Embed Size (px)
Citation preview

Atherosclerosis, Atherosclerosis, Dyslipidaemia and Dyslipidaemia and
DiabetesDiabetes

Section 1 - Epidemiology and Risk Factors Section 2 - Classification of Dyslipidaemias and Pathogenesis
of Atherosclerosis Section 3 - Lipoproteins and Lipid Metabolism Section 4 - Guidelines and Unmet Need Section 5 - Statins and Lipid-modifying Therapies Section 6 - Key Statin Trials Section 7 - Diabetes: a Risk Factor for CHD? Section 8 - The Metabolic Syndrome Section 9 - Outcome Trials in Diabetes
Atherosclerosis, Dyslipidaemia and Atherosclerosis, Dyslipidaemia and Diabetes Diabetes ContentsContents

Section 1 Section 1
Epidemiology and Risk FactorsEpidemiology and Risk Factors

0
500
1000
CVD deathsCHD deaths
Mortality from CVD and CHD in Mortality from CVD and CHD in Selected CountriesSelected Countries
Mor
talit
y ra
te p
er 1
00
,00
0 p
opu
lati
onM
orta
lity
rate
per
10
0,0
00
pop
ula
tion
(men
aged
35
(men
aged
35 -
- 74
yea
rs)
74
yea
rs)
Adapted from I nternational Cardiovascular Disease Statistics 200Adapted from I nternational Cardiovascular Disease S tatistics 200 3; American Heart Association3; American Heart Association

The Framingham Study: The Framingham Study: Relationship Between Cholesterol Relationship Between Cholesterol
and CHD Riskand CHD Risk
0
Adapted from Castelli WP. Am J Med 1984;76:4–12
25
50
75
100
125
150
<204 205–234 235–264 265–294 >295
CHD
inci
denc
e pe
r 10
00
Serum cholesterol (mg/100 mL)

35
Seven Countries Study: Seven Countries Study: Relationship of Relationship of Serum Cholesterol to MortalitySerum Cholesterol to Mortality
Adapted from Verschuren WM et al. J Am Med Assoc 1995;274(2):131–136
Serum total cholesterol (mmol/L)
30
25
20
15
10
5
0
Dea
th r
ate
from
CH
D/1
000
men
2.60 3.25 3.90 4.50 5.15 5.80 6.45 7.10 7.75 8.40 9.05
Northern Europe
United States
Southern Europe, Inland
Southern Europe, Mediterranean
Japan
Serbia

Cholesterol: A Modifiable Cholesterol: A Modifiable Risk FactorRisk Factor
In the USA, 37% (102 million) have elevated total cholesterol (>200 mg/dL, 5.2 mmol/L)1
In EUROASPIRE II, 58% of patients with established CHD had elevated cholesterol (5 mmol/L, 190 mg/dL)2
10% reduction in total cholesterol results in: 15% reduction in CHD mortality (p<0.001) 11% reduction in total mortality (p<0.001)3
LDL-cholesterol is the primary target to prevent CHD
Adapted from: 1. American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Adapted from: 1. American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Study Group. Study Group. Eur Heart JEur Heart J 2001; 2001;2222:554–572; 3. Gould AL :554–572; 3. Gould AL et al. Circulationet al. Circulation 1998; 1998;9797:946–952:946–952

Risk Factors for Cardiovascular DiseaseRisk Factors for Cardiovascular Disease
Modifiable Smoking Dyslipidaemia
• Raised LDL-cholesterol• Low HDL-cholesterol• Raised triglycerides
Raised blood pressure Diabetes mellitus Obesity Dietary factors Thrombogenic factors Lack of exercise Excess alcohol consumption
Non-modifiable Personal history of CHD Family history of CHD Age Gender
Adapted from: Pyörälä K Adapted from: Pyörälä K et al. Eur Heart Jet al. Eur Heart J 1994; 1994;1515:1300–1331:1300–1331

Levels of Risk Associated with Smoking, Levels of Risk Associated with Smoking, Hypertension and HypercholesterolaemiaHypertension and Hypercholesterolaemia
x1.6 x4
x3
x6
x16x4.5 x9
HypertensionHypertension(SBP 195 mmHg)(SBP 195 mmHg)
Serum cholesterol levelSerum cholesterol level(8.5 mmol/L, 330 mg/dL)(8.5 mmol/L, 330 mg/dL)
SmokingSmoking
Adapted from Poulter N et al., 1993

Section 2Section 2
Classification of Dyslipidaemias and Classification of Dyslipidaemias and Pathogenesis of AtherosclerosisPathogenesis of Atherosclerosis

Classification of Dyslipidaemias:Classification of Dyslipidaemias:Fredrickson (WHO) ClassificationFredrickson (WHO) Classification
LDL – low-density lipoprotein; IDL – intermediate-density lipoprotein; VLDL – very low-density lipoprotein. (High-density lipoprotein (HDL) cholesterol levels are not consideredin the Fredrickson classification.)
Phenotype
I
IIa
IIb
III
IV
V
Lipoproteinelevated
Chylomicrons
LDL
LDL and VLDL
IDL
VLDL
VLDL and chylomicrons
Atherogenicity
None seen
+++
+++
+++
+
+
Prevalence
Rare
Common
Common
Intermediate
Common
Rare
Serumcholesterol
Normal to
Normal to
Normal to
Serumtriglyceride
Normal
Adapted from Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391

