Embed Size (px)
Citation preview

10/8/21
1
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Backed into a Bacteremia Corner
Crystal K. Howell, PharmD, BCIDP, BCPSJohn W. Millard, PharmD, BCGP, BCIDP, BCPS
1
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Meet the SpeakersCrystal K. Howell, PharmD, BCIDP, BCPS• Current Role: Assistant Professor at the University of North Texas
Health Science Center College of Pharmacy• PGY2 in Infectious Diseases: Emory University Hospital Midtown and
Emory University Hospital
• PGY1: Emory University Hospital
John W. Millard PharmD, BCGP, BCIDP, BCPS• Current Role: Clinical Pharmacist Practitioner at the Robert J. Dole VA
Medical Center • VISN-15 Antimicrobial Stewardship Commission Co-Chairman
• Adjunct clinical assistant professor at the Kansas University School of Pharmacy
2

10/8/21
2
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Disclosure
• Disclosures:• Dr. Howell does not have any conflicts of interest in relation to this activity• Potential conflicts of interest for Dr. Millard:
• Invested into the TSP funds with no control over individual assets allocation and as a result may directly own portions of the companies which products are herewith in discussed
• Presenter holds medical device and utility patents in diagnostic modalities regarding neurological and meningeal infectious etiology and are outside the scope of this presentation
• Disclaimers:• The views expressed in this presentation reflect those of the presenter, and
not those of the Department of Veteran Affairs.
3
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Learning Objectives
1. Interpret criteria for appropriate oral treatment of bacteremia.2. Utilize alternative pharmacokinetic administrations of
antimicrobials for bacteremia to optimize antimicrobial activity.3. Integrate new data for long-acting glycopeptides and bacteremia
into practice.4. Apply site and microbiology specific concepts to patient cases.
4

10/8/21
3
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
When Can PO Therapy Be Used for Bacteremia?
5
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Recent Literature That Indicates PO Might Be Okay
Iversen, et al. N Engl J Med 2019;380:415-24. Li, et al. N Engl J Med 2019;380:425-36.
6

10/8/21
4
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
What is Uncomplicated Bacteremia?MRSA Guideline Criteria for Uncomplicated Bacteremia:
• No endocarditis (IE)• No prostheses• Blood cultures clear within 2 - 4
days • Defervescence within 72hrs of
therapy• No evidence of metastases
Newer Data on Risk Factors for Prolonged / Recurrent Bacteremia:• MRSA > MSSA• IE or other endovascular cause• Lack of or delayed ID consult• ICU admission• Lack of source control• > 3 days of bacteremia• Pitt bacteremia score/ APACHE II score• Black race• Hemodialysis
Liu et al. Clin Infect Dis 2011;1-38Minejima et al. Clin Infect Dis 2020;3;70(4):566-573Choi et al. Clin Infect Dis 2021;1;71(11):1891-1899
MRSA = Methicillin-resistant Staphylococcus aureus, MSSA = Methicillin-susceptible Staphylococcus aureus, ID = infectious diseases, IE = infective endocarditis, ICU = intensive care unit
7
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Oral Step Down Therapy Can Improve Transitions of Care Without Increasing Risk of Harm
Citation Bacteria Intervention Efficacy Outcomes Other
Tamma JAMA Internal Med 2019
Enterobacteriaceae bacteremia with source control
Empiric IV then either IV or (PO FQ or SMX/TMP) or PO beta-lactam
• No difference in mortality between PO and IV (13.1% vs 13.4%, NS)
• No difference in mortality between PO groups (11% vs 12.3%, NS)
• ↓ LOS (5d PO vs 7d IV)• ↓ 30d recurrence in beta-lactam vs
FQ or SMX/TMP (0% vs 0.6%)
• ~3 vs 14d of IV • ~14 DOT• ~ 40% of source
were urinary tract
Willekens CID 2018
Staphylococcus aureus low-riskbacteremia
Standard IV therapy then changed to PO linezolid or kept on IV
PO Linezolid had: • ↓ 90d relapses (2.2% vs 4.4%)• Protective in risk factor analysis of
30d mortality• ↓ LOS (8 vs 19d)
• ~ 7 d of IV• ~ 15 DOT
Tamma et al. JAMA Intern Med 2019;179(3):316-323Willekens et al. Clin Infect Dis 2019;69(3):381-387
IV = intravenous, PO = oral, FQ = fluoroquinolone, SMX/TMP = sulfamethoxazole/trimethoprim, LOS = length of stay, DOT = duration of therapy
8

