Embed Size (px)
Citation preview

www.aana.com/aanajournalonline.aspx AANA Journal February 2012 Vol. 80, No. 1 61
AANA Journal CourseUpdate for Nurse Anesthetists
Awake Craniotomy: A Practice Overview
Garry Brydges, CRNA, DNP, ACNP-BCRoxanne Atkinson, CRNA, MSNMonie James Perry, CRNA, MSNDarline Hurst, CRNATravis Laqua, CRNA, MSNJohn Wiemers, CRNA, MSN
ObjectivesAt the completion of this course, the reader should be able to:
1. Identify the anatomical structures and functions of the “eloquent” cerebral cortex.
2. Understand the need for careful planning and implementation of anesthetic care in a patient un-dergoing an awake craniotomy.
3. List and discuss the components of a regional scalp block and associated caveats.
4. Describe the potential complications of cortical mapping and associated management techniques.
5. Articulate the overall anesthesia techniques used in performing awake craniotomies.
IntroductionAnesthesia providers are familiar with the gross anatomy of the human brain, ie, the cortex, midbrain, and brain-
stem. However, within the cerebral cortex, the anatomi-cal locations of the highly functional components are much more variable. It is the unique location of these areas in each person that poses a challenge in modern neurosurgical procedures. The areas of the cortex that contain speech and language centers and the motor strip are termed eloquent. More specifically, these areas include the Broca area, Wernicke area, arcuate fascicu-lus, insular brain, and motor and sensory cortexes of the brain.1,2 The Broca area is responsible for speech produc-tion and language processing, whereas the Wernicke area is mainly responsible for language comprehension. The arcuate fasciculus is a bundle of neurons that trans-fers information from these areas. The insular brain is a complex, subcortical structure involved in the perception of pain, emotion, self-awareness, speech articulation, motor skills, and other functions.
Specialized imaging techniques can locate some criti-
*AANA Journal Course No. 31 (Part 6): AANA Journal course will consist of 6 successive articles, each with objectives for the reader and sources for additional reading. At the conclusion of the 6-part series, a final examination will be published on the AANA website and in the AANA Journal. Successful completion will provide the participant 6 CE credits (6 contact hours). This course has been prior-approved by the American Association of Nurse Anesthetists for 6 CE credits; AANA code number: 1025705, expiration date: July 31, 2012. The American Association of Nurse Anesthetists is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. This educational activity is being presented with the understanding that any conflict of interest on behalf of the planners and presenters has been reported by the author(s). Also, there is no mention of off-label use for drugs or products.
6 CE Credits*
6
Craniotomies are a common neurological intervention for intracranial tumor resections. Anesthesia tech-niques allow surgeons to aggressively and optimally resect neoplastic tissue while sparing normal cerebral tissue. Awake craniotomies are surgical techniques that enable surgeons to avoid damaging normal cere-bral regions and allow real-time patient feedback. Such surgical interventions would not be possible without anesthesia. The role of anesthesia providers is critical in gaining the trust and motivation of the patient. Preoperative evaluation, regional anesthesia,
general anesthesia, and monitored anesthesia are necessary to achieve a successful surgical intervention with awake craniotomy. As awake craniotomy gains more popularity, dependable anesthesia techniques remain critical. A discussion follows of the role of anesthesia providers in awake craniotomy during the entire perioperative continuum.
Keywords: Awake craniotomy, Broca area, cortical mapping, scalp block, Wernicke area.

