Embed Size (px)
Citation preview

Arch. Dis. Childh., 1969, 44, 406.
Autonomic Nerves in Rectum and Colon inHirschsprung's Disease
A Cholinesterase and Catecholamine Histochemical Study*
J. R. GARRETT, E. R. HOWARD, and H. H. NIXONFrom King's College Hospital and The Hospitalfor Sick Children, London
The autonomic nervous system innervatesnormal bowel in a complicated manner. Studyof these nerves has been facilitated by histo-chemical techniques which enable separate identi-fication of adrenergic- and acetylcholinesterase(AChE)-containing nerves. The latter are usuallyconsidered to be cholinergic, and while theirpresence in the muscle layers of the bowel wall iswell known, little attention has been paid to theirdetailed distribution. It has usually been con-sidered that the adrenergic nerves are also distri-buted directly to the muscle layers, but recentstudies by Norberg (1964), Jacobowitz (1965),and Baumgarten (1967) have shown that thesenerves are mainly associated with the myentericganglia. The ganglion cells themselves do notcontain catecholamines, but possess variableamounts of AChE-activity (Koelle, 1955; Caunaet al., 1961; Gunn, 1968).
In a classical case of Hirschsprung's disease, anundilated rectum is found to be devoid of ganglioncells on routine histology, though large nervetrunks are present. More proximal bowel appearsnormal. Recent studies of the morphology ofnerves in aganglionic bowel from Hirschsprung'sdisease have been reported by Smith (1967)using silver staining, and by Ehrenpreis, Nor-berg, and Wirsen (1968) using catecholaminefluorescence. These workers suggested that themuscle layers themselves were virtually denervated,and that unopposed muscle activity was responsiblefor the contracted appearance of affected bowel.Meier-Ruge (1968), on the other hand, as a resultof cholinesterase studies, suggested that thecontraction was due to an increase in muscular
Received November 5, 1968.* This work was supported by a grant from the Medical Research
Council to E. R. H. during a research appointment at The Hospitalfor Sick Children, London.
innervation, and implied that this always accom-panied aganglionosis.
It is difficult to understand, from either of theseconflicting ideas, why two patients with similarlengths of aganglionic bowel sometimes presentin different ways. For example, one patientmight present with a severe intestinal obstructionin the neonatal period, while another might beseen much later in life with a history of constipation.Furthermore, if muscular denervation is consideredto be the mechanism responsible for the undilateddistal bowel, a difficulty is raised by the conditionknown as Chagas' disease, where the ganglion cellsof the myenteric plexus are destroyed by theorganism Trypanosonia cruizi, yet the resultingaperistaltic bowel shows dilatation, not contraction.
Histochemical studies have shown that thelarger nerve bundles in the intermuscular zone ofaganglionic segments from cases of Hirschsprung'sdisease are AChF-positive (Kamijo, Hiatt, andKoelle, 1953; Adams, Marples, and Trounce,1960; Niemi, Kouvalainen, and Hjelt, 1961), andthat there is also an increase of AChE-positivenerves in the circular muscle (Niemi et al., 1961;Meier-Ruge, 1968). A preliminary report byBennett, Garrett, and Howard (1968) showed thatthe normal arrangement of adrenergic nervesaround myenteric ganglia was absent in the affectedsegment of Hirschsprung's disease, but that therewas a tendency for the numbers of adrenergicnerves in the muscle layers themselves to beincreased.The aim of the present investigation was to
examine the distribution of the muscular nervesboth in normal large bowel of children, and indifferent areas of gut resected from cases ofHirschsprung's disease. The results have beenassessed in conjunction with the clinical presenta-tion, in order to ascertain whether the pattern of
406
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Autonomic Nerves in Rectum and Colon in Hirschsprung's Diseasedistribution of the nerves helps to explain theclinical variability of the disease.
Materials and MethodsGut resected because of Hirschsprung's disease
from 19 children aged from 3 months to 2 years 8months has been investigated. In addition, 4 segmentsof normal recto-sigmoid, removed at operation forother reasons from children aged from 5 months to4 years, have served as controls.
Several small full-thickness blocks of gut were cut ina longitudinal direction from each of a number ofdifferent levels of resected bowel. The most distalblocks always came from the lower end of the rectum,but the levels of the other blocks depended on thelength of bowel resected. Adjacent blocks from eachlevel were placed cut-surface downwards on thincarding, to aid orientation and to minimize buckling.They were then immediately immersed in either ahexane/solid CO2 mixture for rapid freezing, or informol-phosphate-sucrose at 4 'C. for 4 hours. Theformalin-fixed blocks were washed in phosphate-sucrose overnight and then rapidly frozen, as above.