10/8/21
5
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Not All Beta-lactams Have Low BioavailabilitySelect Drugs Oral Absorption
Cefaclor 93%
Cefadroxil “well-absorbed”, 90%
Cefprozil 95%
Cephalexin* 90%
• Modifications to R1 of the cephalosporin nucleus increases oral absorption
• Some ester prodrugs can also enhance bioavailability
Select Drugs Oral Absorption
Amoxicillin 75%
Amoxicillin/clavulanate “well-absorbed”, 75%
Lexicomp Online, Lexi-Drugs; Micromedex® (electronic version); Johns Hopkins ABX Guide.;Doi Y. Chapter 20 Penicillins and B-Lactamase Inhibitors. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition;Lepak AJ et al. Chapter 21 Cephalosporins. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition.
Image created with the support of: https://chem-space.com/search
*Cephalexin susceptibility not routinely done, infer susceptibility from cefazolin
9
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Oral Beta Lactams Have Some Retrospective Data For Treatment of Bacteremia
Citation Bacteria Intervention Efficacy Outcomes Other Info
Saad BMC ID 2020 E. coli bacteremia from a urine source
Empiric IV beta-lactam then step - down to PO FQ or PO beta-lactam
• ↓Clinical cure: 98% FQ vs 94% in beta-lactam (p = 0.13)
• No difference in 30d mortality, CDI, or LOS (~6 d)
• ~ 5 d of IV• ~ 14 DOT
Sutton JAMA Network Open 2020
Enterobacteralesbacteremia from a urine source
Empiric IV then step -down to PO either (SMX/TMP or FQ) or beta-lactam
• No difference in composite 30d mortality or recurrent bacteremia
• ~ 5 d of IV
Arensman AAC 2020
Uncomplicated Streptococcalbacteremia
Empiric IV then step -down to PO FQ or beta-lactam
• No difference in clinical success (~92%)
• No difference in reason for clinical failures
• No difference in adverse events including CDI
• ~5 d of IV• ~14 DOT
Saad S et al. BMC Infectious Diseases 2020;20:785; Sutton et al. JAMA Network Open. 2020;3(10):e2020166; Arensman et al. Antimicrob Agents Chemother 64:e01515-20
IV = intravenous, PO = oral, FQ = fluoroquinolone (not moxifloxacin for urine sources), SMX/TMP = sulfamethoxazole/trimethoprim, CDI = Clostridioides difficile infection, LOS = length of stay, DOT = duration of therapy
10

10/8/21
6
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
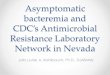
Bacteriostatic Drugs Require Higher Concentrations to Kill As Quickly But Still Kill
Bacteriostatic: 103 decrease in bacterial density after 24 hours at concentrations > 8 fold above the MIC
Bactericidal:103 decrease in bacterial density after 24 hours at concentrations ≤ 4 fold above the MIC
Time (hours)
0 2 4 6 8
1010
108
106
104
102
1
Viab
le ce
ll de
nsity
(CFU
s)
Viab
le ce
ll de
nsity
(CFU
s)
0 2 4 6 8
1010
108
106
104
102
1
Time (hours)
Legend:Unexposed organism
Antibiotic exposed organism
Spellburg B. Chapter 17 Principles of Antiinfective Therapy. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition;Pai MP et al. Chapter 19 Pharmacokinetics and Pharmacodynamics of Antiinfectives Agents. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition.
11
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Systematic Review of 56 Randomized Controlled Trials- 49 (81%) of articles found no difference between bacteriostatic and
bactericidal agents- Six trials demonstrated bacteriostatic superiority over bactericidal agents- One trial had a bactericidal agent that was more effective than the
bacteriostatic agent
Wald-Dickler et al. Clin Infect Dis 2018;66(9):1470–4
12

