Embed Size (px)
Citation preview

Hereditary Hemochromatosis
Hereditary hemochromatosis (HHC; HFE 1) is a com-
mon hereditary disorder of iron metabolism and the
most common inherited autosomal recessive disorder
in Caucasians with a prevalence of 1 in 300 to 1 in 500
individuals. It is characterized by inappropriately high
iron absorption resulting in progressive iron overload.
Synonyms and Related Disorders
Hemochromatosis
Genetics/Basic Defects
1. Inheritance: autosomal recessive
2. Cause: result of a single faulty HFE gene on
chromosome 6p21.3 near the HLA complex that
codes for a glycoprotein called HFE, which binds
to the transferrin receptor and reduces its affinity for
iron-bound transferrin, allowing cellular uptake of
iron-based transferrin
3. Two common mutations (missense)
a. C282Y.
i. Accounts for most cases of HHC
ii. Homozygotes for C282Y mutation (>80%
cases world-wide) are at high risk for HHC.
iii. Heterozygote for C282Y mutation.
a) Have increased levels of transferrin
saturation
b) Rarely have organ damage
b. H63D: Homozygotes for H63D (often
has a potentiator, such as hepatitis C infection,
b-thalassemia trait) are unlikely to develop HHC.
c. C282Y/H63D (11% present phenotypically):
Compound heterozygotes for C282Y/H63D have
a milder form of HHC than C282Y homozygotes.
4. Other HFE mutations
a. Missense mutations
i. S65C: the third most common mutation
ii. G93R
iii. I105T
iv. Q127H
v. R330M
b. Frameshift mutations
i. P160DCii. V68DT
c. Nonsense mutations
d. Spice site mutation
5. Clinical expression of the disease
a. Homozygotes: affected clinically
b. Heterozygotes
i. Can have minor abnormalities of the param-
eters that reflect body iron status
ii. Can develop significant iron overload
only when other diseases that affect iron
metabolism coexist, such as:
a) Heterozygous b-thalassemia
b) Hereditary spherocytosis
c) Sporadic porphyria cutanea tarda
6. Hereditary hemochromatosis not attributable to
mutations in HFEa. A subgroup of hereditary hemochromatosis
indistinguishable from HFE-associated HHC
b. Does not have mutations in HFE.c. The disease does not appear to be linked to the
HLA complex.
d. The genetic basis has not been defined.
H. Chen, Atlas of Genetic Diagnosis and Counseling, DOI 10.1007/978-1-4614-1037-9_116,# Springer Science+Business Media, LLC 2012
1025

7. Pathophysiology (Whittington and Kowdley, 2002)
a. Inappropriately high intestinal iron absorption:
the most important pathophysiological step in
body iron loading
b. Effects of mutations on iron absorption: central
to the understanding of the pathological basis of
hereditary hemochromatosis
Clinical Features
1. Variable clinical presentation
2. Median age at presentation of symptoms
a. Fifty one years in males
b. Female homozygotes
i. Less likely to develop symptomatic disease
ii. Median age: age 50
3. Asymptomatic: abnormal serum iron studies on
routine screening
4. Early manifestations
a. Often subtle
b. Vague arthralgias
c. Fatigue
d. Lethargy
e. Apathy
f. Weight loss
5. Later manifestations as tissue iron progressively
accumulates
a. Discoloration of the skin
b. Arthropathy
i. Due to iron accumulation in joint tissues.
ii. Arthritis with joint swelling most com-
monly involves:
a) Metacarpophalangeal (MCP) joints
b) Proximal interphalangeal joints
c) Knees
d) Feet
e) Wrists
f) Back
g) Neck
iii. Chondrocalcinosis.
a) Involves the knees and wrists
b) May be asymptomatic
iv. Symptoms usually do not respond to iron
removal.