Catecholamine fluorescence studies. Tissuesfrom 18 cases of Hirschsprung's disease and the 4controls were used. Adrenergic nerves were studiedin 8 ,u sections from freeze-dried blocks which hadbeen heated with formaldehyde vapour (after Eranko,1967). The catecholamine fluorescence, thereby in-duced, was examined as described by Bennett et al. (1968)in a preliminary communication concerning 5 of thepresent cases of Hirschsprung's disease and 2 of thecontrols.
Cholinesterase studies. Tissues from 15 of thecases of Hirschsprung's disease and 3 of the controlswere investigated.AChE activity was studied by the Gomori (1952)
modification of the Koelle and Friedenwald (1949)thiocholine technique. Acetylthiocholine iodide wasused as substrate and iso-OMPA (tetraisopropylpyro-phosphoramide) 3 x 104 M was used to inhibit non-specific cholinesterase activity (see Garrett 1966,1967). Cryostat sections, cut at 10-12 ,t from unfixedfrozen blocks and also frozen-fixed blocks, were testedby the histochemical procedure over a range of in-cubation times, up to 24 hours. It was found that thebest results were obtained by using unfixed blocks,mounting the sections on gelatine-faced slides, andfixing with formol-sucrose for 10 minutes before thehistochemical procedure (as in Garrett, 1966). Thiscontrasts with adult human salivary tissue, in whichpre-fixed blocks gave the best results (Garrett, 1967).Some sections, adjacent to those used in both the
above methods, were stained by haematoxylin andeosin for conventional appearances.
ResultsThe results will be restricted to observations on
nerves in the circular muscle, the intermuscularzone, and the longitudinal muscle of the bowel.In light microscopical representations of nervesmany variables influence assessment. Not allnerves are always made visible, separate nerves inthe same field may sometimes represent recur-rences of the same nerve, and orientation of theblock influences appearances. Furthermore, eachindividual fibre seen is usually an aggregaterepresentation of a Schwann-axon bundle ratherthan a single axon (see Garrett, 1966), and thepresence of such gives no indication of the numberof possible neuro-effector sites that would berecognizable by electron microscopy. No attempthas therefore been made to give an absolute assess-ment of the numbers of nerves in the tissues.Only large differences in the numbers of nervesare detectable, and therefore only such differenceswill be mentioned.
Acetylcholinesterase activityControls (see Fig. 1A). Ganglia and nerves
were stained to advantage. All sections containedganglia in the intermuscular zone, but the ganglionicmasses were variable in size, structure, and AChEstaining, and it was not possible to interpret theappearances in precise terms. This is not alto-gether surprising when one considers the immenselycomplex structural organization of the myentericganglia as revealed by electron microscopy(Richardson, 1958). In the present investigationthe ganglion cells also varied both in size andAChE staining. Many cells showed moderaterather than strong staining, and some cells appearedto be negative. Much of the tissue between andaround the cellular parts showed strong activity.This tissuc was probably mainly axonal, butseldom showed fibre-like appearances. Nervetrunks, rich in AChE activity, were sometimesfound passing through the longitudinal musclelayer to the ganglia; others were sometimes seenbetween ganglia.
In the circular muscle, moderate numbers ofthin AChE-positive fibres were present amongthe smooth muscle cells. They radiated from theintermuscular zone to the mucosal layer, and wereseen occasionally to connect with ganglia. In thelongitudinal muscle there were somewhat fewernerves which radiated down the long axis of thislayer. The numbers of muscular nerves appearedto be relatively constant throughout the length ofbowel from any one individual, but there wereslight differences between one individual andanother.
Adjacent to the mucosal surface of the circular
407
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

408 Garrett, Howard, and Nixon
~~0 ...,,%,-..i
-
/4
r*'% ' ; i ^ 1K¢;% >\
A . 4'. . . ..1; . . , >I ~~ -r ¾Z
%
A. a; ;:~~~~~~~~~~~~~~~0 , , U t:a a
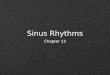
FIG. 1.-Normal rectum (circular muscle layer in the bottom half of each picture. (A) Stainedfor AChE activity (4-hourcounterstained with haemalum), showing dark AChE-positive nerves in the longitudinal muscle and circular muscle. Theganglia between these two layers exhibit variable staining. ( x 88.) (B) Formalin-inducedfluorescence showingfluorescentadrenergic nerves arranged in a complex manner within and between the myenteric ganglia. Few nerves are present in
the muscle layers. ( x 88.)
