Embed Size (px)
Citation preview

Cite this article as: Spinella G, Finotello A, Conti M, Faggiano E, Gazzola V, Auricchio F et al. Assessment of geometrical remodelling of the aorticarch after hybrid treatment. Eur J Cardiothorac Surg 2018; doi:10.1093/ejcts/ezy397.
Assessment of geometrical remodelling of the aorticarch after hybrid treatment
Giovanni Spinellaa,*†, Alice Finotelloa,b,†, Michele Contic, Elena Faggianoc, Valerio Gazzolaa,
Ferdinando Auricchioc, Nabil Chakfed,e, Domenico Palomboa and Bianca Panea
a Department of Vascular and Endovascular Surgery, Ospedale Policlinico San Martino, University of Genoa, Genoa, Italyb Department of Experimental Medicine, University of Genoa, Genoa, Italyc Department of Civil Engineering and Architecture, University of Pavia, Pavia, Italyd Department of Vascular Surgery and Kidney Transplantation, University Hospital of Strasbourg, Strasbourg, Francee European Group for Research on Prostheses Applied for Vascular Surgery (GEPROVAS), Strasbourg, France
* Corresponding author. Vascular and Endovascular Surgery Unit, Ospedale Policlinico San Martino, University of Genoa, Largo Rosanna Benzi, 10, 16132 Genoa,Italy. Tel: +39-010-5552424; fax: +39-010-5556653; e-mail: [email protected] (G. Spinella).
Received 2 August 2018; received in revised form 17 October 2018; accepted 25 October 2018
Abstract
OBJECTIVES: The aim of this study was to measure the morphological remodelling of the ascending aorta, aortic arch and thoracic aortaafter aortic arch hybrid treatment including debranching and stent graft implantation.
METHODS: Preoperative, 1-month and 1-year follow-up of computed tomography angiography scans of 22 patients were analysed tocompute the lumen centreline from the aortic root to the coeliac trunk, and the following measurements were derived: the total centrelinelength, distance from the aortic root to the left subclavian artery, distance from the left subclavian artery to the distal landing zone. Forboth pre- and postoperative centrelines, the pointwise curvature was measured at the proximal and the distal landing zones. The mean
†The first two authors contributed equally to this paper.
CO
NV
ENTI
ON
AL
AO
RTI
CSU
RG
ERY
VC The Author(s) 2018. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
European Journal of Cardio-Thoracic Surgery 0 (2018) 1–9 ORIGINAL ARTICLEdoi:10.1093/ejcts/ezy397
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

curvature values of the whole aortic segment and the endografting region of the ascending and the descending aorta were measured.Surface outerline was computed as well, and curvature values at the endograft landing points were extracted.
RESULTS: At the 1-month follow-up, centreline length were already significantly increased (382.66 ± 48.69 to 388.1 ± 50.75 mm; P = 0.01).Centreline pointwise curvature increased in the proximal (+29%, P = 0.011) and the distal zones (+63%, P = 0.004). Similarly, pointwisecurvature of the outerline significantly increased in the proximal (+77%, P = 0.01) and the distal landing zones (+100%, P = 0.04). The centre-line mean curvature increased in the ascending aorta (+7%, P = 0.02) and decreased in the endografting region (-3.3%, P = 0.004). No evi-dence of a relationship of such a remodelling with the type of endograft and the type of pathology was observed. This remodelling trendwas confirmed by the analysis of 1-year computed tomography angiographies.
CONCLUSIONS: Hybrid arch repair was associated with a significant elongation of the vessel and a significant increase in the curvature onthe ascending aorta and the descending aorta and on the endograft proximal and the distal landing zones.
Keywords: Aortic diseases • Aortic arch • Hybrid procedure • Geometric analysis
INTRODUCTION
Although recent guidelines recommend the endovascular ap-proach as the treatment of choice for patients affected by thor-acic aortic diseases [1], the anatomy of the thoracic aorta mayaffect the feasibility of this approach in many settings. In particu-lar, the need to obtain an adequate proximal landing zone of thehealthy aorta is crucial to avoid proximal type I endoleak orendograft migration [2]. Indeed, proximal landing zones with anat least 20 mm-long, healthy and relatively straight neck areneeded for thoracic endograft placement [3].
On the contrary, in patients with short and highly angulatedlanding zones, a hybrid arch treatment performed in Ishimaru’szones 0, 1 or 2 [4] has been introduced as a feasible techniquefor revascularization of the supra-aortic vessels to obtain an ad-equate proximal landing zone for thoracic endovascular aorticrepair (TEVAR).
Unfortunately, the aortic arch is a critical zone for device deliv-ery, and its intrinsic shape plays a crucial role in the rate of acutefailure of thoracic endografts [5]. Indeed, the deployment of anendograft inside the flexible aortic tissue might lead to hard-to-predict morphological variations of the vessel shape that can becorrelated with short-, mid- and long-term complications.Identifying the changes in aortic arch morphology between pre-and postoperative configuration could, therefore, be importantto understand the causes of such complications and to predictprocedure-related adverse events.
