Embed Size (px)
Citation preview
ASEAN Training Manual on Risk Communication
i
ASEAN Training Manual on Risk Communication
ASEAN Secretariat and
Malaysian Technical Working Group

ii
Advisors, Technical Working Groups & Contributors
iii
Advisors for the Risk Communication Training Manual
· Y.Bhg. Dato’ Sri Dr. Hasan Abdul Rahman Director General of Health, Malaysia Ministry of Health Malaysia
· Dr. Lokman Hakim Sulaiman
Deputy Director General (Public Health) Ministry of Health Malaysia
· Dr. Chong Chee Kheong
Director of Disease Control Ministry of Health Malaysia
· Ms Siti Sa’adiah Hassan Nudin
Director of Institute for Behavioural Research Ministry of Health Malaysia
Technical Working Group on Risk Communication, Malaysia.
· Dr. Norhizan Ismail · Thavaraj Subramaniam · Dr. Sulaiman Che Rus · Dr. Husnina Ibrahim · Dr. Devan Kurup · Zawaha Hj. Idris · Abdul Jabar Ahmad · Munshi Abdullah · Mohd Nasir Abdullah · Suraiya Syed Mohamed · Ricky Gayoh · Vanitha Subramaniam · Sasitheran Krishnan Kutty Nair · Norrafizah Jaafar
iv
Contributors
1. The ASEAN Emerging Infectious Diseases Programme Secretariat 70A Jalan Sisingamangaraja, Jakarta 12110, INDONESIA
2. Brunei Darussalam
Environmental Health Services Department of Health Services Ministry of Health Commonwealth Drive Bandar Seri Begawan BB3910 Negara Brunei Darussalam
3. Cambodia Communicable Disease Control Department Ministry of Health No 151-153 Kampuchea Krom Blvd., Phnom Penh
4. Indonesia
Directorate General of Disease Control and Environmental Health (DG DC & EH) Ministry of Health Jl. No State Printing. 29, PO Box 223, 10560th Jakarta - Indonesia
5. Laos PDR Department of Hygiene and Prevention Ministry of Health Samsenthai road, Ban thatkhao, Sisattanack District, Vientiane Capital, Laos PDR
6. Malaysia Disease Control Division Department of Public Health 8th Floor, Block E10, Kompleks E Federal Government Administrative Centre 62590, Putrajaya
7. Myanmar Department of Health(Disease Control) Ministry of Health

v
8. Philippines National Center for Disease Prevention and Control (NCDPC) Department of Health San Lazaro Compound, Sta. Cruz, Manila
9. Singapore Communicable Diseases Division Ministry of Health College of Medicine Building 16 College Road, Singapore 169854
10. Thailand
Department of Disease Control. Ministry of Public Health Tivanon. Talat Kwan. Muang., Nonthaburi Province. 11000.
11. Vietnam
Department of Communicable Diseases Control and Vaccine Management, Administration of Preventive Medicine, Ministry of Health 138A Giang Vo, Ba Dinh, Ha Noi.
vi
ACKNOWLEDGEMENT
This ASEAN Training Manual on Risk Communication was developed under the auspices of the ASEAN Plus Three Emerging Infectious Diseases (EID) Programme. It showcases the Training Module developed by the representatives of the ASEAN Member States during the workshop held on 21-23 October 2008 in Kuala Lumpur. This Module was used in a Regional Pilot Training on Risk communication participated by public health professionals, animal health experts and disaster management officers held on 21-23 April 2009 in Kuala Lumpur.
Sincere appreciation goes to all the representatives of the ASEAN Member States who participated in the series of activities that led to the development and production of this Training Manual.
Special acknowledgement is extended to the Ministry of Health of Malaysia, especially to the Technical Working Group, for taking the lead role in the ASEAN Initiatives on Risk communication.
The development of this Training Manual was made possible with the support of the Australian Agency for International Development (AusAID) through the ASEAN Plus Three EID Programme, managed by the ASEAN Secretariat.
vii
PREFACE BY ASEAN SECRETARIAT
Emerging infectious diseases (EIDs) pose a constant threat to countries in this region. ASEAN countries have developed a regional plan to meet the threat of EID. One of the important strategies of the EIDs Regional Plan is on communication and information. Risk communication has thus been identified as one of the important element of the communication and information strategy.
Malaysia and Philippines are identified as proponent countries in leading on the strategy for risk communication. The Philippines conducted a survey among member countries on risk communication preparedness. The result of the survey was utilized by Malaysia to formulate the Regional and Country Risk Communication Strategic Plans. Malaysia’s expertise and training experience on risk communication was utilized for a regional workshop to formulate the Regional Risk Communication Training Module. Subsequently a Regional Training of Trainers (TOT) on risk communication was conducted by Malaysia.
This training module is the culmination efforts of the Risk Communication Technical Working Group of Malaysia and the ASEAN Secretariat who reviewed and improved the ASEAN Regional Training Module on Risk Communication. The generic training module will be use by ASEAN member country as a training reference and tailor accordingly to their own needs. Over time ASEAN member countries would develop a critical mass of trainers to enable member countries have sufficient capability and capacity in risk communication in preparedness of potential threat of outbreaks due to EIDs.
The ASEAN countries have also agreed for the establishment of Risk Communication Resource Centre to be located in Malaysia. Therefore, Malaysia will continue to conduct the Regional Training Workshop on Risk communication, collate risk communication resource materials, conduct applied research and responsible for updating the training module.
However, other countries are welcome to use this training module for their training needs. Malaysia welcomes any inquiries or comments for improvements of this module.
ASEAN Secretariat
viii
PREFACE BY MINISTRY OF HEALTH MALAYSIA
Outbreaks due to Emerging Infectious Diseases (EIDs) remain a continuing health threat globally as well as to this part of the region. Malaysia had its own experiences of managing various outbreaks due to local and imported infectious agents. The experience of managing a serious outbreak due to a novel virus (Nipah virus) in 1998, highlighted the importance of risk communication as an integral component of the disease outbreak management.
Building on this and past experiences prompted the Ministry of Health to initiate its capability and capacity building on risk communication among its local staff through an organised training programme since 1999. The training programme is conducted for relevant personnel at the national, state and district levels. Therefore, Malaysia accepted the ASEAN proposal as the proponent country for ASEAN in leading the strategy for risk communication by virtue of its experiences and expertise on risk communication gained over the years.
Malaysia is glad to contribute towards the development of the ASEAN Regional Risk Communication Training Module through the participation of its two local experts on risk communication and the adoption of its National Risk communication Training Module as the main resource material. Malaysia’s commitment to regional capacity in risk communication will be further enhanced with the formal establishment of the regional Risk Communication Resource Centre under the Ministry of Health, Malaysia. The centre is envisaged to be a premier centre for training and research on risk communication. The current training module which is in an initial phase will then be regularly revised from time to time to ensure its relevance and address the changing regional needs.
Malaysia would like to thank member countries and international organisations in supporting its role as the lead proponent on risk communication. Malaysia also welcomes contributions by member countries to share their experiences on risk communication in managing local outbreaks. The inputs from member countries will be incorporated in the Regional Risk communication Training Module which will be revised on a regular basis. This coordinated regional effort will contribute significantly towards its preparedness and effectiveness in swiftly managing future regional EID outbreaks.
Regards,
Director General of Health, Malaysia
1
TABLE OF CONTENTS
Advisors, Technical Working Group And Module Contributors
ii
Acknowledgement vi
Preface vii
Table Of Contents 1
Introduction To Publication 3
Training Strategies 5
Introduction To Module 6
Workshop Requirements
1.0 Facilitators’ Guide: 7
1.1 Introduction 7
1.2 The Role Of Facilitators 8
1.3 Pre Requisites Of Organising Workshop 9
1.4 Suggestion For Facilitators 12
1.5 Summary 14
2.0 Workshop Organization: 15
2.1 Overview Of Workshop 15
2.2 Pre-Workshop Checklist 15
2.3 Workshop Objectives 16
2.4 Proposed Workshop Schedule 17
2.5 Ice-Breaking 19
Module 1
Introduction To Risk Communication 20
Unit 1: Risk, Crisis And Health Crisis Management
Unit 2: The Concept And Principles Of Risk Communication
Unit 3: Outbreak Management And
Experiences
2
**- Powerpoint presentations of the lectures is in the folder
Module 2
Risk Communication Strategies 32
Unit 1: Advocacy With Government Stakeholders
Unit 2: Encouraging Community Participation And Forging Partnerships.
Unit 3: Reaching Vulnerable Groups
Unit 4: Collaborate With International Organisations And Neighbouring Countries, Including Cross Border Issues
Module 3
Communicating Health Risk 59
Unit 1: Identification And Understanding The Audience
Unit 2: Message Development
Unit 3: Basic Skills Of Media Spokesperson
Unit 4: Media Management And Engagement
Module 4
Ethical And Legal Implication Of Risk Communication
73
Unit 1: Ethical Implication In Risk Communication
Unit 2: Legal Implication In Risk Communication
Unit 3: Politics in risk communication
Annexes 80
References 116
3
INTRODUCTION TO THE PUBLICATION
In response to epidemics and threats to human lives, ASEAN Countries have developed The ASEAN Plus Three (China, Korea and Japan) EID Programme which is funded by the Australian Government through the Australian Agency for International Development (AusAID). This Programme is also in line with the WHO Asia Pacific Strategy for Emerging Diseases (APSED). Phase I (2004-2006) of the ASEAN Plus Three EID Programme focuses on Epidemiological Surveillance and Response, Networking and Laboratory Surveillance and Institutional Strengthening.
Building on the gains of Phase I, the ASEAN Plus Three Health Ministers, at their 2nd Meeting in June 2006 in Yangon, Myanmar, endorsed Phase II of the Programme (2007-2009). One of the important strategies implemented in Phase II is the Communication, Information Sharing and Networking. The Communication Focal Points of the ASEAN Plus Three Countries were identified and are tasked to share information regarding outbreaks, under the guidance of an agreed regional protocol on communication and information. The communication workshop also recognized an urgent need for the application of risk communication in engaging the public for their perceptions and opinions and the need for decision makers to integrate risk communication in managing the epidemic itself.
Past regional outbreak experiences and experiences in managing epidemics in other parts of the world, have clearly shown the failure to practice risk communication resulted in negative perceptions by the public of the responsible health authorities and less effective control of the epidemics.
Therefore, in meeting the challenges and the delicate situation, ASEAN Plus Three Countries have come up with a regional risk communication mechanism and operational strategy to ensure policy makers and stakeholders as well as international bodies are well informed and prepared for the rapid response and containment whenever the threat occur. The project is implemented with Malaysia and Philippines as the main coordinators. Malaysia is entrusted for developing risk communication mechanism and operational strategy.
A workshop to formulate a regional and country risk communication plan was hosted by Malaysia on 24-26 March 2008 and attended by representatives of all ASEAN Plus Three Countries. The Regional Risk communication Plan which outlines strategic plans based on three Phases (Pre-, During and Post- crisis), the risk communication mechanism and the operational strategy was successfully developed. Based on the regional strategic plan, participants
4
also developed country specific risk communication plans in the same workshop. The ASEAN Secretariat subsequently obtained official endorsement of the Regional Risk communication Plan by all ASEAN Plus Three Countries.
A follow-up workshop to formulate a generic training module on risk communication for use by the region was also hosted by Malaysia on 21-23 October 2008. The workshop was attended by members from ASEAN Plus Three countries, Malaysia Technical Working Group (TWG), ASEAN Secretariat, partner organizations {WHO Western Pacific Region (WPRO), WHO South-East Asia Regional Office (SEARO), World Organization for Animal Health (OIE)} and Indonesia National Committee for Avian Influenza Control.
Recognizing the importance of risk communication to hasten the containment of a public health emergency and to mitigate the social and economic impact of a crisis, a Training of Trainers (TOT) on Risk communication using the generic regional risk communication training module was successfully conducted for officers of the Human Health and Animal Health sectors from all 10 ASEAN Member States and hosted by Malaysia. The module that was used for the TOT training was further refined by the Technical Working Group (TWG) from Malaysia and with the cooperation of the ASEAN Secretariat.
This module is indeed the culmination efforts of many sectors within and without ASEAN. This module will be invaluable to assist ASEAN member countries in conducting risk communication training locally. However, member countries are at liberty to tailor the module according to their training needs.
The ASEAN Secretariat wishes to record its appreciation to Malaysia and all member countries for their contribution in developing the module which is one of its kinds and a pride of ASEAN Countries.
Thank you.
5
TRAINING STRATEGY
A multi-pronged strategy will be instituted to meet the objectives of this training programme.
o Training will be conducted at various levels from national level, state and
district levels. o Training will be conducted in three phases. The first phase will be the
training of programme managers at national level. The second phase will encompass the training of managers at state level. Finally, the training will involve field staff at district level. Participants may also include other government agencies and non-governmental organizations (NGOs).
o The training programme should utilize interagency collaboration for expertise including from universities, Legal Training Institute, Media Consultants besides expertise from the Ministry of Health.
o Findings on regional research on risk communication will also be utilised to enhance the training module.
o Further exposures on risk communication will be made through seminars, conferences, fellowships and attachments locally and overseas.
6
INTRODUCTION TO MODULE
Risk communication has evolved from a simple one way communication to an approach that requires multidiscipline involvements. However, in United Kingdom and United States of America, the requirement to inform the public of health risks is required by the law. The concept, scope and need for risk communication have expanded to critical events such as health emergencies, crisis and disasters for which risk communication is an integral part of managing the emergency/crisis/disaster. ASEAN countries have recognized the need for building capability and capacity in risk communication to manage the continued threats of Emerging Infectious Diseases (EIDs) which pose significant health risks to ASEAN Countries in view of the ever expanding global economies and travels.
ASEAN Countries have developed a training manual on risk communication as a result of various technical meetings and workshops. The objectives of this training module are to provide skills in planning for risk communication action plan, preparing appropriate messages, media planning, and working effectively with various stakeholders such as the media. This training module which is meant for facilitators could be tailor made or custom made to cater to the various categories of staff in the health or health related sector and non health sector. Although this is the first training manual of its kind in risk communication, it is hoped it can be further improved from time to time to cater to the needs of changing times and types of emerging diseases. This training manual consists of four modules. The objectives of these modules are:
i. Module 1 - to familiarize trainees with the definitions, concepts, principles and implications of risk communication;
ii. Module 2 - to equip trainees with the knowledge of various strategies that could be employed in risk communication;
iii. Module 3 - to provide trainees with specific knowledge and skills in conducting risk communication; and
iv. Module 4 - to expose trainees to the implications of risk communication.
7
WORKSHOP REQUIREMENTS
1.0 FACILITATORS’ GUIDE
1.1 Introduction
Risk communication currently has been widely accepted as a key strategy for the management of risk of public health importance particularly risks that resulted in health emergency, crisis or disaster. The concept and practice of risk communication has been evolving since 1980s due to the complexity and diversity of risk, the development in the arts of communication and the complex nature of stakeholders, media and the well-informed community. Failure to communicate the risk may mitigate control measures for the management of disease outbreak and may affect the credibility and image of the health authority.
Risk identification, quantification and its management may not be an exact science particularly with increasing incidence of new emerging infectious diseases. This resulted in the difficulty by health care provider in devising the appropriate information and action which the public may view as over or under reaction.
The art of communication and the ever demanding media are further challenges to the health care providers. The target audience comprises of various segments of the community with different perceptions and information needs. Public risk communication information may result in different responses by the various segments of the population. The ever demanding media for information that are newsworthy may not be easily met on risk that is ongoing and chronic in nature in spite of its important to public health. Transparency of information may also be an issue when it affects the national interest or has legal implication.
Public perception and response to risk may not directly correspond entirely to the magnitude or importance of the risk. Risk communication need to address the outrage factor in formulation of messages. It is critical that the information needs assessment of the public be conducted prior to any delivery of public health messages particularly during health crisis where public tolerance is very low.
Therefore, all countries must have the capability and capacity in risk communication in meeting the potential outbreaks due to emerging infectious diseases (EIDs). Every country should develop a training module on risk communication suitable to the
8
needs of the country. In meeting this challenge, regional and global cooperation is needed in providing experts resources to the training programme.
1.2 ROLE OF FACILITATOR
1.2.1 Who is a facilitator?
A facilitator is a person who helps the participants to acquire the skills presented in the course materials, usually through individual discussions. The ideal facilitators should have expertise in both risk assessment and communication. However, it is acceptable to have facilitators with separate expertise on risk assessment and risk communication.
As a facilitator, you will need to be very familiar with the materials being taught. You should answer questions, talk with participants about the exercises, lead group discussions, and generally give participants any help they need to successfully complete the course. You will be expected to use various training methodology to teach the course contents.
1.2.2 What does the facilitator do?
A facilitator should:
1.2.2.1 Instruct
o Make sure that each participant understands how to work through materials of each module and exercise.
o Answer the participant’s questions as they occur.
o Clarify any information that the participant finds confusing and help the participants to understand the main purpose of each exercise.
o Guide group activities, such as group discussions and FGD to ensure the learning objectives are accomplished.
o Evaluate each participant’s work and giving correct answers.
o Identify weaknesses in the participant's skills or understanding and providing explanation or practice to correct them.
9
o Help the participant to understand and apply concepts taught in the course to practical problems.
1.2.2.2 Motivate
o Compliment the participant on his/her correct answers, improvements, or progress.
o Provide a conducive learning environment (such as not too noisy or inadequate lighting).
o Promote a friendly and co-operative relationship.
o Respond positively to questions.
1.2.2.3 Manage
o Make sure that each participant has access to the right supplies and materials.
o Be receptive to each participant's questions and needs.
1.3 PRE REQUISITES OF ORGANISING WORKSHOP
1.3.1 Selection of facilitators/organising committee:
o All facilitators/organising committee should have undergone risk communication training. In the absence of a trained facilitator, seek assistance from ASEAN Secretariat.
o Facilitators/organising committee should have basic knowledge of risk communication.
o Facilitators/organising committee should have involvement in risk communication related programmes.
o Select appropriate resource persons for specific topics (e.g. epidemiologist, communication specialist, legal advisor, physicians, etc).
1.3.2 Selection of participants
o Risk communication is a tool that can be used in many areas of public health.
10
o The level of knowledge and skill on risk communication varies according to the various levels of category of work and functions.
o Therefore, the content of the training module and the training methods need to be tailored according to local requirements and suitability of participants.
1.3.3 Preparing for training workshop
o One month before the course:
· Appoint a chief facilitator and ensure co-facilitators are identified for the workshop.
· Meeting with facilitators - to identify role and functions during workshop.
· Meet to identify training venue and layout of the workshop.
· Acquire the necessary audio visual aids e.g. computers, LCD and course materials for use in the workshop.
o Two weeks before the course:
· Ensure checklist for workshop is ready.
· Prepare training schedule.
· Prepare Pre & Post course participants’ assessment questionnaires.
· Prepare Evaluation Form for the conduct of Risk communication Workshop.
1.3.4 Beginning of the workshop
o Participants should be in groups of eight with a facilitator for each group. Ideally, a workshop should consist of thirty two participants with at least four facilitators.
o Facilitators should read through the training manual to ensure that they are familiar with the workshop manual.
11
1.3.5 During the training workshop
o To facilitate the workshop, all facilitators should:
· Read the topic before each exercise.
· Meet at the end of the day to review daily activities and plan schedule for the next day.
· Plan how to implement the module.
· Identify and overcome controversial issues and anticipate questions from participants.
· Identify skills taught in the manual and its application in the participants’ area of work.
· Anticipate questions from participants on how to utilise and apply these skills in their area of work
o Keep presentations lively :
· present information conversationally rather than read it
· move around room · use gestures · speak clearly. Vary pace and pitch of voice · use variety of methods to present information
1.3.6 Post Workshop Activities
It is extremely important to plan some workshop follow-up activities to determine the impact that the training has had on the performance of each participant. This should determine whether the participants are able to apply the skills they learned in the workshop.
o Review Pre-workshop performance
o Conduct Post-workshop Evaluation
o Maintain a register of:
· Resource persons
· Facilitators
12
· Lecturers
· Participants trained
o Facilitate networking among participants by providing address list
o Review and update training manual according to feedbacks from the participants to improve future training workshops
o Identify and improve weaknesses of workshop
1.4 SUGGESTIONS FOR FACILITATORS
1.4.1 Techniques for motivating participants
Interact at least once with every participant, and encourage the participants to interact with you frequently. In response, the participants will overcome their shyness and will continue to interact with you throughout the remainder of the course.
Check to see if participants have any problems. Show interest and give each participant attention to motivate them. They are more likely to ask for help if they need it. Be available and approachable to the participants at all times.
1.4.2 Do’s and don’ts
o Ask questions to check participants’ understanding and to keep them actively thinking and participating. Ask open ended questions.
o Avoid questions that can be answered by just one word.
o Give participants time to think and formulate a response. A common mistake is to ask a question and then answer it yourself.
o If no one answers your question, rephrasing it can help to break the tension of silence.
13
o Acknowledge all participants' responses. This will make the participants feel valued and encourage them to participate.
o Call participants by name.
o Maintain eye contact when interacting with reticent participant.
o Write key ideas on a flip-chart board to acknowledge responses from participants.
o Do not turn your back to the group for long period of time.
o Paraphrase and summarise frequently to keep participants focused.
o Do not let several participants talk at once. When this occurs, stop and assign an order for speaking.
o Thank participants whose comments are succinct and to the point.
o Encourage quiet participants to talk.
1.4.3 Key points in handling difficult participants
1.4.3.1 Participant who talks too much
o Walk towards the participant when he is talking to make him feel self-conscious.
o Walk away from the participant or turn your back to him to focus attention away from him.
o Do not ask the talkative participant too many questions.
o Divert the attention to other participants.
1.4.3.2 The quiet participant
o Encourage quiet participants to talk by directing questions to him/her.
o Keep eye contact.
14
o Give positive reinforcement verbally and non-verbally.
o Give time for participants to answer questions.
1.5 SUMMARY
In training workshops for Risk communication, the emphasis must be on the practical rather than theoretical aspects of risk communication. This is to provide an effective means of active learning. Facilitators should work as a team, assisting each other in providing individual feedback and conducting group discussions. This joint effort will enable the objectives of the workshop to be met and make each workshop a success.
15
WORKSHOP ORGANIZATION
2.1 OVERVIEW OF WORKSHOP
This section contains typical learning objectives and schedule for a 4-days training workshop on Risk communication. Each daily schedule includes references to various activities, which are described within each day’s schedule and are grouped together at the end of the Manual. Facilitators will need to review chapters assigned to them and prepare the materials and space as needed in order to assure the smooth progress of the training.
2.2 PRE-WORKSHOP CHECKLIST
Prepare at least 2 weeks before date of workshop. Checklist of supplies and space needed for the workshop are as below:
2.2.1 Supplies needed for each participant
o Name tag with pin
o Paper
o Ball point pen
o Pencil
o Folder with Programme schedule, Course outline and information leaflet on venue of workshop, meals and other facilities.
2.2.2 Supplies needed for each group
o Copies of workshop references
o Flip-chart stand with paper and felt pens
o Computer and LCD
2.2.3 Supplies needed for workshop
o Photocopy machine
o Camera to record activities
16
2.2.4 Space required for workshop
o A large room for plenary session
o 4 small rooms for group work
o Adequate tables and chairs
o Room for secretariat
2.3 WORKSHOP OBJECTIVES
2.3.1 General Objective
The training programme on risk communication aims to achieve the following objectives:
o To provide knowledge, strengthen skills and develop
appropriate mechanism in communicating health risks
o To develop a country specific risk communication training programme
2.3.2 Learning Objectives
o To familiarize participants with the concepts,
definition, framework, application and process of risk communication.
o To equip the participants with knowledge of the
general principles, concepts and application of risk communication within the framework of the public health system
o To develop appropriate knowledge and skills in
engaging stakeholders in advocacy and communication about Emerging Infectious Diseases (EID).
o To equip participants with relevant knowledge and skills for effective risk communication.
