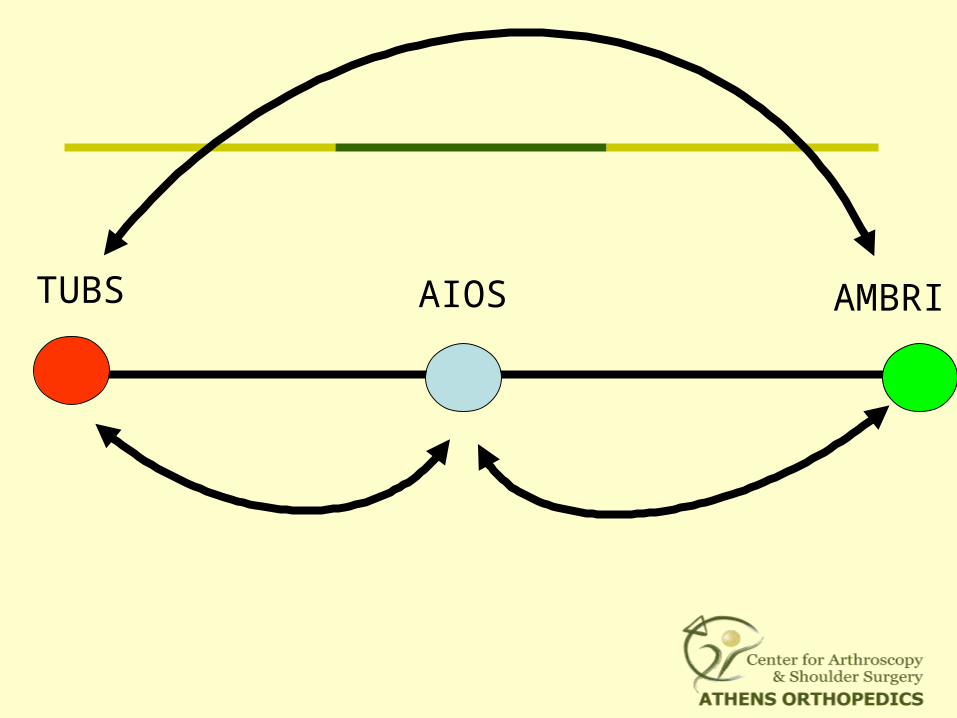
TUBS AIOS AMBRI
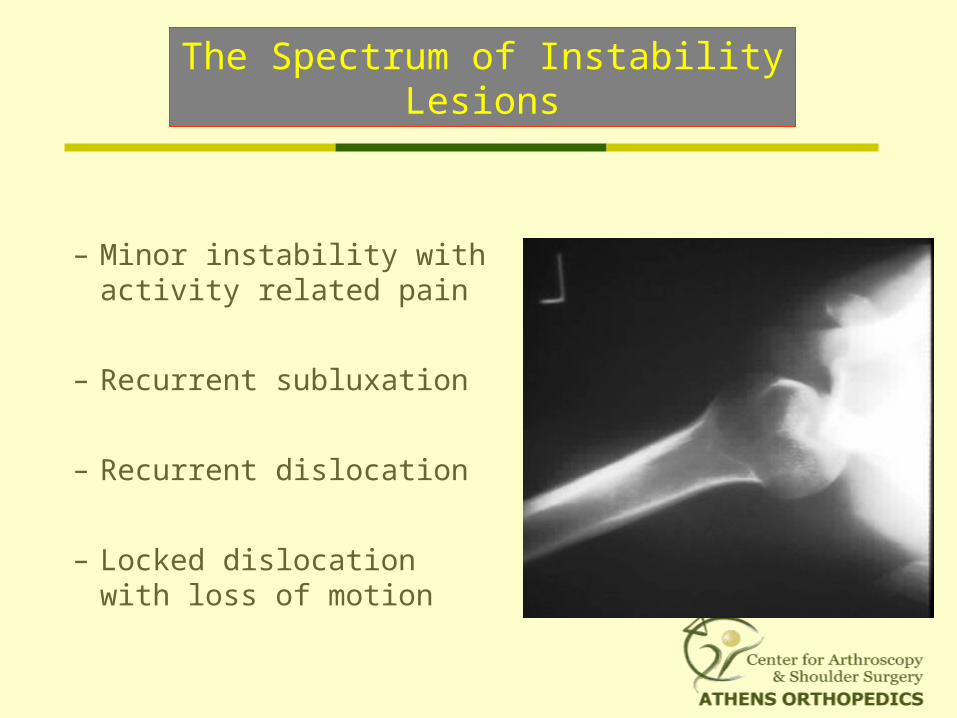
The Spectrum of Instability Lesions
– Minor instability with activity related pain
– Recurrent subluxation
– Recurrent dislocation
– Locked dislocation with loss of motion

The Most Important Factors In Treating Instability Are
Recognizing It And Defining It.
Instability
Biomechanical Dysfunction
Failure of static and dynamic stabilizers
Ranges from mild subluxation to
traumatic dislocation
Direction of the Instability
Unidirectional
Bidirectional
Multidirectional
Anterior
Posterior
Mechanisms of Glenohumeral Stability
• Static
• Dynamic
• Negative Intra- articular pressure
Labrum (50% of Glenoid depth)CapsuleLigaments- Glenohumeral- Superior, Middle & Inferior
(stability & proprioception) Rotator cuff tension
Glenohumeral LigamentVariations
66% - Well defined SGHL, MGHL & IGHL
7% - Confluent MGHL & IGHL19% - Cordlike MGHL with a high