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Autonomic Nerves in Rectum and Colon in Hirschsprung's Diseasemuscle a number of small ganglia were present,and these ganglia frequently showed less AChEactivity than in the intermuscular zone. Some ofthe cells were AChE-negative, and around such cellsAChE-positive nerves were often evident.The above findings have also been supported by
studying AChE activity in the rectum and colonfrom 3 necropsy specimens of infants aged 18months to 41 years. Pictorially the results wereless pleasing than in the surgical material; neverthe-less, it was evident that the numbers of nervesand their pattern of distribution were relativelyconstant throughout the same length of bowel.
Hirschsprung's disease(a) Proximal tissue (see Fig. 5A and B). It
has not been possible in every case to examinesatisfactorily tissues adjacent to the proximalcut edge of the resected specimens, becauseoperative procedures have tended to damage them.Furthermore, whenever a colostomy has previouslybeen established only tissue distal to the colostomyhas been available for study. In 10 cases, gang-lionic tissue was seen in the proximal parts of theresected specimens, but in all of these there werefewer AChE-positive muscular nerves than normalin the most distal parts of this ganglionic tissue.In fact, in only 3 cases were normal numbers ofnerves seen in the most proximal parts of the gang-lionic tissue. Sometimes the most distal gang-lionic tissue showed only small infrequent gangliain the intermuscular zone, and when this occurredthere tended to be some overlap with large trunks,more characteristic of the aganglionic bowel.One case, in which the whole of the colon wasaffected by the Hirschsprung's process, showed aprogressive loss of ganglia and muscular nerves inthe lower end of the ileum.Whenever ganglia were found, they showed a
similar variable AChE staining to the normalganglia.,
(b) Distal tissue (see Fig. 2A, 3A, 4A, 5C and Dand Table). No ganglia were found in the mostdistal tissue from the 15 cases examined, butAChE-positive nerve trunks were present in theintermuscular zone. The length of bowel that wasaganglionic varied from case to case.
In the most distal aganglionic tissue there werelarge differences in the numbers of nerves in thecircular muscle layer; in 7 cases there were manymore nerves than normal, and in 5 the number ofnerves was at the upper limit of normal. In all ofthese 12 cases the nerves tended to be more AChE-positive than normal, and also somewhat thicker,probably indicating that there were more axons in the
9A
Schwann-axon bundles (see Garrett, 1966). Thesenerves often stained more strongly and morequickly than the large trunks in the intermuscularzone. In the 3 remaining cases fewer nerves thannormal were found in the circular muscle. Asone ascended the bowel there was always somedecrease in the numbers of nerves in the circularmuscle before reaching the ganglionic tissue, butthe amount of this decrease and the length overwhich it occurred varied.The numbers of AChE-positive nerves in the
longitudinal muscle differed less from normalcontrols.Sunmary of findings in Hirschsprung's disease.
From the foregoing study a distinct pattern of thedistribution of the nerves emerges (see Fig. 5).Passing along the bowel in a caudad direction,gradual changes occur which may be divided into4 regions.
(i) Normal ganglionic bowel, with normal numbersof nerves in the muscle layers (seen, however in,only 3 cases).
(ii) Distal ganglionic bowel, in which ganglia arepresent, sometimes apparently reduced in numberand size. In the circular muscle nerves are in-variably scanty.
(iii) Proximal aganglionic bowel, in which nervetrunks but no ganglia are seen in the intermuscularzone. In the circular muscle there are usuallymore nerves than in (ii) but less than in normalcontrols.
(iv) Distal aganglionic bowel, at which level morenerve trunks are seen in the intermuscular zone.In the circular muscle more nerves are presentthan in (iii), and are often more plentiful, morestrongly AChE-positive, and thicker than in normalcontrols.
Sometimes regions (;i) and (iii) overlap andgreat differences may occur in the lengths of eachregion and the amount of change within them.
Catecholamine fluorescenceControls (Fig. 1B). As described previously
(Bennett et al., 1968), fluorescent adrenergicnerves were found principally in association withthe myenteric ganglia, and few fluorescent nerveswere present in the muscle layers proper. Thearrangement of the fluorescent nerves was complexand irregular within the ganglionic masses andnot always precise. These nerves were usuallymost concentrated towards the periphery of theganglia, some appearing to be associated with theganglion cells which were non-fluorescent. Lessconspicuous fluorescence was seen in associationwith the small ganglia on the mucosal surface of
409
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

I
*s i 'I ,,i' j | t
.4 1
4 ',I v
44 1 E
4 f,,1
I w.