To date, other investigators have already focused on the roleof anatomical factors in positioning outcomes [6] or have eval-uated the changes in the aortic arch curvature following TEVAR[7]. However, little is known about the geometric changes thatoccur at landing zones after aortic arch hybrid treatment andhow these could be related to possible complications.
On the basis of these considerations, the aim of our study wasto measure the morphological remodelling of the thoracic aortain patients who underwent aortic arch hybrid treatment. Aorticremodelling was measured by a quantitative analysis of the aorticgeometry before and after a hybrid arch repair.
MATERIALS AND METHODS
The research protocol was submitted to the local institutionalmedical ethics committee; the need for informed consent fromthe patients was waived because of the retrospective nature ofthe analysis and the use of anonymous data.
Patient selection
A single-centre, retrospective study was conducted on all con-secutive patients who underwent aortic arch hybrid treatmentbetween January 2012 and December 2016.
Only patients treated in zones 0, 1 or 2 according to theIshimaru classification [4] were included in the study, whereaspatients who did not undergo supra-aortic vessels revasculariza-tion or those with previous open repair of the ascending aorta(AsAo) were excluded; type B aortic dissections (n = 3) wereexcluded as well due to the great remodelling of the true lumenafter TEVAR.
On the basis of such criteria, a total of 22 cases were included:the mean age of the patients was 70.4 years (range 31–89 years),and 15 subjects were men. Nine patients presented with thoracicaortic aneurysms, 9 had penetrating aortic ulcer complicated bya pseudoaneurysm and 4 had an aortic intramural haematoma.Proximal landing zones 0 (Z0), 1 (Z1) and 2 (Z2) were involved in10, 3 and 9 patients, respectively. Patient characteristics are listedin Table 1.
All procedures were performed under general anaesthesia: 9were single-staged and 13 were 2-staged. In the 2-stage repair,the first stage consisted of supra-aortic vessels revascularization,and the second stage was the endovascular endograft deploy-ment. The median time interval between the 2 procedures was21 days; the median time interval between preoperative and 1-month computed tomography angiography (CTA) and betweenpreoperative and 1-year CTA was 40 and 378 days, respectively.
Patients with landing zone 0 underwent debranching of thesupra-aortic vessels (Fig. 1). This surgical procedure was carried
Table 1: Patient data and comorbidities
Total Group Z0 Group Z1–2
n 22 10 12Age (years), mean ± SD 70.4 ± 12.5 72.7 ± 6.9 68.5 ± 15.5Female, n (%) 7 (32) 3 (30) 4 (33)Hypertension, n 17 8 9Diabetes, n 3 0 3Chronic obstructive pulmonary
disease, n8 6 2
Coronary heart disease, n 5 3 2Atrial fibrillation, n 3 2 1Chronic renal failure, n 3 2 1
SD: standard deviation.
2 G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

out by means of an end-to-side anastomosis between the partial-ly clamped AsAo and the brachiocephalic trunk and the left com-mon carotid artery using a bifurcated polyester textile graft. Theleft subclavian artery was revascularized during TEVAR bycarotid–subclavian artery bypass.
Patients with landing zone 1 underwent right common carotidartery to left subclavian artery bypass (using an 8–10-mm diam-eter stretch polyester textile graft), whereas the left common ca-rotid artery was reimplanted on bypass with an end-to-sideanastomosis (Fig. 1).
Patients with a landing zone 2 underwent carotid-subclavianartery bypass. Debranching was carried out by means of an end-to-side anastomosis between the left common carotid artery andthe left subclavian artery using an 8–10-mm diameter stretchpolyester textile graft (Fig. 1).
The technical success was defined by an accurate endograftdeployment without the need for an additional endograft de-ployment and the coverage of target-selected aortic vessels.
Imaging analysis protocol
All 22 patients underwent preoperative and 1-month post-operative contrast-enhanced CTA, while 19 of them were consid-ered for 1-year follow-up analysis; indeed, 3 patients did notundergo 1-year postoperative CTA due to death in 1 case andreintervention in 2 cases before the completion of 1-year follow-up. The slice thickness and the pixel spacing were in the range of0.5–1.25 mm and 0.55–0.97 mm, respectively. All scans weretransferred to a workstation in an anonymous format for imageprocessing as described below. The whole processing procedurewas performed using the open-source Vascular Modelling Toolkitlibrary [8]. An overview of the image processing workflow isshown in Fig. 2. Firstly, we performed a semiautomatic gradient-based level set segmentation to extract a 3-dimensional (3D)model of the thoracic aorta lumen. Segmentation of post-operative images could also be used to retrieve the endografts3D models. Afterwards, each postoperative vessel surface was
Figure 1: Debranching procedures. A schematic representation of the debranching procedure for zones 0, 1 or 2 according to the Ishimaru classification. For eachcase, the bypass is highlighted in green, whereas the red crosses represent the brachiocephalic trunk and the left common carotid artery excluded by ligation or withplug occlusion in case of the left subclavian artery.
