Embed Size (px)
DESCRIPTION
killip
Citation preview

It has been shown that complex alterations in leftventricular geometry can occur after acute myocardialinfarction.1 These changes can profoundly affect leftventricular systolic and diastolic function and therebypatient outcome. It has been demonstrated that leftventricular dilatation may ensue in the earliest phaseof myocardial infarction.1-4 Early identification ofpatients in whom left ventricular dilatation is likely tooccur may have important therapeutic implications.Several sophisticated approaches5,6 have been pro-
posed to identify these patients, but many of them areexpensive, time consuming, and/or demand highlytrained personnel.
The aim of this study was to evaluate the associa-tion of Killip class on admission and the likelihood ofleft ventricular dilatation in the first year after myocar-dial infarction.
MethodsPatients
The study group consisted of 129 consecutive patientswith first acute myocardial infarction who met the followingcriteria: (1) age ≤70 years, (2) chest pain lasting >30 min-utes, (3) ST-segment elevation ≥2 mm in ≥2 electrocardio-graphic leads, (4) transient elevation of creatine kinaseand/or MB isoenzyme, and (5) echocardiogram performedwithin 24 hours from the onset of pain. Killip class onadmission was determined as the following: class 1 patientswere free of rales and a third heart sound; class 2 patients
Association of Killip class on admission and leftventricular dilatation after myocardial infarction: A closer look into an old clinical classificationAleksandar N. Neskovic, MD, Petar Otasevic, MD, Milovan Bojic, MD, PhD, and Aleksandar D. Popovic, MD, PhDBelgrade, Yugoslavia
Background Early identification of patients in whom left ventricular dilatation is likely to occur may have importanttherapeutic implications. Thus the purpose of this study was to evaluate the relation between Killip class on admission andsubsequent left ventricular dilatation after acute myocardial infarction.
Methods and Results We serially evaluated 129 consecutive patients by two-dimensional and Doppler echocar-diography on days 1, 2, 3, and 7, at 3 and 6 weeks, and at 3, 6, and 12 months after infarction. Killip class on admission>1 was found in 29 of 129 (22.5%) patients, and they had significantly higher end-systolic and end-diastolic volume indexesand wall motion score index from day 1 onward compared with patients with Killip class 1, whereas ejection fraction waslower during the follow-up period in these patients. Patients with Killip class >1 showed the progressive increase of end-dias-tolic (68.2 ± 2.99 to 88.0 ± 7.55 ml/m2, p = 0.001) and end-systolic volume indexes (43.9 ± 2.67 to 56.3 ± 6.18 ml/m2,p = 0.004) during the follow-up period, whereas ejection fraction and wall motion score index remained unchanged. Inpatients with Killip class 1, end-systolic volume index did not change (30.8 ± 1.06 to 33.8 ± 2.15 ml/m2, p = 0.064), ejec-tion fraction increased (49.3% ± 0.99% to 51.8% ± 1.17%, p = 0.027), and wall motion score index decreased (1.50 ±0.03 to 1.35 ± 0.04, p < 0.001). End-systolic volume index was the major independent correlate of Killip class, followed byhistory of diabetes and peak creatine kinase level. No association was found between Doppler indexes of diastolic fillingand Killip class on admission.
Conclusions Killip class >1 on admission is associated with both acute and long-term left ventricular dilatation. On theother hand, Killip class 1 is associated with favorable left ventricular functional indices, and it appears that left ventricularfunction in these patients may improve over time. Initial end-systolic volume index but not ejection fraction is the major corre-late of Killip class. (Am Heart J 1999;137:361-7.)
From the Cardiovascular Research Center, Dedinje Cardiovascular Institute and Bel-grade University Medical School.Presented in part at the XIXth Congress of the European Society of Cardiology,August 24-28, 1997, Stockholm, Sweden.Submitted October 23, 1997; accepted January 20, 1998.Reprint requests: Aleksandar D. Popovic, MD, PhD, Cardiovascular Research Center,Dedinje Cardiovascular Institute, Milana Tepica 1, 11040 Belgrade, Yugoslavia.Copyright © 1999 by Mosby, Inc.0002-8703/99/$8.00 + 0 4/1/89744

American Heart JournalFebruary 1999Nes kovic et al362
had rales up to 50% of each lung field regardless of thepresence of the third heart sound; class 3 patients had ralesin more than half of each lung field; and class 4 patientswere in cardiogenic shock.7 Killip class was assessed by asingle physician.