17
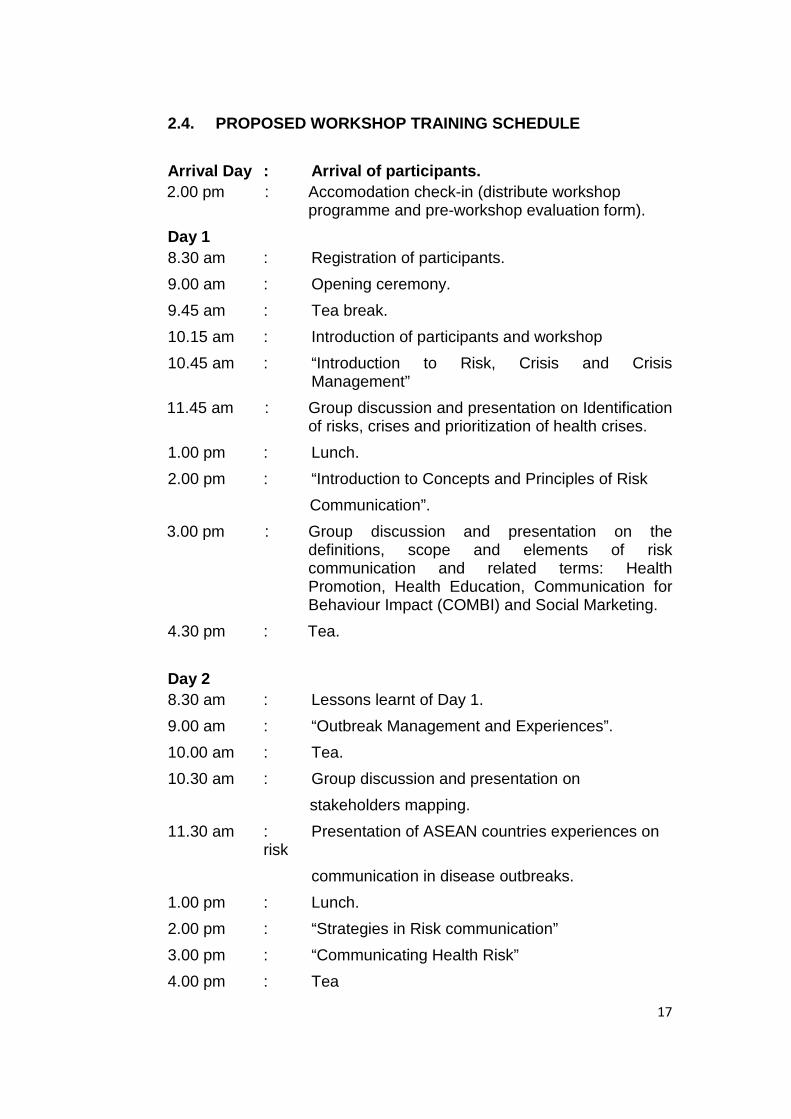
2.4. PROPOSED WORKSHOP TRAINING SCHEDULE
Arrival Day : Arrival of participants. 2.00 pm : Accomodation check-in (distribute workshop
programme and pre-workshop evaluation form).
Day 1 8.30 am : Registration of participants.
9.00 am : Opening ceremony.
9.45 am : Tea break.
10.15 am : Introduction of participants and workshop
10.45 am : “Introduction to Risk, Crisis and Crisis Management”
11.45 am : Group discussion and presentation on Identification of risks, crises and prioritization of health crises.
1.00 pm : Lunch.
2.00 pm : “Introduction to Concepts and Principles of Risk
Communication”.
3.00 pm : Group discussion and presentation on the definitions, scope and elements of risk communication and related terms: Health Promotion, Health Education, Communication for Behaviour Impact (COMBI) and Social Marketing.
4.30 pm : Tea.
Day 2 8.30 am : Lessons learnt of Day 1.
9.00 am : “Outbreak Management and Experiences”.
10.00 am : Tea.
10.30 am : Group discussion and presentation on
stakeholders mapping.
11.30 am : Presentation of ASEAN countries experiences on risk
communication in disease outbreaks.
1.00 pm : Lunch.
2.00 pm : “Strategies in Risk communication”
3.00 pm : “Communicating Health Risk”
4.00 pm : Tea
18
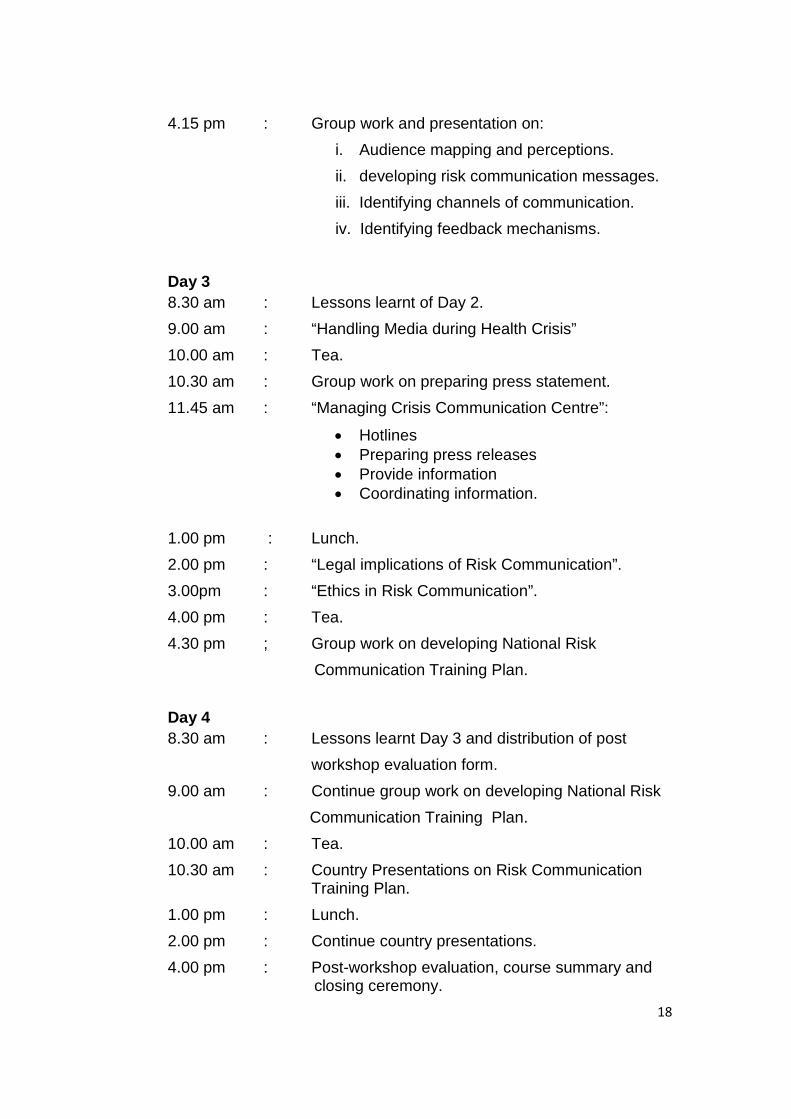
4.15 pm : Group work and presentation on:
i. Audience mapping and perceptions.
ii. developing risk communication messages.
iii. Identifying channels of communication.
iv. Identifying feedback mechanisms.
Day 3 8.30 am : Lessons learnt of Day 2.
9.00 am : “Handling Media during Health Crisis”
10.00 am : Tea.
10.30 am : Group work on preparing press statement.
11.45 am : “Managing Crisis Communication Centre”:
· Hotlines · Preparing press releases · Provide information · Coordinating information.
1.00 pm : Lunch.
2.00 pm : “Legal implications of Risk Communication”.
3.00pm : “Ethics in Risk Communication”.
4.00 pm : Tea.
4.30 pm ; Group work on developing National Risk
Communication Training Plan.
Day 4 8.30 am : Lessons learnt Day 3 and distribution of post
workshop evaluation form.
9.00 am : Continue group work on developing National Risk
Communication Training Plan.
10.00 am : Tea.
10.30 am : Country Presentations on Risk Communication Training Plan.
1.00 pm : Lunch.
2.00 pm : Continue country presentations.
4.00 pm : Post-workshop evaluation, course summary and closing ceremony.
19
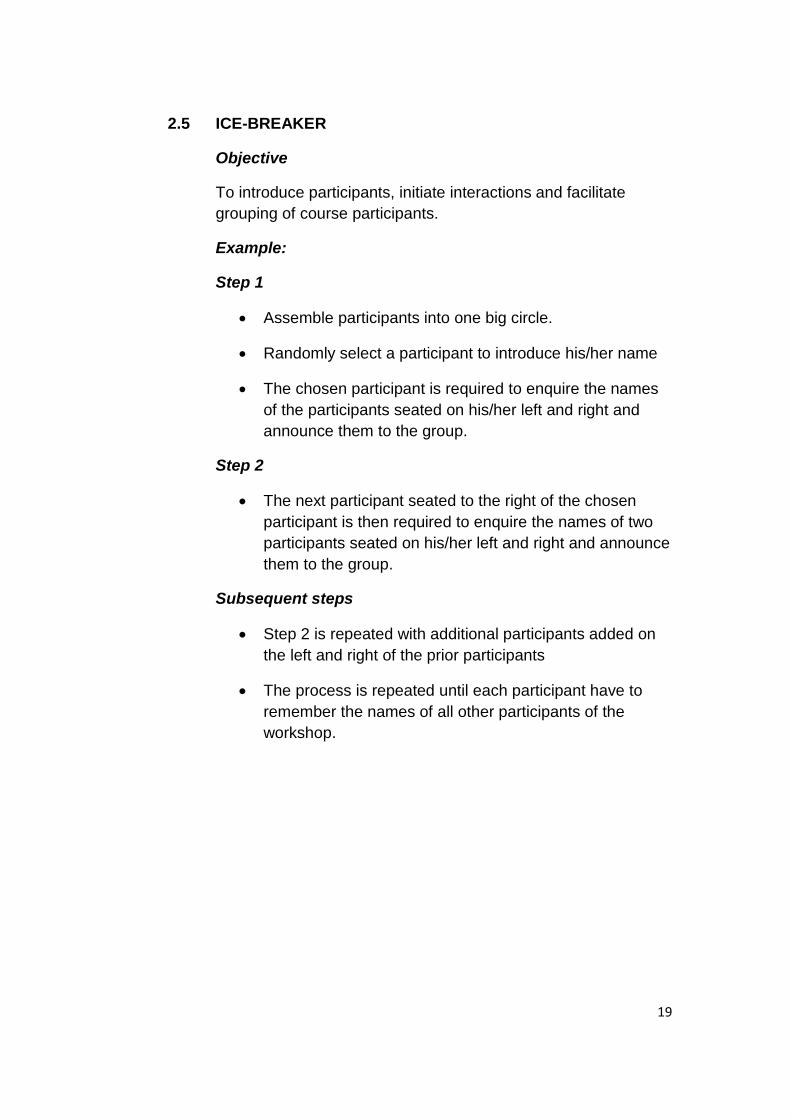
2.5 ICE-BREAKER
Objective
To introduce participants, initiate interactions and facilitate grouping of course participants.
Example:
Step 1
· Assemble participants into one big circle.
· Randomly select a participant to introduce his/her name
· The chosen participant is required to enquire the names of the participants seated on his/her left and right and announce them to the group.
Step 2
· The next participant seated to the right of the chosen participant is then required to enquire the names of two participants seated on his/her left and right and announce them to the group.
Subsequent steps
· Step 2 is repeated with additional participants added on the left and right of the prior participants
· The process is repeated until each participant have to remember the names of all other participants of the workshop.
20
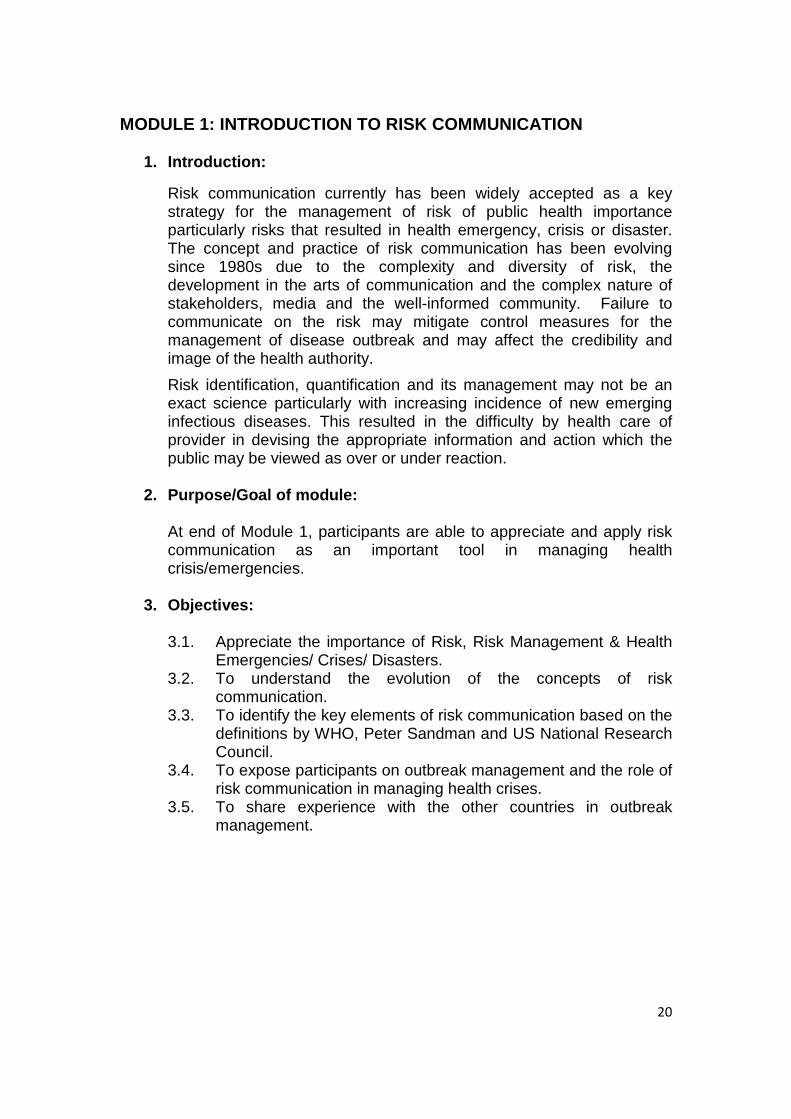
MODULE 1: INTRODUCTION TO RISK COMMUNICATION
1. Introduction:
Risk communication currently has been widely accepted as a key strategy for the management of risk of public health importance particularly risks that resulted in health emergency, crisis or disaster. The concept and practice of risk communication has been evolving since 1980s due to the complexity and diversity of risk, the development in the arts of communication and the complex nature of stakeholders, media and the well-informed community. Failure to communicate on the risk may mitigate control measures for the management of disease outbreak and may affect the credibility and image of the health authority.
Risk identification, quantification and its management may not be an exact science particularly with increasing incidence of new emerging infectious diseases. This resulted in the difficulty by health care of provider in devising the appropriate information and action which the public may be viewed as over or under reaction.
2. Purpose/Goal of module:
At end of Module 1, participants are able to appreciate and apply risk communication as an important tool in managing health crisis/emergencies.
3. Objectives:
3.1. Appreciate the importance of Risk, Risk Management & Health Emergencies/ Crises/ Disasters.
3.2. To understand the evolution of the concepts of risk communication.
3.3. To identify the key elements of risk communication based on the definitions by WHO, Peter Sandman and US National Research Council.
3.4. To expose participants on outbreak management and the role of risk communication in managing health crises.
3.5. To share experience with the other countries in outbreak management.
21
4. Contents of Module 1:
UNIT 1: Risk, Crisis and Health Crisis Management:
· Hazard, its identification, dose-response assessment, exposure assessment & risk characterization.
· Risk management. · Health Crisis. · Management of Health Crisis.
UNIT 2: The Concepts and Principles of Risk Communication:
· Evolution of concepts of risk communication. · Definitions, scope and essential elements of risk
communication and comparison to other related terms.
· Goals of Risk communication: o Vary according to situation. o Why Risk communication is important. o How RC is useful?
· Risk perceptions (scientific risk, and emotional assessment)
and responses towards risk messages of public and media. · Types of Risk Communication (Peter Sandman):
o Precaution advocacy. o Crisis communication. o Public relation (health education). o Outrage management.
· Risk Communication Best Practices (WHO):
o Trust o Transparency o Announcing early o Listening o Planning
22
· Seven Cardinal Rules of Risk communication: o Accept and involve the receiver of risk information as a
legitimate partner. o Plan and tailor risk communication strategies. o Listen to your audience. o Be honest, frank and open. o Coordinate and collaborate with other credible sources. o Plan for media influence. o Speak clearly and with compassion.
· What is not risk communication?
Different concepts and terms related to risk communication: o Health education. o Health promotion. o Communication for Behavioural Impact (COMBI). o Social mobilization. o Social marketing. o Public information. o Public relations. o Media relations. o Community participation, citizen involvement. o Advocacy. o Include other terminology as needed.
UNIT3: Outbreak Management Experiences
· Presentation of a typical outbreak management.
· Sharing country experiences in risk communication during health crisis by ASEAN member countries..
5. Instructional Guide:
UNIT 1: Risk, Crisis, and Health Crisis Management.
Learning Objectives: · Recognize the importance of Risk, Crisis and Health
Crisis Management.
Methodology: · Lecture, brainstorming and discussion.
23
Learning Process: · Activity 1 - Lecture. · Activity 2 – Brainstorming & Group Discussion.
Activity 1: Lecture Topic (“Risk, crisis and crisis management”).
Content:
1. Hazards and exposures. 2. Risk assessment and characterization. 3. Risk management. 4. Risks leading to health crises. 5. General principles of health crisis management
Activity 2: Brainstorming & Group Discussion on risks
and health crises identification.
Content:
1. Break into groups. 2. Identify health risks in the work settings. 3. Identify risks that have potential of leading to health
crises. 4. Prioritize health crises of importance. 5. Present to the group in power point or flip chart. Teaching Aids: · Power-point. · Hand out notes. · Case studies.
Duration: · Activity 1: 45 minutes. · Activity 2: One and half hour.
Evaluation:
· Q & A.
Technical Resource: · Occupational Health Specialist. · Epidemiologist. · Public Health Physician.
24
UNIT 2 – The Concepts and principles of Risk Communication.
Learning Objectives: · Able to explain the evolution of the concepts of risk
communication. · To identify the key elements of risk communication
based on the definitions by WHO, Peter Sandman and US National Research Council.
· Apply the usage of risk communication especially in the context of health crises.
Methodology: · Lectures. · Group discussion and presentation.
Learning Process:
· Activity 1 - Lecture · Activity 2 – Group work.
Optional: o Simulation video o Animation Spot (e.g. clip of press statement) o Illustration of concepts o Checklist to review the content o Short quizzes
Activity 1: Lecture Topic (“Concepts and Principles of Risk
Communication”)
Content:
1. Evolution of the concepts of risk communication. 2. Definitions and essential elements of risk
communication. 3. Goals of Risk communication. 4. Risk Perceptions. 5. Types of Risk communication. 6. Complexities of risk communication. 7. WHO Best Practise in Outbreak Communication. 8. Seven Cardinal Rules of Risk communication.
Activity 2: Group Work
1. Break into groups. 2. Group discussion on the definitions of risk
communications.
25
3. Identify the important scope/elements of risk communication.
4. Present to the group in power point or flip chart.
Teaching Aids: o Power-point. o Hand out notes.
Optional: o Compact Disc. o Video. o Audiovisuals.
Duration:
· Activity 1 – 45 minutes. · Activity 2 – one and half hour.
Evaluation:
Q & A. Technical Resource: · Occupational Health Specialist/Epidemiologist. · Communication experts
UNIT 3: Outbreak Management experiences
Learning Objective
At end of the session, participants will be able to:
a) Exposure and sharing experience on outbreak management
b) Identify the various existing mechanisms in information management.
c) Role of risk communication in outbreak management.
Methodology
a) Lecture (45 minutes) b) Country presentation on outbreak experiences
(one and half hour)
Learning Process
Activity 1: Lecture
26
Content:
a) Information management during crisis b) Mechanisms in managing information
c) Information management in risk communication
Activity 2: Country Presentations on Outbreak Management of each member country.
Teaching Aids
a) Computer b) LCD c) Power point presentation d) Handouts
Duration
Activity 1 – 45 minutes and Q&A. Activity 2 - One and half hour.
Assessment Method
Pre and post test
27
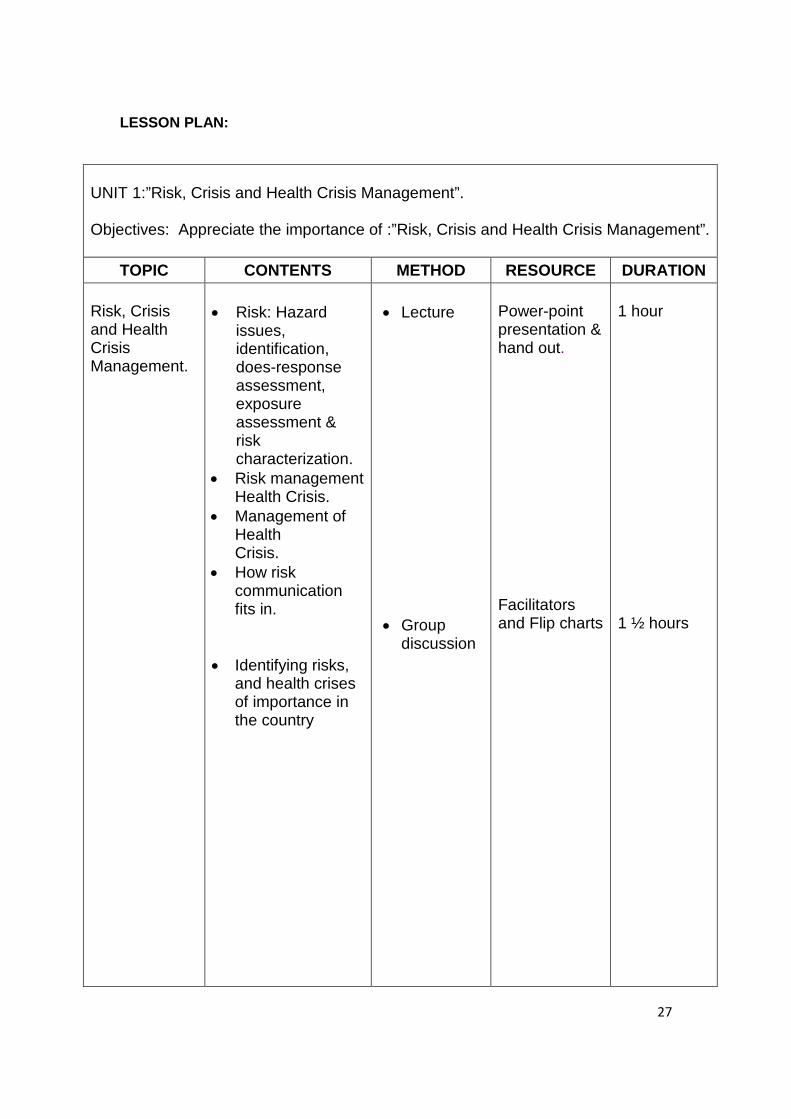
LESSON PLAN:
UNIT 1:”Risk, Crisis and Health Crisis Management”. Objectives: Appreciate the importance of :”Risk, Crisis and Health Crisis Management”.