10/8/21
7
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
When to Consider Oral Therapy for Bacteremia
Consider PO• Uncomplicated with source
control• Organism susceptibility• Organism without much
virulence?• Initial IV therapy completed• Anticipated duration 14 days• Patient can tolerate PO• High bioavailability PO agent
Stick with IV• Endovascular source or
complicated bacteremia• Unable to tolerate PO• Low bioavailability• Multidrug resistant organism
(MDRO)
13
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self Assessment Case 1.
75 yo F admitted from an assisted living facility (ALF) with pan-S Enterococcus faecalis bacteremia secondary to gut translocation from severe constipation associated with narcotics PMH: COPD, OA, HTN; Ht 5’3’’, Wt 55kgInsurance: Medicare, per social work in the donut holeHospital Course: Rapid defervescence after empiric therapy
- Empiric therapy: vancomycin and piperacillin/tazobactam- Micro:
Enterococcus faecalis is ampicillin susceptibleCleared blood cultures within 48 hours
- ID consult De-escalated to ampicillin continuous infusionAnticipated duration: 14 days from 1st negative blood culture
14

10/8/21
8
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self Assessment Question 1.
She is now on D12 of therapy after the first negative blood culture with a negative transesophageal echocardiogram (TEE) and ID is trying to help with outpatient IV therapy. Her ALF will not approve ampicillin or ampicillin/sulbactam for stability/nursing reasons. ID consults pharmacy for PO options. Which of the following options would be BEST for this 75 yo patient in the Medicare donut hole?
• Ampicillin 500mg PO q 6 h x 14 days• Amoxicillin/ clavulanate 875/125 mg PO bid x 12 days• Cephalexin 500mg PO q 6 h x 12 days• Daptomycin 10mg/kg IV q24h
15
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Optimizing Pharmacokinetics (PK) and Pharmacodynamics (PD) in
Complicated Bacteremia
16

10/8/21
9
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
When Patients Don’t Read the Textbook…. Examples of When Source Control Isn’t An Option
Patient
• Not a surgical or transplant candidate• Surgical complications already
exist• Foreign device dependent
• Ex: can’t do a line holiday, ICD dependent, etc.
• Challenging social situations
Bug/ Disease
• Hardware +/- biofilm• Not big enough of a fluid
collection to drain• Comorbidities +/- drugs that
impair immune function
17
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
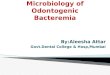
In-Vitro See-Saw Benefit of Combination Therapy with Daptomycin and Beta-lactams
Daptomycin uses calcium to become positively charged then binds to negative
phospholipids in the cell membrane
Monotherapy Mechanism of Action
Combination Therapy Mechanism of Action
Beta-lactams decrease cell positivity allowing a stronger attraction between
daptomycin and the negative phospholipidsMunita et al. Chapter 31 Daptomycin and Quinupristin-Dalfopristin.. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition.; Jenson et al. Antimicrob Agents Chemother 2020;64(9):e00890-20; Mehta et al. Antimicrob Agents Chemother 2012;56(12):6192-200
18

10/8/21
10
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
In-Vivo Controversial Combinations for Clearing Bacteremia with Staphylococcus aureus
Blood Culture Clearance
Daptomycin+ ???
MSSA
MRSAMethicillin Susceptible
Staphylococcus aureus (MSSA) Bacteremia:
Rifampin + gentamicin + nafcillinfor endocarditis
X Beta-lactam + daptomycinX DASH trial: daptomycin + anti-
staphylococcal beta-lactam CAMERA-2: flucloxacillin + vancomycin or daptomycin
Methicillin Resistant Staphylococcus aureus (MRSA)
Bacteremia:
Rifampin + gentamicin + vancomycin for endocarditis
X Beta-lactam + daptomycinDaptomycin + ceftarolineDaptomycin + fosfomycin (IV)
Grillo, et al. Clin Infect Dis 2019;69(9):1480–8; Jorgensen, et al. Clin Infect Dis 2020;71(1):1–10; Cheng, et al. Clin Infect Dis. 2021;72(9):e196-e203; Tong, et al. JAMA. 2020;323(6):527-537. Baddour, et al. Circulation. 2015 Oct 13;132(15):1435-86; Geriak, et al. Antimicrob Agents Chemother. 2019;63(5):e02483-18. Pujol, et al. Clin Infect Dis. 2021;72(9):1517-1525
19
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Combination vs Monotherapy for Gram Negative Resistant Organisms• Empiric therapy -> Antibiogram!• Combination vs monotherapy anti-Pseudomonal agents
• Balance of efficacy and safety• Determined by local resistance rates• Optimize PK/PD where possible
• Ex: extended interval dosing for concentration-dependent aminoglycosides, extended intervals for time-dependent beta-lactams to overcome intermediate resistance
• Organisms that typically require combination therapy• Acinetobacter baumanii• +/- carbapenem producing Enterobacterales
Tamma et al. Clin Infect Dis. 2021;72(7):e169-e183
20