riding attachment8% - No discernable MGHL – IGHL but
one confluent anterior capsular sheath
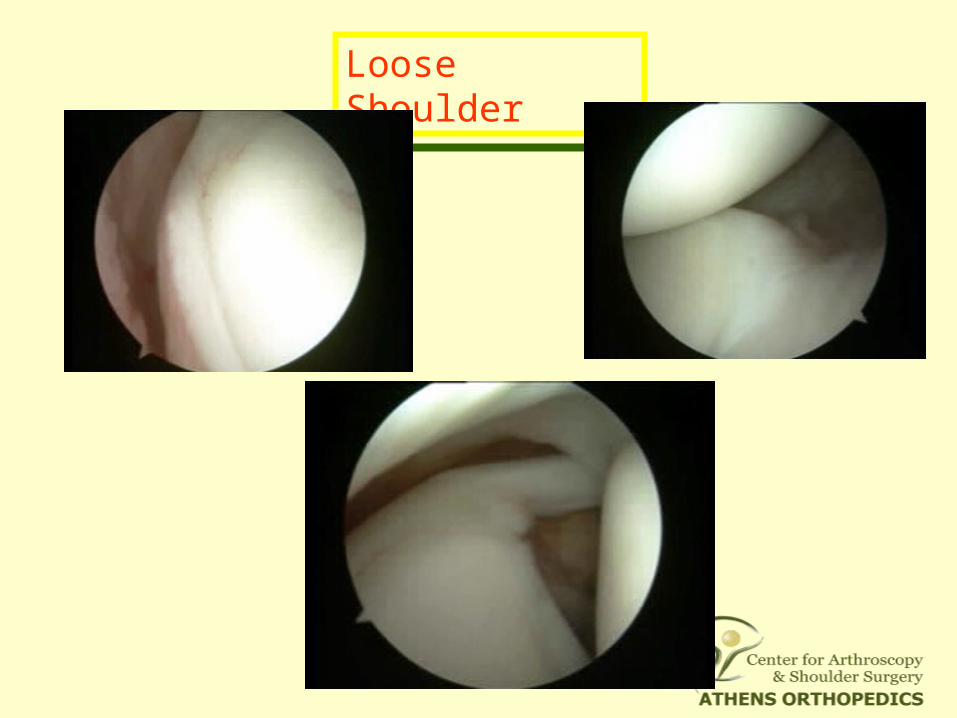
Loose Shoulder
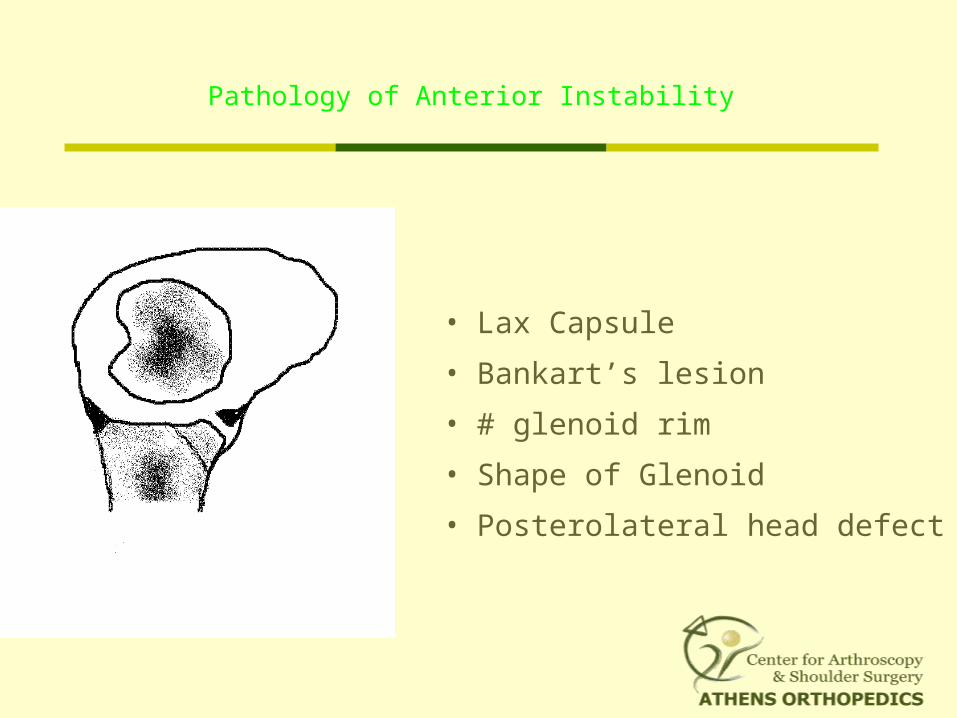
Pathology of Anterior Instability
• Lax Capsule
• Bankart’s lesion
• # glenoid rim
• Shape of Glenoid
• Posterolateral head defect
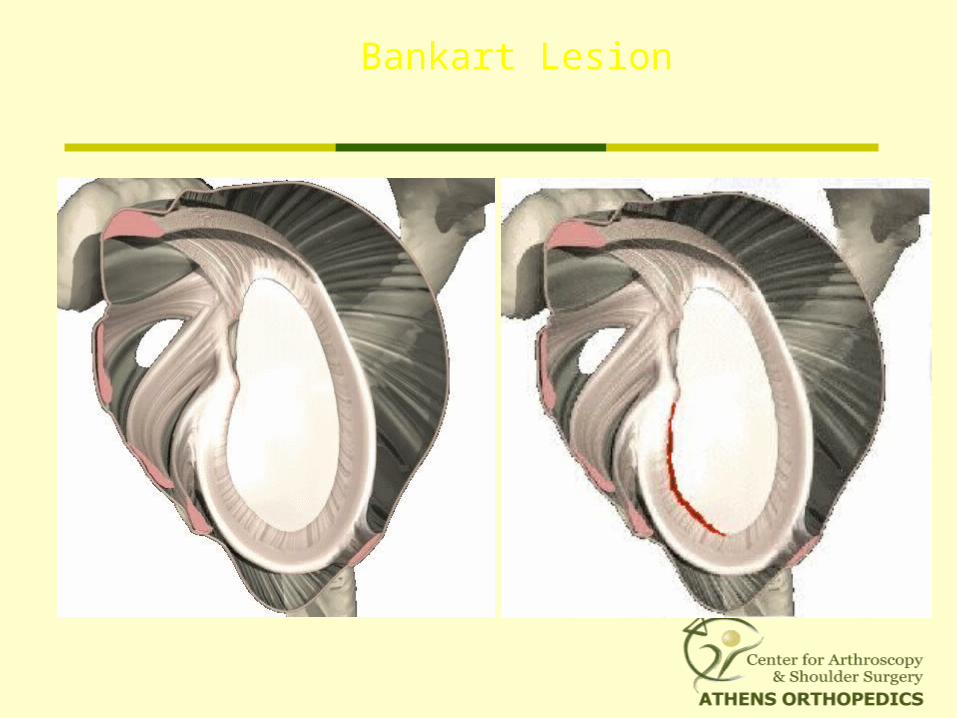
Bankart Lesion
the essential lesion
Avulsion of the IGHL from the glenoid rim
from 2 o’clock to 6 o’clock
Primary restraint to anterior translation
at 90o of abduction
85% in traumatic anterior dislocations
Not enough to induce symptomatic instability
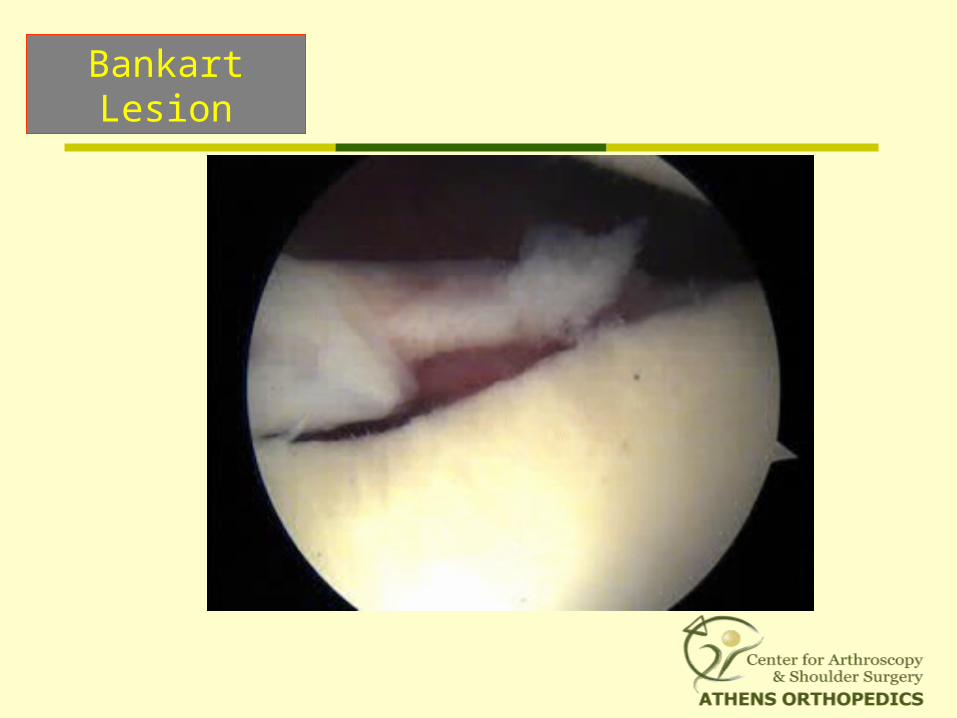
Bankart Lesion
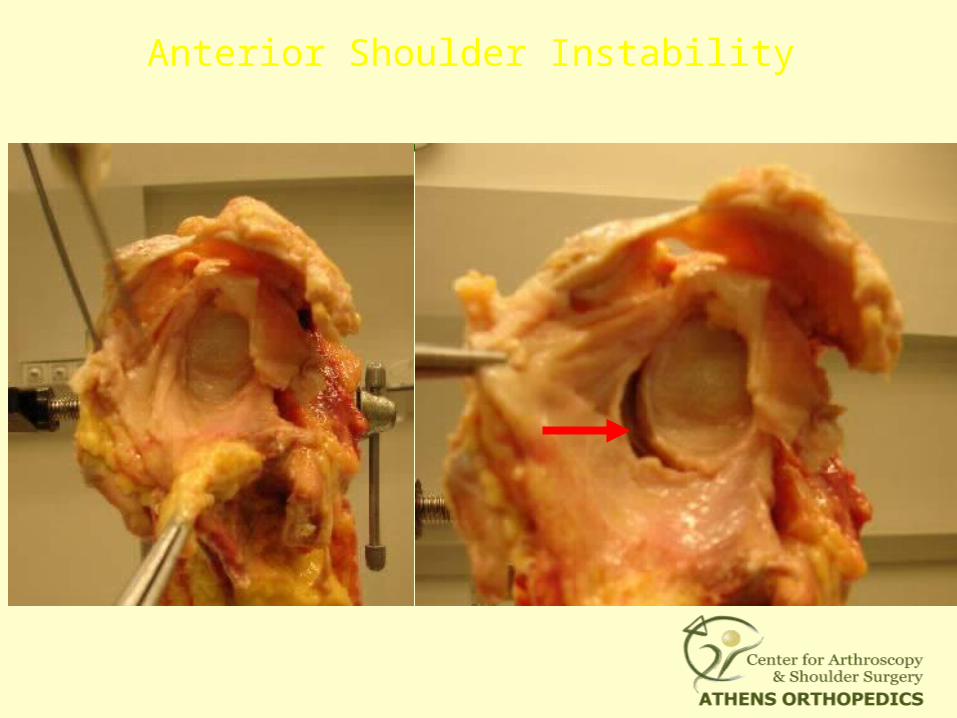
Anterior Shoulder Instability
Bankart Lesion
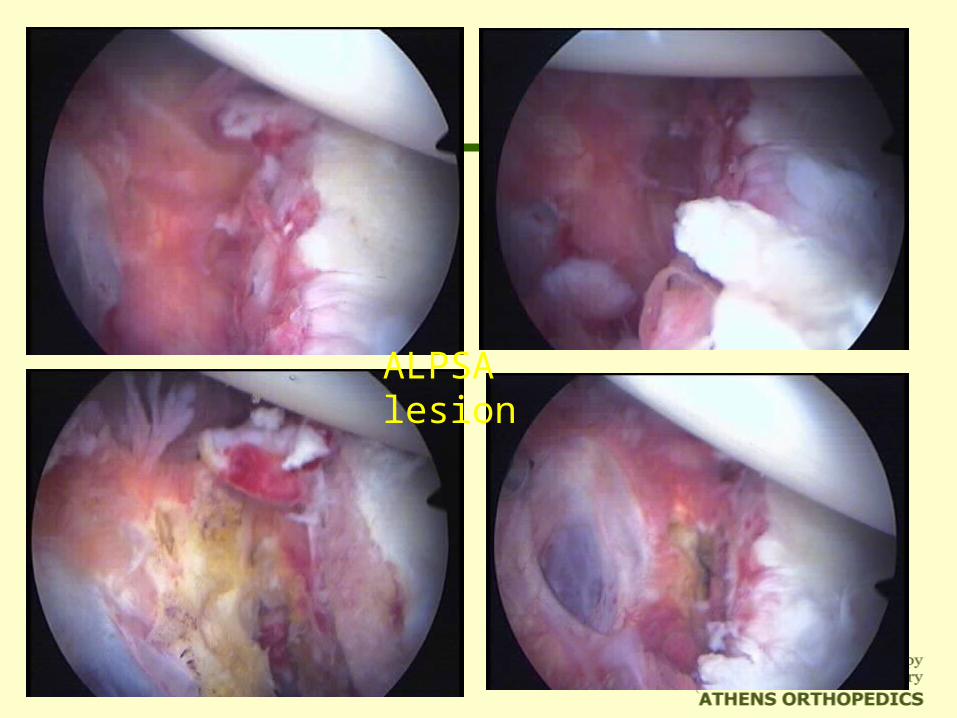
ALPSA lesion
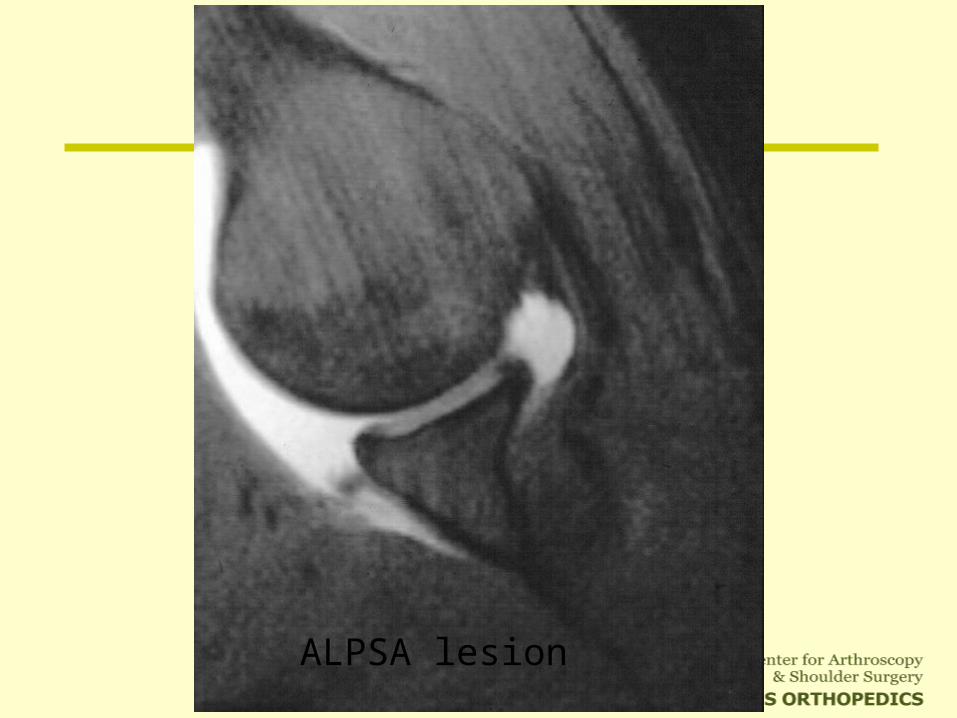
ALPSA lesion
Recurrent dislocations also can cause
stretching of the glenohumeral capsule and
ligaments
This plastic deformation occurs