62 AANA Journal February 2012 Vol. 80, No. 1 www.aana.com/aanajournalonline.aspx
cal areas of the brain, but the techniques are somewhat imprecise. Only 50% of areas relevant to speech located by direct stimulation coincide with magnetic resonance imaging results.3 Awake craniotomies are often used to identify and, thus, avoid the eloquent areas of the brain that allow speech, motor, and vision functions. During an awake craniotomy, a patient is conscious as the surgeon stimulates different areas of the brain while asking the patient to perform certain tasks. With the patient awake, the eloquent areas of the brain can be precisely mapped before tumor resection.4 This mapping minimizes the risk of new functional deficits developing postoperatively and allows for aggressive resection of the tumor and, thus, better neurological and oncological outcomes.5,6
Negative cortical mapping results are associated with a decreased risk of postoperative deficits.5 With positive cortical mapping results, less of the tumor may be safely resected because of the proximity or involvement of the eloquent area, causing an increased risk of neurological deficits and poor outcomes.6,7
According to a study at The University of Texas MD Anderson Cancer Center, Houston, reported by Kim et al5 in 2009, tumor histologic features, tumor location, and preoperative deficits did not prove to be predictors of neurological outcome, whereas cortical mapping results, the extent of the resection, and intraoperative neurologi-cal changes were all predictors of neurological outcome. With an average of 75 awake craniotomies performed each year at the MD Anderson Cancer Center, the neu-roanesthesia team combined its experience with findings in the current literature to develop an evidence-based practice that regularly enables patients to be cooperative, alert, and oriented, and facilitates cortical mapping.
Anesthetic Objectives for Awake CraniotomiesThe primary anesthetic objectives of an awake crani-otomy are to allow for accurate cortical mapping of the eloquent cortex and to maximize patient comfort. To achieve these objectives, anesthesia providers must main-tain hemodynamic stability and adequate ventilation throughout the entire procedure.5 In addition, preven-tion of nausea and vomiting is paramount because any increase in intracranial pressure may cause subsequent brain edema and associated detrimental effects.8
Different approaches to achieving these objectives may be used. The awake craniotomy is effectively divided into 3 segments: preparation and pinning, cortical mapping, and resection and closure. Anesthetic techniques have been de-veloped to meet the needs of each stage. These techniques include a monitored anesthesia care (MAC) technique throughout the entire procedure and an asleep-awake-awake technique or an asleep-awake-asleep technique, with or without use of a laryngeal mask airway (LMA).
The monitored anesthesia care and asleep-awake-awake technique involve continuous intravenous seda-
tion while the patient breathes spontaneously during a portion or all of the procedure. However, without the ability to control ventilation, the potential for hyper-capnia due to sedation often makes surgical exposure less than optimal. It is for this reason that the asleep-awake-asleep technique, with the use of an LMA, is the most widely used technique at the MD Anderson Cancer Center. The use of an LMA allows anesthesia provid-ers to augment ventilation and avoid hypercapnia and hypoventilation.4 Use of an LMA also facilitates greater depth of anesthesia during the painful components of the surgery and while the scalp block is performed.9 Once the surgeon is ready for mapping, all sedation may be discontinued, allowing the patient to be as alert and responsive as possible.
Regardless of the technique used, anesthesia drugs that rapidly dissipate are the most desirable. Infusion techniques using short-acting medications allow for deli-cate control of the anesthetic level in awake and asleep patients and with spontaneous and controlled ventilation (Tables 1 and 2).
Preoperative PreparationPatients undergo a comprehensive and extensive preop-erative interview the day before surgery with their anes-thesia provider. This discussion is invaluable for evaluat-ing and optimizing a patient’s emotional readiness for this unique surgical experience.10 The primary predictor of the success of awake craniotomy is prudent patient selection. Patients who are not candidates for awake cra-niotomy include patients with decreased mental capacity, a history of substance abuse, or a history of violent awak-enings from anesthesia.11
On the day of surgery, baseline testing is performed using flash cards for picture and word identification. Benzodiazepine premedication is avoided because of its residual sedative and amnestic effects during the intraop-erative assessment phase; however, the avoidance of ben-zodiazepines in this setting continues to be debated.10,12
A useful substitute for midazolam in an adult un-dergoing cortical mapping and tumor resection is a preoperative discussion in which good rapport and a trusting relationship are established between the patient and the anesthesia provider. If a patient remains tre-mendously anxious, a diminutive infusion of propofol may be titrated to effect en route to the operating room. Other preoperative pharmacological adjuncts consist of gastrointestinal premedication with aprepitant, metoclo-pramide, or famotidine. In addition, patients may receive antiepileptic prophylaxis levetiracetam or fosphenytoin.
InductionOn arrival in the operating room, patients are asked to make themselves comfortable on the operating room table in the surgical position, usually a lateral position.

