Embed Size (px)
Citation preview
Rrrrirh J o i m m ; ofb’rology ( 1 993), 72, 478--483 (111 1993 British Journalof Urology
Audit and its Impact in the Management of Advanced Prostatic Cancer
A. RANA, G. D. CHISHOLM, S. CHRISTODOULOU, MARGARET MclNTYRE and R . A. ELTON
University. Department of SurgerylUrology and Department of Pathology, Western General Hospital; Medical Statistics Unit, University of Edinburgh, Edinburgh
Summary-From a prospective database of 6 14 consecutive men with newly diagnosed prostatic cancer an audit of outcome was studied in 169 men who presented with bone metastases and subsequently received hormonal manipulation in the form of monotherapy. The cohort was divided into 2 groups according to serum alkaline and acid phosphatase enzyme levels. M e n with normal alkaline phosphatase levels (41 5%) had a better prognosis (median survival 38 months) than those with elevated levels at presentation (58.5%) (median survival 19 months). This difference was highly significant. A similar stratification on prostatic acid phosphatase levels did not yield any prognostic significance. With regard to cause-specific survival, serum alkaline phosphatase was an even more powerful prognosticator, with a median survival of 45 and 2 1 months for patients with normal and elevated levels respectively. Thus monotherapy is recommended for metastatic prostate cancer patients with normal serum alkaline phosphatase, but for those with elevated alkaline phosphatase the alternative avenues of treatment must be explored.
Hormonal manipulation is an effective method of palliation in patients with advanced carcinoma of the prostate (CAP). However, the use of oestrogens or orchiectomy has recently come under scrutiny (Rasmussen, 1989). Not satisfied with symptomatic palliation alone, clinicians are continuing the quest to improve survival. Forty years after the pioneering work of Huggins and Hodges(l941), Labrie et al. ( 1983) polarised the medical community with their theory of total androgen blockade as a new approach in the treatment of advanced CAP. This led to numerous clinical trials and the significance of the results is still controversial. Even those who have reported better results with total androgen blockade have not been able to reproduce the “dramatic response” claimed by Labrie ef al. (1985). Hence monotherapy in the form of orchiectomy remains the standard treatment (Schroeder, 1991).
This department has used monotherapy, mostly in the form of subcapsular orchiectomy, for ad-
Accepted for publication 28 Janaury 1993
vanced carcinoma of the prostate. A database was established in 1978 in order to evaluate and compare the results with those of alternative treatments. Two important questions have arisen. Should there be a change to total androgen blockade? Are the added costs of these drugs justified? We have analysed the clinical outcome of a consecutive series of men presenting with advanced CAP with a mimimum follow-up of 1 year in order to relate our results to those of other recently reported series.
Patients and Methods
The database was a prospective cohort of 614 consecutive men with newly diagnosed CAP pre- senting between January 1978 and December 1990; 169 men had bone metastases (M1 disease) at the time of presentation and they constituted the study group.
Bone scintigraphy was performed on all patients after intravenous administration of 99mtechnetium methylene diphosphonate. Hot spots were further radiographed in order to confirm bone metastases
478
AUDIT AND ITS IMPACT IN THE MANAGEMENT OF ADVANCED PROSTATIC CASCER 479
or exclude benign abnormalities. Total serum alkaline phosphatase was measured by an enzy- matic method and a cut-off level was set at 140 u/l , dividing the cohort into 2 groups with normal and elevated levels. Serum PAP was also measured by an enzymatic method and a cut-off upper level was set at 2u/ 1 (Byar and Corlc, 198 l), thus dividing the cohort into 2 groups.
These men were treated with subcapsular or- chiectomy within 6 weeks of diagnosis. They were then monitored every 3 months with clinical, haematological and biochemical investigations. Follow-up bone scans and chest X-rays were performed as dictated by their symptoms and/ or serum enzymes.
All men were followed up until the end of December 1991. Deaths and the causes were recorded. The overall survival was estimated by the Kaplan and Meier method for the complete cohort and within the subgroups defined by the alkaline phosphatase and acid phosphatase levels at diag- nosis. The log rank test was used to assess any difference in the survival of strata.