from repetitive loading
Bankart Lesion Equivalent
BONY LESIONS• Humeral Head• Glenoid rim
LABRAL - LIGAMENTOUS INJURY • Bankart lesion• A.L.P.S.A.• H.A.G.L. • Capsular Tear
INCREASED CAPSULAR VOLUME • Atraumatic elongation• Traumatic stretch
Associated Lesions
BICEPS LESIONS
ROTATOR CUFF TEARS • Partial thickness • Full thickness
ROTATOR INTERVAL PATHOLOGY• Widening• Synovitis• Rupture
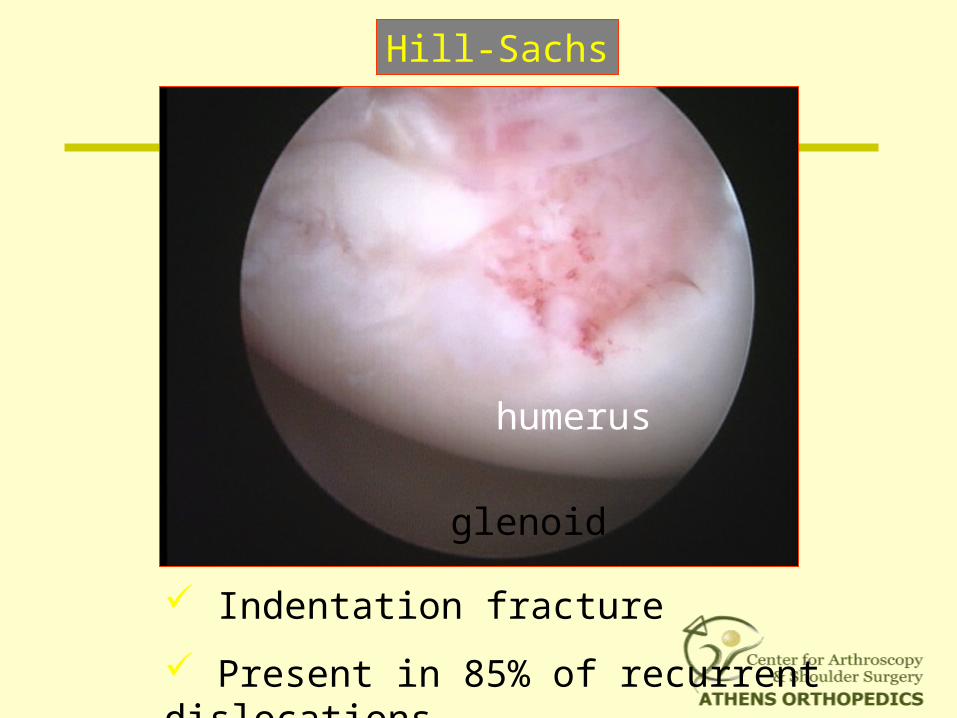
Hill-Sachs
humerus
glenoid
Indentation fracture
Present in 85% of recurrent dislocations
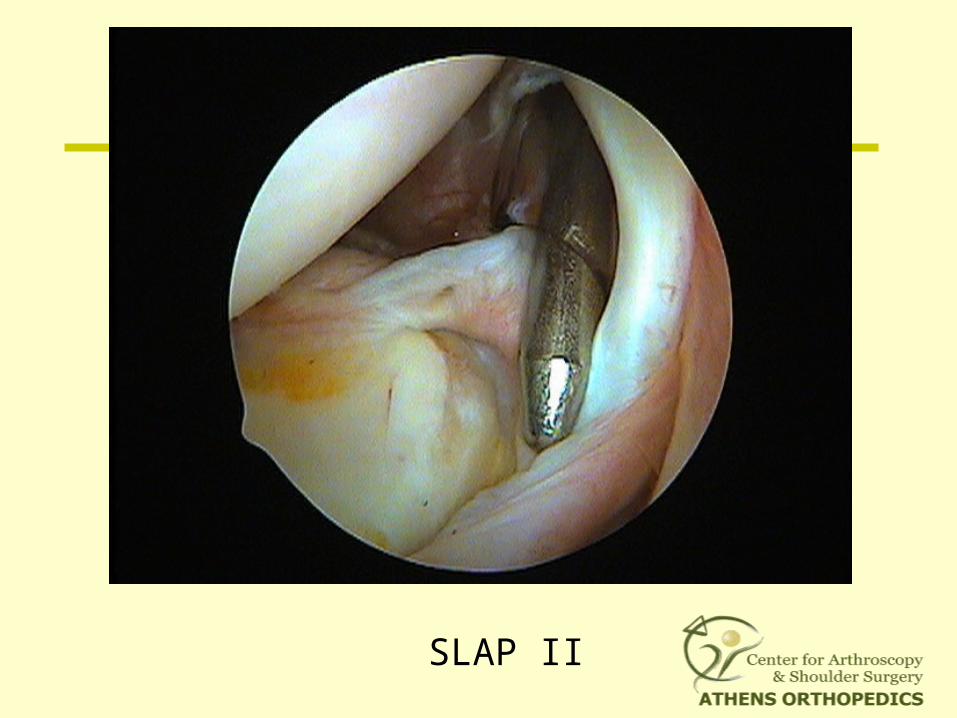
SLAP II
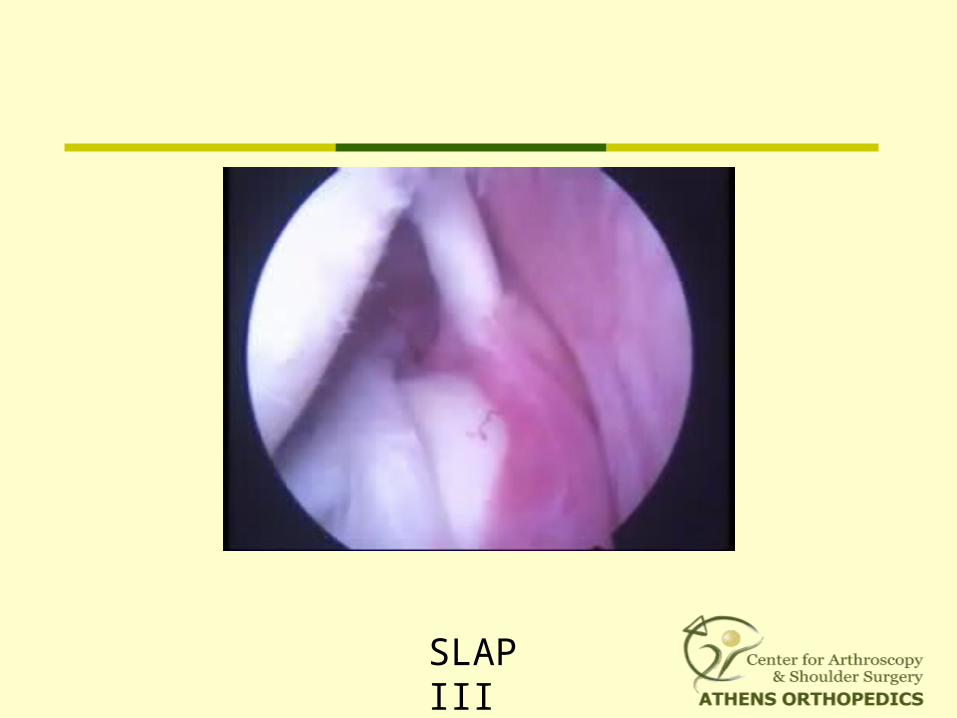
SLAP III
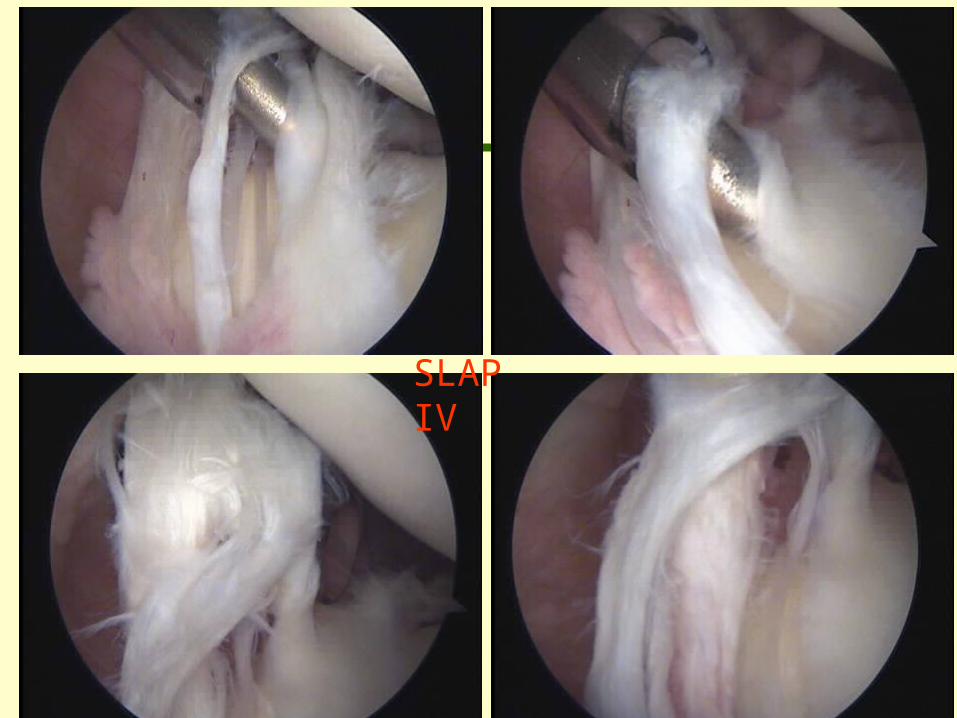
SLAP IV
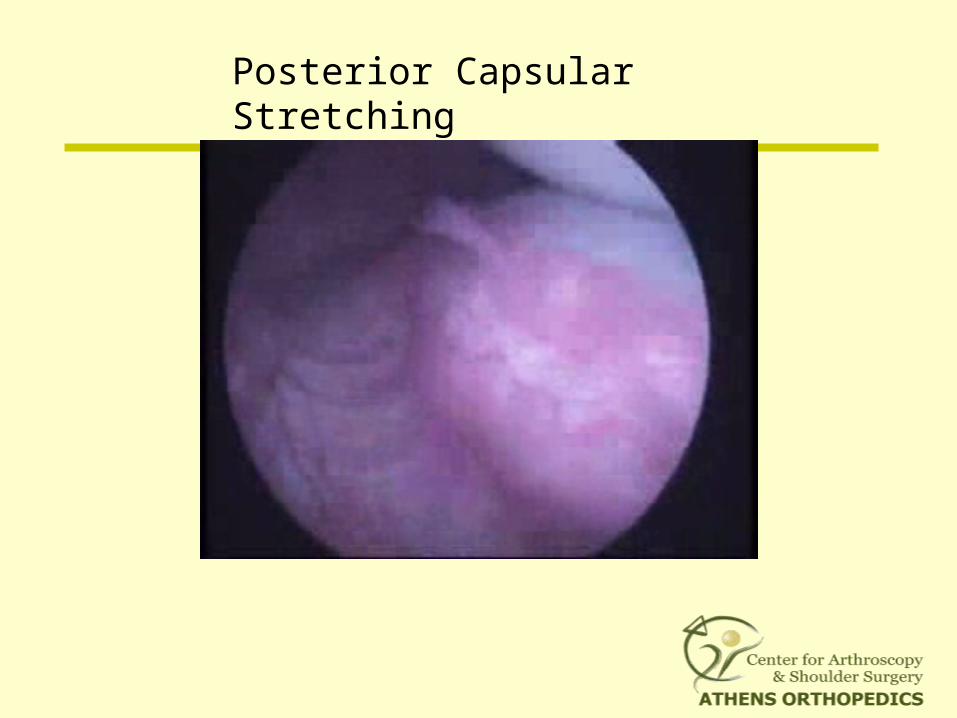
Posterior Capsular Stretching
Patients of all ages and all activity levels with recurrent anterior instability who are impaired functionally and in whom nonoperative treatment has failed
Revision stabilization
First-time, acute shoulder dislocations
