Embed Size (px)
Citation preview

The Plans of Choice forMedicare SupplementalCoverage
Blue Cross ofCalifornia
ClaimFree® Standard Plan A Medicare Supplement Plan
Blue Cross Senior ClassicSM C Medicare Supplement Plan
Blue Cross Senior Classic F Medicare Supplement Plan
Blue Cross Senior Classic I Medicare Supplement Plan
Blue Cross Senior Classic J Medicare Supplement Plan

MEDICARE AND BLUE CROSSBOTH SIDES OF THE STORY
When it comes to Medicare, it’s important that youknow both sides of the story, and understand theadvantages and disadvantages of relying solely onMedicare to provide for your health care needs.
Though Medicare covers many health care costs,there are many medical services that Medicare doesnot cover. This point is clearly made in the "Guide toHealth Insurance for People with Medicare," whichis published yearly by the Centers for Medicare &Medicaid Services (CMS) of the U.S. Department ofHealth and Human Services. As the guidebooksuggests, "There are health care costs that Medicareeither does not pay in full or does not pay at all. Ifyou need or want services not covered by Medicare,you must pay the bill." To help fill the gaps in yourMedicare coverage, you have the option of buyingsupplemental insurance policies known as "Medigap"plans. Our ClaimFree Standard Plan A MedicareSupplement Plan, Blue Cross Senior Classic CMedicare Supplement Plan; Blue Cross SeniorClassic F Medicare Supplement Plan; Blue CrossSenior Classic I Medicare Supplement Plan; andBlue Cross Senior Classic J Medicare SupplementPlan are supplement plans that help pay the billsMedicare does not, and provide you with protectionfrom the ever-increasing gaps in Medicare.
Why should I consider buying supplementalinsurance?
Before Medicare will pay for any of the medical servicesyou want or need, you must first pay Medicare'sdeductibles. When combined with the coinsurance youare also required to pay, you may be out hundreds, eventhousands of dollars before any benefits are paid byMedicare! These are bills you are expected to pay.
The Advantages Are Yours With:! Blue Cross Senior Classic C Medicare
Supplement Plan! Blue Cross Senior Classic F Medicare
Supplement Plan! Blue Cross Senior Classic I Medicare
Supplement Plan! Blue Cross Senior Classic J Medicare
Supplement Plan
! Freedom to use the doctor of your choice,including nearly 50,000 Prudent Buyer® Physiciansand specialists.
! Freedom to use the hospital of your choice,including more than 300 Participating Hospitals.
! Pays all Medicare deductibles.*
! Coverage for Skilled Nursing FacilityCoinsurance.
! Benefits for Medicare Part A and B Coinsurance.
! Benefits for Foreign Travel Emergency.
! Full conventional Medicare benefits at allproviders, inside and outside California — anywhere in the U.S.
! You get to keep your Medicare card and yourright to basic Medicare benefits too!
Blue Cross Senior Classic C Medicare SupplementPlan, Blue Cross Senior Classic F MedicareSupplement Plan, Blue Cross Senior Classic IMedicare Supplement Plan and Blue Cross SeniorClassic J Medicare Supplement Plan are Medicare SELECT plans.
*Pays the Medicare Part A $992 deductible. Pays the Medicare Part B $131 annual deductible only when you use aParticipating Prudent Buyer Provider. Part B deductible is covered when using a non-participating provider inlimited circumstances, including emergency care. Medicare Part B deductible not covered for Blue Cross SeniorClassic I Medicare Supplement Plan.

1
FREEDOM OF CHOICE
You’ve earned the right to have a choice of the doctoror hospital you want to use, and we respect thatright. Our ClaimFree Standard Plan A MedicareSupplement Plan, Blue Cross Senior Classic CMedicare Supplement Plan, Blue Cross SeniorClassic F Medicare Supplement Plan, Blue CrossSenior Classic I Medicare Supplement Plan andBlue Cross Senior Classic J Medicare SupplementPlan offer you access to the Prudent Buyer network,as well as any Medicare-participating physician andany Medicare-approved hospital in the state. You arecovered whether or not you use a Prudent BuyerPhysician.
PRUDENT BUYER NETWORK OFPARTICIPATING DOCTORS AND HOSPITALS
The Prudent Buyer network offers you the choice of awide variety of physicians and hospitals convenientlylocated throughout the state to help you with all ofyour health care needs. This is the largest network inCalifornia, with over one half of all physicians andhospitals in the state being Participating PrudentBuyer Providers. Nearly 50,000 physicians and morethan 300 hospitals are Participating Prudent BuyerProviders, so there’s a good chance that your currentphysician or hospital is already a member of ournetwork.
PROTECTION AGAINST EXCESS CHARGES
Under Part B of Medicare, you could have out-of-pocket costs if your physician or medical supplierdoes not accept assignment of your Medicare claimand charges more than Medicare’s approved amount.The difference to be paid is called the ‘excesscharge.’
Blue Cross Senior Classic F Medicare SupplementPlan, Blue Cross Senior Classic I MedicareSupplement Plan and Blue Cross Senior Classic JMedicare Supplement Plan can save you theexpense and worry about paying significant out-of-pocket costs because of gaps in Medicare. When youutilize Blue Cross of California’s Prudent Buyernetwork, your doctor’s charges for Medicare’scovered services are paid in full, and most plans alsocover the Medicare Part B deductible.* Even if youreceive medical services from a provider that is not amember of the Prudent Buyer network, your doctor’scharges for Medicare’s covered services are still paidin full, except for the Medicare Part B $131deductible, except in limited circumstances,including emergency care.
CLAIMFREE® SERVICE
You may never have to fill out another claim formever again. Blue Cross of California has created away to put an end to the frustration caused byburdensome and tedious claim forms. It’s calledClaimFree service, and we are the only health carrierin the state that provides you with this worry-freeautomatic claims payment service for both Parts Aand B of Medicare.
The way it works is simple. When providers billMedicare, a computerized display of the informationis automatically sent to Blue Cross of California forprocessing. We then pay your doctor or hospitaldirectly. This results in your medical bills beingprocessed faster and more accurately.
* Blue Cross Senior Classic I Medicare Supplement Plan covers ‘excess charges’ but not the Medicare Part B $131 deductible.
2
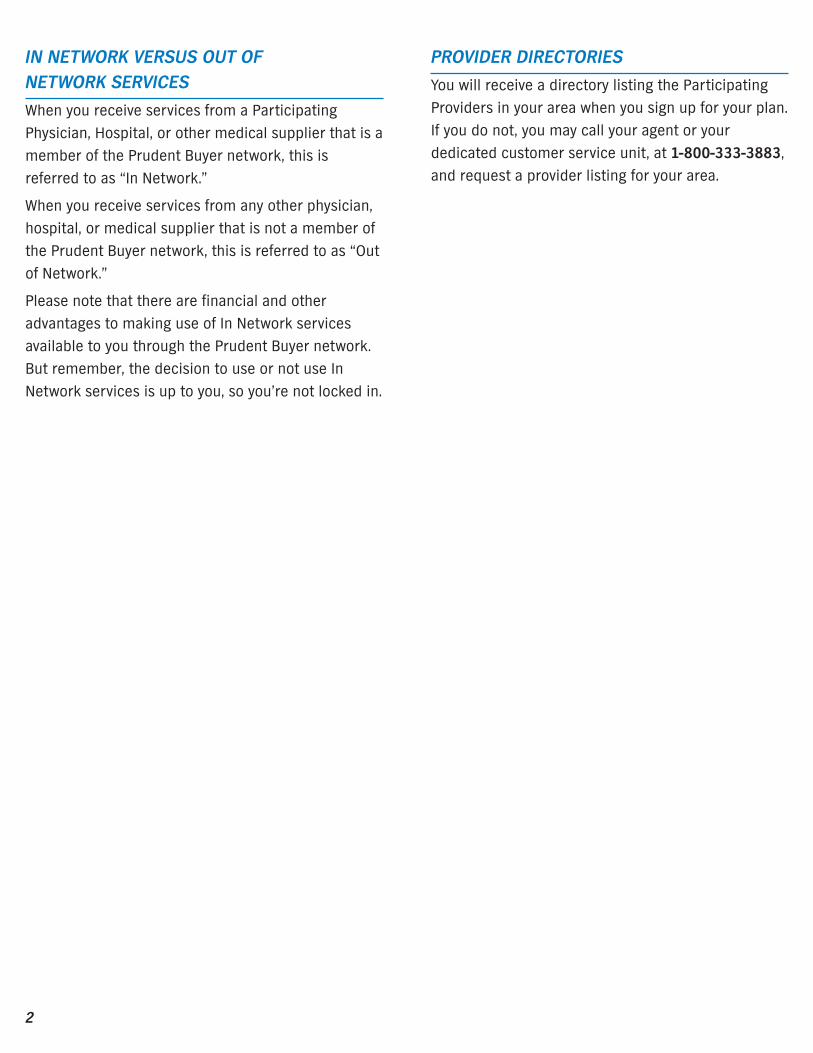
IN NETWORK VERSUS OUT OF NETWORK SERVICES
When you receive services from a ParticipatingPhysician, Hospital, or other medical supplier that is amember of the Prudent Buyer network, this isreferred to as “In Network.”
When you receive services from any other physician,hospital, or medical supplier that is not a member ofthe Prudent Buyer network, this is referred to as “Outof Network.”
Please note that there are financial and otheradvantages to making use of In Network servicesavailable to you through the Prudent Buyer network.But remember, the decision to use or not use InNetwork services is up to you, so you’re not locked in.
PROVIDER DIRECTORIES
You will receive a directory listing the ParticipatingProviders in your area when you sign up for your plan.If you do not, you may call your agent or yourdedicated customer service unit, at 1-800-333-3883,and request a provider listing for your area.

