Embed Size (px)
Citation preview

Appendix A
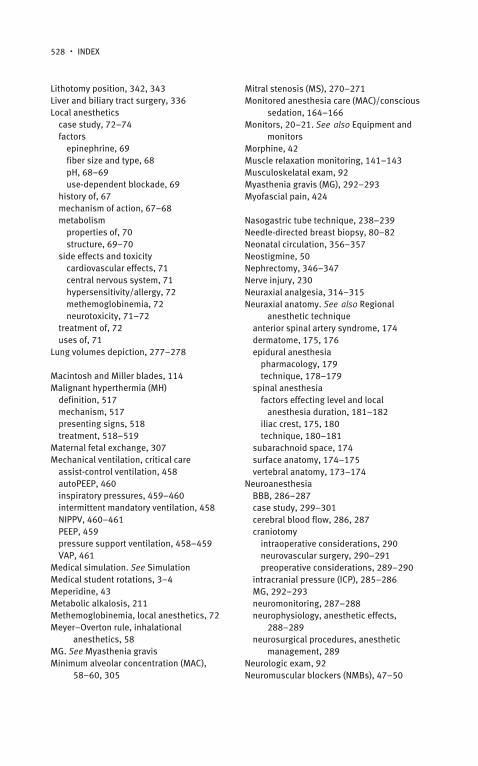
ASA Difficult Airway Algorithm
Excerpted from “Standards for Basic Anesthetic Monitoring” (Approved by House of Delegates on October 21, 1986, and last amended on October 25, 2005), of the American Society of Anesthesiologists. A copy of the full text can be obtained from ASA, 520 N. Northwest Highway, Park Ridge, IL 60068-2573, USA.
RECOGNIZED
DIFFICULT AIRWAY
UNRECOGNIZED
PROPERPREPARATION
INDUCE GENERAL ANAESTHESIA
FAIL TO INTUBATE
CALL FOR HELP
MASK VENTILATIONADEQUATE ? NO
LMA ORTRANSTRACHEALJET VENTILATION
FAIL
EMERGENCYCRICO-
THYROIDOTOMY
SUCCEED
INTUBATIONCHOICES
AWAKEN
WHEN
APPROPRIATEEXTUBATION
(OVER JET STYLET)
YES
INTUBATION CHOICES
FAIL SUCCEED
FAIL AFTERMULTIPLE ATTEMPTS
AWAKENMASK OR
TRACHEOSTOMYTO FINISH CASE CONFIRM
VENTILATION WITHET CO2, SaO2 and
OTHER TESTS
Uncooperative
Patient
PROPERPREPARATION
AWAKEINTUBATION
CHOICES
FAIL SUCCEED
TRACHEOSTMYOR
CRICO-THYROIDOTOMY
515
Appendix B
Malignant Hyperthermia
Richard D. Urman
DefinitionMalignant Hyperthermia (MH) is an inherited disorder of skeletal muscle, which is characterized by a hypermetabolic state and can be triggered by potent volatile anesthetics (but not nitrous oxide) and depolarizing muscle relaxants such as succinylcholine. Patients with some congenital myopathies may also be at increased risk when exposed to triggering anesthetic agents. However, all intravenous hypnotic agents are considered safe. MH is a potentially fatal disorder if it is not promptly recognized and treated, and the overall incidence during general anesthesia is about 1:50,000–1:100,000. For any patient presenting for anesthesia, a preoperative history should include questions about prior MH episodes or family history suggestive of MH.
MechanismIn a vast majority of cases, MH-susceptible patients have a defective calcium channel (known as ryanodine receptor) that is located on the sarcoplasmic reticulum membrane. In normal cells, calcium is released into the cell during muscle contraction. In MH, there is a problem with calcium reuptake, and therefore there is a massive increase in intracellular calcium leading to sustained muscle contractions. Consequently, there is an increased demand for oxygen and ATP in the muscle cells, leading to glycolysis and lactic acidosis. If left untreated, this uncontrolled hypermetabolism results in cell hypoxia, rhabdomyolysis, organ failure, and death.
517

518 ● ANESTHESIA STUDENT SURVIVAL GUIDE
Presenting Signs and DiagnosisThe most common presenting features of MH include significant, unexplained elevation in expired CO2, tachycardia, steady temperature rise, muscle rigidity, rhabdomyolysis, acidosis, and hyperkalemia. MH may occur at any time during anesthesia and in the postoperative period. The earliest signs are usually tachycardia and an increase in expired CO2; a rise in temperature may follow. Diagnosis of MH can be made on the basis of these signs, although the variability in the order and time of the onset of signs often makes clinical diagnosis difficult. These signs may present during or after the administration of the anesthetic. Table B.1 outlines possible presenting signs of MH.
Diagnosis is made based on the presenting signs, and other potential condi-tions that might cause the same symptoms should be ruled out. Genetic testing is also available, which can be done on an outpatient basis at an MH Testing Center. If MH is suspected, treatment should be initiated as soon as possible.
