Embed Size (px)
Citation preview

Letters to the Editors
Sporadic Geniospasm (Chin Trembling):Report of a Case
Geniospasm (chin trembling/quivering) is a rare movementdisorder characterized by recurrent episodes of involuntarymovements of the chin.1 The cases described in the literaturehave included approximately 25 families with autosomal dom-inant geniospasm.2 We present here the first case of typicalgeniospasm but without evidence of family history.
We evaluated a 15-year-old right-handed girl with involun-tary, intermittent movements of the mentalis muscle datingsince infancy and first noted while she was sucking on herbottle. They occurred at random and were not triggered by anyparticular activity, including chewing, swallowing, talking, oryawning. Movements were increased by emotional stress andtemperature changes. The condition affected the patient’s qual-ity of life because of social embarrassment, eating, and drink-ing difficulties. The patient did not report any additional symp-toms during her episodes. Results of computed tomography,magnetic resonance imaging, and electroencephalogram inves-tigations were normal. Before her evaluation at our clinic, shehad already received botulinum toxin A injections to the men-talis muscle (20 units/session) on two occasions, both treat-ments causing an 80% improvement in symptoms benefit last-ing over 4 months.
She had a normal development and was an average student.Two older sisters (ages 31 and 26) were examined and had nomovement disorder. We interviewed family members who af-firmed that there was no history of a similar condition affectingrelatives in at least two prior generations.
The patient’s general neurological examination was unre-markable. Small amplitude bilateral involuntary contractions ofthe mentalis muscle occurred intermittently during theexamination.
Since her first evaluation, the patient has had six additionalsessions of botulinum toxin type A injections, in doses of up to25 units in each mentalis muscle with excellent response (95%subjective improvement) at a mean interdose interval of 9months.
We report the first sporadic case of otherwise typical genio-spasm. Until now, geniospasm had only been reported withinthe context of a positive family history. Hereditary geniospasmoccurs in infancy or in early life, and the episodes tend todecrease in frequency with advancing age.3 Episodes may lastfrom seconds to several hours, and they may be precipitated bystress, concentration, and emotion.4 Geniospasm is a neurolog-ically benign movement disorder; but patients may find itsocially disabling.5 Regular botulinum toxin injections to thementalis muscle have been effective in the treatment of hered-
itary geniospasm5 The disorder has been linked to a chromo-some 9q13-q21 locus6 but linkage has not been consistentlyfound by all investigators.4 We did not test our current casebecause the patient was lost to follow-up.
Possible explanations for the lack of family history in ourpatient include reduced penetrance and the possibility of ourpatient having a new mutation. New mutations have beenreported to account for � 1% of cases in other dominantlyinherited diseases such as Huntington’s disease.7
Spiridon Papapetropoulos, MD, PhDCarlos Singer, MD
University of MiamiMiller School of Medicine
Miami, Florida
References
1. Grossman BJ. Trembling of the chin; an inheritable dominant char-acter. Pediatrics 1957;19:453–455.
2. Diaz S, Scorticati MC, Micheli F. Hereditary chin tremor/myoclo-nus: a report from Latin America. Mov Disord 1999;14:180–182.
3. Soland VL, Bhatia KP, Sheean GL, Marsden CD. Hereditary ge-niospasm: two new families. Mov Disord 1996;11:744–746.
4. Grimes DA, Han F, Bulman D, Nicolson ML, Suchowersky O.Hereditary chin trembling: a new family with exclusion of thechromosome 9q13–q21 Locus. Mov Disord 2002;17:1390–1392.
5. Gordon K, Cadera W, Hinton G. Successful treatment of hereditarytrembling chin with botulinum toxin. J Child Neurol 1993;8:154–156.
6. Jarman PR, Wood NW, Davis MT, et al. Hereditary geniospasm:linkage to chromosome 9q13–q21 and evidence for genetic heter-ogeneity. Am J Hum Genet 1997;61:928–933.