c. Liver involvement
i. Abdominal pain associated with
hepatomegaly
ii. Hepatomegaly, the most common physical
abnormality
iii. Splenomegaly
iv. Cirrhosis
v. Portal hypertension
a) Ascites
b) Encephalopathy
vi. Hepatocellular carcinoma in about 30% of
cases
d. Cardiac involvement
i. Dilated cardiomyopathy
ii. Arrhythmias
iii. Cardiac failure
e. Endocrine abnormalities
i. Diabetes mellitus
ii. Pituitary hypogonadism
a) Decreased libido and impotence (tes-
ticular atrophy) in men
b) Amenorrhea in women
iii. Hypothyroidism
6. Suspect diagnosis from characteristic clinical
manifestations
a. Classical clinical triad of “bronzed cirrhosis
with diabetes” in a middle-aged man:
i. Diffuse hyperpigmentation (melanodermia),
often with a metallic gray or “bronze” rather
than a brown discoloration
ii. Hepatomegaly, with the liver markedly
enlarged, firm and sharp to palpation but
without signs of hepatocellular insuffi-
ciency (no palmar erythema, no spider
nevi, no bruises, normal prothrombin time)
or of portal hypertension
iii. Diabetes mellitus, often requiring insulin
b. Presence of cardiomyopathy
c. Diagnosis at this late stage: considered a
diagnostic failure
7. Suspect diagnosis from earlier signs and
symptoms
a. Sex and age: Both young adults and older women
are at risk.
b. “Rule of three A’s”
i. Asthenia: unexplained chronic fatigue
ii. Arthralgia
a) A “painful” handshake: resulting from
chronic arthritis of the second and third
MCP joints.
b) Other joints affected especially the
knees and wrists.
1026 Hereditary Hemochromatosis

c) Can also suffer from pseudogout (pyro-
phosphate arthropathy).
d) Arthritis greatly diminishes the quality
of life.
iii. Aminotransferase (transaminases) elevation
8. Cause of death
a. Liver failure
b. Cancer
c. Congestive heart failure
d. Arrhythmia
9. Other conditions associated with significant iron
overload
a. Non-HFE hereditary hemochromatosis
(Pietrangelo, 2010)
i. Transferrin receptor 2 gene (TFR2, on 7q22)hemochromatosis
a) Caucasian or non-Caucasian
b) Male or female
c) Thirty to forty years
d) Cardiomyopathy
e) Endocrinopathy
f ) Liver disease
g) Elevated transferrin saturation (TS) and
serum ferritin (SF)
ii. Hemojuvelin (HJV on 1q21) or hepcidin
gene (HAMP, on 19q13) juvenile
hemochromatosis
a) Caucasian or non-Caucasian
b) Male or female
c) Fifteen to twenty years
d) Impotence/amenorrhea and/or
cardiomegaly
e) High TS and SF
iii. Ferroportin disease (SLC40A1, on 2q32)
a) Caucasian or non-Caucasian
b) Male or female
c) Ten to eighty years
d) One patient with unexplained
hyperferritinemia
e) Unexplained elevation of SF and normal
TS
b. Secondary iron overload
i. Iron-loading anemias (ineffective erythropoi-
esis, increased iron absorption, blood
transfusions)
a) b-thalassemia
b) Congenital dyserythropoietic anemias
c) Sideroblastic anemia
d) Pyridoxine-responsive anemia
ii. Hypoplastic anemias (blood transfusions)
a) Aplastic anemia
b) Myelodysplastic syndromes
c) Pure red cell aplasia
iii. Chronic hemolytic anemias (increased iron
absorption)
a) Spherocytosis
b) Sickle cell anemia
c) Pyruvate kinase deficiency
iv. Parental iron overload
a) Red blood cell transfusion
b) Iron dextran injections
c) Long-term hemolysis
v. Neonatal hemochromatosis
vi. Ceruloplasmin deficiency (acerulo-
plasminemia) (decreased ferroxidase
activity)
vii. Sub-Saharan iron overload (increased die-
tary iron, increased iron absorption)
viii. Porphyria cutanea tarda (increased iron
absorption)
ix. Hepatic disorders
a) Chronic viral hepatitis
b) Alcoholic cirrhosis
c) Portacaval shunts (increased iron
absorption)
Diagnostic Investigations
1. Biochemical testing
a. High serum ferritin levels
b. High transferrin-iron saturation value: an early
and reliable indicator for risk of iron overload/
HFE-HHC
i. A fasting transferrin-iron saturation of�60%
for men and�50% for women on at least two
occasions, in the absence of other known
causes of elevated transferrin-iron saturation,
is observed in about 80% of individuals with
HFE-HHC and is considered suggestive of
HFE-HHC.