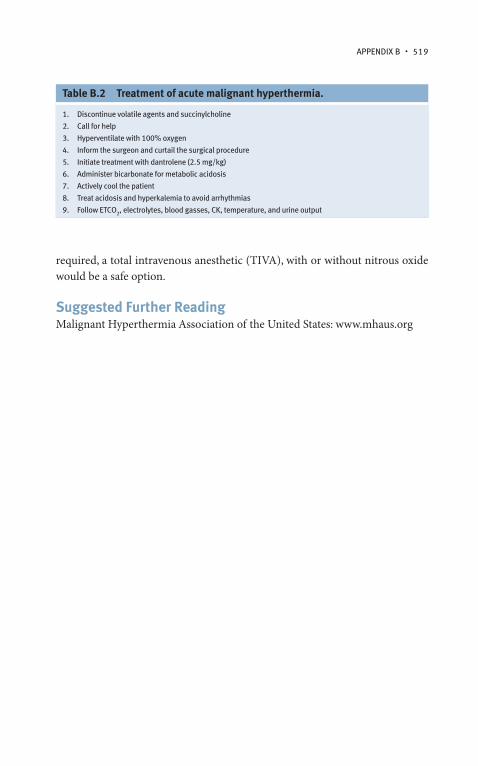
TreatmentAll triggering agents should be discontinued immediately, the surgical procedure should either be aborted or finished quickly, and patient cooling begun. Dant-rolene, a muscle relaxant which abolishes excitation–contraction coupling in muscle cells, is the main drug of choice. Important treatment modalities for MH are outlined in Table B.2.
Over the last several decades, thanks to provider education and increased knowledge about MH, perioperative patient mortality from MH has dropped from 80% to less than 5%. An MH-susceptible patient is still a candidate for any type of anesthetic, including general, regional, or local. If general anesthetic is
Table B.1 Main clinical features of malignant hyperthermia.
Rising ETCO2 and PaCO2
Tachycardia
Tachypnea
Muscle rigidity and masseter spasm
Hemodynamic instability
Cardiac arrhythmias
Increased body temperature
Metabolic acidosis
Hyperkalemia
Myoglobinuria
APPENDIx B ● 519
required, a total intravenous anesthetic (TIVA), with or without nitrous oxide would be a safe option.
Suggested Further ReadingMalignant Hyperthermia Association of the United States: www.mhaus.org
Table B.2 Treatment of acute malignant hyperthermia.
1. Discontinue volatile agents and succinylcholine
2. Call for help
3. Hyperventilate with 100% oxygen
4. Inform the surgeon and curtail the surgical procedure
5. Initiate treatment with dantrolene (2.5 mg/kg)
6. Administer bicarbonate for metabolic acidosis
7. Actively cool the patient
8. Treat acidosis and hyperkalemia to avoid arrhythmias
9. Follow ETCO2, electrolytes, blood gasses, CK, temperature, and urine output

Index
Abdominal compartment syndrome, 335Abdominal hernia, 116–118Abdominal hysterectomy, 10–14Abdominal surgeries
anesthesia considerationsintraoperative, 332–333postoperative, 333–334preoperative evaluation, 331–332
bowel surgery, 335esophageal surgery, 335hemorrhoid surgery, 335–336hernia surgery, 337liver and biliary tract surgery, 336pancreatic surgery, 337spleen surgery, 336stomach surgery, 335
Acetylcholinesterase inhibitors, 50Acid base analysis
anion gap (AG), 210arterial blood gas panel, 210blood gas analysis, 210–212disorders, 212primary acid–base disorders, 212
Activated factor VII (FVIIa), 215Acute lung injury (ALI), 457Acute respiratory distress syndrome
(ARDS), 457Acute respiratory failure (ARF)
ALI and ARDS, 457hypercapnic respiratory failure, 455–456hypoxemic respiratory failure, 455management, 457
Adjunct agentsantiemetics, 76–78antihypertensives, 78–79case study, 80–82dexmedetomidine, 79NSAIDS, 79sympathomimetics, 75–76
Adjunctive drugs, 13AICDs. See Automatic implantable
cardioverter-defibrillatorsAirway evaluation and management
anatomyglottis and epiglottis, 108upper airway anatomy, 107
case study, 116–118difficult airway algorithm, 115direct laryngoscopy and tracheal
intubationMacintosh and Miller blades, 114oral, pharyngeal, and laryngeal axes
relationship, 113fiber-optic intubation, 115laryngeal mask airway (LMA), 111–112Mallampati classification system, 109optimal face mask ventilation, 109–110physical examination features, 107–108RSI
pulmonary aspiration, risk factors, 113–114
vs. standard induction, 114–115video assisted endotracheal intubation, 115
Alfentanil, 42Allowable blood loss (ABL) formula, 213Alpha-2-agonist/tizanidine, 421Ambulatory surgery
case study, 392–394intraoperative management
midazolam, 385multimodal analgesia, 385PONV, 386S.A.F.E. principles, 385
postoperative management, 386–387preoperative considerations
common procedure, 383outpatient management, 384patient selection factors, 382
521

522 ● INDEx
procedure-related considerations, 383testing, 384
American Society of Anesthesiologists (ASA), 165, 473, 483–485
airway algorithm, 515closed claims study, 484–485monitoring standards, 134physical status and classifications, 96,
99–100Amides, 69Anesthesia
consent form, 96, 99equipment and monitors (see Equipment
and monitors)history
airway management, 21–22autonomy, 22–23case study, 24–26chloroform, 18–20CPR, 22ether, 16–18life outside anesthesia, 24monitors, 20–21prestige, 23–24slumber of anesthesiologists, 23
induction, 11–12machine
alarms, 126breathing systems, 127–129case study, 129–131checkout, 127cylinders, 121, 123fail-safe system, 123flowmeters, 124, 125gas outlet, 125–126high and low pressure systems, 120humidifiers, 129modern day, 121oxygen flush valve, 127pipeline inlets, 120, 122pressure regulation, 123two-gas machine, flow arrangement,
122vaporizers, 124–126waste-gas scavengers, 127
maintenance, 12–13Anesthesiology
case study, 478–481match, 5–6
professionalismdefinition, 472etiquette based medicine, 474–475key elements, 474responsibility, 473