www.aana.com/aanajournalonline.aspx AANA Journal February 2012 Vol. 80, No. 1 63
Allowing patients to place themselves in the position required for the procedure optimizes patient comfort during the many hours they are awake and confined to the designated operative position. In addition to in-creasing comfort, self-positioning enables patients to recognize this position as a point of reference during emergence from the asleep phase of the anesthetic. The
anesthesia team manages the patient’s airway from the side of the patient during the entire procedure.
Standard monitors are applied, with the addition of a bispectral index (BIS) monitor and an arterial line, which is usually inserted after induction. Hemodynamic moni-toring is augmented with the use of a minimally invasive continuous cardiac output and stroke volume variation
Drug Mechanism of action Advantages Disadvantages Classification
Propofol GABAA agonist Rapid onset; antiemetic; Respiratory depression Intravenous anesthetic antiepileptic; decreased in combination with intracranial pressure other narcotics
Remifentanil Selective µ-opioid agonist Rapid offset; blunted Bradycardia Opioid hemodynamic responses
Dexmedetomidine Selective α2-agonist Anxiolysis, analgesia; Bradycardia; Adrenergic receptor respirations maintained hypotension agonist
Fentanyl, avoid Opioid agonist Pain control Prolongs wakeup; Opioid respiratory depression
Midazolam, avoid GABAA agonist Amnesia Causes confusion Benzodiazepine during awakening
Table 1. Anesthetics Agents Used in Awake CraniotomyAbbreviation: GABAA, γ -aminobutyric acid ionotropic receptor family A.
Table 2. Awake Craniotomy Drug Dose Chart
Drug Dose Advantages Disadvantages
Induction medicationsRemifentanil 0.5-2.0 µg/kg/min Short half-life Bradycardia; caution with
β-blockade
Propofol 1.0-2.0 mg/kg Rapid onset of action; rapid change of level of sedation with dose; antiemetic effect; antiepileptic effect; decreased intracranial pressure
Rocuronium 50 mg IV
Maintenance (asleep)Remifentanil 0.05-0.1 µg/kg/min
Propofol 50 µg/kg/min
Desflurane 0.5 minimum alveolar concentration
Scalp block
Ropivacaine 0.5% with 30-60 mL Pain control 1:200,000 epinephrine
Maintenance (awake)
Remifentanil 0.01-0.04 µg/kg/min Pain control for extended time in same position
Maintenance (closure)
Remifentanil 0.05-0.1 µg/kg/min Pain control Respiratory depression
Propofol 50 µg/kg/min Sedation Incidence of respiratory depression, especially in combination with other narcotics or sedatives
Dexmedetomidine 0.2-0.4 µg/kg/h Sedative, anxiolysis, and analgesic Dose-dependent bradycardia properties and hypotension reported; possible increase or decrease in seizure threshold

64 AANA Journal February 2012 Vol. 80, No. 1 www.aana.com/aanajournalonline.aspx
sensor. Two large-bore intravenous lines are adequate unless excessive blood loss is expected or the possibility of air embolism due to tumor location is anticipated. In either of these cases, central intravenous access is preferred.13
In female patients, indwelling urinary catheter place-ment is done in the supine position, and patients receive brief propofol sedation, which is then terminated for self-positioning. Urinary catheter placement in male patients occurs after induction of general anesthesia. Lidocaine jelly is used during insertion to lessen the discomfort of the catheter during the awake component of the surgery.
General anesthesia is induced using remifentanil and propofol. These medications are used for induction and maintenance of anesthesia because of their ability to provide smooth and rapid wake up of a cooperative patient. With the patient secured in the lateral position, one member of the anesthesia team maintains the mask fit while the other ventilates the patient. One dose of ro-curonium (30-50 mg) may be given to facilitate full pha-ryngeal relaxation and LMA placement. The anesthesia provider inserts the LMA while facing the patient, who remains in the lateral position. This approach ensures the ability to manage the airway during the procedure should the patient become apneic or restless or his or her condition become unstable and full induction of general anesthesia and controlled ventilation be required. Administering a paralytic agent and managing the LMA and patient’s airway from the patient’s side reinforce the ability to do so and ventilate the patient for any reason should it become necessary.