3
Blue Cross of California products aredesigned to meet the health coverageneeds of people who are enrolled in bothParts A and B of Medicare. Plus, youreceive the following benefits:
! Affordable monthly plan premiums.
! No annual maximums for Medicare-covered services.
! Guaranteed renewable.
! ClaimFree processing for all Medicareclaims.
! Toll-free dedicated customer servicephone number: 1-800-333-3883.
FIVE GREAT PLANS – CHOOSE THE PLAN THATBEST MEETS YOUR NEEDS
ClaimFree StandardPlan A MedicareSupplement Plan
Blue Cross SeniorClassic C MedicareSupplement Plan
Blue Cross SeniorClassic F MedicareSupplement Plan
Blue Cross SeniorClassic I MedicareSupplement Plan
Blue Cross SeniorClassic J MedicareSupplement Plan
1
23
45
4
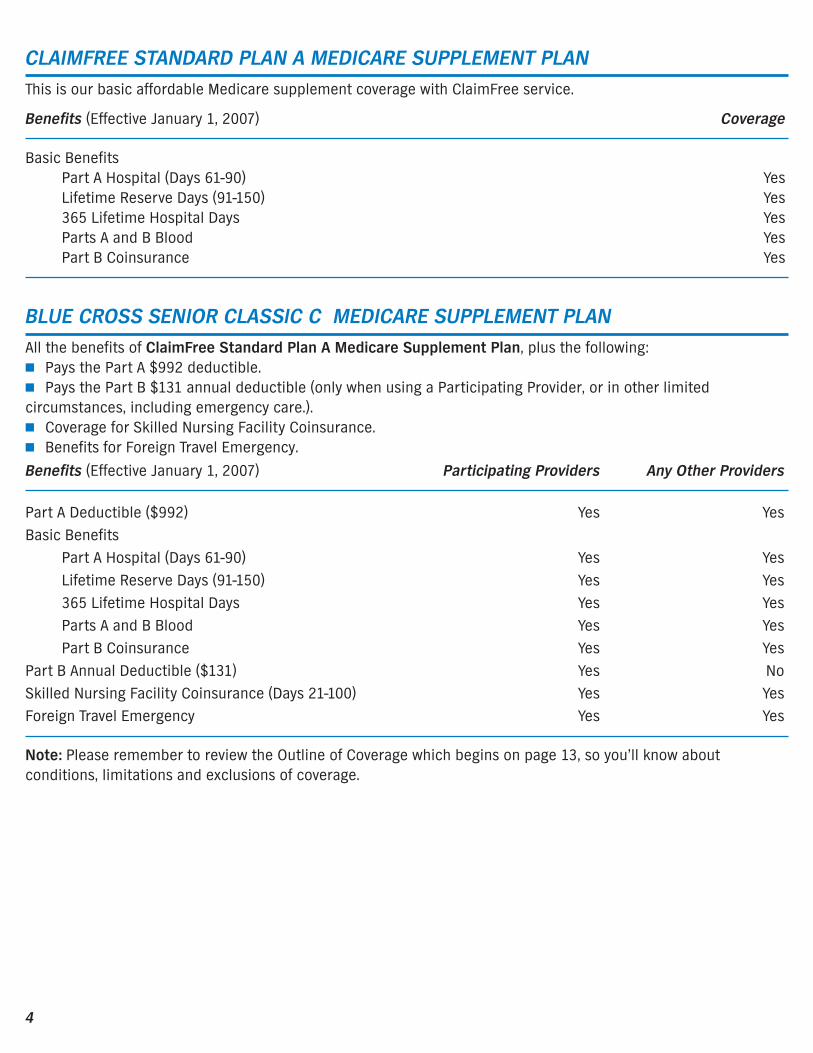
CLAIMFREE STANDARD PLAN A MEDICARE SUPPLEMENT PLANThis is our basic affordable Medicare supplement coverage with ClaimFree service.
Benefits (Effective January 1, 2007) Coverage
Basic BenefitsPart A Hospital (Days 61-90) YesLifetime Reserve Days (91-150) Yes365 Lifetime Hospital Days YesParts A and B Blood YesPart B Coinsurance Yes
BLUE CROSS SENIOR CLASSIC C MEDICARE SUPPLEMENT PLANAll the benefits of ClaimFree Standard Plan A Medicare Supplement Plan, plus the following:! Pays the Part A $992 deductible.! Pays the Part B $131 annual deductible (only when using a Participating Provider, or in other limitedcircumstances, including emergency care.).! Coverage for Skilled Nursing Facility Coinsurance.! Benefits for Foreign Travel Emergency.
Benefits (Effective January 1, 2007) Participating Providers Any Other Providers
Part A Deductible ($992) Yes YesBasic Benefits
Part A Hospital (Days 61-90) Yes YesLifetime Reserve Days (91-150) Yes Yes365 Lifetime Hospital Days Yes YesParts A and B Blood Yes YesPart B Coinsurance Yes Yes
Part B Annual Deductible ($131) Yes NoSkilled Nursing Facility Coinsurance (Days 21-100) Yes YesForeign Travel Emergency Yes Yes
Note: Please remember to review the Outline of Coverage which begins on page 13, so you’ll know aboutconditions, limitations and exclusions of coverage.
5
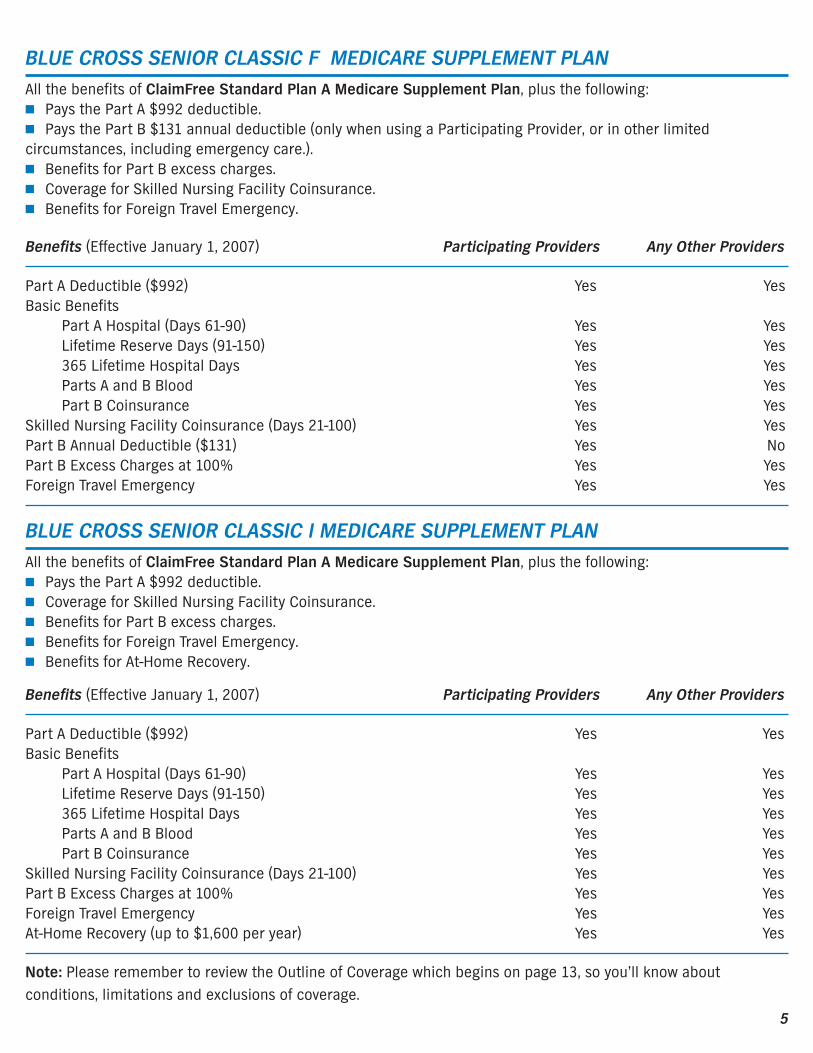
BLUE CROSS SENIOR CLASSIC F MEDICARE SUPPLEMENT PLANAll the benefits of ClaimFree Standard Plan A Medicare Supplement Plan, plus the following:! Pays the Part A $992 deductible.! Pays the Part B $131 annual deductible (only when using a Participating Provider, or in other limitedcircumstances, including emergency care.).! Benefits for Part B excess charges.! Coverage for Skilled Nursing Facility Coinsurance.! Benefits for Foreign Travel Emergency.
Benefits (Effective January 1, 2007) Participating Providers Any Other Providers
Part A Deductible ($992) Yes YesBasic Benefits
Part A Hospital (Days 61-90) Yes YesLifetime Reserve Days (91-150) Yes Yes365 Lifetime Hospital Days Yes YesParts A and B Blood Yes YesPart B Coinsurance Yes Yes
Skilled Nursing Facility Coinsurance (Days 21-100) Yes YesPart B Annual Deductible ($131) Yes NoPart B Excess Charges at 100% Yes YesForeign Travel Emergency Yes Yes
BLUE CROSS SENIOR CLASSIC I MEDICARE SUPPLEMENT PLANAll the benefits of ClaimFree Standard Plan A Medicare Supplement Plan, plus the following:! Pays the Part A $992 deductible.! Coverage for Skilled Nursing Facility Coinsurance.! Benefits for Part B excess charges.! Benefits for Foreign Travel Emergency.! Benefits for At-Home Recovery.