7. Durr A, Dode C, Hahn V, et al. Diagnosis of “sporadic” Hunting-ton’s disease. J Neurol Sci 1995;129:51–55.
Autoimmune Thyroid Disease and SegmentalMyoclonus
We describe a patient with Graves’ disease and segmentalmyoclonus. There was a correlation of the myoclonus with boththe severity of the hyperthyroidism and the titer of antithyroidantibodies.
A 38-year-old Caucasian man developed postural-actiontremors of both upper limbs about 5 years ago. Within the pastyear, the tremors worsened, and he developed heat intolerance,tachycardia, increased appetite, and weight loss. Although thethyroid gland was not appreciably enlarged, he was diagnosedas having Graves’ disease on the basis of increased free tri-
Published online 28 November 2006 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.21239
Published online 10 January 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.21279
Movement DisordersVol. 22, No. 3, 2007, pp. 434–443© 2006 Movement Disorder Society
434

iodothyronine (T3) and free thyroxin (T4) and suppressedthyroid-stimulating hormone (TSH) serum concentrations. Heunderwent treatment with radioactive iodine (RAI) and diazole.The tachycardia was treated with propranolol.
Several days after the RAI treatment, he developed irreg-ular clonic movements that affected the trunk, especially therectus abdominus, oblique abdominal muscles, and lumbarparaspinal muscles; the diaphragm and thoracic and limbmuscles were not involved. The movements seemed morevigorous when he was active; they continued, but were notas vigorous, during sleep. He was fatigued and unable towork because of the movements. Contractions were briefand bilaterally symmetrical; he could suppress them brieflyby concentration. Apart from mild postural-action tremor,worse on the right, the neurological and general physicalexaminations were normal.
Electromyography was normal apart from the bilaterally syn-chronous twitches, maximal in the rectus abdominus, but affectingthe abdominal and lower paraspinal muscles as well. Magneticresonance imaging of the brain and spinal cord were unremark-able; cerebrospinal fluid showed no pleocytosis, normal cellcounts, and was negative for oligoclonal banding, an index ofintrathecal antibody production. The electroencephalogram, per-formed during myoclonic movements, was normal. Antithyro-globulin antibodies were elevated at 132 (normal � 35) IU/ml;antithyroglobulin antibodies were increased at 757 (normal � 40)IU/ml. Serum antiglutamic acid decarboxylase-65 (GAD) antibod-ies were negative. There was no evidence of underlying malig-nancy. Antinuclear antibodies were moderately positive with ahomogeneous pattern but anti–double-stranded DNA was nega-tive/normal; C3, C4, and CH-50 were normal and rheumatoidfactor, anti-ENA, anti-SM, RNP, SSA/RO, SCL-70, JO-1, p-ANCA, and c-ANCA and anticentromere antibodies were nega-tive. Serum IgG, IgA, and IgM were normal.
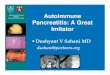
The truncal myoclonus showed a rough correlation with bothelevated free T4 and T3 values as well as titers of antithyroidantibodies (Table 1). Treatment with clonazepam 2.0 mg/dayand valproic acid 1,500 mg/day (maximally tolerated doses)and prednisone 40 mg/day had no apparent effect. The myo-clonus spontaneously decreased 2 months later to be far lessfrequently bothersome. Clonazapam, valproate, and prednisonewere tapered off and there was no increase in myoclonus
Because of the hyperthyroid state, the patient was diagnosedas having Graves’ disease, although the presence of antithyroidantibodies raised the possibility of an overlap with Hashimoto’sthyroiditis.1 The latter has been associated with an encephalop-athy, an autoimmune, steroid-responsive encephalopathy, often
accompanied by epileptic seizures.2 In our case, there was noevidence of brain (cerebral or brain stem) dysfunction, and it ismore likely that the movements related to a problem in thelower thoracic and upper lumbar segments of the spinal cord. Itis interesting that they could be partially suppressed by volition(descending inhibitory pathways). That they were so consistentand present in sleep essentially rules out psychogenic andtic-like phenomena; they did not have the more persistentcontractions and widespread feature of stiff-person syndromeand anti-GAD antibodies were negative. We have encounteredone case in which stiff-person syndrome occurred in associa-tion with Graves’ disease, hence the relevance of testing forthis.3
A single case of spasmodic truncal flexion in associationwith Graves’ disease was recently reported, in which the flex-ion movements were jerky and partially suppressible by voli-tion.4 Since the movements abated with vigorous treatment ofthe hyperthyroidism, they were attributed to thyrotoxicosis. Weobserved the same general phenomenon, but there was also acorrelation with titers of antithyroid antibodies. It seems morelikely that the myoclonus is related to an antibody-mediatedeffect on segmental spinal cord function, as segmental myo-clonus is not a feature of a moderate hyperthyroid state itself.The elevations in thyroid hormones and antithyroid antibodiesmay be surrogate markers for fluctuations in the autoimmunestate, with unrecognized serum antibodies directed toward in-hibitory neurons in the spinal cord. We have no evidence thatthe myoclonus was related to intrinsic nervous system disease(negative MRI scans of spinal cord and brain and normal CSFwith negative oligoclonal banding). It therefore seems morelikely that the problem is a systemic one. Perhaps a trial ofplasmapheresis or intravenous immunoglobulin could be con-sidered in future attacks/cases.