1.00 -
0.75
0 . 2 5 -
0.00 -
Results
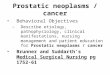
A total of 169 men with prostate cancer had bone metastases at presentation as confirmed with 9 9 m T ~ labelled MDP bone scans and skeletal radiographs; 70 men (mean age 71 years, median Gleason score 6.5) presented with bone metastases and normal serum AP: 41 (59%) had prostate cancer related deaths (CR), 12 (17%) had non-cancer related deaths (NCR), and the remaining 17 (24%) were alive at the end of the follow-up. Of the remaining 99 men (mean age 69 years, median Gleason score 7) with elevated serum AP and bone metastases, 75 (76%) succumbed to their cancer, 13 (13%) had non-cancer deaths and the remaining 1 1 ( 1 1 %) were alive. Figure 1 compares the overall survival by the Kaplan-Meier method for these men stratified into a normal and elevated level of serum AP at presentation. Men with normal serum AP survived longer than those with elevated levels, and the difference was highly significant (log rank x 2 = 14.9, P < 0.01). The median survival times for the 2 groups were 38 and 19 months respectively.
Log-rank Chi square 14.88 p<o.o1
Serum Alkphos 4 4 0 Age =71 yr, GI = 6.5 ,140 Age 4 9 yr, GI = 7 .......__........_.._
-3 I I I I I I I I
0 20 4 0 60 8 0 100 1 2 0 140 160
T i m e (months)
Fig. 1 Prognostic significance of low and elevated serum alkaline phosphatase on survival in metastatic prostate cancer
4x0 BRITISH JOURSAL OF UROLOGY
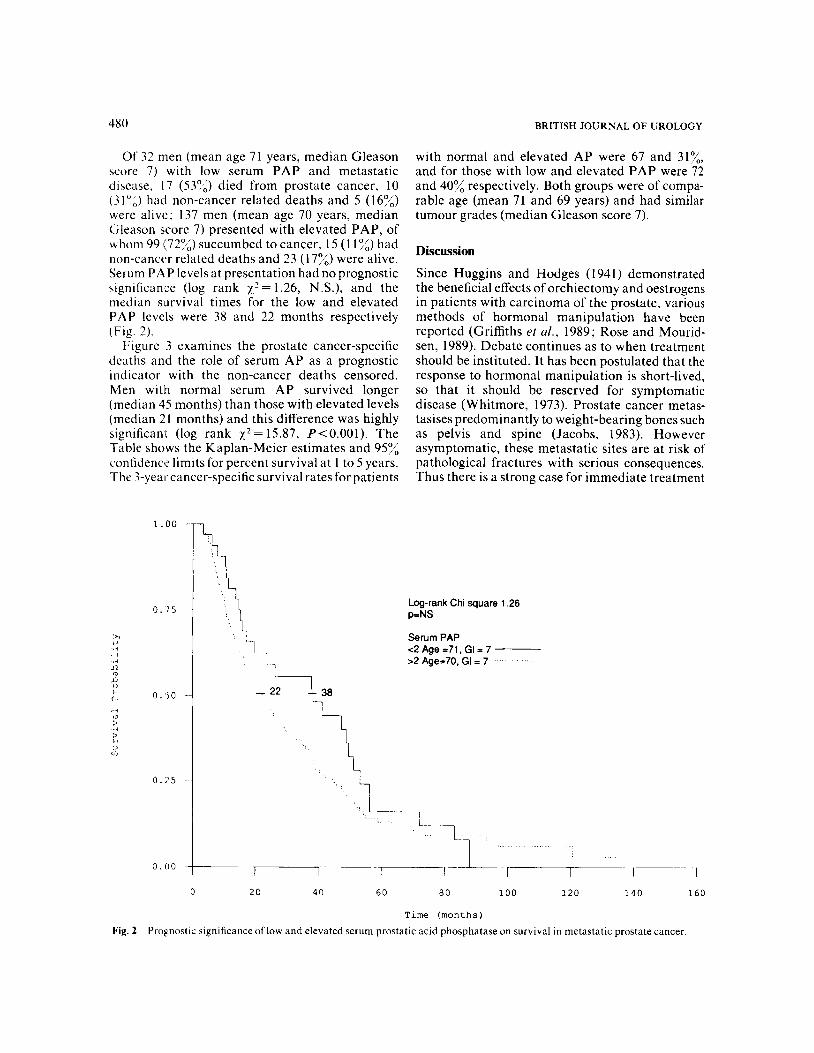
Of 32 men (mean age 71 years, median Gleason score 7) with low serum PAP and metastatic disease, 17 (539,) died from prostate cancer, 10 ( 3 1 ",) had non-cancer related deaths and 5 ( 1 6%) were alive; 137 men (mean age 70 years, median Gleason score 7) presented with elevated PAP, of whom 99 (72";) succumbed to cancer, 15 (1 1"/',) had non-cancer related deaths and 23 ( 1 759 were alive. Serum PAP levels at presentation had no prognostic significance (log rank y.'= 1.26, N.S.), and the median survival times for the low and elevated P A P levels were 38 and 22 months respectively (Fig. 2).
