Embed Size (px)
Citation preview

Title Self-cleaning vascular shunts for battlefield-treatment of combat trauma
1. Optimized Vascular Shunts for Prolonged Field Care
2. Thrombosis-resistant shunts for major vascular injury in Prolonged Field Care
Principal Investigator Sachin VelankarDept. of Chemical EngineeringUniversity of PittsburghPittsburgh PA 15261Phone: 412-624-9984Email: [email protected]
This White Paper is submitted pursuant to the RPP MTEC-17-08-Multi-Topic
Care of combat casualtiesDate of Submission 09/28/2017
Non-traditional Defense contractor University of Pittsburgh
Willingness to allow MTEC Officers access to your White Paper for the purposes of engaging in out-reach activities with private sector entities : YES
MTEC Member Yes
We are allowed five pages including this cover page. References need to fit within these five pages. So right now about quarter or half page over. But the animal experiment section needs to change alto-gether
Can you do the following:
1. address comment #3 (just verifying that the sentence is right) 2. address comment #7 (which will take a good 15 minutes). The current experimental paragraph
(lifted from the NIH) refers to grafts. But it need to be rewritten for shunts. If you are too busy with this, skip it. I will request Tzeng to fill in.
3. Send this to Drs. Elias and Watson. First, they should make sure that I am not misrepresenting their affiliations. Second, if they are able to read through the first page especially, it would be very useful.
1

2

Specific area of interest: Care of combat casualties Title I WILL REPEAT TITLE HEREPrincipal investigator Sachin Velankar, University of Pittsburgh
1. Background & military relevance We have discovered that a change in surface topography (i.e. a smooth surface becomes rough or vice versa) can force deadhesion of adlayers that form on surfaces. Blood contact experiments show that soft synthetic tubular conduits whose inner surfaces undergo such changes in topography (dubbed TopoGrafts) show greatly reduced platelet adhesion. We propose translational research to develop TopoGrafts, chiefly as vascular shunts for treatment of wartime trauma injuries, and secondarily as vascular grafts for bypass reconstruction.
Major vascular injury is common in the complex poly-trauma seen in modern combat situations1, 2, but its management can be radically different from that in civilian settings2, 3. In most civilian trauma, a major vascular injury, e.g. penetrating trauma proximal to the knee or elbow, is under ATLS guidelines automatically classified as a level 1 alert. The patient is rapidly transported to a major resource-rich level 1 trauma center where a trauma surgeon can rapidly assess the patient and mobilize sub-specialists such as vascular surgeons. Accordingly, the preferred approach to major vascular injury in a civilian setting is primary surgical repair and/or bypass with autologous vein graft, an approach that has recently been reviewed by our own institution (UPMC) with a busy level 1 center3. In contrast, in military settings, vascular injury management depends on resource availability. Level 3 facilities (Army’s combat support hospitals and the Air Force’s theater hospitals) function like a civilian level 1 trauma center1, 2. However with the diverse multi-centric nature of many of our current conflicts, increasing pressure is placed on military surgeons to provide prolonged care in austere resource-poor environments (level 2 care). In these settings, the mainstay of operative management of major vascular trauma is vascular shunting with the principle of restoring distal blood flow while obtaining hemorrhage control1-3. Shunts placed in larger caliber extremity vessels (> 4mm) such as common femoral, superficial femoral, and brachial arteries have shown to be efficacious modalities leading to limb preservation once definitive repair can be undertaken at a higher level of care. The two major complications of shunts include thrombosis and dislodgment. Multiple researchers have reported that the rate of these complications, especially thrombosis, increases with the time a shunt must stay in-situ, and also with the decrease in caliber of the arteries being shunted1, 2. The duration for which a patient needs to be cared for under austere forward deployment circumstances also varies by service branch. For instance an Air Force expeditionary medical support unit may have access to rapid evacuation to a level 3 hospital, while a forward surgical team embedded with a US Army special operations team may not. Furthermore, the challenge of conflicts such as Afghanistan where air superiority is not always established limits the ability to transport injured soldiers to higher levels of care. For these reasons, novel technologies need to be developed to optimize shunt performance. Current shunts are simply adapted from civilian use where shunting is mostly utilized in operations on at-risk vascular beds, such as the carotid artery, for short periods (few hours), usually in a fully anti-coagulated patient. In contrast, in the military field care setting, a shunt may need to function for days in a patient who receives no systemic anti-coagulation due to their potential other injuries, especially close head injuries that cannot be ruled in austere environments given lack of CT capabilities. No current shunt design meets these needs. Furthermore, there is unmet need for shunts designed to function in smaller caliber vessels which have dismal failure rates. For instance, over 24 hour timescales thrombosis rates in > 4mm arteries is < 20% while in smaller distal arteries it approaches > 90%3. Thus any existing shunt placed in a smaller vessel for any prolonged period of time is highly likely to occlude. While it is often believed that distal vessel ligation does not increase risk for major amputation, limb salvage does not equate to preserved optimal limb function once healing has occurred. Some of our data experience form a civilian setting suggest decreased limb functional outcomes with distal vessel ligation. Decrease functional outcomes are of heightened importance in military settings, where soldiers rely on top physical performance for their job. Finally, with increasing number of women serving our country, there is need to optimize performance in smaller blood vessel sizes. Distal SFA/popliteal arteries in women are known to be smaller than in men: 4-6mm versus 5-7mm4. Current shunts would likely have
3