Figure 2: Workflow of the medical image analysis. (A) Starting from the computed tomography angiography images, the lumen (red) and the endograft (yellow) wereautomatically segmented; (B) the postoperative lumen surface (blue) and the endograft surface (yellow) were superimposed to the preoperative lumen surface (red);and (C) the centrelines were automatically computed from the aortic root (endpoint E1) to the coeliac trunk (endpoint E2).
CO
NV
ENTI
ON
AL
AO
RTI
CSU
RG
ERY
3G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

automatically registered to the preoperative one by means of theIterative Closest Point algorithm [9], a robust method for a rigidregistration of 3D data, which is implemented in the VascularModelling Toolkit as well. Finally, pre- and postoperative centre-lines were automatically computed [10] from the sinotubularjunction of the aortic root (AR) to the plane crossing the coeliactrunk.
When the preoperative 3D geometries involved saccularaneurysms, a virtual preoperative surface model excluding theaneurysmal sac was created. This procedure was performed toprevent the vessel centreline from being affected by the bulbousprotrusion. The removal of the saccular aneurysm was performedby identifying the centreline points that define the area of influ-ence of the sac, removing the portion of centreline among theseextremities and finally creating a new interpolated parent arterycentreline. The original method already implemented in theVascular Modelling Toolkit was partially modified to manuallyadjust the position of the 2 points delimiting the aortic aneurys-mal sac.
Given the lumen centreline, we performed the following meas-urements: length of the whole centreline (L); length of the centre-line covered by the endograft(s) (CL); distance from the AR to theproximal edge of the left subclavian artery (DAR-LSA); distancefrom the left subclavian artery proximal edge to the distal landingzone (DLSA-D). CL was automatically computed by projecting the3D model of the endograft(s) into the postoperative aortic lumencentreline. All these measurements are illustrated in Fig. 3A.
In addition to the centreline path, a custom script was imple-mented to extract the external path (outerline) of the vessel sur-face (Fig. 3B).
Curvature was quantified along the extracted paths (the cen-treline and the outerline) for all patients. At a given point, curva-ture is defined as the inverse of the radius of the local osculatingcircle, i.e. the circle approximating the curve at a given point. Onthe basis of this definition, the value of curvature at a certainpoint quantifies its deviation from a straight line as illustrated inFig. 3C.
As preoperative and postoperative vessel surfaces were auto-matically registered with the Iterative Closest Point algorithm, theposition of the endograft was also identified onto thepreoperative path lines, thus allowing us to measure the localcurvature values on both pre- and postoperative paths (centre-line and outerline) in 2 specific points: the proximal (P1) and thedistal (D1) extremities of the aortic portion involved in the endo-vascular implant(s). The position of these points is highlighted inFig. 3B.
Furthermore, the values of local curvature computed along thecentreline were averaged to obtain the preoperative and post-operative mean curvatures of the total aorta (from the AR to thecoeliac trunk), the AsAo (from the AR to P1), the endografting re-gion (ER) (from P1 to D1) and the descending aorta (from D1 tothe coeliac trunk).
Calculations were made both for the whole group of patients(n = 22) and for the 2 sub-groups, i.e. Z0 (n = 10) and Z1–2(n = 12). Patients with landing zones Z1 and Z2 were grouped to-gether (Z1–2) due to the limited number of Z1 cases (n = 3) andsimilar aortic arch morphology between Z1 and Z2. As men-tioned before, at 1-year, 3 patients were lost to follow-up (2patients in the Z0 group and 1 patient in the Z1–2 group).
Statistical analysis
All statistical analyses were performed using the JMP 13.0 (SASInstitute Inc. Cary, NC, USA) software.
Data are shown as absolute frequencies, percentages, medianwith a range and mean ± standard deviation, where appropriate.The Shapiro–Wilk’s test and the visual investigation of data withhistograms were used to assess the normal distribution of thedata. All significant differences between pre- and postoperativegeometric measurements were analysed by means of thePaired-samples t-test. Comparisons between different groups ofdevices and the various pathologies were performed individual-ly using the one-way analysis of variance for unequal sample
Figure 3: A geometric analysis of the aortic centreline. (A) Performed measurements: centreline length (L), DAR-LSA and DLSA-D. (B) Curvature was evaluated at the prox-imal (P1) and the distal (D1) landing points for both the centreline and the outerline paths. (C) Local curvature computation: in each point, the curvature value isextracted as the inverse of the radius in the local osculating circle. DAR-LSA: distance from the AR to the proximal edge of the left subclavian artery; DLSA-D: distancefrom the left subclavian artery proximal edge to the distal landing zone.
4 G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

sizes. Univariate correlations were examined using the Pearson’scorrelation coefficient. P-values <0.05 were considered statistic-ally significant in all statistical tests. No correction for multipletesting was performed, thus all significant values should beinterpreted with caution.
