Embed Size (px)
Citation preview

9/23/19
1
Medical Malpractice -How to Avoid a Lawsuit (?) Sarah Hoper MD,JD
Avoiding Litigation?} 1452 closed claims reviewed by trained physicians:
◦ 37% of closed claims à no error
◦ 27% of closed claims without errors à compensated
◦ 27% of closed claims with errorsà no compensation
* Studder, DM. et al. “Claims Errors, and Compensation Payments in Medical Malpractice Litigation.” New England Journal of Medicine 354 (May 11, 2006): 2024-2033.
Avoiding Litigation?
} Less than 15% of patients with valid claim filed a suit
} Negligence found in only 15% of filed claims
Weiler et al. A measure of Malpractice: Medical Injury, Malpractice Litigation, and Patient Compensation (Cambridge, MA: Harvard University Press 1993)
PA Demographics
�120,000 PA in the US
�66.7% Female
�30-34 years old
�5-9 years of clinical experience
PA Specialties�18.4% Family Practice
�10.3% Orthopedics
�8.9% Emergency Medicine

9/23/19
2
PA Medical Liability 1991-2007� National Practitioner Data Bank 1991-2007
� 1 case for every 32.5 PAs
� 1 case for every 2.7 physicians
Physician Assistant Malpractice History: Comparing PAs to Physicians and Nurse Practitioners by Jeffrey G. Nicholson, PhD, PA-C, Journal of Medical Licensure and Discipline, Volume 95, Number 2, 2009.
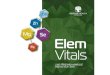
PA Medical Liability 1991-2007� Average and median APN pay outs:
$350,540 and $190,898.
� Average and median physician pay outs: $301,150 and $150,821
� Average and median PA pay outs: $173,128 and $80,003.
PA Medical Liability 1991-2007�APN were working in higher risk
specialties
�Anesthesia (47%)
�Obstetrics (25%)
PA Medical Liability 2005-2014� National Practitioner Data Bank 2005-2014
� Physicians:11.2 cases to 19.0 per 1,000
� PAs: 1.4 cases to 2.4 per 1,000
� NPs: 1.3 cases per 1,000
Brock DM1, Nicholson JG2, Hooker RS3. Med Care Res Rev. Physician Assistant and Nurse Practitioner Malpractice Trends. 2017 Oct;74(5):613-624. doi: 10.1177/1077558716659022. Epub 2016 Jul 25.
Median Pay Outs Relative Risk Ratios

9/23/19
3
Becoming A Physician Assistant by Jody Tomic PA-C
�LEADING Complaint in PA Med Mal Cases:�Failure of the PA to contact the
physician.�Did not see the need to contact�Apprehensive about disturbing
their supervising physician with frequent questions.
� Older the physician à more likely to be sued
�Under 40 : 8% (15.3%*)
�55+: 50% (60.5%*)
Guardado, J. Medical Liability Claim Frequency Among US Physicians. AMA Benchmarking Survey 2016.
*Kane, C. Policy Research Perspectives: Medical Liability Claim Frequency: A 2007-2008 Snapshot of physicians.” (Chicago, IL: American Medical Association 2010).
Whose Getting Sued… Whose Getting Sued
} Men > women
◦ Men: 47.5%
◦ Women: 23.9%
Whose Getting Sued} Men concentrated in HIGH RISK specialties
o 23.8 % of menà surgeons or OB/GYNs� 14.8% women à surgeons or OB/GYNs
o 25.1% of women àpediatricians or psychiatrists� 13.2% of men à pediatricians or psychiatrists
} 33% of Men are 55+ v. 15% of women >55
CRICO 2011 Annual Benchmarking Report: Emergency Medicine

9/23/19
4
Whose Getting Sued…� Specialties most likely to be sued..
1. OB/GYN
2. General Surgeons
3. Surgical Sub –Specialties
4. Emergency Medicine
5. Radiology
Cases from 2006-15 Physician Insurers Association of America
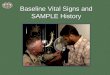
The Award…Ave. Indemnity 2006-2015 The Award…
� Of cases that resulted in a payment
�Settled = 91.8%
�Plaintiff Verdicts = .9%
� 68% of cases are dropped, dismissed or withdrawn
PIAA Closed Claim Comparative, 2016 Edition.
PIAA Closed Claim Comparative, 2014 Edition.