ii. A threshold transferrin-iron saturation
of 45% is more sensitive for detecting
HFE-HHC suggested by recent studies.
iii. Some overlap occurs in serum transferrin-iron
saturation among homozygotes and
heterozygotes.
Hereditary Hemochromatosis 1027

2. Radiography
a. Arthropathy
i. Squared-off bone ends and hook-like
osteophytes in the MCP joints, particularly
in the second and third MCP joints
ii. Subchondral arthropathy
iii. Chondrocalcinosis
3. MRI of the liver
a. The most promising noninvasive technique for
identification of HHC. High hepatic iron content
causes:
i. A decrease in signal intensity of the liver
ii. A marked decrease in transverse (T2) relaxa-
tion time
4. Liver biopsy to assess histologic hepatic iron stores
a. Usually not indicated for diagnostic purposes in
HFE-HHC.
b. Recommended to C282Y homozygotes with
a serum ferritin concentration of >1,000 ng/mL
to determine if cirrhosis is present; those with
a serum ferritin concentration <1,000 ng/mL
need not undergo biopsy.
c. Useful to determine hepatic iron overload, par-
ticularly in patients with presumed hemochro-
matosis who lack the common HFE mutations
associated with HFE-HHC.
5. Molecular genetic testing (Kowdley et al. 2006)
a. Mutation analysis for the disease-causing alleles
in the HFE gene (C282Y and H63D)
i. C282Y/C282Y homozygotes (60–90%)
ii. C282Y/H63D compound heterozygotes
(3–8%)
iii. H63D/H63D homozygote (1%)
iv. H63D/? (4%)
v. C282Y/? (1%)
vi. ?/? (6%)
b. Testing strategy for a proband
i. Mutation analysis warranted in adults with
serum transferrin-ion saturation of >45%
ii. Individuals with homozygous C282Y/
C282Y or compound heterozygous C282Y/
H63D: have genetic makeup to develop
HFC-HHC
iii. Individuals who are not C282Y homozygotes
a) Generally represent a heterogeneous
group.
b) Many have liver disease unrelated to
HFE-HHC or other metabolic syndromes.
c) Somemay have primary iron overload in
a pattern identical to HFE-HHC.