Benefits (Effective January 1, 2007) Participating Providers Any Other Providers
Part A Deductible ($992) Yes YesBasic Benefits
Part A Hospital (Days 61-90) Yes YesLifetime Reserve Days (91-150) Yes Yes365 Lifetime Hospital Days Yes YesParts A and B Blood Yes YesPart B Coinsurance Yes Yes
Skilled Nursing Facility Coinsurance (Days 21-100) Yes YesPart B Excess Charges at 100% Yes YesForeign Travel Emergency Yes YesAt-Home Recovery (up to $1,600 per year) Yes Yes
Note: Please remember to review the Outline of Coverage which begins on page 13, so you’ll know aboutconditions, limitations and exclusions of coverage.
6
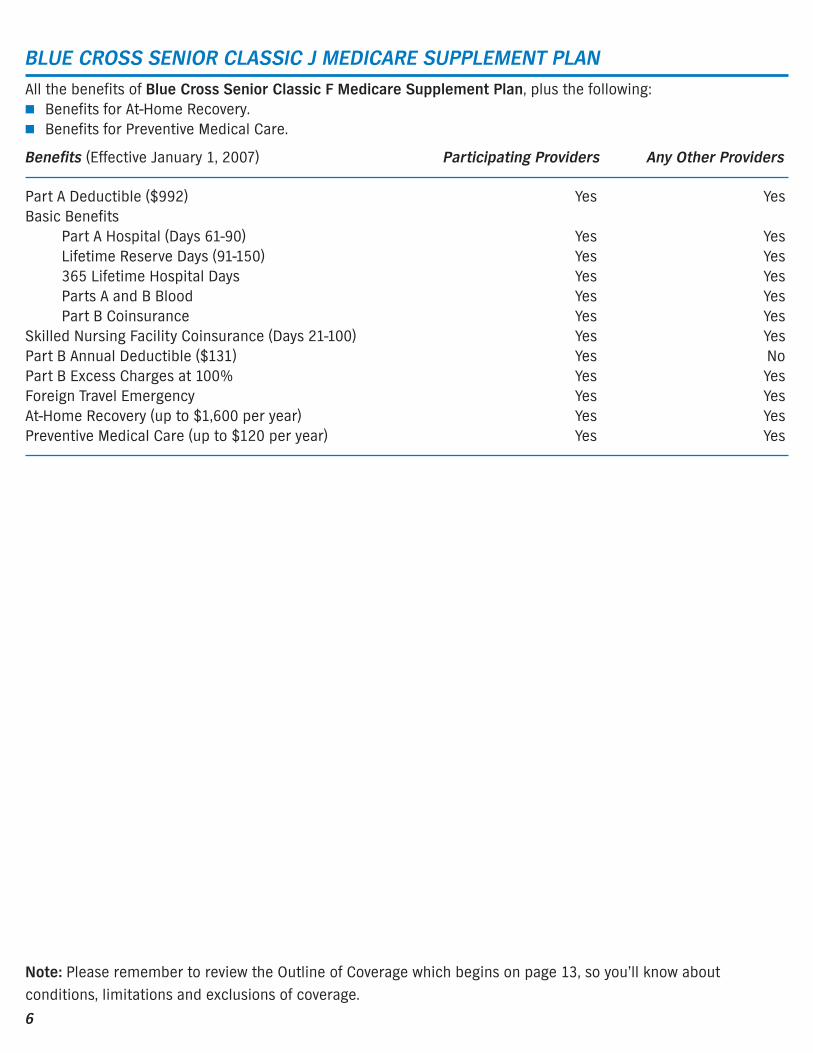
BLUE CROSS SENIOR CLASSIC J MEDICARE SUPPLEMENT PLANAll the benefits of Blue Cross Senior Classic F Medicare Supplement Plan, plus the following:! Benefits for At-Home Recovery.! Benefits for Preventive Medical Care.
Benefits (Effective January 1, 2007) Participating Providers Any Other Providers
Part A Deductible ($992) Yes YesBasic Benefits
Part A Hospital (Days 61-90) Yes YesLifetime Reserve Days (91-150) Yes Yes365 Lifetime Hospital Days Yes YesParts A and B Blood Yes YesPart B Coinsurance Yes Yes
Skilled Nursing Facility Coinsurance (Days 21-100) Yes YesPart B Annual Deductible ($131) Yes NoPart B Excess Charges at 100% Yes YesForeign Travel Emergency Yes YesAt-Home Recovery (up to $1,600 per year) Yes YesPreventive Medical Care (up to $120 per year) Yes Yes
Note: Please remember to review the Outline of Coverage which begins on page 13, so you’ll know aboutconditions, limitations and exclusions of coverage.

7
EXAMPLEHere is an example of how you could save money when you have incurred a $2,000 charge for services where Medicarehas established a $1,750 allowable level charge (assume that your Medicare Part B deductible has been satisfied):
ClaimFree Standard Plan A Doctor Accepts Doctor Does Not AcceptMedicare Supplement Plan Medicare Assignment Medicare Assignment
Medicare pays $1,400 $1,400Blue Cross pays $ 350 $ 350You pay $ 0 $ 250
Blue Cross Senior Classic C Doctor Accepts Doctor Does Not AcceptMedicare Supplement Plan Medicare Assignment Medicare Assignment
Medicare pays $1,400 $1,400Blue Cross pays $ 350 $ 350You pay $ 0 $ 250
Blue Cross Senior Classic F Medicare Supplement Plan, Blue Cross Senior Classic I Medicare Supplement Plan or Blue Cross Senior Classic J Doctor Accepts Doctor Does Not Accept Medicare Supplement Plan Medicare Assignment Medicare Assignment
Medicare pays $1,400 $1,400Blue Cross pays $ 350
Pays the difference between the negotiated rate/ $ 600billed charges and Medicare’s payment
You pay $ 0 $ 0
8
OUTLINE OF MEDICARE SUPPLEMENTCOVERAGE AND PREMIUM INFORMATION
Use this outline to compare benefits and premiumsamong policies.
Medicare supplement coverage/policies of thiscategory are designed to supplement Medicare bycovering some hospital, medical and surgicalservices that are partially covered by Medicare.Coverage is provided for hospital inpatient chargesand some physicians’ charges, subject to anydeductibles and coinsurance provisions which maybe in addition to those provided by Medicare, andsubject to other limitations which may be set forth inthe policy.
POLICY REPLACEMENT
If you are replacing other health coverage, do NOTcancel it until you have actually received your newcontract and are sure you want to keep it.
NOTICE
This contract may not fully cover all of your medicalcosts. Neither Blue Cross of California nor its agentsare connected with Medicare.
This outline of coverage does not give all the detailsof Medicare coverage. Contact your local SocialSecurity office or consult “The Medicare Handbook”for further details and limitations applicable toMedicare.
READ YOUR AGREEMENT
This brochure provides a brief description ofimportant features of your program. This is not theAgreement and only the Agreement sets forth, indetail, the rights and obligations of both you and BlueCross of California. You will receive your Blue Cross ofCalifornia Agreement once you enroll. It is importantthat you read your Agreement carefully uponreceiving it.
9
Use theeasy-to-readcharts onthe next 6pages tolearn howwe can helpyou coverthe gaps inMedicarewith
1
23
45
ClaimFree StandardPlan A MedicareSupplement Plan
Blue Cross SeniorClassic C MedicareSupplement Plan
Blue Cross SeniorClassic F MedicareSupplement Plan
Blue Cross SeniorClassic I MedicareSupplement Plan
Blue Cross SeniorClassic J MedicareSupplement Plan

10
Part
A S
ervi
ces
Services Benefit Medicare Pays
ClaimFreeStandard Plan AMedicareSupplement PlanPays
Blue Cross SeniorClassic C MedicareSupplement PlanPays
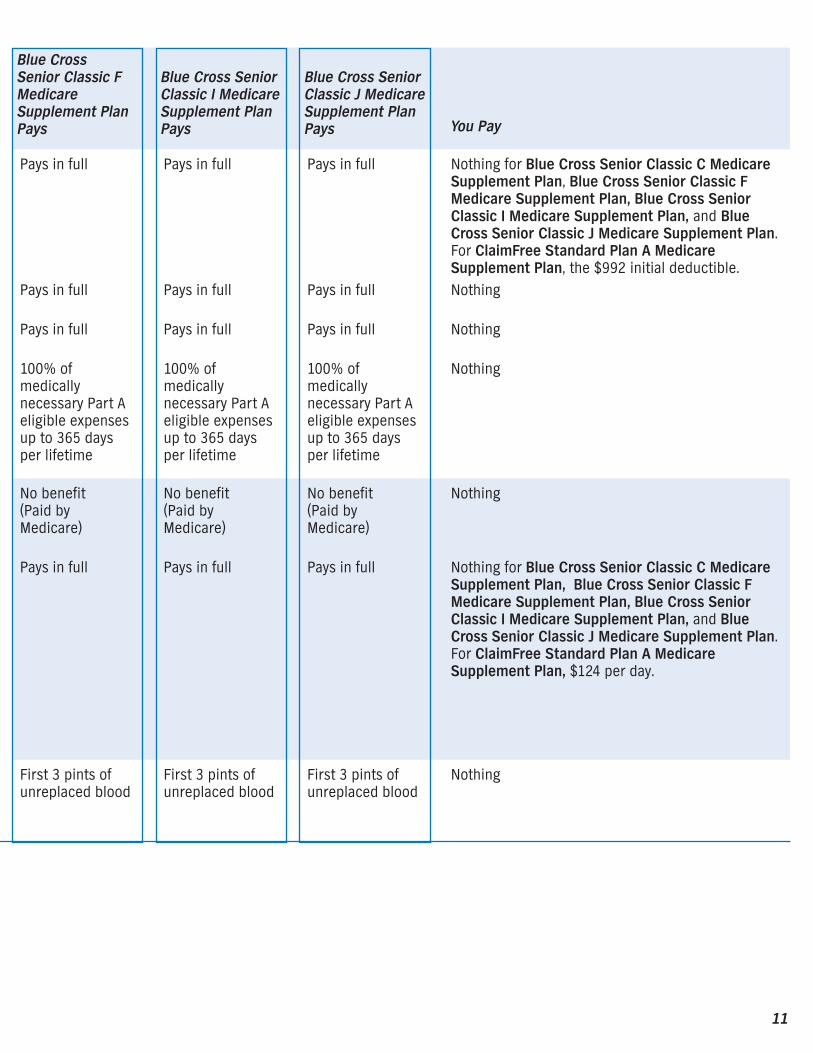
HospitalizationSemiprivate roomand board, generalnursing and otherhospital servicesand supplies, suchas drugs, x-rays, labtests and operatingroom.