9/23/19
5
The Cost to Defend….2013Iowa Data - National Practitioner Data Bank
Iowa Data - National Practitioner Data Bank
Iowa Data - National Practitioner Data Bank
Iowa Data - National Practitioner Data Bank
�There are four elements to a malpractice case:
�Duty�Breach of Duty�Injury�Damage
Elements of Malpractice

9/23/19
6
� A duty is owed =practitioner undertakes care or treatment of a patient
◦ EMTALA = ALL patients evaluated and stabilized
◦ Other practitioners may choose not to treat a pt
Element 1 - DutyBreached Duty = provider fails to provide
relevant standard of care
� The standard of care is proved by expert testimony
� 40% of states have locality rule
� 60% of states have national standard of the profession
Element 2- Breach of Duty
Breach of Duty: Dizzy Patient� 50 y/o HTN, HLD, non-smoker, no family
h/o stroke, DVT, early MI comes in with dizziness. Better when laying down and worse with standing up and looking to the right and left started 90 minutes ago.
�No nystagmus�Difficulty with heel to toe�Finger to Nose difficult but intact�No protator drift�5/5 strength in all extremities�EKG: NSR
Breach of Duty: Dizzy Patient
�Pt gets 2 mg of IV Versed
� Reassessment still dizzy but better
�Pt discharged with vertigo on meclizine
Breach of Duty: Dizzy Patient
�Pt returns 2 days later MRI shows vertebral artery thrombus causing partial occlusion�Shower of emboli to brain
�A practitioner must exercise the reasonable degree of learning and skill ordinarily possessed by practitioners in the locality where the practitioner practices
Breach of Duty: Locality Rule

9/23/19
7
�Better protection for rural practitioners
� May not have access to consultants
Breach of Duty – Locality Rule
�A practitioner has a duty to use the degree of care and skill that is expected of a reasonably competent practitioner in the same class to which he or she belongs, acting in the same or similar circumstances
Beach of Duty: National Rule
� The breach must:
� Cause an injury � Be a proximate cause of the injury
� MD orders Gabapentin on the wrong pt
� Pt is notified – is drowsy
� NO INJURY� Pt has an MI
�NO PROXIMATE CAUSE
Element 3- Injury�Damages:
�physical or emotional�Patient wrongly receives
gabapentin� Drowsy� No intervention required� No Damage
Element 4 -Damage
2017 Iowa Medical Liability Reform�Noneconomic damages capped at
$250,000
�Except where jury finds care resulted in substantial or permanent loss or impairment of bodily function, substantial disfigurement or death
�Certificate of merit �Expert witness to certify standard
of care was breached
�Submited within 60 days of the defendant’s response to the initial notice and before discovery starts
� No certificate = lawsuit dismissed and cannot be refilled
2017 Iowa Medical Liability Reform

9/23/19
8
� Expert witness standards
� Expert witness = licensed + in the same or a substantially similar, field as the defendant
� Witness must be in active practice or academia within the five years before the incident in the lawsuit occurred
2017 Iowa Medical Liability Reform Case 1: HPI
�10 y/o boy, no daily medications..�Headache + Fever
�No photophobia�No neck stiffness�No rash�No N/V
Case 1� PMHX: asthma� SHX: 4th grade� Vitals:
� T 102.2 HR 130 Resp 22 110/80
Case 1: Physical Exam� Mental Status: Awake alert� Head/Neck: no meningismus� Eyes: EOMI, PERRLA� Chest: CTAB� Card: RRR� Ab: benign� GU: uncircumcised, testes descended� Skin: no rash� Neuro: cranial and cerebellar fxn nl,
motor/sensation intact
Case 1� What do want to do…
� CBC� CMP� UA� CXR� Blood cultures� LP
Case 1� Results:
� WBC 4,000 – bands� Platelets – nl� CXR – nl� UA - nl