Although the pipeline we proposed allowed us to minimizethe users’ interaction, the semiautomatic segmentation phase ofthe vessel could potentially lead to slight measurement differen-ces. Therefore, to validate the obtained results, 2 independent,skilled observers performed segmentation of CTA images andsubsequent centreline extraction and measurements, and one ofthem conducted it twice, allowing for interobserver and intraob-server variability analysis using the intraclass correlation coeffi-cient (ICC). The results were presented with the 95% confidenceinterval (CI).
RESULTS
Study subjects
Altogether, 41 endografts corresponding to 3 different types ofdevices were deployed for 22 procedures: 10 patients (45%)received the Low-Profile Zenith Alpha endograft (Cook,Bloomington, IN, USA), 7 (32%) received the Relay NBS endograft(Bolton, Barcelona, Spain) and 5 (23%) the Gore C-TAG endograft(W.L. Gore and Associates, Flagstaff, AZ, USA).
Technical success was achieved in 100% of cases. No intrao-perative deaths, paraplegia or other major complicationsoccurred. The following complications were observed duringfollow-up: 1 case of type Ib endoleak at 1-month follow-up, 1case of asymptomatic retrograde type A aortic dissection(rTAAD) revealed by 1-month CTA which required reinterven-tion, 1 case of aortic dissection on the distal landing zone at 3-month follow-up resolved by open repair and 1 case of pseudoa-neurysm with aortic rupture on the distal landing zone at 1 yearof follow-up with required endovascular reintervention. Twodeaths occurred within the 1-year follow-up due to complica-tions after reintervention. Of these 2 patients, 1 died from sepsisafter open repair for rTAAD and another patient died 2 monthsafter reintervention for aortic rupture.
Analysis of geometrical remodelling
One-month results. The values of computed geometricalquantities regarding both pre- and postoperative aortic centre-lines are reported in Table 2 (the total group of patients), Table 3(the Z0 group) and Table 4 (the Z1–2 group). The percentage ofthe endograft coverage CL was 60 ± 17 and 1.8 ± 0.7 endograftswere used per patient. Although not statistically significant, lon-ger segments of the aorta were stented in subjects in the Z0group compared to those in the Z1–2 group (65 ± 20% vs56 ± 15%, P = 0.1).
After hybrid repair, the centreline length significantly increased(P = 0.01) for the whole group of patients, albeit to a rather smalldegree, i.e. 1.35%. Such a change in length was statistically signifi-cant in the Z0 group (P = 0.04) alone, showing an average in-crease of 2.3%; conversely, the Z1–2 group did not showcentreline lengthening (P = 0.1).
The degree of pointwise curvature at the endograft landingpoints was assessed numerically (Fig. 4). Just 1 month after treat-ment, centreline local curvature was significantly greater in bothP1 (P = 0.011) and D1 (P = 0.004). Considering the Z0 group, theincrease in curvature in P1 was detected even if no statistical sig-nificance was reached (P = 0.06), whereas centreline local curva-ture significantly increased (P = 0.04) in the distal landing zoneD1. With regard to the Z1–2 group, a significant increase in thecurvature was found in both the P1 (P = 0.03) and the D1(P = 0.02) zones.
Similarly, the pointwise curvature of the surface outerline(Fig. 4) significantly increased in P1 (P = 0.01) and D1 (P = 0.04)for the total group of patients. No statistical significance wasreached for the Z0 group even if an increase of approximately40% of curvature values was detected in P1 (P = 0.055), whereas asignificant increase was observed on both P1 (P = 0.01) and D1(P = 0.03) when the Z1-2 group was considered.
Following hybrid repair, the centreline mean curvature showeda significant increase (+7%) in the AsAo (P = 0.02) and a significantdecrease (-3.3%) in the ER (P = 0.004). Regarding the mean curva-ture values in group Z0, a statistically significant increase(+14.5%) in the mean curvature was observed in the AsAo(P = 0.008) together with a decrease (-3%) in the mean curvaturein the ER (P = 0.05). For group Z1–2, a significant reduction
Table 2: Measurements for the whole group of patients
Measurements Preoperative 1-Month follow-up 1-Year follow-up
L (mm), mean ± SD 382.7 ± 48.7 388.1 ± 50.7; P = 0.010 395.1 ± 47.7; P = 0.001DAR-LSA (mm), mean ± SD 114.1 ± 18.7 117 ± 19.3; P = 0.02 119.7 ± 17.9; P < 0.001DLSA-D (mm), mean ± SD 190.51 ± 79.90 192.51 ± 74.64Centreline curvature� 10 (1/mm), mean ± SD
P1 0.22 ± 0.08 0.27 ± 0.16; P = 0.011 0.4 ± 0.2; P < 0.001D1 0.09 ± 0.063 0.15 ± 0.12; P = 0.004 0.23 ± 0.13; P < 0.001TA 0.18 ± 0.02 0.18 ± 0.02; P = 0.12 0.21 ± 0.04; P = 0.04AsAo 0.19 ± 0.04 0.21 ± 0.04; P = 0.02 0.24 ± 0.08; P = 0.05ER 0.20 ± 0.04 0.19 ± 0.03; P = 0.004 0.20 ± 0.04; P = 0.06DsAo 0.11 ± 0.05 0.12 ± 0.07; P = 0.090 0.18 ± 0.07; P = 0.02
Outerline curvature� 10 (1/mm), mean ± SDP1 0.32 ± 0.23 0.49 ± 0.37; P = 0.01 0.5 ± 0.18; P = 0.04D1 0.11 ± 0.06 0.18 ± 0.09; P = 0.04 0.41 ± 0.04; P = 0.04
ASAo: ascending aorta; DAR-LSA: distance from the AR to the proximal edge of the left subclavian artery; D1: distal; DLSA-D: distance from the left subclavian arteryproximal edge to the distal landing zone; DsAo: descending aorta; ER: endografting region; P1: proximal; SD: standard deviation; TA: total aorta.