TOPIC CONTENTS METHOD RESOURCE DURATION Risk, Crisis and Health Crisis Management.
· Risk: Hazard
issues, identification, does-response assessment, exposure assessment & risk characterization.
· Risk management Health Crisis.
· Management of Health Crisis.
· How risk communication fits in.
· Identifying risks, and health crises of importance in the country
· Lecture · Group
discussion
Power-point presentation & hand out. Facilitators and Flip charts
1 hour 1 ½ hours
28
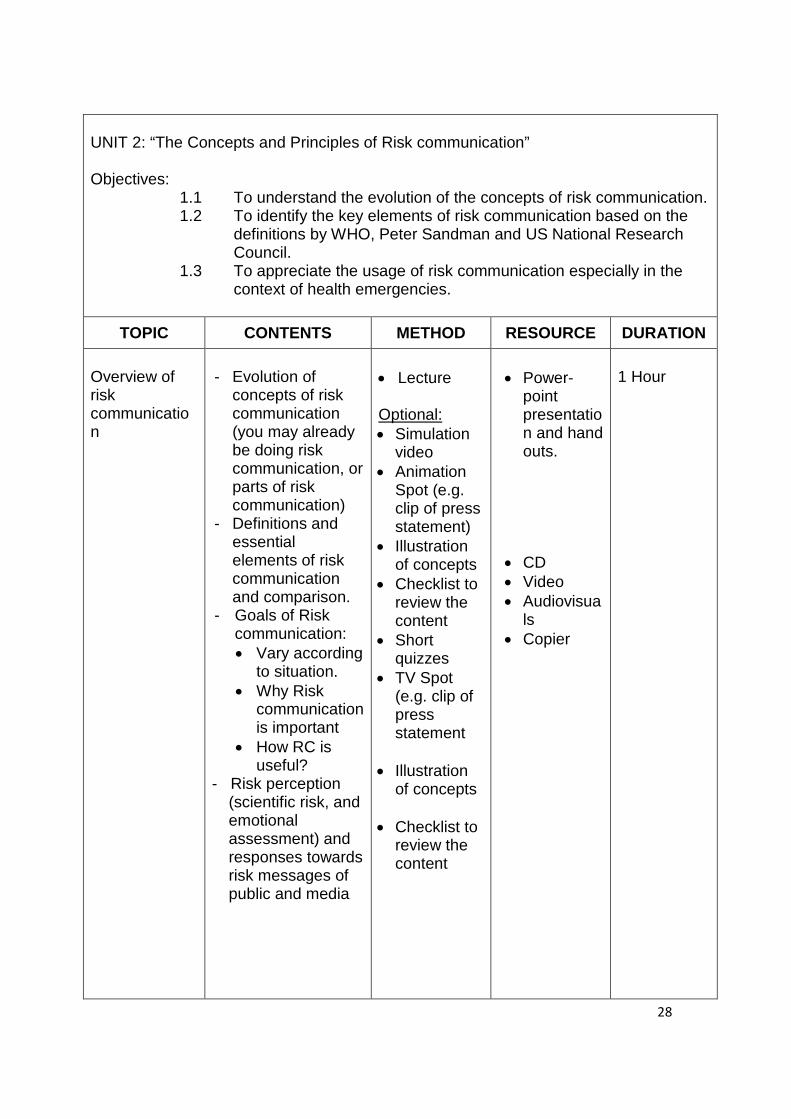
UNIT 2: “The Concepts and Principles of Risk communication” Objectives:
1.1 To understand the evolution of the concepts of risk communication. 1.2 To identify the key elements of risk communication based on the
definitions by WHO, Peter Sandman and US National Research Council.
1.3 To appreciate the usage of risk communication especially in the context of health emergencies.
TOPIC CONTENTS METHOD RESOURCE DURATION
Overview of risk communication
- Evolution of
concepts of risk communication (you may already be doing risk communication, or parts of risk communication)
- Definitions and essential elements of risk communication and comparison.
- Goals of Risk communication: · Vary according
to situation. · Why Risk
communication is important
· How RC is useful?
- Risk perception (scientific risk, and emotional assessment) and responses towards risk messages of public and media
· Lecture Optional: · Simulation
video · Animation
Spot (e.g. clip of press statement)
· Illustration of concepts
· Checklist to review the content
· Short quizzes
· TV Spot (e.g. clip of press statement
· Illustration
of concepts · Checklist to
review the content
· Power-
point presentation and hand outs.
· CD · Video · Audiovisua
ls · Copier
1 Hour
29
Types of Risk communication (Peter Sandman) · Precaution
Advocacy · Crises
communication · Public relation
(health education)
· Outrage management
Risk communication Principles (WHO) · Trust · Transparency · Announcing
early · Listening · Planning
Seven Cardinal Rules of Risk communication · Accept and
involve the receiver of risk information as a legitimate partner.
· Plan and tailor risk communication strategies.
· Listen to your audience.
· Be honest, frank and open.
· Coordinate and collaborate with other credible sources.
· Plan for media influence.
· Group work Facilitators and flip charts
1 ½ hours
30
What is not risk communication? Different concepts and terms related to risk communication: · Health
education · Health
promotion · Communication
for Behavioural Impact (COMBI)
· Social mobilization
· Social marketing · Public
information · Public relations · Media relations · Community
participation, citizen involvement
· Advocacy · Include other
terminology as needed.
Man: · Expertise
in RC & media relations.
· Experienced trainer.
· Money: · Fund for
consultancy fees
· Travel, accommodation & training materials
Material: · Handouts · CD · Video · Audiovisu
als · Copier · Flip chart
31
UNIT 3:” Outbreaks Management and Experiences”. Objectives: Appreciate the importance of risk communication in outbreaks
management”.
TOPIC CONTENTS METHOD RESOURCE DURATION
Participants will expose to outbreak management and the important role of risk communication
· Exposure on how
to manage outbreak
· What is management of information?
· Who will manage
information?
· Effective delivery channels for information
· Disclosure of
information
· Lecture
· Country presentation
· EID
Program manager
· Health
Education Department
· Communic
ation Expert
· Public
Relation Officer
1 hour 1 ½ hours
· Risk assessment
of public health threat and dissemination of information, Interpretation and verification of the information (real and perceived threat)
· Preparing
communities for actions to take with information
· Communicating
risk with information to prevent panic.
· EID
Program manager/
· Epidemiologist
· Communic
ation Expert /Health promoter
· Health
Education Department
32
MODULE 2: RISK COMMUNICATION STRATEGIES
1. Introduction
Risk communication strategies are known as seeking cooperation from governmental, non governmental agencies and stakeholders in order to elicit advocacy, networking and community participation. The strategy should obtain and gather feedback during crisis, building up partnership and collaboration with the respective organization. A customized training programme need to be carried out as well as conducting process and impact assessment.
2. Purpose of module
Participants will understand and apply the risk communication strategies during health crisis.
3. Module Objective
In this module, participants will acquire knowledge and skills on how to identify and advocate to the stakeholders, build networking, using appropriate risk communication strategies in reaching vulnerable groups and empower community for active participation during health crisis
33
4. Contents of Module 2
UNIT 1 - Advocacy and networking with stakeholders
· Definition of advocacy · Elements of advocacy · Levels and process of advocacy · Definition of networking for risk communication · Definition of stakeholders and Identify key stakeholders · Types of stakeholders. · List of internal and external stakeholders involved in health
crisis · Needs and preferences of stakeholders · The role of networking and advocacy in the context of risk
communication
UNIT 2 - Encouraging community participation and forging partnerships
· Definition of community & community participation · Community mobilisation for risk communication · Community and public meetings · Peer education · Generating support from stakeholders and others
UNIT 3 - Reaching vulnerable groups (e.g., migrant workers and indigenous groups, mothers, children etc)
· Identification of vulnerable groups and their information
needs. · Message development and dissemination – access
community and local radio. · Enabling mechanisms for preparedness response and recovery. · Identification and networking with local NGOs and leaders
of migrants/workers and others
34
UNIT 4 - Collaborate with international organisations and neighbouring countries, including cross border issues
· Orientation on existing protocol and mechanisms for
sharing information on public health emergencies. · Maximising web-based information dissemination to reach
others. · Developing and sharing messages (e.g., cultural
considerations, translation / language, etc.) for cross border relevant sectors (e.g., customs, quarantine, livestock, health, police, tourism, etc.)
5. Instructional Guide
UNIT 1 - Advocacy and networking with stakeholders
Learning Objective 1
At end of the session, participants will be able to:
1. Discuss advocacy and networking in the context of risks
communication in health crisis 2. Explain the importance of advocacy and networking plan
for risk communication 3. Identify collaborating partners for risk communication 4. Define roles of partners in risk communication.
Methodology 1. Brainstorming (10 minutes) 2. Lecture (40 minutes) 3. Discussion (10 minutes)
Learning Process Activity 1: Brainstorming Sharing ideas’ session among participants in order to understand the concept of advocacy and networking in the context of risk communication in health crisis before starting the lecture.
35
Activity 2: Lecture Contents: · Definition of advocacy · Elements of advocacy · Level & Process of advocacy · Definition of networking for risk communication · The role of networking and advocacy in the context of risk
communication Activity 3: Discussion 1. Discussion on advocacy and networking in the context of
risk communication in health crisis. · Divide participants into groups. · Discuss the scenario given within the group’s member. · Present group’s findings to other groups. · Q & A Teaching Aids Computer LCD Power point presentation Duration 1 hour Assessment Method Q & A
36
Activity 1: Brainstorming
Brainstorming activity can be a useful approach for generating participants existing understanding on advocacy, its level and process of advocacy. The facilitator shall pair or group participants to make suggestions with no restrictions on the extent of their understanding.
Participants in the exercise use the Post-It Notes to write down additional ideas. Participants stick the notes on the wall - randomly at first - and then moved and grouped together as the exercise plays out.
The participants will encounter ideas of (limit the probing according to the needs and preferences):
a) What do you understand about advocacy? b) What are the elements of advocacy? c) Explain the level and process of advocacy.
In order to ensure a successful exercise, it is vital that participants feel comfortable about sharing ideas. This technique is ideal for participants who have not encountered scenario planning before as it offers the opportunity to become actively involved very quickly before the lecture.
Activity 2: Lecture
Prepare Power Point presentation based on the key contents, Exercise Notes Unit 3.1 and Appendix 1.
37
Activity 3: Discussion
Scenario: Adapted from Crisis and Emergency Risk Communication, CDC 2002
Case Study. H5N1 Virus Outbreak Investigation, Hong Kong, 1997–1998
In May 1997, a 3-year-old Hong Kong boy became ill with fever, dry cough, and a sore throat. He was hospitalized, continued a downward course, and died. Only influenza A virus was cultured from this child.
Scientists identified the virus as influenza A/(H5N1). This virus had never before been cultured from a human specimen. The subsequent investigation ruled out laboratory contamination, and concluded that the child’s illness was consistent with influenza complicated by viral pneumonia. Investigators believed, based on laboratory evidence, that the virus was transmitted directly from an avian source to the child, possibly in the outdoor garden area of his school. This was the first reported case of an avian virus being transmitted directly to a human. During the August–September investigation, no other cases were found.
In late November, the Hong Kong Department of Health contacted CDC’s Influenza Branch to report that a second H5N1 infection had been detected. CDC sent a team of medical epidemiologists and field investigators.
CDC and health organizations around the world engage in ongoing, active surveillance to attempt to quickly detect the possibility of a pandemic influenza virus spreading among humans. Influenza viruses mutate easily. Most often the mutation is slight and occurs over time, a process called “drift.” Occasionally, an influenza virus will suddenly mutate significantly; this is called “shift.” A virus that shifts is a potential pandemic strain. To qualify as a potential pandemic strain, the virus must meet 3 criteria: (1) it must be genetically novel, (2 ) it must be virulent, and (3) it must be efficiently transmitted between humans.
In late December, cases were accumulating and young healthy adults were dying of this viral infection. The H5N1 virus in this outbreak met 2 of the 3 criteria: it was novel and it was virulent. CDC, Hong Kong DOH and a number of collaborators began an intense investigation to determine whether this was the start of an influenza pandemic. Indeed, public health officials know, based on trend analysis, that a pandemic is overdue. Investigators concentrated on determining the virus’ ability to transmit from person to person. An increase in person-to-person virus transmission would have suggested that the virus was adapting to humans, with the potential for epidemic spread.
In mid-December, a veterinarian virologist collaborating on the investigation held a telephone worldwide news conference and announced this was the “pandemic” strain that health officials were expecting. The immediate media uproar severely disturbed the investigators’ attempts to collect information in Hong Kong. The Hong Kong DOH and the CDC field team requested that a CDC public information officer (PIO) join the team in Hong Kong, the first time CDC had assigned a PIO on an overseas field investigation. During the field assignment, the CDC PIO represented CDC, DHHS and WHO on public information issues.
38
Learning Objective 2 At end of the session, participants will be able to: 1. Identify role & responsibilities of key stakeholder groups. Methodology 1. Mapping Exercise (15 minutes) 2. Group Presentation (5 minutes per group) 3. Lecture (40 minutes) Learning Process Activity 1: Mapping Exercise & Group Presentation · Divide participants into groups · Groups to identify & list down internal and external stakeholders
involve in health crisis · Present group’s findings to other groups. Activity 2: Lecture Contents: · Definition of stakeholder · Types of stakeholder · Needs and preferences of stakeholders · Advocacy to the key decision makers – budget, finance,
parliament, veterinary, tourism, education, quarantine, manpower/interior (e.g., legal and illegal migrant workers), customs, national defence, police, trade, industry, information, etc.
Teaching Aids Kraft / Mahjong paper Marker pen White board Computer LCD Power point Pointer
39
Duration
1 hour
Assessment Method
Q & A
Resources
1. Manpower - the field experts. 2. Please refer to Annex 1
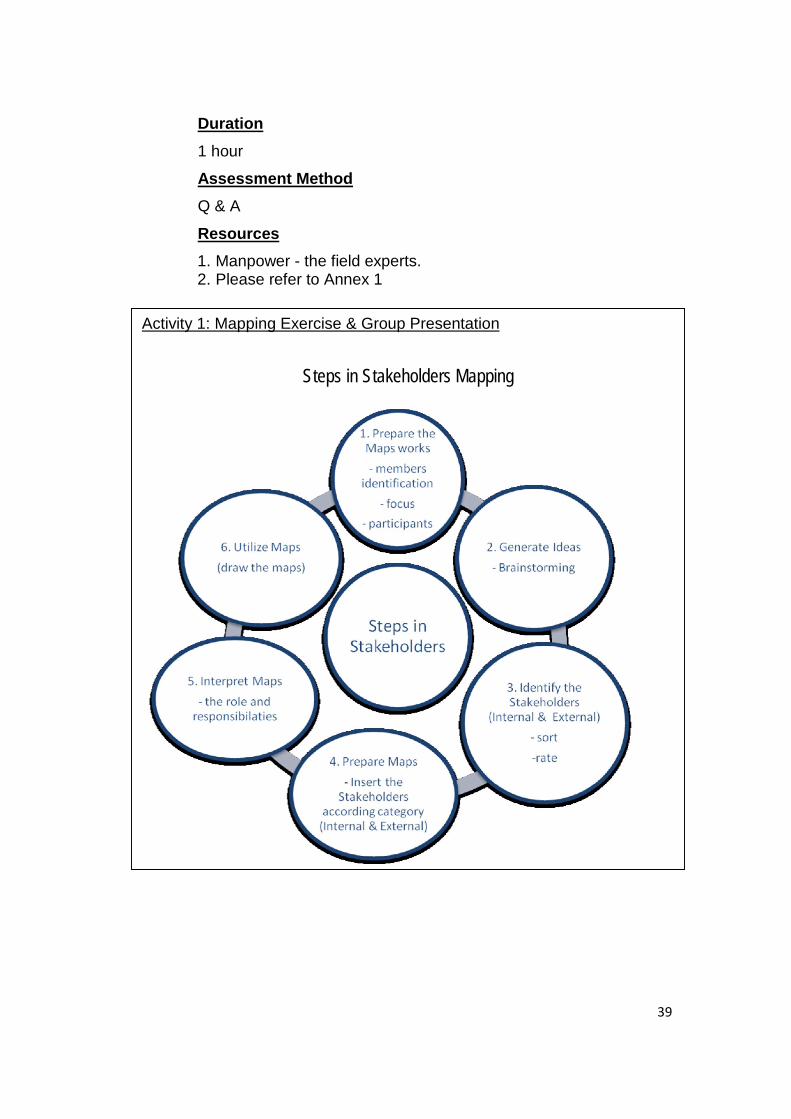
Activity 1: Mapping Exercise & Group Presentation
Steps in Stakeholders Mapping

40
STAKEHOLDERS
EXAMPLE: STAKEHOLDERS MAPPING DURING OUTBREAK OF INFLUENZA IN MALAYSIA
External stakeholders INTERNAL
STAKEHOLDER
Ministry of Health Malaysia
NIH
PHL
CDC CRC
PHIMDD
IHBR
National Security Council
Ministry of Education
FHDD
Surveillance CDC
HED
Public Relation Division, MOH
Media
NGOs MMA
MAHEO Community organization
Internal External media
Employment agencies (Foreign workers)
HED: Health Education Division MDD: Medical Development Division FHDD: Family Health Development Division PHL: Public Health Laboratory IHBR: Institute for Health Behavioural Research PHI: Public Health Institute CRC: Clinical Research Centres
41
EXAMPLE IN THE PROVINCE/STATE: (adapted from Health Department, Pahang, Malaysia)
ROLES AND FUNCTIONS OF OTHER DEPARTMENTS AND NON-GOVERNMENTAL
ORGANISATIONS IN PAHANG DURING INFLUENZA PANDEMIC
STATE GOVERNMENT
a) To ensure co-ordination in issues related to security and public order on the Influenza
pandemic
b) To give advice on security issues related to the Influenza Pandemic.
c) To provide security cover, if needed during enforcement of PCIDA 1998.
d) To facilitate all matters pertaining to security and public order e.g reduce spreading of
myths related to the Influenza Pandemic.
DEPARTMENT OF AGRICULTURE
a) To help in all matters on international relation pertaining to the Influenza Pandemic.
b) To obtain information on the latest situation and updated development on the Influenza
Pandemic in the affected countries.
c) To facilitate all matters related to the control of the Avian Influenza.
ROAD AND TRANSPORT DEPARTMENT
a) To ensure compliance of all control measures on the Influenza Pandemic agreed upon
regarding public transportation in and out of entry point in the country.
b) To co-ordinate issues in the control of the Influenza pandemic, related o the movement of
public transportation and people.
c) To facilitate all transportation issues related to the Influenza Pandemic.
d) To ensure all passengers boarding airplanes from country affected by the Influenza
Pandemic to Pahang have their medical screening prior to departure, completed health
declaration forms on board the planes before disembarking and isolation on board if the
passengers are suspected cases of Influenza.
42
DEPARTMENT OF INFORMATION
a) To disseminate relevant information to the community regarding the status of outbreak
and educational materials and public information on the Influenza Pandemic.
b) To coordinate press conferences and all mass media activities on the Influenza
Pandemic.
c) To facilitate all matters as regards the print and electronic media related to SARS.
DEPARTMENT OF SOCIAL WELFARE
a) To help in the Influenza Pandemic control measures by printing and disseminating
information on the Influenza Pandemic.
b) To implement and enforce preventive and control measures in all childcare centre under
its jurisdiction.
c) To coordinate all activities for the families related to Influenza.
d) To facilitate all matters concerning families and community related to Influenza.
EDUCATON DEPARTMENT/ DEPARTMENT OF HIGHER EDUCATION
a) To disseminate updated information on the control measures of the Influenza Pandemic
to all teachers and students.
b) To remind all students, their parents or guardians that student who are ill with symptoms
and signs similar to Influenza to be examined and treated by doctors and not to allow
them to attend school during in the period of illness.
c) To request parents or guardians to monitor the health status of their children and to refer
to doctors if they are ill.
d) To facilitate all measures on the prevention and control of Influenza at the school level
and especially college and university level where many foreign students come to study
in the state.
e) To help implement the screening of foreign students returning to the colleges and
universities after their holidays from affected Influenza Pandemic countries.
43
MINISTRY OF RURAL DEVELOPMENT
a) To help disseminate information of the Influenza Pandemic to the rural communities.
b) To facilitate all matters related to the Influenza Pandemic in the rural areas.
c) To implement and enforce preventive and control measures in the childcare centre under
their supervision.
STATE TOURISM BOARD
a) To help print and disseminate all official information issued by the Ministry Of Health to all
those related to the tourism industries.
b) To help give feedbacks the State Inter - sectoral Committee on Influenza pandemic on
matters concerning tourism.
c) To facilitate all matters on the influenza Pandemic related to the tourism sector.
DEPARTMENT OF IMMIGRATION
a) To facilitate the screening process of people/travellers at entry points into the country.
b) To help coordinate all health Influenza issues related to the movements of all aliens
especially foreign workers into the country.
c) To help identify ill individuals/travellers coming through immigration check points.
d) To facilitate all matters on the Influenza Pandemic related to immigration.
e) To be stringent in the issues of visa/temporary visa of travellers from the Influenza
Pandemic affected countries.
DEPARTMENT OF OCCUPATIONAL SAFETY AND HEALTH
a) To monitor the health of workers and to take remedial action to rectify if needed.
b) To help print and distribute education materials on Influenza Pandemic and to advise on
the risk factors in the work place and surroundings.
c) To facilitate all matters concerning dangers of the surroundings related to the spread of
the Influenza.
44
ROYAL MALAYSIAN POLICE
a) To ensure coordination of security and public order in the control of the Influenza
Pandemic.
b) To give advice on security matters pertaining to the Influenza Pandemic if any.
c) To provide security cover, if needed, in the enforcement of PCIDA 1998.
d) To facilitate all matters concerning security and public order if any pertaining to the
Influenza Pandemic e.g. rumour mongering.
ASSOCIATION OF PRIVATE HOSPITALS, MALAYSIA (PAHANG BRANCH)
a. To disseminate all information regarding Influenza including the hospital management of
Influenza to all members of the association.
b. To coordinate all activities and measures on Hospital Infection Control in private hospitals in
dealing with infectious diseases.
c. To quickly refer all suspected / probable Influenza patient/s to the nearest Influenza Pandemic
Designated Hospital/s when indicated in the guidelines of MOH.
PAHANG PRIVATE PRACTITIONERS SOCIETY (MMA)
a. To help disseminate all information regarding Influenza and the pandemic to its members.
b. To help teach the community who are ill to come for early treatment.
c. To help detect early any person/s who may present with symptoms of Influenza for referral to
designated hospitals when indicated by MOH guidelines.
MALAYSIAN MEDICAL ASSOCIATION (PAHANG BRANCH)
a. To help disseminate all information regarding Influenza and the pandemic to its members.
b. To help teach the community who are ill to come for early treatment.
c. To help detect early any person/s who may present with symptoms of Influenza for referral to
designated hospitals when indicated by MOH guidelines.
d. To facilitate all matters pertaining to the primary care Influenza.