Ventilation through the LMA must be satisfactory because it will facilitate brain relaxation and control of intracranial pressure. The ProSeal LMA (LMA North America, Inc, San Diego, California) is most often used because of its gastric access and high-pressure seal; however, use of the Supreme LMA (LMA North America, Inc, San Diego, California) offers an integral bite block, which is preferred by some providers. Patients receive propofol (75-125 mg/kg/min) and remifentanil (0.2-0.5 µg/kg/min) infusions and desflurane via the LMA for anesthetic maintenance. The use of dexmedetomidine is commonly cited in the literature as part of the anesthetic for awake craniotomies.14,15 However, when added to remifentanil and propofol infusions, dexmedetomidine can delay emergence and removal of the LMA. At the MD Anderson Cancer Center, dexmedetomidine is typically reserved for the postresection and closure phase of the procedure.
Scalp BlockPatient comfort is paramount during the awake com-ponent of cortical mapping and tumor resection. Skull pins, which are inserted during surgical preparation, can be very stimulating.16 In addition to the occurrence of hypertension and tachycardia, stress hormones such as
cortisol and adrenocorticotropic hormone are released in response to such noxious stimuli.17,18 Achievement of the surgical procedure, therefore, ultimately depends on a successful scalp block being performed by the anes-thesia provider. In addition, local anesthetic infiltration of the temporal muscle flap and dura are performed by the neurosurgeon; these techniques offer hemodynamic and stress response control and enhance patient coopera-tion. During the postinduction period, a comprehensive, well-executed scalp block can prove to be the difference between a comfortable, compliant, awake patient and a patient requiring resedation.
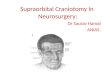
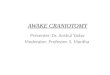
Most studies recommend the use of 0.25% or 0.5% bupivacaine, with or without epinephrine, for a scalp block.17,18 However, bupivacaine increases the risk of depressed cardiac contractility and conductivity.17 Thus, 0.5% ropivacaine, which has a pharmacological profile similar to that of bupivacaine, along with epinephrine, 5 µg/mL (1:200,000), in a total volume of 30 to 60 mL, is the common practice at the MD Anderson Cancer Center. In addition, before opening the dura, the surgeon can infiltrate the dura and temporalis muscle flap with an equal mixture of 1% lidocaine and 0.25% bupivacaine preservative-free local anesthetic. The scalp block con-sists of 7 main nerve blocks, as outlined in Table 3.
Intraoperative Wake UpOnce the dura is opened, the surgeon will ask the anes-thesia team to awaken the patient for neurological evalu-ation and speech and/or motor testing. It is customary to have 2 anesthesia providers caring for the patient. While one is devoted to calmly reassuring and orient-ing the patient during the emergence phase, the other manages the patient’s blood pressure and heart rate and prepares for headache management and reinduction if general anesthesia becomes necessary. Nicardipine, la-betalol, metoprolol, and esmolol should be available to control hypertension and tachycardia, and ephedrine and phenylephrine should be available to treat hypotension. Headaches are treated with lidocaine infusion or remi-fentanil at a low infusion rate. In addition, preoperative acetaminophen may prevent headaches.12 Ondansetron is administered before awakening the patient (typically before the bone flap is raised) to prevent nausea and vomiting. Propofol and dexamethasone, with their anti-emetic properties, also help to reduce the occurrence of nausea and vomiting. Manninen and Contreras10 found that the frequency of nausea and vomiting in the early postoperative period is significantly lower in patients awake during craniotomy than in patients undergoing general anesthesia.
Monitoring with the BIS score may be used as an adjunct for timing the safe removal of the LMA and creating a smooth transition from anesthesia.19 A BIS value of 40 to 60 is a reliable indicator of adequate depth

www.aana.com/aanajournalonline.aspx AANA Journal February 2012 Vol. 80, No. 1 65
Tab
le 3
. S
calp
Blo
ck T
ech
niq
ue
(Fro
m O
sbor
n an
d S
ebeo
J.17
)a
Loca
l ane
sthe
tic m
ixtu
re: 0
.5%
rop
ivac
aine
with
epi
neph
rine,
5 µ
g/m
L (1
:200
,000
) in
a to
tal v
olum
e of
30-
60 m
L.(Il
lust
ratio
ns b
y D
avid
Ate
n, M
A, C
MI,
seni
or m
edic
al il
lust
rato
r, M
D A
nder
son
Can
cer
Cen
ter,
Hou
ston
, Tex
as.)
