Embed Size (px)
Citation preview
Autism and
Occupational Therapy –
Optimizing Function
Occupational Therapy Enhancing function in
activities of daily living:– dressing, bathing, toileting,
eating Promoting participation in
play and social activities. Optimizing sensory
processing and motor development.
Facilitating self-regulation. Ensuring safety.
Law M, 2005
Environments Home: increasing
independence through structuring tasks.
Daycare and preschool: self-regulation for transitions; pre-literacy skill building.
School: paying attention for learning, printing.
Clinic: improve sensory and motor development.
Luthman MR, 2010 and Marr D, 2010

Self Care: Activities of Daily Living Dressing: sequencing,
over/under dressing, taking clothes off.
Bathing: hygiene, refusal, fear of water.
Toileting: bowel or bladder incontinence.
Eating: choking, sensory sensitivities, fine motor skills.
Cox DJ (2012)
Productivity: Play and School Home: getting ready for
preschool, cleaning up toys. Daycare/Preschool:
following instructions, participating in activities.
School: starting, maintaining, and completing tasks, paying attention.
Leisure: Fun, Fitness and Friends
Requires creativity and imagination
Play is a critical factor in development.
Play teaches children physical, social and language skills, as well as an understanding of others emotions.
Rosenbaum, P (2013, 2012) Potvin, MC
Motor Development 50-75% of children with Autism experience substantial motor
coordination deficits across a wide range of behaviours.
Fournier et al. 2010, J. Autism Dev. Disorders
Treatment of identified sensory-motor delays assessed by OT’s or PT’s.
Cox DJ, 2012
Specific motor skill research includes delays in both fine and gross motor skills:– Clumsiness– Gait disturbance, arm movements– Lack of hand dominance– Motor stereotypies– Poor balance, postural stability deficits– Toe walking
Gross Motor Control
• Balance: active and standing• Ball skills: catch, throw, aim,
bounce, hit• Postural stability: pelvic and
shoulder girdle• Gait: walk, run, jump
Kimberley 2010
• Developmentally, gross motor development precedes fine motor control
Fine Motor Control The ability to control the
trunk, arms, hands, mouth, fingers and eyes to accomplish a task:
dress, eat, build, paint, draw, cut
printing legibility and output speed, reading
computer keyboarding
Social
Talk and listen. Appropriate topics. Initiate communication or
play with other children. Allowing turn taking. Participating in group play.
Greenspan S, 2006
Self RegulationBeing in control of energy states
Soothes self when upset Waits turn Transitions from task to task Listens Accepts challenges Pays attention and learns
Greenspan 2006, Russo 2010
Sensory Processing Incidence - Autism
94.4% of adults with ASD reported extreme levels of sensory processing on at least one sensory quadrant of the Adult/Adolescent Sensory Profile, Crane et al 2009.
69% of children with Autism demonstrated sensory symptoms on the Sensory Experiences Questionnaire, Baranek et al 2006, J. Child Psychology and Psychiatry.
95% of children with Autism demonstrated some degree of sensory processing dysfunction on the Short Sensory Profile Total Score, with the greatest differences reported on the Underresponsive/Seeks Sensation, Auditory Filtering and Tactile Sensitivity sections, Tomchek & Dunn, 2007.
New research supports decades of clinical and anecdotal evidence that individuals with ASD process sensory information such as sound, touch and vision differently than typically developing children, Russo et al 2010.
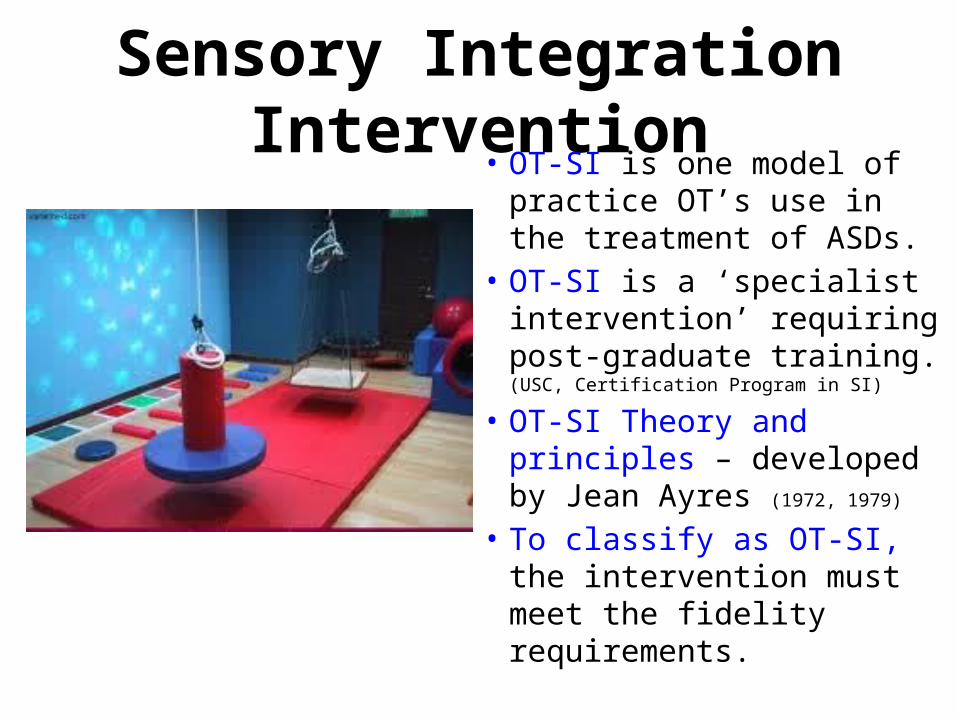
Sensory Integration Intervention• OT-SI is one model of
practice OT’s use in the treatment of ASDs.