CO
NV
ENTI
ON
AL
AO
RTI
CSU
RG
ERY
5G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

(P = 0.04) in the mean curvature values was observed in the ER(-3.4%).
No device-related differences were observed among the 3groups. Subsequently, considering the pathology, no significantdifferences were detected for any of the computed parameters,except for the change in the centreline length. In particular, agreater increase in the centreline length was observed in the an-eurysm group.
Considering the number of deployed stents, no differenceswere found regarding the changes in the centreline lengths. Nostatistically significant correlation was found between the cover-age length CL and other computed quantities. No correlationwas found between the centreline length increase and the meancurvature increase.
One-year results. The analysis performed at 1-year follow-upconfirmed the remodelling trend of the aorta. In particular, asconcerns the centreline length, a mean increase of +12.3 mm wasobserved when compared to preoperative configuration. At1-year follow-up, values of pointwise curvature at proximal anddistal landing zones confirm the increase already observed at1-month follow-up; the same applies with the mean curvature
increase in the unstented regions of both the ascending aortaand the descending aorta.
Intraobserver and interobserver reproducibilityanalyses
Intraobserver and interobserver reproducibility analyses werecomputed by the ICC. The intraobserver ICC index resulted in0.98 (95% CI 0.97–1.00) for length measurements. An interob-server analysis showed an ICC index of 0.97 (95% CI 0.97–0.98)for length measurements. These results indicated an excellentintraobserver agreement and an interobserver agreement forlength measurements.
DISCUSSION
The endovascular treatment of aortic diseases involving the thor-acic area presents several anatomical challenges (i.e. a complex3D anatomy and the presence of supra-aortic vessels).
In particular, the high variability of the aortic arch anatomy [6,11], which is further modified by the pathologies [12], leads to a
Table 4: Measurements for the Z1–2 group
Measurements Preoperative 1 Month 1 Year
L (mm), mean ± SD 381.6 ± 50.9 384.11 ± 50.92; P = 0.13 395.77 ± 56.83; P = 0.05DAR-LSA (mm), mean ± SD 116.5 ± 18.4 118.3 ± 20.5; P = 0.06 123.75 ± 21.46; P = 0.01DLSA-D (mm), mean ± SD 186.2 ± 73.3 188.81 ± 83.32Centreline curvature� 10 (1/mm), mean ± SD
P1 0.18 ± 0.07 0.24 ± 0.15; P = 0.03 0.36 ± 0.13; P = 0.02D1 0.09 ± 0.06 0.16 ± 0.15; P = 0.02 0.25 ± 0.13; P < 0.001TA 0.18 ± 0.02 0.17 ± 0.02; P = 0.2 0.21 ± 0.04; P = 0.006AsAo 0.20 ± 0.03 0.020 ± 0.02; P = 0.3 0.24 ± 0.04; P = 0.03ER 0.19 ± 0.04 0.18 ± 0.03; P = 0.04 0.2 ± 0.03; P = 0.1DsAo 0.12 ± 0.06 0.12 ± 0.03; P = 0.4 0.19 ± 0.08; P = 0.006
Outerline curvature� 10 (1/mm), mean ± SDP1 0.40 ± 0.28 0.64 ± 0.42; P = 0.01 0.58 ± 0.2; P = 0.03D1 0.11 ± 0.05 0.21 ± 0.10; P = 0.03 0.45 ± 0.1; P = 0.05
ASAo: ascending aorta; DAR-LSA: distance from the AR to the proximal edge of the left subclavian artery; D1: distal; DLSA-D: distance from the left subclavian arteryproximal edge to the distal landing zone; DsAo: descending aorta; ER: endografting region; P1: proximal; SD: standard deviation; TA: total aorta.