Ner
ves
Ner
ve b
ran
ch
Sen
sory
in
ner
vati
on
S
tep
s an
d l
and
mar
ks
Sup
raor
bita
l Tr
igem
inal
ner
ve
Fore
head
; ant
erio
r pa
rt o
f sc
alp;
P
alpa
te s
upra
orbi
tal n
otch
; ins
ert
need
le a
t th
e ne
rve
(V
1 di
strib
utio
n,
top
of h
ead
up
per
orbi
tal m
argi
n pe
rpen
dicu
larly
(1 c
m m
edia
l
opht
halm
ic d
ivis
ion
to
sup
raor
bita
l for
amen
); st
art
at t
he s
upra
orbi
tal
in
to f
ront
al n
erve
)
notc
h; r
opiv
acai
ne 0
.5%
, 1-3
mLa
Sup
ratr
ochl
ear
Tr
igem
inal
ner
ve (V
1 Fo
rehe
ad; a
nter
ior
part
of
scal
p M
edia
l exp
ansi
on o
f th
e su
prao
rbita
l blo
ck; 1
fin
ger
nerv
e di
strib
utio
n, o
phth
alm
ic
br
eadt
h m
edia
l to
supr
aorb
ital n
erve
blo
ck; s
tay
divi
sion
into
fro
ntal
abov
e th
e ey
ebro
w li
ne; r
opiv
acai
ne 0
.5%
, 1-3
mLb
nerv
e)
(m
edia
l)
Zygo
mat
ico-
Tr
igem
inal
ner
ve (V
2 Te
mpo
ral,
face
to
zygo
mat
ic r
egio
n 1
cm la
tera
l and
1 c
m s
uper
ior
to la
tera
l can
thus
of
tem
pora
l ner
ve
dist
ribut
ion,
max
illar
y
the
eye
abov
e th
e zy
gom
atic
arc
h; in
ject
incr
emen
-
nerv
e)
ta
lly (w
hile
with
draw
ing
need
le t
hrou
gh t
empo
ralis
m
uscl
e); d
eep
and
supe
rfic
ial i
nfilt
ratio
n fr
om t
he
post
erio
r po
rtio
n of
zyg
omat
ic a
rch
to t
he s
upra
-or
bita
l mar
gin;
ner
ve a
rises
bet
wee
n su
prao
rbita
l an
d au
ricul
otem
pora
l ner
ves;
rop
ivac
aine
0.5
%, 3
-5
mLb
Aur
icul
otem
pora
l Tr
igem
inal
ner
ve (V
3
Tem
pora
l, lo
wer
lip,
low
er f
ace,
A
t th
e tr
agus
, 1-1
.5 c
m a
nter
ior
to t
he a
uric
le,
nerv
e di
strib
utio
n, m
andi
bula
r au
ricle
, and
sca
lp a
nter
ior-
supe
rior
palp
ate
the
supe
rfic
ial t
empo
ral a
rter
y (in
tem
pora
l
nerv
e)
to a
uric
le
regi
on a
t pi
nna
supe
rior
to t
he t
empo
rom
andi
bula
r jo
int)
; ear
sho
uld
mov
e po
ster
iorly
as
inje
ctio
n oc
curs
; rop
ivac
aine
0.5
%, 1
-3 m
Lb
Imag
e
cont
inue
s on
pag
e 66

66 AANA Journal February 2012 Vol. 80, No. 1 www.aana.com/aanajournalonline.aspx
Imag
e
Tab
le 3
. S
calp
Blo
ck T
ech
niq
ue
(Fro
m O
sbor
n an
d S
ebeo
J.17
)a
Loca
l ane
sthe
tic m
ixtu
re: 0
.5%
rop
ivac
aine
with
epi
neph
rine,
5 µ
g/m
L (1
:200
,000
) in
a to
tal v
olum
e of
30-
60 m
L.(Il
lust
ratio
ns b
y D
avid
Ate
n, M
A, C
MI,
seni
or m
edic
al il
lust
rato
r, M
D A
nder
son
Can
cer
Cen
ter,
Hou
ston
, Tex
as.)