i.) 4 t
i x, ,r lF
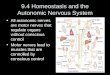
FIG. 2.-Distal aganglionic bowel from 2 cases of Hirschsprung's disease (circular muscle layer in the right half of eachpicture). (A) Stained for AChE activity (4 hours counterstained with haemalum), showing absence of ganglia, but apositive nerve trunk is present in the intermuscular zone. A dense arrangement ofstrongly positive nerves is present in thecircular muscle, fewer nerves are present in the longitudinal muscle (graded + + + in the Table). ( x 165.) (B) Formalin-induced fluorescence, showing a dense arrangement of nerves in the circular muscle and to a lesser extent in the longi-tudinal muscle. The larger nerve trunks appear to be mainly non-fluorescent. ( x 83.) (This tissue contained the most
adrenergic nerves; unfortunately, tissue was not available for AChE staining as well.)
#1
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

c-4r I A.4
04;-4 .4b-- -
I -4--. *.1' -r
- -- - - t.t4
- 0 * A- -.
r - S- .-.----- -
>r .7. Kr . -
A - r.
-1-
t._d ., ....
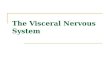
FIG. 3.-Distal aganglionic bowel from a case of Hirschsprung's disease (circular muscle layer in the top half of eachpicture). (A) Stained for AChE activity (4 hours counterstained with haemalum), showing a dense c*rrangement of thick,dark, somewhat overstained nerves in the circular muscle. Some thinner nerves are just becoming evident in the longi-tudinal muscle (graded+++ in the Table). (x 165.) (B) Formalin-induced fluorescence, showing fluorescentadrenergic nerves in the same segment as (A). The nerves are more nunerous in the longitudinal muscle than in the
circular muscle but become morefrequent again in the submucosa. ( x 83.)On
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Garrett, Howard, and Nixon
I~~~~~~~~~~~~~
a0 II
,W.fb'.r{r. rf.r~
_
A
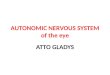
FIG. 4.'-Distal aganglionic bowel from a case of Hirschsprung's disease (circular iuscle layer in the top half of eachpicture), (A) Stainedfor AChE activity (4 hoursfaintly counterstained with haemalum), showing that despite the presenceof a large positive nerve trunk in the intermuscular zone there are very few nerves in the muscle layers (graded ± inthe Table). (x 165.) (B) Formalin-inducedfluorescence, showing that veryfew adrenergic nerves are present. (x 165.)
This case showed no constricted segment on barium enema.
412
¶,*A
I
*.,_#.
'Yrdko*
/O_-
8
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

f
AkRI W1 .' X ,_..
FIG. 5.-Segments of bowel from different levels in the same case of Hirschsprung's disease. All sections have beensomewhat overstained for AChE activity in order to show up the smallest nerves and so help comparisons (counterstainedwith haemalum). (The circular muscle is on the right.) (A) Proximal ganglionic zone (24 hours incubation), showing aganglion and normal numbers of nerves in the muscle layers. ( x 109.) (B) Distal ganglionic zone (24 hours incubation),showing a ganglion but very few nerves in the muscle layers. ( x 109.) (C) Proximal aganglionic zone (24 hoursincubation), showing nerve trunks but few nerves in the muscle layers. (x 109.) (D) Distal aganglionic zone(6 hours incubation), showing nerve trunks and many thickish, very positive, nerves in the circular muscle (graded + +
in the Table). ( x 109.)
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Garrett, Howard, and Nixonthe circular muscle. These ganglion cells were
also non-fluorescent.Normal rectum and colon showed no variations
in the pattern of distribution at different levels.
Hirschsprung's disease(a) Proximal tissue. Ganglia were seen in the
most proximal tissues of the resected specimens in14 out of the 18 cases. The fluorescence associatedwith these ganglia had a similar pattern to thecontrols but was often more diffuse, perhaps as
a consequence of the operative procedure. Suffi-cient ganglionic tissue was removed from 9 of these14 cases to permit examination of both proximaland distal parts. In 8 cases more fluorescencewas found in association with the more proximalganglia; in 1 case the picture was similar in bothparts.Very few fluorescent nerves were detected in
the muscle layers proper in any parts of the gang-
lionic bowel.(b) Distal tissue (Figs. 2B, 3B, and 4B). No
ganglia were present, but in the intermuscularzone widely differing numbers of fluorescentnerves were found, varying from very few in 4cases to large numbers in 9 cases.The larger nerve trunks in this zone were non-
fluorescent apart from an occasional fibre passingthrough, but medium-sized and smaller nerves
were often strongly fluorescent.Corresponding with these differences, big
differences also occurred in the numbers ofnerves in the muscle layers of the most distaltissue. Thus the 4 cases mentioned above alsoshowed very few fluorescent nerves in the musclelayers, which in this respect were similar to thecontrols. In 5 cases there were somewhat more
nerves than in the controls, with more in thelongitudinal than in the circular muscle in 3,the distribution being approximately equal in theother 2. The 9 remaining cases had many nervesin the muscle layers, there being more in thelongitudinal muscle in 6 of them, more in thecircular muscle in 2, and an approximately equaldistribution in both layers in 1 case.