Arthroscopic Shoulder Stabilization
Patient Selection
Arthroscopic Shoulder Reconstruction
Goal of the Operation:
Restoration of the Labrum to
its anatomic attachment
Reestablishment of the appropriate tension
in the GH ligaments
and capsule
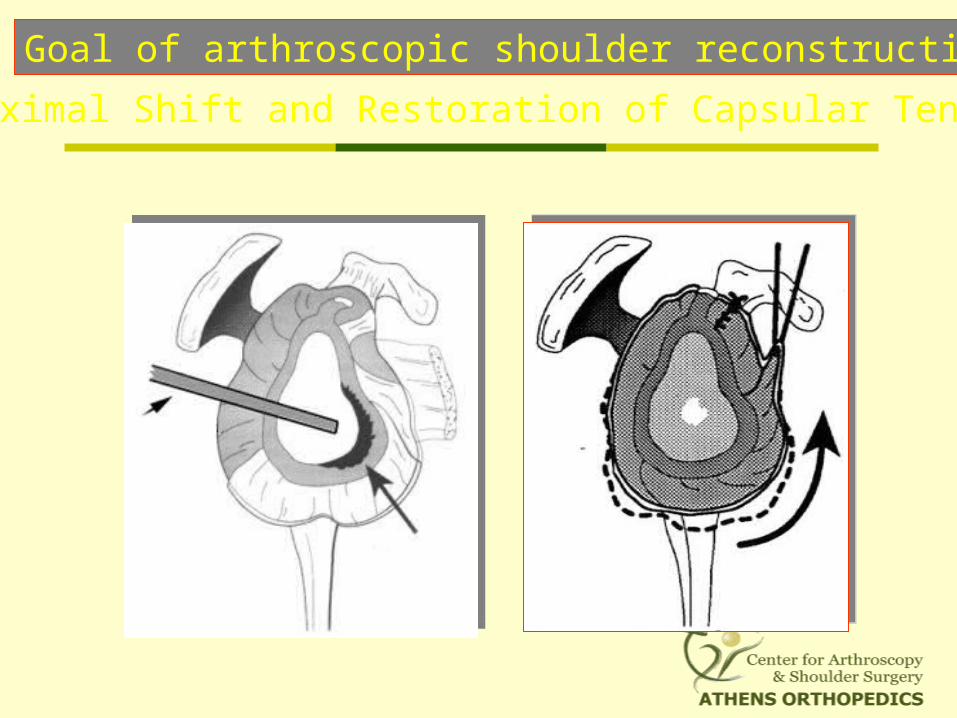
Goal of arthroscopic shoulder reconstruction
Proximal Shift and Restoration of Capsular Tension
Examination Under Anaesthesia
In various degrees of abduction and ER
Side-to-side comparisons
Sulcus sign
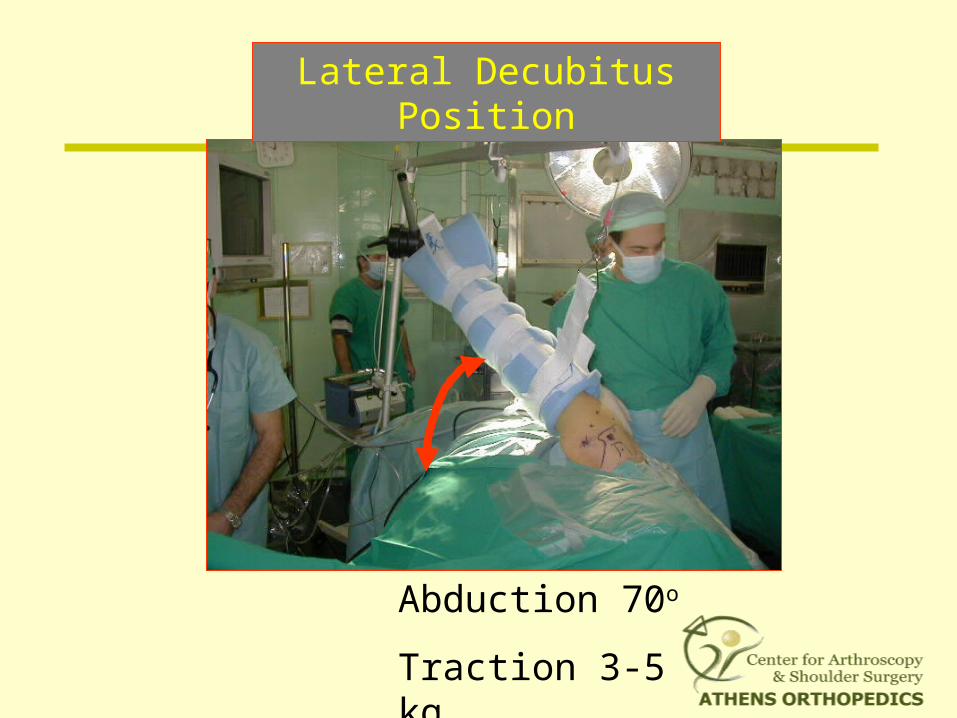
Lateral Decubitus Position
Abduction 70o
Traction 3-5 kg
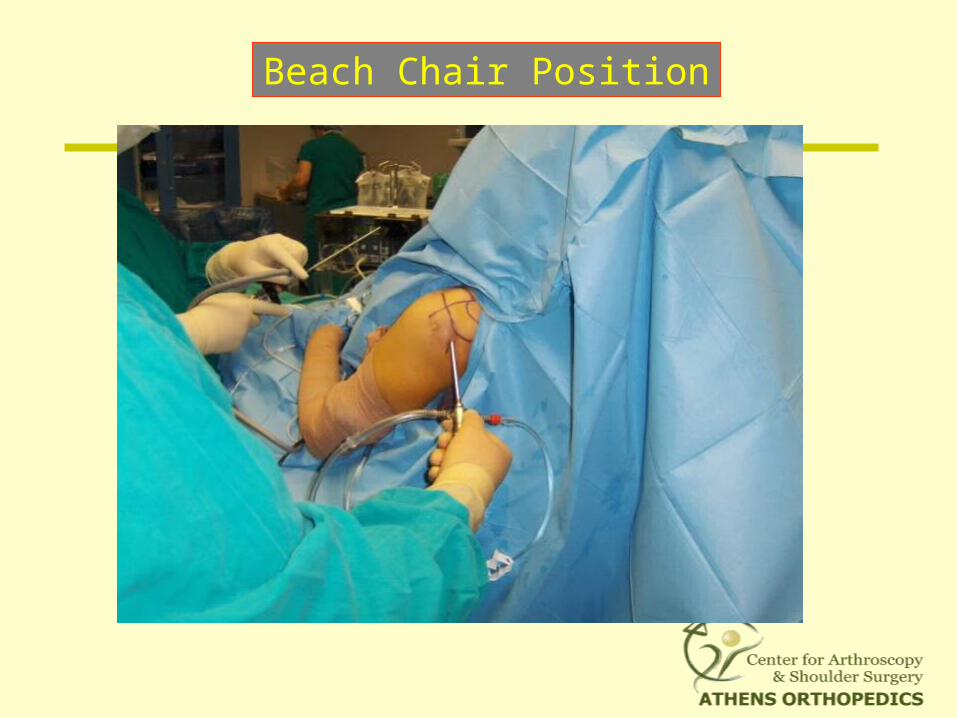
Beach Chair Position
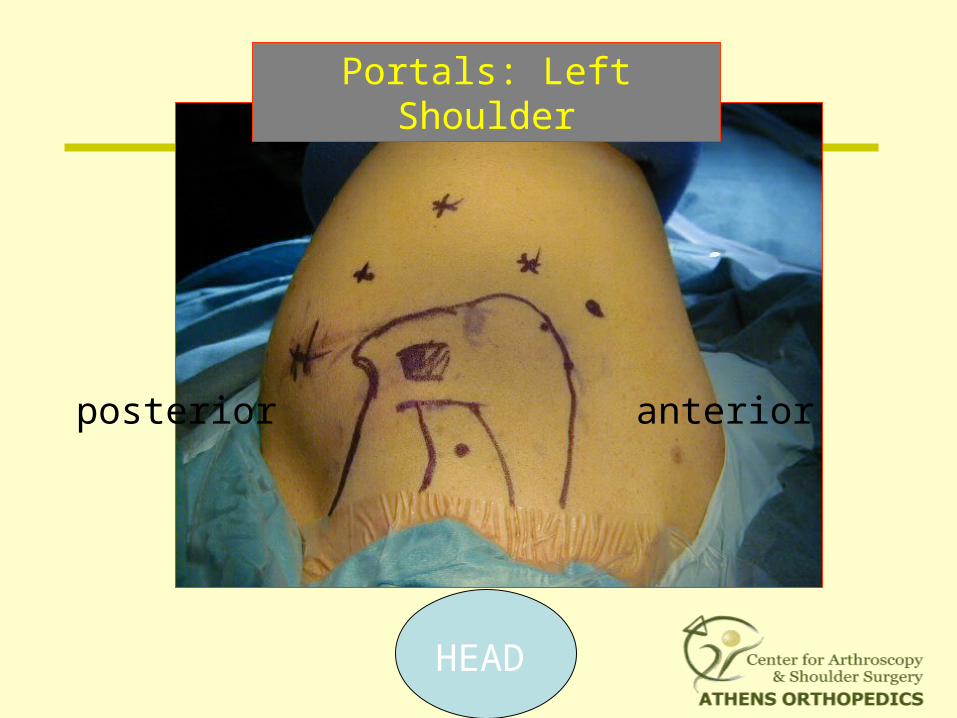
Portals: Left Shoulder
HEAD
anteriorposterior
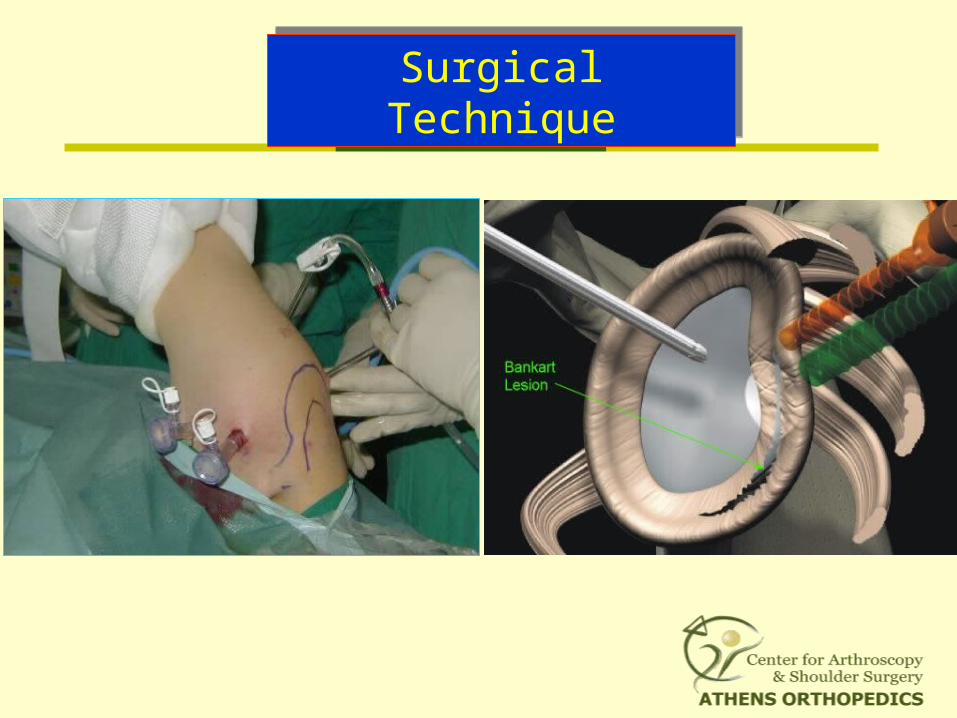
Surgical TechniqueSurgical Technique
Arthroscopic Reconstruction: Technique
1. Define Pathology
2. Debride damaged tissue
3. Release capsule to/past 6 o’clock
4. Free off subscapularis
5. Abrade glenoid