In 79 patients, intravenous streptokinase was adminis-tered in a dose of 1,500,000 U over 30 to 60 minutes. Theremaining 50 patients did not receive thrombolytic therapyat the discretion of their attending cardiologist because theywere admitted late after the onset of pain or they had con-traindication for thrombolysis.
EchocardiogramsComplete two-dimensional and Doppler echocardiographic
examinations were performed on days 1, 2, 3, and 7, at 3and 6 weeks, and 3, 6, and 12 months after acute myocardialinfarction, as a part of the study protocol. We used the Acu-son 128 imaging system (Mountain View, Calif.) with a 2.5
MHz transducer, and studies were stored on videotape forfurther analysis.
Left ventricular end-diastolic volume, end-systolic volume,and ejection fraction were determined from apical two- andfour-chamber views with Simpson’s biplane formula. Tracing ofendocardial borders in end-diastole and end-systole was per-formed in the technically best cardiac cycle. The volumes werenormalized to body surface area and expressed as indexes.
Transmitral flow recordings were obtained after quietexpiration at the tips of the mitral leaflets. Modal velocitywas traced in three consecutive beats and averaged. Studieswith atrial fibrillation, severe mitral regurgitation, and heartrate >100 beats/min were excluded. The following Dopplerindexes were measured: (1) early filling deceleration time,(2) peak early and (3) atrial filling velocities, and (4) theratio of peak early and atrial filling velocities.
Wall motion score index was calculated by dividing theleft ventricle into 16 segments according to the recommen-dations of the American Society of Echocardiography.8
Coronary angiographyCoronary angiography was performed in 108 patients
before hospital discharge as a part of the study protocol.Seventy percent area stenosis of the major coronary vesselwas considered significant. Patency of the infarct-relatedartery was assessed with Thrombolysis In Myocardial Infarc-tion (TIMI) criteria.9 Successful reperfusion was defined asTIMI grade 3.
Statistical analysisAll data are expressed as mean ± standard error. The chi-
square test and t test were used for comparisons between thesubgroups for categorical and continuous variables, respec-tively. A p value < 0.05 was considered significant. A multiplelogistic regression model (that included age, sex, history of
Killip class 1 Killip class >1 p Value
Age (years) 54.5 ± 0.88 58.1 ± 1.54 0.045Sex (F/M) 24/76 12/17 NSDiabetes mellitus 13/99 (13.1%) 11/28 (39.3%) 0.002Hypertension 37/99 (37.4%) 11/28 (39.3%) NSCigarette smoking 62/99 (62.6%) 7/28 (25%) 0.001Anterior infarct 34/100 (34%) 19/29 (65.5%) 0.002Q-wave infarction 87/100 (87%) 28/29 (96.5%) NSPeak CK level (IU/L) 964 ± 61.34 1607 ± 250.64 0.001Thrombolysis 32/100 (32%) 18/29 (62.1%) 0.003Multivessel CAD 51/89 (57.3%) 9/19 (68.4%) NSTIMI <3 39/89 (43.8%) 13/19 (68.4%) NSDiuretics 30/97 (30.9%) 20/27 (74.1%) 0.0001ACE inhibitors 6/97 (6.2%) 9/27 (29.6%) 0.0001Digoxin 6/97 (6.2%) 8/27 (29.6%) 0.00011-Year mortality 3/100 (3%) 9/29 (31%) 0.001
Values are given as mean ± standard error. NS, nonsignificant.