10/8/21
11
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Indulge With Extended and Continuous Infusions
Plasma Concentration
Time
Minimum Inhibitory Concentration (MIC)
Time > MIC
Cp
AUC / MIC
Cp / MIC
Spellburg B. Chapter 17 Principles of Antiinfective Therapy. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition. Pai MP, et al. Chapter 19 Pharmacokinetics and Pharmacodynamics of Antiinfectives Agents. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition.
21
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
The Goal for Beta-lactams is to Have the Drug Concentration Above the MIC Around Half of the Dosing Interval
Plasma Concentration
Time
MIC
Beta-lactam Goal % of Time > MIC = ~ 50%
Lepak AJ, et al. Chapter 21 Cephalosporins. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth Edition.
22

10/8/21
12
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Biofilm Bonanza
Biofilm Penetration
• Rifampin• Combination
therapy
Lock Therapy
• Ethanol locks• Antibiotic locks
Novel Agents
• Bacteriophage therapy
• Photodynamic therapy
• Nanoparticles• Anti-platelet drugs
Sticky Bug Conglomeration Slimy Biofilm
Lancellotti P et al. JAMA Cardiol. 2019;4(6):596-599; Hoiby N et al. Clin Microbiol Infect. 2015;21 Suppl 1:S1-25; Suresh MK, et al. Int J Med Microbiol. 2019;309(1):1-12; Hu X et al. Front Microbiol. 2018;9:1299; Haddad LE, et al. Clin Infect Dis. 2019;69(1):167-178; Fabijan AP, et al. Nat Microbiol. 2020;5(3):465-472; Chegini Z, et al. Ann Clin Microbiol Antimicrob. 2020;19(1):45.; Aslam Curr Opin Infect Dis. 2020;33(4):298-303. Gordilloa Altamirano FL et al. Clin Microbiol Rev. 2019;32(2):e00066-18; Caflisch KM, et al. Expert Rev Anti Infect Ther. 2019;17(12):1011-1041
23
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self Assessment Case 2.67 yo M is being transferred from an acute care hospital to your skilled nursing facility on treatment for ventilator associated pneumonia secondary to Pseudomonas aeruginosa.
Drug MIC Interpretation
Ceftazidime ≥ 32 R
Cefepime ≥ 32 R
Ciprofloxacin ≥ 2 R
Gentamicin ≥ 16 R
Meropenem 4 I
Piperacillin/ tazobactam
> 64/4 R
Tobramycin ≥ 16 R
PMH: DM, COVID 8 mo ago with significant residual lung disease, HFpEF, LVAD, not a transplant candidate
Ht 6’7’’, Wt 120kg (dry), other labs WNL for chronic disease states
Hospital Course: - Empiric therapy: vancomycin +
piperacillin/tazobactam + tobramycin- ID prescribed meropenem 2g IV q8h as an
extended infusion over 4 hrs
BAL Culture: Pseudomonas aeruginosa
24

10/8/21
13
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self Assessment Question 2. Your facility has a policy against q8h medications because of the nursing requirements and asks you if it’s really needed for this patient. Which of the following is the BEST rationale for why this patient requires 2g as an extended infusion q8h.
A. Meropenem has a post antibiotic effect time that allows it to be dosed q12h so this patient should be changed to 2g IV q12h
B. Carbapenems are AUC > MIC dependent and must be dosed this way with therapeutic drug monitoring
C. The patient should be transferred back to the hospital to complete treatment with meropenem or be switched to extended interval aminoglycoside like tobramycin
D. 2g of meropenem is needed to overcome the intermediate MIC; extended infusions are needed to reach the target time > MIC of ~ 50%
25
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Glycopeptides and Lipoglycopeptides and
Bacteremia
26