Normal Arterial WallNormal Arterial Wall
Tunica adventitiaTunica mediaTunica intima
Endothelium
Subendothelial connective tissue
Smooth muscle cellInternal elastic membrane
Elastic/collagen fibres
External elastic membrane
Adapted from Weissberg PL. Eur Heart J Supplements 1999:1:T13–18

Pathogenesis of Atherosclerotic Pathogenesis of Atherosclerotic PlaquesPlaques
Protective response results in production of cellular adhesion molecules
Monocytes and T lymphocytes attach to ‘sticky’ surface of endothelial cells
Migrate through arterial wall to subendothelial space
Lipid-rich foam cells
Endothelial damage
Macrophages take up oxidised LDL-cholesterol
Fatty streak and plaque

CELLULAR ADHESION MOLECULES
induces cell proliferation and a prothrombic state
activated activated endotheliumendothelium
attracts monocytes and T lymphocytes
which adhere to endothelial cells
cytokines (e.g. IL-1, TNF-)
chemokines (e.g.MCP-1, IL-8)
growth factors (e.g. PDGF, FGF)
Adapted from Koenig W. Eur Heart J 1999;1(Suppl T);T19–26
The ‘Activated’ EndotheliumThe ‘Activated’ Endothelium

Adapted from Adapted from Ross RRoss R. N Engl J Med. N Engl J Med 1999; 1999;362362:115–126:115–126
Endothelial Dysfunction in Endothelial Dysfunction in AtherosclerosisAtherosclerosis
Upregulation of endothelial
adhesion molecules
Increased endothelial
permeability
Migration of leukocytesinto the
artery wall
Leukocyteadhesion

Adapted from Ross R. N Engl J Med 1999;362:115–126
Fatty Streak Formation in Fatty Streak Formation in AtherosclerosisAtherosclerosis
Formationof foam cells
Activation of T cells
Adherence and aggregation ofplatelets
Adherence andentry of
leukocytes
Migration ofsmooth
muscle cells

Adapted from Ross R. N Engl J Med 1999;362:115–126
Formation of the Complicated Formation of the Complicated Atherosclerotic PlaqueAtherosclerotic Plaque
Formation of the fibrous cap
Accumulation ofmacrophages
Formation ofnecrotic core

Adapted from Ross R. N Engl J Med 1999;362:115–126
The Unstable Atherosclerotic PlaqueThe Unstable Atherosclerotic Plaque
Rupture of the
fibrous cap
Thinning of thefibrous cap Haemorrhage from
plaquemicrovessels

Adapted from Weissberg PL. Eur Heart J Supplements 1999:1:T13–18
Atherosclerotic Plaque Rupture and Atherosclerotic Plaque Rupture and Thrombus FormationThrombus Formation
Intraluminal thrombus Growth of thrombus
Intraplaque thrombus Lipid pool
Blood FlowBlood Flow

Adapted from Libby P. Circulation 1995;91:2844–2850
The Synthesis and Breakdown ofThe Synthesis and Breakdown of Atheromatous Plaques

Adapted from Libby P. Circulation 1995;91:2844–2850
The Vulnerable Atherosclerotic PlaqueThe Vulnerable Atherosclerotic Plaque

Clinical Manifestations of Clinical Manifestations of AtherosclerosisAtherosclerosis
Coronary heart disease Angina pectoris, myocardial infarction,
sudden cardiac death Cerebrovascular disease
Transient ischaemic attacks, stroke Peripheral vascular disease
Intermittent claudication, gangrene

Section 3Section 3
Lipoproteins and Lipid MetabolismLipoproteins and Lipid Metabolism

Structure of LipoproteinsStructure of Lipoproteins
Free cholesterol
Phospholipid Triglyceride
Cholesteryl esterApolipoprotein

Classification of LipoproteinsClassification of Lipoproteins
Based on density: Chylomicrons Very low-density lipoprotein (VLDL) Intermediate-density lipoprotein (IDL) Low-density lipoprotein (LDL) High-density lipoprotein (HDL)

LDL-CholesterolLDL-Cholesterol
Strongly associated with atherosclerosisand CHD events
10% increase results in a 20% increasein CHD risk
Risk associated with LDL-C is increased by other risk factors: low HDL-cholesterol smoking hypertension diabetes

TriglyceridesTriglycerides Associated with increased risk of CHD events Link with increased CHD risk is complex
may be related to:• low HDL levels• highly atherogenic forms of LDL-cholesterol• hyperinsulinaemia/insulin resistance• procoagulation state• hypertension• abdominal obesity
May have accompanying dyslipidaemias Normal triglyceride levels <150 mg/dL Very high triglycerides (>1000 mg/dL,
11.3 mmol/L) increase pancreatitis risk

HDL-CholesterolHDL-Cholesterol
HDL-cholesterol has a protective effect for risk of atherosclerosis and CHD
The lower the HDL-cholesterol level, the higher the risk for atherosclerosis and CHD low level (<40 mg/dL) increases risk
HDL-cholesterol tends to be low when triglycerides are high
HDL-cholesterol is lowered by smoking, obesity and physical inactivity