Table I. Clinical and angiographic characteristics
p Value
Initial end-systolic volume index 0.0004Diabetes mellitus 0.0044Peak creatine kinase level 0.0048Age 0.059Smoking 0.131Initial wall-motion score index 0.186Thrombolysis 0.291Sex 0.361Initial ejection fraction 0.417Extent of coronary artery disease 0.454Initial end-diastolic volume index 0.516Patency of the infarct-related artery 0.619Infarct location 0.620
Table II. Independent correlates of Killip class on admission

American Heart JournalVolume 137, Number 2 Nes kovic et al 363
smoking and diabetes, infarct location, peak creatine kinaselevel, thrombolysis, initial end-diastolic volume index, end-systolic volume index, ejection fraction, and wall motionscore index, extent of coronary artery disease, and patencyof the infarct-related artery) was used for identification ofindependent correlates of Killip class on admission.
ResultsKillip class 1 was found in 100 of 129 (77.5%)
patients; Killip class >1 was found in 29 of 129 (22.5%)
patients (26 patients with class 2 and 3 patients withclass 3) on admission. Baseline clinical and angio-graphic characteristics of patients enrolled are shownin Table I. Patients with Killip class 1 and Killip class>1 were similar regarding sex, history of hypertension,incidence of Q-wave infarction, extent of coronaryartery disease, and patency of the infarct-relatedartery. However, in patients with Killip class >1 therewas a higher incidence of diabetes and anterior infarc-tion and a lower incidence of cigarette smoking; in
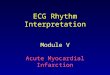
Figure 1
A, Association of end-diastolic volume and Killip class 1 year after myocardial infarction. EDVi, End-diastolic vol-ume index.*p < 0.01 between groups; †p < 0.001 between groups. B, Association of end-systolic volume and Kil-lip class 1 year after myocardial infarction. ESVi, End-systolic volume index.*p < 0.01 between groups; †p <0.001 between groups. Values are given as mean ± standard error.

American Heart JournalFebruary 1999Nes kovic et al364
addition, they were older, had higher peak creatinekinase level, and had higher 1-year mortality rates.Thrombolysis, diuretics, digoxin, and angiotensin-con-verting enzyme (ACE) inhibitors were more frequentlyused in patients with Killip class >1. Likewise, the useof ACE inhibitors and diuretics was more common inthese patients during the follow-up period. However,the rate of myocardial revascularization was similar inboth groups.
Multiple logistic regression identified end-systolicvolume index as the major independent correlate ofKillip class, followed by history of diabetes and peakcreatine kinase level (Table II).
Patients with Killip class >1 had significantly higherleft ventricular end-diastolic and end-systolic volumeindexes (Fig. 1, A and B), and left ventricular wallmotion score index (Fig. 2) from day 1 onward com-pared with patients with Killip class 1. Conversely,
ejection fraction was significantly lower during thefollow-up period in patients with Killip class >1 (Fig.3). Patients with Killip class >1 showed progressiveincrease of end-diastolic (68.2 ± 2.99 to 88.0 ± 7.55ml/m2, p = 0.001) and end-systolic volume indexes(43.9 ± 2.67 to 56.3 ± 6.18 ml/m2, p = 0.004) duringthe follow-up period; ejection fraction (37.0% ±1.94% to 38.1% ± 2.50%, p = 0.66) and wall motionscore index (1.79 ± 0.08 to 1.77 ± 0.12, p = 0.84)remained unchanged. However, in patients with Kil-lip class 1, despite an increase in end-diastolic vol-ume index (59.7 ± 1.15 to 67.2 ± 2.52 ml/m2, p <0.001), end-systolic volume index did not change(30.8 ± 1.06 to 33.8 ± 2.15 ml/m2, p = 0.064); in addi-tion, ejection fraction increased (49.3% ± 0.99% to51.8% ± 1.17%, p = 0.027) and wall motion scoreindex decreased (1.50 ± 0.03 to 1.35 ± 0.04, p <0.001) at 1 year.
Figure 2
Association of wall motion score index and Killip class 1 year after myocardial infarction. WMSi, Wall motionscore index. †p < 0.001 between groups. Values are given as mean ± standard error.