First 60 days
61st thru 90th day
91st thru 150thday*151st thru 515thday
All but the first $992(Part A deductible)
All but $248 per daycoinsuranceAll but $496 per daylifetime reserveNothing
No benefit
Pays in full
Pays in full
100% of medicallynecessary Part Aeligible expensesup to 365 days perlifetime
Pays in full
Pays in full
Pays in full
100% of medicallynecessary Part Aeligible expensesup to 365 days perlifetime
Skilled NursingFacility Care(must be approvedby Medicare)You must have beenin a hospital for atleast 3 days, enter aMedicare-approvedfacility generallywithin 30 days afterhospital discharge,and meet otherprogramrequirements.
First 20 days
21st thru 100thday
100% of approvedamount
All but $124 per day
No benefit(Paid by Medicare)
No benefit
No benefit(Paid by Medicare)
Pays in full
Blood Unlimited ifmedicallynecessary
All but first 3 pintsper calendar year
First 3 pints ofunreplaced blood
First 3 pints ofunreplaced blood
* 60 lifetime reserve days may be used only once** These charges are covered in full when using any other provider if services are for a medical emergency, services are
immediately required for an unforeseen illness, injury or condition, or it is unreasonable to obtain services through anetwork provider.
11
You Pay
Nothing for Blue Cross Senior Classic C MedicareSupplement Plan, Blue Cross Senior Classic FMedicare Supplement Plan, Blue Cross SeniorClassic I Medicare Supplement Plan, and BlueCross Senior Classic J Medicare Supplement Plan.For ClaimFree Standard Plan A MedicareSupplement Plan, the $992 initial deductible.Nothing
Nothing
Nothing
Nothing
Nothing for Blue Cross Senior Classic C MedicareSupplement Plan, Blue Cross Senior Classic FMedicare Supplement Plan, Blue Cross SeniorClassic I Medicare Supplement Plan, and BlueCross Senior Classic J Medicare Supplement Plan.For ClaimFree Standard Plan A MedicareSupplement Plan, $124 per day.
Nothing
Blue Cross Senior Classic FMedicareSupplement PlanPays
Blue Cross SeniorClassic I MedicareSupplement PlanPays
Blue Cross SeniorClassic J MedicareSupplement PlanPays
Pays in full
Pays in full
Pays in full
100% ofmedicallynecessary Part Aeligible expensesup to 365 daysper lifetime
Pays in full
Pays in full
Pays in full
100% ofmedicallynecessary Part Aeligible expensesup to 365 daysper lifetime
Pays in full
Pays in full
Pays in full
100% ofmedicallynecessary Part Aeligible expensesup to 365 daysper lifetime
No benefit(Paid byMedicare)
Pays in full
No benefit(Paid byMedicare)
Pays in full
No benefit(Paid byMedicare)
Pays in full
First 3 pints ofunreplaced blood
First 3 pints ofunreplaced blood
First 3 pints ofunreplaced blood

12
Part
B S
ervi
ces
Excess Charges Medicalexpenses inexcess ofMedicare’sapprovedcharges
Nothing No benefit No benefit
Medical ExpensesPhysician’sservices, inpatientand outpatientmedical andsurgical servicesand supplies,physical andspeech therapy,diagnostic tests,durable medicalequipment, andother services.
Medical servicesin or out of thehospital
80% of approvedamount (50% ofapproved chargesfor most outpatientmental healthservices) after the$131 Part Bdeductible
Remainder ofMedicareapproved amount(Medicarecoinsurance)No benefit for the$131 Part Bdeductible
Remainder ofMedicare approvedamount (Medicarecoinsurance)100% of theMedicare Part Bdeductible whenusing aParticipatingProvider**
Blood Unlimited ifmedicallynecessary
80% of approvedamount (after $131deductible andstarting with 4thpint)
First 3 pints of unreplaced bloodand coinsuranceamount
First 3 pints ofunreplaced bloodand coinsuranceamount
Services Benefit Medicare Pays
ClaimFreeStandard Plan AMedicareSupplement PlanPays
Blue Cross SeniorClassic C MedicareSupplement PlanPays
* 60 lifetime reserve days may be used only once** These charges are covered in full when using any other provider if services are for a medical emergency, services are immediately
required for an unforeseen illness, injury or condition, or it is unreasonable to obtain services through a network provider.

13
Nothing for Blue Cross Senior Classic C MedicareSupplement Plan, Blue Cross Senior Classic FMedicare Supplement Plan, and Blue CrossSenior Classic J Medicare Supplement Plan,when using a Participating Provider. ForClaimFree Standard Plan A MedicareSupplement Plan, and Blue Cross Senior ClassicC Medicare Supplement Plan, and for Blue CrossSenior Classic F Medicare Supplement Plan,Blue Cross Senior Classic I MedicareSupplement Plan, and Blue Cross Senior ClassicJ Medicare Supplement Plan, when using anyother provider, the $131 deductible.
Nothing for Blue Cross Senior Classic FMedicare Supplement Plan, Blue Cross SeniorClassic I Medicare Supplement Plan, and BlueCross Senior Classic J Medicare SupplementPlan. For ClaimFree Standard Plan A MedicareSupplement Plan and Blue Cross Senior ClassicC Medicare Supplement Plan, any amounts over100% of Medicare’s approved charges if you goto a provider who does not accept Medicareassignment.
Nothing
100% 100% 100%
Remainder ofMedicareapprovedamount(Medicarecoinsurance)100% of theMedicare Part Bdeductible whenusing aParticipatingProvider**
Remainder ofMedicareapprovedamount(Medicarecoinsurance)No benefit forthe $131 Part Bdeductible
Remainder ofMedicareapprovedamount(Medicarecoinsurance)100% of theMedicare Part Bdeductible whenusing aParticipatingProvider**
First 3 pints ofunreplacedblood andcoinsuranceamount
First 3 pints ofunreplacedblood andcoinsuranceamount
First 3 pints ofunreplacedblood andcoinsuranceamount
Blue Cross Senior Classic FMedicareSupplement PlanPays
Blue Cross SeniorClassic I MedicareSupplement PlanPays
Blue Cross SeniorClassic J MedicareSupplement PlanPays You Pay
14
Services Medicare Pays
ClaimFree StandardPlan A MedicareSupplement Plan Pays
Blue Cross SeniorClassic C MedicareSupplement Plan PaysBenefit
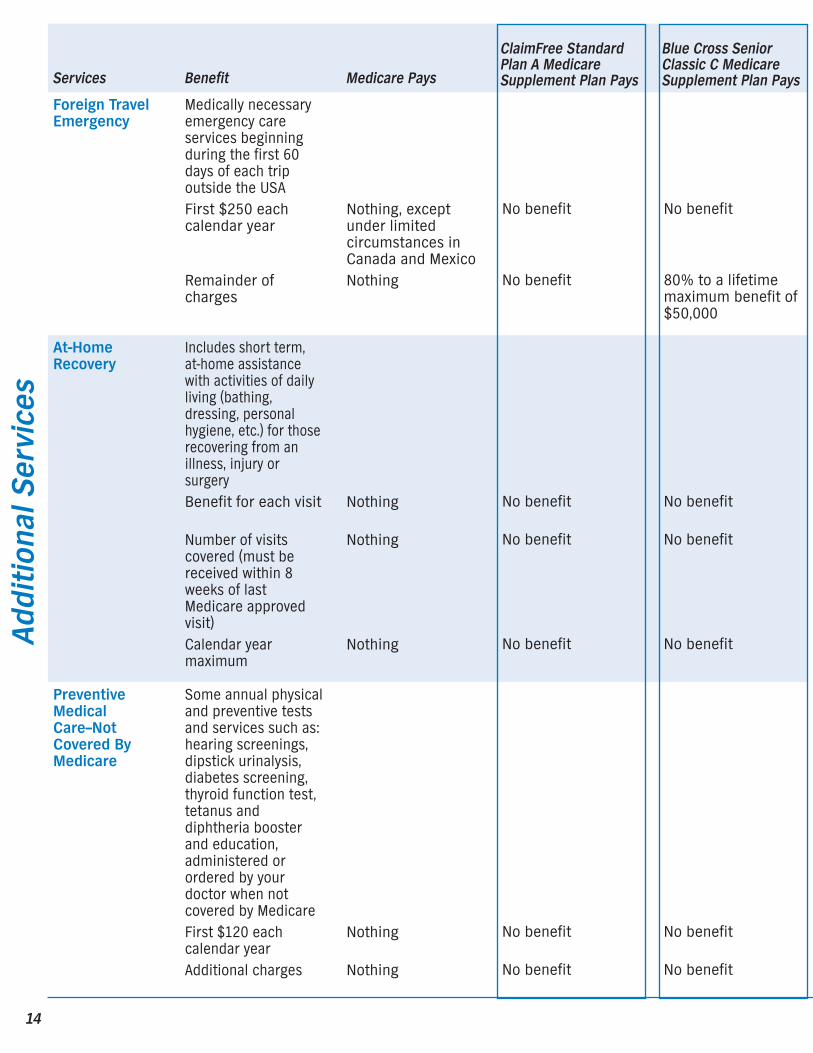
PreventiveMedicalCare–NotCovered ByMedicare
Nothing
Nothing
No benefit
No benefit
No benefit
No benefit
Some annual physicaland preventive testsand services such as:hearing screenings,dipstick urinalysis,diabetes screening,thyroid function test,tetanus anddiphtheria boosterand education,administered orordered by yourdoctor when notcovered by MedicareFirst $120 eachcalendar yearAdditional charges
Foreign TravelEmergency
Nothing, exceptunder limitedcircumstances inCanada and MexicoNothing
No benefit
No benefit
No benefit
80% to a lifetimemaximum benefit of$50,000
Medically necessaryemergency careservices beginningduring the first 60days of each tripoutside the USAFirst $250 eachcalendar year
Remainder ofcharges
At-HomeRecovery
Nothing
Nothing
Nothing
No benefit
No benefit
No benefit
No benefit
No benefit
No benefit
Includes short term,at-home assistancewith activities of dailyliving (bathing,dressing, personalhygiene, etc.) for thoserecovering from anillness, injury orsurgeryBenefit for each visit
Number of visitscovered (must bereceived within 8weeks of lastMedicare approvedvisit)Calendar yearmaximum
Addi
tion
al S
ervi
ces

15
You Pay
For Blue Cross Senior Classic CMedicare Supplement Plan, Blue CrossSenior Classic F Medicare SupplementPlan, Blue Cross Senior Classic IMedicare Supplement Plan, and Blue Cross Senior Classic J MedicareSupplement Plan, the $250 calendar yeardeductible, plus any charges above 80%of the billed charges for Medicare-eligibleexpenses, plus any amounts over the$50,000 lifetime maximum benefit. ForClaimFree Standard Plan A MedicareSupplement Plan, all costs.
