Embed Size (px)
Citation preview
Kasabach–Merritt Syndrome
Kasabach–Merritt syndrome (or phenomenon) is
the association of a vascular tumor and throm-
bocytopenic coagulopathy (Enjolras et al. 2000). It is a
life-threatening, localized consumptive coagulopathy,
characterized by profound thrombocytopenia and
microangiopathic anemia.
In 1940, Kasabach and Merritt described the
first case of Kasabach–Merritt syndrome with
a case report of consumptive coagulopathy associa-
ted with a hemangioma. However, it is now recog-
nized that Kasabach–Merritt syndrome is usually
associated with Kaposiform hemangioendothelioma
and tufted angioma, rather than the classic
involuting hemangioma of infancy (Enjolras et al.
1997).
Synonyms and Related Disorders
Hemangioma-thrombocytopenia syndrome
Genetics/Basic Defects
1. Genetics
a. Sporadic in majority of cases
b. Autosomal dominant inheritance in rare reports
c. Can be a part of recognized syndromes
2. Pathophysiology (Hall 2001)
a. Platelet trapping by abnormally proliferating
endothelium within the hemangioma, resulting
in the activation of platelets with a secondary
consumption of clotting factors
b. Continued consumption of both platelets and
clotting factors along with the initiation of
fibrinolysis eventually resulting in intralesional
bleeding which manifests as rapid enlargement
of the hemangioma
Clinical Features
1. Diverse clinical presentation (Enjolras et al. 2000;
Hall 2001)
a. Type of hemangiomas
i. Kaposiform hemangioendothelioma: often
found in noncutaneous sites such as the
retroperitoneum, mediastinum, and pelvis,
as well as the skin
ii. Tufted angioma
iii. Mixture of Kaposiform hemangioen-
dothelioma and tufted angioma
iv. Not “true” common hemangioma of infancy
b. Reddish brown skin lesion progressing to
a violaceous bulging mass
i. Often painful
ii. Aggressive infiltration with ulceration
iii. Bruising in other areas
iv. Possible infection
c. Bleeding from thrombocytopenia and intravas-
cular coagulopathy
d. Increase in size and becoming tense, woody,
and purplish of preexisting hemangiomas during
pregnancy
2. Cutaneous involvement of Kaposiform
hemangioendothelioma
a. Smooth, shiny, dark purple, indurated, tender,
and poorly delineated
b. Nearly always single
H. Chen, Atlas of Genetic Diagnosis and Counseling, DOI 10.1007/978-1-4614-1037-9_139,# Springer Science+Business Media, LLC 2012
1219
3. Visceral involvement of hemangiomata
a. Single
b. Multiple
c. Isolated within one organ as single or diffuse
lesions
d. Retroperitoneal hemangiomata
i. Often giant in size
ii. Easily missed clinically: diagnosis suspected
in patients presenting with an unexplained
thrombocytopenia and coagulopathy
iii. Generally associated with high mortality
4. Diffuse and multiple nature
a. Diffuse infantile (neonatal) hemangiomatosis
i. Presence of multiple cutaneous and visceral
hemangiomata
ii. High morbidity and mortality
b. Intraosseous and soft tissue hemangiomata
5. Lifelong hemangioma in adults
a. Hormone alterations and increase in blood
volume in pregnancy may affect preexisting
lesions, triggering episodes of acute dissemi-
nated intravascular coagulation
b. Development of acute consumptive coagulopathy
after surgery of other unrelated tumor
6. Thrombocytopenic coagulopathy in patients with
hemangiomata as a part of a recognized syndrome
a. Klippel–Trenaunay syndrome
i. A rare congenital generalized mesodermal
abnormality
ii. Macular vascular nevus, skeletal/soft tissue
hypertrophy
iii. Venous and lymphatic anomalies including
viscera and facial hemangiomata
b. Blue rubber bleb nevus syndrome
i. Multiple cutaneous cavernous hemangiomata
ii. Cutaneous and occasional visceral
hemangiomata
c. Gorham–Stout disease (“vanishing bone
disease”)
i. Massive osteolysis (Gorham sign)