9/23/19
9
Case 1� 15 minutes after LP
� Mom alerts MD to pink patches on patients’ lower legs
� “Consistent with patient being held for LP”
Case 1� LP –
� clear no xanthochromia� No WBC� Protein/glucose – nl� Gram stain (-)
Case 1� Repeat vitals:
� Temp 38� HR 120
Case 1� What Next…
� Pt discharged @ noon� Dx: viral syndrome
Case 1� 17:30 – EMS
� “10 y/o male. Limp and agonal respirations with thready pulse. BVM in process, IO placed.”
� Rash: Purpuric
Case 1� 20 ml/kg IVF
� IV ABT: vancomycin and ceftriaxone� Dopamine started
� Cardiac arrest….

9/23/19
10
Case 1� Blood and CSF cultures:
� Neisseria meningitidis
� DX:� Meningococcemia� Sepsis
Case 1� What was missed:
� Leukopenia with bands� Rash� Start IV antibiotics while waiting for LP
results?
Case 2: MD’s HPI 39 white overweight female w 1 month h/o cough and congestion
� PCP tx’ed w antibiotics 1 month ago à got better
Case 2: MD’s HPI� Now cough + yellow sputum returned
� Sharp frontal chest pain w cough radiates to back
� Post-tussive vomiting� No fever� No SOB
Case 2: Past Hx� Meds: Birth Control Pills� No past medical history� No Allergies� Social: smoke 1.5 ppd, etoh 6pack/daily
Case 2: Physical Exam� Vitals: T 97.4 P 72 R 18 138/93 Pain 8/10� Constitutional: slightly obese, no acute distress� HEENT: mouth/pharynx clear� Neck: supple, no LAD, no JVD� Lungs: wheezing at the bases� Chest: TTP over the anterior chest wall� Cards: RRR, nl S1S2� Back: non-tender� Ext: no cyanosis, edema

9/23/19
11
Case 2� What Do you want to do…
� CXR: no infiltrate or edema, normal heart size
� Tylenol 975 mg
� Albuterol neb
Case 2: Reassessment� 1 hour later:
� chest pain is improved from 8/10 to 5/10� Lungs now clear
Case 2: Dx� Acute Bronchitis
� Tx:� 10 days of Azithromycin
Case 2: At home� Pt goes home and rests, husband goes to
work� @ 16:00 still not feeling well but makes
dinner for family� @17:15 Pt falls to the floor unresponsive� Husband calls 911 thinks she has choked
on food
Case 2: EMS� 17:21 Asystole on arrivalà
� CRP started � Intubated� Several rounds of epi
� 17:40 V Fib à shocked 200-300-360� 18:01 arrive at hospital
� 18:09 Code Called
Case 2: Autopsy� Focal area of LAD with 99% luminal
narrowing
� Cause of Death: Acute MI

9/23/19
12
Case 2-Triage Nurse� Woke up from sleep w back pain, chest
pain and arm pain� Took Mortinà no improvement
� Pain b/w shoulder blades� Radiates down the R arm� Midsternal chest pressure
Case 2: What was missed� Better history of chest pain
� Worse w exertion?� Radiation?� Diaphoresis?� Chest pain when you are not coughing?
Case 2: What was missed� Correlation b/w Triage and MD notes
� Must address all the problems presented in triage note
� “mid sternal chest pressure radiates to R arm”
Case 2: What was missed� Cardiac Risk Factors
� 1.5 ppd smoker� Obese� Birth Control Pills� Family History?
� Brother died at age 32 of MI
Case 2: What was missed
EKG
Case 3: HPI� 15 y/o otherwise healthy female with
� Fatigue and Dizziness x 2 days� RLQ abdominal aching pain� Worse with movement/walking

