Embed Size (px)
DESCRIPTION
second year of uni, small group practical
Citation preview

Attitudes of atheists and Muslims toward
euthanasia.
Dionne Angela Donnelly
Module: PSYC222: Research Methods & Statistics
Word Count: 2056 (excluding tables and quotations)
2642 (including tables and quotations)

Abstract
Research has shown that people who are religious are less likely to support euthanasia. The
researchers hypothesised that Muslims would be less likely than atheists to agree with the
practise of euthanasia. An opportunity sample of 25 Muslim and 25 atheist participants were
surveyed on their attitudes towards euthanasia using a 5 response Likert scale. Following
reliability analysis, 19 items were removed and the questionnaire was redistributed to the
original participants. The scale was found to be tridimensional and showed inter-item
consistency and reliability over time. Atheists were significantly more likely to agree with the
practice of euthanasia than Muslims. The results support previous research in the area,
indicating a strong relationship between religion and attitude toward euthanasia. Future
research could follow a more qualitative route to provide a better understanding of the
relationship between religion and euthanasia.
Euthanasia is defined as “intentionally causing the death of a person, to...protect [them] from further
suffering” (Perry, n.d.). Assisted suicide occurs when the patient “performs the act of suicide. The
other person simple helps” (Perry, n.d.). In this study, ‘euthanasia’ was used to refer to both terms.
There are conflicting views as to whether euthanasia should be legalised (e.g. Mak, Elwyn &
Finlay, 2003; Roscoe, 1998; Wilson et al., 2000). Religious people are more likely to oppose
euthanasia (Gielen, van den Branden & Broeckart, 2009; see also, Anderson & Caddell, 1993; Aslan
& Cavlak, 2007; Førde, Aasland & Falkum, 1997; Haghbin, Streltzer & Danko, 1998; Ward & Tate,
1994).
Muslims believe we should “not take life which God has made sacred except in the course of
Justice” (Qur’an, 6:151, cited in Zahedi, et al., 2007, p.11). But, in Islamic law, removing
1

hindrances to death (i.e. life support) to ease suffering is allowed as long as death is not the primary
motivation (Sachedina, 2005, see also, Ebrahim, 2005). One study found that 85 per cent of Muslim
doctors are opposed to euthanasia (Ahmed, Kheir, Rahman, Ahmed & Abdalla, 2001). However,
other research suggests this high figure may be more to do with doctors’ experience with dying
patients (Roscoe, 1998). Aslan and Cavlak (2007) found that 40 per cent of Muslim students were
opposed to euthanasia. Conversely, they also found that 47 per cent accepted it.
An explanation may be degree of religiosity. Gearing and Lizardi (2009) state that decreased
suicidal behaviour is related to religious commitment, not membership of a specific religion (see
also Aslan & Cavlak, 2007; Donnison, 1997; Grassi, Magnani & Ercolani, 1999; Haghbin et al.,
1998). Therefore, it is important to compare religious groups with groups that are non-religious.
Although atheists have no specific belief system, they generally do not believe in God or the
afterlife (Lizardi & Gearing, 2009). Smith-Stoner (2007) found that 95 per cent of self-reported
atheists supported euthanasia. Aslan and Cavlak found that 86.7 per cent of atheist students were in
favour of euthanasia (2007). This is higher than the average: Horsfall, Alcocer, Duncan and Polk
(2001), found that 72-74 per cent of students had a positive attitude towards euthanasia.
An attitude is predisposition to attend to the social world in a favourable or unfavourable way
(Oskamp & Schultz, 2005, see also Reich & Adcock, 1976). Attitudes consist of three components:
affective, behavioural, and cognitive (ABC) (Triandis, 1971). Likert scales are used in the majority
of survey research measuring attitudes (Hinkin, 1998; Taylor & Heath, 1996).
New measures are important because attitudes change over time: Wolfe, Fairclough, Clarridge,
Daniels and Emanual (1999), observed that one third of patients changed their attitude to euthanasia
in a follow-up interview (see also, DeCesare, 2000). Also, people’s attitudes towards euthanasia
2