For Blue Cross Senior Classic I MedicareSupplement Plan and Blue Cross SeniorClassic J Medicare Supplement Plan, anycharges above $40 per visit, any visitsexceeding 7 per week, and any amountsover $1,600 per year. For ClaimFreeStandard Plan A Medicare SupplementPlan, Blue Cross Senior Classic CMedicare Supplement Plan and Blue Cross Senior Classic F MedicareSupplement Plan, all costs.
For Blue Cross Senior Classic J MedicareSupplement Plan, any amounts over $120per year. For ClaimFree Standard Plan AMedicare Supplement Plan, Blue CrossSenior Classic C Medicare SupplementPlan, Blue Cross Senior Classic FMedicare Supplement Plan, and Blue Cross Senior Classic I MedicareSupplement Plan all costs.
Blue Cross SeniorClassic F MedicareSupplement Plan Pays
Blue Cross SeniorClassic I MedicareSupplement Plan Pays
Blue Cross SeniorClassic J MedicareSupplement Plan Pays
No benefit
No benefit
No benefit
No benefit
Up to $120 per year
No benefit
No benefit
80% to a lifetimemaximum benefit of$50,000
No benefit
80% to a lifetimemaximum benefit of$50,000
No benefit
80% to a lifetimemaximum benefit of$50,000
No benefit
No benefit
No benefit
Actual charges up to $40 per visitUp to the number ofMedicare-approvedvisits, not to exceed7 each week
$1,600
Actual charges up to $40 per visitUp to the number ofMedicare-approvedvisits, not to exceed7 each week
$1,600
16
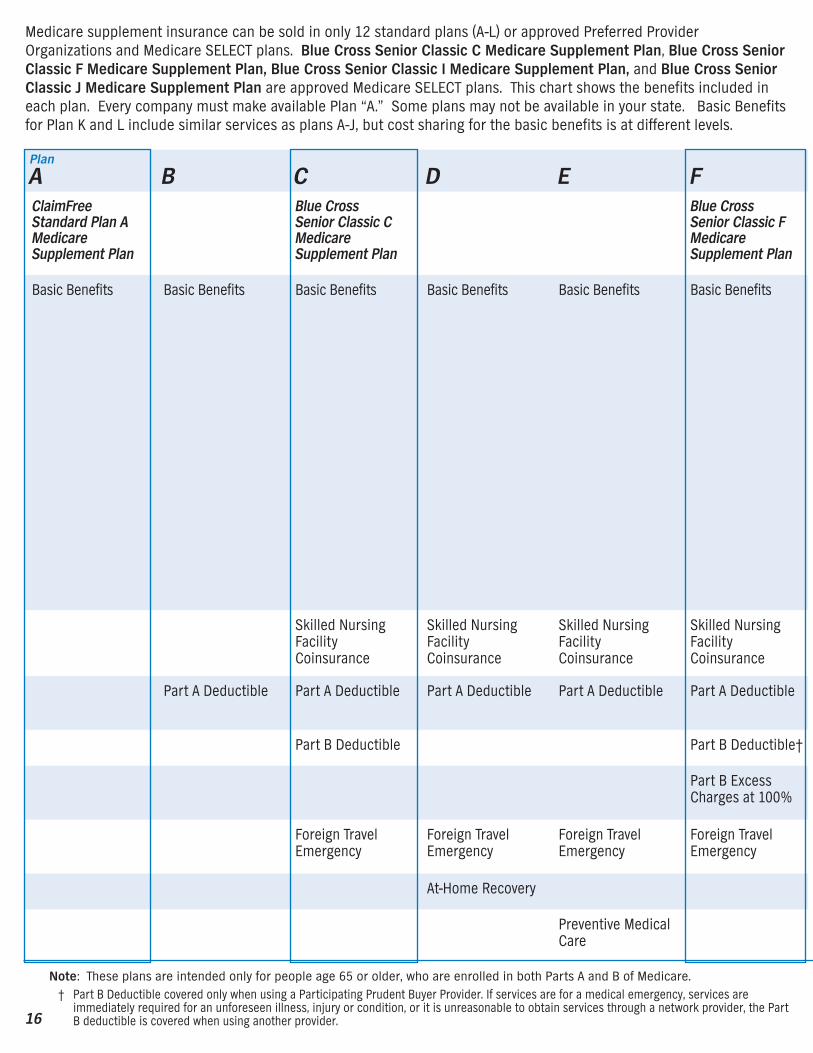
Medicare supplement insurance can be sold in only 12 standard plans (A-L) or approved Preferred ProviderOrganizations and Medicare SELECT plans. Blue Cross Senior Classic C Medicare Supplement Plan, Blue Cross SeniorClassic F Medicare Supplement Plan, Blue Cross Senior Classic I Medicare Supplement Plan, and Blue Cross SeniorClassic J Medicare Supplement Plan are approved Medicare SELECT plans. This chart shows the benefits included ineach plan. Every company must make available Plan “A.” Some plans may not be available in your state. Basic Benefitsfor Plan K and L include similar services as plans A-J, but cost sharing for the basic benefits is at different levels.
A B C D E FClaimFreeStandard Plan AMedicareSupplement Plan
Blue CrossSenior Classic CMedicareSupplement Plan
Blue CrossSenior Classic FMedicareSupplement Plan
Basic Benefits Basic Benefits Basic Benefits Basic Benefits Basic Benefits Basic Benefits
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
Part A Deductible Part A Deductible Part A Deductible Part A Deductible Part A Deductible
Part B Deductible Part B Deductible†
Part B ExcessCharges at 100%
Foreign TravelEmergency
Foreign TravelEmergency
Foreign TravelEmergency
Foreign TravelEmergency
At-Home Recovery
Preventive MedicalCare
Note: These plans are intended only for people age 65 or older, who are enrolled in both Parts A and B of Medicare.† Part B Deductible covered only when using a Participating Prudent Buyer Provider. If services are for a medical emergency, services are
immediately required for an unforeseen illness, injury or condition, or it is unreasonable to obtain services through a network provider, the PartB deductible is covered when using another provider.
Plan

17
Basic Benefits: Included in All Plans.! Hospitalization: Part A coinsurance plus coverage for 365 additional days after Medicare benefits end.! Medical Expenses: Part B coinsurance amount.! Blood: First 3 pints of blood each year.Medicare SELECT Disclosure about your right to purchase other plans. You may replace your Medicare SELECT plan withany Medicare supplement plan we offer of comparable or lesser benefits. This offer does not require proof of good health.
†† Plans K and L provide for different cost-sharing for items and services than Plans A-J. Once you reach the annual limit, the plan pays 100% of theMedicare copayments, coinsurance, and deductibles for the rest of the calendar year. The out-of-pocket annual limit does NOT include chargesfrom your provider that exceed Medicare-approved amounts, called "Excess Charges". You will be responsible for paying excess charges.
††† The out-of-pocket annual limit will increase for each year for inflation.