6. Repair capsulolabral complex
7. Associated Injuries (Posterior capsule, Rotator Interval, SLAP)
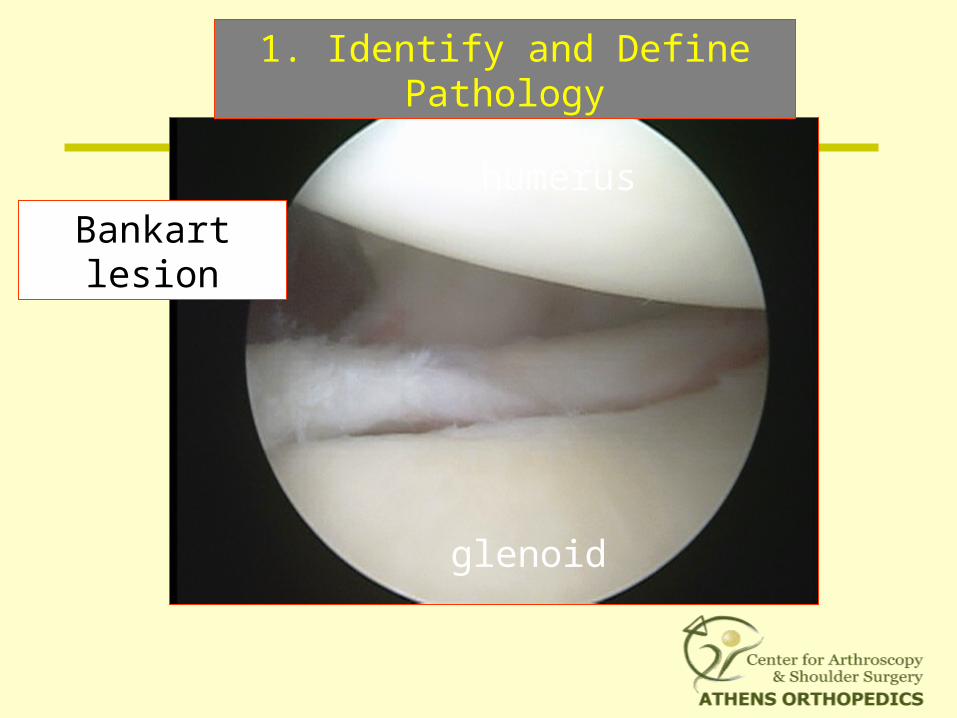
humerus
Bankart lesion
glenoid
1. Identify and Define Pathology
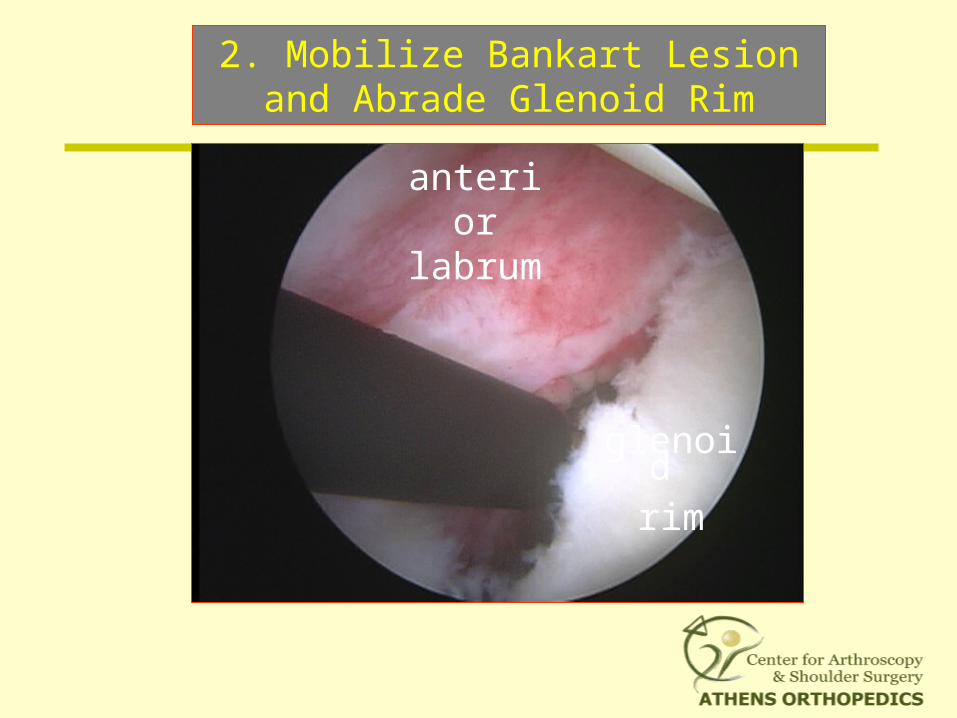
glenoid rim
anterior labrum
2. Mobilize Bankart Lesion and Abrade Glenoid Rim
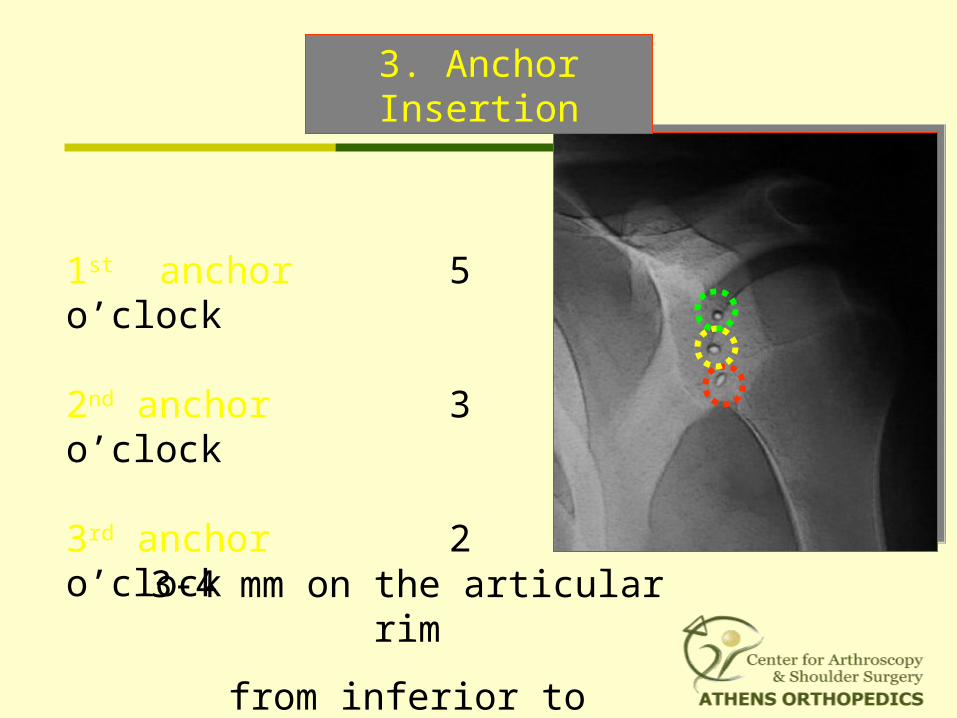
1st anchor 5 o’clock
2nd anchor 3 o’clock
3rd anchor 2 o’clock
3. Anchor Insertion
3-4 mm on the articular rim
from inferior to superior
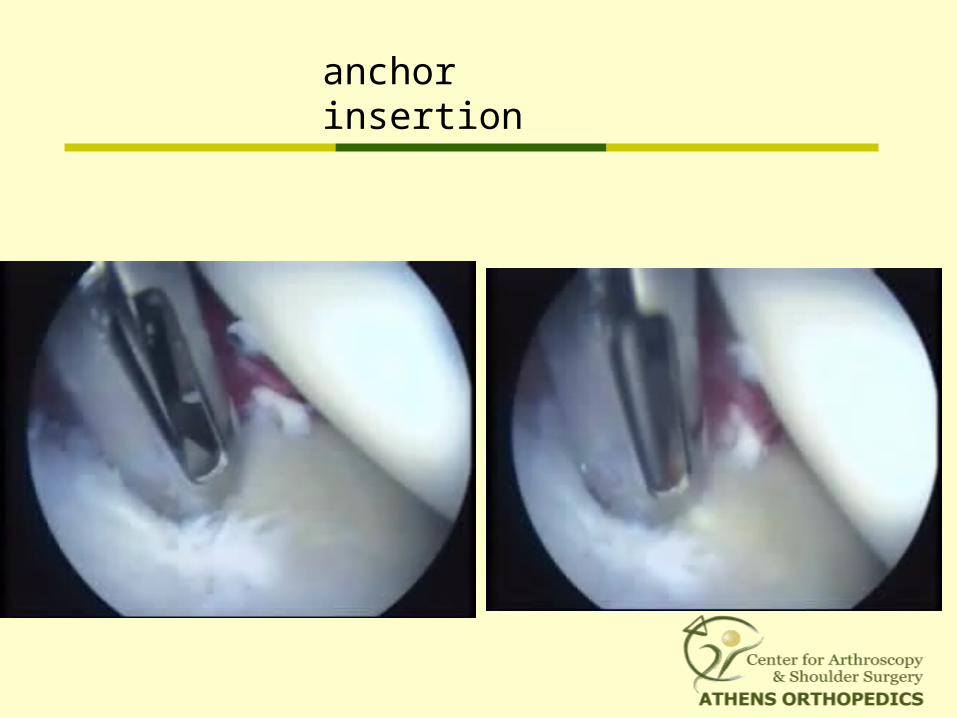
anchor insertion
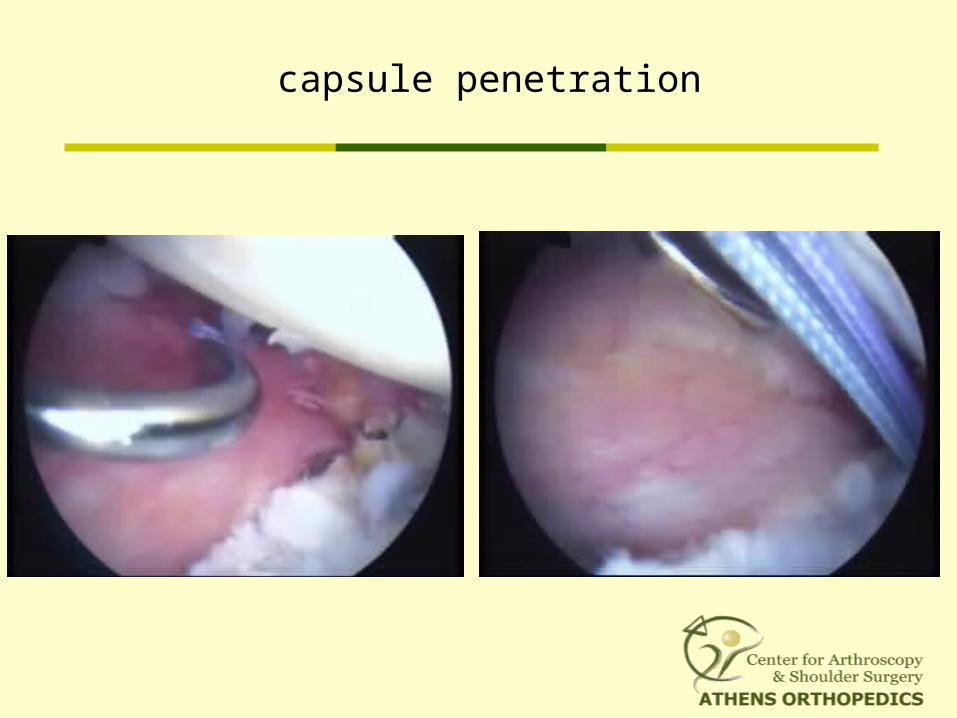
capsule penetration
humerus
labrum
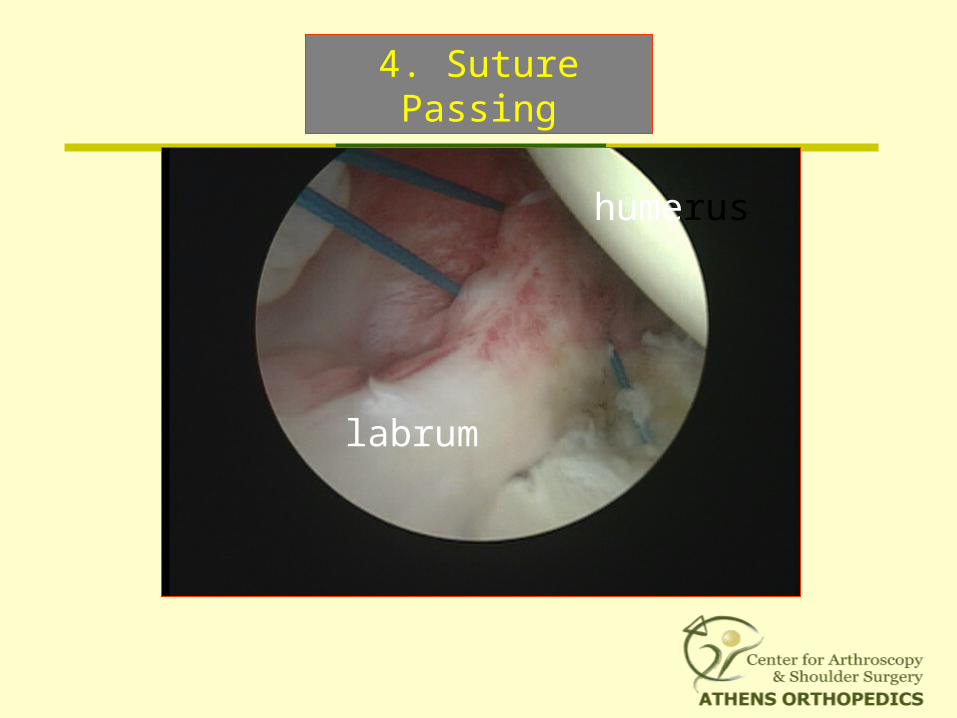
4. Suture Passing
humerus
labrum
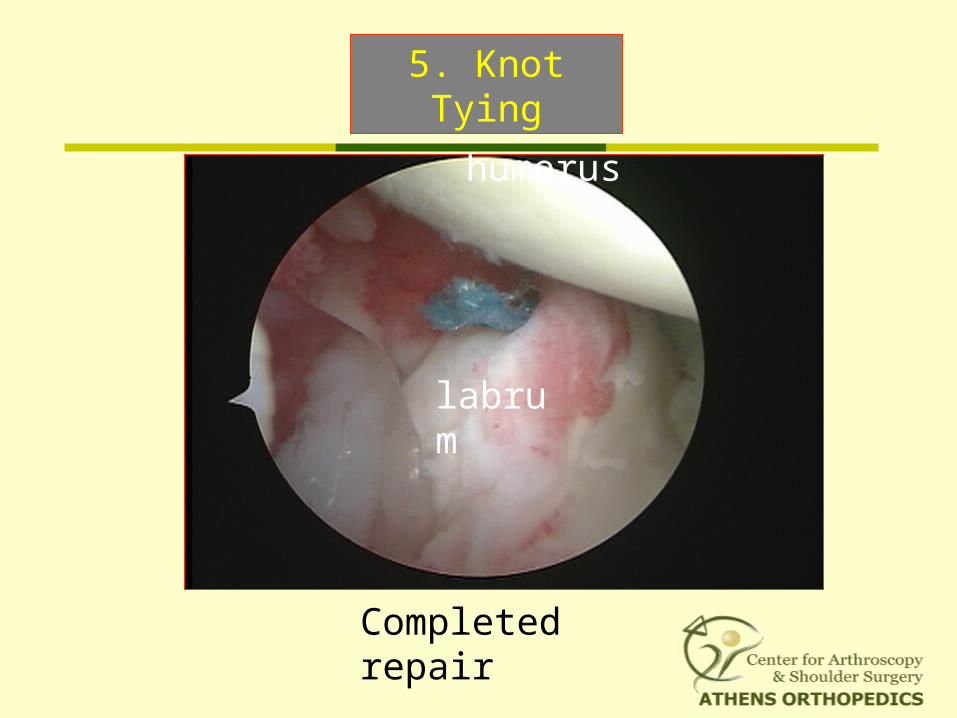
Completed repair
Capsular shift
5. Knot Tying
humerus
labrum
completed repair
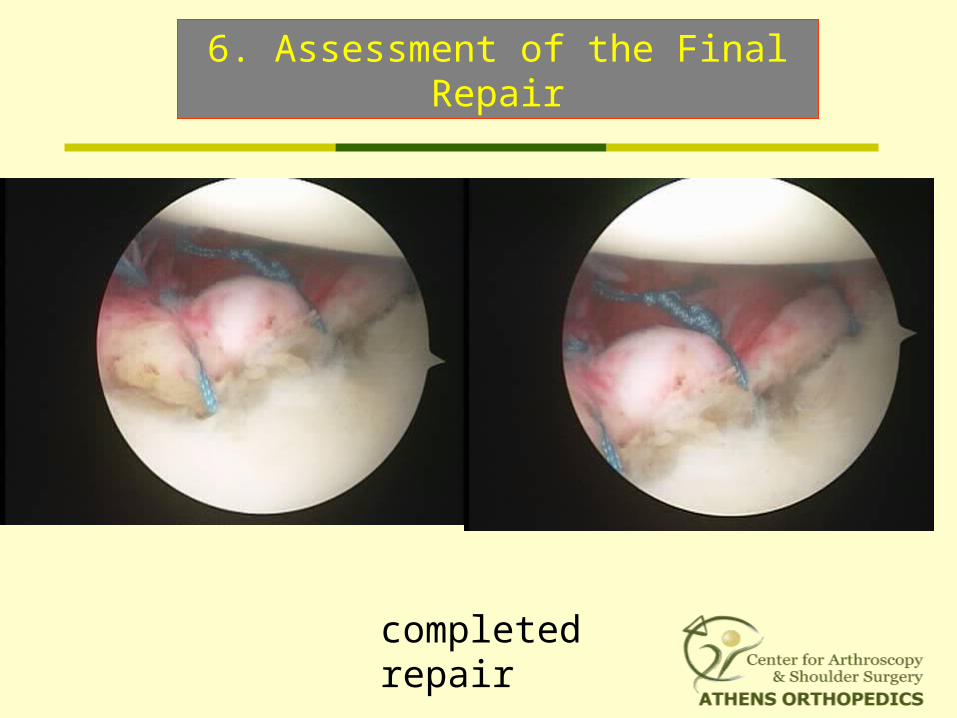
6. Assessment of the Final Repair
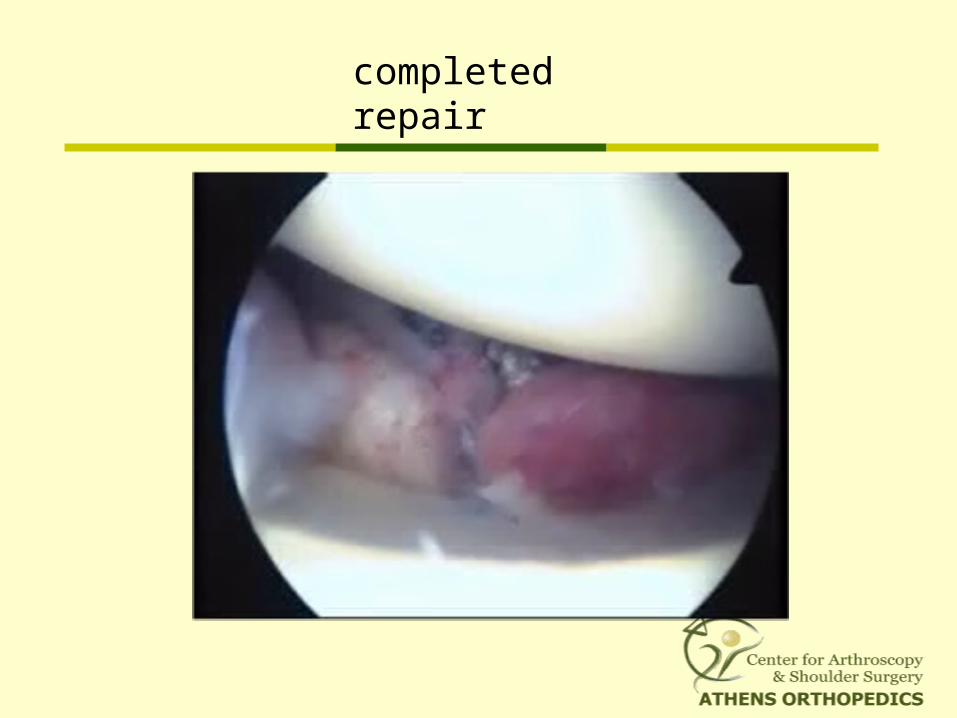
completed repair
7. Associated Pathology