45
PAHANG VETERINARY SERVICE DEPARTMENT
a. To develop their own risk communication for those involved in handling poultries activities.
b. To disseminate information on Good Farming Practices in Poultry .
c. To reinforce Guidelines an Acts on Poultry activities to prevent Avian Influenza.
MEDIA (RADIO, TV AND LOCAL NEWSPAPERS)
Some general Guidelines were put forward to keep the media on tract and help avoid sensational
reporting.
a. To anticipate media needs; to get full cooperation and support in disseminating correct
information to the public on Influenza Pandemic latest situation.
b. To help Local Authority /Health Department to disseminate Health Educating Materials.
c. To concentrate on facts and figures but humanize the situation with metaphors and anecdotes.
46
PAHANG MALAYSIA RED CRESCENT SOCIETY
a. To help in transporting the Pandemic Influenza patient (when needed), especially during Phase
5-6.
b. To help in logistics (e.g. Preparation food and shelter for the affected people).
PAHANG ST JOHN AMBULANCE
a. To help in transporting the Pandemic Influenza patient (when needed), especially during Phase
5-6.
b. To help in logistics (e.g. Preparation food and shelter for the affected people).
PAHANG CIVIL DEFENSE DEPARMENT (JPA3)
a. To help in transporting the Pandemic Influenza patient (when needed), especially during Phase
5-6.
b. To help in first aid and logistics (e.g. Preparation food and shelter for the affected people).
DISTRICT OFFICE
a. To get good support in regards of security, logistic, welfare of local people.
b. To develop District Committee on Influenza Pandemic Preparedness Plan.
c. To coordinate with other agencies on Influenza Control activities.
LOCAL AUTHORITY
a. To highlight issues in council meeting regarding Influenza.
b. To coordinate Public Health activities within their authority.
c. To enforce Local Authority Act on Disease Prevention Control.
47
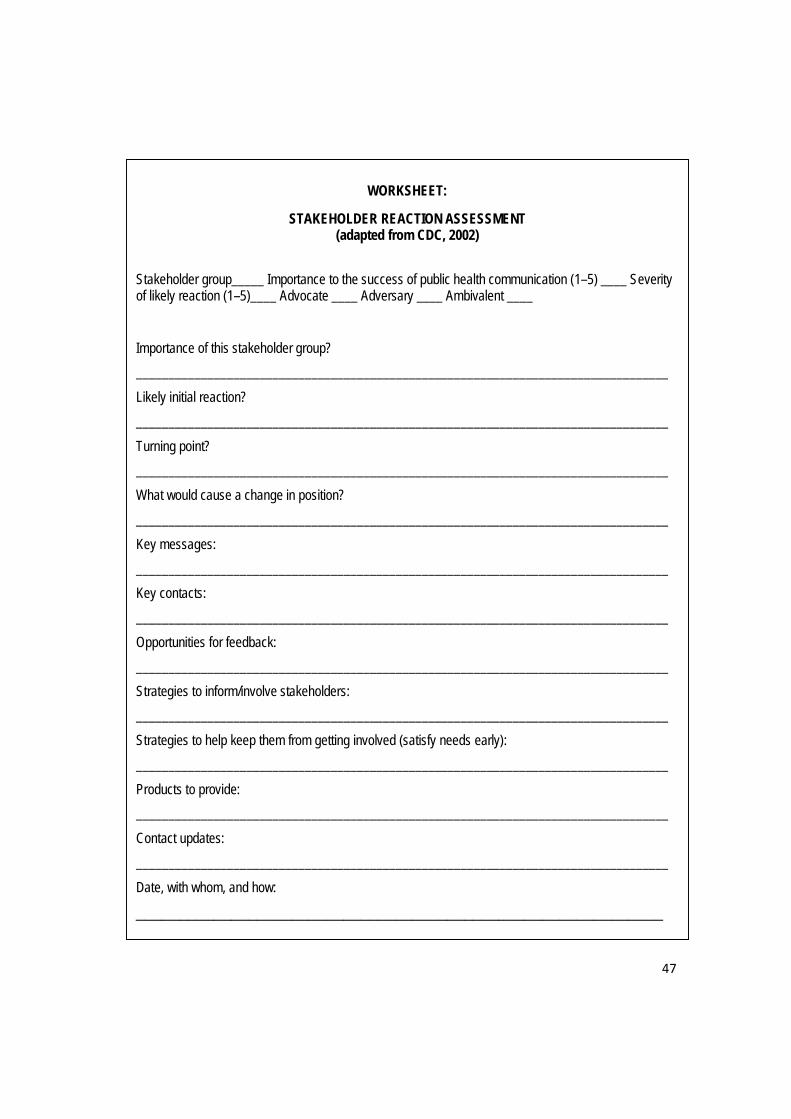
WORKSHEET:
STAKEHOLDER REACTION ASSESSMENT (adapted from CDC, 2002)
Stakeholder group_____ Importance to the success of public health communication (1–5) ____ Severity of likely reaction (1–5)____ Advocate ____ Adversary ____ Ambivalent ____
Importance of this stakeholder group?
__________________________________________________________________________________
Likely initial reaction?
__________________________________________________________________________________
Turning point?
__________________________________________________________________________________
What would cause a change in position?
__________________________________________________________________________________
Key messages:
__________________________________________________________________________________
Key contacts:
__________________________________________________________________________________
Opportunities for feedback:
__________________________________________________________________________________
Strategies to inform/involve stakeholders:
__________________________________________________________________________________
Strategies to help keep them from getting involved (satisfy needs early):
__________________________________________________________________________________
Products to provide:
__________________________________________________________________________________
Contact updates:
__________________________________________________________________________________
Date, with whom, and how:
_____________________________________________________________
48
UNIT 2: Encouraging community participation and forging partnerships.
Learning Objective 1 At end of the session, participants will be able to:
1. Identify the community’s perception and needs, thus respond to them
2. Develop knowledge and skills on how to encourage community participation and forging partnership
Methodology
1. Lecture (40 minutes) 2. Sharing the experiences / country’s (60 minutes)
experiences & lesson learnt
OPTIONAL
3. Case study 4. Role Play
Learning Process Activity 1: Lecture Contents:
· Definition of community · Definition of community participation · The importance of community participation / involvement · Factors that influence public perception · Skills on how to encourage community participation &
forging partnership · Community mobilisation for risk communication · Community and public meetings · Peer education · Generating support from stakeholders and others
49
Activity 2: Sharing the experiences / country’s experiences & lesson learnt Participant sharing experience & lesson learnt on encouraging community participation & forging partnership. · Q & A
OR (for country’s experiences)
1. Invite spokesperson from the chosen country & sharing experiences on encouraging community participation & forging partnership.
· Q & A OR through video presentation (OPTIONAL)
Activity 3: Case Study · Divide participants into groups · Discuss the scenario given with your group members · Present group’s findings to other groups · Q & A
(OPTIONAL) Activity 4: Role Play · Request volunteers or select participants · Discuss the scenario given with your group members · Conduct the role play · Evaluate and Q & A
Teaching Aids Computer LCD Power point presentation Video
50
Duration 1 hour & 40 minutes Assessment Method Feedback on presentation Q & A Resources
1. Manpower - the field experts. 2. Please refer to Annex 2
51
UNIT 3: Reaching vulnerable groups
Learning Objective 1 At end of the session, participants will be able to:
1. Identify vulnerable groups in the community 2. Identify correct messages for vulnerable groups in the
community Methodology
1. Lecture (40 minutes) 2. Sharing the experiences / country’s
experiences & lesson learnt (30 minutes)
Learning Process Activity 1: Lecture Contents:
· Definition of vulnerable groups · Identification of correct messages for different target
audience and dissemination · Enabling mechanisms for preparedness response and
recovery · Identification and networking with local NGOs and leaders of
migrants/workers and others. Activity 2: Sharing the experiences / country’s experiences & lesson learnt
1. Participant sharing experience & lesson learnt · Q & A
OR (for country’s experiences)
2. Invite spokesperson from the chosen country & sharing experiences
· Q & A
52
Teaching Aids Computer LCD Power point presentation
Duration
1 hour 10 minutes Assessment Method
Feedback on presentation Q & A
Resources
1. Manpower - the field experts. 2. Please refer to Annex 3
53
UNIT 4: Collaborate with international organisations and neighbouring countries, including cross border issues
Learning Objective 1 At end of the session, participants will be able to:
1. Identify networking between international and neighbouring countries
2. Develop knowledge on maximising collaboration between international organisation and neighbouring countries, including cross border issues
Methodology
1. Lecture (40 minutes)
Learning Process
Activity 1: Lecture
Contents: · Orientation on existing protocol and mechanisms for sharing
information on public health emergencies. · Maximising web-based information dissemination to reach others. · Identify, developing and sharing messages
Teaching Aids
Computer LCD Power point presentation
Duration
40 minutes Assessment Method
Q & A Resources
1. Manpower - the field experts. 2. Please refer to Annex 4 and 5
54
LESSON PLAN
LEARNING OBJECTIVES
CONTENT METHOD RESOURCE DURATION
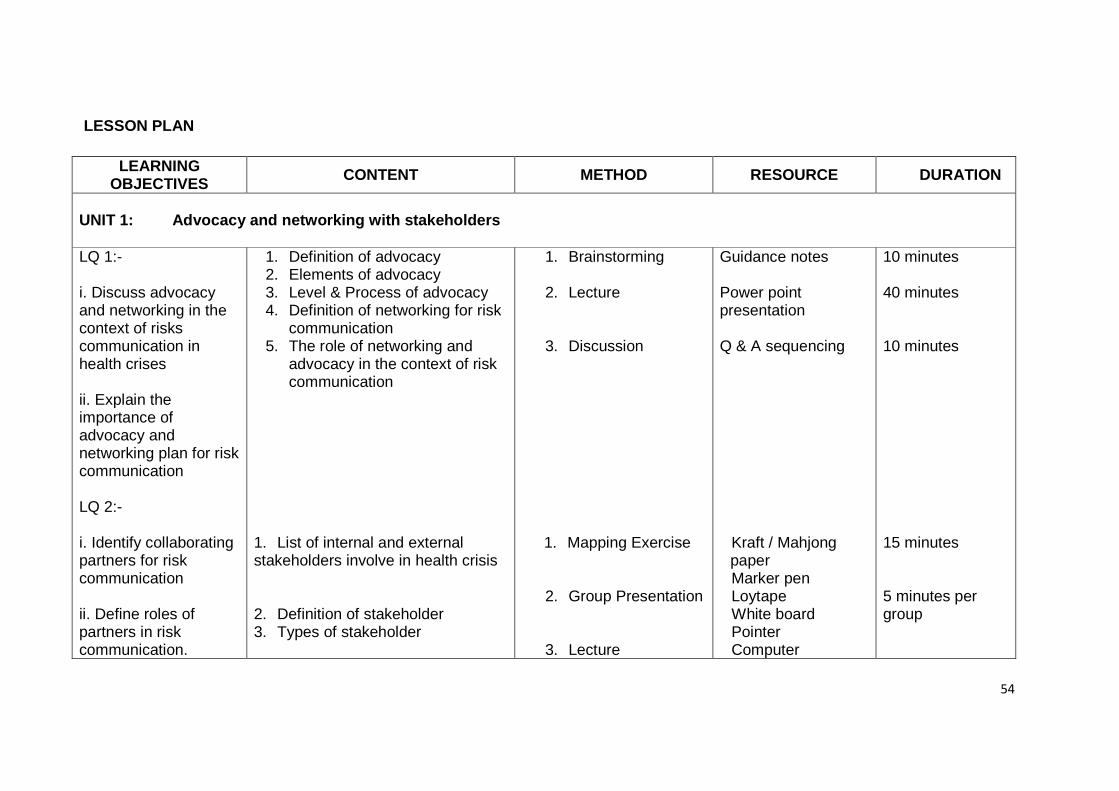
UNIT 1: Advocacy and networking with stakeholders LQ 1:- i. Discuss advocacy and networking in the context of risks communication in health crises ii. Explain the importance of advocacy and networking plan for risk communication LQ 2:- i. Identify collaborating partners for risk communication
ii. Define roles of partners in risk communication.
1. Definition of advocacy 2. Elements of advocacy 3. Level & Process of advocacy 4. Definition of networking for risk
communication 5. The role of networking and
advocacy in the context of risk communication
1. List of internal and external stakeholders involve in health crisis 2. Definition of stakeholder 3. Types of stakeholder
1. Brainstorming 2. Lecture
3. Discussion
1. Mapping Exercise
2. Group Presentation
3. Lecture
Guidance notes Power point presentation Q & A sequencing Kraft / Mahjong paper Marker pen Loytape White board Pointer Computer
10 minutes 40 minutes 10 minutes 15 minutes 5 minutes per group
55
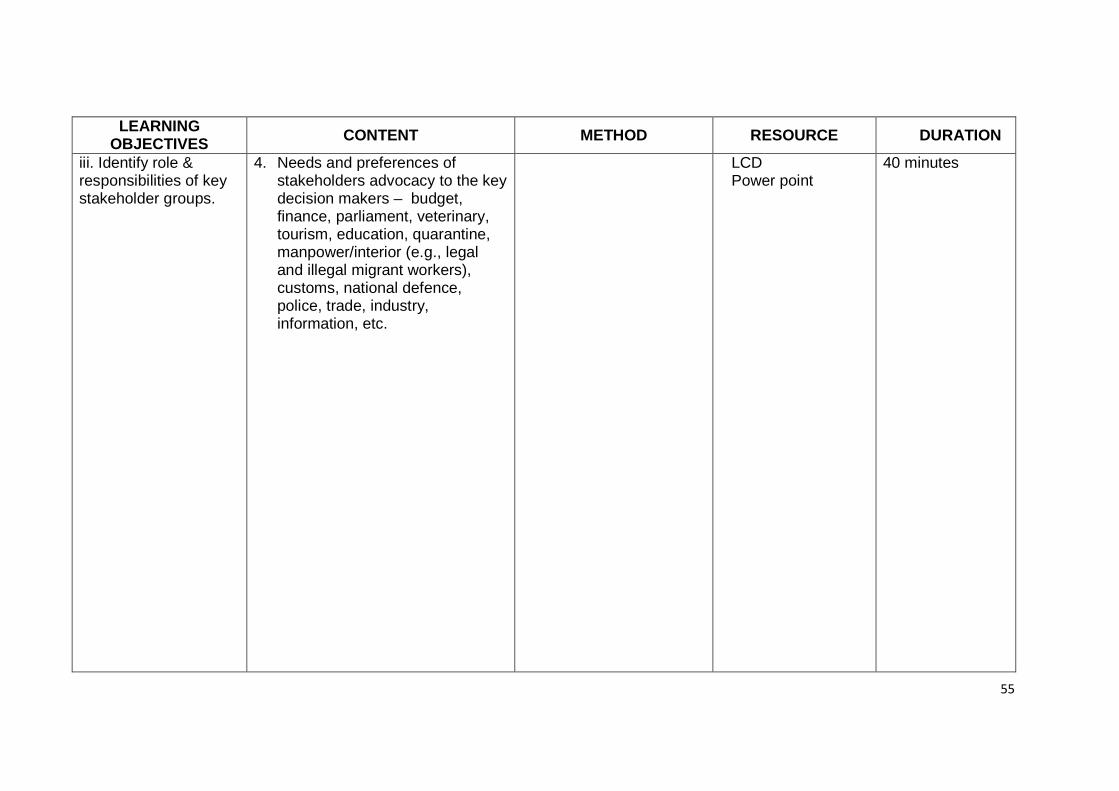
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
iii. Identify role & responsibilities of key stakeholder groups.
4. Needs and preferences of stakeholders advocacy to the key decision makers – budget, finance, parliament, veterinary, tourism, education, quarantine, manpower/interior (e.g., legal and illegal migrant workers), customs, national defence, police, trade, industry, information, etc.
LCD Power point
40 minutes
56
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
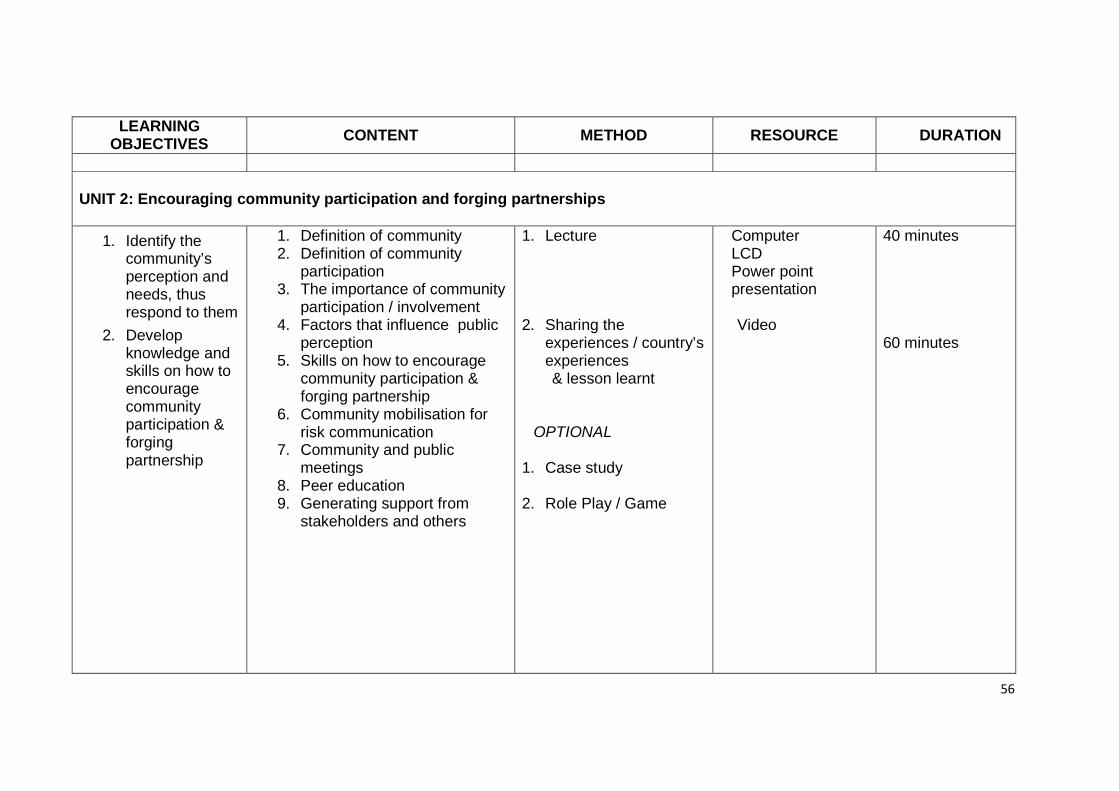
UNIT 2: Encouraging community participation and forging partnerships
1. Identify the community’s perception and needs, thus respond to them
2. Develop knowledge and skills on how to encourage community participation & forging partnership
1. Definition of community 2. Definition of community
participation 3. The importance of community
participation / involvement 4. Factors that influence public
perception 5. Skills on how to encourage
community participation & forging partnership
6. Community mobilisation for risk communication
7. Community and public meetings
8. Peer education 9. Generating support from
stakeholders and others
1. Lecture
2. Sharing the
experiences / country’s experiences
& lesson learnt
OPTIONAL 1. Case study
2. Role Play / Game
Computer LCD Power point presentation
Video
40 minutes 60 minutes
57
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
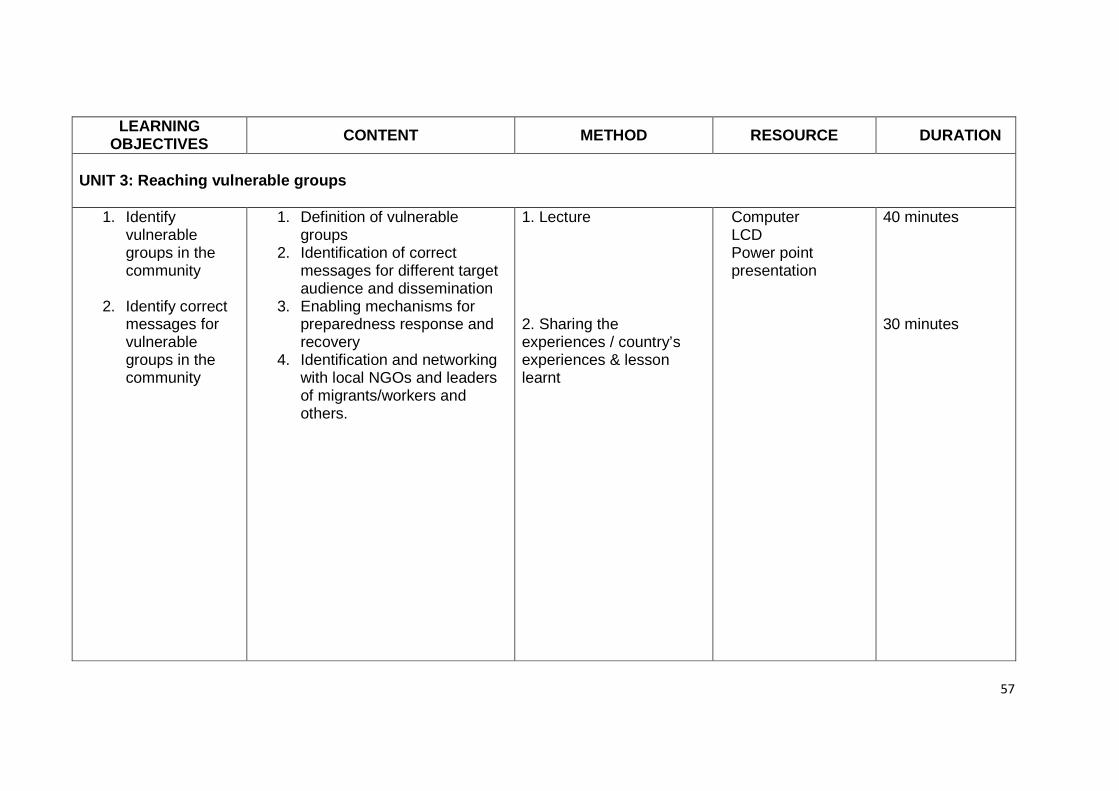
UNIT 3: Reaching vulnerable groups
1. Identify vulnerable groups in the community
2. Identify correct
messages for vulnerable groups in the community
1. Definition of vulnerable groups
2. Identification of correct messages for different target audience and dissemination
3. Enabling mechanisms for preparedness response and recovery
4. Identification and networking with local NGOs and leaders of migrants/workers and others.
1. Lecture 2. Sharing the experiences / country’s experiences & lesson learnt
Computer LCD Power point presentation
40 minutes 30 minutes
58
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
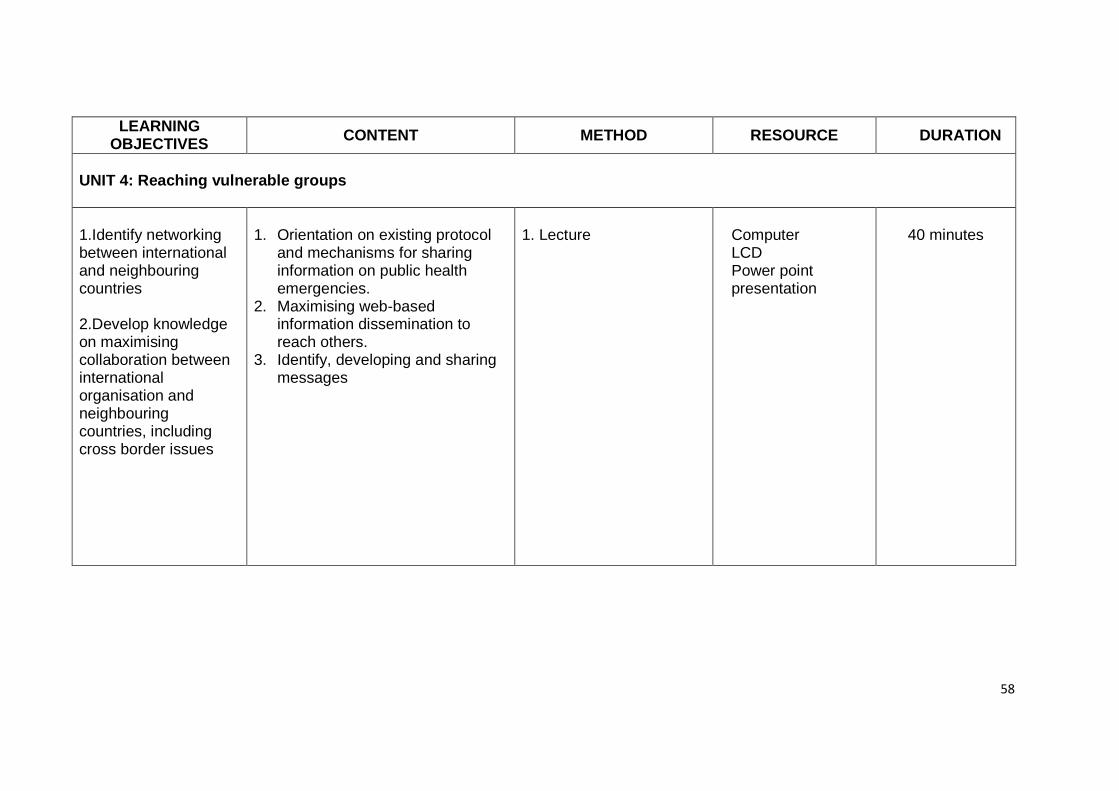
UNIT 4: Reaching vulnerable groups 1.Identify networking between international and neighbouring countries
2.Develop knowledge on maximising collaboration between international organisation and neighbouring countries, including cross border issues
1. Orientation on existing protocol
and mechanisms for sharing information on public health emergencies.