may be more developed following exposure to the issue, especially since the case of Terry Schiavo
(e.g. Annas, 2005; Perry, Churchill & Kirshner, 2005).
This study aimed to create a uni-dimensional Likert scale, assess the reliability of the scale over
time, and assess whether commitment to a religion leads to opposition of euthanasia. We predicted
that atheists would be more likely to agree with the practise of euthanasia than Muslims, as
indicated by previous research.
Method
Participants
25 Muslims and 25 atheists were found using opportunity sampling. Participants were aged between
17 and 36 (M = 21.38, SD = 3.07). Other demographics were not collected as they were deemed
unnecessary.
Materials
The pilot questionnaire (T1) (see Appendix 1) was created by a brainstorming session focusing on a
balance of positive and negative items to avoid acquiescence bias (Taylor & Heath, 1996).
Attempts at a balance between affective, behavioural and cognitive related items were made.
Questionnaire T1 consisted of 50 short, simple statements (in accordance with Hinkin, 1998)
relating to attitudes toward euthanasia. It was designed so that positive attitudes towards euthanasia
would achieve a high score and negative attitudes a low score. The participant information sheet
(see Appendix 3) was attached to both T1 and T2 (see Appendix 2) questionnaires. Following the
reliability analysis (see Appendix 5) 19 items were removed from the questionnaire (see Table 1).
As Cronbach’s alpha was high (.98, see Appendix 5), removal criteria were stringent and included
removal for violation of only one assumption. Questionnaire T2 consisted of 31 items originally
from Questionnaire T1.
3

Table 1: Item deletion list.Item No.
Item Reasons for deletion
1 I view death as a positive and natural life occurrence. 1, 2, 3, 4, 5, 64 Euthanasia should be punished by law. 413 Death is random and not determined by a higher power. 215 I would be morally obliged to euthanize someone who was
incapable of making the decision themselves.1, 2, 4, 5, 6
16 I would actively seek to punish those who assisted with eu-thanasia.
1, 2
19 When I think of someone committing suicide it makes me feel sad.
1, 2, 4, 6
21 I feel that death is the end. 3, 5, 626 Euthanasia is an easy way out of a difficult situation. 4, 5, 632 Death never really crosses my mind. 4, 5, 636 Religious or spiritual people are more likely to have a neg-
ative view of euthanasia.1, 2, 3, 4, 5, 6
37 I would never consider ending my own life. 1, 438 I am not afraid of death 1, 4, 639 Euthanasia is immoral and the same as murder. 440 I would assist someone who wished to commit suicide. 141 Others’ judgement would stop me assisting euthanasia. 2, 4, 5, 646 Those who believe in the afterlife have a more positive
view of euthanasia.1, 2, 3, 4, 5
47 Everybody has the right to choose how and when they die. 448 I feel that everyone can be pushed to believe that suicide is
their only option.4
50 The method used to carry out euthanasia would affect my decision to carry it out on either myself or another person.
1, 41
Design
This study was a mixed design as participants filled out the scale twice (to test scale reliability) and
their responses then compared against one another to test for differences. This was done using a 5
response Likert scale (optimal for reliability, validity, discriminating power and test-retest
reliability, Preston & Colman, 1999). The independent variable (IV) was religious belief and
consisted of two levels; as participants were either Muslims or atheists (groups perceived by the
researchers to have strong opinions on death, to avoid central tendency bias). The dependent
variable (DV) was the extent to which participants would agree with the practise of euthanasia (i.e.
11= disparate mean [below 2.5, above 3.5]. 2 = disparate SD [below 1.05, above 1.7]. 3 = Negative inter-item correlations [for more than 10 items]. 4 = Low inter-item correlation [below .4 (Kim & Mueller, 1978, cited in Hinkin, 1998) in more than 5 items]. 5 = increases Cronbach’s alpha. 6 = Pearson’s correlation below .5.
4