RI laxity
Posterior Capsule
Ant. Capsular Stretch
HAGL
SLAP
Hill-Sachs
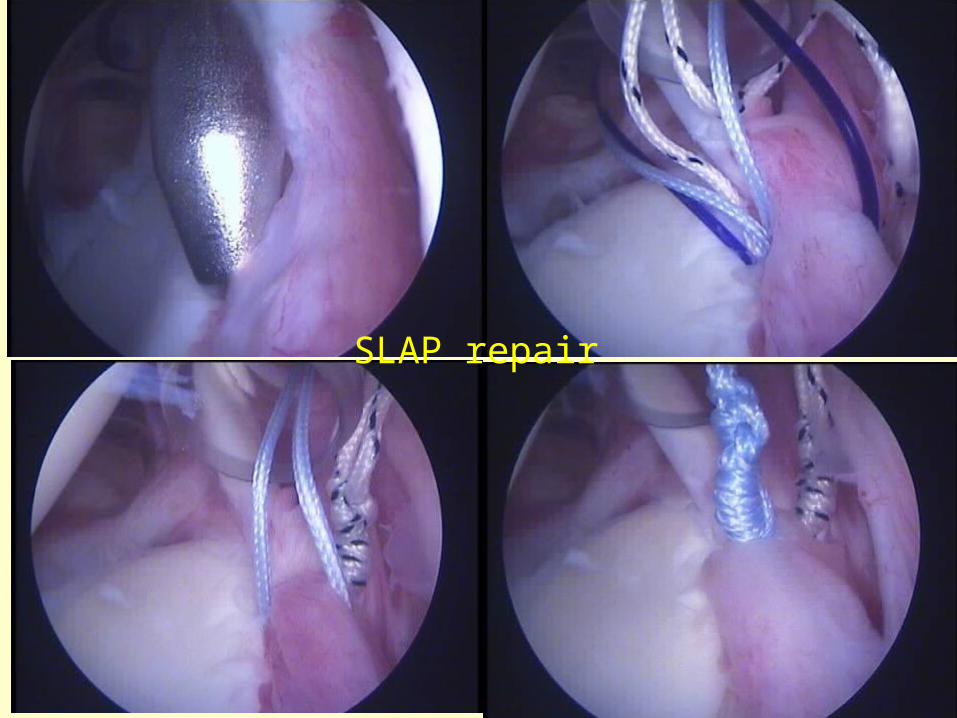
SLAP repair
the capsular “pinch-tuck” technique
adjunctive thermal treatment
rotator interval closure
How to Reduce Capsule Redundancy
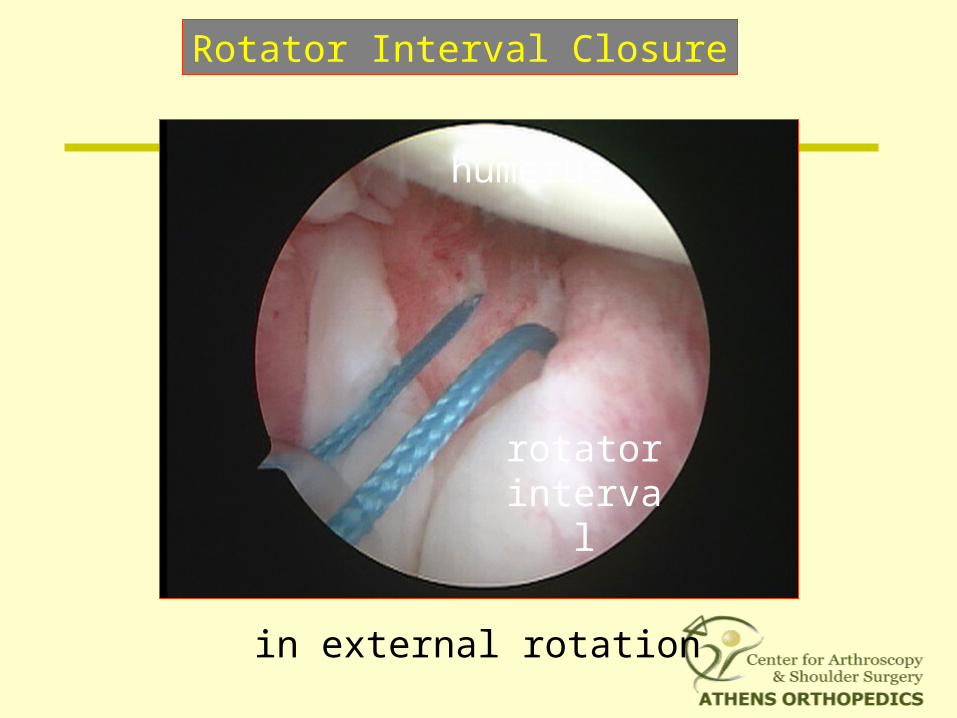
humerus
rotator interval
Rotator Interval Closure
in external rotation
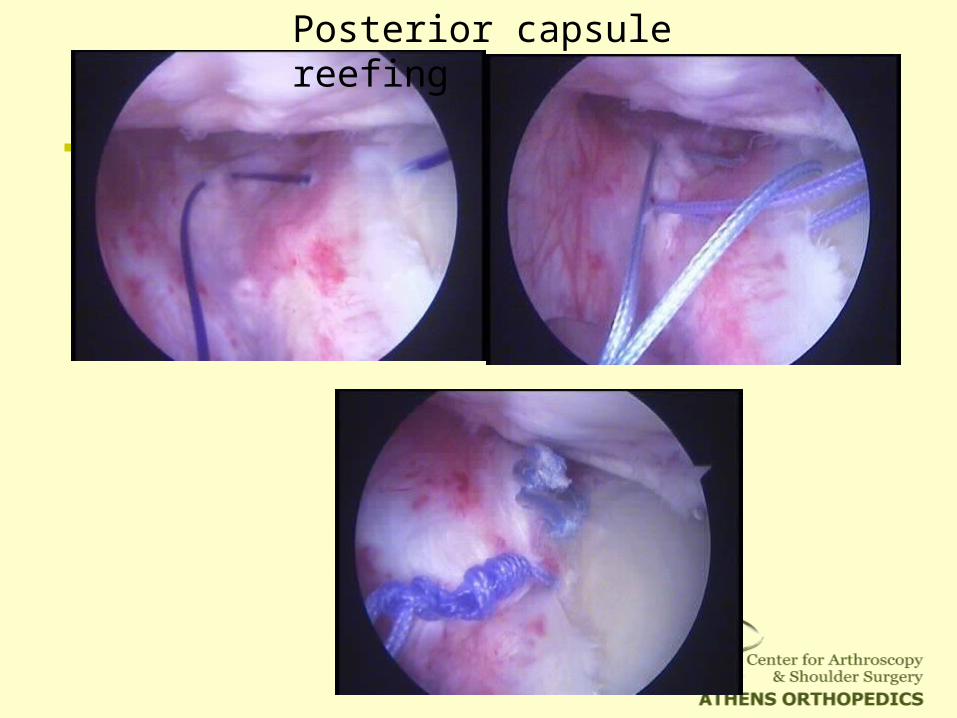
Posterior capsule reefing
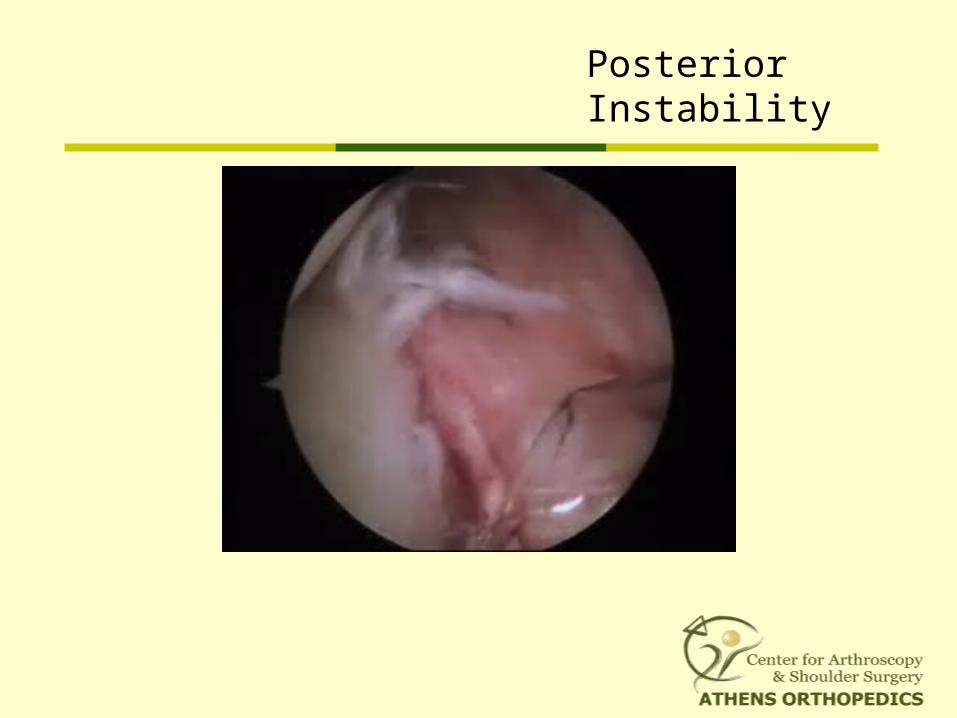
Posterior Instability
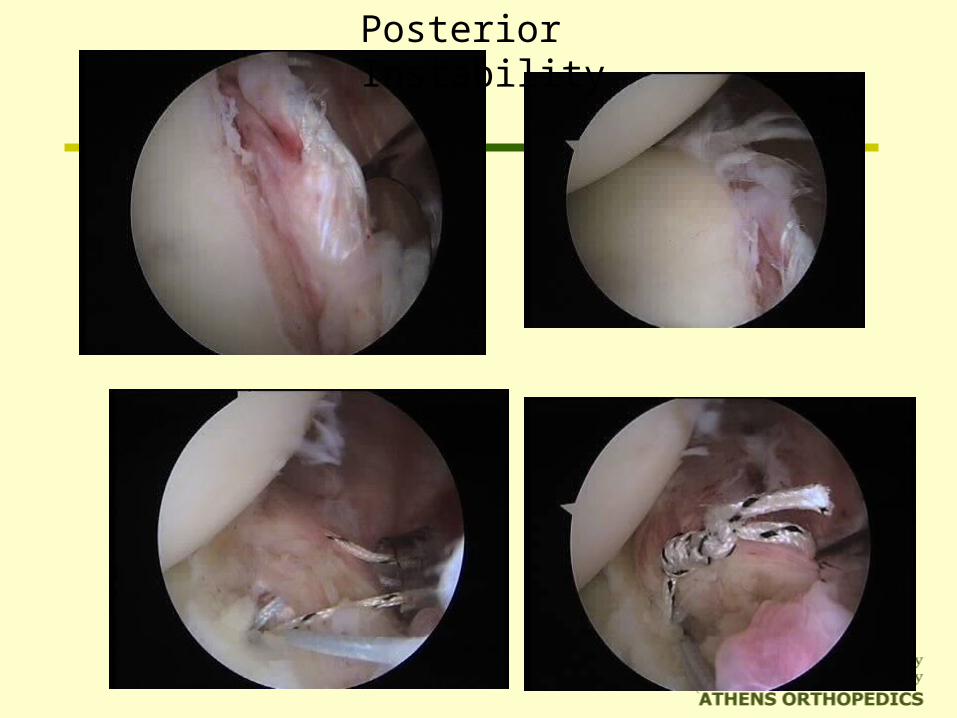
Posterior Instability
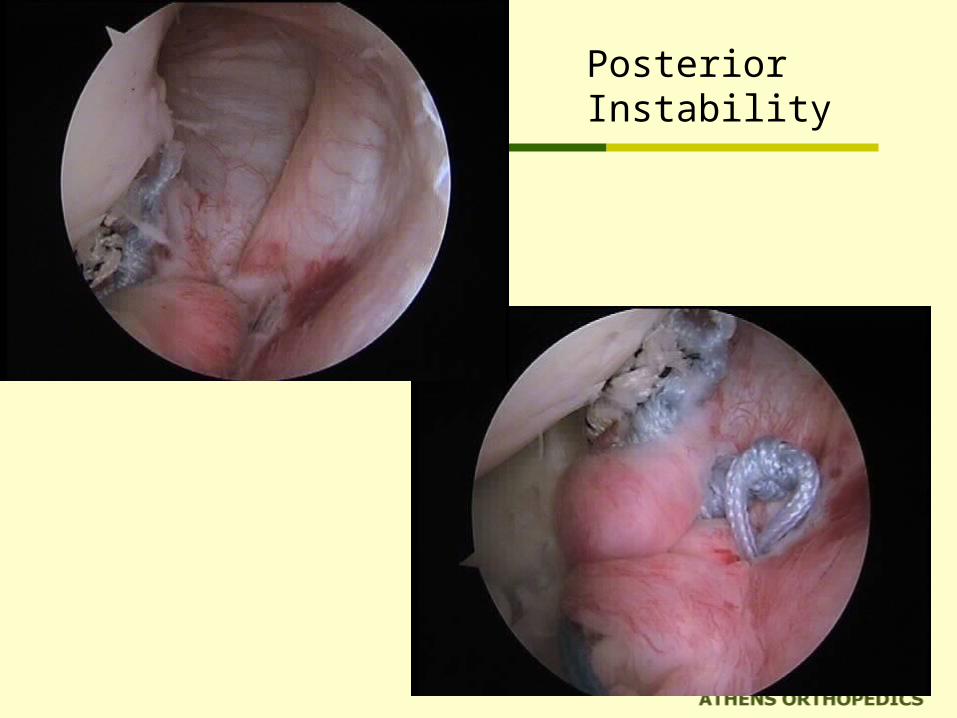
Posterior Instability
Bankart Lesion Healing
A second-look arthroscopic study
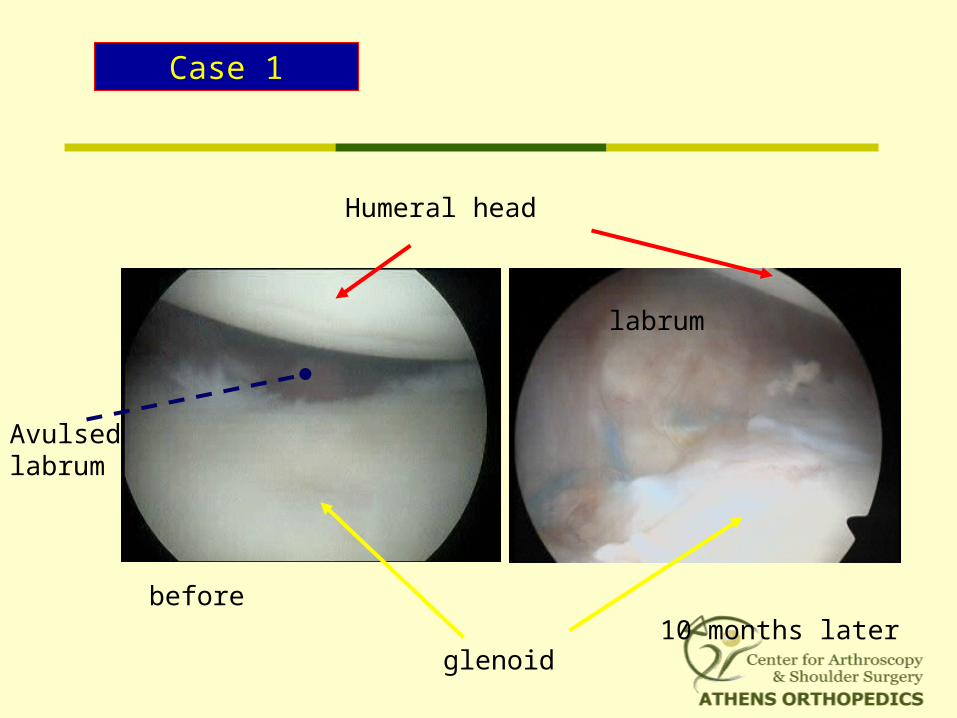
Case 1
labrum
Humeral head
glenoid10 months later
before
Avulsed labrum
Postoperative Rehabilitation
Sling for 4/52
Isometrics and pendulum exercises immediately
Active forward elevation may begin after 3/52
External rotation to 30° to 40° at 4/52