As one ascended the bowel there was always a
decrease in the numbers of nerves in the musclelayers, so that by the time the most proximalpart of the aganglionic tissue was reached very
few fluorescent nerves were usually found.
Correlation between adrenergic nerves andAChE-positive nerves, in distal aganglionictissue. Corresponding tissues have been examinedby both methods in 14 cases, and in this group all
of the specimens that contained more adrenergicnerves than normal in the muscle layers also con-tained many AChE-positive nerves. The tissuesshowing the most nerves by one method did notnecessarily show the most by the other method.The adrenergic nerves tended to be more con-spicuous in the longitudinal muscle, but in thecircular muscle there always appeared to be moreAChE-positive nerves than adrenergic nerves.The 3 cases with very few AChE-positive
nerves also had very few adrenergic nerves. Oneodd case is left which contained fairly large numbersof AChE-positive nerves but very few adrenergicnerves.
Correlation between AChE-positive nervesand the clinical presentation (see the Table).The previous paper (Bennett et al., 1968) and thepresent study have shown a correlation betweenthe patients with many nerves in the distal part ofthe bowel and a severe form of presentation.
TABLENumerical Assessment of AChE-positive Nerves inCircular Muscle of Distal Aganglionic Bowel from
Hirschsprung's Disease (15 cases)
Clinical PresentationLength of Agan-glionic Segment Constipation Severe
of Bowel Simple and NevereConstipation Intermittent Neonatal
Obstruction Obstruction
(a) 1-2 cm. .. Case ± Case 8 + + +Case 2 ±
(b) 5-7 cm. Case 3 + + Case 5 + + Case 9 + + +Case 10++ +
(c) Ending in Case 6 + + Case 11 + + +sigmoid Case 7 + +colon
(d) Long segment Case 4 + Case 12++ +disease .. Case 13 + +
Case 14 + + +Case 15 + + +
Note: The number of nerves in normal bowel lies between +and + +.
It was difficult to subdivide the cases intosatisfactory groups because of the numerousdifferences in this disease. Nevertheless, anattempt has been made by dividing the cases into4 groups according to the length of aganglionicbowel present, and into 3 groups according to theseverity of the symptoms. The gross numbers ofAChE-positive nerves in the circular muscle of themost distal tissue have been assessed on a plus
414
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Autonomic Nerves in Rectum and Colon in Hirschsprung's Diseaseand minus basis. From the Table it is evidentthat the cases with the most severe presentationtended to have the most nerves and the mildestcases tended to have the fewest nerves. In factthe 3 cases with the fewest nerves all failed to showa characteristic constricted segment on bariumenema, including one in which the whole of thecolon was aganglionic (see Fig. 4).
It is appreciated that other factors also influencethe effects of this disease, and they will be mentionedin the discussion.There was less correlation between the numbers
of adrenergic nerves and the clinical presentation.
DiscussionThe aim of this histochemical study was to
demonstrate the distribution of AChE-positiveand catecholamine-containing nerves in rectumand colon of children with and withoutHirschsprung's disease. An attempt will be madein this discussion to correlate these morphologicalfindings with the results of physiological experi-ments on muscular activity in both normal andaganglionic bowel. The significance of the varia-tions in the autonomic nerve supply in differentcases of Hirschsprung's disease will also be con-sidered.
Cholinesterase histochemistry shows that thereis a mixed population of myenteric ganglion cellswhich differ both in size and AChE activity innormal human rectum and colon. This is similarto the small intestine (Koelle, 1955; Cauna et al.,1961) and large intestine (Gunn, 1968) in experi-mental animals. These cells contrast with theuniform population of large, strongly AChE-positivecells in conventional parasympathetic gangliasuch as ciliary ganglia in animals (Koelle, 1955)and in the submandibular gland of the cat (Garrett,1966) or human (Garrett, 1967). The myentericganglia therefore should not be considered assimple parasympathetic ganglia. The muscle lay-ers in normal colon and rectum contained moderatenumbers of strongly AChE-positive nerves inamong the muscle cells. Most of these nerveswere probably cholinergic efferents, for it isgenerally agreed that cholinergic autonomic nervesare the most strongly AChE-positive.