ApolipoproteinsApolipoproteins
Main protein content of lipoproteins Functions include:
Facilitation of lipid transport Activation of three enzymes in lipid
metabolism• lecithin cholesterol acyltransferase
(LCAT)• lipoprotein lipase (LPL)• hepatic triglyceride lipase (HTGL)
Binding to cell surface receptors

IntestineIntestine
Skeletal muscleSkeletal muscle
Adipose tissue
Adipose tissue
ChylomicronChylomicron
Chylomicron remnant
Chylomicron remnant
Remnant receptorRemnant receptor
LiverLiver
Dietary triglycerides and cholesterol
Dietary triglycerides and cholesterol
LP lipaseLP lipase
Exogenous Pathway of Lipid Metabolism
Exogenous Pathway of Lipid Exogenous Pathway of Lipid MetabolismMetabolism
to atheromato atheroma
FFAFFA

Endogenous Pathway of Lipid Metabolism
Endogenous Pathway of Lipid Endogenous Pathway of Lipid MetabolismMetabolism
IDLIDLIDL
Large VLDL
Large VLDL
SmallVLDLSmallVLDL
LDLreceptorLDLreceptor
LiverLiver
LPL Lipoprotein lipaseLPL Lipoprotein lipase
HL Hepatic lipaseHL Hepatic lipase
LDLLDL
LPLLPL
LPLLPL
LPLLPL
HLHL
HLHL
HLHL

Reverse cholesterol transportReverse Cholesterol Transport
Peripheraltissuestissues
CellCellmembranemembrane
VLDL, IDL, LDLVLDL, IDL, LDL
LDLLDL receptorreceptor
LCATLCAT CETPCETPFCFC
CECECECE
TGTGHDLHDL HDL3HDL3
TGTGCECE
Free cholesterolFree cholesterolTriglyceridesTriglyceridesCholesterol estersCholesterol esters
CETPCETP Cholesteryl ester transfer proteinCholesteryl ester transfer proteinLCATLCAT Lecithin cholesterol acyl transferaseLecithin cholesterol acyl transferase
SRB1SRB1
FCFC
ABCA1ABCA1
LiverLiver

Section 4Section 4
Guidelines and Unmet NeedGuidelines and Unmet Need

Joint European Guidelines: ESC, Joint European Guidelines: ESC, EAS, ESH, ISBM, ESGP/FM, EHN EAS, ESH, ISBM, ESGP/FM, EHN
Estimate absolute CV risk using chart and initial TC value
Absolute CHD risk <20% over 10 years, TC 5 mmol/L
Absolute CHD risk 20% over 10 years
Measure fasting lipids, give lifestyle advice, with repeat lipids after
3 months
Lifestyle adviceAim: TC<5 mmol/L and
LDL-C <3.0 mmol/L Follow-up at 5-year intervals
TC <5 mmol/L and LDL-C <3.0 mmol/LMaintain lifestyle advice with annual
follow-up
TC 5 mmol/L and/or LDL-C 3 mmol/LMaintain lifestyle advice with drug
therapy
Adapted from Wood D et al. Atherosclerosis 1998;140:199–270

NCEP ATP III: Focus on NCEP ATP III: Focus on Multiple Risk factorsMultiple Risk factors
Uses Framingham projections of 10-year absolute CHD risk to identify certain patients with 2 risk factors for more intensive treatment
Raises persons with diabetes without CHD to the level of CHD risk equivalent
Identifies persons with multiple metabolic risk factors (metabolic syndrome) as candidates for intensified TLC*
National Cholesterol Education Program, Adult Treatment Panel III, 2001. JAMA 2001:285;2486–2497
*TLC: therapeutic lifestyle changes*TLC: therapeutic lifestyle changes

NCEP ATP III: Modifications of NCEP ATP III: Modifications of Lipid ClassificationLipid Classification
Identifies LDL-cholesterol <100 mg/dL (2.6 mmol/L) as optimal
Raises categorical low HDL-cholesterol from <35 to <40 mg/dL (<0.9 to <1 mmol/L)
Lowers TG cutpoints to: normal: <150 mg/dL (<1.7 mmol/L) borderline high: 150–199 mg/dL
(1.7–2.2 mmol/L) high: 200–499 mg/dL (2.2–5.6 mmol/L) very high: 500 mg/dL (5.6 mmol/L)
National Cholesterol Education Program, Adult Treatment Panel III, 2001. JAMA 2001:285;2486–2497

NCEP ATP III GuidelinesNCEP ATP III Guidelines
Patients withPatients with Drug therapy Drug therapy considered if LDLconsidered if LDL-C
* TLC: therapeutic lifestyle changes* TLC: therapeutic lifestyle changes
National Cholesterol Education Program, Adult Treatment Panel III. National Cholesterol Education Program, Adult Treatment Panel III. JAMA JAMA 2001;2001;285285:2486–2497:2486–2497
Initiate TLC* Initiate TLC* if LDLif LDL-CC
LDLLDL-C C treatment treatment
goalgoal
00-1 risk factors1 risk factors 160 mg/dL160 mg/dL†† 190 mg/dL 190 mg/dL (160(160 – 189 mg/dL:189 mg/dL:
drug optional)drug optional)
<160 mg/dL<160 mg/dL††
2 risk factors2 risk factors(10(10-year risk year risk 20%)20%)
130 mg/dL130 mg/dL†† -1010 year risk 10year risk 10–
20%: 20%: 130 mg/dL 130 mg/dL 10-year risk <10%:10-year risk <10%:
160 mg/dL160 mg/dL
<130 mg/dL<130 mg/dL††
CHD and CHD risk CHD and CHD risk equivalentsequivalents(10(10- year risk >20%)year risk >20%)
100 mg/dL100 mg/dL†† <100 mg/dL<100 mg/dL††
†† 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L
130 mg/dL 130 mg/dL
drug optional)drug optional)(100–129 mg/dL:(100–129 mg/dL:

NCEP ATP III: LDL-Cholesterol Goals NCEP ATP III: LDL-Cholesterol Goals
National Cholesterol Education Program, Adult Treatment Panel III, 2001. JAMA 2001:285;2486–2497
CHD or CHD risk
equivalents
<2 risk factors
≥2 risk factors
LDL-
chol
este
rol l
evel
100 -
160 -
130 -
190 -
Target 100mg/dL
Target 130mg/dL
Target 160mg/dL
100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L

NCEP ATP III Guidelines Increase the NCEP ATP III Guidelines Increase the Number of Patients Eligible for TreatmentNumber of Patients Eligible for Treatment
RiskRisk NCEP NCEP ATP IIATP II
NCEP NCEP ATP IIIATP III
% increase in % increase in drug-eligible drug-eligible
patientspatients
HighHighModerate Moderate LowLow
TotalTotal
8,6128,61219,55519,5551,2641,264
29,43129,431
14,71314,71323,66323,6631,2641,264
39,64039,640
7171212100
3535
Adapted from Davidson MH. Am J Cardiol 2002;89(Suppl 5A):1C–2C

L-TAP: Achieving NCEP ATP II Goal L-TAP: Achieving NCEP ATP II Goal on Lipid-modifying Therapyon Lipid-modifying Therapy
0
20
40
60
80
100Pe
rcen
tage
of p
atie
nts
85% of patients
received lipid-modifying therapy
39% of patients receiving
lipid-modifying therapy reached
NCEP ATP II LDL-C goal
* LDL-C 100 mg/dL
(n=4888) (n=4137)
<20% of CHD patients who receiving lipid-modifying
therapy reached NCEP ATP II LDL-C goal*
(n=1352)
Adapted from Pearson TA et al. Arch Intern Med 2000;160:459–467

EUROASPIRE II: Achieving Joint EUROASPIRE II: Achieving Joint European TC GoalEuropean TC Goal
0
20
40
60
80
100Pe
rcen
tage
of p
atie
nts
61% of high-risk
patients* received lipid-modifying
therapy
51% of patients
reached Joint European TC
goal**
*CABG, PTCA, MI or ischaemia, ** TC <5 mmol/L
Adapted from EUROASPIRE II. Euro Heart J 2001;22:554–772

Section 5Section 5
Statins and Lipid-modifying Statins and Lipid-modifying TherapiesTherapies

Effect of lipid-modifying therapies Effect of lipid-modifying therapies on lipids on lipids
Therapy
Bile acidsequestrantsNicotinic acid
Fibrates(gemfibrozil)Probucol
Statins*
Ezetimibe
TC–total cholesterol, LDL–low density lipoprotein, HDL–high density lipoprotein, TG–triglyceride. * Daily dose of 40mg of each drug, excluding rosuvastatin.
TC
Down 20%
Down 25%
Down 15%
Down 25%
Down 15–30%
LDL
Down 15–30%Down 25%
Down 5–15%Down
10–15%Down
24–50%Down
15–20%
HDL
Up 3–5%Up
15–30%Up 20%
Down20–30%
Up 6–12%
Up4–9%
TG
Neutral or up
Down 20–50%Down
20–50%Neutral
Down 10–29%
Patienttolerability
Poor
Poor toreasonable
Good
Reasonable
Good
Good
Adapted from Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391, Knopp RH. N Engl J Med 1999;341:498–511, Gupta EK, Ito MK. Heart Dis 2002;4:399–409

Mechanism of Action of Statins: Mechanism of Action of Statins: Cholesterol Synthesis PathwayCholesterol Synthesis Pathway
acetyl CoA
HMG-CoA
mevalonic acid
mevalonate pyrophosphate
isopentenyl pyrophosphate
geranyl pyrophosphate
farnesyl pyrophosphate
squalene
cholesterol
dolicholsubiquinones
HMG-CoA synthase
HMG-CoA reductase
Squalene synthase
X Statins

Statin Protein binding
(%)
Metabolisedby CYP450
Lipophilic Half-life (h)
rosuvastatinatorvastatinsimvastatin pravastatinfluvastatin
~90%>98%95–8%~50%>98%
NoYesYes No Yes
NoYesYes No No
~19~15~3~2~3
Pharmacokinetics of StatinsPharmacokinetics of Statins
Adapted from Horsmans Y. Eur Heart J Supplements 1999;1(Suppl T):T7–12, Vaughan CJ et al. J Am Coll Cardiol 2000;35:1–10. Rosuvastatin data from Core Data Sheet

Effects of Statins on LipidsEffects of Statins on Lipids
rosuvastatin (10 mg)atorvastatin (10 mg)simvastatin (20 mg)pravastatin (20 mg)fluvastatin (20 mg)
LDL-C% change
-52-39-38-32-22
HDL-C% change
+14+6+8+2+3
TG% change
-10-19-19-11-12
Adapted from Product Data Sheets.