ii. Followed by replacement of the bony matrix
by proliferating thin-walled vascular and
lymphatic channels
iii. Extension of these angiomatous masses into
soft tissues
7. Prognosis
a. Incomplete regression of the lesion after months
or years
b. Visceral involvement
i. Mediastinum
ii. Neck
iii. Retroperitoneum
iv. Pelvis
c. Hemorrhage by aggressive invasion
d. Petechiae, ecchymoses, or purpura
e. Profound thrombocytopenia
f. Anemia
g. Congestive heart failure
h. Severe infections
i. Residual lesions after “cure” of Kasabach–Merritt
phenomenon (Enjolras et al. 2000)
i. Common after the resolution of thrombocy-
topenia and coagulopathy
ii. Clinical patterns
a) Cutaneous red stain with or without asso-
ciated red papules
b) Telangiectatic streaks and swelling
c) A minor, firm, irregular subcutaneous
mass assessed by palpation or deep
infiltration evidenced by CT scan or MRI
d) Sequelae in muscles and/or joints
j. Overall mortality (estimated to be 20–30%)
(El-Dessouky et al. 1988) due to complications
such as (Enjoiras et al. 1990):
i. Disseminated intravascular coagulation
ii. Respiratory failure due to a pressured
airway
iii. High-output heart failure due to presence of
a huge tumor
Diagnostic Investigations
1. Laboratory studies (Hall 2001)
a. Generally severe thrombocytopenia: occurs in
1–2 per 300–700 cases of hemangioma
b. Consumptive coagulopathy
i. Prominent fibrinogenopenia
ii. Usually elevated fibrin split (degradation)
products
iii. Usually elevated D-dimers (a measure of
fibrin split products)
iv. Depressed clotting factors V and VII
2. Ultrasound, MRI, or CT
a. To assess extent of the lesions
b. To identify the occult lesions
1220 Kasabach–Merritt Syndrome
3. Histology to determine subtypes of hemangioma
a. Kaposiform hemangioendothelioma of infancy
and childhood
i. The most frequently reported histological
type
ii. A locally aggressive, low-grade malignant
tumor
iii. Lobules or sheets of tightly packed spindle
cells or more rounded endothelial cells and
pericytes
iv. Infiltrative pattern of the cellular areas in the
dermis and subcutaneous fat and muscles,
generally containing few obvious vascular
lumina
v. Aggregates of rounded dilated capillaries,
lined by attenuated endothelial cells with
small dark nuclei and filledwith red blood cells
vi. Containing lymphatic-like vessels
b. Tufted angioma
i. A benign lesion
ii. Small tufts or lobules of rounded capillaries
with small lumina
iii. Tufts: discrete and evenly distributed in a
cannon ball pattern, characterized by periph-
eral crescentic slit-like vessels and fibrosis
iv. Aggregates of rounded dilated capillaries,
lined by attenuated endothelial cells with
small dark nuclei and filledwith red blood cells
Genetic Counseling
1. Recurrence risk
a. Patient’s sib: not increased unless a parent is
affected
b. Patient’s offspring: 50% in case of autosomal
dominant inheritance
2. Prenatal diagnosis: Prenatal diagnosis of fetal facial
hemangioma in a case of Kasabach–Merritt
syndrome
3. Management (Ryan et al. 2010)
a. General premise regarding treatment: Resolution
of the lesion will lead to a correction of the
consumptive coagulopathy, which is heralded
by a recovery in the platelet count.
b. Principle of management of thrombocytopenia
in Kasabach–Merritt syndrome should be to
“treat the patient and not the numbers.”
c. Prompt and vigorous management
i. Help to optimize the outcome
ii. No one treatment modality established as
consistently efficacious
d. Blood product support in the presence of sudden
decompensation or enlargement of the lesion
i. Fresh frozen plasma
ii. Cryoprecipitate if fibrinogen still less than
1.0 g/L
iii. Platelets transfusion should be reserved for
thrombocytopenic patient who is actively
bleeding or in preparation for a surgical
procedure.