d) The next diagnostic step: perform liver
biopsy with assessment of histology
and measurement of hepatic iron
concentration
c. Carrier detection: identification of carriers and
noncarriers in at-risk family members possible
provided both HFE alleles have been identified
in the proband
6. Screening for HHC
a. HHC: a prime target for screening because of its
high prevalence, morbidity, and mortality, as
well as the benefits of early diagnosis and
treatment
b. Initial screening probe for HHC diagnosis
i. Transferrin saturation
ii. Unsaturated iron-binding capacity
Genetic Counseling
1. Recurrence risk (Kowdley et al. 2006)
a. Patient’s sib
i. Twenty-five percent if both parents are HFE-
HHC heterozygotes
ii. Fifty percent if one parent is HFE-HHC het-
erozygotes and other parent HFE-HHC
homozygote
b. Patient’s offspring: 5% risk to be affected due to
the high carrier rate forHFEmutant alleles in the
general population
i. The risk that the partner of an individual with
HFE-HHC is heterozygous for the C282Y
allele is 1/9
ii. Therefore, the risk to the offspring to be
a homozygote for C282Y allele is 1/2 �1/9 ¼ 1/18 (about 5%)
2. Prenatal diagnosis
a. Technically feasible when both parents carry
identified HFE mutations
b. Highly unusual to request prenatal diagnosis
because HHC is an adult-onset, treatable disease
3. Management (Kowdley et al. 2006)
a. Early diagnosis and treatment
i. Can completely prevent the development of
clinical complications
ii. Offer patients a normal life expectancy
1028 Hereditary Hemochromatosis

b. Treatment of iron overload
i. Periodic phlebotomy
a) Goal of therapy: to achieve and maintain
a serum ferritin concentration of
�50 ng/mL
b) Usual therapy: removal of the
excess iron by weekly phlebotomy until
the serum ferritin concentration is
�50 ng/mL
ii. Dietary management
a) Avoid medicinal iron
b) Avoid mineral supplements
c) Avoid excess vitamin C which increases
intestinal absorption of inorganic iron
d) Avoid uncooked shellfish or other sea-
food which can be contaminated with V
vulnificus causing sepsis in patients with
HHC
e) Avoid alcohol consumption for patients
with liver involvement
iii. Iron chelation therapy: not recommended
unless the patient has an elevated serum ferri-
tin concentration and concomitant anemia that
makes therapeutic phlebotomy impossible
c. Conventional therapies for diabetes, hepatic fail-
ure, and cardiac failure
d. Cirrhosis: screen for hepatocellular cancer
i. Biannual abdominal ultrasound
ii. Annual serum alpha-fetoprotein testing
e. Orthotopic liver transplantation for end-stage
liver disease from decompensated cirrhosis
f. Surveillance of at-risk asymptomatic adults with
C282Y homozygotes
i. Monitor serum ferritin concentrations yearly
starting in early adulthood
ii. Initiate therapeutic phlebotomy when serum
ferritin concentrations are elevated
References
Andrews, N. C. (1999). Disorders of iron metabolism. The NewEngland Journal of Medicine, 341, 1986–1995.
Bothwell, T. H., & MacPhail, A. P. (1998). Hereditary hemo-
chromatosis: Etiologic, pathologic, and clinical aspects.
Seminars in Hematology, 35, 55–71.Brittenham, G. M., Weiss, G., Brissot, P., et al. (2000) Clinical
consequences of new insights in the pathophysiology
of disorders of iron and heme metabolism. HematologyAmerican Society of Hematology Education Program, 39–50
Camaschella, C., & Piperno, A. (1997). Hereditary hemochro-
matosis: Recent advances in molecular genetics and clinical
management. Haematologica, 82, 77–84.Edwards, C. Q., Griffen, L. M., Dadone, M. M., et al. (1986).
Mapping the locus for hereditary hemochromatosis: Locali-
zation between HLA-B and HLA-A. American Journal ofHuman Genetics, 38, 805–811.
Feder, J. N., Gnirke, A., Thomas,W., et al. (1996). A novelMHC
class I-like gene is mutated in patients with hereditary
haemochromatosis. Nature Genetics, 13, 399–408.Fleming, R. E., & Sly, W. S. (2002). Mechanisms of iron accu-
mulation in hereditary hemochromatosis. Annual Review ofPhysiology, 64, 663–680.
Hanson, E. H., Imperatore, G., & Burke, W. (2001). HFE gene
and hereditary hemochromatosis: A HuGE review. Human
Genome Epidemiology. American Journal of Epidemiology,154, 193–206.
Harrison, S. A., & Bacon, B. R. (2003). Hereditary hemochroma-
tosis: Update for 2003. Journal of Hepatology, 38(Suppl 1),S14–S23.