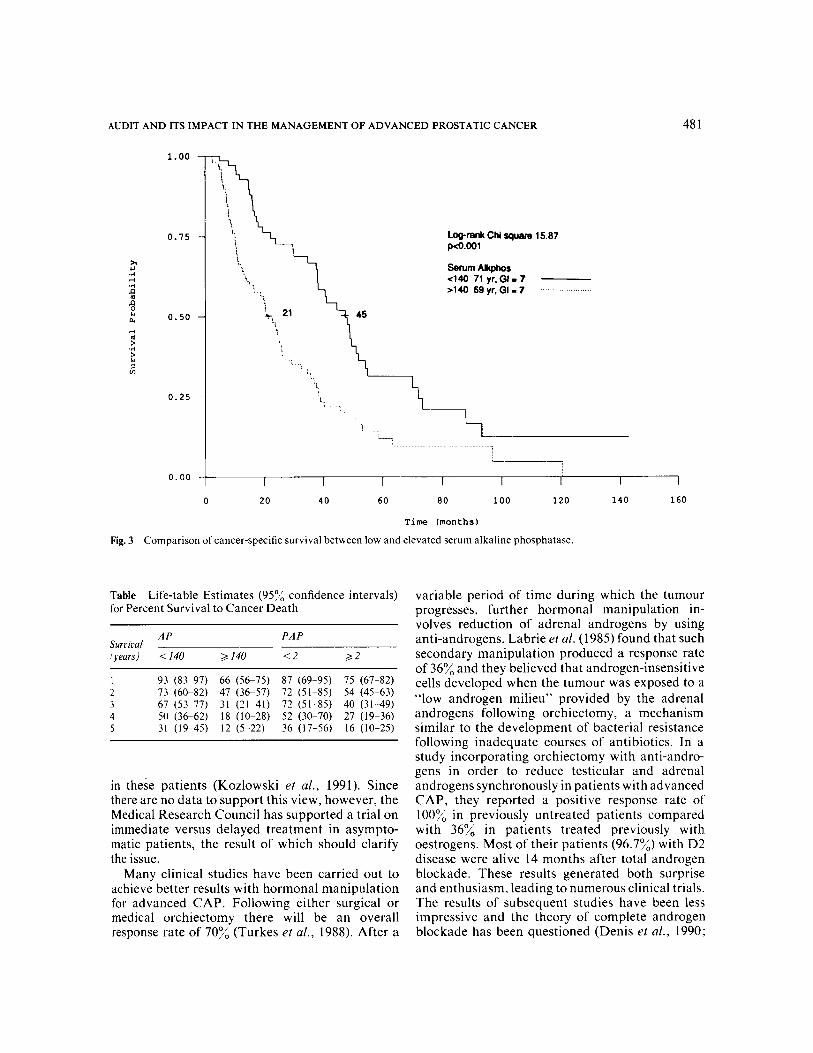
Figure 3 examines the prostate cancer-specific deaths and the role of serum AP as a prognostic indicator with the non-cancer deaths censored. Men with normal serum AP survived longer (median 45 months) than those with elevated levels (median 21 months) and this difference was highly significant (log rank x 2 = 15.87, P<O.OOI). The Table shows the Kaplan-Meier estimates and 95% confidence limits for percent survival at 1 to 5 years. The 3-year cancer-specific survival rates for patients
with normal and elevated AP were 67 and 31%, and for those with low and elevated PAP were 12 and 4004 respectively. Both groups were of compa- rable age (mean 71 and 69 years) and had similar tumour grades (median Gleason score 7).