0
30000
60000
non-actuatedflat silicone
I II III
platelets deposited per mm
2
A
B
1 cm
100 mm Hg 200 mm Hg
C
50 mm Hg
D
poorer performance in such vascular beds, increasing the risk of limb loss the injured female soldiers.
In summary, civilian practice does not address the DoD’s need for new kinds of vascular shunts which would remain patent for longer periods in smaller caliber vascular beds. Indeed, the MTEC recently solicited proposals for the Permanent Vascular Repair (PVR) program to address these needs. Our technology focuses on developing vascular conduits (shunts or grafts for formal reconstruction) with a self-cleaning mechanism that prevents platelet adhesion and thrombosis on the conduit surface, allowing for improved patency in difficult vascular beds such as an injured vessel, small caliber target, or patient incapable of receiving anti-coagulation or anti-platelet medications. This approach can be applied to a variety of applications including long-functioning shunts, vascular grafts or dialysis access grafts for improved patency.
2. Approach Current arterial shunts are made of PVC or silicone, which although flexible, are still much stiffer than arteries. Prosthetic grafts are made of PTFE or polyester (“Dacron®”), which are even stiffer. But apart from this “compliance mismatch”, they also lack two key features of natural arteries. First, arteries expand and contract about 10% between systole and diastole during every heartbeat whereas prosthetics are too stiff to pulsate with blood pressure. Second, arteries have a highly corrugated lumen, and evidence suggests that the diameter changes cause continual transition between a more and a less wrinkled state5. We will refer to these two phenomena as diameter pulsation and dynamic topography respectively.
Inspired by natural arteries, we tested whether surfaces with diameter pulsation and dynamic topography could resist platelet adhesion and thrombus formation better than analogous static surfaces. Early experiments showed excellent promise6 with dynamic surfaces showing up to 97% decrease in platelet deposition as compared to the same surfaces helt static.
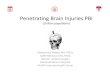
In subsequent experiments, we constructed soft cylindrical tubes, TopoGrafts, with a wrinkled lumen (Fig. 1A). Pressurizing and depressurizing the TopoGrafts induced diameter plusation, which in turn induced dynamic topography at the luminal surface (Fig. 1B&C). TopoGrafts were then subjected to pulsatile blood flow. Once again, diameter pulsation and dynamic topography both greatly reduced platelet fouling (Fig. 1D), but furthermore, smaller wavelengths were be more effective in reducing fouling. Very limited animal experiments support the same conclusion.
Fig. 1: A. Tubular conduit with wall slit to illustrate the two-layer structure. B. Optical coherence tomography (OCT) image of the cross section of cylindrical silicone tube showing how the wrinkles become less prominent as internal pressure inflates the tube. C. Platelet deposition after blood contact of tubular samples with various internal wavelengths. The control sample (left) was static. The others were inflated and deflated continuously throughout blood contact. D. Simulation of how adlayer as it builds up elastic energy of deformation, which drives deadhesion.
One potential explanation for this result relies on the mechanics of adhesion of soft bodies such as thrombus onto a surface. Briefly, the thrombus (treated as a soft elastic film in simulations, Fig. 1E), seeks to conform to the changing geometry of the surface, but this increases its elastic energy. Eventually, the elastic energy overcomes the adhesion energy, thus inducing deadhesion. This model is in semi-qualitative agreement with experiments7. Other phenomena, e.g. the influence of topography on the fluid mechanics of blood flow, may also contribute to the reduced fouling.
4