2. Maximising web-based information dissemination to reach others.
3. Identify, developing and sharing messages
1. Lecture
Computer LCD Power point presentation
40 minutes
59
MODULE 3: COMMUNICATING HEALTH RISK
1. Introduction
The right message at the right time is a resource multiplier which is needed to assist response officials to get their job done. Many of the predictable harmful individuals and community behaviours can be mitigated with effective crisis and emergency communication. Officials need to anticipate what mental stresses the population will be experiencing and apply appropriate communication strategies to attempt to manage these stresses in the population. Hence, officials managing crisis situation need to be equipped with appropriate risk communication tools.
2. Purpose
The purpose of this module is to enable the participants to develop skills essential for communicating health risk.
3. Module Objective
To equip participants with relevant knowledge and skills for effective risk communication
4. Module Contents
UNIT 1 - Identification and understanding the audience
UNIT 2 - Message development
UNIT 3 - Basic skills of media spokespersons
UNIT 4 - Media Management and Engagement
60
UNIT 1 - Identification And Understanding The Audience
1. Define the audience 2. Analyze the audience 3. Carry out audience segmentation
Duration
1 hour UNIT 2 - Message Development
1. Discuss factors that help determine audience acceptance of messages.
2. Identify and apply the steps in developing messages Duration
2 hours UNIT 3 - Basic Skills Of Media Spokesperson
1. Identify principles of a good spokesperson 2. Identify the Skills and requirement for effective communication
Duration
1 hour UNIT 4 - Media Menagement And Engagement
1. Describe how media people work. 2. Identify the media needs 3. Describe process of handling media 4. Develop skills in preparing materials for media 5. Discuss preparation to meet the media
Duration
3 hours
61
5. Instructional Guide UNIT 1: Identification And Understanding The Audience
Learning Objectives At end of the session, participants will be able to:
1. Define the audience 2. Analyze the audience 3. Carry out audience segmentation
Methodology
1. Brainstorming (10 minutes) 2. Lecture (20 minutes) 3. Discussion (30 minutes)
Learning Process
Activity 1: Brainstorming 1. Break into groups. 2. Each group list down on how to carry out audience
segmentation. 3. Present to the group in power point or flip chart.
Activity 2: Lecture Content: 1. Define audience Analysis 2. Identify the purpose of Audience Analysis 3. Describe the steps in Audience Analysis 4. Explain Audience Segmentation 5. Enumeration the classification of Audience
Activity 3: Group Discussion
1. Break into groups. 2. Do exercise 1 & 2

62
3. Present to the group in power point or flip chart.
Resource
Please refer to Annex 6
Teaching Aids
Computer with Microsoft Power point presentation LCD Checklist
Duration
1 hour
Assessment Method
Q & A
63
UNIT 2 - MESSAGE DEVELOPMENT
Learning Objectives
At end of the session, participants will be able to:
1. Identify factors determining audience acceptability of health messages
2. Identify and apply the steps in developing messages 3. State the steps in developing messages (using message
mapping as tool) Methodology
1. Lecture (30 minutes) 2. Brainstorming (30 minutes) 3. Discussion (1 hr)
Learning Process
Activity 1: Lecture Content: 1. Factors determining audience acceptability of health messages 2. Identify and apply the steps in developing messages 3. State the steps in developing messages (using message
mapping as a tool) Activity 2: Brainstorming (refer to exercise 3 in Appendix 5.3 )
1. Break into groups.
2. Each group list out;
a. The factors determining audience acceptability of health messages.
b. State the steps in developing messages (using message mapping as a tool)
3. Present to the group in power point or flip chart.
64
Activity 3: Group discussion (refer to exercise 4 in Appendix 5.4)
1. Break into groups.
2. Do exercise 4
3. Present to the group in power point or flip chart.
Resource
Please refer to Annex 7 Teaching Aids
Computer with Microsoft Power point presentation LCD Checklist
Duration
2 hrs Assessment Method
Q & A
65
UNIT 3 - BASIC SKILLS OF MEDIA SPOKESPERSONS
Learning Objectives
At end of the session, participants will be able to: 1. Identify principles of a good spokesperson 2. Identify the skills and requirement for effective communication
Methodology
1. Discussion (60 minutes) Learning Process Activity 1: Group discussion
1. Break into groups. 2. Do exercise 5 3. Present to the group in power point or flip chart.
Resources
Please refer to Annex 8 Teaching Aids
Computer with Power point LCD Checklist
Duration
1 hr Assessment Method
Q & A
66
UNIT 4 – MEDIA MENAGEMENT AND ENGAGEMENT
Learning Objectives At end of the session, participants will be able to:
1. Describe how media people work. 2. Identify the media needs 3. Describe process of handling media 4. Demonstrate skills in preparing materials for media 5. Describe the steps to prepare to meet the media
Methodology
1. Brainstorming ( 1 hour) 2. Discussion ( 1 hour) 3. Lecture ( 45 minutes)
Learning Process
Activity 1: Brainstorming 1. Break into groups. 2. Each group list out;
a. The needs of the media. b. Describe the process of handling media.
Activity 2: Group discussion
1. Break into groups. 2. Do exercise 6, 7 & 8 3. Present to the group in power point or flip chart.
67
Activity 3: Lecture
Content: 1. Explain the important of media in Risk communication- national
and local media 2. Describe preparing the media:
· Pre crisis (e.g. encouraging the media to write features story on EID, etc. · During crisis · After crisis
3. State how to deal with media · The dos and the don’ts · Empathy & caring · Competence & expertise · Honesty & openness · Commitment · Accountability · Good listener · Confidence · Humility
4. Describe Media monitoring 5. State Media Needs 6. Describe the processes involved in handling media
Resource
Please refer to Annex 9 Teaching Aids
Computer with Power point and design soft ware Flip chart Sample materials LCD
Duration
3 hrs Assessment Method
Q & A Peer Critics and feedback
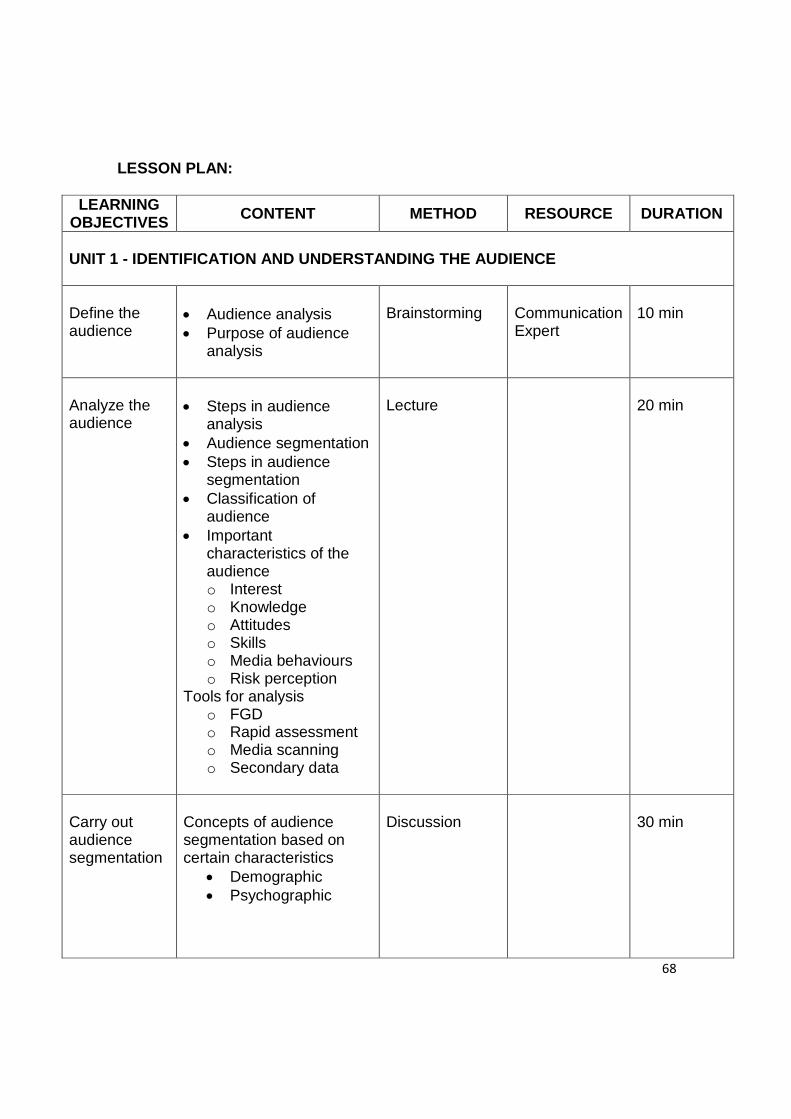
68
LESSON PLAN:
LEARNING OBJECTIVES
CONTENT METHOD RESOURCE DURATION
UNIT 1 - IDENTIFICATION AND UNDERSTANDING THE AUDIENCE Define the audience
· Audience analysis · Purpose of audience
analysis
Brainstorming
Communication Expert
10 min
Analyze the audience
· Steps in audience
analysis · Audience segmentation · Steps in audience
segmentation · Classification of
audience · Important
characteristics of the audience o Interest o Knowledge o Attitudes o Skills o Media behaviours o Risk perception
Tools for analysis o FGD o Rapid assessment o Media scanning o Secondary data
Lecture
20 min
Carry out audience segmentation
Concepts of audience segmentation based on certain characteristics
· Demographic · Psychographic
Discussion
30 min
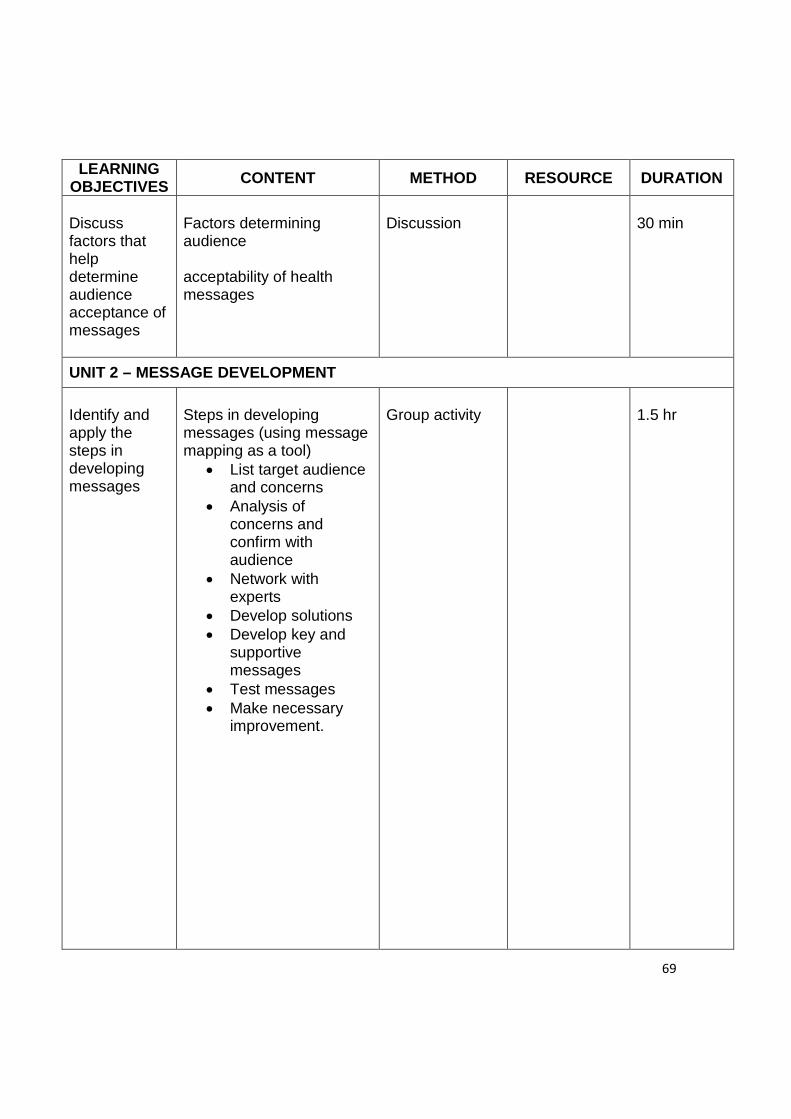
69
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
Discuss factors that help determine audience acceptance of messages
Factors determining audience acceptability of health messages
Discussion
30 min
UNIT 2 – MESSAGE DEVELOPMENT
Identify and apply the steps in developing messages
Steps in developing messages (using message mapping as a tool)
· List target audience and concerns
· Analysis of concerns and confirm with audience
· Network with experts
· Develop solutions · Develop key and
supportive messages
· Test messages · Make necessary
improvement.
Group activity
1.5 hr
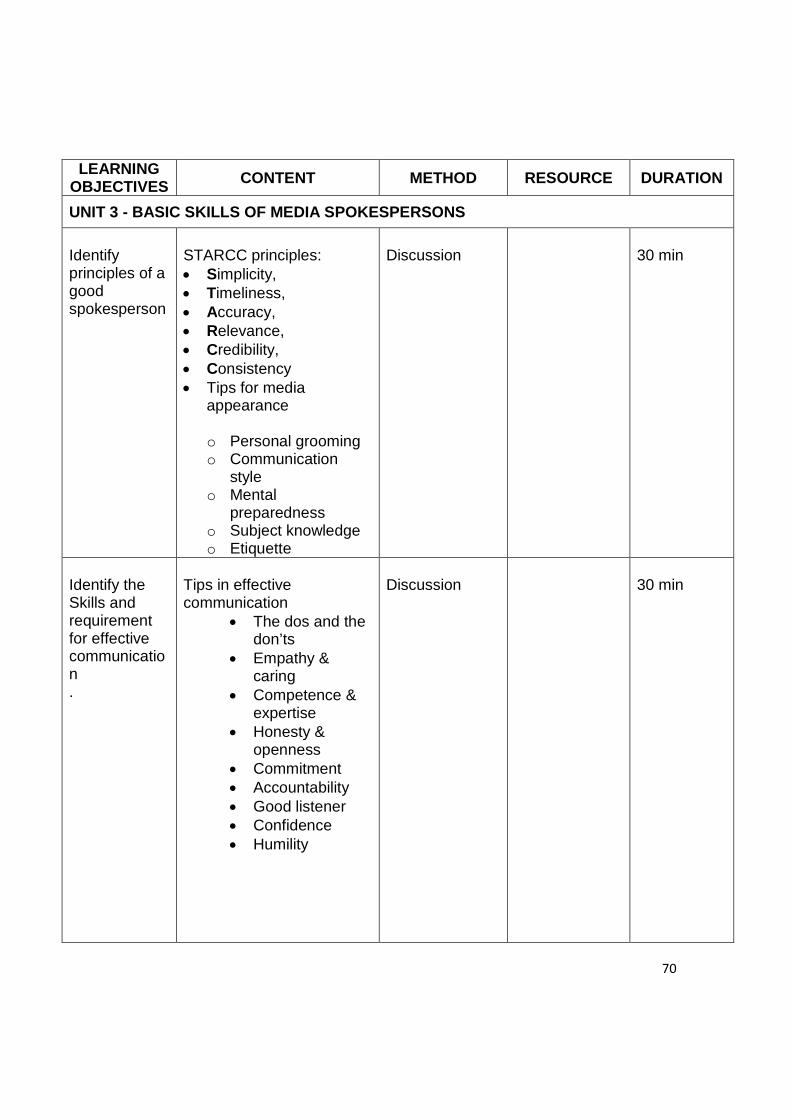
70
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
UNIT 3 - BASIC SKILLS OF MEDIA SPOKESPERSONS
Identify principles of a good spokesperson
STARCC principles: · Simplicity, · Timeliness, · Accuracy, · Relevance, · Credibility, · Consistency · Tips for media
appearance
o Personal grooming o Communication
style o Mental
preparedness o Subject knowledge o Etiquette
Discussion
30 min
Identify the Skills and requirement for effective communication .
Tips in effective communication
· The dos and the don’ts
· Empathy & caring
· Competence & expertise
· Honesty & openness
· Commitment · Accountability · Good listener · Confidence · Humility
Discussion
30 min
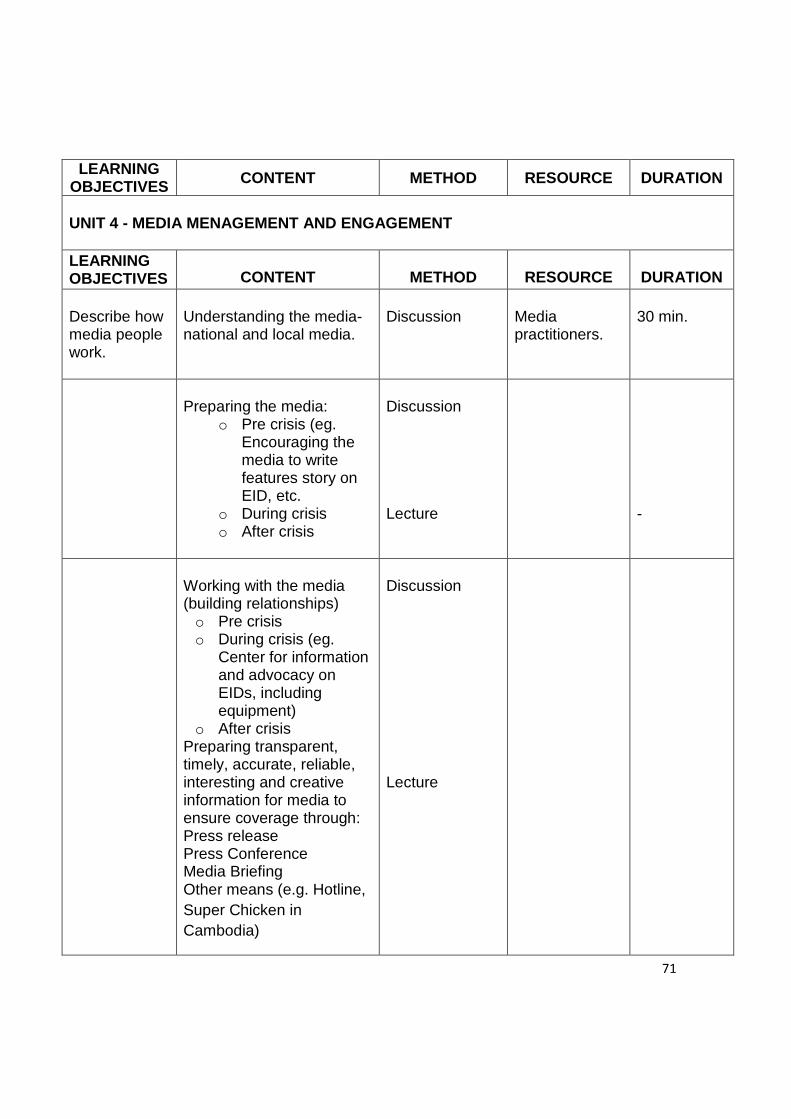
71
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
UNIT 4 - MEDIA MENAGEMENT AND ENGAGEMENT LEARNING OBJECTIVES
CONTENT
METHOD
RESOURCE
DURATION
Describe how media people work.
Understanding the media- national and local media.
Discussion
Media practitioners.
30 min.
Preparing the media:
o Pre crisis (eg. Encouraging the media to write features story on EID, etc.
o During crisis o After crisis
Discussion Lecture
-
Working with the media (building relationships) o Pre crisis o During crisis (eg.