Kowdley, K. V., Tait, J. F., Bennett, R. L., et al. (2006) HFE-
associated hereditary hemochromatosis. GeneReviews.Updated December 4, 2006. Available at: http://www.ncbi.
nlm.nih.gov/bookshelf/br.fcgi?book¼gene&part¼hemochr-
omatosis
Mclaren, G. D., Gordeuk, V. R. (2009). Hereditary hemochro-
matosis: Insights from the hemochromatosis and iron
overload screening (HEIRS) study. Hematology AmericanSociety of Hematology Education Program, 195–206
McLaren, C. E., McLachlan, G. J., Halliday, J. W., et al. (1998).
Distribution of transferrin saturation in an Australian popu-
lation: Relevance to the early diagnosis of hemochromatosis.
Gastroenterology, 114, 543–549.Merryweatherclarke, A. T., Pointon, J. J., Shearman, J. D., et al.
(1997). Global prevalence of putative haemochromatosis
mutations. Journal of Medical Genetics, 34, 275–278.Morrison, E. D., Brandhagen, D. J., Phatak, P. D., et al. (2003).
Serum ferritin level predicts advanced hepatic fibrosis among
U.S. patients with phenotypic hemochromatosis. Annals ofInternal Medicine, Ann Intern Med 138, 627–633.
Nichols, G. M., & Bacon, B. R. (1989). Hereditary hemochro-
matosis: Pathogenesis and clinical features of a common
disease. American Journal of Gastroenterology, 84,851–862.
Niederau, C., Fischer, R., Purschel, A., et al. (1996). Long-term
survival in patients with hereditary hemochromatosis. Gas-troenterology, 110, 1107–1119.
Niederau, C., Fischer, R., Sonnenberg, A., et al. (1985). Survival
and cause of death in crirrhotic and noncirrhotic patients with
primary hemochromatosis. The New England Journal ofMedicine, 313, 1256–1262.
Phatak, P. D., & Cappuccio, J. D. (1994). Management of hered-
itary hemochromatosis. Blood Reviews, 8, 193–198.Phatak, P. D., Guzman, G., Woll, J. E., et al. (1994). Cost-
effectiveness of screening for hereditary hemochromatosis.
Archives of Internal Medicine, 154, 769–776.Piertrangelo, A. (2003). Haemochromatosis. Gut, 52(Suppl II),
ii23–ii30.
Hereditary Hemochromatosis 1029

Pietrangelo, A. (2010). hereditary hemochromatosis: Pathogene-
sis, diagnosis, and treatment.Gastroenterology, 139, 393–408.Ramrakhiani, S., & Bacon, B. R. (1998). Hemochromatosis:
Advances in molecular genetics and clinical diagnosis. Jour-nal of Clinical Gastroenterology, 27, 41–46.
Tavill, A. S. (2001). Diagnosis and management of hemochro-
matosis. Hepatology, 33, 1321–1328.Whittington, C. A., & Kowdley, K. V. (2002). Review article:
Haemochromatosis. Alimentary Pharmacology and Thera-peutics, 16, 1963–1975.
1030 Hereditary Hemochromatosis

Fig. 1 Father (40-year-old) and son (12-year-old) both carry
heterozygous C282Y mutation. H63D and S65C were not
detected. The father currently receives periodic phlebotomy
with fasting transferrin-iron saturation level of 56% (15–50)
and ferritin level of 1,238 ng/mL (20–345). The son is currently
asymptomatic. Approximately 3–5% of patients with hereditary
hemochromatosis have this genotype. The molecular results do
not rule out the possibility of disease causing mutations in other
regions of the HFE gene or in other as yet undefined genes
Temperature (°C)
48.0 50.0 52.0 54.0 56.0 58.0 60.0 62.0 64.0 66.0 68.0 70.0 72.0 74.0 76.0
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0
−1.0
Flu
ores
cenc
e -d
(F2)
/dT
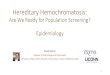
Fig. 2 Real-time PCR of HFE
gene in another patient. The
patient is homozygous for
C282Y mutation,
demonstrated by the green line
(melting point (Tm) ¼ 62.89)
Hereditary Hemochromatosis 1031