Bryan YoungDepartment of Clinical Neurological Sciences
Faculty of Medicine and DentistryUniversity of Western Ontario
London, ON, Canada
Albert DriedgerJohn Wojcik
Department of MedicineFaculty of Medicine and Dentistry
University of Western OntarioLondon, Ontario, Canada
TABLE 1. Myoclonus and test results
Date Free T4, Free T3 Antibodies Myoclonus
18 May 2005 Antithyroglobulin 1151 ����7 June 2005 Free T4 15, free T3 4.0 pmol/L ��21 June 2005 Free T4 20.9, free T3 4.7 Anti-TPO 132, Antithyroglobulin 757 ����12 July 2005 Free T4 6, free T3 2.4 ��28 July 2005 Free T4 7, free T3 2.8 ��3 August 2005 Anti-TPO 73, antithyroglobulin 328 �19 August 2005 Free T4 17; free T3 5.724 August 2005 Free T4 29.2, free T3 7.7 ���9 September 2005 �
LETTERS TO THE EDITORS 435
Movement Disorders, Vol. 22, No. 3, 2007

References
1. Weetman AP. Autoimmune thyroid disease. Autoimmunity 2004;37:337–340.
2. Fatourechi V. Hashimoto’s encephalopathy: myth or reality? anendocrinologist’s perspective. Best Pract Clin Endocrinol Metab2005;19:53–66.
3. Morrison T, Young B. Progressive encephalomyelitis with rigid-ity (PREM) in a young woman with GAD-65 antibodies andother autoimmune dysfunction. Can J Neurol Sci 2003;30(Suppl.2):S54.
4. Loh LM, Hum AYM, Teoh HL, Lim ECH. Graves’ disease asso-ciated with spasmodic truncal flexion. Parkinsonism Relat Disord2005;11:117–119.
Case of Spinocerebellar Ataxia Type 17(SCA17) Associated with only 41 Repeats of
the TATA-Binding Protein (TBP) Gene
Spinocerebellar ataxia (SCA17) is an autosomal dominant neu-rodegenerative disorder characterized by progressive limb andgait ataxia, dysarthria, motor, cognitive, and psychiatric abnor-malities.1 It is caused by expansion of the CAG/CAA repeat inthe Tata binding protein (TBP) gene.2 The currently definedrepeats ranges are as follows: normal, �42; reduced pen-etrance, 43 to 48; full penetrance, �49 repeats.3 The higher thenumber of repeats, the younger the onset age. Minimum re-ported repeats associated with SCA17 are 43 with onset at age52; maximum is 66 with onset at age 3 years.3,4 Almost allnormal individuals have �39 repeats, with distribution skewedtoward a smaller number.3 We hereby describe a patient withthe SCA17 phenotype but who has only 41 repeats, thus pos-sibly expanding the definition of the pathologic genotype as-sociated with spinocerebellar ataxia type 17.