Center for information and advocacy on EIDs, including equipment)
o After crisis Preparing transparent, timely, accurate, reliable, interesting and creative information for media to ensure coverage through: Press release Press Conference Media Briefing Other means (e.g. Hotline, Super Chicken in Cambodia)
Discussion Lecture
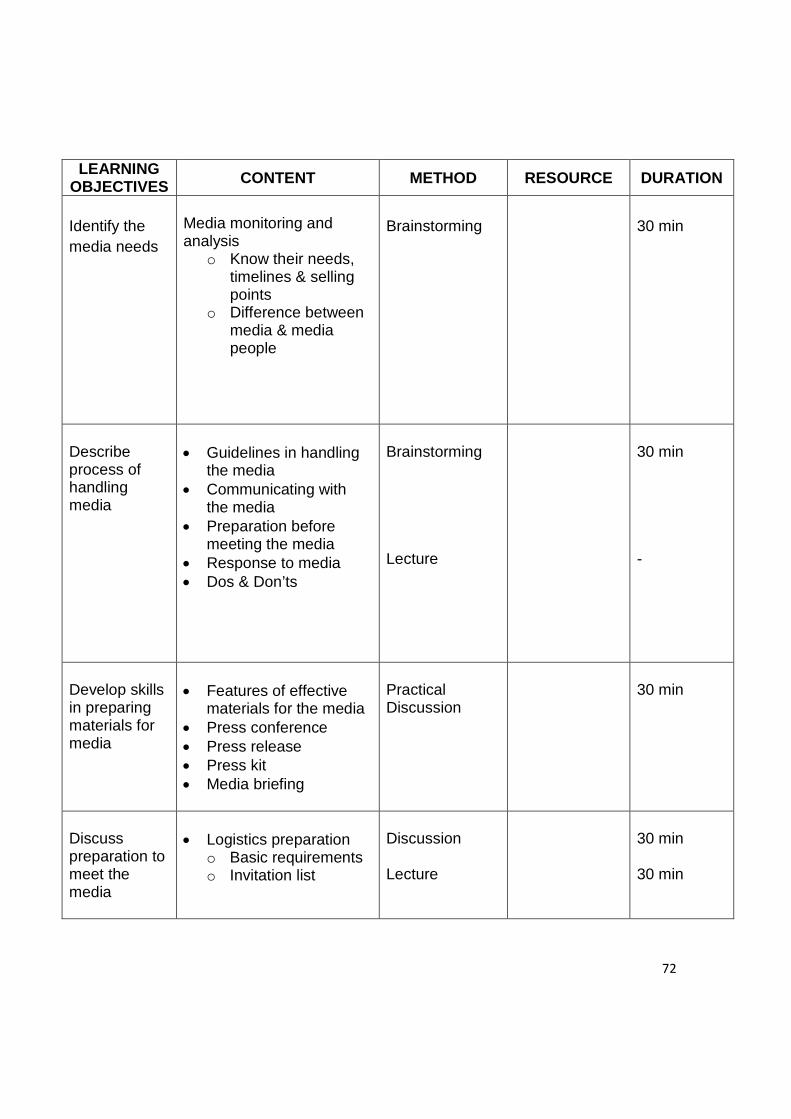
72
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
Identify the media needs
Media monitoring and analysis
o Know their needs, timelines & selling points
o Difference between media & media people
Brainstorming
30 min
Describe process of handling media
· Guidelines in handling
the media · Communicating with
the media · Preparation before
meeting the media · Response to media · Dos & Don’ts
Brainstorming Lecture
30 min -
Develop skills in preparing materials for media
· Features of effective
materials for the media · Press conference · Press release · Press kit · Media briefing
Practical Discussion
30 min
Discuss preparation to meet the media
· Logistics preparation
o Basic requirements o Invitation list
Discussion Lecture
30 min 30 min
73
MODULE 4: ETHICAL AND LEGAL IMPLICATIONS OF RISK COMMUNICATION
1. Introduction
It is important that the health staff be aware of the political, legal and ethical implications inherent to public health in handling risk communication in a health crisis situation. They should also be aware of the existing mechanisms for inter-sectoral collaboration, roles and responsibilities of key actors involved, and management of information with regard to risk communication during a health crisis. This module therefore addresses the political legal and ethical considerations in risk communication. In terms of the mechanism the personnel involved are identified and how information is managed during a crisis is also dealt with. This is appropriate during every level of the crisis that is pre, during, and post crisis. The areas discussed are also applicable at the national, state and ground levels. The key personnel trained need to have a good understanding of the various elements discussed so that the rights, dignity and honour of the target group is not compromised. They need to know the existing mechanism and their role in it so that can participate effectively in bringing the crisis to a quick end.
2. Purpose
The participants should know how to use the existing laws to assist in their handling of the crisis. At the same time they need to be aware of the limitations within the laws, so that individual rights are not compromised. It is essential that the trainee-participants realize at the end of the module, that the core principals of ethics must always be upheld within the context and requirements of the law.
3. Objective
3.1 General Objective
To expose participants to the ethical and legal implications of risk communication.
3.2 Specific Objectives
3.2.1 Participants to familiarize themselves with political, ethical and
legal considerations and principles for a pre-crisis/crisis situation
74
3.2.2 Participants to apply political, ethical and legal considerations and principles in a crisis situation
4. Contents of Module 4
UNIT 1: Ethical Implication In Risk Communication
a) Definition and principles of political, ethical and legal issues b) Application of the ethical principles in a crisis situation c) Public’s right to know about information d) Ethical Dilemmas due to legal constraints e) Consequences of breaches of ethics f) Issues related to human rights and liberty g) Issues related to animal welfare h) Perceptions about ethics in different societies i) Importance of transparency and early announcement
UNIT 2: Legal Implication Of Risk Communication
a) What are the relevant laws? b) Enactment of new laws to new situations (emerging
diseases) c) Understanding of various existing regulations at the national
and international levels, provisions under the various enactments that empower the officer-in-charge to handle the crisis, legal instruments which enable enforcement, International convention: IHR 2005 dealing with Public Health Emergencies of International Concern
d) Possible breaches of the law e) Consequences and dilemma of disclosure and non-
disclosure of information f) Legal implications for false media reporting and
sensationalism
UNIT 3: Politics In Risk Communication
a) Information disclosure and/or non-disclosure with political consideration
b) How to deal with political interference c) Advocating (educating) to politicians d) Seeking political support for community actions and
behaviour change
75
e) International relations, i.e. information sharing with neighbours, border committee and international organizations
f) Engaging the politicians.
5. Instructional Guide
UNITS 1-3: Political, Ethical And Legal Issues In The Pre-Crisis/Crisis Situation
Learning Objectives:
At end of the session, participants will be able to:
a) Familiarize themselves with political, ethical and legal considerations and principles for a pre-crisis/crisis situation.
b) Apply political, ethical and legal considerations and principles in a crisis situation.
Methodology
a) Brainstorming/Discussion ( 30 minutes) b) Lecture ( 45 minutes) c) Case illustration/studies ( 30 minutes) d) Debate ( 30 minutes, optional) e) Workshop ( 30 minutes)
Learning Process
Activity 1: Brainstorming/ Discussion
Brain storming/discussion session among participants in order to understand the principles of ethics and the law in the pre-crisis/crisis situation in the context of risk communication in health crisis.
Activity 2: Lecture
Content: a) Principles of law b) Application of law and conflicting rules c) Ethical principles d) Application of the ethical principles in a crisis
situation
76
Activity 3: Case Illustration/studies
a) The ‘law’ facilitator is to discuss relevant court decisions in workshop/discussion.
b) The “ethics” facilitator will discuss consequences of breaches of ethics based on past crisis and scenarios
c) The “politics” facilitator will discuss pointers on how to engage with politicians to get their support and also overcome political interference based on previous experiences and scenarios too.
Activity 4: Debate (optional)
Participants will present opposing views on issues and dilemmas that are likely to arise or has arisen in the past crisis but focused on risk communication.
Activity 5: Workshop
a) Break into groups. b) Each group list down on how the participants actively
formulate response to the ethical and legal issues with created scenarios.
c) Present to the group in power point based on their own scenarios.
Teaching Aids
a) Computer b) LCD c) Power point presentation d) Handouts
Duration
4 hrs
Assessment Method
Pre and post test
Resource
Please refer to Annex 10
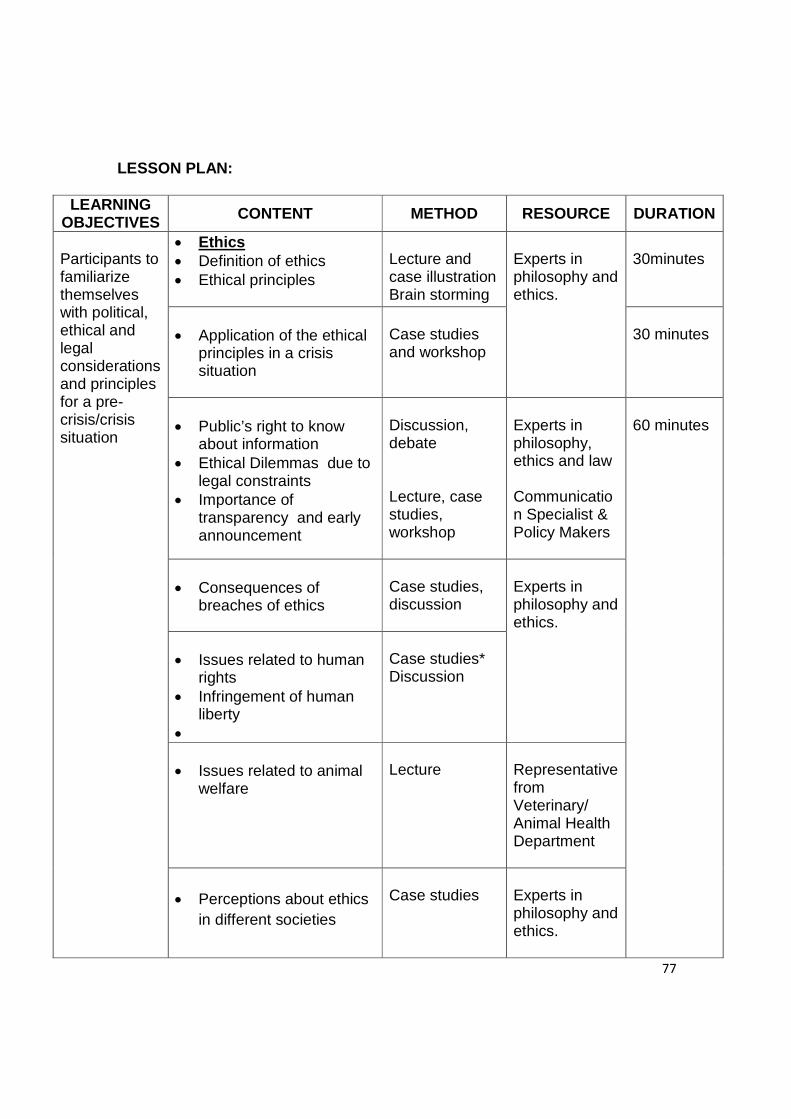
77
LESSON PLAN:
LEARNING OBJECTIVES
CONTENT METHOD RESOURCE DURATION
Participants to familiarize themselves with political, ethical and legal considerations and principles for a pre-crisis/crisis situation
· Ethics · Definition of ethics · Ethical principles
Lecture and case illustration Brain storming
Experts in philosophy and ethics.
30minutes
· Application of the ethical
principles in a crisis situation
Case studies and workshop
30 minutes
· Public’s right to know
about information · Ethical Dilemmas due to
legal constraints · Importance of
transparency and early announcement
Discussion, debate Lecture, case studies, workshop
Experts in philosophy, ethics and law Communication Specialist & Policy Makers
60 minutes
· Consequences of
breaches of ethics
Case studies, discussion
Experts in philosophy and ethics.
· Issues related to human
rights · Infringement of human
liberty ·
Case studies* Discussion
· Issues related to animal
welfare
Lecture
Representative from Veterinary/ Animal Health Department
· Perceptions about ethics
in different societies
Case studies
Experts in philosophy and ethics.
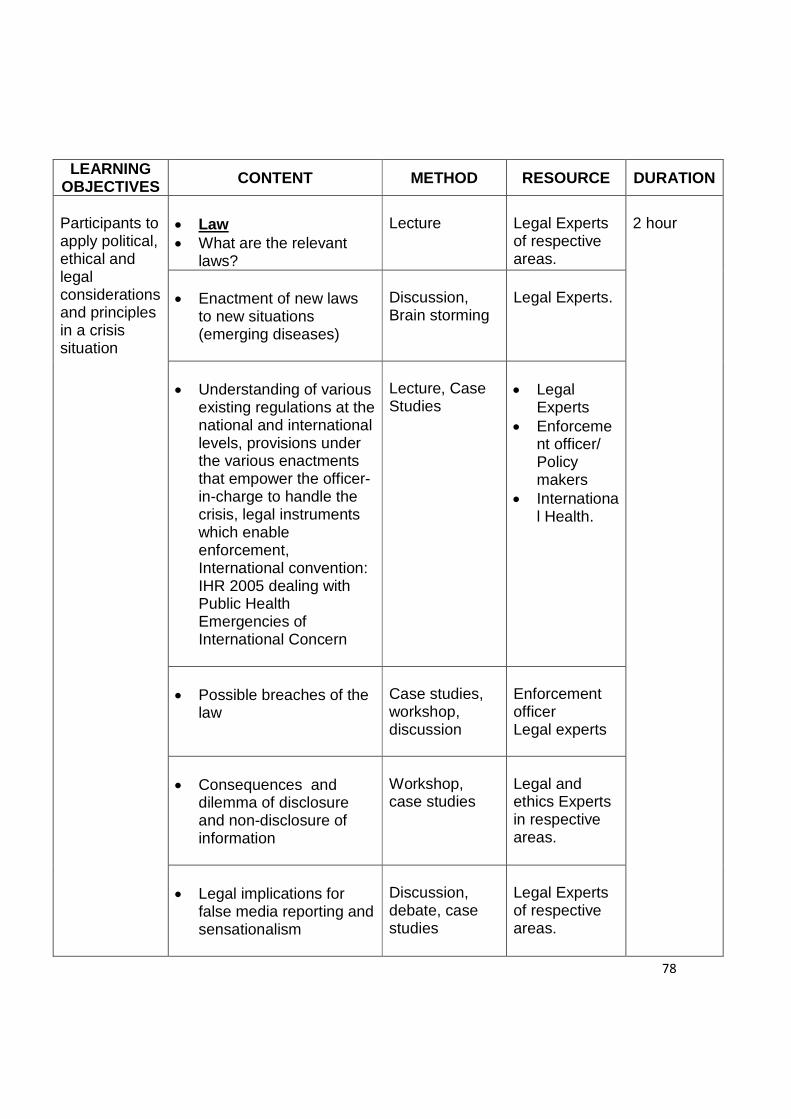
78
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
Participants to apply political, ethical and legal considerations and principles in a crisis situation
· Law · What are the relevant
laws?
Lecture
Legal Experts of respective areas.
2 hour
· Enactment of new laws
to new situations (emerging diseases)
Discussion, Brain storming
Legal Experts.
· Understanding of various
existing regulations at the national and international levels, provisions under the various enactments that empower the officer-in-charge to handle the crisis, legal instruments which enable enforcement, International convention: IHR 2005 dealing with Public Health Emergencies of International Concern
Lecture, Case Studies
· Legal
Experts · Enforceme
nt officer/ Policy makers
· International Health.
· Possible breaches of the
law
Case studies, workshop, discussion
Enforcement officer Legal experts
· Consequences and
dilemma of disclosure and non-disclosure of information
Workshop, case studies
Legal and ethics Experts in respective areas.
· Legal implications for
false media reporting and sensationalism
Discussion, debate, case studies
Legal Experts of respective areas.
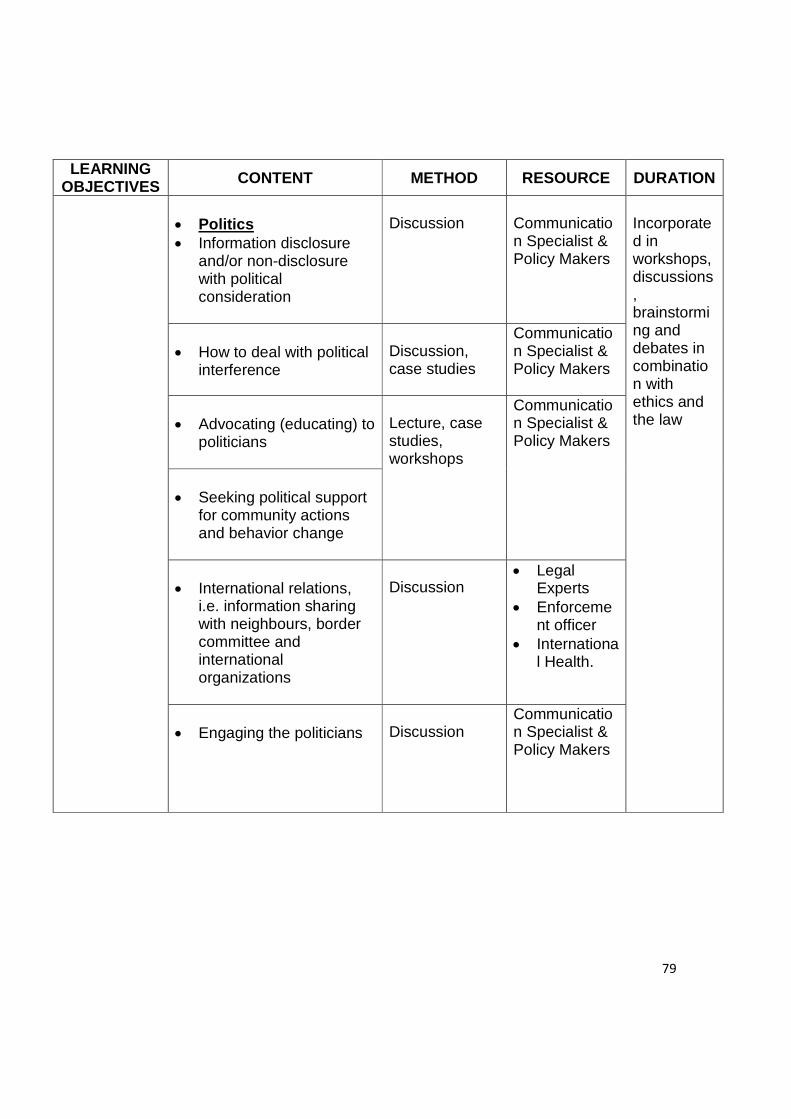
79
LEARNING OBJECTIVES CONTENT METHOD RESOURCE DURATION
· Politics · Information disclosure
and/or non-disclosure with political consideration
Discussion
Communication Specialist & Policy Makers
Incorporated in workshops, discussions, brainstorming and debates in combination with ethics and the law
· How to deal with political
interference
Discussion, case studies
Communication Specialist & Policy Makers
· Advocating (educating) to
politicians
Lecture, case studies, workshops
Communication Specialist & Policy Makers
· Seeking political support
for community actions and behavior change
· International relations, i.e. information sharing with neighbours, border committee and international organizations
Discussion
· Legal Experts
· Enforcement officer
· International Health.
· Engaging the politicians
Discussion
Communication Specialist & Policy Makers
80
Annexes
81
Annex 1
Notes on Advocacy with government stakeholders 1.1 Definition of advocacy
Advocacy is defined as an act or process to demand, defend and maintaining a cause. It involves trying to get others to support the cause so it also entails speaking up, drawing attention to the issue and directing decision makers towards a solution. The ultimate goal of advocacy is social change form of, among others, behaviour modification, policy or legislative acts, etc (Regional training course on risk communication in health emergencies).
Advocacy occurs when a person in authority or an agency in position of influence represents the interests on behalf of an individual, group or community in order to change or improve their situation (Tabbot & Verrinder, 2005).
• An advocate is a person who speaks up for and defends the rights of
him or herself or of another person
• A self-advocate is a person who speaks up for him/herself and defends his/her own rights.
Why Advocate? § Mobilise resources
- Advocacy usually argues for a different distribution of funds to what is currently in place during crisis
§ Change opinions
- Advocacy may involve persuading those in decision making positions to see an alternative perspective during a crisis
§ Catalyse change
- Sometimes individuals or agencies may wish to change their perspective or approach , but need guidance to commence or to implement new policies that are appropriate to another worldview
§ Cause action - Advocates can act as mentors to guide implementation of
different strategies.
82
1.2 Elements of advocacy
The essential elements in advocacy are basically the same elements of risk communication.
1.3 Types of advocacy
• Ideological advocacy: in this approach, groups fight, sometimes during protests, to advance their ideas in the decision-making circles.
• Interest-group advocacy: lobbying is the main tool used by interests
groups doing mass advocacy. It is a form of action that does not always succeed at influencing political decision-makers as it requires resources and organisation to be effective.
• Mass advocacy: is any type of action taken by large groups
(petitions, demonstrations, etc.). • Media advocacy: is “the strategic use of the mass media as a
resource to advance a social or public policy initiative” (Jernigan and Wright, 1996).
• Bureaucratic advocacy: people considered “experts” have more
chance to succeed at presenting their issues to decision-makers. They use bureaucratic advocacy to influence the agenda, however at a slower pace.
• Legislative advocacy: legislative advocacy is the “reliance on the
state or federal legislative process” as part of a strategy to create change (Loue, Lloyd and O’Shea, 2003).
• Budget advocacy: Budget advocacy is another aspect of advocacy
that ensures proactive engagement of Civil Society Organizations with the government budget to make the government more accountable to the people and promote transparency. Budget advocacy also enables citizens and social action groups to compel the government to be more alert to the needs and aspirations of people in general and the deprived sections of the community.
• Health advocacy: Health advocacy supports and promotes patient's
health care rights as well as enhance community health and policy initiatives that focus on the availability, safety and quality of care.
83
1.4 Definition of stakeholders
Stakeholders are people or organizations with a special connection to you and your involvement in the emergency. Anticipate and assess the incident from the stakeholders’ perspective (CDC, 2002).
1.5 Identify key stakeholders
In crisis communicating planning, the first step in responding to stakeholders is to identify them (CDC, 2002).
· Who are the internal and external stakeholders · What are their needs and preferences
1.6 Networking for risk communication
Focusing on the structure of relationship between people from various stakeholders including primary, secondary and tertiary audience and mobilizing the skills and resources that are already available both in disaster areas and non-disaster areas.
1.7 The role of networking and advocacy in the context of risk
communication The rule of networking and advocacy in risk communication is presented in the figure.
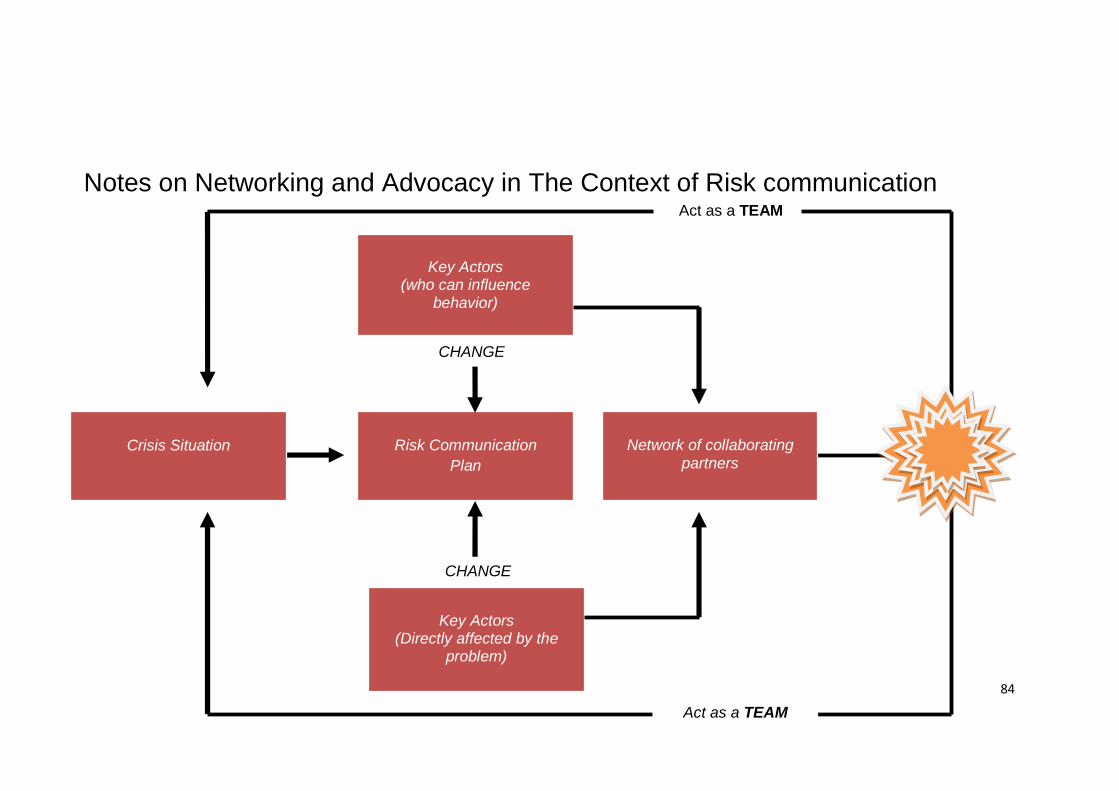
84
Notes on Networking and Advocacy in The Context of Risk communication Act as a TEAM
CHANGE
CHANGE
Crisis Situation
Key Actors (who can influence
behavior)
Risk Communication Plan
Key Actors (Directly affected by the
problem)
Network of collaborating partners
Act as a TEAM
85
Annex 2 Notes on Encouraging community participation and forging Partnerships
2.1 Definition of community & community participation
Community defined as a group of individuals who regardless of the diversity of their backgrounds or society as a group of people with common characteristics, identity and belonging and culture. Active community participation is a key to building an empowered community. Monitoring of target participation is essential for programs wherein acceptance and participation are voluntary. Any intervention or treatment that requires the target population to change their habit/behaviour, learn new skills, procedure, or take instructions may encounter difficulty in attracting target groups. Monitoring is needed to verify whether a program of such nature is reaching individuals with specified and appropriate characteristics for which the program was designed. The issue encountered in soliciting of target participation is often overlooked by planners during the development phase of the program. It is assumed that targets are motivated to participate.