100 um
3 mm i.d.
Innovation: Our approach exploits an entirely new anti-thrombotic mechanism based on “mechanical” aspects of adhesion rather than the “chemical” modification approaches that have had only a modest effect on long-outcomes. TopoGrafts can readily be combined with existing chemical modifications like heparin bonding for synergistic effects, where the active topography keeps the chemically modified surface clean for better long term efficacy8, 9. We emphasize that such TopoGrafts are practical only if diameter pulsation and dynamic topography appear passively, i.e. without external power sources. We propose to use the natural pulse, i.e. systolic to diastolic pressure variations, as a power source.
3. Objectives The goals of the proposed research are (1) to develop grafts capable of dynamic topography using FDA-approved materials, (2) scale up their manufacture to a reliable, reproducible, and tunable process, (3) test these grafts in large animal models, and (4) initiate the process for FDA approval as a Class II device.
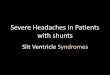
3.1. Technical strategy Materials and design approach: Translation towards clinical practice requires FDA-approved materials, rather than the industrial-grade materials used in our previous research. Calculations suggest that systole-diastole pressure variations can realize 10% diameter pulsations if conduit walls have a modulus of 0.1 MPa. A few commercially-available implantable silicones which can realize this value will be used in our research. A heavily wrinkled luminal topography will be realized (as in our previous experiments) by bonding a few-micron-thick layer of stiff silicone to the lumen of the conduit under strain mismatched conditions. This approach has the advantage of easy manufacturability since micron-scare topography can be realized without micropatterning equipment. We have already selected suitable materials and developed laboratory methods of achieving the desired structure (Fig. 2).
Fig. 2 Cross section of a seamless conduit with wrinkled luminal topography (middle image). Far right shows the luminal topography of a real artery in fluorescence.
Scalable manufacturing: Our lab-based manufacturing techniques have too much variability to be acceptable for any significant translational efforts. We propose to sub-contract with a silicone device contract manufacturer to ensure reproducible quality. Briefly, fluoroelastomeric tubes (serving as inflatable mandrels) will be dip-coated with a solution of the stiff layer under inflated conditions. The mandrel will be deflated, and a thicker layer of the softer material will be overmolded onto the surface. Apart from the use of the inflatable mandrel, this is a standard overmolding process, and informal conversations with contract manufacturers of medical silicone devices suggest no exceptional issues. The design process will be guided by simulations. The measured mechanical properties of the different materials will be used to predict the geometric parameters that will give the desired diameter pulsation and surface topography within the desired pressure range. Fabrication will be followed by surface functionalization with polyethylene glycol or albumin to make the surfaces more biocompatible using standard flow-through methods10.
Experiments: The as-manufactured TopoGrafts will first be tested and optimized in vitro using methods developed in our previous research to verify that varying luminal pressure in the normal blood pressure range (70-140 mm Hg) induces the desired 10% diameter pulsation, and dynamic topography. The latter will be verified with an optical coherence tomography (OCT) catheter as done for Fig. 1B.
Optimized TopoShunts will be tested in two animal model systems: acute hemorrhagic shock non-survival pig model (with which our institution has extensive experience) and a short-term survival pig model. We propose a total of 6 animals/group. In the non-survival group, hemorrhagic shock is induced via standard protocols and the animal subsequently resuscitated, after the resuscitative stage bilateral
5

carotid arteries will be exposed with one side shunted using TopoShunt and the other a standard commercially available shunt (Argyl Carotid Shunt, Medtronic). Patency will be monitored using duplex US throughout the resuscitative stage of the animal upwards to 24 hours. The importance of testing our product in a shock model comes from extensive clinical knowledge that hemorrhagic shock can induce sever coagulopathies, which come to the forefront in the first 24-48 hours post-injury. After 24 hours, the animals will be euthanized and the shunts explanted and their surfaces characterized for platelet/thrombus adhesion using SEM. The second group of animals will undergo more traditional interposition grafting using bypass technique, the incisions will be closed, and animals kept alive for a duration of 1 week. Graft patency will evaluated daily using duplex US. The purpose of this group is to compare longer term patency in a normotensive animal.
Optimized TopoGrafts will be implanted into sheep common carotid arteries (CCA) as interposition, end to end grafts. Control implants will be placed in the left CCA and will include similar grafts with a smooth lumen as well as standard PTFE grafts (N=6/group). Diameter changes between systole and diastole will be quantified from video recordings of the implants and the native arteries adjacent to the grafts. CT angiograms immediately after the implant will establish a baseline evaluation of patency and anatomic features of the anastomoses. Biweekly duplex imaging of the carotid arteries will determine graft patency. If one graft is thrombosed but the other graft is patent, we will continue to observe the animal until the 1 month time point in initial experiments. If both grafts are occluded, the animal will be euthanized and the grafts will be isolated for analysis. At 1 month, animals will be anesthetized and the grafts exposed. Vessel/graft diameter pulsations will be re-quantified by video and compared to the baseline measurements to look for any evidence of graft fatigue over time. OCT imaging will be used to examine the perianastomotic regions and the graft itself. Luminal surface changes will be examined, focusing on the behavior of the wrinkles with pulsation and on platelet and thrombus accumulation in the graft. After this, the grafts will be excised with a 1 cm cuff of native artery proximal and distal to the graft. The mid-graft will be used for SEM to examine the accumulation of surface platelets, thrombus and other foulants. The distal anastomotic region will be used for immunostaining to look at neointima formation and for thrombus formation.
[3.2.] Anticipated outcomes At the end of this grant, we will have (1) scalable, reproducible, and tunable manufacturing of a new kind of vascular conduit which mimics the compliance, distensibility, and dynamic topography of natural arter-ies, and (2) validation from animal studies that these conduits have superior antithrombotic properties and patency as compared to existing shunts. In summary, this grant will allow TopoGrafts to translate from an idea that has only been proven in vitro to one with adequate animal implant data for an FDA application.
3.2.[3.3.] Technology readiness level & Commercialization strategy This technology is presently at TRL3. Using current funding, by the end of 2017, we expect to have performed limited animal experiments using the conduits of Fig. 2, bringing us at or close to TRL 4. By the end of this proposed project, we anticipate being at TRL5, and anticipate having filed a 510(k) premarket submission to the FDA as a Class II device for permission to conduct small-scale human trials.
Intellectual property will be protected via patents (one provisional patent will be converted into a non-provisional patent in Oct. 2017). Our team recently participated in an NSF I-Corps technology commercialization program to fully understand the technical and economic ecosystem of vascular conduits. We anticipate starting a company to commercialize this technology within 12 months. The same technology can be applied to improve vascular grafts for treating arterial disease or for dialysis access, both of which face patency problems, albeit over longer durations than shunts. Thus this project offers tremendous subsidiary benefits to the civilian and VHA population and improves prospects for commercialization.
4. Participants, Period of performance, and Rough budget Dr. Sachin Velankar, Assoc. Prof., Chemical Engineering, expert in polymer science with wide-ranging knowledge of materials selection and fabrication, will coordinate the overall project. Dr. Edith Tzeng,
6