Formalin-induced fluorescence showed thatadrenergic myenteric nerves were present in closerelation with myenteric ganglion cells, but veryfew of these nerves were found in the musclelayers of normal bowel; thus confirming thefindings of Norberg (1964), Jacobowitz (1965), andBaumgarten (1967). This seems to indicate thatthe sympathetic nerves exert an indirect effect on
bowel musculature through an influence on ganglioncell activity.The bowel resected from cases of Hirschsprung's
disease varied in the distribution of AChE-positivenerves at different levels from the same case, andlarge differences also existed between differentcases. Distal zones of aganglionic bowel tendedto contain more AChE-positive nerves in thecircular muscle than normal. Ascending thebowel there was a reduction in the numbers ofnerves and often the most proximal zone of agang-lionic bowel contained fewer nerves than normal.Immediately above this, the most distal ganglionicbowel, sometimes called the 'transitional zone',usually had even fewer nerves in its muscle layers.These results are consistent with the manometricestimates of AChE activity by Kamijo et al. (1953),who found that there was much less activity in themore proximal ganglionic tissue in Hirschsprung'sdisease than in the distal aganglionic bowel, andalso less than in a normal control. The observa-tions suggest that the AChE-positive nerves in thedistal aganglionic bowel originate in the sacraloutflow, enter from below, and are distributed in acephalad direction (see Smith, 1967).Where the ganglion cells are absent in
Hirschsprung's disease, there is a concomitantloss in the normal distribution pattern of adrenergicnerves, which then tend to be distributed to avariable extent through both muscle layers.
Before discussing the functional significance ofthese morphological findings, one must considerthe physiology of the nervous control of muscularactivity in normal colon and rectum; a complexand ill-understood subject. The sacral outflowof the parasympathetic system has a motor functionwhich extends proximally from the anal sphincterto the mid-transverse colon; Garry (1933) showedthat division of these nerves in the cat resulted in adilated distal colon, with difficulty in bowel empty-ing, and these results were confirmed by Adamsonand Aird (1932). The lumbar outflow of thesympathetic system, on the other hand, has aninhibitory activity, and stimulation of the lumbarsympathetic ganglia has long been known to causeinhibition of peristalsis in the colon (Langley andAnderson, 1895).The finding that adrenergic nerves have a
functional relation with myenteric ganglion cellsrather than with the muscle cells directly (Norberg,1964; Jacobowitz, 1965) makes it apparent that thecontrol of bowel activity is far more complex thanthe usually held simple concept of a 'motor para-sympathetic' and an 'inhibitory sympathetic'innervation of the muscular tissue. The myenteric
415
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Garrett, Howard, and Nixonganglion cells, as well as co-ordinating peristalticwaves, appear to be concerned with co-ordinatinginhibitory sympathetic activity through theirintimate connexion with the networks of adrenergicaxons. Further, an inhibitory mechanism inthe bowel wall, which may depend on a non-adrenergic system, has recently been postulatedfrom pharmacological evidence in animals(Burnstock, Campbell, and Rand, 1966; Day andWarren, 1968) and also in the human (Bucknell,1966), and this evidence suggests that a proportionof neurones in the bowel wall may in themselvesbe inhibitory in action.The absence of ganglia in the distal segment of
bowel, in Hirschsprung's disease, leads to anabsence of normal peristalsis with a hold-up tothe forward propulsion of bowel contents at thehighest level of aganglionosis. Furthermore, theabsence of the normal arrangement of ganglioncells and surrounding sympathetic nerves makes itlikely that effective inhibitory mechanisms, in-ducing relaxation, are absent in the affectedsegment of bowel. This has been borne out byrecent physiological experiments which have con-stantly shown an absence of recto-anal inhibitoryreflexes in this condition (Lawson and Nixon,1967; Howard, 1968). AChE-positive nerves, onthe other hand, are often present in increasednumbers in the circular muscular layer, especiallyin more distal segments. Their presence, inconjunction with the absence of a normal in-hibitory mechanism, probably explains the con-tracted state of the bowel in a typical case ofHirschsprung's disease. Sometimes there is alsoan accompanying increase in the number ofadrenergic nerves to the muscle layers, but evenif these adrenergic nerves can produce an inhibition,it appears that the cholinergic nerves exert anoverwhelming effect. Evidence that nerves doexert a predominantly contractile effect on theaganglionic bowel in Hirschsprung's disease wasgiven by Bodian, Stephens, and Ward (1949),when they found that spinal anaesthetic producedrelaxation of the distal segment, during bariumenema examination in 3 cases. They consideredthat this finding indicated that there was a 'spasticobstructive factor'. Ehrenpreis (1946) had previ-ously reported similar findings in 2 cases, relaxationbeing observed through a proctoscope.The present morphological investigation of
cases of Hirschsprung's disease suggests that, aswell as the absence of ganglia and the increasednumbers of AChE-positive nerves in the distalbowel, a further factor may be at least partlyresponsible for the severe bowel dysfunction.