2.2 Community mobilisation for risk communication
· Community and public meetings and briefings
Identify and establish networking between community leaders, local committee, religious leaders, community representative (e.g women, youth, and senior citizens), political wings, etc. A public meeting is a large meeting open to the public, where experts present information and answer questions, and community members ask questions and offer comments.
2.3 Arranging a public meeting
§ Create an agenda. Involve citizens in developing the agenda.
§ Hold the meeting in a public, comfortable setting that is easily accessible, well lit, and has adequate parking and seating, especially for persons with disabilities.
§ Be sensitive to special needs of community members. Consider translations for non-English speakers or sign language for hearing-impaired participants.
86
§ Announce the meeting in local media 2 weeks in advance if possible. Distribute flyers to community members and groups interested in attending. Clarify that the meeting is not a formal public hearing, but rather, a place to exchange information and comments.
2.4 Community – level education
Education at the level of the community or population is a more complex process than education at the individual, group or organisational level-even more planning and teamwork is needed if it is to be successful. (Tablot & verrinder, 2005). The World Health organization (1988 p.175) suggests three points: a) Get the support of influential people in the community-those who are
called “opinion leaders” or key people”. b) Be sure that all the people of the community are informed about the
problem and are kept up to date on plans and progress. All available channels of communication should be used for this purpose.
c) Get the maximum number of people involved so that the community will
really strengthen its capacity to do things for its health. This can be done through community health committees, advisory or planning boards, etc
2.5 Peer self-help groups
Peer self-help groups may work for social change or for personal change in their members, or a combination of both. Their roles include “mutual support”, education, advocacy, lobbying, research and information and service provision to both their members and other consumers of the health system (Markos 1991, p4).
Mutual support is given to group members with similar problems of a personal nature that affect them directly. The members share experiences and identify common needs and areas for social action for themselves or on behalf of others in similar situations (Tabbot & Verrinder, 2005).
2.6 Generating support from stakeholders and others.
2.7 Community social responsibility programmes (CSR).
87
Annex 3 Notes on Reaching Vulnerable Group
3.1 Identification of vulnerable groups and their information needs Vulnerable groups are population with special needs, including individuals
who have disabilities, medical disorders, specific dependencies, are institutionalized, senior citizens, are from diverse cultures and have limited language proficiency.
Vulnerable group are often not able to access and use the standard resources
in crisis preparedness, response and recovery. e.g: migrant workers and indigenous groups, children, pregnant mothers, senior citizens, children etc)
Information needs § It is critical that public health emergency risk communication is non-
discriminatory (2) and that all individuals have equal and ample access to information about the nature of the emergency/crisis, comprehensive emergency/crisis preparedness plans, response and recovery guidelines will include provisions for how best to inform and educate vulnerable group.
3.2 Identification of correct messages for different target audience and
dissemination
Effective risk communication can promote trust, awareness and motivation to act among the vulnerable group.
The message dissemination § Two way communication and interactive § Messages should be locally and personally relevant to the vulnerable
group § Avoid technical jargons § Precise and easy understanding to specific groups § Appropriate Language for each specific groups
Medium of dissemination § Appropriate medium and format for dissemination of information e.g
senior citizens may have difficulties with mobility, could have hearing limitations and visual impairments) in multiple formats (e.g television, print (verbal, pictorial), audio, internet, interpersonal)
88
§ Offer frequent communication in multiple modes :
o Messages shall be provide early and often o Messages shall be accessible and credible
Enabling mechanisms for preparedness response and recovery
· Prepare communication plans all phases of crisis. Pre-crisis, Initial, Maintenance, Resolution and evaluation for vulnerable group or incorporate with national/state communication plan for crisis.
· This is where all of the planning and most of work should be done to
enabling vulnerable group during health crisis. Reasonable questions can be anticipated pertaining issues on vulnerable group and preliminary answers sought. Spokespersons and resources, mechanisms can be identified. Training and refinements of plans and messages can be made. Vulnerable group alliances and partnerships can be fostered to ensure that experts are disseminating messages with one voice.
3.3 Identification and networking with local NGOs and leaders of migrants/workers and others.
· Identify the NGOs (local organization) and the organization objectives.
Prepare a list of local NGO’s and organizations representing vulnerable group and their objectives. Identify their expertise, manpower, resources to act during health crisis.
o Study the background of their manpower to solicit their
expertise in communication and information dissemination.
o Identify the employers of workers in risk
o Identify agency dealing migrant workers
89
Annex 4
Notes on Collaborate with international organisations and neighbouring countries, including cross border issues
4.1 Orientation on existing protocol and mechanisms for sharing
information on public health emergencies. The Protocol provides the basic guidelines to the ASEAN Countries towards institutionalizing a fully functional information sharing mechanism for issues related to prevention and control of emerging infectious diseases (EID).
§ ASEAN countries shall establish a common protocol for sharing information on public health emergencies with neighbouring countries, The protocol shall outline neighbouring technical support, provision of expertise , laboratory coordination and supplies and logistics
§ Develop a checklist for communication process with international
organisations and neighbouring countries
§ Identify the mechanisms for sharing information between neighbouring countries : e.g country’s crisis web site, cross boarder meetings, reports etc
The Communication and Information Sharing Protocol addresses five main questions:
§ What kind of information to share (content areas)
§ How should the information be shared (mechanism)
§ Who/what institution should ensure that information sharing happens (responsibility)
§ How often should information sharing occurs (regularity)
§ How should we disseminate and monitor compliance to the protocol (mainstreaming)
4.2 Maximising web-based information dissemination to reach others.
The web-based information has been demonstrated to be a successful communication tools in sharing information between neighbouring countries. Internet-based messaging is especially effective at overcoming communication barriers commonly encounters within neighbouring countries. Each ASEAN countries should; § Establish web site information
90
§ Update and enhance the current web site § The design shall be made user-friendly, and easily accessible.
4.3 Developing and sharing messages
The following areas need to be considered when developing and sharing messages:
§ Cultural and religious considerations. § Appropriate language with translation. § Customs regulations, international health regulation (quarantine),
livestock regulation, health policies, international security act, tourism regulations, etc.
91
Annex 5
Notes on Stakeholders To Consider
· Employees
· Families
· Retirees
· Board members
· External advisors
· Your organizations’ clients/consumers
· Local residents
· Business and community leaders
· Elected officials
· Consumer action groups
· Union or labor organizations
· Competitors
· Legal advocates
· Media
· Public
· Others
Consider plans to provide advance notice to important audiences. Prioritize stakeholders according to the type of emergency.
5.1 Partnership Development
A partner may be defined as anyone with a role in aiding in the response. Partner relationships should be developed in advance of the crisis. One of the best methods of building partnerships is to start building relationships informally through community and social networks. Strong, collegial relationships can be very helpful when emergency coordination is required. Partnerships should be based on the partners’ common purpose of serving the community.
92
Each potential partner should play a specific role during a crisis, and this role should be determined and agreed upon before a crisis situation occurs (or at the very least, in the first few hours of a crisis event). It is helpful to assess what each partner brings to the table, including strengths, weaknesses, and unique abilities.
The partner organization will most likely choose its representative. That representative should be someone who will be able to execute the partner’s role and has the organization’s authority to make decisions and speak on its behalf. Usually this person is not the head of the organization, but typically will keep the leader of the organization informed.
Tips for developing partnerships:
§ Design a plan for building relationships before the crisis.
§ Create a partner contact sheet with every available phone number and e-mail address (e.g., work, home, cell, etc.), Obtain permission to contact the people by any means necessary in an emergency.
§ Draft a plan for partner communication during a crisis (e.g., e-mail alerts, twice-daily faxes, conference calls) to which everyone agrees.
Reality Check: Despite every good intention to allow partners a preview of a press statement or release, it may be impossible to do so. With some time sensitive issues, you may have to consider the increased risk of leaks and choose not to share. If possible, consider telling partners to expect a release on a subject or ensure that they get the release and any supporting documents at the same time as the media.
5.2 Community relations
Research indicates that community leaders and institutions (e.g., schools, employers, community organizations, churches/religious institutions, and major employers) can be valuable partners in gaining support for public health actions, distributing information, or countering rumors surrounding an emergency event. These partners may be familiar, trusted, and influential with your target audience, and may be more likely than media alone to motivate the public to take recommended actions. Also, the partners can reach groups of people in a familiar setting.
In pre-event planning, make an effort to reach out to these groups. Consider memoranda of understanding with partners to engage them as information disseminators during a public health emergency. Consider supplying them with background information before or soon after an emergency occurs. Develop fast and reliable channels of communication directly to these community leaders so that they will have the facts when their constituencies begin to ask questions. Invite them to tour emergency facilities. Brief them on
93
such issues as the national pharmaceutical stockpile or public health emergency laws.
5.3 Strategies to navigate a process for consensus building
Don’t leave it to the media to negotiate public controversies during an emergency response effort. Instead, consider engaging a neutral party to speak for the diverse group of stakeholders to help resolve differences. The neutral party can speak to the media on behalf of all involved or facilitate a face-to-face meeting. The neutral party can express both consistent and inconsistent points of view from the entire group in an effort to find consensus.
5.4 Convening a citizens’ forum
A professional facilitator, comfortable with the culture of the community, who is perceived by all sides as neutral, should convene the public forum. Conduct a needs assessment to determine the stakeholders in this issue. Representatives from all elements of the community must be considered, not just those from a vocal advocacy group.
5.5 Empower group decision making with the following steps:
· Identify the options and discuss the pros and cons of each alternative.
· Analyze the costs and benefits, weaknesses and strengths of each.
· Present all known scientific or technical information about the alternatives.
· Choose the “must” versus “want” criteria for the decision.
· Be able to express why one alternative was chosen over the others (e.g., the highest number of people will be helped with a minimum disruption to self-reliance and community sovereignty).
· Reach a clear, justifiable decision.
5.6 Quality listening
Asking questions shows that you care. The first step in solving problems is to know what’s really going on. Questions can do that. Good listeners are perceived as more intelligent. Listening actively reduces mistakes—like believing you understand what is being asked of you, only to discover later that you are mistaken.
· Listen for intent (feeling).
· Listen for content (facts).
94
· Listen for who is speaking.
o Is this person qualified to give expert opinions on this subject?
o Does this person have underlying motives?
o Does this person have prejudices or beliefs that will compromise objectivity?
5.7 Dealing with an angry public
When risks are uncertain, because science has not reached an answer or a consensus answer, controversies will arise. Add the need to make decisions under the enormous time pressure of a crisis, and the uncertainty may seem unbearable to both response officials and the public. When science cannot lead to a clear path, decision-makers must make choices about what is and is not acceptable. In non-pressure environments, the public may turn to the courts to settle differences about the amount of acceptable or perceived risk.
In a crisis, as in the emergency room, where imperfect decisions must be made in minutes, not months, the fallout can be incredibly harsh, especially after the crisis is resolved and the decisions are reviewed with the omniscient power of hindsight. With the strongly held sense of self-determination among Americans, the struggle of imposing some risk on individuals or suspending some civil liberties to protect communities may be great. Great, unless, even in the crisis situation, response officials make an effort to empower the public.
At the community level, that may mean a face-to-face meeting. Involving stakeholders and building consensus is the most powerful way to advance compliance with public safety requirements before and during an emergency. Anything less will invite civil unrest and greater mistrust of the institutions or government responding to the crisis. These public forums sooth tempers and help the community to work toward a mutually agreeable solution to the common problem.
Communication experts and psychologists agree that anger is a defensive response to pain or the threat of pain. Experts identify three basic circumstances where anger is likely to arise:
· When people have been hurt
· When they feel threatened by risks not of their own making
· When they believe that their fundamental beliefs are being challenged.
The intensity of that anger can be confounded by related factors. For example, when people feel weak in the face of others who are more powerful, their anger is increased. When people feel that they have not been treated fairly or with respect, their anger multiplies. If they have been manipulated, trivialized, ignored—or worse still, lied to—anger and a sense of unfairness
95
will build. However, don’t forget that displays of anger may be a form of manipulation by another party, especially in public, to bully others into accepting their demands. Of course, more than one anger-causing element can be involved in a single situation.
Don’t make the error of defining anger as either rational or irrational. That’s judgmental, counterproductive, and truly in the eye of the beholder. It’s dangerous to label others as irrational because you may then feel justified in dismissing them, which will only heighten their sense of injustice.
Don’t lecture! Let the audience discover the answer.
No one willingly accepts a lecture, and seldom have lectures changed anyone’s mind or behavior. Lecturing is easy—the lecturer gets to vent his or her emotions and doesn’t have to take others’ points of view into account. That which makes it easy also makes it ineffective. A lecture does not engage the audience. Telling is easy, asking is tougher. Asking questions is a deliberate action. It forces the process to slow down and forces everyone to stop and think before replying.
Instead of attempting to persuade an individual or community group to take an action, allow them to persuade themselves through a self-discovery process. The key is to not give the solution, but help your audience to discover its own solution.
How do you help an audience discover its own answers? By asking the right questions using feedback as your tool, you can ask the audience questions that will create awareness about the situation in such a way as to empower them to make a difficult choice. As many therapists will attest, a person who comes up with his own answer and says something in his own voice will take ownership of that idea. It’s better for you to ask a leading question than to make an interpretation. The right questions can help an audience to make the necessary connections. This strengthens the audience’s tendency to claim ownership for the insight.
For example, was a severe communicable disease outbreak to occur, a challenge for officials in emergency response and public health is the possibility that civil rights may need to be temporarily suspended to control the spread of disease. A extreme case would be the need to quarantine individuals or communities. It makes sense that a population that understands the need to quarantine will be more likely to uphold the curfews or quarantine requirements.
Questions to help people persuade themselves:
■ Start with broad, open-ended questions.
Example: What challenges have (you or your community) faced that required consensus building to solve the problem? How did it go? What did
96
you learn from those experiences? Were there difficult choices to make?
■ Then, ask questions to discover the explicit wants, needs, and desires of your audience.
Example: What is most important to (you or your community) when faced with a problem to solve? Consensus building? Putting the greater good for the greater number first? Avoiding conflict?
That the solution is fair and equitably distributed? Ensuring that everyone has a voice and is heard? Those reasonable alternatives are fully explored?
■ Follow with questions that are more specific to the situation now being faced by the audience.
Example: What are the ramifications to (you, your family, your community, the nation) when faced with this current problem? What consequences are you hoping to avoid? What do you see as the worst outcome for (you or your community)? What courses of action do you believe could mitigate this outcome?
■ Then, ask questions that encourage audience members to state the benefits they would like to see result from a course of action.
Example: What benefits would (you or your community) expect if this disease did not spread further? Since you’ve brought up quarantine, what benefits would (you or your community) expect if you accepted quarantine as a course of action to reduce spread of disease?
■ Once the audience sees and expresses the benefits, it will be much easier to demonstrate how your strategy can solve the problem.
Example: “From what I understand, you are looking for a way to protect (yourself, family, community) from more illness or death? If I can go ahead and explain how quarantine will meet those needs, are you open to implementing it? If you think quarantine would work in this effort, how do you see the quarantine being explained to the entire community and implemented?”
Allowing people to persuade themselves is not an easy process. Done poorly, it can seem condescending or manipulative. It takes practice and a great deal of empathy. However, it’s worth the effort, because it is truly the most effective way to gain acceptance in thought and behavior.
How to de-escalate the conflict?
Start by trying to agree on issues that may not be core to the conflict—not the hot button issue that anyone is willing to concede. Agree whenever you can. It is hard
97
to attack someone who agrees with you. You don’t have to concede a thing. Find the elements that bring some agreement among both groups. Set up guidelines for interaction and make an effort to “humanize” each side for the other.
· At all times, seek common principles on which to base a common dialogue.
· Remain open to reason and allow yourself to consider that you might be wrong.
· Strive for fairness in the process, especially where a real or perceived inequity has occurred.
· Work to get input from all stakeholders.
· Leave the community or population better off than how you found it.
· Decision makers in the community should have access to open and complete scientific information.
Try to get as many “yeses” as you can. If someone says, “Your proposal is totally unrealistic,” try this response: “Are you saying that you don’t see how my proposal can (respect citizens’ rights and stop the spread of disease)?” When person says “yes,” this transforms the relationship. Each question you offer that allows a “yes” answer from the other side further reduces the tension. Don’t say “but”—say “yes, and.”
Typically, people express their differences by prefacing their responses with, “but.” The other group will be more receptive if you first acknowledge their views with a “yes” and then preface your view with an “and.” Example: “Yes, we want to protect people’s rights and we want to keep them alive to enjoy those rights.”
5.8 Notes on Selecting And Using Communication Channels During A
Public Health Emergency
Here are two major communication issues beyond working with the media that must be addressed in preparation for crises. First, at the community, state, and national level, the public expects access to its government during an emergency. One of the most effective ways to give them this access is through e-mail and toll-free information telephone lines. Second, as a public health crisis evolves beyond 24 to 48 hours, the demand for information outside traditional media channels—radio, TV, newspaper, and news Web sites—increases. The public information official must choose the right method of delivery to address various audiences. This module addresses both of these important issues.
Public telephone and e-mail services during an emergency Consider the following when planning for toll-free number services (or building capacity inhouse).
98
· Decide between rapid expansion of an existing phone number or a “new” toll-free number generated specifically for the emergency.
· The service must be expandable in terms of number of calls managed per hour or day and the hours of operation.
· The toll-free number must be answered by trained people who can reassure callers, provide requested information, and/or refer callers as needed.
· Precleared materials on multiple subjects should be easily accessible during an emergency. The following are concerns about predeveloped materials:
– Materials must be specific to the emergency and the community impact.
– They must be easy to read and understand.
– They must be available in multiple languages based on community needs.
– They must be field tested for cultural sensitivity and preferences.
· Standards of performance and evaluation should be considered: customer satisfaction, response capacity, accuracy, etc.
· Call managers must be able to quickly integrate new information into their emergency responses.
These issues must be considered for your public e-mail response service. State up front how long it will be before the public gets a response to an e-mail (2 hours, 24 hours, same week) and provide a way to reach your organization if the need is more urgent. Be sure to advise people to seek out their health care providers or 911 for a personal medical emergency.
The CDC Public Response Service (PRS) began in October 2001, and is available free-of-charge to local and state health departments. PRS provides a rapid, turnkey toll-free hotline and interactive e-mail service that will provide both local information specific to the emergency (e.g., where to get shots in your community) and CDC-approved background health and medical information. This service is available to help a community or state manage its public information requirements during a public health emergency.
The service works with the general public, public health professionals, and emergency response teams. Service is available for Spanish and English speakers and the deaf and hearing impaired.
99
Achieving effective communication with your audiences depends on selecting methods of communication that will reach them. This is especially important in health risk communication, where the audience participants can become disenfranchised quickly if they do not feel they are getting information.
Message delivery channels include:
· Face-to-face (e.g., health care professional to patient, or your organization’s staff member to state partner organization or individuals in the community)
· Group delivery (e.g., small group or public meetings)
· Organizational (e.g., constituents of influential community organizations)
· Mass media (e.g., radio, television, newspaper, or direct mail)
· Community (e.g., employers, schools, malls, health groups, or local government agencies)
· Combination of any or all of these (i.e., most likely to work best).
Questions to ask:
· Which channels are most appropriate for the health risk problem/issue and messages?
· Which channels will the target audience find credible and accessible?
· Which channels fit the program purpose (e.g., inform, influence, allay fears, influence attitudes, or change behavior)?
· Which channels and how many channels are feasible, considering your schedule and budget?
Identifying Specific Communication Tools
The tools you will use depend on your audience, how participants prefer to receive information, and the information you need to communicate. Possible tools include:
Briefings
Briefing is a session with key state and local officials, media representatives, and community leaders. Agency staff conduct sessions in person. Briefings
100
help to notify key state and local officials, media representatives, and community leaders of developments at the site, such as results of studies or actions that should be taken to protect health. A briefing can be used to introduce your organization and explain its role and work process. Briefings are not usually open to the general public.
Conducting a briefing:
· Schedule the briefing in a small public room, such as a hotel meeting
room or a conference room.
· Hold the briefing in a neutral location, particularly when dealing with an antagonistic situation.
· Prepare a factsheet or question and answer sheet.
· Present a short, official statement about the agency’s findings, health concerns, or recent developments.
· Use simple language.
· Avoid jargon, acronyms, and overly technical terms.
· Answer questions about the statement.
· Work with your organization to coordinate briefings.
Benefits of a briefing :
· Allows state and local officials, the media, and citizens to question your organization directly about any activity before the public release of information
· Prepares officials and citizen leaders to answer questions from their constituents when the information becomes public
· Allows for the exchange of information and concerns.
101
Limitations of a briefing:
· Although briefings can be effective, they could become the only means of communicating with site communities. Briefings should always be complemented by activities to inform the general public, such as small group or public meetings.
· Negative feelings or bad publicity could result if some people believe that they should be invited to the briefing and are not. Be sure not to exclude such persons or convey favoritism toward certain parties.
Community mailings
A community mailing sends information to key contacts and concerned or involved members of the community. It disseminates information quickly and easily in writing, and it is particularly useful when you have updates for the community.
If the updates are straightforward, non controversial, and easy to understand, the mailing can stand on its own. However, if the updates are more complicated and require discussion or further explanation, the mailing should augment a public meeting or small group meetings. The community mailing can announce upcoming meetings and provide advance information or serve as a follow up for people who did not attend previous meetings.
Developing a community mailing
Compile a mailing list and include:
· State and local officials (check with city clerk for assistance)
· Community leaders (check with local chamber of commerce)
· Local residents of the site area (check with city clerk for assistance)
· Community members who have signed up to receive information.
Creating mailing materials
Include:
· A cover letter that introduces you, briefly explains the purpose of the mailing, and provides contact information for comments or questions
· A factsheet, newsletter, report, or other documents
· First-class postage to deliver the mailing quickly.
102
5.9 Notes on Evaluating Your Plan after Crisis
o Evaluate how useful the plan was. o Identify any problems revealed during the incident
o Determine if the plan’s procedures were followed and if they were
effective. If not, examine ways to improve them.
o Determine how quickly the Crisis Action Team was able to organize and begin to function.
o Determine the adequacy of the facilities and resources provided to the
Crisis Action Team. Consider how they can be improved.
o Determine if information was shared effectively and fully within the Crisis Action Team and identify any reasons for a negative answer.
o Determine if the team members and support personnel were familiar with
the organisation’s operating procedures and chain of command.
o Determine if your organization’s personnel were familiar with the procedures of other involved organizations.
o Examine the effectiveness of your organisation’s liaison(s) with external
actors such as government officials, families and the media.
o Determine if routine matters were referred to appropriate personnel or whether the Crisis Action Team allowed itself to be distracted by them.
o Review your reports and statements to determine if information was
reported accurately, on a timely basis, and in the proper fashion. Determine if appropriate analyses were prepared as required. Check that the proper people and organizations were kept informed.
o Determine whether your supplies were adequate.
o Review the effectiveness of your public affairs management.
o Determine the effectiveness of your rumours control mechanism.
o Examine the composition of your crisis action team to determine if
personality factors impeded effective crisis management.