Discussion
Since Huggins and Hodges (1941) demonstrated the beneficial effects of orchiectomy and oestrogens in patients with carcinoma of the prostate, various methods of hormonal manipulation have been reported (Griffiths et al., 1989; Rose and Mourid- sen, 1989). Debate continues as to when treatment should be instituted. It has been postulated that the response to hormonal manipulation is short-lived, so that it should be reserved for symptomatic disease (Whitmore, 1973). Prostate cancer metas- tasises predominantly to weight-bearing bones such as pelvis and spine (Jacobs, 1983). However asymptomatic, these metastatic sites are at risk of pathological fractures with serious consequences. Thus there is a strong case for immediate treatment
Log-rank Chi sauare 1.26
Serum PAP c2Age=71, GI= 7 ~
>2 Age=70, GI = 7 1
'-1
- 2 2 1 , 38
'1
0 20 40 60 8 0 100 120 140 1 6 0
T i m e (months)
Fig. 2 Prognostic significance of low and elevated seruni prostatic acid phosphatase on survival in metastatic prostate cancer.
AUDIT AND ITS IMPACT IN THE MANAGEMENT OF ADVANCED PROSTATIC CANCER 48 1
1.00
0 .75
>r -4 4 .4 n 3
0.50 rl 4
..-I z u)
0.25
0.00
@-rank Chi square 15.87 FUO.001
Serum Akphos 4 4 0 71 yr. GI I 7 ,140 69 yr, GI I 7 ...........__.__.....
1 I 1 I I I I I 0 20 40 60 80 100 120 140 160
T i m e (months)
Fig. 3 Comparison of cancer-specific survival between low and elevated serum alkaline phosphatase.
Table Life-table Estimates (957; confidence intervals) for Percent Survival to Cancer Death
A P PAP Suriiral iyears) < 140 2 140 <2 22
1 93 (83-97) 66 (56-75) 87 (69-95) 75 (67-82) 2 73 (60-82) 47 (36-57) 72 (51-85) 54 (45-63) 3 67 (53-77) 31 (21-41) 72 (51-85) 40 ( 3 1 4 9 ) 4 50 (36-62) 18 (10-28) 52 (30-70) 27 (19-36) 5 31 (19-45) 12 (5-22) 36 (17-56) 16 (10-25)
in these patients (Kozlowski et al., 1991). Since there are no data to support this view, however, the Medical Research Council has supported a trial on immediate versus delayed treatment in asympto- matic patients, the result of which should clarify the issue.
Many clinical studies have been carried out to achieve better results with hormonal manipulation for advanced CAP. Following either surgical or medical orchiectomy there will be an overall response rate of 70% (Turkes et al., 1988). After a
variable period of time during which the tumour progresses, further hormonal manipulation in- volves reduction of adrenal androgens by using anti-androgens. Labrie er al. (1985) found that such secondary manipulation produced a response rate of 36% and they believed that androgen-insensitive cells developed when the tumour was exposed to a “low androgen milieu” provided by the adrenal androgens following orchiectomy, a mechanism similar to the development of bacterial resistance following inadequate courses of antibiotics. In a study incorporating orchiectomy with anti-andro- gens in order to reduce testicular and adrenal androgens synchronously in patients with advanced CAP, they reported a positive response rate of lOOYA in previously untreated patients compared with 36% in patients treated previously with oestrogens. Most of their patients (96.7%) with D2 disease were alive 14 months after total androgen blockade. These results generated both surprise and enthusiasm, leading to numerous clinical trials. The results of subsequent studies have been less impressive and the theory of complete androgen blockade has been questioned (Denis et af., 1990;

482 BRITISH JOURNAL OF UROLOGY
Iversen, 1990; Lunglmayr, 1990; Schroeder, 1991 ; Tyrrell e ta / . , 1991).
