Embed Size (px)
Citation preview

AII
�emica
�ctMd
�Mucsaira
�ubc
K���
AEi
C
TP
CD
J
A
1r
PEER-REVIEW REPORTS
W
wake Craniotomy, Electrophysiologic Mapping, and Tumor Resection With High-Fieldntraoperative MRI
an F. Parney1, Stephan J. Goerss1, Kiaran McGee2, John Huston III2, William J. Perkins3, Frederic B. Meyer1I
Amfqt(saiqtHhshqd
seilwafstpiaei
C
AsaspcaubcH
T
RltstssodFautf878-8750/$ - see front matter © 2010 Elsevier Inc. All
ights reserved.
ORLD NEUROSURGERY 73 [5]: 547-55
NTRODUCTION
wake craniotomy and electrophysiologicapping (EPM) are established techniques to
acilitate safe resection of lesions near elo-uent cortex (14, 15). High-field (�1.5 T) in-
raoperative magnetic resonance imagingiMRI) is an attractive strategy to enable exten-ive glioma resection (2, 11). Combining EPMnd iMRI would be a potent technique to facil-tate safe, extensive glioma resection near elo-uent cortex. This was first reported more
han 10 years ago using low-field iMRI (3).owever, techniques for combining EPM andigh-field iMRI have only recently been de-cribed (7, 18). The delay in applying EPM toigh-field iMRI may reflect the draping re-uired to maintain a sterile field during inter-
electrophysiologic mapping (EPM) is ann of near eloquent cortex. Intraoperativeasingly used to aid in the resection ofls in high-field iMRI units make awakehave previously reported combined EPM
ase describing a simple technique forigh-field iMRI. A movable platter is usedo a transport trolley and into the adjacental position. This system allows excessiotomy.
n presented with new onset seizures.large left temporal mass. The patient
iotomy. The EPM demonstrated a singleyrus. After an initial tumor debulking, thend was covered with additional drapes,trimmed. An iMRI was obtained. Thed the patient was redraped. Additionalmoval of what proved to be an anaplastic
ithout any new neurological deficits.
sitioning and draping in high-field iMRIThis straightforward technique for com-fe removal of large lesions in eloquent
issection imaging. In many high-field iMRI p
1, MAY 2010 ww
ystems, patients’ heads and upper bodies aressentially “cocooned” in sterile drapes dur-ng intradissection imaging (17). This is prob-ematic for awake craniotomies due to issues
ith both patient comfort (claustrophobia forlert patients) and safety (airway protectionor sedated patients). In this report, we de-cribe a simple minimal draping techniquehat enables intradissection imaging to beerformed easily and safely in a high-field
MRI and still maintaining sterility. This hasllowed us to combine awake craniotomy andlectrophysiologic mapping with high-fieldMRI.
ASE REPORT
57-year-old right hand-dominant man pre-ented with generalized tonic clonic seizuresnd one episode of transient expressivepeech arrest. His neurological and generalhysical examination between seizures wasompletely normal. The MRI scans showedlarge mass in his left temporal lobe. Henderwent an uncomplicated stereotacticiopsy at another institution that dis-losed an anaplastic astrocytoma (Worldealth Organization grade 3).
ECHNIQUE
epeat MRI at our institution showed a simi-ar tumor, although new edema was seen athe biopsy site (Figure 1A). A functional MRIhowed bilateral activation for speech in bothhe frontal and temporal lobes, suggestingome language reorganization (data nothown). The patient was taken to a dedicatedperating room for iMRI adjacent to a stan-ard 1.5-T MRI scanner (General Electric,airfield, CT, USA) (Figure 2A). This systemllows standard ferromagnetic tools to besed in the operating room (with the excep-
ion of the head holder, which must be non-erromagnetic). A mobile patient transfer
BACKGROUND: Awake craniotomy andstablished technique to facilitate the resectioagnetic resonance imaging (iMRI) is incre
ntracranial lesions. Standard draping protocoraniotomies challenging, and only two groupsnd high-field iMRI.