safety and teamworkclosed loop communication, 475communication failure, 476
team trainingadvantages, 477CRM-based teamwork, 476–477
Anesthetic managementcardiopulmonary bypass (CPB)
circuit, 274–275considerations, 273–274induction and maintenance, 273intraoperative myocardial ischemia
management, 274minimally invasive cardiac
procedures, 276monitoring, 273post operative care, 276preoperative evaluation, 272–273wean, 275–276
elderly patients, 374–375neurosurgical procedures, 289preoperative examination, 374–375urological surgery
cystoscopy/ureteroscopy/TURBT, 344ESWL, 348laser surgery, urology, 345nephrectomy, 346–347orchiectomy, 347–348radical cystectomy, 346renal transplantation, 347TURP, 344–345
Anesthetic techniquesaction sequence of, 164case study, 170–172components of, 167drugs, 161induction and emergence, 161–162IV portion of, 161machine check, 160maintenance phase of, 162monitored anesthesia care (MAC)/
conscious sedation, 164–166M.S.M.A.I.D.S. mnemonic, 159–160operating room to PACU, 163
INDEx ● 523
physiology ofsedative-hypnotic medications, 167total intravenous anesthesia
(TIVA), 169volatile anesthetics, 167–169
selection of, 166special equipment, 161stages of, 163suction, 160wake up and extubation, 162–163
Anion gap-acidosis, 211Anticholinergics, 36, 51Anticholinesterase, 36Anticonvulsants, 421Antiemetics, 36, 76–78Antihypertensives, 78–79Aortic regurgitation (AR), 271Aortic stenosis (AS), 271Aortocaval compression, 304Apgar score, 310–311Arrythmia management, 271–272Arterial line placement
anatomy, 232physiology, 233radial artery cannulation, 232technique, 233
Arterial puncture potential complications, 230
ASA. See American Society of Anesthesiologists
Assist-control ventilation, 458Atrioventicular (AV) node, 266Atropine, 51Automatic implantable cardioverter-
defibrillators (AICDs), 272
Barbiturate, 36Bariatric surgery. See also Abdominal
surgeries; Obesityabdominal surgeries
bowel surgery, 335esophageal surgery, 335hemorrhoid surgery, 335–336hernia surgery, 337intraoperative considerations, 332–333liver and biliary tract surgery, 336pancreatic surgery, 337postoperative considerations, 333–334preoperative evaluation, 331–332
spleen surgery, 336stomach surgery, 335
case study, 337–339obesity
airway challenges, 329anesthetic considerations, 330–331BMI, 325–326cardiovascular system, 326–327endocrine and metabolic system, 328gastrointestinal system, 327–328neurological and psychological
problems, 328–329respiratory system, 327surgery for, 329types of, 325
Baseline vital signs, physical exam, 92BBB. See Blood brain barrierBenzodiazepines, 36, 40–41Bier block. See Intravenous regional
anesthesiaBispectral Index (BIS) monitoring system, 143Bleeding disorders, 91Blood brain barrier (BBB), 286Blood pressure monitoring
arterial line waveform, cardiac cycle, 137equipment, 136oscillometry, 135
Blood products transfusionABL formula, 213coagulation panels, 214EBV formula, 213–214HCT, 213–214practical aspects, 215
Blood volume and fluid compartments, 201–202
Body mass index (BMI), 325–326Body temperature, 151Bowel surgery, 335Breathing systems, 127–129
Cancer pain, 422Capnography and ventilation monitoring,
139–141Cardiac anesthesia
b-adrenergic stimulation, 268cardiac cycle
definitions and equations, 269systole and diastole, 268ventricular isovolumetric relaxation, 269

524 ● INDEx
case study, 281–283coronary arteries, 265–266disease states affecting heart
arrythmia management, 271–272
heart failure, 272ischemic heart disease, 269–270valvular disease, 270–271
heart anatomy, 266–267Cardioplegia solution, 274Cardiopulmonary bypass (CPB). See
Anesthetic managementCardiopulmonary exam, 92Cardiopulmonary resuscitation
(CPR), 22Cardiovascular system
elderly patients, 370–371local anesthetics, 71obesity, 326–327preoperative patient evaluation,
87–89, 100Career options, 4–5Cauda equina syndrome (CES), 183Celebrex. See CelecoxibCelecoxib, 79Central anticholinergic syndrome, 51Central nervous system, local anesthetics,
71Central venous catheters, 145Central venous line (CVL)
anatomy, 233cannulation via anterior approach,
234–236femoral vein, anatomy, 236insertion site, 237internal jugular vein, 233–234subclavian vein, 234
Central venous pressure (CVP), 214–215, 449–451
Cerebral blood flow, 286, 287Cerebral physiology, anesthetic agents,
287–288Cesarean section anesthesia
epidural anesthesia, 316–317general anesthesia, 317–318qualities of, 315spinal anesthesia, 316
Chloroform, 18–20Cholinergic crisis, 50
Chronic pain management. See Perioperative acute and chronic pain management
Clinical simulation. See SimulationComplex regional pain syndrome, 423–424Continuous lumbar epidural analgesia,
312–313Continuous spinal analgesia, 313Corneal abrasions, 259Coronary artery supply, 265–266Coronary perfusion maintain, 252CPR. See Cardiopulmonary resuscitationCraniotomy