U. Pittsburgh and Chief of Vascular Surgery at the VA Pittsburgh Healthcare System is an expert on in translational vascular research, large animal models, and clinical vascular reconstruction, and will conduct animal experiments. Dr. Luka Pocivavsek, surgeon with expertise in mechanics, will conduct all the simulations needed to guide the graft design. Dr. Gregory Watson, Asst. Prof. of Surgery at Pitt & Lt. Col, United States Army Reserve and Dr. Garth Elias, Assoc. Prof. of Surgery & Col. United States Army Reserve, have both served in Iraq and Afghanistan and will advise on the military needs of shunts, and how they differ from civilian practice. Mr. Joseph Pugar, Entrepreneurial Fellow, Innovation Institute will leading the commercialization effort. He led our participation in the NSF-I-Corps program mentioned above and also conducted some of the preliminary research cited in Section 2. One post-doctoral fellow will be recruited for coordinating the fabrication efforts and assisting with animal experiments.
The research will be conducted over ## years with the following approximate budget.
LaborMaterialsEquipment / fabricationSurgery costsAnimal costs
References
1. Rasmussen, T.E., et al., The use of temporary vascular shunts as a damage control adjunct in the management of wartime vascular injury. Journal of Trauma-Injury Infection and Critical Care, 2006. 61: p. 8.
2. Rasmussen, T.E. and C.J. Fox, Chapter 160: Vascular Trauma: Military, in Rutherford’s Vascular Surgery. 2014, Elsevier.
3. Abou Ali, A.N., et al., Vascular Shunts in Civilian Trauma. Frontiers in Surgery, 2017. 4.4. Wolf, Y.G., Z. Kobzantsev, and L. Zelmanovich, Size of normal and aneurysmal popliteal arteries:
A duplex ultrasound study. Journal of Vascular Surgery, 2006. 43: p. 488.5. Greensmith, J.E. and B.R. Duling, Morphology of the constricted arteriolar wall - Physiological
implications. American Journal of Physiology, 1984. 247: p. H687.6. Pocivavsek, L., et al., Active wrinkles drive self-cleaning: Anti-thrombotic surfaces for vascular
conduits. submitted.7. Pocivavsek, L., et al., Geometric tools for controlling soft surface adhesion. In preparation.8. Devine, C. and C. McCollum, Heparin-bonded Dacron or polytetrafluorethylene for
femoropopliteal bypass: Five-year results of a prospective randomized multicenter clinical trial. Journal of Vascular Surgery, 2004. 40: p. 924.
9. Ye, S.-H., et al., Simple surface modification of a titanium alloy with silanated zwitterionic phos-phorylcholine or sulfobetaine modifiers to reduce thrombogenicity. Colloids and Surfaces B-Bioin-terfaces, 2010. 79: p. 357.
10. Zhang, H.B. and M. Chiao, Anti-fouling Coatings of Poly(dimethylsiloxane) Devices for Biological and Biomedical Applications. Journal of Medical and Biological Engineering, 2015. 35: p. 143.
7