METHODS: We present an illustrative combining awake craniotomy and EPM with h
o transfer the patient from the operating table tRI and still maintaining the patient’s surgic
rapes to be removed, facilitating awake cran
RESULTS: A 57-year-old right-handed maagnetic resonance imaging demonstrated a
nderwent an awake, left frontotemporal cranritical area for speech in his inferior frontal gcalp flap was loosely approximated, the wound the excess surrounding drapes weremage-guidance system was re-registered anesection was performed, allowing extensive restrocytoma. The patient tolerated this well w
CONCLUSIONS: Standard protocols for ponits make awake craniotomies problematic.ined awake EPM and iMRI may facilitate saortex.
ey wordsAwake craniotomyElectrophysiologic mappingHigh-field intraoperative MRI
bbreviations and AcronymsPM: Electrophysiologic mapping
MRI: Intraoperative magnetic resonance imaging
From the Departments of 1Neurologic Surgery,2Radiology, and 3Anesthesiology, Mayo Clinic
ollege of Medicine, Rochester, Minnesota, USA
o whom correspondence should be addressed: Ian F.arney, M.D., Ph.D. [E-mail: [email protected]]
itation: World Neurosurg. (2010) 73, 5:547-551.OI: 10.1016/j.wneu.2010.02.003
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
latter attached to the operating table allows
w.WORLDNEUROSURGERY.org 547

tiTtirt
mswtwtM
SSTepaptpmlsts
Flt
5dpbastMlo
PEER-REVIEW REPORTS
IAN F. PARNEY ET AL. AWAKE CRANIOTOMY IN HIGH-FIELD MRI
5
he patient to be moved to a transport trolleyn pinions without any change in positioning.hey are transferred approximately 20 feet to
he adjacent multipurpose MRI scanner formaging before returning to the operatingoom. The scanning room is separated fromhe operating room by retractable doors.
After moderate intravenous sedation (dex-edetomidine) and generous local anesthe-
ia (bupivacaine), he was positioned supineith a role placed under the left shoulder and
he head turned slightly to the left. The headas held in place with nonferromagnetic
hree-point pin fixation. The preoperative
T2
T1
A
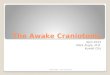
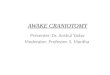
Figure 1. (A) Preoperative T1 and T2 afteshowing a predominantly nonenhancinghyperintense mass in the medial left teenhancement (thick arrow) is seen, alonbiopsy tract (thin arrows) and some edebiopsy site. (B) Interdissection magneticshowing residual tumor (arrows). (C) Poresonance imaging showing an extensivresidual tumor was deliberately left adjavessels and in the most posterior and sparahippocampal gyrus.
RI was registered to the patient using a m
48 www.SCIENCEDIRECT.com
TEALTH image guidance system (Stealth-tation, Medtronic, Minneapolis, MN, USA).his included functional MRI sequences forxpressive speech. The operative field wasrepped and draped in the standard fashionnd a left frontotemporal craniotomy waserformed. After opening the dura, the pa-
ient’s sedation was lightened and electro-hysiologic stimulation motor and speechapping was performed using a 5-mm bipo-
ar electrode as described elsewhere (14, 15). Aingle, critical area for speech where stimula-ion caused naming and counting arrest waseen in the posterior inferior frontal gyrus and
T1
T2
T1
T2
B
C
trast axial imagespointense/T2l lobe. A small area ofh the stereotacticrrowhead) next to thenance imagingrative magneticection. Some minorto the middle cerebralr aspect of the
arked with a sterile letter “E” (“English”; t
WORLD NEUROSURGE
igure 2B). Interestingly, this did not corre-ate exactly with critical areas for speech iden-ified by functional MRI (Figure 2C).