intraoperative considerations, 290neurovascular surgery, 290–291preoperative considerations, 289–290
Crew resource management (CRM), 476–477Crisis resource management, 506Critical care
acute respiratory failure (ARF)ALI and ARDS, 457hypercapnic respiratory failure,
455–456hypoxemic respiratory failure, 455management, 457
case study, 465–467hemodynamic monitoring
cardiac output, 447–449central venous pressure, 449–451goals, 446invasive arterial blood pressure,
446–447pulmonary artery catheter, 451
initial assessment, 443mechanical ventilation
assist-control ventilation, 458autoPEEP, 460inspiratory pressures, 459–460intermittent mandatory ventilation, 458NIPPV, 460–461PEEP, 459pressure support ventilation, 458–459VAP, 461
oxygen balance and tissue perfusion, 445–446
oxygen transport, 444–445shock
classification, 451–452hemodynamic disturbances, 452management, 452–453
INDEx ● 525
septic shock, 453–454vasoactive agents, 453
supportive care, ICUethical decisions and end-of-life, 464glucose management, 462nosocomial infections, preventive
measures, 462nutrition, 464sedation management, 462stress ulcer prophylaxis, 463thromboprophylaxis, 462–463
Cryoprecipitate, 215C-Trach, 115Cushing’s response, 286CVL. See Central venous lineCVP and PA catheters, volume assessment,
214–215
Deceleration patterns principal, 308–310Delirium, 373Depolarizing neuromuscular blocking agent,
36Desflurane, 63Dexamethasone, 77Dexmedetomidine, 79Diabetes mellitus, 91, 101–102Diameter-index safety system (DISS), 120,
122Dilutional anemia, 305Discogenic pain, 423Dopamine, 76Double lumen tubes (DLT), 279–281Droperidol, 78Dysfunctional pain, 417Dysrhythmias, 255–257
nonhemolytic febrile transfusion reactions, 254
severe transfusion reaction management, 258
E-cylinders, 123Edrophonium, 50Elderly patients
age and organ function relationship, 370anesthetic management, 374–375care of, 369case study, 377–379intraoperative management
general vs. regional anesthesia, 376
induction agents, 376monitoring, 375premedications, 375thermoregulation, 376
physiological changescardiovascular system, 370–371nervous system, 373pharmacokinetic and pharmacodynamic
changes, 374postoperative cognitive dysfunction and
delirium, 373–374pulmonary changes, 371–372renal changes, 372
postoperative period, 376–377Electrocardiographic monitoring, 136–137Electrolyte and non-electrolyte solute
composition, 201Electrolytes and fluid compartments
abnormal fluid shifts, intracellular to extracellular, 199
of body and composition, 199–200Endocardium, 265Endocrine, preoperative patient evaluation,
91Endoscopic sinus surgery, 296Ephedrine, 75Epidural catheter placement level, 334Epiglottis, 108Epinephrine, 69Equipment and monitors
ASA monitoring standards, 134blood pressure monitoring, 134–137capnography and ventilation monitoring,
139–141case study, 151–154central venous pressure, 145depth of anesthesia, 143–144electrocardiographic monitoring, 136–138muscle relaxation, 141–143pulmonary artery pressure, 146–147, 150pulse oximetry, 137–139standards for
body temperature, 151circulation, 150–151oxygenation, 149ventilation, 149–150
temperature, 144visual and auditory surveillance, 133–134
Esophageal surgery, 335

526 ● INDEx
Esters, 69Estimated blood volume (EBV) formula,
213–214Ether, 16–18Ethical and legal issues
advanced directives, 498–499case study, 499–501do not resuscitate (DNR)/do not intubate
(DNI), 499informed consent, 497–498malpractice, 498
Etiquette based medicine, 474–475Etomidate, 46Extensive rectal hemorrhoids, 281–283Extracellular–intravascular space, 201–202Extracorporeal shock wave lithotripsy
(ESWL), 348
Face mask ventilation, airway evaluation, 109–110
Facet arthropathy, 423Factor Ix concentrate, 215Fentanyl, 42FFP. See Fresh-frozen plasmaFiber size and type, local anesthetics, 68Fibreoptic intubation (FOI), 330Fluid management, patient evaluation
euvolemic, 204hypervolemic and hypervolemic, 204intravascular, clinical indicators of,
202–203Fluid replacement options
advantages, disadvantages, 208–209case study, 224–226colloids, 204, 206–207crystalloids, 204, 207
Fluid requirements calculation, 204–206Flumazenil, 41Frank–Starling curve, 446, 448Fresh-frozen plasma (FFP), 215
Gamma-aminobutyric acid (GABA) enhancement, 58
Gastric tube placement techniques. See also Arterial line placement; Central venous line (CVL)
nasogastric tube technique, 238–239orogastric tube technique, 238
Gastrointestinal exam, 92
Glidescope, 115Glottis and epiglottis, 108Glycopyrrolate, 36, 51
Heart anatomy, 266–267HELLP syndrome, 306Hematocrit (HCT), 213–214Hemodynamic monitoring, critical care
cardiac output, 447–449central venous pressure monitoring,