Very few AChE-positive nerves were found in themuscle layers of the distal ganglionic bowel sothat this zone, which may be of variable length,is probably deficient in propulsive power. Thismay accentuate the obstructive effect of the moretonic distal bowel.The clinical presentation in this disease is
variable. Bodian et al. (1949) commented thatit was not possible to correlate the degree ofintestinal obstruction in Hirschsprung's diseasewith the length of affected bowel. Similarly,Hope, Borns, and Berg (1965) stated that 'severityof symptoms are not just a matter of the length ofaganglionic segment, but sometimes, given twobabies with the same amount of bowel involved,one may be completely obstructed whilst the otheris only slightly obstructed'. Does the presentmorphological investigation help to explain theseclinical differences ?Though there is an absence of normal ganglia
throughout a length of distal bowel in trueHirschsprung's disease, the present study showsthat in the circular muscle of this segment, thenumbers of AChE-positive nerves vary consider-ably. This wide range ofAChE activity, extendingfrom few nerves to many more than normal, isreflected in the results of manometric studies byAdams et al. (1960), for they also found a greaterrange of activity in aganglionic tissue fromHirschsprung's disease than in normal controls.This variation may account for some of the differ-ences in obstructive symptoms. The greatestnumbers of AChE-positive nerves were found inthe circular muscle of distal aganglionic bowelfrom those children who had needed a colostomyfor severe intestinal obstruction in the neonatalperiod. Patients presenting later in life hadfewer AChE-positive muscular nerves extendinga lesser distance along the aganglionic bowel.The 3 patients from this group with the fewestnerves in the muscular layers even showed noconstricted segment on barium enema.
Finally, because of the wide variations thatexist in the numbers of AChE-positive nervesin differing lengths of bowel from Hirschsprung'sdisease, it is advisable to have adequate morpho-logical controls, using AChE histochemistry,whenever muscle from this disease is being investi-gated.
SummaryThe distribution of adrenergic and acetyl-
cholinesterase positive (cholinergic) nerves in themuscle layers of large bowel was studied in resectedspecimens from 23 young children: 4 normal
416
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from

Autonomic Nerves in Rectum and Colon in Hirschsprung's Disease 417controls, and 19 cases of Hirschsprung's disease.The number of cholinergic nerves in the circular
muscle of the aganglionic bowel in Hirschsprung'sdisease varied from case to case, but a correlationwas found between the number of such nerves andthe severity of the disease.The junctional zone between normal and
aganglionic bowel, though containing ganglia,was deficient in muscular nerves.The morphological findings are discussed in
relation to functional activity in normal andaganglionic bowel, and it is suggested that morethan one factor is responsible for the bowel mal-function in Hirschsprung's disease. Aganglionosisresults in a failure of co-ordinated contraction andinhibition. Cholinergic muscular nerves are prob-ably responsible for the typically contracted stateof the distal bowel. In the junctional zone betweennormal and aganglionic bowel, the deficiency ofmuscular nerves probably means that this segmentof bowel can exert only a poor propulsive force.
We wish to thank Miss M. Egan for technical assist-ance and Mr. K. J. Davies for help with the photography.
REFERENCES
Adams, C. W. M., Marples, E. A., and Trounce, J. R. (1960).Achalasia of the cardia and Hirschsprung's disease: the amountand distribution of cholinesterases. Clin. Sci., 19, 473.
Adamson, W. A. D., and Aird, I. (1932). Megacolon: evidence infavour of a neurogenic origin. Brit. J. Surg., 20, 220.
Baumgarten, H. G. (1967). Ober die Verteilung von Catecholami-nen im Darm des Menschen. Z. Zellforsch., 83, 133.
Bennett, A., Garrett, J. R., and Howard, E. R. (1968). Adrenergicmyenteric nerves in Hirschsprung's disease. Brit. med. J.,1, 487.
Bodian, M., Stephens, F. D., and Ward, B. C. H. (1949). Hirsch-sprung's disease and idiopathic megacolon. Lancet, 1, 6.