Table 3: Measurements for the Z0 group
Measurements Preoperative 1-Month follow-up 1-Year follow-up
L (mm), mean ± SD 382.6 ± 45.9 391.6 ± 45.9; P = 0.04 406.00 ± 42.4; P = 0.008DAR-LSA (mm), mean ± SD 109.6 ± 19.0 113.1 ± 19.00; P = 0.08 117.0 ± 18.1; P = 0.008DLSA-D (mm), mean ± SD 196.1 ± 91.5 198.1 ± 66.5Centreline curvature� 10 (1/mm), mean ± SD
P1 0.27 ± 0.07 0.35 ± 0.19; P = 0.06 0.47 ± 0.29; P = 0.05D1 0.09 ± 0.07 0.14 ± 0.09; P = 0.04 0.23 ± 0.12; P = 0.05TA 0.10 ± 0.02 0.19 ± 0.03; P = 0.3 0.21 ± 0.06; P = 0.08AsAo 0.18 ± 0.04 0.21 ± 0.05; P = 0.008 0.24 ± 0.10; P = 0.05ER 0.20 ± 0.03 0.19 ± 0.03; P = 0.05 0.20 ± 0.04; P = 0.1DsAo 0.1 ± 0.04 0.12 ± 0.06; P = 0.02 0.14 ± 0.04; P = 0.08
Outerline curvature� 10 (1/mm), mean ± SDP1 0.21 ± 0.06 0.29 ± 0.13; P = 0.055 0.39 ± 0.05; P = 0.05D1 0.13 ± 0.08 0.14 ± 0.07; P = 0.09 0.23 ± 0.10; P = 0.07
ASAo: ascending aorta; DAR-LSA: distance from the AR to the proximal edge of the left subclavian artery; D1: distal; DLSA-D: distance from the left subclavian arteryproximal edge to the distal landing zone; DsAo: descending aorta; ER: endografting region; P1: proximal; SD: standard deviation; TA: total aorta.
6 G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

specific adaptation between the endograft and the aortic wall de-pending on each type of morphology.
Therefore, with the currently available thoracic endoprosthe-ses, a total endovascular repair of the aortic arch requires devicesthat need to be customized for each patient’s anatomy andpathological condition, and often surgical left subclavian arteryrevascularization is required.
Thus, the hybrid procedure of the aortic arch, which includessupra-aortic vessels transposition to obtain an adequate proximallanding zone for TEVAR in zones 0, 1 and 2, has proved to be aneffective alternative, especially in high-risk patients, in an effort to
reduce perioperative death and complications related to opensurgical repair [13]. However, the long-term outcomes of the hy-brid treatment still remain a source of concern, and severe com-plications could occur during follow-up [14]. When passivelybent inside a highly curved artery as the aortic arch, the endog-raft exerted a spring-back force at the proximal and distal endsdue to the inherent tendency to recover its original straight status[15]. As already postulated, this spring-back force could cause anincrease in stress on the outer wall, especially at the endograftlanding zones, ultimately leading to endograft-related vessel inju-ries [16].
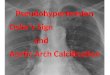
Figure 4: Pointwise curvature changes on centreline and outerline. Curvature changes at the proximal (P1) and the distal (D1) landing zones between preoperativeand postoperative configurations are highlighted. The left column concerns the centreline values, whereas in the right column, the vessel outerline is considered. Bothlines are coloured with respect to the pointwise curvature value: colour scale legend ranges from blue (minimum value) to red (maximum value).
CO
NV
ENTI
ON
AL
AO
RTI
CSU
RG
ERY
7G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

The aim of this study was to analyse the geometric changes ofthe aortic arch after the hybrid treatment, with particular focuson the endograft landing zones, attempting to enhance theunderstanding on the possible reasons for the development ofdevice-related complications.
Our results indicated that a hybrid treatment modifies themorphology of the aortic arch tract, with both a significantelongation of the vessel and an increase in the pointwise andmean curvature.
In particular, with regard to the centreline length, a mean in-crease of 5.3 mm (P = 0.010) was already observed at 1 monthafter the treatment and it increased to +12.3 mm (P = 0.001) at 1-year follow-up; this result is consistent with the outcomesreported by Nauta et al. [17] and Naguib et al. [18].
After the hybrid treatment, the local curvature of the centrelinewas significantly greater in the endograft proximal landing zonecompared to the preoperative configuration, which supports thefindings by Midulla et al. [19]. Moreover, we also observe a sig-nificant increase in the centreline local curvature at the distal fix-ation zone, for which no comparative results can be found in theliterature.