10/8/21
14
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Full Circle• Drug of choice for MRSA infections = vancomycin
• 2009 guideline recommendation(s)• No more vancomycin peak levels • Targeting AUC/MIC of 400 or greater• Trough concentration of 15 – 20 mcg/mL acts as surrogate marker
• 2020 guideline recommendation(s)• Trough-only monitoring targeting 15 – 20 mcg/mL is no longer
recommended
Rybak et al. Clin. Infect. Dis. 2020;71(6):1361-1364
27
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Preferred Dosing Methodology???• Bayesian statistics• Draw peak at least 1 hour after the end of infusion• Draw trough level at end of the dosing interval
• With a large sample of vancomycin data loaded into the Bayesian prior, it may be sufficient for a lone vancomycin trough level to estimate AUC
• PK equations drawing levels at steady state• Draw peak level at least 1 hour after the end of infusion• Draw trough level at end of the dosing interval
Rybak et al. Clin. Infect. Dis. 2020;71(6):1361-1364Broeker et al. Clin Microbiol Infect. 2019 Oct;25(10):1286.e1-1286.e7
28

10/8/21
15
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Standard of practice – Staphylococcus aureus bacteremia
• 1st line• Parenteral antibiotics for 2 – 6 weeks• Peripherally inserted central catheter (PICC)• Outpatient parenteral antibiotic therapy program (OPAT)• Skilled nursing facility
• Exclusions from 1st line options• People who inject drugs (PWID)• Repeated discharges against medical advice (AMA)• Social, behavioral, or health system barriers
Liu C. et al. Clin. Infect. Dis. 2021;52(3):e18-e55Bork et al. Infect Dis Ther. 2019;8(2):171-184.
29
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Lipoglycopeptides
• Dalbavancin and Oritavancin have extremely long half-life’s• Found to be non-inferior to vancomycin• FDA approved for acute bacterial skin and skin structure infections (ABSSSI)
• Spectrum of activity?• Yes: MRSA, MSSA, Streptococcus, Enterococcus faecalis• Unclear: Vancomycin resistant Enterococcus, Enterococcus faecium
Medication Dose Duration & Administration Half-life
Dalbavancin 1500 mg 1 dose over 30 minutes 204 hours vs 345 hours
Dalbavancin 1000 mg x 1 dose over 30 minutes then 7 days later another dose of 500 mg over 30 minutes
204 hours
Oritavancin 1200 mg 1 dose over 3 hours 245 hours
Dalvance™ (dalbavancin) [package insert]Orbactiv™ (oritavancin) [package insert]
30

10/8/21
16
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
What does the literature say…
Citation Study design Infection Population Outcome Microbiology/Other
Raad, 2005 RCT CRBSI 33(DAL)/34(VAN) Test of cure:DAL 87% CI [73.2 – 100%]VAN 50% CI [31.5 – 68.5%]
MSSA, MRSA, CoNS, Enterococcus faecalis
Redell, 2019 Retrospective observation
SSTI/bacteremia N= 401/9 (ORI) Clinical success:89%/100%
Cohort n = 32 received multi-dose with clinical success 93.8%
RCT: randomized control trial, CRBSI: catheter related blood stream infection, DAL: dalbavancin, VAN: vancomycin, MSSA: methicillin-susceptible Staphylococcus aureusMRSA: methicillin-resistant Staphylococcus aureus, CoNS, coagulase-negative Staphylococci, ORI: oritavancin, SSTI: skin and soft tissue infection
Raad I. et al. Clin. Infect. Dis. 2005; 40:374-80Redell M. et al. Open Forum Infect Dis. 2019;6(11):ofz479
31
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Lipoglycopeptides in practice
• Increasing amount of literature supporting use in additional infections• Osteomyelitis• Osteoarticular joint infections• Bacteremia• Infective Endocarditis
Medication Dose Duration Half-life
Dalbavancin 1500 mg 1 dose every 14 days 204 hours vs 345 hours
Oritavancin 1200 mg 1 dose every ~9 – 14 days
245 hours
Ajaka et al. Antibiotics. 2020 Oct 15;9(10):700.Redell et al. Open Forum Infect Dis. 2019;6(11):ofz479
32