Progressive strengthening at 8/52
Return to sport at 18 to 36 weeks
supervised and individualized
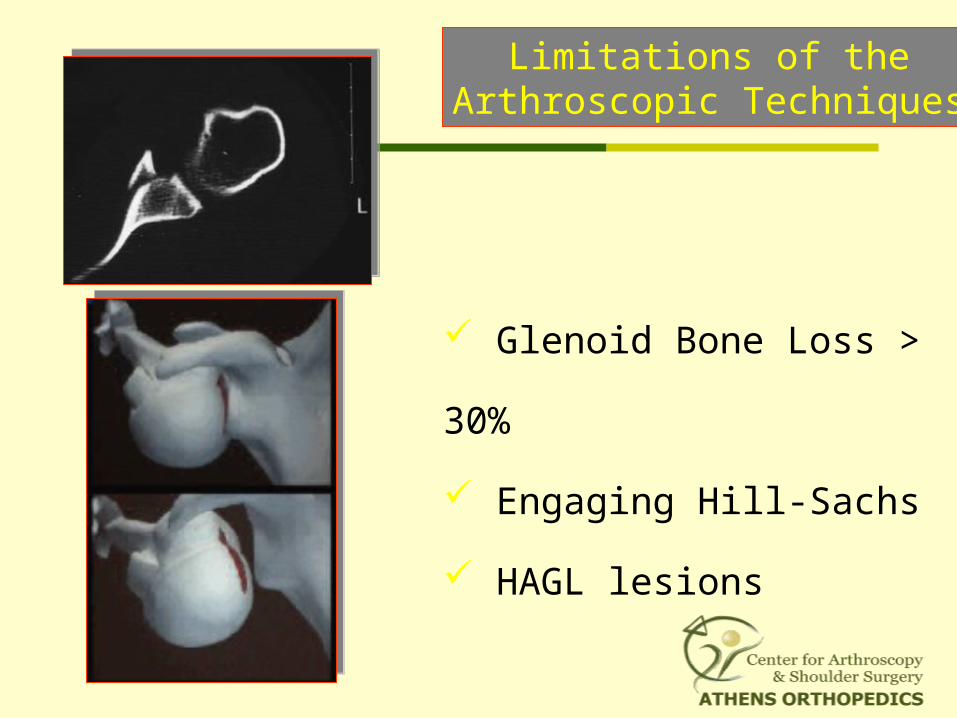
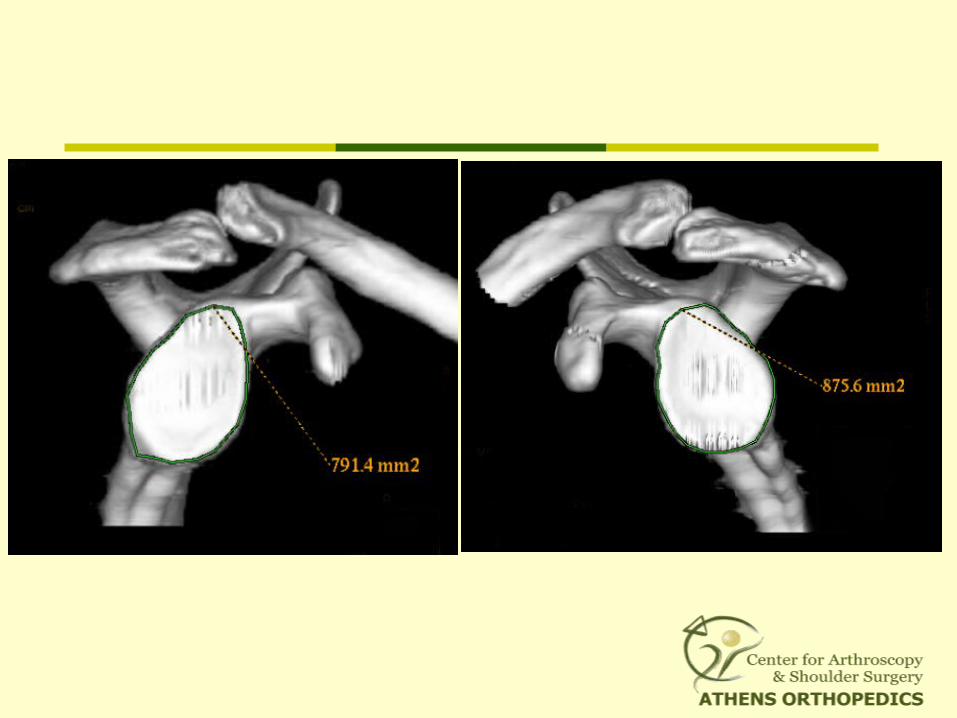
Glenoid Bone Loss > 30%
Engaging Hill-Sachs
HAGL lesions
Limitations of theArthroscopic Techniques
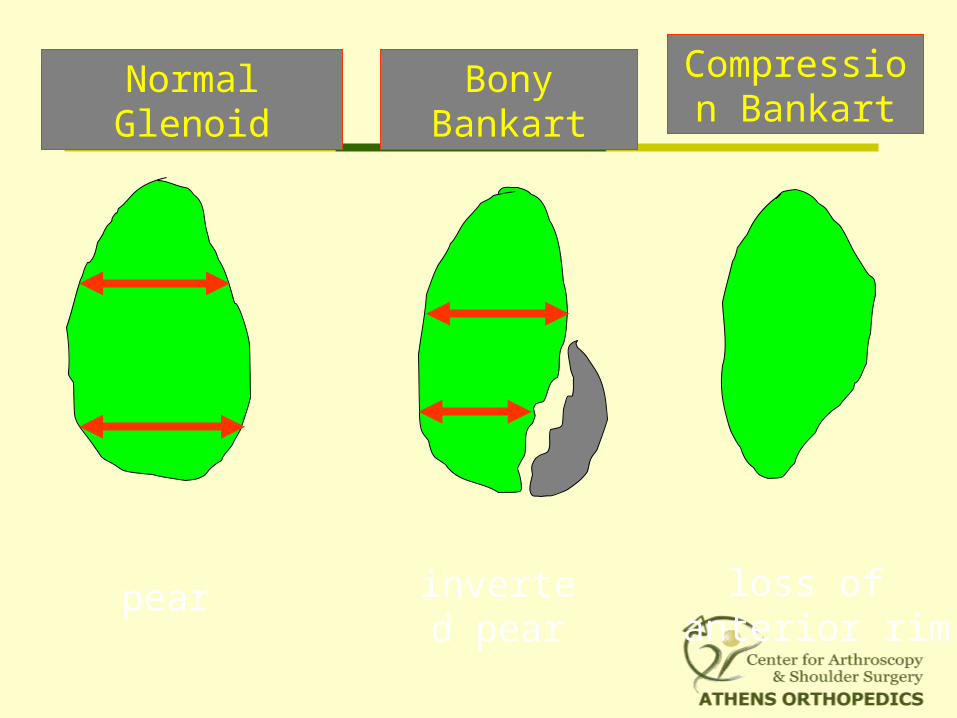
Normal Glenoid
inverted pear
Bony Bankart
pear
Compression Bankart
loss of anterior rim
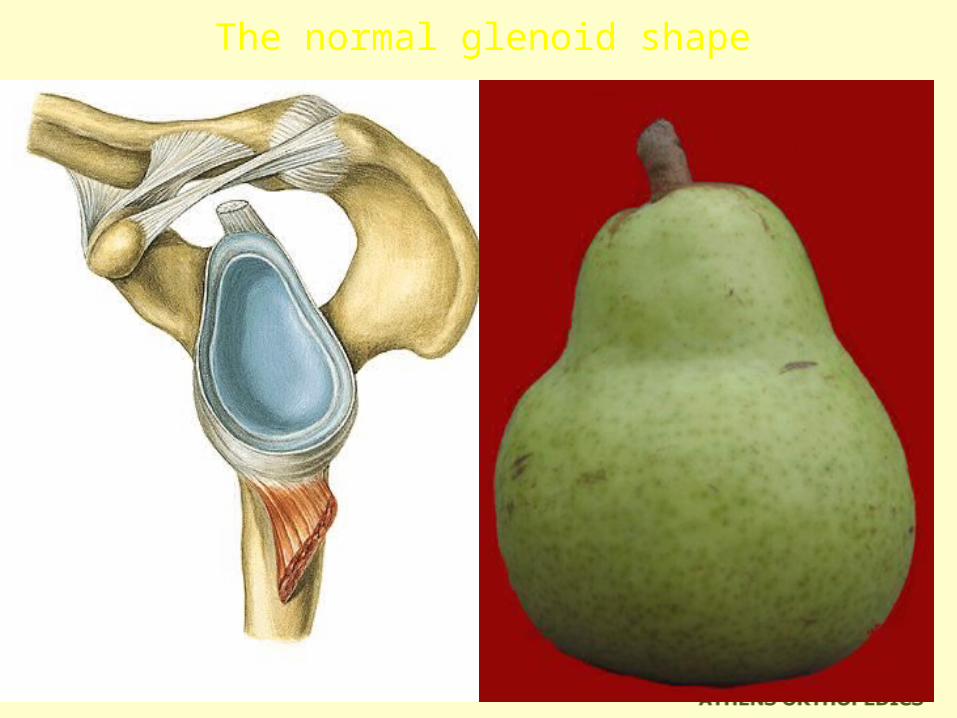
The normal glenoid shape

Inverted pear glenoid
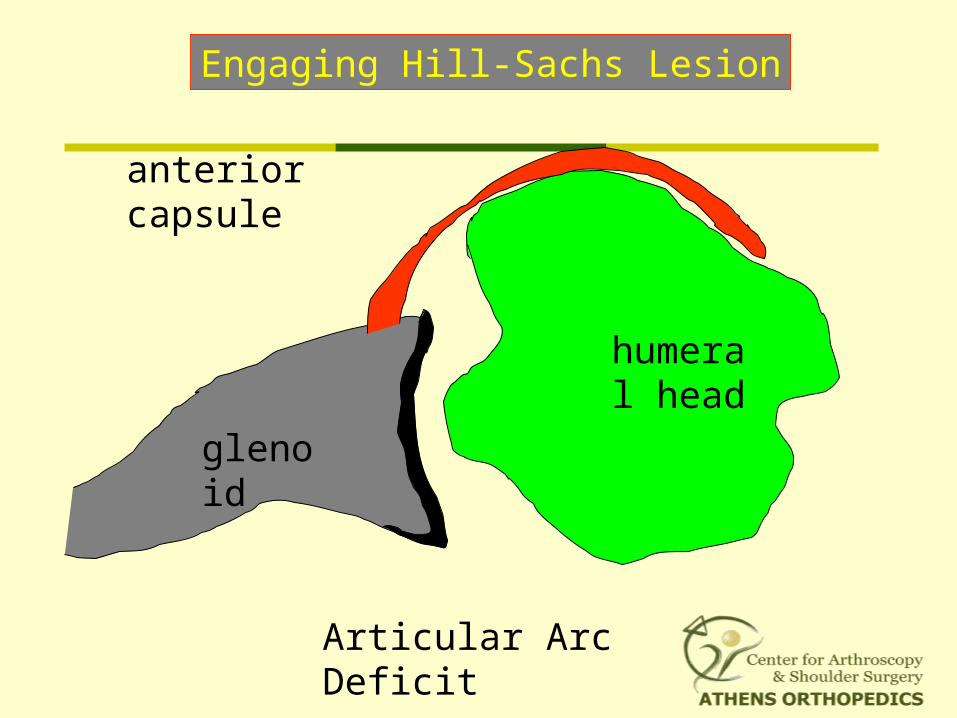
Engaging Hill-Sachs Lesion
Articular Arc Deficit
glenoid
humeral head
anterior capsule
Arthroscopic vs Open Shoulder Reconstruction
Less trauma
Better cosmesis
Addresses associated pathology
Less postoperative pain
On an outpatient basis
Faster surgery
Better ROM
Return to sports
Similar recurrence rate
Patient Demand
Insurance Policy (Less cost)
Equipment dependent
Open Shoulder Reconstruction
familiar to most orthopaedic surgeons
requires little special equipment
reasonably reproducible recurrence rate
addresses large glenoid bone defects
Neither technique is "easy"
The operation should be tailored to the patient and not the patient to the operation.
Both techniques are equivalent in terms of “success”
Arthroscopic Techniques are suitable
for almost every instability problem
Arthroscopic stabilization is the technique of choice
when confronted with the patient exhibiting
unilateral anterior shoulder instability
Keys to Success
• Mobilization of capsule
• South to north transfer
• Anchors on the glenoid
• At least 3 double suture loaded anchors
• Address secondary lesions
• Address capsular laxity
• Individualized and supervised rehabilitation
Conclusions
• Arthroscopic instability repair gained wider acceptance
• Results are equivalent to open repairs
• It is technically demanding but feasible
• With experience most of the instability problems can be treated arthroscopic