G H I J K†† L††
Blue CrossSenior Classic IMedicareSupplement Plan
Blue CrossSenior Classic JMedicareSupplement Plan
Basic Benefits Basic Benefits Basic Benefits Basic Benefits 100% of Part AHospitalizationCoinsurance pluscoverage for 365Days afterMedicare BenefitsEnd
50% Hospice cost-sharing
50% of Medicare-eligible expensesfor the first threepints of blood
50% Part BCoinsurance,except 100%Coinsurance forPart B PreventiveServices
100% of Part AHospitalizationCoinsurance pluscoverage for 365Days afterMedicare BenefitsEnd
75% Hospice cost-sharing
75% of Medicare-eligible expensesfor the first threepints of blood
75% Part BCoinsurance,except 100%Coinsurance forPart B PreventiveServices
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
Skilled NursingFacilityCoinsurance
50% SkilledNursing FacilityCoinsurance
75% SkilledNursing FacilityCoinsurance
Part A Deductible Part A Deductible Part A Deductible Part A Deductible 50% Part ADeductible
75% Part ADeductible
Part B Deductible†
Part B ExcessCharges at 80%
Part B ExcessCharges at 100%
Part B ExcessCharges at 100%
Foreign TravelEmergency
Foreign TravelEmergency
Foreign TravelEmergency
Foreign TravelEmergency
At-Home Recovery At-Home Recovery At-Home Recovery
Preventive MedicalCare
$4000 Out ofPocket Limit†††
$2000 Out ofPocket Limit†††
18
POLICY EFFECTIVE DATE! Policy effective dates are the 1st and 15th of themonth. If you are replacing a health insurance policythat terminates on a date other than the 1st or 15th,your coverage will be effective the date your otherplan ends.
! Your fully completed application must be receivedby the Blue Cross Senior Enrollment Departmentprior to your requested effective date. Applicationsreceived after your requested effective date will beprocessed for the next available effective date (the1st or 15th of the month).
! Blue Cross of California reserves the right to rejectyour application. If your application is rejected, youwill be notified in writing and any payment you madewill be refunded.
MEMBER BILLING! If your effective date of coverage is the 15th of themonth, the first premium bill you receive will be forone-and-a-half (1 1/2) months. Thereafter, Blue Crossof California will bill you every two (2) months.
! If your effective date of coverage is the 1st of themonth, Blue Cross of California will bill youbimonthly.
MONTHLY CHECKING ACCOUNT DEDUCTIONWith the Blue Cross of California Monthly CheckingAccount Deduction Program, you can have yourmonthly Blue Cross dues withdrawn directly fromyour checking account on the sixth (6th) day of eachmonth. When you receive your bank statement andcleared checks, your Blue Cross of California monthlychecking account deduction will be included. To findout more about this convenient service, contact yourBlue Cross of California Authorized Agent, or call ustoll-free at 1-800-333-3883.
CONVENIENCE OF SUMMARY BILLINGSummary Billing offers you the convenience ofconsolidating your billing with any other Blue Crossof California Senior Plan Member, such as a spouseor relative. This means that we can combineseparate billings onto a single statement, even if youand the other person(s) are enrolled in different BlueCross of California Senior Plans.
The result is less paperwork for you because onestatement, one check and one envelope does the job.Summary Billing is also available if you choose themonthly checking account deduction option.
GUARANTEED RENEWABLEBlue Cross of California Medicare supplements areguaranteed renewable.
After the first one (1) month’s payment, the term ofthis coverage is for two (2) months if you have chosenbimonthly coverage, or monthly if you have chosenmonthly checking account deductions. It renewsautomatically, subject to the right of Blue Cross ofCalifornia to change subscription charges. Any suchchanges would be made only upon 30 days writtennotice to all persons covered under the same plan as you.
We will not cancel your coverage, except for thereasons listed below:
! If we discover any concealment of material factsupon enrollment
! If you do not pay your subscription charges, your coverage will end automatically without noticefrom us
! You cease to be covered under both Parts A and Bof Medicare
! You enroll in a Medicare Coordinated Care Plan
Coordinated Care Plans (also sometimes referred toas Medicare-at-Risk Plans) are special HealthMaintenance Organizations (HMOs) and CompetitiveMedical Plans (CMPs) that seniors eligible forMedicare may be able to join. They essentiallycombine Medicare benefits with supplementalbenefits. People who join must generally get allhealth care from providers affiliated with the plan,and they do not receive regular Medicare benefits forservices obtained outside the plan.
QUALITY ASSURANCEIn accordance with California law, Blue Crosscontinuously reviews the quality of care provided toyou under this contract. Under Blue Cross’ quality ofcare review system, Participating Providers arecredentialed regularly, and the quality of the carethey provide is reviewed on both a concurrent and

19
prospective basis. Because members may obtaincare from any Nonparticipating Provider they choose,Blue Cross is unable to review the credentials of suchNonparticipating Providers or to include them inprospective and concurrent review programs.Nevertheless, Blue Cross reviews the servicesprovided by all providers, both participating andnonparticipating retrospectively.
30-DAY RIGHT TO EXAMINEIf you’re not satisfied with your coverage, forwhatever reason, just send back your Policy within 30days of receiving it. The insurance will be canceledand your premium will be promptly refunded — noquestions asked. What could be safer than that?
MEDICARE CHANGESBlue Cross of California will send an annual notice toyou 30 days prior to the effective date of Medicarechanges, which will describe these changes and thechanges in your Medicare supplement coverage.
GUARANTEED ACCEPTANCEAcceptance of your application is guaranteed if youare 65 or older and apply within six (6) months ofyour initial enrollment in Part B of Medicare. Youmust already be enrolled in both Parts A and B ofMedicare to apply for these plans. Acceptance for thiscoverage is also guaranteed and preexistingconditions will be waived if you meet any of thefollowing conditions:
1 The individual is enrolled under an employeewelfare benefit plan that provides health benefits thatsupplement the benefits under Medicare, and theplan either terminates or ceases to provide all ofthose supplemental health benefits to the individual.
2 The individual is enrolled with a MedicareAdvantage organization under a Medicare Advantageplan under Medicare Part C, and any of the followingcircumstances apply:
A) The certification of the organization or plan hasbeen terminated.
B) The organization has terminated or otherwisediscontinued providing the plan in the area in whichthe individual resides.
C) The individual is no longer eligible to elect theplan because of a change in the individual’s place ofresidence or other change in circumstances specifiedby the secretary. Those changes in circumstancesshall not include termination of the individual’senrollment on the basis described in Section1851(g)(3)(B) of the federal Social Security Act wherethe individual has not paid premiums on a timelybasis or has engaged in disruptive behavior asspecified in standards under Section 1856, or theplan is terminated for all individuals within aresidence area.
D) The Medicare Advantage plan in which theindividual is enrolled reduces any of its benefits orincreases the amount of cost sharing or discontinuesfor other than good cause relating to quality of care,its relationship or contract under the plan with aprovider who is currently furnishing services to theindividual. An individual shall be eligible under thissubparagraph for a Medicare supplement contractissued by the same issuer through which theindividual was enrolled at the time the reduction,increase, or discontinuance described above occursor, commencing January 1, 2007, for one issued by asubsidiary of the parent company of that issuer or bya network that contracts with the parent company ofthat issuer.
E) The individual demonstrates, in accordance withguidelines established by the secretary, either of thefollowing:
(i) The organization offering the plan substantiallyviolated a material provision of the organization’scontract under this article in relation to theindividual, including the failure to provide on a timelybasis medically necessary care for which benefits areavailable under the plan or the failure to provide thecovered care in accordance with applicable qualitystandards.
(ii) The organization, or agent or other entity actingon the organization’s behalf, materiallymisrepresented the plan’s provisions in marketingthe plan to the individual.
F) The individual meets other exceptionalconditions as the secretary may provide.
20
3 The individual is 65 years of age or older, isenrolled with a Program of All-Inclusive Care for theElderly (PACE) provider under Section 1894 of theSocial Security Act, and circumstances similar tothose described in paragraph (2) exist that wouldpermit discontinuance of the individual’s enrollmentwith the provider, if the individual were enrolled in aMedicare Advantage plan.
4) The individual meets both of the followingconditions:
A) The individual is enrolled with any of thefollowing:
(i) An eligible organization under a contract underSection 1876 of the Social Security Act (Medicarecost).
(ii) A similar organization operating underdemonstration project authority, effective for periodsbefore April 1, 1999.
(iii) An organization under an agreement underSection 1833(a)(1)(A) of the Social Security Act(health care prepayment plan).
(iv) An organization under a Medicare Select policy.
B) The enrollment ceases under the samecircumstances that would permit discontinuance ofan individual’s election of coverage under paragraph(2) or (3).
5 The individual is enrolled under a Medicaresupplement contract, and the enrollment ceasesbecause of any of the following circumstances:
A) The insolvency of the issuer or bankruptcy of thenonissuer organization, or other involuntarytermination of coverage or enrollment under thecontract.
B) The issuer of the contract substantially violateda material provision of the contract.
C) The issuer, or an agent or other entity acting onthe issuer’s behalf, materially misrepresented thecontract’s provisions in marketing the contract to theindividual.
6 The individual meets both of the followingconditions:
A) The individual was enrolled under a Medicaresupplement contract and terminates enrollment andsubsequently enrolls, for the first time, with any
Medicare Advantage organization under a MedicareAdvantage plan under Medicare Part C, any eligibleorganization under a contract under Section 1876 ofthe Social Security Act (Medicare cost), any similarorganization operating under demonstration projectauthority, any PACE provider under Section 1894 ofthe Social Security Act, or a Medicare Select policy.
B) The subsequent enrollment under subparagraph(A) is terminated by the individual during any periodwithin the first 12 months of the subsequentenrollment (during which the enrollee is permitted toterminate the subsequent enrollment under Section1851(e) of the federal Social Security Act).
7 The individual upon first becoming eligible forbenefits under Medicare Part A at age 65 years ofage, enrolls in a Medicare Advantage plan underMedicare Part C or with a PACE provider underSection 1894 of the Social Security Act, anddisenrolls from the plan or program not later than 12months after the effective date of enrollment.