Ner
ves
Ner
ve b
ran
ch
Sen
sory
in
ner
vati
on
S
tep
s an
d l
and
mar
ks
Gre
ater
P
oste
rior
ram
us o
f se
cond
P
oste
rior
part
of
scal
p an
d oc
cipi
tal
Pal
pate
occ
ipita
l art
ery;
inje
ct m
edia
l to
arte
ry
occi
pita
l ner
ve
cran
ial n
erve
roo
t (c
ervi
cal
area
be
twee
n m
asto
id p
roce
ss a
nd o
ccip
ital p
rotu
-
plex
us, C
2-3)
bera
nce
and
mar
k be
fore
indu
ctio
n; 2
.5 c
m la
tera
l to
nuc
hal m
edia
n lin
e (e
nsur
e ne
gativ
e bl
ood
as
pira
tion)
; the
n in
ject
rop
ivac
aine
0.5
%, 3
-5 m
Lb
Less
er o
ccip
ital
Ven
tral
ram
i of
C2
and
C3
Pos
terio
r pa
rt o
f sc
alp
Fiel
d bl
ock
behi
nd e
ar a
nd o
ccip
ital a
rea;
cre
ate
nerv
e (p
oste
rior
of
spi
nal n
erve
s
a “w
all”
of
loca
l or
fiel
d bl
ock
from
pos
terio
r ea
r au
ricul
ar)
area
to
grea
ter
occi
pita
l ner
ve; i
nfilt
rate
2.5
cm
late
ral t
o gr
eate
r oc
cipi
tal n
erve
, alo
ng t
he s
uper
ior
nuch
al li
ne; r
opiv
acai
ne 0
.5%
, 3-5
mLb
Gre
ater
aur
icul
ar
Cer
vica
l ple
xus
of C
2 an
d C
3 M
asto
id p
roce
ss; p
oste
rior
auric
ular
In
ject
at
the
leve
l of
the
trag
us, 1
.5 c
m p
oste
rior
to
nerv
e
th
e ea
r; r
opiv
acai
ne 0
.5%
, 3-5
mLb
cont
inue
d fr
om p
age
5

www.aana.com/aanajournalonline.aspx AANA Journal February 2012 Vol. 80, No. 1 67
of anesthesia for incision through the dural opening of the brain.19 At a BIS value greater than 80, return to spontaneous respiration generally occurs and LMA removal quickly follows.11 On removal of the LMA, oxygen delivery is initiated via a nasal cannula inserted during the initial LMA insertion. Approximately 10 to 20 minutes are required for a patient to wake up once intra-venous and inhalational anesthetics are discontinued.11 An awake patient is given time to restore alertness to the preoperative level. It is important for a patient to see familiar faces of the anesthesia team during this time. A calm, familiar voice helps keep agitation and confusion to a minimum. Discomfort from the skull pins, intracranial vascular retraction, prolonged positioning may necessi-tate the administration of small amounts of opiates.
Many complications are possible during the time from the asleep to the awake phase of the procedure. Lightening of anesthesia during the wake-up phase in-creases the metabolic rate and cerebral blood flow, and this change increases cerebral volume, which can com-promise the surgical field by creating brain “tightness.” In addition, it is crucial to avoid the Valsalva maneuver, coughing, and vomiting, which can cause bulging of the brain.20 Small amounts of ice chips can help with dry mouth and decrease the need to cough.20
Cortical MappingIf speech centers are involved, picture cards that were evaluated for accuracy preoperatively are reviewed before cortical mapping to ensure that these centers have not been breached during exposure. If motor mapping of the extremities is needed, the patient must demonstrate movement of the affected extremity before cortical mapping takes place. The Ojemann neurostimulator (Radionics, Inc, Chicago, Illinois), with 5-mm spacing between the electrodes, is used. For localization of the primary language and motor cortex, the stimulator is applied in increments of 1 mA. A cortical area is consid-ered eloquent if a motor response or twitch is generated or language errors or pauses are noted in multiple trials.5
Cortical mapping may last from 15 minutes to, in rare cases, 3 hours or more.