T2 score). The predictor variable (PV) was T1 score and the outcome variable (OV) was T2 score.
Procedure
Questionnaire T1 was created by a group of five Psychology undergraduates as a pilot scale.
Questionnaires were distributed to self-reported Muslims and atheists. Participants were informed
of their right to withdraw and assured that their data would be confidential and anonymous (for
ethical reasons and to help avoid social desirability bias). Once the data was collected it was
analysed using SPSS to test for reliability, using the most accepted measure of reliability -
Cronbach’s alpha (Price and Mueller, 186, cited in Hinkins, 1998). Questionnaire T2 contained 31
questions which were all originally from Questionnaire T1. These were re-distributed to the same
participants as Questionnaire T1. This was followed by a second reliability analysis, t-test, and
linear regression analysis. No questions were excluded following the final analysis.
Results
T1 Reliability
A reliability analysis was conducted using the SPSS programme. Cronbach’s alpha was .98 (see
Appendix 5) indicating that the questionnaire had internal consistency. However, the mean inter-
item correlation was .42 (see Table 2), which is relatively low and indicated that the questionnaire
may be multi-dimensional. Therefore, a factor analysis using Varimax orthogonal rotation was
conducted which extracted 8 factors with Eigen values ≥ 1.0. These factors accounted for 79.47 per
cent of variation in participants’ responses (see Table 4 and Appendix 6). This means that whilst the
scale was measuring 8 different psychological constructs, only approximately 20 per cent of
responses were due to ‘noise’ in the data. The mean item means were 2.9, close to the optimal
number of 3, meaning that one group responded with mostly ‘strongly agree’ and the other ‘strongly
disagree’, the mean therefore showing a balance between the two extremes. Mean item variances
were 1.87 (see Table 2).
5

Table 2: Summary Item data – T1.
T2 Reliability
Cronbach’s alpha was .98 (see Appendix 7), an increase on the previous questionnaire due to the
removal of 19 items from T1 (based on criteria set out in Table 1). Mean inter-item correlation
was .66 (see Table 3), which indicated that there were fewer factors than the previous questionnaire.
Factor analysis using Varimax orthogonal rotation extracted 3 factors with Eigen values ≥1.0. They
accounted for 77.67% of variation in participants’ responses (see Table 4 and Appendix 8). This
meant the scale was multi-dimensional, and only approximately 22 per cent of responses were due
to ‘noise’. In this instance, mean item-means decreased to 2.88, indicating that respondents were
less likely to respond in the extreme to the items. Mean item variances increased to 2.17 (see Table
3).
Table 3: Summary Item Data – T2.
Table 4: Factor Analysis – T1 and T2
Factors FoundVariance Accounted
For (%)
T1 8 77.62
T2 3 79.47
Test-Retest ReliabilityBivariate correlatory analysis showed that there was a significant positive relationship between
participants’ T1 and T2 scores (N = 50, r = .96, p < .001, see Appendix 9), indicating that the scale
6
N Mean (Variance)
Item Means 50 2.9 (.28)
Item Variances 50 1.87 (.5)
Inter-Item Correlations 50 .42 (.13)
N Mean (Variance)
Item Means 31 2.88 (.08)
Item Variances 31 2.17 (.42)
Inter-Item Correlations 31 .66 (.03)

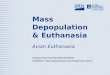
was reliable over time. Linear regression analysis showed that scores on T1 predicted 91 per cent of
variance of T2 scores (R2 = .92, ∆R2 = .91, F (1, 48) = 522.7, p < .001, VIF = 1) (see Appendix 11).
The regression equation is y = .92x + 1.41 (where y = bx + c) (see Figure 1).
Figure 1: Scatterplot and regression line showing the relationship between T1 and T2 scores.
Criterion
Levene’s Test for Equality of Variance was non-significant. Therefore, homogeneity of variance was
assumed. An independent sample t-test (one-tailed) found that atheists were significantly more
likely to agree with the practise of euthanasia (M = 116.28, SD = 11.64) than Muslims (M = 50.96,
SD = 10.3), (t(48) = 20.99, p < .01) (see Table 5 and Appendix 10).
Table 5 – Total means for each group at T1 and T2.
7
Group N Mean (SD)
T1 Total Score Atheist 25 122.96 (11.89)
Muslim 25 55.2 (10.82)
T2 Total Score Atheist 25 116.28 (11.64)
Muslim 25 50.96 (10.33)