Crawford et al. (1989) reported a large multi- centre placebo-controlled double-blind prospective randomised study comparing testicular androgen blockade with total androgen blockade in 603 patients with metastatic disease. The median survival (overall) was 35.6 and 28.3 months respec- tively. There were statistically significant advan- tages in terms of disease progression and survival in favour of total androgen blockade. However, it should be borne in mind that strict inclusion criteria in that study may have minimised the common cardiovascular morbidities of old age, with a consequent reduction in non-cancer deaths, and thus an apparent increase in their median survival. In contrast, the present study has not excluded poor risk patients from audit and statistical analysis. The Canadian Anandron study group reported a prospective randomised study comparing orchiec- tomy and placebo with orchiectomy and Anandron in metastatic disease. In terms of subjective and objective response and median length of survival, there were significant benefits with total androgen blockade. Janknegt et al. (1991) reported a large double-blind prospective randomised trial compar- ing testicular androgen blockade with total andro- gen blockade. Again, in terms of objective response and cancer-specific survival there were significant advantages, and the median survival was increased by 5 months in the total androgen blockade group.
Similar studies have compared the outcome between monotherapy and combination therapy. EORTC 30853 did not demonstrate any survival benefit with total androgen blockade and the median survival was approximately 30 months in both groups (Denis et al., 1990). Subjective and objective progression was, however, significantly delayed (P=0.02 and P=0.03). The majority of patients (82%) died from prostate cancer and 10% from cardiovascular disease. Again, this can be attributed to their selection criteria. Patients over the age of 80, with a life expectancy of less than 3 months and WHO performance status worse than 2 were excluded in their series. Iversen (1990) reported the Danish prostate cancer group study comparing orchiectomy with LHRH analogues plus flutamide in 262 men with advanced CAP. The survival, time to disease progression and subjective response did not differ between the 2 arms but the objective response was better with total androgen blockade (P= 0.047). The Interna- tional Prostate Cancer Study Group conducted another large multicentre randomised trial compar-
ing the effects of LHRH analogues with LHRH analogues plus flutamide in 571 men with advanced CAP. There were no differences in subjective and objective response or in survival between the 2 arms, and the median survival was 24 months for metastatic disease (Tyrrell e ta / . , 1991).
Whilst the theory of total androgen blockade may be logical, the clinical results are conflicting, The extra cost of drugs has become another key issue. This prompted us to review our database and to look for a cohort in whom such treatment could be justified.
When the representatives of American, Cana- dian, Danish and EORTC clinical groups and their statisticians met and analysed their results, the subjective and objective responses were found to have different interpretations (Robinson, 1990). Different entry criteria and interpretation of re- sponse alone can influence the results of randomised trials. Crawford (1990) stressed that cancer-specific survival should be determined in non-randomised studies, hence we have stratified our data accord- ingly. In the analysis of cancer deaths in metastatic disease, the median survival was 45 months following monotherapy in patients with normal serum AP, marginally better than the results (35.6 months) with total androgen blockade reported by Crawford (1990). In contrast, men with elevated serum AP had a median survival of only 21 months. Thus serum AP level at diagnosis is an excellent prognostic indicator in metastatic prostate cancer.
Elevation of serum PAP has been known to precede the development of a bone metastasis, which is then followed by an elevation of serum AP (O’Donoghue et al., 1978; Merrick et al., 1985). Serum AP level was reported to be as useful as scintigraphy in predicting survival even in the majority of patients with non-metastatic disease (Merrick et al., 1985). Nevertheless, without bone scan and skeletal radiographs, serum AP level alone cannot differentiate bone metastasis from benign disease (Merrick and Merrick, 1985). The present study included men with unequivocal bone metas- tases identified by a bone scan and relevant skeletal radiographs.