Doppler indexes Killip class 1 Killip class >1 p Value
Early filling deceleration time (msec) 184 ± 6.93 164 ± 11.25 0.15Peak E-wave velocity (m/sec) 0.52 ± 0.01 0.46 ± 0.06 0.42Peak A-wave velocity (m/sec) 0.58 ± 0.02 0.58 ± 0.04 0.99E/A ratio 1.01 ± 0.07 0.82 ± 0.11 0.16
Values are given as mean ± standard error.
Table III. Doppler indexes of left ventricular filling

American Heart JournalVolume 137, Number 2 Nes kovic et al 365
No association was found between Killip class andmeasured Doppler indexes of left ventricular filling(Table III).
DiscussionOur findings demonstrate that Killip class on admis-
sion may predict subsequent left ventricular dilatationand changes in left ventricular systolic function in 1year after myocardial infarction. The evidence of heartfailure on admission identifies patients who willincrease both end-diastolic and end-systolic volume inthe following period. White et al.10 have demonstratedthat end-systolic volume is the major determinant ofsurvival in patients after myocardial infarction. Simi-larly, our patients with Killip class >1 had higher end-systolic volume from day 1 onward, which was trans-lated into a higher 1-year mortality rate. On the otherhand, our data revealed that patients in Killip class 1on admission would not increase their end-systolicvolume and were likely to improve ejection fractionand regional wall motion over 1 year after infarction. Itis well known that clinical evidence of heart failureafter acute myocardial infarction is usually presentwhen the region of abnormal contraction exceeds 20%to 25% of the total left ventricular perimeter deter-mined by angiography,11 and both animal12 and clini-cal studies13 have demonstrated that left ventricular
dilatation is related to the extent of myocardial necro-sis in a linear fashion. In addition to infarct size,14-16
anterior infarct location17 and patency of the infarct-related artery18 have been identified as major predic-tors of left ventricular dilatation after myocardialinfarction. We found that patients with Killip class >1had larger infarcts, more extensive regional wallmotion abnormalities, and more frequently had ante-rior infarction. Furthermore, initial end-systolic volumeand peak creatine kinase level were identified as theindependent correlates of Killip class.
Although we have previously shown that early fillingdeceleration time correlates with infarct size,19 noassociation was found between Killip class and this aswell as with the other indexes of left ventricular dias-tolic function. It has been reported that the ratio ofpeak early and atrial filling velocities was not helpfulin identifying patients with pump failure after myocar-dial infarction.20
Left ventricular enlargement after myocardial infarc-tion is associated with decreased survival from conges-tive heart failure,21 and the risk of death is directlyrelated to left ventricular size.22 According to ourstudy, it appears that by using simple clinical Killipclassification, patients in whom left ventricular dilata-tion is likely to occur can be identified on admission.This is extremely important because attempts to pre-
Figure 3
Association of ejection fraction and Killip class 1 year after myocardial infarction. EF, Ejection fraction. †p <0.001 between groups. Values are given as mean ± standard error.

American Heart JournalFebruary 1999Nes kovic et al366
vent or minimize this process can be initiated immedi-ately. Because infarct size is the major determinant ofleft ventricular dilatation, an energetic attempt towardits reduction should be made by using thrombolysis,23-25
or direct26 or rescue angioplasty.27 Favorable effectson left ventricular volumes, probably through modifi-cation of distending or deforming forces, have beendemonstrated for ACE inhibitors28 and intravenousnitroglycerin.29 Considering possible hazards of theadministration of ACE inhibitors during first hours ofinfarction,10 identification of patients prone to left ven-tricular dilatation by using Killip classification onadmission may allow early administration of theseagents only in selected patients who are likely to ben-efit the most and to avoid or postpone their use inothers. Also, there is a wealth of evidence demonstrat-ing that the administration of an ACE inhibitor within afew days after acute myocardial infarction markedlyreduces mortality rates in patients with impaired leftventricular function.31
LimitationsThe major limitation of the study is the small num-
ber of patients in Killip class 3 and the fact that noneof them was in Killip class 4. However, when only Kil-lip class 1 and 2 patients were included in the analysis,the results were the same. Also, because electrocardio-graphic inclusion criterion required at least 2 mm ofST-segment elevation, it is possible that severalpatients with small infarcts were not included in thestudy. Because they would probably be Killip class 1patients, we believe that their potential exclusion didnot affect the results of the study.