Discussion
It was found that atheists were significantly more likely to agree with euthanasia than Muslims.
This is in concordance with previous research suggesting that Muslims are likely to be opposed to
the practise of euthanasia, due to their religious views (e.g. Sachedina, 2005, Ahmed et al., 2001;
Ebrahim, 2005; Zahedi, et al., 2007) and level of religious commitment (Gearing & Lizardi, 2009,
see also Donnison, 1997; Grassi, Magnani & Ercolani, 1999; Haghbin et al., 1998). Furthermore,
atheists have been shown to be highly supportive of euthanasia (Aslan & Cavlak, 2007; Smith-
Stoner, 2007). This study therefore provides supporting evidence for the above research.
In this study 88 per cent of atheists disagreed or strongly disagreed (the remaining 12 per cent were
neutral) with the statement “Euthanasia is never acceptable, even when performed by a loved one or
qualified physician” (see Appendix 2, Item 4). This points to their acceptance of the practise of
euthanasia. Despite being a high figure, it was lower than the 95 per cent of atheists who agreed
with euthanasia in Smith-Stoner’s (2007) study. The difference may be due to participant
characteristics, as her participants were all members of an atheist organisation, and the majority had
cared for an atheist who had died. However, the figure is slightly higher than the 86.7 per cent
found by Aslan and Cavlak (2007), which may be due to their smaller sample size (30 atheist
participants).
All Muslim participants agreed or strongly agreed with Item 4 thus indicating their opposition to
euthanasia. This figure is much higher than the 40 per cent who opposed euthanasia in the study by
Aslan & Cavlak (2007) and the 85 per cent found by Ahmed et al. (2001). This may be due to the
fact that the above studies were conducted in Islamic countries, and respondents in the UK may feel
more pressure to respond in a socially desirable way (Saroglou & Galand, 2004) in order to
strengthen other groups’ view of commitment to their religion. Conversely, atheists do not have
rigid set of beliefs (Gearing & Lizardi, 2009) and so may not feel as pressured to conform to others’
8

view of them.
Aside from assessing the effect of religion on attitudes to euthanasia, this study aimed to create a
uni-dimensional Likert scale, and assess the reliability of the scale over time. Ultimately a
tridimensional scale was created which was found to be highly reliable over time. However, there
were several limitations of the study; the first being a relatively small sample size, which could
cause difficulty for generalising to a wider population. The researchers also had difficulty in
balancing ABC components of the scale, meaning the scale may have been biased in favour of
affective and cognitive items.
In light of such limitations, there are a number of implications for future research. Other groups,
such as agnostics and Christians, could be included to evaluate whether different religious beliefs
will contrast with atheism as strongly as Islam did. Also, a more qualitative study could be
conducted, presenting hypothetical situations and asking participants to decide how they would
behave, followed by open questions asking about their opinions. This could help establish the
reasons why there is a difference between the groups. This may also establish if other factors, such
as the type of illness and time left to live, have an effect on whether euthanasia is deemed
appropriate.
In conclusion, it was found that atheists were significantly more likely to approve of euthanasia than
Muslims. This is in accordance with the majority of research into this area, which states that
religiosity exerts an effect on attitudes towards euthanasia.
9

References
Ahmed, A. M., Kheir, M. M., Rahman, A. A., Ahmed, N. H. & Abdalla, M. E. (2001). Attitudes
towards euthanasia and assisted suicide among Sudanese doctors. Eastern Mediterranean Health
Journal, 7(3), 551-555.
Anderson, J. G. & Caddell, D. P. (1993). Attitudes of medical professionals toward euthanasia.
Social Science and Medicine, 10(4), 923-928.
Annas, G. J. (2005). "Culture of Life" politics at the bedside - the case of Terri Schiavo. New
England Journal of Medicine, 352(16), 1710-1716.
Aslan, U. B. & Cavlak, U. (2007). Attitudes towards euthanasia among university students: A
sample based on Turkish population. Journal of Medical Science, 7(3), 396-401.
DeCesare, M. A. (2000). Public attitudes toward euthanasia and suicide for terminally ill persons:
1977 and 1996. Social Biology, 47(3/4), 263-276.
Donnison, D. (1997). Not just an issue of life and death – the British Social Attitudes Survey.
Retrieved 5 December 2009 from www.euthanasia.cc/97-1dvd.html
Ebrahim, A. F. M. (2005). [Review of the book Islamic Ethics of Life: Abortion, War and
Euthanasia, by Brockopp, J. (Ed.)]. Journal of Islamic Studies, 16(3), 376-378.
Førde, R., Aasland O. G. & Falkum, E. (1997). The ethics of euthanasia: Attitudes and practice
among Norwegian physicians. Social Science and Medicine, 45, 887-892.
Gearing, R. E. & Lizardi, D. (2009). Religion and suicide. Journal of Religion and Health, 48,332-
341.
Gielen, J, van den Branden, S. & Broeckart, B. (2009). Religion and nurses’ attitudes to euthanasia
and physician-assisted suicide. Nursing Ethics, 16(3), 303-318.
Grassi, L., Magnani, K. & Ercolani, M. (1999). Attitudes toward euthanasia and physician-assisted
suicide among Italian primary care physicians. Journal of Pain and Symptom Management,
17(3), 188-196.
Haghbin, Z., Strelzer, J. & Danko, G. P. (1998). Assisted suicide and AIDS patients: A Survey of
10