103
o Review the involvement of your Crisis Action Team in planning and preparation of your emergency procedures to determine its adequacy and effectiveness.
o Review the composition of your Crisis Action Team to determine its
adequacy.
o Review the training of your emergency personnel to determine its effectiveness, completeness and adequacy.
104
Annex 6 Notes on Exercises Exercise 1: Audience Analysis o Audience are not always the same o Audience can be segmented o Each segment possesses certain characteristics and should be considered when
preparing messages and material.
Instruction to participants: 1. Divide into groups at least 5 members. 2. Each Group will be given one set of communication messages. 3. Read the messages carefully 4. Discuss with the group members the intended audience for each message and
your reason for the choice. 5. To facilitate sharing, prepare your presentation using the table below: Message Target Audience Reason Message 1 Message 2 Summarizing key points: 1. Risk communication messages should fit needs of the intended audience. 2. Therefore it is important that the intended audiences are segmented an
analyzed.
105
Exercise 2 Audience Analysis and Segmentation Instruction to the participants: 1. Using the data gathered during situational analysis, conduct audience
segmentation. 2. Identify the possible target audience. 3. Rank the target audience according to priority and classify them as primary,
secondary, or tertiary. 4. State reasons for identifying targeted audiences. 5. Write your analysis on the flip chart or power point presentation 6. Use the following template for presentation of outputs: Time allocated: 30 minutes Objective: Participants will be able to do audience analysis audience segmentation. Name of disaster: Place: Audience segmentation Audience
Prioritization
Classification
Reason for choice of this audience group
106
Annex 7 Notes on Exercises Exercise 3 Message development The crucial concern is how to develop messages that can mobilize target groups into specific action. In this unit participants will be introduced to the importance of audience segmentation and the processes or steps involved in developing messages. Instruction to the participants: 1. Divide into groups at least 5 members. 2. Each Group will be given one set of white board. 3. Discuss with the group members the factors determining audience acceptability
of health messages and your reason for the choice. 4. Write your analysis on the flip chart or power point presentation 5. To facilitate sharing, prepare your presentation using the table below: Time allocated: 30 minutes Factors audience acceptability Target Audience Reason Factor 1 ---------------------------------------------------------------------------------------------------------------- Factor 2 Summarizing key points: 1. Successful health risk communication involves communicating the right message
to the right audience at the right time with the right tone using the right channel for the right purpose.
2. Developing Risk communication messages should fit needs of the intended audience.
107
Exercise 4 Developing messages. To develop key messages:
o Brainstorm – Think freely and jot down all pieces of information you wish to communicate.
o Select key messages – Identify the most important ideas. Repeat the process until you list it down to three items.
o Identifying supporting data – Review your brainstorming ideas and background materials for information that provides support to you key messages.
Instruction to the participants: 1. Divide into groups at least 5 members. 2. Each Group will be given one set of communication messages. 3. Discuss with the group members the main concern of the target group and
develop key messages and supporting messages. 4. Write your analysis on the flip chart or power point presentation 5. To facilitate sharing, prepare your presentation using the table below: Time allocated: 1 hour Target Audience
Message objective
Main Concern (Key Message)
Supporting messages
Target group 1
Objective 1 Objective 2
Key message 1
1. 2. 3.
Target group 2
Objective 1 Objective 2
Key message 2
1. 2. 3.
Summarizing key points: 1. Understand the specific communication objective, and tailor your messages to
the specific audience. 2. The key messages are the points that you want your audience to have in mind. 3. A key message may consist of a whole sentence or just 2 or 3 keywords, which
were later being develop into full messages. 4. The messages should be relevant, clear, simple, concise, consistent, timely,
accurate, acceptable and complete to your audience. 5. Pre testing provides useful information about accuracy, acceptability, relevancy,
credibility and completeness of the messages.
108
Annex 8 Notes on exercise Exercise 5 Skills for Media Spokesperson. The media are the primary means for communicating with the public. Forming positive relationships with journalist and understanding their needs is crucial to the communications success. Instruction to the participants: 1. Divide into groups at least 5 members. 2. Each Group will be given one set of communication messages. 3. Discuss with the group members about:
a. ”What makes a good spokesperson? b. Role as a spokes person.
4. Write your analysis on the flip chart or power point presentation 5. To facilitate sharing, prepare your presentation using the table below: Time allocated: 1 hour
Table 1: What makes a good spokesperson?
Characteristics of a good spokesperson
Reasons
Table2: Role as a spokes person Roles and responsibility as a spokesperson
Reasons
Summarizing key points: Positive relationships with journalist and understanding their needs are crucial to the communications success.
109
Annex 9 Notes on exercises Exercise 6 Working with the media. Media practitioners need information fast. Public also rely on them for information, which can sometime console or cause panic. They need to be provided timely and correct information. In this session participants will be introduced to the media process and get some tips on how to manage and work with media practitioners. Instruction to the participants: 1. Divide into groups at least 5 members. 2. Each Group will be given one set of scenario. 3. Discuss with the group members
a. The role of media b. How the media works.
4. Write your analysis on the flip chart or power point presentation 5. To facilitate sharing, prepare your presentation using the table below: Time allocated: 1 hour
Discuss what are the opportunities of media in health crisis? Opportunities of media in health crisis
Reasons
Summarizing key points: Media like most on stories that are; o Front page news stories o Human interest stories o People’s perspectives o Yes or no/safe or unsafe answers
110
Exercise 7 Communicating with the public When communicating to the general public during an outbreak or any crisis situation, people have different concern and needs. They were concern about their family’s safety or just want to know what is going on. This session will look into these differences and how they can be addressed when preparing risk communication messages. Instructions to the participants
1. Divide into groups at least 5 members 2. Each group will be given one case study 3. Based on the scenario prepare talking point for the media 4. Choose one of the participants within the group member. 5. Do the practical session facing the media.
Time allocated: 1 hour Work in groups of about five. Goal: Using the risk communication strategies discussed in this workshop, write some talking points for the officials who are going to announce the disaster to the media. Scenario: Adapted from Crisis and Emergency Risk communication, CDC 2002 Case Study. H5N1 Virus Outbreak Investigation, Hong Kong, 1997–1998
In May 1997, a 3-year-old Hong Kong boy became ill with fever, dry cough, and a sore throat. He was hospitalized, continued a downward course, and died. Only influenza A virus was cultured from this child.
Scientists identified the virus as influenza A/(H5N1). This virus had never before been cultured from a human specimen. The subsequent investigation ruled out laboratory contamination, and concluded that the child’s illness was consistent with influenza complicated by viral pneumonia. Investigators believed, based on laboratory evidence, that the virus was transmitted directly from an avian source to the child, possibly in the outdoor garden area of his school. This was the first reported case of an avian virus being transmitted directly to a human. During the August–September investigation, no other cases were found.
In late November, the Hong Kong Department of Health contacted CDC’s Influenza Branch to report that a second H5N1 infection had been detected. CDC sent a team of medical epidemiologists and field investigators.
111
CDC and health organizations around the world engage in ongoing, active surveillance to attempt to quickly detect the possibility of a pandemic influenza virus spreading among humans. Influenza viruses mutate easily. Most often the mutation is slight and occurs over time, a process called “drift.” Occasionally, an influenza virus will suddenly mutate significantly; this is called “shift.” A virus that shifts is a potential pandemic strain. To qualify as a potential pandemic strain, the virus must meet 3 criteria: (1) it must be genetically novel, (2) it must be virulent, and (3) it must be efficiently transmitted between humans.
In late December, cases were accumulating and young healthy adults were dying of this viral infection. The H5N1 virus in this outbreak met 2 of the 3 criteria: it was novel and it was virulent. CDC, Hong Kong DOH and a number of collaborators began an intense investigation to determine whether this was the start of an influenza pandemic. Indeed, public health officials know, based on trend analysis, that a pandemic is overdue. Investigators concentrated on determining the virus’ ability to transmit from person to person. An increase in person-to-person virus transmission would have suggested that the virus was adapting to humans, with the potential for epidemic spread.
In mid-December, a veterinarian virologist collaborating on the investigation held a telephone worldwide news conference and announced this was the “pandemic” strain that health officials were expecting. The immediate media uproar severely disturbed the investigators’ attempts to collect information in Hong Kong. The Hong Kong DOH and the CDC field team requested that a CDC public information officer (PIO) join the team in Hong Kong, the first time CDC had assigned a PIO on an overseas field investigation. During the field assignment, the CDC PIO represented CDC, DHHS and WHO on public information issues. Task: You are communication officers. Your technical experts tell you about the outbreak/crisis. Prepare talking points for the media. Think about what you want the public to know, and also list some of the questions you think they will ask. Consult other departments in deciding what to say? Sources of the outbreak, steps taken, prevention, others? Use risk communication strategies from this workshop. Summarizing key points: Preparing messages must address the needs and concern of the public.
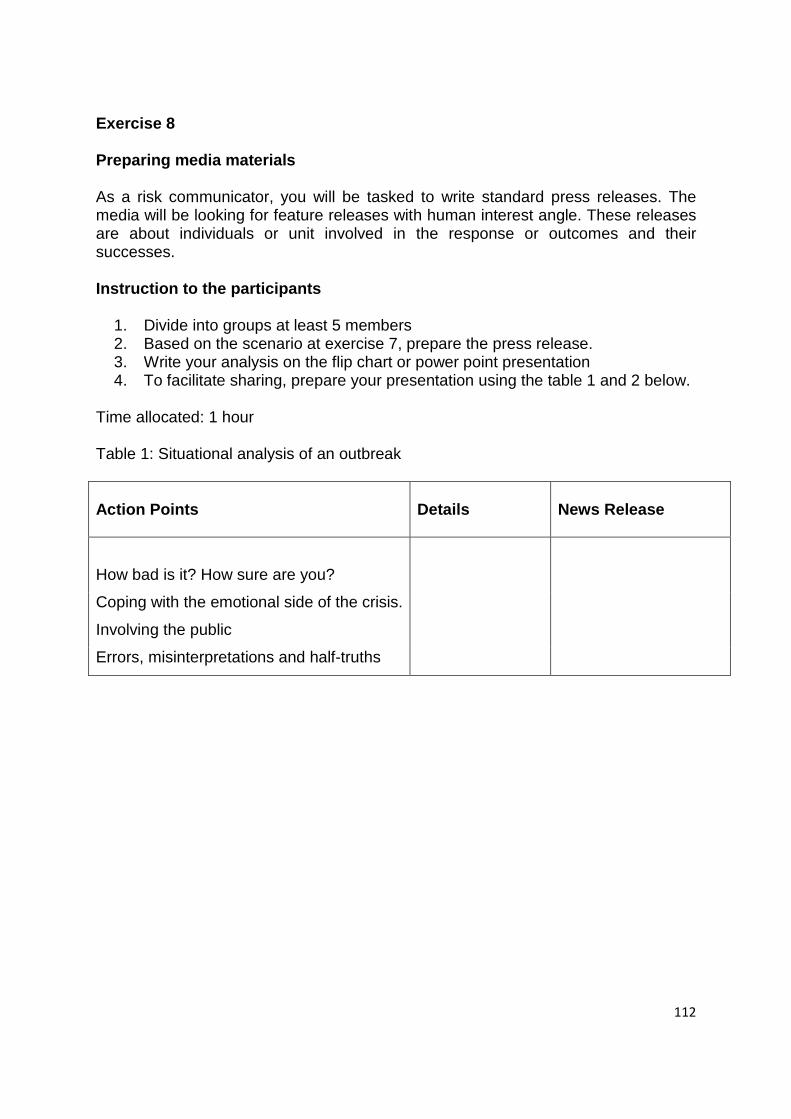
112
Exercise 8 Preparing media materials As a risk communicator, you will be tasked to write standard press releases. The media will be looking for feature releases with human interest angle. These releases are about individuals or unit involved in the response or outcomes and their successes. Instruction to the participants
1. Divide into groups at least 5 members 2. Based on the scenario at exercise 7, prepare the press release. 3. Write your analysis on the flip chart or power point presentation 4. To facilitate sharing, prepare your presentation using the table 1 and 2 below.
Time allocated: 1 hour Table 1: Situational analysis of an outbreak Action Points
Details
News Release
How bad is it? How sure are you?
Coping with the emotional side of the crisis.
Involving the public
Errors, misinterpretations and half-truths
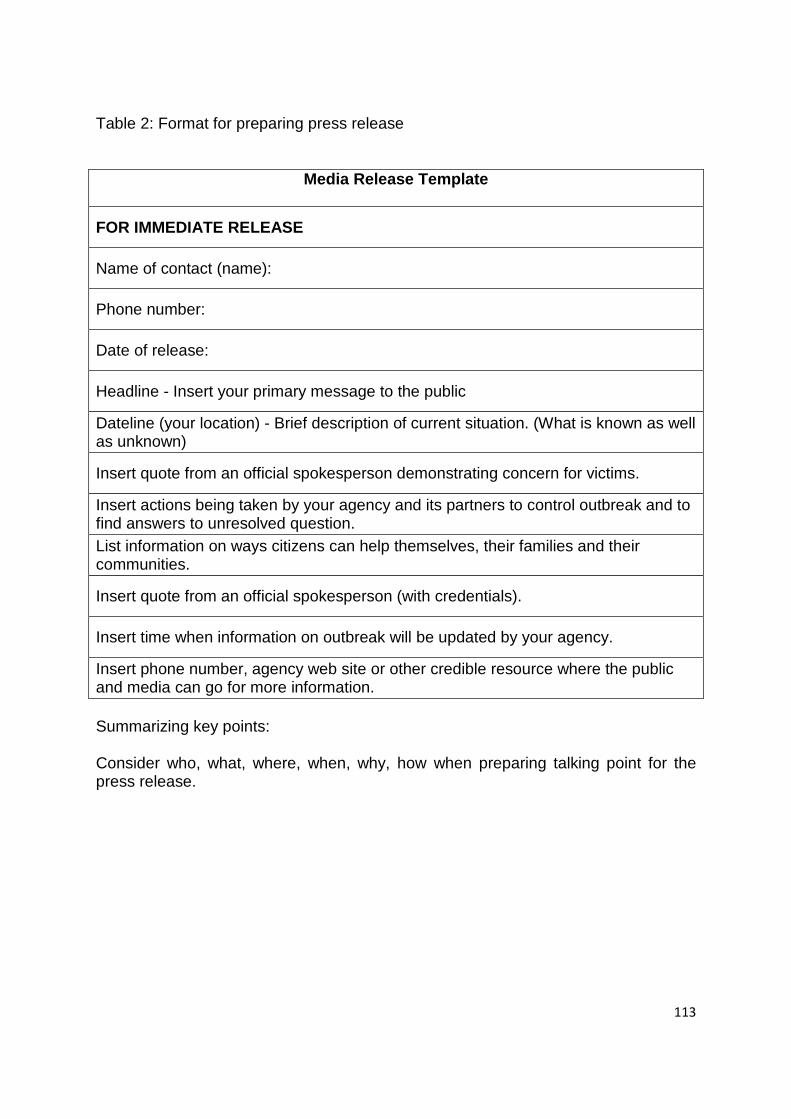
113
Table 2: Format for preparing press release
Media Release Template
FOR IMMEDIATE RELEASE
Name of contact (name):
Phone number:
Date of release:
Headline - Insert your primary message to the public
Dateline (your location) - Brief description of current situation. (What is known as well as unknown)
Insert quote from an official spokesperson demonstrating concern for victims.
Insert actions being taken by your agency and its partners to control outbreak and to find answers to unresolved question. List information on ways citizens can help themselves, their families and their communities.
Insert quote from an official spokesperson (with credentials).
Insert time when information on outbreak will be updated by your agency.
Insert phone number, agency web site or other credible resource where the public and media can go for more information. Summarizing key points: Consider who, what, where, when, why, how when preparing talking point for the press release.
114
Annex 10
Notes on Brainstorming/ Discussion
Brainstorming/Discussion activity can be useful approach for generating participants existing understanding on advocacy, its level and process of advocacy. The facilitator shall pair or groups participants to make numbers of suggestions with no restrictions on the extent to their understanding.
Participants in the exercise use the Post-It Notes to write down additional ideas. Participants stick the notes on the wall - randomly at first - and then moved and grouped together as the exercise plays out.
The participants shall encountered ideas of (limit the probing according to the needs and preferences:
a) What do you understand about advocacy b) What are the elements in advocacy c) Explain the level and process of advocacy
In order to ensure a successful exercise it is vital that participants feel comfortable about sharing ideas. This technique is ideal for participants who have not encountered scenario planning before as it offers the opportunity to become actively involved very quickly before the lecture.
Notes on Debate
Debates allow participants to take part in an interactive way and assimilate the knowledge that they have gained during the course. It allows the facilitator to gauge the understanding the participants have of the topic and allows them to identify gaps in their knowledge.
Participants can be divided into two groups of three each. Other participants who are not in the selected group can contribute ideas from the floor at the end of each participant’s presentation or at the end of each group’s presentation.
It is suggested that each participant speak for five minutes with another five minutes for the group leader to rebut and summarise the points raised.
The debate can be concluded with points of observation and summary from the facilitator.
Suggested topics of debate for the ethics component:
· Ethics is incompatible with risk management · Ethics cannot be considered at a time of disease outbreak.
115
· All the principles of ethics must have an equal weight-age in risk communication
· The principles of ethics were not used during the disease outbreaks that happened in the country.
Facilitators are free to choose any other suitable topic for the debate that would allow the participants to utilize the principles of ethics and the law.
Notes on Role Play
Participant to involve in Role Play will be based on the given scenario or previous experience. Each participant will be given certain roles related relevant stakeholder. The participants execute their functions in risk communication according to the given scenario Role Play activity can be useful approach for generating participants to understand on the management of information pertaining to risk communication and how to apply it in pre crisis or crisis situation. The facilitator shall break the participants into groups with specific position or task and need to act and respond according to their position or task. The participants shall encountered and internalized the situation and have a better understanding of the needs of different stakeholders In order to ensure a successful role play it is vital that participants feel comfortable about sharing ideas and try to simulate as the given position or task for each particular stakeholder.
116
References
117
References Module 1
1. American Health Organization. Communicating the Risk. Regional Office of
the WHO, Washington, Perspectives in Health, Volume 10 No. 2: 2005 (Reprint 2007).
2. Chartier J, Gabler S 2001, Risk communication and Government; Theory
and Application for the Canadian Food Inspection Agency, http//www.inspection.gc.ca/English/corpaffr/publications/riscomm/riscomme.shtmal retrieved on 27/8/2008.
3. Covello VT, Sandman P, Slovic P (1988). Seven cardinal rules of risk
communication. Washington, D.C.:U.S. Environmental Protection Agency. 4. Covello VT, McCallum DB, Pavlova MT. Effective Risk communication.
Lenum Press, New York, 1989.
5. Case Definition for Infectious Diseases in Malaysia 2nd Edition Jan 2006.
6. Department of Health, November 1997. Communicating about Risks to Public Health – Pointers to Good Practice. Department of Health, London.
7. Directive 20, National Security Council, Prime Minister’s Department. 8. Ed-Pres Communications Bhd. (2000). Media Relations Workshop for
Ministry of Health. Institut Kesihatan Umum, Kementerian Kesihatan, Malaysia.
9. Infectious Diseases Outbreak Rapid Response Manual, 1st Edition June 2003
10. Institute of Public Health (2002). Risk communication Training Module for Facilitators. Ministry of Health, Malaysia.
11. Lanard J. Strengthening Risk communication: An introduction to the
principles and skills. Presentation at ASEAN Plus Three Risk communication Workshop, 24-26 March 2008, Kuala Lumpur, Malaysia.
12. Lee TR 1986, Effective communication of information about chemical
hazards. The Science of the Environment 51, 149-183. 13. Lum MR, Tinker TL (1994). A Primer on Health Risk communication:
Principles and Practices. Atlanta, Georgia, U./S. Department of Health and Human Services.
118
14. Mitroff I, Alpaslan M. Thinking the unthinkable. In: Boss, June 2003. 15. National Research Council (1989). Improving risk communication.
Washington, D.C., National Academy Press. 16. Renn O.”The Role of Risk communication and Public Dialogues for
Improving Risk Management, Risk, Decision and Policy, 1998, vol.3, No.1, pp.5-30.
17. Sandman PM. Responding to Community Outrage. American Industrial
Hygiene Association, Fairfax, 1996.
18. Standard Operating Procedure for Potential Infectious Disease, 1st Edition 2004
19. The Royal Society (1993). “Risk: Analysis, Perception and Management.
London, Royal Society. 20. University of Kentucky, College of Agriculture. AGRIPEDIA,
http://frost.cas.uky.edu/agripedia/. 21. Vohra D (1996). Communication in crisis situations. In: Readings and Notes
in Crisis management. Institut Tadbiran Awam Negara (INTAN) (Unpublished).
22. WHO, Europe. Sixth Futures Forum, Reykjavik, Iceland, 10-11 May 2004.
WHO Regional Office for Europe, Denmark, 2004. 23. WHO 2005. Outbreak communication – Best practices for communicating
with the public during an outbreak. Report of the WHO Expert Consultation on Outbreak Communication held in Singapore, 21-23 September 2004.
Module 2
1. Borman, Ernest G. (1975). Discussion and Group Methods. Second Edition. New York: Harper and Row Publishers, Inc.
2. Communication in risk situations: Responding to the communication
challenges posed by Bioterrorism and Emerging Infectious Diseases, 2002. 3. Crisis and Emergency Risk communication, CDC,September 2002. 4. Leeds, Dorothy. (2000). The 7 Powers of Questions. New York: Berkley
Publishing Group.
119
5. Smith, Larry. (2001). The ICM Crisis Management Certification Course.
Louisville, Kentucky: Institute for Crisis Management. 6. Ury, William. (1993). Getting Past No: Negotiating your way from
confrontation to cooperation. New York: Bantam Books.
Module 3
1. Anon. (2009). Effective Risk communication: A Message- Centered Approach, New York.
2. Davis, M & Macdowall, W. (2006) Health Promotion Theory, Open University Press.
3. Department of Human Services. (2007).Risk communication Plan: Environmental Public Health Tracking Program, State of Oregon.
4. Department of Health (2001).Communicating Health Risk to the Public, Planning Conference Report WHO/UK
5. ILGRA Inter-Departmental Liaison Group on Assessment. (1998). Risk communication: A Guide to Regulatory Practice W HO. (2008). WHO OUTBREAK Communication Planning Guide
6. Lundgren, R. E. , McMakin, A. H. (2009). Risk communication: A Handbook for Communicating, Environmental, Safety and Health Risk, Forth Edition, New Jersey.
7. US department of Health.(2002). Communicating in a crisis: Risk communication Guidelines for public officials.
Module 4
1. Beckmann CRB, Ling FW, Herbert WNP, Laube DW, Smith RP, Barzansky BM. Obstetrics & Gynaecology. 3rd Edition. Williams & Wilkins, Baltimore 1995: 25-30.
2. Code of Medical Ethics. Malaysian Medical Association; 2002 3. Medical Ethics Today – The BMA’s Handbook of ethics and law. 2nd Edition.
British Medical Association Ethics Department. BMJ Publishing Group 2004