10/8/21
17
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Lipoglycopeptides clinical pearls
• Patient(s) selection• Gram positive infection• Social, behavioral, or health system barriers, frequent AMAs, or PWID• Documented negative blood cultures prior to therapy initiation
• Poor outcomes for PWID with IE
•What risks are there in treating these patients?
Ajaka et al. Antibiotics. 2020 Oct 15;9(10):700. Schranz Clin Infect Dis. 2020;71(3):572-573Bork et al. Infect Dis Ther. 2019;8(2):171-184 Redell et al. Open Forum Infect Dis. 2019;6(11):ofz479
33
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Patient Case #3
• RW is a 62-year-old male who presented to the ED after experiencing 5 days of shortness of breath, chills, weakness, and decreased appetite. The ED provider noted suspected needle tracks on RLE with associated erythema. Patient admits to using IV meth and “missed his mark about 7 days ago”. • PMH: Polysubstance dependence, PWID, Hypertension, Diabetes
mellitus, Seizures, HFrEF, Hyperlipidemia, MDD, PTSD• Vitals: T 98.9⁰F; BP 148/53; HR 118; RR 29 • Labs: WBCs 24.7; bands 18%; SCr 0.66 mg/dL, Lactic acid 3.0• UA: WBCs 21-30, RBCs 3-5, LE large, nitrite negative
34

10/8/21
18
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Patient case #3
• Urine and blood cultures identify the following bacterial isolate: MRSA
• Repeat blood cultures are 5 days negative today and RW is threatening to leave AMA
• Transition of care pharmacist reports that patient is only adherent with his prazosin, citalopram, and carvedilol medications
35
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self-Assessment Question 3
Identify the optimal antimicrobial agent for RW.
A. Vancomycin 750 mg IV every 12 hour for 9 daysB. Oritavancin 1200 mg IV nowC. Dalbavancin 500 mg IV now, and Dalbavancin 1000 mg IV on day 7D. Linezolid 600 mg PO every 12 hour for 9 days
36

10/8/21
19
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Microbiological Nuance and Bacteremia
37
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Culture of Culturing
• Pathogen or contaminant?
• Ideally draw blood cultures prior to antibiotic therapy
• Blood culture technique1. Disinfect skin for venipuncture2. Disinfect bottle top tubes3. Allow to dry4. 2 or 3 blood culture sets from separate venipuncture sites
approximately 15 minutes apart
Septimus Ed. https://www.cdc.gov/antibiotic-use/core-elements/collecting-cultures.html.
38

10/8/21
20
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Blood culture – what now?
• Typically each set of blood cultures have two different tubes• Aerobic tube filled 1st with anaerobic tube filled 2nd
• Laboratory confirmed bloodstream infection1. One positive blood culture with recognized pathogen2. Skin flora present in two or more cultures drawn on separate occasions for
identical organism plus clinical symptoms• Skin flora examples: Staphylococcus epidermidis, Staphylococcus hominis,
Staphylococcus capitis, Micrococcus, Bacillus species…etc
Septimus Ed. https://www.cdc.gov/antibiotic-use/core-elements/collecting-cultures.html.
39
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Culture of Culturing – Catheter site
• Central vascular catheters (CVCs)
• Blood culture technique1. Disinfect skin for venipuncture2. Disinfect bottle top tubes3. Allow to dry4. 1 or 2 blood culture sets from separate venipuncture sites
approximately 15 minutes apart and an additional set of blood cultures through the catheter device or line
Septimus Ed. https://www.cdc.gov/antibiotic-use/core-elements/collecting-cultures.html.
40

10/8/21
21
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Catheter-related blood stream infection (CR-BSI)?
• Laboratory suspected CR-BSI• Both cultures from catheter and venipuncture must be positive for same
organism with clinical signs and symptoms and no other recognized source
• Laboratory suspected contaminant• Positive culture from the catheter with negative venipuncture culture• Positive cultures from the catheter for organism A and organism B from
venipuncture
• Catheter tip culture alone are not diagnostic for CR-BSI
Septimus Ed. https://www.cdc.gov/antibiotic-use/core-elements/collecting-cultures.html.
41
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
CR-BSI Pathogenesis
• Recognized routes• Migration of skin organisms into the cutaneous catheter tract and
colonization of catheter tip• Direct organisms cross-contamination of catheter from non-sterile source• Hematogenous catheter seeding from alternative source• Contaminated fluid infusion e.g. non-sterile admixture or compounding
Grady et al. Clin. Infect. Dis. 2011;52(9):e162-93
42