Constant communication can be tiresome to patients and anesthesia providers. This is yet another reason why it is imperative to build an excellent rapport with the patient preoperatively, as it facilitates communica-tion intraoperatively. Often, a patient’s family member in the waiting room is called on a speakerphone to give the patient a break from the steady stream of flashcards. This approach helps to renew patient focus and provides additional support.
Cortical mapping can induce seizures. Although most seizures are focal, they have the potential to advance rapidly into general seizures. The reported intraopera-tive seizure incidence varies from 0% to 32%.20 If sei-
zures are encountered, they are treated with ice saline irrigation to the brain until the seizures cease. Most sei-zures, whether focal or general, terminate spontaneously or are terminated by the ice saline irrigation; however, occasionally, seizures continue and become generalized tonic-clonic seizures that necessitate the administration of antiepileptic drugs followed by resedation with pro-pofol and LMA insertion.
When the resection is complete, general anesthesia may be induced and an LMA reinserted. Hemostasis and dural, bone flap, and scalp closure are performed under general anesthesia. Propofol and remifentanil infusions are restarted, with the possible addition of a dexmedeto-midine infusion for patients who are resedated only via total intravenous anesthesia.
Once the procedure is complete, the patient is awak-ened and taken to an overnight postoperative anesthesia care unit or to the intensive care unit, depending on co-morbidities, surgical length, and outcomes.
The Future of Awake CraniotomyResearch has indicated that aggressive resection of certain brain tumors can lengthen survival.21,22 When these tumors arise near eloquent areas of the brain, the only way to confirm the sparing of these highly func-tional areas is to have the patient awake and participating during mapping of the brain. Although there are many promising functional brain mapping techniques that are being refined, such as functional magnetic resonance imaging, positron emission tomography scanning, mag-netoencephalography, intrinsic optical signals, and tran-scranial magnetic stimulation, awake cortical mapping continues to definitively reveal the locations of language and motor centers specific to each patient.
REFERENCES 1. Gupta DK, Chandra PS, Ojha BK, Sharma BS, Mahapatra AK, Mehta
VS. Awake craniotomy versus surgery under general anesthesia for resection of intrinsic lesions of eloquent cortex: a prospective ran-domised study. Clin Neurol Neurosurg. 2007;109(4):335-343.
2. Sarang A, Dinsmore J. Anaesthesia for awake craniotomy: evolution of a technique that facilitates awake neurological testing. Br J Anaesth. 2003;90(2):161-165.
3. Tonn JC. Awake craniotomy for monitoring of language function: benefits and limits [editorial]. Acta Neurochir (Wien). 2007;149(12): 1197-1198.
4. Berkenstadt H, Perel A, Hadani M, Unofrievich I, Ram Z. Monitored anesthesia care using remifentanil and propofol for awake crani-otomy. J Neurosurg Anesthesiol. 2001;13(3):246-249.
5. Kim SS, McCutcheon IE, Suki D, et al. Awake craniotomy for brain tumors near eloquent cortex: correlation of intraoperative cortical mapping with neurological outcomes in 309 consecutive patients. Neurosurgery. 2009;64(5):836-846.
6. Shinokuma T, Shono S, Iwakiri S, Shigematsu K, Higa K. Awake cra-niotomy with propofol sedation and a laryngeal mask airway: a case report [in Japanese]. Masui. 2002;51(5):529-531.
7. Shinoura N, Yoshida M, Yamada R, et al. Awake surgery with con-tinuous motor testing for resection of brain tumors in the primary motor area. J Clin Neurosci. 2009;16(2):188-194.

68 AANA Journal February 2012 Vol. 80, No. 1 www.aana.com/aanajournalonline.aspx
8. Bonhomme V, Franssen C, Hans P. Awake craniotomy. Eur J Anaes-thesiol. 2009;26(11):906-912.
9. Gadhinglajkar S, Sreedhar R, Abraham M. Anesthesia management of awake craniotomy performed under asleep-awake-asleep tech-nique using laryngeal mask airway: report of two cases. Neurol India. 2008;56(1):65-67.