An anterior temporal lobectomy extendingcm from the temporal pole and initial tumorebulking was performed. At the end of thisrocedure, a large resection cavity was createdut the tumor was still present superomedi-lly and posteriorly. The sylvian fissure hadhifted 1 cm inferiorly from its position iden-ified by STEALTH using the preoperative
RI, suggesting that image guidance was noonger accurate. Accordingly, we choose tobtain an interdissection MRI and re-register
r conT1 hy
mporag witma (areso
stopee rescentuperio
he STEALTH system. This was done to iden-
RY, DOI:10.1016/j.wneu.2010.02.003

ttgro6s
cttkau
smTawi
ed by
PEER-REVIEW REPORTS
IAN F. PARNEY ET AL. AWAKE CRANIOTOMY IN HIGH-FIELD MRI
W
ify the exact location and extent of residualumor and facilitate further safe image-uided resection. The scalp flap was looselyeapproximated. Sterile sponges were placedver the wound and an approximately 60 �0-cm sterile drape was placed over the
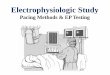
Figure 2. (A) Schematic showing the operating taplatter, and transfer trolley. (B) Intraoperative phelectrophysiologic mapping. A single critical areainferior frontal gyrus is marked with the letter “Eprior stereotactic biopsy is seen in the temporalIntraoperative screen shot from image-guidancearrow) placed on the critical speech area identifi
ponges and secured with a large adhesive l
ORLD NEUROSURGERY 73 [5]: 547-55
lear plastic drape. The excess drapes wererimmed to allow the patient to be transferredo the MRI table (Figure 2D). The patient wasept in position with three-point pin fixationnd brought into the adjacent MRI scannersing the transfer platter and transport trol-
atient transferph afterpeech found in thee entry point for the(arrow). (C)m with probe (blueelectrophysiologic
mapping. Note that thiidentified by functiona(D) Drapes before intea 60 � 60-cm sterile ddrape. The anterior MRExcess surrounding drpatient’s face.
ey. An interdissection MRI was obtained, t
1, MAY 2010 ww
howing the expected residual tumor supero-edially and posteromedially (Figure 1B).
he patient was removed from the scannernd returned to the adjacent operating roomhere he was transferred back to the operat-
ng table, still maintaining his position with
pproximately 1 cm from speech areasetic resonance imaging (MRI) (white pixels).
ction MRI. The wound has been covered withecured with a large, adhesive clear plastichas been similarly secured on top of this.ave been trimmed to give easy access to the
ble, potografor s.” Thlobesyste
s is al magnrdisserape sI coil
apes h
hree-point pin fixation. He remained alert
w.WORLDNEUROSURGERY.org 549

apttdtm
rumdtgfNwcaoehwpccsvm
D
Pam2iqpgpmaclmemtlsdmmt
h
dms(rahaaaristgtamsoimtaaiawa
atihki2ttfifihimfspitctpcipd
ead
atgrovseeotplEtt
R
PEER-REVIEW REPORTS
IAN F. PARNEY ET AL. AWAKE CRANIOTOMY IN HIGH-FIELD MRI
5
nd comfortable throughout this imagingrocess. The interdissection MRI was regis-
ered to the patient using the STEALTH sys-em. This entire process (partial closure,raping, imaging, redraping, re-registering
he STEALTH system) took approximately 40inutes.The patient was redraped and additional
esection was performed with the aid of thepdated image-guidance system. Some tu-or was deliberately not resected superome-
ially next to the middle cerebral artery and inhe posterior aspect of the parahippocampalyrus where the patient became mildly con-used when we began to work in this area.evertheless, an extensive resection (�90%)as performed. The patient’s wound was
losed, he was removed from pin fixation, andfull head dressing was applied. A final post-perative MRI was obtained confirming thextent of the resection (Figure 1C). The patientad an unremarkable postoperative courseith no new neurological deficits. The finalathological diagnosis was anaplastic astro-ytoma (World Health Organization grade 3),onfirming the results of his earlier biopsyample. He has subsequently received adju-ant external beam radiation and temozolo-ide chemotherapy.