In conclusion, our data demonstrate that Killip classon admission can be used to identify patients in whomleft ventricular dilatation is likely to occur after myocar-dial infarction. Early identification of these patientswith the use of simple clinical classification may haveimportant therapeutic implications. Killip class >1 isassociated with both acute and long-term dilatation. Onthe other hand, Killip class 1 is associated with favor-able left ventricular functional indices, and it appearsthat left ventricular function in these patients mayimprove over time. Initial end-systolic volume but notejection fraction is the major correlate of Killip class.
References1. McKay RG, Pfeffer MA, Pasternak RC, Markis JE, Come PC, Nakao
S, et al. Left ventricular remodeling after acute myocardial infarction: acorollary to infarct expansion. Circulation 1986;74:693-702.
2. Erlebacher JA, Weiss JL, Eaton LW, Kallman C, Weisfeldt ML, BulkleyBH. Late effects of acute infarct dilation on infarct size: a two-dimen-sional echocardiographic study. Am J Cardiol 1982;49:1120-6.
3. Picard MH, Wilkins GT, Ray PA, Weyman AE. Natural history of leftventricular size and function after acute myocardial infarction: assess-ment and prediction by echocardiographic endocardial surface map-ping. Circulation 1990;82:484-94.
4. Popovic AD, Nes kovic AN, Babic R, Obradovic V, Bozinovic LJ,Marinkovic J, et al. Independent impact of thrombolytic therapy andvessel patnecy on left ventricular dialtion after myocardial infarction:serial echocardiographic follow-up. Circulation 1994;90:800-7.
5. Chareonthaitawee P, Christian TF, Hirose K, Gibbons RJ, RumbergerJA. Relation of initial infarct size to extent of left ventricular remodelingin the year after acute myocardial infarction. J Am Coll Cardiol1995;25:567-73.
6. Gaudron P, Eilles C, Kugler I. Ertl G. Progressive left ventricular dys-function and remodeling after myocardial infarction: potential mecha-nisms and early predictors. Circulation 1993;87:755-63.
7. Killip T, Kimball JT. Treatment of myocardial infarction in coronary careunit. A two-year experience with 250 patients. Am J Cardiol1967;20:457-67.
8. Schiller N, Shah PM, Crawford M, DeMaria A, Devereux R, Feigen-baum H, et al. Recommendations for quantitation of the left ventricleby two-dimensional echocardiography. J Am Soc Echocardiogr1989;2:358-68.
9. The TIMI study group. The thrombolysis in myocardial infarction (TIMI)trial. N Engl J Med 1985;312:932-6.
10. White HD, Norris RM, Brown MA, Brandt PWT, Whitlock RML, WildCJ. Left ventricular end-systolic volume as the major determinant of sur-vival after recovery from myocardial infarction. Circulation1987;76:44-51.
11. Klein MD, Herman MV, Gorlin RG. A hemodynamic study of left ven-tricular aneurysm. Circulation 1967;35:614-25.
12. Hochman JS, Choo H. Limitation of myocardial infarct expansion byreperfusion independent of myocardial salvage. Circulation1987;75:299-306.
13. Picard MH, Wilkins GT, Ray PA, Weyman AE. Progressive changes inventricular structure and function during the year following acutemyocardial infarction. Am Heart J 1992;124:24-31.
14. Fletcher PJ, Pfeffer JM, Pfeffer MA, Braunwald E. Left ventricular dias-tolic pressure-volume relations in rats with healed myocardial infarction.Circ Res 1981;49:618-26.
15. Jeremy RW, Allman KC, Bautowich G, Harris PJ. Patterns of left ventric-ular dilatation during the six months after myocardial infarction. J AmColl Cardiol 1989;13:304-10.