The significant increase in centreline curvature and outerlinecurvature at endograft landing points reveals the tendency of theendograft to spring back to its original straight status, as alreadypostulated by Dong et al. [15] and Janosi et al. [20] for aortic dis-sections treated with TEVAR. The possibility that the elastic recoilof the endograft might cause new entry tears in the proximal andthe distal landing zones has been described as well. On the basisof our data, we could assume that the force exerted by theendograft proximal and distal ends on the aortic wall might con-tribute to neck degeneration, which is ultimately related to an-eurysm formation or endoleak development. After intervention,the mean curvature of the centreline in the AsAo showed a sig-nificant increase, which positively correlated with an increase inthe reaction force on the wall [21], ultimately leading to the de-velopment of rTAAD [22]; such an increase in the mean curvaturewas higher in patients treated in the most proximal landing zone(i.e. zone 0). According to Chen et al. [23], the occurrence rate ofrTAAD in zone 0 was demonstrated to be higher than in otherlanding zones. Moreover, Redheuil et al. [24] previously demon-strated a strong correlation between proximal aortic arch mor-phological changes and left ventricular remodelling, togetherwith increases in the brachial blood pressure and the pulse pres-sures in subjects with no overt cardiovascular diseases. In add-ition, as documented by Kadoglou et al. [25], the pulse wavevelocity, a clinically recognized marker of arterial stiffness, signifi-cantly increased after TEVAR.
Differences of in vivo behaviour with different models ofendografts compared to their differences in the mechanical char-acteristics could help in designing future generations of endog-rafts with better conformability and thus lowering the risk ofintrinsic damages [26].
Our findings confirm that the aortic arch segment is a criticalzone for endograft apposition. As mentioned above, 2 complica-tions were observed at 1-month follow-up: 1 case of type IBendoleak and 1 case of rTAAD. The former patient exhibited anincrease in centreline curvature of 110% and outerline curvatureof 75% in the distal landing point, whereas in the latter, a signifi-cant increase in both outerline and centreline curvatures at theP1 level (more than 100% increase) along with a 22.5% increasein the centreline mean curvature of the AsAo were detected.
Our results stress the importance of continued surveillancewith CTA imaging for patients with this type of surgery to detectif any deformation or possible lesion at the impact point of thestent on the aorta outer wall will occur during follow-up.
Limitations
The main weakness of this study is the small number of enrolledpatients, although the sample size is consistent with recent stud-ies regarding quantitative assessment of aortic arch geometry [7].Another limitation relates to the absence of a standardizedprotocol for the acquisition of CTA images, which is due to theretrospective design of the study. In addition, CTA acquisitionswere not electrocardiogram (ECG) synchronized because thistechnique was not available at our centre for daily clinicalpractice. However, it is worth noting that even other studies,which are similar to the present one, did not make use of ECG-gated CTAs [7, 18, 19].
CONCLUSION
In conclusion, we have demonstrated that the hybrid treatment isassociated with a significant elongation of the vessel and a signifi-cant increase in curvature on the AsAo and on the endograft land-ing zones, which could be predictive of the development ofdevice-related complications. This issue reveals the need for furtherinvestigation into more conformable and dedicated endografts, oreven precurved endografts, for different thoracic aortic diseases.
Future studies involving the analysis of diameter changes andits correlation with aortic centreline elongation, endograft over-sizing and radial force on the proximal and the distal landingzones should be performed [27].
Conflict of interest: none declared.
REFERENCES
[1] Riambau V, Bockler D, Brunkwall J, Cao P, Chiesa R, Coppi G et al.Editor’s choice–management of descending thoracic aorta diseases: clin-ical practice guidelines of the European Society for vascular surgery(ESVS). Eur J Vasc Endovasc Surg 2017;53:4–52.
[2] Nation DA, Wang GJ. TEVAR: endovascular repair of the thoracic aorta.Semin Intervent Radiol 2015;32:265–71.
[3] Fanelli F, Dake MD. Standard of practice for the endovascular treatmentof thoracic aortic aneurysms and type B dissections. CardiovascIntervent Radiol 2009;32:849–60.
[4] Mitchell RS, Ishimaru S, Ehrlich MP, Iwase T, Lauterjung L, Shimono Tet al. First International Summit on Thoracic Aortic Endografting: round-table on thoracic aortic dissection as an indication for endografting.J Endovasc Ther 2002;9(Suppl 2):II98–105.
[5] Findeiss LK, Cody ME. Endovascular repair of thoracic aortic aneurysms.Semin Intervent Radiol 2011;28:107–17.
[6] Boufi M, Guivier-Curien C, Loundou AD, Deplano V, Boiron O,Chaumoitre K et al. Morphological analysis of healthy aortic arch. Eur JVasc Endovasc Surg 2017;53:663–70.
[7] Mestres G, Garcia ME, Yugueros X, Urrea R, Tripodi P, Gomez F et al.Aortic arch and thoracic aorta curvature remodeling after thoracicendovascular aortic repair. Ann Vasc Surg 2017;38:233–41.
[8] Antiga L, Piccinelli M, Botti L, Ene-Iordache B, Remuzzi A, Steinman DA.An image-based modeling framework for patient-specific computationalhemodynamics. Med Biol Eng Comput 2008;46:1097–112.
[9] Besl PJ, McKay ND. A method for registration of 3-D shapes. IEEE TransPattern Anal Mach Intell 1992;14:239–56.
8 G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019

[10] Piccinelli M, Veneziani A, Steinman DA, Remuzzi A, Antiga L. A frame-work for geometric analysis of vascular structures: application to cere-bral aneurysms. IEEE Trans Med Imaging 2009;28:1141–55.