Pleiotropic Effects of StatinsPleiotropic Effects of Statins
Improving or restoring endothelial function Enhancing the stability of atherosclerotic
plaques Decreasing oxidative stress Decreasing vascular inflammation Anti-thrombotic effects
Adapted from Takemoto M, Liao JK. Arterioscler Thromb Vasc Biol 2001;21:1712–1719

Section 6Section 6
Key Statin TrialsKey Statin Trials

Design of Key Statin TrialsDesign of Key Statin Trials
4S1
WOSCOPS2
CARE3
LIPID4
AFCAPS/TexCAPS5
HPS6
ASCOT-LLA7
Statin
Existing CHD
Patients Cholesterol
Follow-up (years)
simvastatin20 mg od
pravastatin 40 mg od
pravastatin 40 mg od
pravastatin 40 mg od
lovastatin 40 mg od
Yes
No MI,angina(5%)
Yes
Yes
No
Raised Mean LDL-C 4.87 mmol/L,
188 mg/dL
Raised Mean LDL-C 4.97 mmol/L,
192 mg/dL
Average Mean LDL-C 3.59 mmol/L,
139 mg/dL
Average Mean LDL-C 3.80 mmol/L,
147 mg/dL
Average Mean LDL-C 3.89 mmol/L,
150 mg/dL
5.4
4.9
5.0
6.1
5.2
4444 male and female, aged 35–70
6595 male, aged 45–64
4159 male and female, aged 21–75
9014 male and female, aged 31–75
6605 male and female, aged 45–73
Study
YesYes
In some In some patientspatients
simvastatinsimvastatin40 mg od40 mg od
20536 male 20536 male and female, and female, aged 40–80aged 40–80
Low/average Low/average Mean LDL-C 3.4 mmol/L, Mean LDL-C 3.4 mmol/L,
130 mg/dL130 mg/dL
5.05.0
3.33.3atorvastatinatorvastatin10 mg od10 mg od
Low/averageLow/averageMean LDL-C 3.4 mmol/L, Mean LDL-C 3.4 mmol/L,
130 mg/dL130 mg/dL
10305 male 10305 male and female, and female, aged 40–79aged 40–79

Key Statin Trials and Key Statin Trials and Spectrum of Risk Spectrum of Risk
4S4S11
LIPIDLIPID22
CARECARE44
WOSCOPSWOSCOPS66
AFCAPS/TexCAPSAFCAPS/TexCAPS77
CHD/high cholesterol
CHD/average to high cholesterol
CHD/average cholesterol
No MI/high cholesterol
No CHD/average cholesterol
HPSHPS33 CHD*/average to high cholesterol
*CHD or CHD risk equivalent, e.g. diabetes
Increasing absolute CHD risk
ASCOT-LLAASCOT-LLA55 Some patients with CHD/average cholesterol

simvastatin(n=2221)
4S Cardiovascular Endpoints4S Cardiovascular EndpointsPost-MI or Angina Patients with Raised CholesterolPost-MI or Angina Patients with Raised Cholesterol
Number of events
Outcomes placebo
(n=2223)
Risk reduction (%)
p-value
Total mortality*
Coronary death
Major coronary events
PCTA/CABG
256
189
622
383
182
111
431
252
30
42
34
37
<0.001
<0.001
<0.001
<0.001
* primary endpoint
The Scandinavian Simvastatin Survival Study Group. Lancet 1994;344:1383–1389

4S: Total Mortality4S: Total Mortality
0.85
0.80
0.000.0
1.00
0.95
0.90
Prop
ortio
n al
ive
Years since randomisation
placeboplacebosimvastatinsimvastatin
64321 5
Log rank p=0.0003
This improvement in survival is accounted for by the 42% reduction in coronary death.
The Scandinavian Simvastatin Survival Study Group. Lancet 1994;344:1383–1389

placebo
(n=3293)
pravastatin(n=3302)
Risk reduction (%)
p-value
Non-fatal MI/CHD death*CHD deathNon-fatal MIPCTA/CABGStrokeAll cardiovascular deathsTotal mortality#
248
52204805173
135
174
38143514650
106
31
283137032
22
<0.001
ns<0.0010.009
ns0.033
0.051
* primary endpoint# study not powered to detect differences in this endpoint
WOSCOPS: Cardiovascular EndpointsWOSCOPS: Cardiovascular EndpointsSubjects with No Previous MI but Raised CholesterolSubjects with No Previous MI but Raised Cholesterol
Outcomes
Number of events
Shepherd J et al. N Engl J Med 1995;333:1301–1307

WOSCOPS: Non-fatal MI and CHD WOSCOPS: Non-fatal MI and CHD DeathDeath
YearsYears
0011
22
44
66
Perc
ent w
ith e
vent
Perc
ent w
ith e
vent
88
1010
1212
22 3 3 44 55 66
pravastatin (n=3302)pravastatin (n=3302)placebo (n=3293)placebo (n=3293)
31% 31% relativerelativerisk risk reductionreductionpp<0.001<0.001
Shepherd J et al. N Engl J Med 1995;333:1301–1307

placebo(n=2078)
pravastatin(n=2081)
Risk reduction (%)
p-value
Non-fatal MI/CHD death*CHD deathNon-fatal MIPCTA/CABGUnstable anginaStroke
274
11917339135978
212
9613529431754
24
2023271331
0.003
ns0.020.0090.070.03
CARE: Cardiovascular EndpointsCARE: Cardiovascular EndpointsPost-MI Patients with Average CholesterolPost-MI Patients with Average Cholesterol
* primary endpoint
Outcomes
Number of events
Sacks FM et al. N Engl J Med 1996;335:1001–1009