Why is alkaline phosphatase a powerful prognos- tic factor in advanced CAP? We believe that prostate cancer dissemination to bone is accurately sensed by the osteoblasts, which respond by elevating the AP level locally and then in the serum. The other potential source of serum AP is liver secondaries, but we have not seen an instance of deranged liver function or ultrasonic evidence of liver deposits in our surviving patients with elevated

AUDIT AND ITS IMPACT IN THE MANAGEMENT OF ADVANCED PROSTATIC CANCER 483
serum AP, and routine estimation of the liver isoenzyme does not seem justified. Although 99mTc labelled methylene diphosphonate (MDP) bone scan is more sensitive and skeletal radiographs are more specific for identifying bone metastases, a raised level of serum AP is an objective evidence of tumour load in the bones and is certainly a more valid predictor of poor prognosis despite testicular androgen blockade. In men with elevated serum AP, cancer-specific survival with monotherapy is so poor (3-year survival 3 1 % uersus 67% for normal AP) that an alternative therapy must be considered. To date, the better alternative is total androgen blockade and the present audit can justify the cost and side effects of drugs involved in such a select group of men.
In conclusion, we advocate monotherapy in metastatic prostate cancer with normal serum AP. However if the serum AP is elevated at presenta- tion, the prognosis is poor with monotherapy alone and therefore alternative avenues of treatment, including total androgen blockade, must be ex- plored.
Acknowledgement We are grateful to Mrs Elizabeth Brunton, prostate cancer secretary, for her dedication and expertise.
References Byar, D. P. and Corle, D. K. (I98 I ) . VACURG randomised trial
of radical prostatectomy for stages I and I1 prostate cancer. Urology (Suppl.), 17,7-1 I .
Crawford, E. D. (1990). Round table discussion. Eur. Urol, (Suppl. 3) , 18.64.
Crawford, E. D., Eisenberger, M. A., McLeod, D. G. et d (1989). A controlled trial of Leuprolide with and without Flutamide in prostatic carcinoma. N . Engl. J . Med. , 321,419424.
Denis, L., Smith, P. H., Carneiro DeMoura, J. L. et ol. (1990). Orchidectomy vs. Zoladex plus Flutamide in patients with metastatic prosate cancer. Eur. Urol. (Suppl. 3 ) . 18,3440.
Griffiths, K., Eaton, C. L. and Davies, P. (1989). Prostatic cancer; aetiology and endocrinology. Horm. Res. (Suppl. I ) . 32, 38- 43.
Huggins, C. and Hodges, C. V. (1941). Studies on prostate cancer.1. The effect of castration, of estrogen, and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res.. 1,293-297.
Iversen, P. (1990). Zoladex plus Flutamide vs. orchidectomy for advanced prostatic cancer. Eur. Urol. (Suppl. 3 ) , 18,4144.
Jacobs,.% C. (1983). Spread of prostatic cancer to bone. Urology,
Janknegt, R. A., Fernandezdel Moral, P., Abbou,C. e t d (1991). Effrcacy and tolerance of a total androgen blockade with anandron and orchidectomy : a double blind placebo con- trolled multicenter study. Abstract 852. AUA Eighty-sixth Annual Meeting. Toronto.
2L,337 344.
Advanced prostatic carcinoma. Early versus late endocrine therapy. Urol. Clin. North Am., 18, 15 24:
Labrie, F., Dupont, A. and Belanger, A. (1985). Complete androgen blockade for the treatment of prostate cancer. In Important Advances in Oncology. ed. De Vita, V. T., Jr, Hellman, S. and Rosenberg, S. A. Pp. 193-217. Philadelphia: Lippincott.
Labrie, F., Dupont, A., Belanger, A. et al. ( I 983). New approach in the treatment of prostate cancer: complete instead of only partial withdrawal of androgens. The Proslate, 4,579-594.