449–451goals, 446invasive arterial blood pressure
monitoring, 446–447pulmonary artery catheter, 451
Hemoglobin–oxygen dissociation curve, 247Hemorrhoid surgery, 335–336Hepatic and gastrointestinal disease, 90–91Hernia surgery, 337High-fidelity simulation, 505–506Humidifiers, 129Hydromorphone, 42Hypercarbia, 251Hyperchloremic acidosis, 211Hypersensitivity/allergy, local anesthetics,
72Hypocarbia, 251Hypoventilation, 431Hypoxemia, 431
corrective actions, 248hemoglobin–oxygen dissociation curve,
247
ICP. See Intracranial pressureInduction agents, 44–47Inflammatory pain, 417Inhalational anesthetics, 36
case study, 63–66concentration effect, 61minimum alveolar concentration (MAC),
58–59nitrous oxide, 59–61second gas effect, 61–62theories of, 58uptake, distribution and elimination
pharmacokineticsemergence, 55–56fresh gas flow rate, 57induction, 55

INDEx ● 527
inspired concentration, 56–57minute ventilation, 57–58tissue and blood solubility, 56
volatile anesthetics, 62–63Inner ear surgery, 296Internal jugular (IJ) vein, 233–234Interventional pain procedures, 419Intracranial pressure (ICP), 299–301Intraoperative management. See also Elderly
patientsgeneral vs. regional anesthesia, 376induction agents, 376monitoring, 375premedications, 375thermoregulation, 376
Intraoperative problemsanaphylactic/anaphylactoid reactions, 252awareness, 252–253case study, 260–262delayed emergence, 252and differential diagnoses, 244–246dysrhythmias, 255–257
nonhemolytic febrile transfusion reactions, 254
severe transfusion reaction management, 258
foley (bladder) catheters, 257gastric acid aspiration, 254general concepts, 243–247hypercarbia, 251hypocarbia, 251hypotension, 248–249hypoxemia
corrective actions, 248hemoglobin-oxygen dissociation curve,
247myocardial ischemia, 251–252nasogastric (NG)/orogastric (OG) tube
related problems, 257, 259patient movement/waking up during
surgery, 253postoperative complications, 259regional anesthesia failed, 253venous air embolism, 253–254ventilation failure, 250
Intrapartum fetal evaluation, 308–310Intravenous anesthetic agents
acetylcholinesterase inhibitors, 50anticholinergics, 51
balanced anesthesia, 39–40benzodiazepines, 40–41induction agents
cardiovascular effects of, 47etomidate, 46–47ketamine, 47propofol, 45–46recommended dosages for, 45thiopental, 46
neuromuscular blockers (NMBs)depolarizing NMBs, 48–49nondepolarizing NMBs, 49–50
opioidsadverse side effects, 44context-sensitive half time, 43dose, peak effect and duration for, 42fentanyl, 42meperidine, 43morphine, 42receptor subtypes and effects, 41remifentanil, 43sufentanil and alfentanil, 42
Intravenous (IV) linesanatomy, 229–230case study, 239–241complications, 231infiltration, 259peripheral cannulation technique,
230–231veins physiology, 230
Intravenous regional anesthesia, 193Invasive arterial blood pressure, 446–447Ischemic cardiac disease, 269–270Isoflurane, 37–38, 63
Ketamine, 47Ketorolac, 79
Labor analgesia, 320–322Laparoscopic surgery, 332–333Laparotomy/open surgery, 332–333Laryngeal mask airway (LMA), 111–112Laryngoscopy and tracheal intubation
Macintosh and Miller blades, 114oral, pharyngeal, and laryngeal axes
relationship, 113Laryngospasm, 430–431Laser surgery, 345Left ventricular assist devices (LVAD), 272
528 ● INDEx
Lithotomy position, 342, 343Liver and biliary tract surgery, 336Local anesthetics
case study, 72–74factors
epinephrine, 69fiber size and type, 68pH, 68–69use-dependent blockade, 69
history of, 67mechanism of action, 67–68metabolism
properties of, 70structure, 69–70
side effects and toxicitycardiovascular effects, 71central nervous system, 71hypersensitivity/allergy, 72methemoglobinemia, 72neurotoxicity, 71–72
treatment of, 72uses of, 71
Lung volumes depiction, 277–278
Macintosh and Miller blades, 114Malignant hyperthermia (MH)
definition, 517mechanism, 517presenting signs, 518treatment, 518–519
Maternal fetal exchange, 307Mechanical ventilation, critical care
assist-control ventilation, 458autoPEEP, 460inspiratory pressures, 459–460intermittent mandatory ventilation, 458NIPPV, 460–461PEEP, 459pressure support ventilation, 458–459VAP, 461
Medical simulation. See SimulationMedical student rotations, 3–4Meperidine, 43Metabolic alkalosis, 211Methemoglobinemia, local anesthetics, 72Meyer–Overton rule, inhalational
anesthetics, 58MG. See Myasthenia gravisMinimum alveolar concentration (MAC),
58–60, 305
Mitral stenosis (MS), 270–271Monitored anesthesia care (MAC)/conscious
sedation, 164–166Monitors, 20–21. See also Equipment and
monitorsMorphine, 42Muscle relaxation monitoring, 141–143Musculoskelatal exam, 92Myasthenia gravis (MG), 292–293Myofascial pain, 424