8 The individual while enrolled under a Medicaresupplement contract that covers outpatientprescription drugs enrolls in a Medicare Part D planduring the initial enrollment period, terminatesenrollment in the Medicare supplement contract, andsubmits evidence of enrollment in Medicare Part Dalong with the application for a Medicare supplementpolicy that has a benefit package classified as Plan A,B, C, F (including F with high deductible), K or L, andthat is offered and is available for issuance to newenrollees by the same issuer that issued theindividual’s Medicare supplement policy withoutpatient prescription drug coverage.
COMPLETE ANSWERS ARE VERY IMPORTANTWhen you fill out the application for the new contract,be sure to answer truthfully and completely allquestions about your medical and health history. Thecompany may cancel your contract and refuse to payany claims if you leave out or falsify importantmedical information; this would not apply if you arein your guaranteed acceptance period describedabove. Review the application carefully before yousign it. Be certain that all information has beenproperly recorded.

21
WHAT IS NOT COVEREDSome expenses the ClaimFree Standard Plan AMedicare Supplement Plan agreement does not coverare: the Part A deductible; Skilled Nursing Facility Care;the Part B deductible; excess physician charges (abovethe amount Medicare allows); travel coverage; custodialcare; outpatient drugs; dental care or dentures; routinecheckups or immunizations; foot care; eyeglasses(unless covered by Medicare); hearing aids; chiropracticcare (unless covered by Medicare).
Some expenses the Blue Cross Senior Classic CMedicare Supplement Plan agreement does not coverare: the Part B deductible (out of network); excessphysician charges (above the amount Medicare allows);custodial care; outpatient drugs; dental care ordentures; routine checkups or immunizations; foot care;eyeglasses (unless covered by Medicare); hearing aids;chiropractic care (unless covered by Medicare).
Some expenses the Blue Cross Senior Classic FMedicare Supplement Plan agreement does not coverare: the Part B deductible (out of network), custodialcare; outpatient drugs; dental care or dentures; routinecheckups or immunizations; foot care; eyeglasses(unless covered by Medicare); hearing aids; chiropracticcare (unless covered by Medicare).
Some expenses the Blue Cross Senior Classic IMedicare Supplement Plan agreement does not coverare: the Part B deductible, custodial care; outpatientdrugs; dental care or dentures; routine checkups orimmunizations; foot care; eyeglasses (unless covered byMedicare); hearing aids; chiropractic care (unlesscovered by Medicare).
Some expenses the Blue Cross Senior Classic JMedicare Supplement Plan agreement does not coverare: the Part B deductible (out of network), custodialcare; outpatient drugs; dental care or dentures; routinecheckups or immunizations (unless covered under thePreventive Medical Care Benefit); foot care; eyeglasses(unless covered by Medicare); hearing aids; chiropracticcare (unless covered by Medicare).
Some expenses the ClaimFree Standard Plan AMedicare Supplement Plan, Blue Cross SeniorClassic C Medicare Supplement Plan, Blue CrossSenior Classic F Medicare Supplement Plan, BlueCross Senior Classic I Medicare Supplement Plan,and Blue Cross Senior Classic J Medicare
Supplement Plan agreements do not cover are:private duty nursing; personal comfort items;services for which no charge is made; servicesrendered by relatives; any services or supplies notspecifically listed as covered in your Agreement;services rendered during a hospital stay which beganbefore coverage is in force or after coverage hasbeen terminated; hearing aids; dental care andtreatment; eyeglasses (unless covered by Medicare);eye examinations and chiropractic care (unlesscovered by Medicare); any conditions covered underWorkers’ Compensation; any conditions covered byany Federal Government agency; conditions resultingfrom war, invasion or atomic explosion; custodialcare and rest cures; routine physical examinations(with the exception of the Blue Cross Senior Classic JMedicare Supplement Plan which offers somecoverage); inpatient admissions primarily fordiagnostic studies when inpatient bed care is notmedically necessary; acupuncture; dental work;cosmetic surgery or other services for beautification;services primarily for weight reduction as the mainmethod of treatment and services not approved byMedicare unless specified elsewhere.
As required by law, we are advising you that the lossratios for these plans in 2005 were: 64% for Blue Cross Senior Classic F MedicareSupplement Plan, 62% for Blue Cross Senior ClassicJ Medicare Supplement Plan, 63% for Blue CrossSenior Classic C Medicare Supplement Plan and58% for ClaimFree Standard Plan A MedicareSupplement Plan.
GRIEVANCE PROCEDUREAll complaints and disputes relating to coverageunder this plan must be resolved in accordance withBlue Cross’ grievance procedure. Grievances may bemade by telephone or in writing.
All grievances received by Blue Cross will beacknowledged in writing, together with a descriptionof how Blue Cross of California proposes to resolvethe grievance. Grievances that cannot be resolved bythis procedure shall be submitted to arbitration.
22
MEMBER GRIEVANCE PROCEDUREWe are certain that you will be completely satisfiedwith your Blue Cross of California plan, but if youshould ever have a complaint or problem, pleasefollow the Member Grievance Procedure:
Step 1.Contact Blue Cross of California.You can call us at 1-800-333-3883.You can write to us at P.O. Box 9053, Oxnard, CA93031-9053.
Your grievance will be reviewed and you will receive aresponse within 30 days.
Step 2.If you are not satisfied with the response, you cansubmit the grievance to binding arbitration.
Any dispute between the Member and Blue Crossregarding the decision of Blue Cross must besubmitted to binding arbitration if the amount indispute exceeds the jurisdictional limits of the smallclaims court. This arbitration is begun by theMember making written demand on Blue Cross.
This arbitration will be held before a designatedneutral arbitrator appointed by the county medicalassociation of the county in which the services wereprovided. If the county medical association declinesor is unable to appoint an arbitrator, the arbitrationwill be conducted according to the rules of theAmerican Arbitration Association.
Any dispute regarding a claim for damages within thejurisdictional limits of the small claims court will beresolved in such court.
Any dispute or claim, of whatever nature, arising outof, in connection with, or in relation to, thisAgreement, or breach or rescission thereof, or inrelation to care or delivery of care, including anyclaim based on contract, tort or statute, must beresolved by arbitration if the amount sought exceedsthe jurisdictional limit of the small claims court. Anydispute regarding a claim for damages within thejurisdictional limits of the small claims court will beresolved in such court. The Federal Arbitration Actshall govern the interpretation and enforcement of allproceedings under this BINDING ARBITRATIONprovision. To the extent that the Federal ArbitrationAct is inapplicable, or is held not to requirearbitration of a particular claim, state law governing
agreements to arbitrate shall apply. The Member andBlue Cross agree to be bound by these arbitrationprovisions and acknowledge that they are giving uptheir right to trial by court or jury.
California Health & Safety Code section 1363.1requires that any arbitration agreement include thefollowing notice: "It is understood that any dispute asto medical malpractice, that is as to whether anymedical services rendered under this contract wereunnecessary or unauthorized or were improperly,negligently or incompetently rendered, will bedetermined by submission to arbitration as providedby California law, and not by a lawsuit or resort tocourt process except as California law provides forjudicial review of arbitration proceedings. Bothparties to this contract, by entering into it, are givingup their constitutional right to have any such disputedecided in a court of law before a jury, and insteadare accepting the use of arbitration."
The Member and Blue Cross agree to give up theright to participate in class arbitrations against eachother. Even if applicable law permits class actions orclass arbitrations, the Member waives any right topursue, on a class basis, any such controversy orclaim against Blue Cross and Blue Cross waives anyright to pursue, on a class basis, any suchcontroversy or claim against the Member. Thearbitration findings will be final and binding except tothe extent that state or federal law provides for thejudicial review of arbitration proceedings. Thearbitration is initiated by the Member making writtendemand on Blue Cross. The arbitration will beconducted by Judicial Arbitration and MediationServices ("JAMS"), according to its applicable Rulesand Procedures. If for any reason JAMS is unavailableto conduct the arbitration, the arbitration will beconducted by another neutral arbitration entity, byagreement of the Member and Blue Cross, or byorder of the court, if the Member and Blue Crosscannot agree.

23
The costs of the arbitration will be allocated per theJAMS Policy on Consumer Arbitrations. If thearbitration is not conducted by JAMS, the costs willbe shared equally by the parties, except in cases ofextreme financial hardship, upon application to theneutral arbitration entity to whom the parties haveagreed, in which cases, Blue Cross will assume all ora portion of the costs of the arbitration. Please sendall Binding Arbitration demands in writing to:
Blue Cross of CaliforniaP.O. Box 9053, Oxnard, CA 93031-9053
The California Department of Managed Health Care isresponsible for regulating health care service plans.If you have a grievance against your health plan, youshould first telephone your health plan at 1-800-333-3883 and use your health plan's grievanceprocess before contacting the department. Utilizingthis grievance procedure does not prohibit anypotential legal rights or remedies that may beavailable to you. If you need help with a grievanceinvolving an emergency, a grievance that has notbeen satisfactorily resolved by your health plan, or agrievance that has remained unresolved for morethan 30 days, you may call the department forassistance. You may also be eligible for anIndependent Medical Review (IMR). If you are eligiblefor IMR, the IMR process will provide an impartialreview of medical decisions made by a health planrelated to the medical necessity of a proposedservice or treatment, coverage decisions fortreatments that are experimental or investigational innature and payment disputes for emergency orurgent medical services. The department also has atoll-free telephone number 1-888-HMO-2219 and aTDD line 1-877-688-9891 for the hearing and speechimpaired. The department's Web site atwww.hmohelp.ca.gov has complaint forms, IMRapplication forms and instructions online.
QUESTIONS?After you receive your Agreement, please feel free tocontact your Blue Cross of California AuthorizedAgent, or call us toll-free at 1-800-333-3883.
You can write to us at P.O. Box 9053, Oxnard, CA 93031-9053.