Bucknell, A. (1966). Studies of the physiology and pharmacologyof the colon of man and other mammals. Ph.D. Thesis,London.
Burnstock, G., Campbell, G., and Rand, M. J. (1966). Theinhibitory innervation of the taenia of the guinea-pig caecum.J. Physiol. (Lond.), 182, 504.
Cauna, N., Naik, N. T., Leaming, D. B., and Alberti, P. (1961).The distribution of cholinesterases in the autonomic ganglia ofman and of some mammals. Bibl. anat. (Basel), 2, 90.
Day, M. D., and Warren, P. R. (1968). A pharmacological analysisof the responses to transmural stimulation in isolated intestinalpreparations. Brit. J. Pharmacol., 32, 227.
Ehrenpreis, T. (1946). Megacolon in the newborn. A clinical androentgenological study with special regard to the pathogenesis.Acta chir. scand., Suppl. 112.
-, Norberg, K. A., and Wirsen, C. (1968). Sympathetic in-nervation of the colon in Hirschsprung's disease: a histo-chemical study. J. pediat. Surg., 3, 43.
Eranko, 0. (1967). The practical histochemical demonstration ofcatecholamines by formaldehyde-induced fluorescence. J. roy.micr. Soc., 87, 259.
Garrett, J. R. (1966). The innervation of salivary glands. I.Cholinesterase-positive nerves in normal glands of the cat. ibid.,85, 135.- (1967). The innervation of normal human submandibular and
parotid salivary glands. Demonstrated by cholinesterasehistochemistry, catecholamine fluorescence and electro-microscopy. Arch. oral. Biol., 12, 1417.
Garry, R. C. (1933). The nervous control of the caudal region ofthe large bowel in the cat. J. Physiol. (Lond.), 77, 422.
Gomori, G. (1952). Microscopic Histochemistry. University ofChicago Press, Chicago.
Gunn, M. (1968). Histological and histochemical observations onthe myenteric and submucous plexuses of mammals. J. Anat.(Lond.), 102, 223.
Hope, J. W., Borns, P. F., and Berg, P. K. (1965). Roentgenologicmanifestations of Hirschsprung's disease in infancy. Amer.J. Roentgenol., 95, 217.
Howard, E. R. (1968). Abnormality of anorectal physiology inHirschsprung's disease. Amer. J7. dig. Dis., 13, 432.
Jacobowitz, D. (1965). Histochemical studies of the autonomicinnervation of the gut. J. Pharmacol. exp. Ther., 149, 358.
Kamijo, K., Hiatt, R. B., and Koelle, G. B. (1933). Congenitalmegacolon. A comparison of the spastic and hypertrophiedsegments with respect to cholinesterase activities and sensitivitiesto acetylcholine, DFP, and the barium ion. Gastroenterology,24, 173.
Koelle, G. B. (1955). The histochemical identification of acetyl-cholinesterase in cholinergic, adrenergic and sensory neurons.J. Pharmacol. exp. Ther., 114, 167., and Friedenwa1d, J. S. (1949). A histochemical method forlocalizing cholinesterase activity. Proc. Soc. exp. Biol. (N.Y.),70, 617.
Langley, J. N., and Anderson, H. K. (1895). On the innervationof the pelvic and adjoining viscera. I. The lower portion of theintestine. J. Physiol. (Lond.), 18, 67.
Lawson, J. 0. N., and Nixon, H. H. (1967). Anal canal pressuresin the diagnosis of Hirschsprung's disease. 7. pediat. Surg.,2, 544.
Meier-Ruge, W. (1968). Das Megacolon: seine Diagnose undPathophysiologie. Virchows Arch. path. Anat., 344, 67.
Niemi, M., Kouvalainen, K., and Hjelt, L. (1961). Cholinesterasesand monoamine oxidaase in congenital megacolon. 7. Path.Bact., 82, 363.
Norberg, K. A. (1964). Adrenergic innervation of the intestinalwall studied by fluorescence microscopy. Int. J3. Neuro-pharmacol., 3, 379.
Richardson, K. C. (1958). Electronmicroscopic observations onAuerbach's plexus in the rabbit, with special reference to theproblem of smooth muscle innervation. Amer. J. Anat., 103,99.
Smith, B. (1967). Myenteric plexus in Hirschsprung's disease.Gtut, 8, 308.
Correspondence to Mr. E. R. Howard, King's CollegeHospital, Denmark Hill, London S.E.5.
on 6 August 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.44.235.406 on 1 June 1969. D
ownloaded from