10/8/21
22
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Recognized blood stream pathogens
Gram Positive bacteria
• Staphylococcus aureus (20 – 25%)
• Enterococcus species (5 – 10%)
• Streptococcus pneumoniae (2 – 4%)
• Streptococcus agalactiae (2%)• Other Streptococcus species (~1%)
Gram Negative bacteria
• Escherichia coli (10 – 19%)
• Klebsiella species (6 – 8%)
• Pseudomonas (5%)
• Enterobacter (2 – 3%)
• Proteus mirabilis (~1%)
Grady et al. Clin. Infect. Dis. 2011;52(9):e162-93Diekemia et al. Antimicrob. Agents Chemother. 2019;63(7): e00355-19Lutwick L, et al. In: Memish ZA. Guide to Infection Control in the Healthcare Setting. Brooklyn, MA: International Society for Infectious Diseases
43
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Recognized blood stream pathogen - Yeast
Grady et al. Clin. Infect. Dis. 2011;52(9):e162-93Lutwick L, et al. In: Memish ZA. Guide to Infection Control in the Healthcare Setting. Brooklyn, MA: International Society for Infectious Diseases
• Represents challenging cause of sepsis and septic shock
• High degree of morbidity and mortality
• Account for 10% of BSIs• Risk Factors: CVCs, abdominal
surgeries, abdominal perforations, broad spectrum antibiotics, neutropenic
Candida species
• Commonly isolated from urinary and pulmonary cultures and not typically considered pathogenic in these settings
Why so challenging???
44

10/8/21
23
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Containment(s) or Pathogen?• Laboratory confirmed bloodstream infection
2. Skin flora present in two or more cultures drawn on separate occasions for identical organism plus clinical symptoms
Coagulase negative Staphylococcus
• Most isolated BSI organism(s)
• Represents challenging differential
• Skin flora
• Accounts for up to 31% of BSIs
Grady et al. Clin. Infect. Dis. 2011;52(9):e162-93Becker et al. Clin Microbiol Rev. 2014;27(4):870Wisplinghoff et al. Clin Infect Dis. 2004;39(3):309-317
Lutwick L, et al. In: Memish ZA. Guide to Infection Control in the Healthcare Setting. Brooklyn, MA: International Society for Infectious Diseases
45
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Patient case #4
• Patient KS is a 56-year-old female who presented to the ED for worsening RLE erythema surrounding a diabetic foot ulcer. Blood cultures were drawn and an MRI was obtained that is negative for osteomyelitis – an ulcer is seen in the plantar soft tissues with surrounding soft tissue edema which may represent cellulitis. Patient declined admission and was discharged from the ED on amoxicillin/clavulanate and doxycycline.• All other laboratory data within normal limits• Blood culture 1 set of 2 sets are reported as positive
46

10/8/21
24
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Self-Assessment Question 4
After contacting the lab it was reported that 1 blood culture tube in set 1 identified S. epidermidis. All other culture tubes are no growth final result. Identify the best answer below:
A. No treatment, skin flora identified in one blood culture set and represents a contaminant
B. No treatment, skin flora identified in two blood culture sets and represents a contaminant
C. Treatment recommended, pathogen identified in one blood culture set and represents an infection
D. Treatment recommended, pathogen identified in two blood culture sets and represents an infection
47
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Coagulase negative Staphylococcus differential
• What if patient KS had both blood culture sets result positive for S. epidermidis?• Skin flora present in two or more cultures drawn on separate occasions
for identical organism plus clinical symptoms
Question Answer
Clinical symptoms present?
Skin flora present?
Skin flora present in 2 or more cultures?
Identical organism in 2 or more cultures?
48

10/8/21
25
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
Coagulase negative Staphylococcus differential
Blood Culture Set 1 Blood Culture Set 2
Camerer et al. J Clin Microbiol. 2011 Sep;49(9):3355-7Seybold et al. Infection. 2009 Jun;37(3):256-60Al Wohoush et al. Clin Microbiol Infect. 2011 Apr;17(4):569-71
49
2021 Annual Meeting & ExhibitionNovember 4-7, 2021 | San Diego, California
BSI – Clinical Pearls• Staphylococcus aureus always considered pathogenic from any site
• If cultured from urinary source BSI should be ruled out
• Candida identified in blood culture is a pathogen• Certain skin floral considered S. aureus “like” in virulence and
propensity to cause infection: S. lugdunensis• Bacteria isolated in blood culture can help provider key in on source
• Intra-abdominal: Enterococcus, poly-microbial, Bacteroides• Urine: Enterobacterales• Pulmonary: S. pneumoniae, H. influenzae• Unknown source?
Becker et al. Clin Microbiol Rev. 2014;27(4):870Frank et al. Clin Microbiol Rev. 2008;21(1):111
50