iv. Tranexamic acid for profound fibrinolysis
e. Simple or single lesion
i. Vascular ligation
ii. Embolization
iii. Surgical excision
a) Surgical removal of a giant heman-
gioma: usually hazardous in the
presence of an uncontrolled consumptive
coagulopathy
b) Supporting and stabilizing hemostasis
while trying to remove or ablate the
lesion
c) Partial resection of tumor, reduction of
tumor blood, and vincristine chemother-
apy (Shen et al. 2010): Since the huge
tumor is the major cause of rapid platelet
destruction, the partial removal of the
tumor and U-shaped suture to reduce
tumor blood supply would reduce the
platelet destruction and, therefore, improve
the clinical condition, followed by skin
graft or flaps of the wound, and vincristine
chemotherapy necessary to prevent the
enlargement of the remaining tumor.
f. Diffuse or extensive lesions
i. Prednisone
ii. Alpha interferon
g. Adjuvant therapies
i. Vincristine
ii. Localized radiotherapy
iii. Combination chemotherapy (vincristine,
cyclophosphamide)
iv. Antifibrinolytic or antiplatelet agents
(tranexamic acid, ɛ-amino caproic acid,
pentoxifylline, ticlopidine)
Kasabach–Merritt Syndrome 1221
h. Potential future therapies
i. Laser therapy
ii. Antiangiogenic agents
iii. Pegylated recombinant human megakaryo-
cyte growth and development factor
(peg-rHuMGDF)
References
Alvarez-Mendoza, A., Lourdes, T. S., Ridaura-Sanz, C., et al.
(2000). Histopathology of vascular lesions found in
Kasabach–Merritt syndrome: Review based on 13 cases.
Pediatric and Developmental Pathology, 3, 556–560.Biban, P. (2003). Kasabach–Merritt syndrome and interferon
alpha: Still a controversial issue. Archives of Disease inChildhood, 88, 645–646.
Billio, A., Pescosta, N., Rosanelli, C., et al. (2001). Treatment
of Kasabach–Merritt syndrome by embolisation of a giant
liver hemangioma. American Journal of Hematology, 66,140–141.
Blei, F. (1998). Successful multimodal therapy for kaposiform
hemangioendothelioma complicated by Kasabach–Merritt
phenomenon: Case report and review of the literature.
Pediatric Hematology and Oncology, 15, 293–305.Brizel, H. E., & Raccuglia, G. (1965). Giant hemangioma with
thrombocytopaenia-radioisotope demonstration of platelet
sequestration. Blood, 26, 751–756.Cheerva, A. C., Bartolone, C., & Raj, A. B. (2010). Pediatric
Kasabach–Merritt syndrome. Medscape reference. Updated
Feb 23, 2010. Available at: http://emedicine.medscape.com/
article/956136-overview
de Terlizzi, M., Bonifazi, E., Toma, M. G., et al. (1988).
Kasabach–Merritt syndrome: Successful management of
coagulopathy with heparin and cryoprecipitate. PediatricHematology and Oncology, 5, 325–328.
Dresse, M. F., David, M., Hume, H., et al. (1991). Successful
treatment of Kasabach–Merritt syndrome with prednisone
and epsilon-aminocaproic acid. Pediatric Hematology andOncology, 8, 329–334.
El-Dessouky, M., Azmy, A. F., Raine, P. A. M., et al. (1988).
Kasabach–Merritt syndrome. Journal of Pediatric Surgery,23, 109–111.
Enjoiras, O., Riche, M. C., Merland, J. J., et al. (1990). Manage-
ment of alarming hemangiomas in infancy. Pediatrics, 85,491–498.
Enjolras, O., Mulliken, J. B., & Wassef, M. (2000). Residual
lesions after Kasabach–Merritt phenomenon in 41 patients.
Journal of the American Academy of Dermatology, 42,225–235.
Enjolras, O., Wassef, M., & Mazoyer, E. (1997). Infants with
Kasabach–Merritt syndrome do not have “true” hemangi-
omas. Journal of Pediatrics, 130, 631–640.Esterly, N. B. (1983). Kasabach–Merritt syndrome in infants.
Journal of the American Academy of Dermatology, 8,504–513.
Esterly, N. B. (1995). Cutaneous hemangiomas, vascular stains
and malformations, and associated syndromes. CurrentProblems in Dermatology, 7(3), 65–108.
Frevel, T., Rabe, H., Uckert, F., et al. (2002). Giant cavernous
haemangioma with Kasabach–Merritt syndrome: A case
report and review. European Journal of Pediatrics, 161,243–246.