Nasogastric tube technique, 238–239Needle-directed breast biopsy, 80–82Neonatal circulation, 356–357Neostigmine, 50Nephrectomy, 346–347Nerve injury, 230Neuraxial analgesia, 314–315Neuraxial anatomy. See also Regional
anesthetic techniqueanterior spinal artery syndrome, 174dermatome, 175, 176epidural anesthesia
pharmacology, 179technique, 178–179
spinal anesthesiafactors effecting level and local
anesthesia duration, 181–182iliac crest, 175, 180technique, 180–181
subarachnoid space, 174surface anatomy, 174–175vertebral anatomy, 173–174
NeuroanesthesiaBBB, 286–287case study, 299–301cerebral blood flow, 286, 287craniotomy
intraoperative considerations, 290neurovascular surgery, 290–291preoperative considerations, 289–290
intracranial pressure (ICP), 285–286MG, 292–293neuromonitoring, 287–288neurophysiology, anesthetic effects,
288–289neurosurgical procedures, anesthetic
management, 289Neurologic exam, 92Neuromuscular blockers (NMBs), 47–50

INDEx ● 529
Neuropathic pain, 417Neurotoxicity, local anesthetics, 71–72Nitrous oxide, 59–61Nociceptive pain, 417Nondepolarizing neuromuscular blocking
drug, 36Noninvasive positive-pressure ventilation
(NIPPV), 460–461Nonsteroidal anti-inflammatory drugs
(NSAIDS), 79Norepinephrine, 76
Obesityairway challenges, 329anesthetic considerations
intraoperative considerations, 330–331postoperative considerations, 331preoperative evaluation, 330
BMI, 325–326physiologic changes
cardiovascular system, 326–327endocrine and metabolic system, 328gastrointestinal system, 327–328neurological and psychological
problems, 328–329respiratory system, 327
surgery for, 329Obstetrics
case study, 320–322cesarean section anesthesia
epidural anesthesia, 316–317general anesthesia, 317–318qualities of, 315spinal anesthesia, 316
hemorrhagic emergenciesantepartum/intrapartum hemorrhage,
318–319post-partum hemorrhage, 319
intrapartum fetal evaluationdeceleration patterns principal,
308–309fetal heart rate (FHR), 308
maternal fetal exchange, 307neonatal evaluation, apgar score,
310–311non-obstetric surgery anesthesia,
319–320physiologic changes
cardiovascular, 303–304central nervous system, 305
gastrointestinal, 306hematologic changes, 305–306musculoskeletal, 306–307renal, 306respiratory, 304–305
uteroplacental blood flow, 307vaginal delivery anesthesia
combined spinal-epidural analgesia, 314epidural analgesia, 312–313neuraxial analgesia, 314–315non-pharmacologic options, labor
pain, 312pain pathways, 311regional anesthesia, 312, 313spinal analgesia, 313–314stages, 311systemic medications, labor pain, 312
Oculo-cardiac reflex, 298Omphalocele and gastroschisis, 366Oncotic vs. osmotic pressures, 201One-lung ventilation (OLV), 279Opioid pharmacodynamics and dose,
420–421Opioids, 36, 41–44Orchiectomy, 347–348Orogastric tube technique, 238Orthopedic surgery
blood loss, 407case study, 408–410choice of anesthetic, 404–405fat embolism syndrome, 407methylmethacrylate cement, 406–407positioning injuries, 406postoperative pain management,
405–406tourniquet issues, 406
Oscillometry, 134Otolaryngology (ENT), anesthetic approach
airway surgery, 297case study, 299–301endoscopic sinus surgery, 296inner ear surgery, 296intraoperative issues, 295neck dissection, 295–296ophthalmology
intraocular pressure (IOP), 297retrobulbar and peribulbar blocks,
297–298preoperative planning, 294–295specialized equipment, 293
530 ● INDEx
Out-of-OR (OOR) procedurescase study, 392–394electrophysiology lab (EP), 389–390gastrointestinal (GI) endoscopy, 388–389neuroradiology, 391–392radiology, 390–391unique aspects, 387
Oxygenation, 149Oxygen flush valve, 127Oxyhemoglobin dissociation curve, 307
PA. See Pulmonary arteryPain assessment, 422Pain pathways, gross anatomy of, 414–415Pancreatic surgery, 337Paralytics. See Neuromuscular blockers
(NMBs)Patient and provider safety
ASA closed claims study, 484–485basic anesthetic monitoring, 485–486case study, 491–494challenges, anesthesia provider, 487CMS, 491high quality anesthesia care, 487–488history, 483pay-for-performance concept, 490perioperative complications
dental trauma, 488eye injury, 488–489intraoperative recall, 489–490peripheral nerve injuries, 489
quality assurance (QA), 484Patient preparation, 10–11Pay-for-performance concept, 490Pediatric surgery
anatomytrachea, 355upper airway, 353, 354
case study, 366–368OR equipment and setup
intravenous fluid, 362–363radiant heat loss, 361–362
pharmacology, 359physiology
blood, 359cardiac, 358gastrointestinal, 358–359hepatic, 358neonatal circulation, 356–357
neurologic, 359renal, 358respiratory, 358temperature regulation, 359
preoperative evaluationphysiological assessment, 360–361psychological assessment, 360
techniquesHCT and EBV, 365maintenance, 363–364omphalocele and gastroschisis, 366oximetry, 364pyloric stenosis, 365
venous access, 355–356Pelviscopy, 51–53Perioperative acute and chronic pain