CARE: Non-fatal MI or CHD DeathCARE: Non-fatal MI or CHD Death
0
5
10
Incid
ence
%
Years0.0
15
54321
Change in risk,Change in risk,24% reduction24% reductionpp=0.003=0.003
pravastatinpravastatinplaceboplacebo
Sacks FM et al. N Engl J Med 1996;335:1001–1009

placebo(n=4502)
pravastatin(n=4512)
Riskreduction (%)
p-value
CHD death*CVD deathAll-cause mortalityCHD death or non-fatal MIAny MIPCTA or CABGHosp. for unstable anginaStroke
373433633715
463708
1106
204
287331498557
336585
1005
169
24252224
292012
19
<0.001<0.001<0.001<0.001
<0.001<0.0010.005
0.048
* primary endpoint
Outcomes
LIPID: Cardiovascular EndpointsLIPID: Cardiovascular EndpointsPost-MI or Unstable Angina Patients with Average/raised Post-MI or Unstable Angina Patients with Average/raised
CholesterolCholesterol
Number of events
LIPID. N Engl J Med 1998;339:1349–1357

LIPID: Cumulative Risk of Death LIPID: Cumulative Risk of Death from CHDfrom CHD
Years after Years after randomisationrandomisation
0011
55
Cum
ulat
ive
risk
(%)
Cum
ulat
ive
risk
(%)
1010
22 3 3 44 55 77
pravastatinpravastatinplaceboplacebo 24% risk 24% risk
reductionreductionpp<0.001<0.001
6600
LIPID. N Engl J Med 1998;339:1349–1357

AFCAPS/TexCAPS: Cardiovascular EndpointsAFCAPS/TexCAPS: Cardiovascular EndpointsSubjects with No History of CHD and Average CholesterolSubjects with No History of CHD and Average Cholesterol
placeboplacebo((n=3301n=3301))
lovastatinlovastatin((n=3304n=3304))
RiskRiskreduction (%)reduction (%)
pp-value-value
Fatal or non-fatal MI + unstable angina + sudden cardiac death*RevascularisationsFatal and non-fatal MIUnstable angina
183
15795
87
116
1065760
37
334032
<0.001
<0.0010.0020.02
* primary endpoint
OutcomesOutcomes
Number of eventsNumber of events
Downs JR et al. J Am Med Assoc 1998;279:1615–1622

AFCAPS/TexCAPS: Fatal/Non-fatal MI, AFCAPS/TexCAPS: Fatal/Non-fatal MI, Sudden Cardiac Death, Unstable AnginaSudden Cardiac Death, Unstable Angina
0.03
0.06
0.04
0.010.00
Cum
ulat
ive
incid
ence
Years of follow-upYears of follow-up0.0 >5
0.07
54321
0.05
0.02
37% riskreductionp<0.001
lovastatinlovastatinplaceboplacebo
Downs JR et al. J Am Med Assoc 1998;279:1615–1622

Meta-analysis of 38 primary and secondary intervention trials Meta-analysis of 38 primary and secondary intervention trials
Benefits of Cholesterol LoweringBenefits of Cholesterol Lowering
Total mortality (Total mortality (pp=0.004)=0.004)CHD mortality (CHD mortality (pp=0.012)=0.012)
% in cholesterol reduction% in cholesterol reduction
Mor
talit
y lo
g od
ds ra
tioM
orta
lity
log
odds
ratio
00 44 88 1212 1616 2020 2424 2828 3232 3636-1.0-1.0
-0.8-0.8
-0.6-0.6
-0.4-0.4
-0.2-0.2
-0.0-0.0
4040 4444 4848 5252
Adapted from Gould AL et al. Circulation. 1998;97:946–952

HPS: Statin Benefits Patients with HPS: Statin Benefits Patients with Low Baseline Cholesterol LevelsLow Baseline Cholesterol Levels
RR - relative reduction vs. placebo
0
10
20
30
40
All-causemortality
Major vascularevents
All stroke
Inci
denc
e %
placebo (n=10,267)
simvastatin(n=10,269)-13% RR
P=0.0003
-24% RRp<0.0001
-25% RRp<0.0001
Adapted from HPS Collaborative Group, Lancet 2002;360:7–22

ASCOT-LLA: Statin Benefits ASCOT-LLA: Statin Benefits Hypertensive Patients with Average Hypertensive Patients with Average or Low Baseline Cholesterol Levelsor Low Baseline Cholesterol Levels
Adapted from Sever PS et al. Lancet 2003;361:1149–1158
placeboplacebo((n=5137n=5137))
atorvastatinatorvastatin((n=5168n=5168))
Hazard Hazard ratioratio
pp-value-value
154
486
247
137
121
* primary endpoint, # includes silent MI, excludes silent MI
OutcomesOutcomesNumber of eventsNumber of events
Non-fatal MI# plus fatal CHD*
Total CV events and procedures
Total coronary events
Non-fatal MI plus fatal CHD
Fatal and non-fatal stroke
100
389
178
86
89
0.64
0.79
0.71
0.62
0.73
0.0005
0.0005
0.0005
0.0005
0.0236

Section 7Section 7
Diabetes: a Risk Factor for CHD?Diabetes: a Risk Factor for CHD?