10. Manninen P, Contreras J. Anesthetic considerations for craniotomy in awake patients. Int Anesthesiol Clin. 1986;24(3):157-174.
11. Srejic U. NeuRecipes: The MD Anderson Cancer Center Guide to Anesthe-sia for Neurosurgical Cases. Bloomington, IN: AuthorHouse; 2008.
12. Keifer JC, Dentchev D, Little K, Warner DS, Friedman AH, Borel CO. A retrospective analysis of a remifentanil/propofol general anesthetic for craniotomy before awake functional brain mapping. Anesth Analg. 2005;101(2):502-508, table of contents.
13. Scuplak SM, Smith M, Harkness WF. Air embolism during awake craniotomy. Anaesthesia.1995;50(4):338-340.
14. Almeida AN, Tavares C, Tibano A, Sasaki S, Murata KN, Marino R Jr. Dexmedetomidine for awake craniotomy without laryngeal mask. Arq Neuropsiquiatr. 2005;63(3B):748-750.
15. Ard JL Jr, Bekker AY, Doyle WK. Dexmedetomidine in awake crani-otomy: a technical note. Surg Neurol. 2005;63(2):114-117.
16. Lee EJ, Lee MY, Shyr MH, et al. Adjuvant bupivacaine scalp block facilitates stabilization of hemodynamics in patients undergoing cra-niotomy with general anesthesia: a preliminary report. J Clin Anesth. 2006;18(7):490-494.
17. Osborn I, Sebeo J. “Scalp block” during craniotomy: a classic tech-nique revisited. J Neurosurg Anesthesiol. 2010;22(3):187-194.
18. Geze S, Yilmaz AA, Tuzuner F. The effect of scalp block and local infiltration on the haemodynamic and stress response to skull-pin placement for craniotomy. Eur J Anaesthesiol. 2009;26(4):298-303.
19. De Sloovere V, De Deyne C, Wuyts J, Heylen R. Bispectral index monitoring during asleep-awake technique for craniotomy. Eur J Anaesthesiol. 2009;26(5):443-444.
20. Frost EA, Booij LH. Anesthesia in the patient for awake craniotomy. Curr Opin Anaesthesiol. 2007;20(4):331-335.
21. Ammirati M, Vick N, Liao YL, Ciric I, Mikhael M. Effect of the extent of surgical resection on survival and quality of life in patients with supratentorial glioblastomas and anaplastic astrocytomas. Neurosur-gery. 1987;21(2):201-206.
22. Berger MS, Deliganis AV, Dobbins J, Keles GE. The effect of extent of resection on recurrence in patients with low grade cerebral hemi-sphere gliomas. Cancer. 1994;74(6):1784-1791.
AUTHORSGarry Brydges, CRNA, DNP, ACNP-BC, is chief nurse anesthetist in the Department of Anesthesiology & Perioperative Medicine at University of Texas (UT) MD Anderson Cancer Center, Houston, Texas. Email: gbrydges @mdanderson.org.
Roxanne Atkinson, CRNA, MSN, is manager of nurse anesthesia at UT MD Anderson Cancer Center.
Monie James Perry, CRNA, MSN, is a nurse anesthesia clinician at UT MD Anderson Cancer Center.
Darline Hurst, CRNA, is a nurse anesthesia clinician at UT MD Ander-son Cancer Center.
Travis Laqua, CRNA, MSN, is a nurse anesthesia clinician at UT MD Anderson Cancer Center.
John Wiemers, CRNA, MSN, is a nurse anesthesia clinician at UT MD Anderson Cancer Center.
ACKNOWLEDGMENTSWe thank the following staff at UT MD Anderson Cancer Center for their contributions to the course: Sarah Goss, CRNA, MSN, nurse anesthesia clinician; David Z. Ferson, MD, faculty-professor; Charles E. Cowles Jr, MD, faculty-assistant professor; Anh-Thuy Nguyen, MD, faculty-associate professor; Dave Aten, MA, CMI, senior medical illustrator; Dawn Chalaire, BA, scientific editor, Department of Scientific Publications.