ISCUSSION
enfield and Boldrey (13) first describedwake craniotomy and electrophysiologicapping more than 70 years ago. In the past
0 years, this technique has become increas-ngly applied for glioma resection near elo-uent cortex (14, 15). Although motor map-ing can be performed with patients receivingeneral anesthetic, speech mapping must beerformed awake. Image guidance using fra-eless stereotaxy based on preoperative im-
ging is another established technique to fa-ilitate extensive resection of intracranialesions. This is helpful for planning cranioto-
ies, finding lesions, and determining thextent of resection intraoperatively. Deter-ining the extent of resection is potentially
he most valuable, but is also the most chal-enging. As the tumor is removed, the brainhifts (6), causing significant inaccuracies toevelop in image-guidance systems. This isost likely to occur in patients with large tu-ors (�3 cm in diameter) or tumors adjacent
o the ventricles (1).Intraoperative MRI has been proposed to
elp address this issue. Unlike most clinical d
50 www.SCIENCEDIRECT.com
iagnostic MRI scanners that use high-fieldagnets (1.5 T), the first generation of iMRI
canners used low-field magnets (0.2 to 0.5 T)4, 8). Although useful, the image quality waseduced compared with standard MRI. As anlternative, high-field (�1.5 T) iMRI systemsave been developed that produce quality im-ges (9, 17). Importantly, re-registering im-ge-guidance systems with high-field iMRIppears to facilitate more extensive but safeesection compared with low-field iMRI andmage guidance (2). Functional imaging,uch as diffusion tensor imaging and func-ional MRI, can be incorporated into image-uidance systems, but brain shift makes in-
erpretation difficult as resection proceedsnd questions remain about how closely theseodalities replicate EPM (the accepted gold
tandard) (11, 10). This was demonstrated inur patient, when the critical area for speech
dentified by EPM was shown to be approxi-ately 1 cm away from any speech areas iden-
ified on functional MRI. Diffusion tensor im-ging could be obtained intraoperatively toddress this issue (12). It may be possible toncorporate intraoperative functional MRI forwake patients in the future as well, but thisould clearly need to be balanced against the
mount of time required during craniotomy.Thus, combined EPM, image guidance,
nd high-field iMRI may be an ideal techniqueo facilitate safe extensive resection of lesionsn eloquent cortex. Despite the availability ofigh-field iMRI for more than a decade, to ournowledge no reports combining high-field
MRI with EPM appeared in the literature until009 (7, 18). There may be several reasons forhis, but it may reflect standard draping pro-ocols for interdissection imaging in a high-eld iMRI environment. To keep the sterileeld from contamination, the patient’s entireead and upper body are essentially wrapped
n sterile drapes (17). This creates an environ-ent that is either extremely claustrophobic
or alert patients or potentially suffocating foredated patients without definitive airwayrotection. Our simple draping technique for
nterdissection imaging is much less restric-ive and makes awake craniotomy much lesshallenging. This technique is facilitated byhe transfer platter and trolley that allow theatient to be transferred to and from the adja-ent MRI scanner in pinions without chang-ng the surgical position. The two earlier re-orts of combined EPM and high-field iMRIo not describe the draping protocols for inter-
issection imaging in detail, although NabaviWORLD NEUROSURGE
t al. (7) suggest uncovering the patient’s facend Weingarten et al. (18) describe trimmingrapes hanging below the operating table.
Additional experience with more patientsnd longer follow-up is necessary to defini-ively address outcomes for patients under-oing awake craniotomy, EPM, and gliomaesection aided by high-field iMRI. The rolef cytoreductive surgery in prolonging sur-ival in patients with gliomas still remainsomewhat controversial as only level 2vidence is available at present (5, 16). Nev-rtheless, most neurosurgeons and neuro-ncologist agree that maximal safe resec-
ion is appropriate for newly diagnosedatients. We believe that simple techniques
ike ours for combining awake craniotomy,PM, and high-field iMRI may be an impor-
ant step in facilitating maximal safe resec-ion for large gliomas in eloquent cortex.
EFERENCES
1. Benveniste RJ, Germano IM: Correlation of factorspredicting intraoperative brain shift with successfulresection of malignant brain tumors using image-guided techniques. Surg Neurol 63:542-548 [dis-cussion: 548-549], 2005.
2. Bergsneider M, Sehati N, Villablanca P, McArthurDL, Becker DP, Liau LM: Mahaley Clinical ResearchAward: extent of glioma resection using low-field(0.2 T) versus high-field (1.5 T) intraoperative MRIand image-guided frameless neuronavigation. ClinNeurosurg 52:389-399, 2005.
3. Black PM, Alexander E 3rd, Martin C, Moriarty T,Nabavi A, Wong TZ, Schwartz RB, Jolesz F: Craniot-omy for tumor treatment in an intraoperative mag-netic resonance imaging unit. Neurosurgery45:423-431 discussion: 431-433, 1999.
4. Black PM, Moriarty T, Alexander E 3rd, Stieg P,Woodard EJ, Gleason PL, Martin CH, Kikinis R,Schwartz RB, Jolesz FA: Development and imple-mentation of intraoperative magnetic resonanceimaging and its neurosurgical applications. Neuro-surgery 41:831-842 discussion: 842-845, 1997.