Health Maintenance Organizations (HMO) require thata specific primary care physician (gatekeeper)authorize all medical services outside the scope ofhis or her office. A Preferred Provider Organization(PPO) allows members to choose their own physicianand specialist anytime, anywhere within the providernetwork. Blue Cross of California’s ClaimFreeStandard Plan A Medicare Supplement Plan , BlueCross Senior Classic C Medicare Supplement Plan,Blue Cross Senior Classic F Medicare SupplementPlan, Blue Cross Senior Classic I MedicareSupplement Plan, and Blue Cross Senior Classic JMedicare Supplement Plan provide their members anetwork of over 50,000 physicians statewide.
24
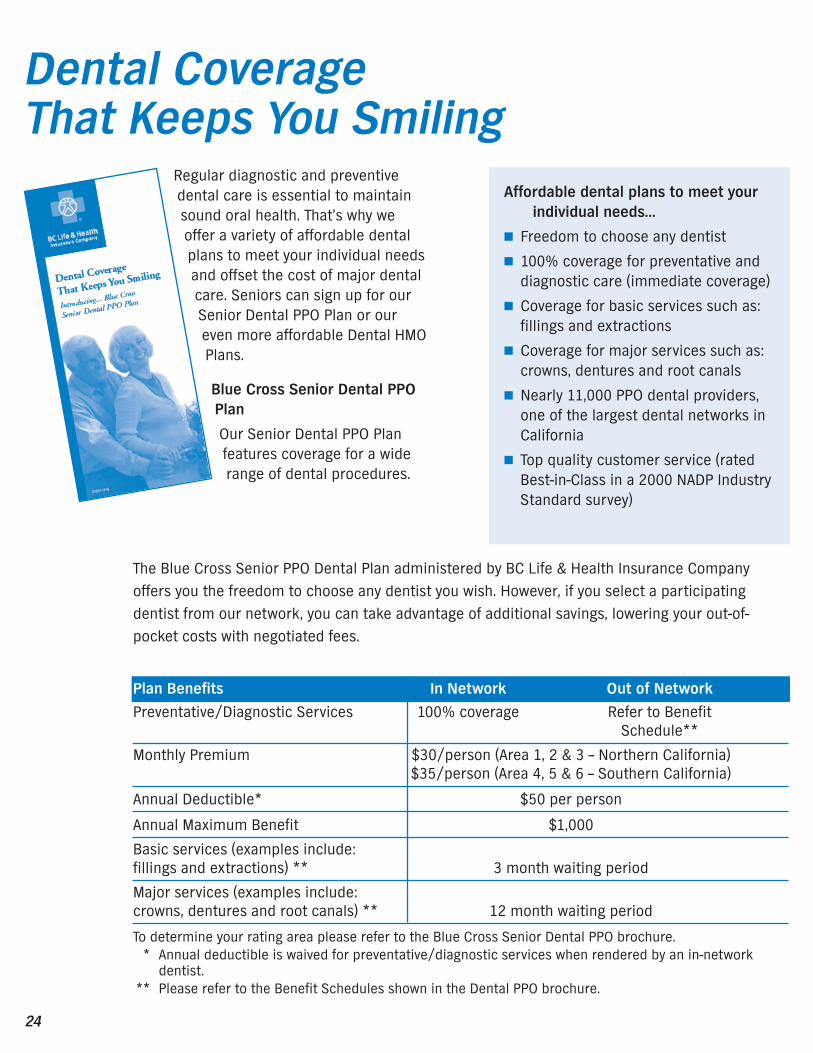
The Blue Cross Senior PPO Dental Plan administered by BC Life & Health Insurance Companyoffers you the freedom to choose any dentist you wish. However, if you select a participatingdentist from our network, you can take advantage of additional savings, lowering your out-of-pocket costs with negotiated fees.
Regular diagnostic and preventivedental care is essential to maintainsound oral health. That’s why weoffer a variety of affordable dentalplans to meet your individual needsand offset the cost of major dentalcare. Seniors can sign up for ourSenior Dental PPO Plan or oureven more affordable Dental HMOPlans.
Blue Cross Senior Dental PPOPlan
Our Senior Dental PPO Planfeatures coverage for a widerange of dental procedures.
Dental Coverage That Keeps You Smiling
Plan Benefits In Network Out of Network
Preventative/Diagnostic Services 100% coverage Refer to Benefit Schedule**
Monthly Premium $30/person (Area 1, 2 & 3 – Northern California) $35/person (Area 4, 5 & 6 – Southern California)
Annual Deductible* $50 per person
Annual Maximum Benefit $1,000
Basic services (examples include: fillings and extractions) ** 3 month waiting period
Major services (examples include: crowns, dentures and root canals) ** 12 month waiting period
To determine your rating area please refer to the Blue Cross Senior Dental PPO brochure.* Annual deductible is waived for preventative/diagnostic services when rendered by an in-network
dentist.** Please refer to the Benefit Schedules shown in the Dental PPO brochure.
Affordable dental plans to meet yourindividual needs…
! Freedom to choose any dentist
! 100% coverage for preventative anddiagnostic care (immediate coverage)
! Coverage for basic services such as:fillings and extractions
! Coverage for major services such as:crowns, dentures and root canals
! Nearly 11,000 PPO dental providers,one of the largest dental networks inCalifornia
! Top quality customer service (ratedBest-in-Class in a 2000 NADP IndustryStandard survey)
25
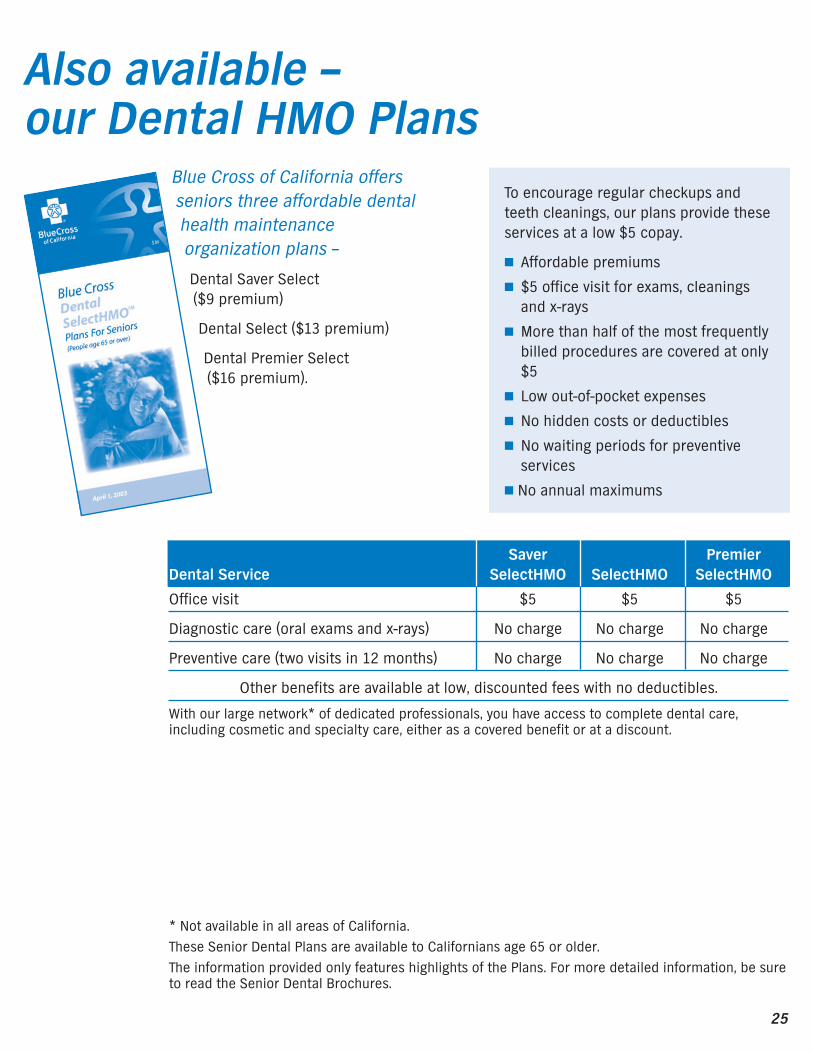
Saver PremierDental Service SelectHMO SelectHMO SelectHMO
Office visit $5 $5 $5
Diagnostic care (oral exams and x-rays) No charge No charge No charge
Preventive care (two visits in 12 months) No charge No charge No charge
Other benefits are available at low, discounted fees with no deductibles.
With our large network* of dedicated professionals, you have access to complete dental care,including cosmetic and specialty care, either as a covered benefit or at a discount.
Blue Cross of California offersseniors three affordable dentalhealth maintenanceorganization plans –
Dental Saver Select ($9 premium)
Dental Select ($13 premium)
Dental Premier Select ($16 premium).
Also available – our Dental HMO Plans
To encourage regular checkups andteeth cleanings, our plans provide theseservices at a low $5 copay.
! Affordable premiums
! $5 office visit for exams, cleaningsand x-rays
! More than half of the most frequentlybilled procedures are covered at only$5
! Low out-of-pocket expenses
! No hidden costs or deductibles
! No waiting periods for preventiveservices
! No annual maximums
* Not available in all areas of California. These Senior Dental Plans are available to Californians age 65 or older. The information provided only features highlights of the Plans. For more detailed information, be sureto read the Senior Dental Brochures.

Visit our Web site www.bluecrossca.com
Not connected with or endorsed by the U. S. Government or the federal Medicare program.
Blue Cross of California and BC Life & Health Insurance Company are Independent Licensees of the Blue Cross Association
The Blue Cross name and symbol are registered marks of the Blue Cross Association.
© 2007 Blue Cross of California
IS7067 1/07