Lunglmayr, G. on behalf of the International Prostate Cancer Study Group (1990). A multicenter trial comparing the luteinising hormone releasing hormone analog Zoladex, with Zoladex plus Flutamide in the treatment of advanced prostate cancer. Eur. Urol. (Suppl. 3 ) . 18,28 29.
Merrick, M. V., Ding, C. L., Chisholm, G . D. et al. (1985). Prognostic significance of alkaline and acid phosphatase and skeletal scintigraphy in carcinoma of the prostate. Br. J . Urol.,
Merrick, M. V. and Merrick, J . M. (1985). Observation on the natural history of Paget’s disease. Clin. Radiol., 30, 169-174.
O’Donoghue, E. P. N., Constable, A. R., Sherwood, T. et d. (1978). Plasma phosphatases in carcinoma of the prostate. Br. J. Urol., 50, 172-177.
Rasmussen, F. (1989). Treatment of advanced prostate cancer. Horm. Res. (Suppl. 1 ) . 32,47-49.
Robinson, M. R. G. (1990). Reasons against total androgen suppression. In EORTC Genitourinary Group Monograph 8 : Treatment of Prostatic Cancer. Facts and Controversies. Pp. 117-124. New York: Wiley-Liss.
Rose, C. and Mouridsen, H. T. (1989). Endocrine management of advanced prostatic cancer. Horm. Res. (Suppl. I ) , 32, 189- 197.
Schroeder, F. H. (1991). Hormonal manipulation of prostatic cancer. Too soon for total androgen blockade? Br. Med. J . , 303,1489.
The Canadian Anandron Study Group (1990). Total androgen ablation in the treatment of metastatic prostatic cancer. Semin. Urol., VIII, 159-165.
Turkes, A. O., Peeling, W. B., Wilson, D. W. et d. (1988). Evaluation of different endocrine approaches in the treatment of prostatic carcinoma. In New Developments in Bioscience, ed. Klosterhalfen, H. Volume 4, pp. 75-86.
Tyrrell,C. J.,Altwein, J. E.,Klippel, F.etal. (1991). A multicenter randomised trial comparing the luttinizing hormone-releasing hormone analogue goserelin acetate alone and with Flutamide in the treatment of advanced prostate cancer. J . Urol., 146,
Whitmore, W. F. (1973). The natural history of prostatic cancer.
57,7 15-720.
1321-1 326.
Cancer, 32, 11041 112.
The Authors A. Rana, MS, FRCS (Glas), FRCS(I), DUrol (Lond), Registrar,
G. D. Chisholm, CBE, ChM, PPRCSE, FRCS, Professor,
S. Christodoulou, MD, Honorary Registrar, University Depart-
Margaret A. McIntyre, FRCPath, Consultant Histopathologist. R. A. Elton, PhD, Senior Lecturer, Medical Statistics Unit,
University Department of Surgery/Urology.
University Department of Surgery/Urology.
ment of Surgery/Urology.
University of Edinburgh.
Requests for reprints to: A . Rana, University Department of Surgery/Urology Western General Hospital, Crewe Road South, Edinburgh EH4 2XU. Kozlowski, J. M, Ellis, W. J. and Grayhack, J. T. ( 1 9 9 1 ) .






![Prostate adenocarcinoma with negative O ...jrms.mui.ac.ir/files/journals/1/articles/9479/... · of prostatic cancer, has been rarely reported.[3,4] We report a case of prostate cancer](https://img.pdfslide.net/doc/110x75/5f26016cbea40f5eaa0b49c8/prostate-adenocarcinoma-with-negative-o-jrmsmuiacirfilesjournals1articles9479.jpg)

![RESEARCH ARTICLE - Prostate Cancer Foundation of … · Electronic Search Strategy (. com) Query run on 22nd May, 2014 (“Prostate cancer”[All Fields] OR “Prostatic neoplasms”[MeSH](https://img.pdfslide.net/doc/110x75/5ba1148309d3f2b66a8b9ec2/research-article-prostate-cancer-foundation-of-electronic-search-strategy.jpg)