managementacute vs. chronic pain
somatic pain, 416types of, 417visceral pain, 417
case study, 425–427pain sensation
modulation, 414pain pathways, gross anatomy, 414–415perception, 416transduction, 413–414transmission, 414
palliative care, 425physical and psychological therapy, 425syndromes, 422–424
complex regional pain syndrome, 423–424
discogenic pain, 423facet arthropathy, 423myofascial pain, 424postherpetic neuralgia, 424radicular pain, 423sacroiliac joint dysfunction, 424spinal stenosis, 422
treatment ofacute pain, 418chronic pain, 419–421
types and definitions, 416Perioperative complications
dental trauma, 488eye injury, 488–489intraoperative recall, 489–490peripheral nerve injuries, 489

INDEx ● 531
Peripheral nerve blocks (PNB)cervical plexus blockade, 186–187target nerve identification, 185–186
Peripheral nerves classification, 414Pharmacodynamics
competitive vs. noncompetitive antagonism, 35
drug dose response relationship, 34receptor systems, 34tolerance and physiological dependence,
35Pharmacokinetics
absorption, 30distribution
free fraction and protein binding, 30redistribution, 31storage, 31volume of distribution (Vd), 31
metabolism and excretionclearance, 32context-sensitive half-time, 33mechanisms of, 31zero vs. first order kinetics, 32, 33
Pharmacologyinhalational anesthetics
case study, 63–66concentration effect, 61minimum alveolar concentration (MAC),
58–60nitrous oxide, 59–61second gas effect, 61–62theories of, 58uptake, distribution and elimination,
55–58volatile anesthetics, 62–63
intravenous anesthetic agentsacetylcholinesterase inhibitors, 50anticholinergics, 51benzodiazepines, 40–41induction agents, 44–47neuromuscular blockers (NMBs), 47–50opioids, 41–44
local anestheticscase study, 72–74factors, 68–69history of, 67mechanism of action, 67–68metabolism, 69–70side effects and toxicity, 71–72
treatment of, 72uses of, 71
principlescase study, 35–38pharmacodynamics, 34–35pharmacokinetics, 30–33
Phenergan. See PromethazinePhenylephrine, 76pH, local anesthetics, 68–69Pin index safety system (PISS), 125Platelets, 215PNB. See Peripheral nerve blocksPneumoperitoneum, 332Positive end-expiratory pressure (PEEP), 459Postanesthesia care unit (PACU), 9–10, 14Post-dural puncture headache (PDPH),
183–184Postherpetic neuralgia, 424Postoperative care unit
case study, 440–442discharge criteria, 438–439hemodynamic complications, 431–434hypothermia and shivering, 438neurologic complications, 434–436pain control, 437–438postoperative nausea and vomiting
(PONV), 436–437respiratory complications, 429–431sample PACU sign-out, 429, 430
Postoperative nausea and vomiting (PONV), 386, 393, 436–437
Pregnancy, normal physiologic changescardiovascular, 303–304central nervous system, 305gastrointestinal, 306hematologic changes, 305–306musculoskeletal, 306–307renal, 306respiratory, 304–305
Preoperative patient evaluationanesthesia consent form, 96, 99case study
ASA physical status, 99–100cardiovascular complications, 100diabetes, 101–102pulmonary complications, 100–101
goals of, 85history
airway, 86–87

532 ● INDEx
bleeding disorders, 91cardiovascular, 87–89endocrine, 91hepatic and gastrointestinal disease,
90–91musculoskeletal, 92neurologic, 92pulmonary, 89–90renal, 91–92
indications for, 94–95interview, 85–86laboratory data, 93–95medical records/family history, 93medications/allergies, 92–93physical exam, 92plan
ASA physical status classifications, 96formulation, patient history,
97–98Pressure support ventilation, 458–459Primary acid–base disorders, 212Professionalism. See also Anesthesiology
definition, 472etiquette based medicine, 474–475key elements, 474responsibility, 473
Promethazine, 77Propofol, 45–46Pulmonary artery (PA), 214–215, 451Pulmonary artery catheters
data, 146–147hemodynamic parameters, 150
Pulmonary aspiration, 305Pulmonary complications, preoperative
patient evaluation, 100–101Pulse oximetry, 137–139Purkinje fibers, 266
Quality assurance (QA), 484. See also Patient and provider safety
Radial artery cannulation, 232Radical cystectomy, 346Radicular pain, 423Rapid sequence induction (RSI)
pulmonary aspiration, risk factors, 113–114
vs. standard induction, 114–115Red blood cells (RBCs), 215
Regional anesthetic techniquebrachial plexus and upper extremity
blocks, 192axillary block, 190–191infraclavicular block, 189–191interscalene block, 187–190supraclavicular block, 189
case study, 195–197caudal anesthesia, 182combined spinal–epidural, 182complications and side effects
cardiovascular changes, 183CES, 183epidural abscess, 185high/total spinal anesthesia, 184intravascular injection, 184post-dural puncture headache (PDPH),
183–184spinal/epidural hematoma, 184–185transient neurologic symptoms, 183urinary retention, 184