physicians’ attitudes.Psychosomatics, 39, 18-23.
Hendin, H. (1995). Suicide, assisted suicide and euthanasia. Crisis, 17(2), 90-93.
Hinkin, T. R. (1998). A brief tutorial on the development of measures for use in survey
questionnaires. Organizational Research Methods, 1(1), 104-121.
Horsfall, S., Alcocer, C. D., Duncan, T. C. & Polk, J. (2001). Views of euthanasia from an east
Texas university. Social Science Journal, 38, 617-627.
Lizardi, D. & Gearing, R. E. (2009). Religion and suicide: Buddhism, Native American and African
religions, atheism and agnosticism. Journal of Religion and Health, Online First, Article 53.
Retrieved 2 December 2009 from http://www.springerlink.com.ezproxy.liv.ac.uk/content/w23
8202221436w03/fulltext.pdf
Mak, Y. Y. W., Elwyn, G. & Finaly, I. G. (2003). Patients’ voices are needed in debates on
euthanasia. British Medical Journal, 327, 213-215.
Oskamp, S. & Schultz, P. W. (2005). Attitudes and Opinions (3rd ed.). New Jersey: Lawrence
Erlbaum Associates.
Perry, C (n.d.). Euthanasia and assisted suicide. Retrieved 2 December 2009 from http://
www.pages.drexel.edu/~cp28/euth1.htm
Perry, J. E., Churchill, L. R. & Kirshner, H. S. (2005). The Terri Schiavo case: Legal, ethical, and
medical perspectives. Annals of Internal Medicine, 143, 744-748.
Preston, C. C. & Colman, A. M (1999). Optimal number of response categories in rating scales:
Reliability, validity, discriminating power, and respondent preferences. Acta Psychologica,
104,1-15.
Reich, B. & Adcock, C. (1976). Values, attitudes and behaviour change. London: Methuen & Co.
Roscoe, L. A. (1998). The many faces of physician-assisted suicide. Journal of Aging and identity,
(1), 35-48.
Sachedina, A. (2005). End-of-life: The Islamic view. Lencet, 366, 774-779.
11

Saroglou, V. & Galand, P. (2004). Identities, values, and religion: A study among Muslim, other
immigrant, and native Belgian young adults after the 9/11 attacks. Identity: An International
Journal of Theory and Research, 4(2), 97–132.
Smith-Stoner, M. (2007). End-of-life preferences for atheists. Journal of Palliative Medicine, 10(4),
923-928.
Taylor, B. & Heath, A. (1996). The use of double-sided items in scale construction. Centre for
Research into Elections and Social Trends Working Paper, 37.
Triandis, H. C. (1971). Attitude and attitude change. New York: John Wiley & Sons.
Ward, B. J. & Tate, P. A. (1994). Attitudes among NHS doctors to requests for euthanasia. British
Medical Journal, 308,1332-1334.
Wilson, K. G., Scott, J. F., Graham, I. D., Kozak, J. F., Chater, S., Viola, R. A., de Faye, B. J.,
Weaver, L. A & Curran, D. (2000). Attitudes of terminally ill patients toward euthanasia and
physician-assisted suicide. Archives of Internal Medicine, 160, 2454-2460.
Wolfe, J., Fairclough, D. L., Clarridge, B. R., Daniels, E. R. & Emanual, E. J. (1999). Stability of
attitudes regarding physician-assisted suicide and euthanasia among oncology patients,
physicians and the general public. Journal of Clinical Oncology, 17, 1274-1279.
Zahedi, F., Larijani, B. & Bazzaz, J. T. (2007). End of life ethical issues and Islamic views. Iranian
Journal of Allergy, Asthma and Immunology, 6(5), 5-15.
Appendices
For appendices, please refer to the compact disc provided.
12