Gianotti, R., Gelmetti, C., & Alessi, E. (1999). Congenital
cutaneous multifocal kaposiform hemangioendothelioma.
American Journal of Dermatopathology, 21, 557–561.Haisley-Royster, C., Enjolras, O., Frieden, I. J., et al. (2002).
Kasabach–Merritt phenomenon: A retrospective study
of treatment with vincristine. Journal of PediatricHematology/Oncology, 24, 459–462.
Hall, G. W. (2001). Kasabach–Merritt syndrome: Pathogenesis
and management. British Journal of Haematology, 112,851–862.
Hatley, R. M., Sabio, H., Howell, C. G., et al. (1993). Successful
management of an infant with a giant hemangioma of the
retroperitoneum and Kasabach–Merritt syndrome with
alpha-interferon. Journal of Pediatric Surgery, 28,1356–1357; discussion 1358–1359.
Hesselmann, S., Micke, O., Marquardt, T., et al. (2002). Case
report: Kasabach–Merritt syndrome: a review of the thera-
peutic options and a case report of successful treatment
with radiotherapy and interferon alpha. British Journal ofRadiology, 75, 180–184.
Kasabach, H. H., & Merritt, K. K. (1940). Capillary hemangi-
oma with extensive purpura. Report of a case. AmericanJournal of Diseases of Children, 59, 1063–1070.
Krafchik, B. R., Hendricks, L. K., & Faquet, G. B. (2010).
Kasabach–Merritt syndrome. Medscape reference. Updated
Feb 22, 2010. Available from: http://emedicine.medscape.
com/article/202455-overview
Larsen, E. C., Zinkham, W. H., Eggleston, J. C., et al. (1987).
Kasabach–Merritt syndrome: Therapeutic considerations.
Pediatrics, 79, 971–980.Lee, J. H., Jr. (1967). Kirk RF: Pregnancy associated with giant
hemangiomata, thrombocytopenia, and fibrinogenopenia
(Kasabach–Merritt syndrome). Report of a case. Obstetricsand Gynecology, 29, 24–29.
Ogino, I., Torikai, K., Kobayasi, S., et al. (2001). Radiation
therapy for life- or function-threatening infant hemangioma.
Radiology, 218, 834–839.Ozsoylu, S. (2002). Treatment of Kasabach–Merritt syndrome
by megadose methylprednisolone. Pediatric Hematologyand Oncology, 19, 373–374.
Phillippe, M., Acker, D., & Frigoletto, F. D., Jr. (1980). Preg-
nancy complicated by the Kasabach–Merritt syndrome.
Obstetrics and Gynecology, 56, 256–258.Powell, J. (1999). Update on hemangiomas and vascular
malformations. Current Opinion in Pediatrics, 11, 457–463.Respondek-Liberska, M., Janiak, K., Jakubek, A., et al. (2002).
Prenatal diagnosis of fetal face hemangioma in a case
of Kasabach–Merritt syndrome. Ultrasound in Obstetrics &Gynecology, 19, 627–629.
Ryan, C., Price, V., John, P., et al. (2010). Kasabach–Merritt
phenomenon: A single centre experience. European Journalof Haematology, 84, 97–104.
1222 Kasabach–Merritt Syndrome
Shen, W., Cui, J., Chen, J., et al. (2010). Kasabach–Merritt with
partial resection of tumor, reduction of tumor blood,
and vincristine chemotherapy. The Journal of CraniofacialSurgery, 21, 215–216.
Singh, G., & Rajendran, C. (1998). Kasabach–Merritt syndrome
in two successive pregnancies. International Journal ofDermatology, 37, 690–693.