epidural anesthesiapharmacology, 179technique, 178–179
indications and contraindications, 175, 177
intravenous regional anesthesia (Bier block), 193
lower extremity peripheral nerve block, 194
ankle block, 193femoral nerve block, 191–192sciatic nerve block, 192–193
mechanism of action, 176–177neuraxial anatomy
anterior spinal artery syndrome, 174dermatome, 175, 176subarachnoid space, 174surface anatomy, 174–175vertebral anatomy, 173–174
PNBcervical plexus blockade, 186–187target nerve identification, 185–186
potential risks, 175, 177spinal anesthesia
factors effecting level and local anesthesia duration, 181–182
iliac crest, 175, 180technique, 180–181
INDEx ● 533
surface anatomy, 174–175ultrasonography, 194–195vertebral anatomy, 173–174
Remifentanil, 43Renal transplantation, 347Respiratory alkalosis, 304Retrobulbar and peribulbar blocks approach,
297–298Rheumatic heart disease, 281–283Roux-en-Y gastric bypass, 337–339RSI. See Rapid sequence inductionRyanodine receptor, 517
Sacroiliac joint dysfunction, 424Safety and team training. See also
Anesthesiologyadvantages, 477closed loop communication, 475communication failure, 476CRM-based teamwork, 476–477
Scopolamine, 78Sedative-hypnotic medications, 167Sensation of pain
modulation, 414pain pathways, gross anatomy, 414–415perception, 416transduction, 413–414transmission, 414
Serotonin antagonists, 36, 77Serotonin-norepinephrine reuptake
inhibitors (SNRI), 421Sevoflurane, 63Shock
classification, 451–452hemodynamic disturbances, 452management, 452–453septic shock, 453–454vasoactive agents, 453
Short-acting, fast-emergence anesthetic (S.A.F.E.) principles, 385
Simulationcase study, 511–514categories, 504, 505crisis resource management, 506definition, 503evidence, 505expectations, 510–511formal assessment, 509–510high-fidelity simulation, 505–506
history, 504–505laboratory
benefits, 508–509mannequin, 507physical layout, 506–507
mannequin, 509Sinoatrial (SA) node, 266SNRI. See Serotonin-norepinephrine
reuptake inhibitorsSpinal–Epidural anesthesia, combined
advantages, 182complications and side effects
cardiovascular changes, 183CES, 183epidural abscess, 185high/total spinal anesthesia, 184intravascular injection, 184post-dural puncture headache (PDPH),
183–184spinal/epidural hematoma, 184–185transient neurologic symptoms, 183urinary retention, 184
Spinal stenosis, 422Spleen surgery, 336Stomach surgery, 335Succinylcholine, 48–49Sufentanil, 42Swan-Ganz catheter, 146Sympathomimetics, 75–76Systole and diastole, cardiac cycle, 268
Team training. See AnesthesiologyTemperature monitoring, 144Thiopental, 46Thoracic anesthesia
anatomy, 276–277anesthetic management, 278–279case study, 281–283double lumen endotracheal tube,
279–281invasive cardiac procedures, 281one-lung ventilation, 279preoperative evaluation, 276–278
Thromboprophylaxis, 462–463Toradol. See KetorolacTotal intravenous anesthesia (TIVA),
169, 295Total knee replacement (TKR), 195–197Tracheae and bronchi, 276–277

534 ● INDEx
Transfusionhazards
bloodproducts, 220–221blood type compatibility matrix, 216,
222hyperkalemia, 223hypocalcemia, 223infectious risks, 216–217transfusion reactions, 216, 218–219transfusion-related acute lung injury
(TRALI ), 222legal and ethical issues
economic issues, 224professional issues, 220–224religious/philosophical issues, 223
Transuretheral resection of prostate/bladder tumor (TURP/TURBT), 344–345
Trauma injuryadvanced trauma life support (ATLS), 398bleeding
coagulopathy, 403hypothermia, 402hypovolemia and acidosis, 402–403massive transfusion protocol, 404
case study, 408–410clearing C-Spine, 401–402epidemiology, 397–398Glasgow coma scale (GCS), 398, 399head trauma, 402mechanisms of, 398trauma airway, 400–401trauma arrest, 400
Tricyclic antidepressants, 421Twitch monitoring, 142Typical general anesthesia case
emergence, 9induction and intubation, 8maintenance, 8–9monitoring, 7
PACU management, 9–10phases of, 7preoperative evaluation, 6–7sedation, 7
Upper airway anatomy, 107, 353, 354Urological surgery
anatomy, 341–342anesthetic management
cystoscopy/ureteroscopy/TURBT, 344ESWL, 348laser surgery, urology, 345nephrectomy, 346–347orchiectomy, 347–348radical cystectomy, 346renal transplantation, 347TURP, 344–345
case study, 350–352complications of
autonomic hyperreflexia, 348bacteremia, 350bladder perforation, 348hypothermia, 350irrigating solutions, 349TURP syndrome, 349
lithotomy position, 342, 343preoperative assessment, 343–344
Uterine atony and retained placenta, 319Uteroplacental blood flow, 307
Vaginal delivery anesthesia. See ObstetricsVaporizers, 124–126Vasopressors. See SympathomimeticsVentilation, 149–150Ventilator-associated pneumonia (VAP), 461Volatile anesthetics, 62–63, 167–169
Waste-gas scavengers, 127Weight loss procedures, 329