5. Laws ER, Parney IF, Huang W, Anderson F, MorrisAM, Asher A, Lillehei KO, Bernstein M, Brem H,Sloan A, Berger MS, Chang S: Survival followingsurgery and prognostic factors for recently diag-nosed malignant glioma: data from the Glioma Out-comes Project. J Neurosurg 99:467-473, 2003.
6. Nabavi A, Black PM, Gering DT, Westin CF, MehtaV, Pergolizzi RS Jr, Ferrant M, Warfield SK, Hata N,Schwartz RB, Wells WM 3rd, Kikinis R, Jolesz FA:Serial intraoperative magnetic resonance imagingof brain shift. Neurosurgery 48:787-797 discussion:797-798, 2001.
7. Nabavi A, Goebel S, Doerner L, Warneke N, UlmerS, Mehdorn M: Awake craniotomy and intraopera-
RY, DOI:10.1016/j.wneu.2010.02.003

1
1
1
1
1
1
1
1
r
CD
J
A
1
PEER-REVIEW REPORTS
IAN F. PARNEY ET AL. AWAKE CRANIOTOMY IN HIGH-FIELD MRI
W
tive magnetic resonance imaging: patient selection,preparation, and technique. Top Magn Reson Imag-ing 19:191-196, 2009.
8. Nimsky C, Ganslandt O, Tomandl B, Buchfelder M,Fahlbusch R: Low-field magnetic resonance imag-ing for intraoperative use in neurosurgery: a 5-yearexperience. Eur Radiol 12:2690-2703, 2002.
9. Nimsky C, Ganslandt O, Fahlbusch R: Comparing0.2 tesla with 1.5 tesla intraoperative magnetic res-onance imaging analysis of setup, workflow, andefficiency. Acad Radiol 12:1065-1079, 2005.
0. Nimsky C, Ganslandt O, Hastreiter P, Wang R, Ben-ner T, Sorensen A, Fahlbusch R: Intraoperative dif-fusion-tensor MR imaging: shifting of white mattertracts during neurosurgical procedures—initial ex-perience. Radiology 234:218-225, 2005.
1. Nimsky C, Ganslandt O, Buchfelder M, Fahlbusch
R: Intraoperative visualization for resection of gli-omas: the role of functional neuronavigation and1
ORLD NEUROSURGERY 73 [5]: 547-55
intraoperative 1.5 T MRI. Neurol Res 28:482-487,2006.
2. Nimsky C, Ganslandt O, Hastreiter P, Wang R, Ben-ner T, Sorensen AG, Fahlbusch R: Preoperative andintraoperative diffusion tensor imaging-based fibertracking in glioma surgery. Neurosurgery 61(1Suppl):178-185 discussion: 186, 2007.
3. Penfield W, Boldrey E: Somatic motor and sensoryrepresentation in the cerebral cortex of man as stud-ied by electrical stimulation. Brain 60:389-443,1937.
4. Ojemann G, Ojemann J, Lettich E, Berger M: Corti-cal language localization in left, dominant hemi-sphere. An electrical stimulation mapping investi-gation in 117 patients. J Neurosurgery 71:316-326,1989.
5. Sanai N, Mirzadeh Z, Berger MS: Functional out-come after language mapping for glioma resection.N Engl J Med 358:18-27, 2008.
6. Stummer W, Pichlmeier U, Meinel T, Wiestler OD,Zanella F, Reulen HJ: Fluorescence-guided surgery r
1, MAY 2010 ww
with 5-aminolevulinic acid for resection of malig-nant glioma: a randomised controlled multicentrephase III trial. Lancet Oncol 7:392-401, 2006.
7. Sutherland GR, Kaibara T, Louw D, Hoult DI, To-manek B, Saunders J: A mobile high-field magneticresonance system for neurosurgery. J Neurosurg 91:804-813, 1999.
8. Weingarten DM, Asthagiri AR, Butman JA, Sato S,Wiggs EA, Damaska B, Hess JD: Cortical mappingand frameless stereotactic navigation in the high-field intraoperative magnetic resonance imagingsuite. J Neurosurg 111:1185-1190, 2009.
eceived 16 July 2009; accepted 30 January 2010
itation: World Neurosurg. (2010) 73, 5:547-551.OI: 10.1016/j.wneu.2010.02.003
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
878-8750/$ - see front matter © 2010 Elsevier Inc. All rights
eserved.w.WORLDNEUROSURGERY.org 551