A 75-year-old man with progressive dysarthria, dysphagia,and limb and gait ataxia developed gait problems with falls atage 50. Since age 73, he required a wheelchair and feedingtube. He had limited knowledge of his father and has nobiological siblings. No known relatives had neurological prob-lems. Neurological examination demonstrated mild cognitiveimpairment, dysarthric speech, limb ataxia, profound gaitataxia, and brisk reflexes. He had no weakness or sensorydeficits. Brain magnetic resonance imaging revealed cerebellaratrophy. Motor and sensory nerve conduction studies werenormal. The Athena Complete Ataxia Evaluation revealed 41CAG/CAA repeats in the TBP gene. No other causes could bedetermined by further investigation. We consider this a case ofinterest because of the patient’s SCA17 phenotype and TBPallele containing only 41 CAA/CAG repeats. We wonder if thiscase suggests that the range of normal genotype values needs tobe expanded, suggesting a possible expansion in definition ofnormal genotype values.
Ashish Nanda, MDSarah A. Jackson, MS
John D. Schwankhaus, MD
W. Steven Metzer, MDUniversity of Arkansas for Medical Sciences
Little Rock, ArkansasCentral Arkansas Veterans Healthcare System
Little Rock, Arkansas
References
1. Rolfs A, Koeppen A, Bauer I, et al. Clinical features and neuropa-thology of autosomal dominant spinocerebellar ataxia (SCA17).Ann Neurol 2003;54:367–375.
2. Nakamura K, Jeong S, Uchihara T, et al. SCA17, a novel autosomaldominant cerebellar ataxia caused by an expanded polyglutamine inTATA binding protein. Hum Mol Genet 2001;10:1441–1448.
3. Silveira I, Miranda C, Guimaraes L, et al. Trinucleotide repeats in202 families with Ataxia. Arch Neurol 2002;59:623–629.
4. Maltecca F, Filla A, Castaldo I, et al. Intergenerational instability andmarked anticipation in SCA-17. Neurology 2003;61:1441–1443.
Predictors of Weight Loss in Parkinson’sDisease: Is Weight Loss the Chicken
or the Egg?
In a recent research article, Uc and colleagues1 proposed thatworsening of Parkinson’s disease (PD) symptoms was a pre-dictor of weight loss. They studied 49 PD patients 7.2 � 0.5years after a first visit. On average, their subjects lost 7.7% �0.7% of body weight, and they suggested that worsening ofparkinsonism was the key predictor of weight loss. Age atdiagnosis, emergence of visual hallucinations, and dementiawere also noted as possible factors. We would like to suggestan alternative interpretation: weight loss could be an importantpredictor of worsening of parkinsonism. This suggestion arisesfrom several recent studies in which increased plasma concen-tration of organochlorine pollutants were observed followingweight loss.2,3
Organochlorine compounds regroup polychlorinated biphe-nyls (PCBs) and organochlorine pesticides (DDT, DDE). Theuse of organochlorine compounds was forbidden in NorthAmerica and Europe in the 1970s because they represent a highrisk for health and environment. A degradation resistance anda food chain accumulation of the organochlorine compoundsresult from their lipophilic property and resultant storage in fatof living organisms.4,5 There are now several studies showingthat plasma organochlorine and pesticide concentrations in-crease following weight loss, whether the weight loss resultsfrom a hypocaloric restriction program or surgery.2,3 We re-cently tested 14 obese subjects (30 � BMI � 39.9 kg/m2) and11 morbidly obese subjects (BMI � 40 kg/m2) for their totalconcentration of 25 compounds at steady state and after weightloss. Six control subjects (BMI � 25 kg/m2) also were testedtwice (6- to 8-month interval). Weight loss was obtained inobese individuals by a hypocaloric diet program until resistanceto loose fat and in morbidly obese individuals by bariatricsurgery. On average, the obese participants lost 12.1% of bodyweight. Three months after the surgery, morbidly obese partic-
Published online 5 December 2006 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.21275
Published online 10 January 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.21203
436 LETTERS TO THE EDITOR
Movement Disorders, Vol. 22, No. 3, 2007