16. Peels KH, Visser CA, Dambrink JHE, Jaarsma W, Wielenga RP, KampO, et al. Left ventricular wall motion score as an early predictor of leftventricular dilation and mortality after first anterior infarction treatedwith thrombolysis. Am J Cardiol 1996;77:1149-54.
17. Warren SE, Royal H, Markis JE, Grossman W, McKay R. Time courseof left ventricular dilatation after myocardial infarction: influence ofinfarct-related artery and success of coronary thrombolysis. J Am CollCardiol 1988;11:12-9.
18. Jeremy RW, Hackworthy RA, Bautowich G, Hutton BF, Harris PJ. Infarctartery perfusion and changes in left ventricular volume in the monthafter acute myocardial infarction. J Am Coll Cardiol 1987;9:989-95.
19. Popovic AD, Neskovic AN, Marinkovic J, Lee J-C, Tan M, Thomas JD.Serial assessment of left ventricular chamber stiffness after acutemyocardial infarction. Am J Cardiol 1996;77:361-4.

American Heart JournalVolume 137, Number 2 Nes kovic et al 367
20. Delemarre BJ, Visser CA, Bot H, de Koning HJ, Dunning AJ. Predictivevalue of pulsed Doppler echocardiography in acute myocardial infarc-tion. J Am Soc Echocardiogr 1989;2:102-9.
21. Multicenter Postinfarction Research Group. Risk stratification and sur-vival after myocardial infarction. N Engl J Med 1983;309:331-6.
22. Pfeffer MA, Pfeffer JM. Ventricular enlargement and reduced survivalafter myocardial infarction. Circulation 1987;75(suppl 4):IV-93-7.
23. Gruppo Italiano per lo Studio della Streptochinasi nell’ Infarto Miocardico(GISSI). Long-term effect of intravenous thrombolysis in acute myocardialinfarction: Final report of the GISSI study. Lancet 1987;2:871-4.
24. The GUSTO Angiographic Investigators. The effects of tissue plasmino-gen activator, streptokinase, or both on coronary artery patency, ven-tricular function, and survival after acute myocardial infarction. N EnglJ Med 1993;329:673-82.
25. Popovic AD, Neskovic AN, Marinkovic J, Thomas JD. Acute and long-term effects of thrombolysis after anterior wall acute myocardial infarc-tion with serial assessment of infarct expansion and late ventricularremodeling. Am J Cardiol 1996;77:446-50.
26. O’Neill W, Weintraub R, Grines CL. A prospective, placebo con-trolled, randomized trial of intravenous streptokinase and angioplastyversus lone angioplasty therapy of acute myocardial infarction. Circu-lation 1992;86:1710-7.
27. Abbottsmith CW, Topol EJ, George BS. Fate of patients with acutemyocardial infarction with patency of infarct-related artery achievedwith successful thrombolysis versus rescue angioplasty. J Am Coll Car-diol 1991;18:1594-601.
28. St John Sutton M, Pfeffer MA, Plappert T, Rouleau J-L, Moyé LA,Dagenais GR, et al. Quantitative two-dimensional echocardiographicmeasurements are major predictors of adverse cardiovascular eventsafter acute myocardial infarction. The protective effects of captopril.Circulation 1994;89:68-75.
29. Jugdutt BI, Warnica JW. Intravenous nitroglycerin therapy to limitmyocardial infarct size, expansion, and complications: effect of timing,dosage, and infarct location. Circulation 1988;78:906-19.
30. Swedburg K, Held P, Kjekshus J, Rasmussen K, Ryden L, Wedel H,on behalf of the CONSENSUS II Study Group. Effects of earlyadministration of enalapril on mortality in patients with acute myocar-dial infarction. Results of the Cooperative North ScandinavianEnalapril Survivial Study II (CONSENSUS II). N Engl J Med1992;327:678-84.
31. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators.Effect of ramipril on mortality and morbidity of survivors of acutemyocardial infarction with clinical evidence of heart failure. Lancet1993;342:821-8.