9/23/19
13
Case 3: HPI� Associated:
� + Nauseaà no vomiting� + Fever� No diarrhea/constipation� No vaginal bleeding/discharge
Case 3: HPI� Past Medical History:
� No abdominal surgeries� No h/o ovarian cysts or endometriosis� Just finish LMP
Case 3: Physical Exam� T 99.8 P 124 R 18 100/64 Pain 10/10� Constitutional: tired, A/O x 3� Throat: nl pharynx, no tonsillar hypertrophy� Neck: supple, no LAD� Card: RRR, no M/R/G� Resp: CTAB� Abd: BS+, soft, ND, + TTP in the RLQ, no
rebound/guarding� Skin: nl for age
Case 3 Treatment� Several doses of:
� Phenergan� Demerol� IVF
Case 3: Work Up� What do you want to do?
� CBC: WBC 17� CMP: unremarkable� Urine Preg: (-)� UA: (-)� CT
Case : Sign Out� MD 1 goes home
� Signs out CT scan to MD 2

9/23/19
14
Case 3: Work Up� CT with contrast:
� Appendix: normal size w/o surrounding inflammation
� R adnexa: several >1 cm ovarian cysts Largest 3 cm – hazy attenuation suggesting recent hemorrhage
Case 3: Diagnosis� Ovarian Cyst
� F/U with OB� RX: Vicodin #20, Phenergan PO and
suppository
Case 3: At home� Pt continues to have pain for 36 hours
� Severe pain throughout the night� Not able to keep anything down
� Called PCP � “I think her ovarian cyst ruptured”� Appointment at 11AM
Case 3: PCP� Pt in wheelchair every ill appearing� Skinà gray� Head bobbing
�SENT TO 2nd ED
CASE 3: ED #2 @ 12:30� Assumed missed appendicitis
� Repeat CT: “inflammation in the pelvis but the appendix looks OK. No ovarian cysts”
� Did not have first CT to compare
Case 3: ED #2� Pelvic
� Pt states she is not sexually active� Right adnexal tenderness� No discharge or cervical motion tenderness

9/23/19
15
Case 3: ED #2� Pelvic Ultrasound:
� Unremarkable� No mention of R ovarian cysts
Case 3: ED #2� Consults:
� OB (repeat pelvic)� Surgery (repeat pelvic)
� Pt continues to deteriorate � Diffuse peritonitis
Case 3: ED #2� OB attending agrees to take patient to
OR for Ex Lap� Patient admits she is sexually active
Case 3: OR @20:15� “Pus poured out through the trochars”
� Changed to open lap� “Purulent material extruded through the
surgical incision and in her pelvis”� “Right ovary is spewing pus”
� DX: Ruptured Ovarian Abscess with Sepsis
Case 3: Diagnosis� Started on antibiotics:
� Cefotan� Doxycycline� Flagyl� Gentamicin
Case 3: ICU� @ 21:30 Hypotensive à Pressors� @7:15 Full arrest à resuscitated and
regains a pulse� @ 7:20 losses pulse

9/23/19
16
Case 3: Legal Case� ED #1 What’s Missing:
� No sexual history� No pelvic exam� No antibiotics in face WBC of 17
� No Explanation that Ovarian Cyst is NOT a definitive diagnosis
Case 3: Legal Defense� Operating OB/GYN was plaintiff's expert
witness� No social history� No pelvic� Defendants argued OB/GYN cannot pass
judgment on standard of care of EM doc
Case 3: Legal Defense� This case is a Zebra!
� ED#2:� CT, US, and pelvic x 3 dx still not made
� Defendants won� Case took 4 years
Case 3: Sign Outs� Very High Risk
� 3 minutes:� 2 minutes to reassess the patient� 1 minute to write a follow up note
Case 3: Of Note� CDC Guidelines on PID Tx:
� “Empiric treatment of PID should be initiated in sexually active young women and other women at risk for STDs if the following minimum criteria are present and no other cause for the illness can be identified:� Uterine/adnexal tenderness or cervical
motion tenderness”
Recap…How not to get sue?1. Don’t See Patients2. Communication is Key3. Address All Complaints4. Address Lab Abnormalities5. Do NOT Ignore Signouts

9/23/19
17
Questions?