Diabetes MellitusDiabetes Mellitus
One of the most common non-communicable diseases
Fourth or fifth leading cause of death in most developed countries
More than 177 million people with diabetes worldwide
Incidence of diabetes is increasing – estimated to rise to 300 million by 2025 expected to triple in Africa, the Eastern Mediterranean and
Middle East, and South-East Asia to double in the Americas to almost double in Europe
Adapted from: International Diabetes Federation websiteAdapted from: International Diabetes Federation website

The Chronic Complications of The Chronic Complications of Diabetes MellitusDiabetes Mellitus
Macrovascular complications: Heart disease
Leading cause of diabetes related deaths (increases mortality and stroke by 2 to 4 times)
Microvascular complications: Retinopathy
Leading cause of adult blindness Nephropathy
Accounts for 43% of new cases of ESRD Neuropathy
60–70% of patients with diabetes have nervous system damage
Adapted from National Diabetes Statistics US 2000

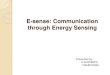
UKPDS: Typical Lipid Profile in Patients with UKPDS: Typical Lipid Profile in Patients with Diabetes Compared with No DiabetesDiabetes Compared with No Diabetes
Adapted from UKPDS. Adapted from UKPDS. Diabetes CareDiabetes Care 1997; 1997;20:20:1683–16871683–1687
p<0.001 p<0.001MenMen WomenWomen
no DMDM DMno DM
1
1.2
1.4
1.6
1.8
2
Triglycerides (mmol/ L)
5
5.2
5.4
5.6
5.8
6
Total cholesterol (mmol/ L)
MenMen
WomenWomen
DMno DM
no DM DM
1
1.2
1.4
1.6
HDL-cholesterol (mmol/ L)
DM DMno DM
no DM
p<0.001
p<0.001
MenMen
WomenWomen
3
3.2
3.4
3.6
3.8
4
LDL-cholesterol (mmol/ L)
p<0.001
MenMen
DMno DM
no DM DM
WomenWomen

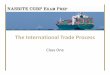
PROCAM: Combination of Risk PROCAM: Combination of Risk Factors Increases Risk of MIFactors Increases Risk of MI
0
20
40
60
80
100
120
Inci
denc
e of
MI/
1000
pts
None
Hyper
tensio
n
only
Diabet
es on
ly
Hyper
tens
+
diabete
s
Dyslip
idaem
ia
Dyslip
idaem
ia +
hype
rtens
+/-
diabe
tes
Prevalence (%): 54.9 22.9 2.6 2.3 9.4 8.0
Adapted from Assman G, Schulte H. Am Heart J 1988;116:1713–1724

Adapted from Malmberg K et al. Circulation 2000;102:1014–1019
OASIS:OASIS: Patients with Diabetes at Similar Patients with Diabetes at Similar Risk to No Diabetes with CVDRisk to No Diabetes with CVD

BARI: Diabetes Results in Less Favourable BARI: Diabetes Results in Less Favourable Outcome After Angioplasty Than No Outcome After Angioplasty Than No
DiabetesDiabetes
0
5
10
15
20
25
30
35
No diabetesNo diabetes DiabetesDiabetes
5-ye
ar m
orta
lity
(%)
CABG PTCA
Adapted from BARI Investigators. N Engl J Med 1996:335:217–225

NHANES: Smaller Changes in CAD Mortality NHANES: Smaller Changes in CAD Mortality Rates in Patients with Diabetes than No Rates in Patients with Diabetes than No
Diabetes Over TimeDiabetes Over Time
-50
-40
-30
-20
-10
0
10
20
% c
hang
e in
mor
talit
y
MenWomen
*p<0.001 vs. baseline
*
DiabetesDiabetes No diabetesNo diabetes
Adapted from Gu K et al. JAMA;281:1291–1297

Section 8Section 8
The Metabolic SyndromeThe Metabolic Syndrome

The Metabolic Syndrome andThe Metabolic Syndrome andAssociated CVD Risk FactorsAssociated CVD Risk Factors
AtherosclerosisAtherosclerosis
Endothelial Dysfunction
Hypertension
Abdominal obesity
Hyperinsulinaemia
Dyslipidaemia• high TGs
• small dense LDL• low HDL-C
Diabetes
Hypercoagulability
Insulin Resistance

NCEP ATP III: The Metabolic SyndromeNCEP ATP III: The Metabolic Syndrome
<40 mg/dL (1.0 mmol/L)<50 mg/dL (1.3 mmol/L)
MenWomen
>102 cm (>40 in)>88 cm (>35 in)
MenWomen
110 mg/dL (6.0 mmol/L)Fasting glucose130/85 mm HgBlood pressure
HDL-C150 mg/dL (1.7 mmol/L)TG
Abdominal obesity (Waist circumference)
Defining LevelRisk Factor
Diagnosis is established when 3 of these risk factors are present
National Cholesterol Education Program, Adult Treatment Panel III, 2001. JAMA 2001:285;2486–2497