[11] Girsowicz E, Georg Y, Lefebvre F, Lejay A, Thaveau F, Roy C et al.Anatomical study of healthy aortic arches. Ann Vasc Surg 2017;44:179–89.
[12] Alberta HB, Takayama T, Smits TC, Wendorff BB, Cambria RP, Farber MAet al. Aortic arch morphology and aortic length in patients with dissec-tion, traumatic, and aneurysmal disease. Eur J Vasc Endovasc Surg 2015;50:754–60.
[13] Milewski RK, Szeto WY, Pochettino A, Moser GW, Moeller P, Bavaria JE.Have hybrid procedures replaced open aortic arch reconstruction inhigh-risk patients? A comparative study of elective open arch debranch-ing with endovascular stent graft placement and conventional electiveopen total and distal aortic arch reconstruction. J Thorac CardiovascSurg 2010;140:590–7.
[14] Geisbusch P, Hoffmann S, Kotelis D, Able T, Hyhlik-Durr A,Bockler D. Reinterventions during midterm follow-up after endo-vascular treatment of thoracic aortic disease. J Vasc Surg 2011;53:1528–33.
[15] Dong Z, Fu W, Wang Y, Wang C, Yan Z, Guo D et al. Stent graft-inducednew entry after endovascular repair for Stanford type B aortic dissection.J Vasc Surg 2010;52:1450–7.
[16] Guan Y, Lin J, Dong Z, Wang L. Comparative study of the effect of struc-tural parameters on the flexibility of endovascular stent grafts. AdvMater Sci Eng 2018;2018:1.
[17] Nauta FJ, van Bogerijen GH, Trentin C, Conti M, Auricchio F, Moll FLet al. Impact of thoracic endovascular aortic repair on pulsatile circum-ferential and longitudinal strain in patients with aneurysm. J EndovascTher 2017;24:281–9.
[18] Naguib NN, Zima B, Nour-Eldin NE, Gruber-Rouh T, Fischer S, Schulz Bet al. Long-term changes in aortic length after thoracic endovascularaortic repair. J Vasc Interv Radiol 2016;27:181–7.
[19] Midulla M, Moreno R, Negre-Salvayre A, Nicoud F, Pruvo JP, Haulon Set al. Impact of endografting on the thoracic aortic anatomy: compara-tive analysis of the aortic geometry before and after the endograft im-plantation. Cardiovasc Intervent Radiol 2014;37:69–76.
[20] Janosi RA, Tsagakis K, Bettin M, Kahlert P, Horacek M, Al-Rashid F et al.Thoracic aortic aneurysm expansion due to late distal stent graft-induced new entry. Catheter Cardiovasc Interv 2015;85:E43–53.
[21] Poullis MP, Warwick R, Oo A, Poole RJ. Ascending aortic curvature as anindependent risk factor for type A dissection, and ascending aortic an-eurysm formation: a mathematical model. Eur J Cardiothorac Surg 2008;33:995–1001.
[22] Taguchi E, Nishigami K, Miyamoto S, Sakamoto T, Nakao K. Impact ofshear stress and atherosclerosis on entrance-tear formation in patientswith acute aortic syndromes. Heart Vessels 2014;29:78–82.
[23] Chen Y, Zhang S, Liu L, Lu Q, Zhang T, Jing Z. Retrograde type A aorticdissection after thoracic endovascular aortic repair: a systematic reviewand meta-analysis. J Am Heart Assoc 2017;6:9.
[24] Redheuil A, Yu WC, Mousseaux E, Harouni AA, Kachenoura N, Wu COet al. Age-related changes in aortic arch geometry: relationship withproximal aortic function and left ventricular mass and remodeling. J AmColl Cardiol 2011;58:1262–70.
[25] Kadoglou NPE, Moulakakis KG, Papadakis I, Ikonomidis I, Alepaki M,Spathis A et al. Differential effects of stent-graft fabrics on arterial stiff-ness in patients undergoing endovascular aneurysm repair. J EndovascTher 2014;21:850–8.
[26] Bussmann A, Heim F, Delay C, Girsowicz E, Del Tatto B, Dion D et al.Textile ageing characterization on new generations of explanted com-mercial endoprostheses: a preliminary study. Eur J Vasc Endovasc Surg2017;54:378–86.
[27] Alberta HB, Secor JL, Smits TC, Farber MA, Jordan WD, Azizzadeh A et al.Comparison of thoracic aortic diameter changes after endograft place-ment in patients with traumatic and aneurysmal disease. J Vasc Surg2014;59:1241–6.
CO
NV
ENTI
ON
AL
AO
RTI
CSU
RG
ERY
9G. Spinella et al. / European Journal of Cardio-Thoracic Surgery
Dow
nloaded from https://academ
ic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezy397/5233431 by R
ete Ligure Infor_Biomed user on 09 January 2019