Kasabach–Merritt Syndrome 1223
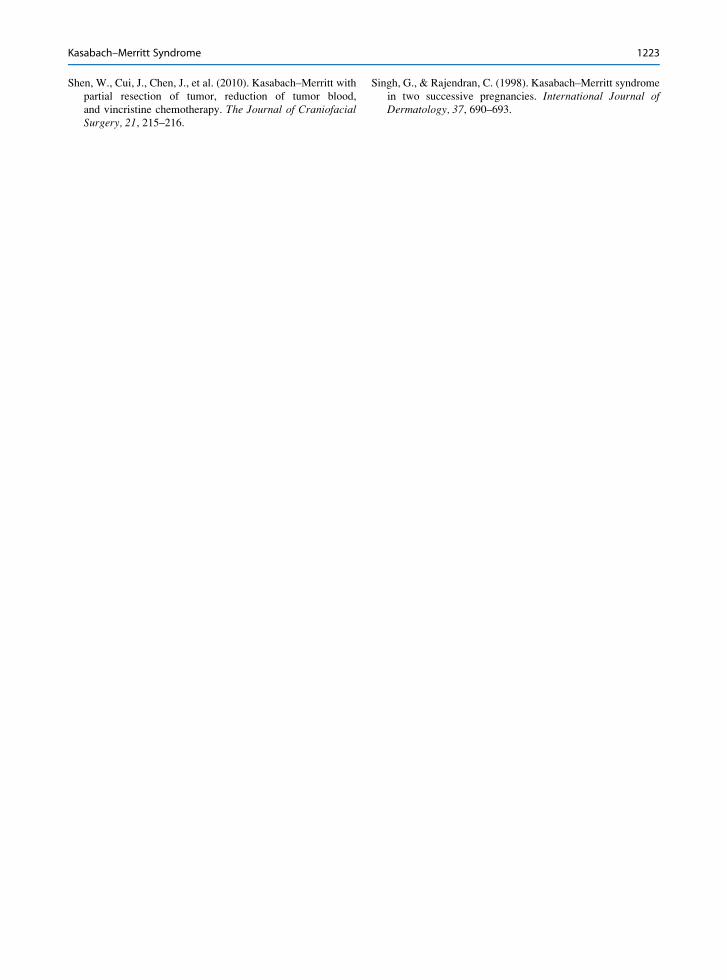
a b
Fig. 1 (a–b) An infant with Kasabach–Merritt syndrome showing a giant cavernous hemangioma over most of the chest
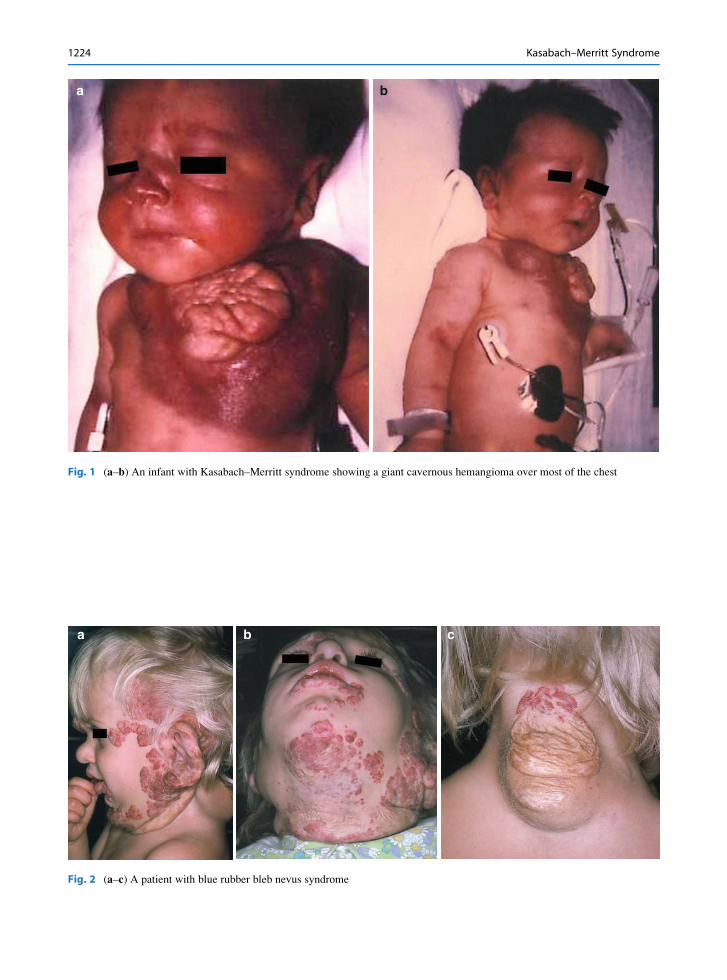
a b c
Fig. 2 (a–c) A patient with blue rubber bleb nevus syndrome
1224 Kasabach–Merritt Syndrome