WHO: The Metabolic SyndromeWHO: The Metabolic Syndrome
A working definition is glucose intolerance, IGT or diabetes mellitus and/or insulin resistance together with two or more of the following:
• Impaired glucose regulation or diabetes• Insulin resistance• Raised arterial pressure 160/90 mmHg• Raised plasma triglycerides (1.7 mmol/L, 150 mg/dL)
and/or low HDL-C (men <0.9 mmol/L, 35 mg/dl; women <1.0 mmol/L, 39 mg/dL)
• Central obesity• Microalbuminuria (UAER 20 g/min or albumin:
creatinine ratio 20 mg/g)
Alberti KGMM, Zimmet PZ for the WHO. Diabet Med 1998:15;539–553

AIR: LDL Particle Size is Related to AIR: LDL Particle Size is Related to the Metabolic Syndromethe Metabolic Syndrome
25
25.5
26
26.5
27LD
L pe
ak p
arti
cle
size
(nm
)
Metabolic Syndrome (n=62)No Metabolic syndrome but 1 or more risk factors (n=252)No risk factors (n=77)
p<0.001
Adapted from Hulthe J et al. Arterioscler Thromb Vasc Biol 2000;20:2140–2147

PARIS: CHD Mortality Increases with PARIS: CHD Mortality Increases with Increased Impaired Glucose ToleranceIncreased Impaired Glucose Tolerance
0
1
2
3
4
5
CHD
mor
talit
y ra
te/1
000
G <140 mg/dL
IGT G 200 mg/dLNewly
diagnosed diabetes
Known diabetes
p<0.001
n=6055 n=690 n=158 n=135
Adapted from Eschwege E et al. Horm Metab Res 1995;17(Suppl):41–46
G - glucoseG - glucose

Section 9Section 9
Outcome Trials in DiabetesOutcome Trials in Diabetes

Trials with Fibrates in Patients with Trials with Fibrates in Patients with DiabetesDiabetes
Frick MH et al. N Engl J Med 1987;317:1237–1245, Koskinen P et al. Diabetes Care 1992;15:820–825, Elkeles RS, Diamond JR, Poulter C et al. Diabetes Care 1998;21(4):641–648, Rubins HB et al. N Engl J
Med 1999;341:410–418, DAIS Investigators. Lancet 2001;357:905–910
Study Effect p-value Comment
Helsinki Helsinki Heart StudyHeart Study(gemfibrozil)(gemfibrozil)
75% 75% eventsevents
nsns Primary prevention; Primary prevention; post-hoc subgroup analysispost-hoc subgroup analysis
SENDCAPSENDCAP(bezafibrate)(bezafibrate)
65% 65% eventsevents
0.010.01 Specifically conducted in Specifically conducted in Type 2 diabetes; post-hoc Type 2 diabetes; post-hoc analysis for IHDanalysis for IHD
VA-HITVA-HIT(gemfibrozil)(gemfibrozil)
24%24%eventsevents
0.050.05 Secondary intervention; Secondary intervention; pre-planned subgroup pre-planned subgroup analysisanalysis
DAISDAIS(fenofibrate)(fenofibrate)
40-42%40-42%focal angio focal angio changeschanges
0.020.02 Specifically conducted in Specifically conducted in Type 2 diabetes; mixed Type 2 diabetes; mixed primary and secondary primary and secondary intervention; angio studyintervention; angio study

Statins Reduce CHD Risk in Patients Statins Reduce CHD Risk in Patients with Diabeteswith Diabetes
StudyStudy % LDL-C % LDL-C loweringlowering
% CHD risk % CHD risk reduction reduction (overall)(overall)
% CHD risk % CHD risk reduction reduction (diabetes)(diabetes)
Primary preventionPrimary preventionAFCAPS/TexCAPSAFCAPS/TexCAPS11 (lovastatin; n=239) (lovastatin; n=239) 2525 37 (37 (pp<0.001)<0.001) 4343
Secondary preventionSecondary preventionCARECARE2 2 (pravastatin; n=586) (pravastatin; n=586)4S4S33 (simvastatin; n=202) (simvastatin; n=202)LIPIDLIPID44 (pravastatin; n=782) (pravastatin; n=782)
28283636
25*25*
23 (23 (pp<0.001)<0.001)32 (32 (pp<0.001)<0.001)
2525
25 (25 (pp=0.05)=0.05)55 (55 (pp=0.002)=0.002)
1919
* value for overall group

Adapted from Kreisberg RA. Am J Cardiol 1998;82:67U–73U
4S/CARE: LDL Lowering in Patients 4S/CARE: LDL Lowering in Patients with Diabeteswith Diabetes

Adapted from Pyörälä K et al. Diabetes Care 1997;20:614–620
4S: CHD Event Reduction in Patients 4S: CHD Event Reduction in Patients with Diabeteswith Diabetes

WOSCOPS: Statin Treatment WOSCOPS: Statin Treatment Protects Against Development of Protects Against Development of
DiabetesDiabetes
Total Total number of number of patientspatients
Patients Patients developing developing diabetesdiabetes
% risk % risk reductionreduction
pp-value-value
59745974 139139 3030 0.0420.042
Adapted from Freeman DJ et al. Circulation 2001;103:357–362