• OT-SI is a ‘specialist intervention’ requiring post-graduate training. (USC, Certification Program in SI)
• OT-SI Theory and principles – developed by Jean Ayres (1972, 1979)
• To classify as OT-SI, the intervention must meet the fidelity requirements.
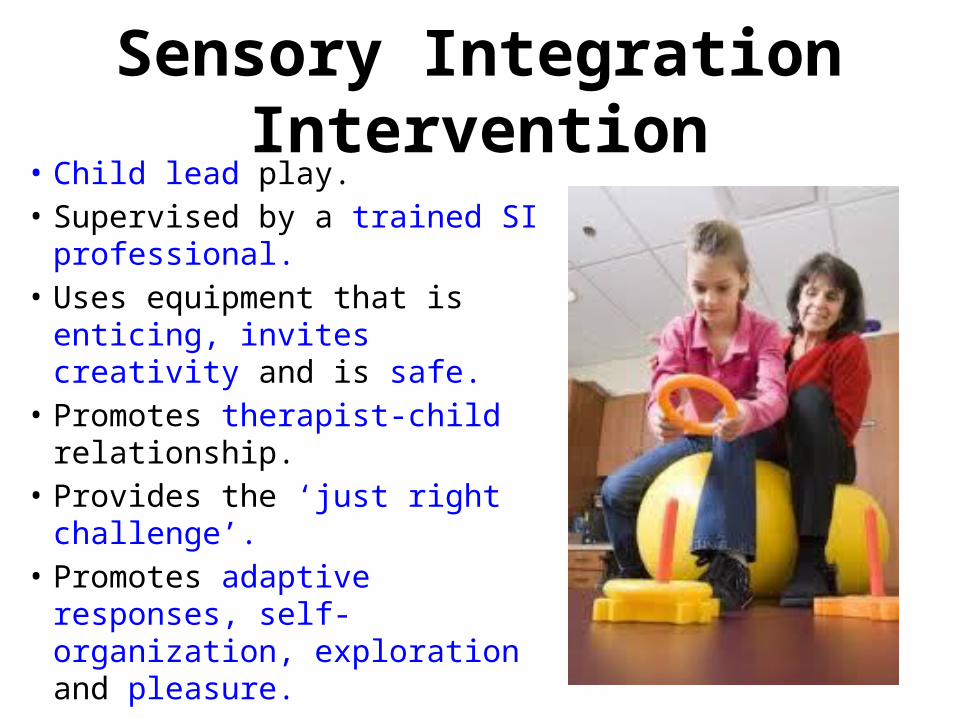
Sensory Integration Intervention• Child lead play.• Supervised by a trained SI
professional.• Uses equipment that is enticing,
invites creativity and is safe.• Promotes therapist-child
relationship.• Provides the ‘just right
challenge’.• Promotes adaptive responses,
self-organization, exploration and pleasure.
Sensory Integration IS NOT:• applying deep pressure to a child.• wearing a weighted vest while seated in class.• using a therapy cushion during circle time Umeda, 2012.
• wearing headphones to block ambient noise.• sitting in a quiet corner to recover after a meltdown.• chewing gum to calm and improve focus.• taking a walk in the hallway.
These are sensory strategies based on SI theory to support improved self-regulation. Research on effectiveness of sensory strategies is mixed and should be considered on a case by case basis by the OT.
Evidence Based Research• OT-SI effectiveness questioned
from both inside and outside the profession. Shaw 2002, Pollack 2007
• Fidelity study: Parham 2007 (AJOT)
• OT-SI Research started afresh in 2007 and began to focus on ASDs as well as other diagnoses.
• New research studies since 2007, which meet fidelity requirements for OT-SI, show promise. Pollack 2007
Current OT-SI Research
• Research lags behind clinical evidence.
• Starts with case reports, group studies then retrospective studies.
• Miller, LJ (2007)• May-Benson et al (2010)• Pfeiffer,B. A et al (2011) • Schaaf, RC et al (2012)
POTC – Autism Group
Includes: Diane Graham, Jane Remocker, Cris
Rowan, Jenny Sexton, Les Smith, and Susan Stacey
and
Giovanna Boniface, CAOT BC
Thank You!!!