Embed Size (px)
Citation preview

Bacteraemia zero: how is it possible?
MERCEDES PALOMAR
SMI H ARNAU DE VILANOVA (LLEIDA)

Objectives of nosocomial infection surveillance in
critically ill patients
• Know the rates of device-related infections acquired in ICU.
• Identify the most frequent microorganisms responsible for each surveyed infection.
• Monitor and assess multiresistance markers.
• Study of intrinsic risk factors and frequency and exposure to extrinsic risk factors.
• Outbreak detection.
• Evaluation of ICU-acquired infection’s impact.
• Study of control measures.

BACTERIEMIA PRIMARIA-CV.
NEUMONIA RELACIONADA CON VM
1 4 ,6 1 4 ,71 4 ,91 8 ,5
1 8
1 5 ,5
1 7 ,5
1 7 ,2
2 3 ,6
1 7 ,8
2 0 ,11 8 ,4
1 6 ,8
1 7 ,1
1 6 ,1
0
5
1 0
1 5
2 0
2 5
199
4
199
5
199
6
199
7
199
8
199
9
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
8
D E N S ID A D D E IN F E C C IO N D E N -V M
N-VM /1000 días de VM
TASA MEDIA NACIONAL
14,6-23.6 o/o o
ICU-ACQUIRED INFECTIONS.
ENVIN-HELICS 1994-2008
INFECCION URINARIA RELACIONADA CON SU
6,9
5,5 5,56
4,9
5,96,7
5,11 5 4,76
6,67,4
6,15,8
6,8
0
1
2
3
4
5
6
7
8
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
TASA MEDIA NACIONAL
4,9-7.4 (O/OO)
INFECCION URINARIA-SU / 1000 DÍAS DE SONDA URETRAL
6,776,22
7,7
6,8
7,947,49
5,044,7 4,89
4,013,67
4,54,02
4,73 4,46
3,19 3,1 3,05
0
1
2
3
4
5
6
7
8
9
10
2000 2001 2002 2003 2004 2005 2006 2007 2008
Nº/
100
0 d
BP-CV (CVC) BP-CV (CVC+CA)
TASA MEDIA NACIONAL
5.09-7.9 (O/OO)
Consolidated surveillance
Rates: no reduction
VENTILATOR ASSOCIATED PNEUMONIA
CATHETER RELATED BACTEREMIA URINARY TRACT INFECTION-UC

PRIMARY BACTERIEMIA (CVC +UNKOWN ORIGEN)
6,776,22
7,7
6,8
7,947,49
5,044,7 4,89
0
1
2
3
4
5
6
7
8
9
10
2000 2001 2002 2003 2004 2005 2006 2007 2008
Nº/
100
0 d

PRIMARY BACTERIEMIA (CVC +UNKOWN ORIGEN)
6,776,22
7,7
6,8
7,947,49
5,044,7 4,89
0
1
2
3
4
5
6
7
8
9
10
2000 2001 2002 2003 2004 2005 2006 2007 2008
Nº/
100
0 d
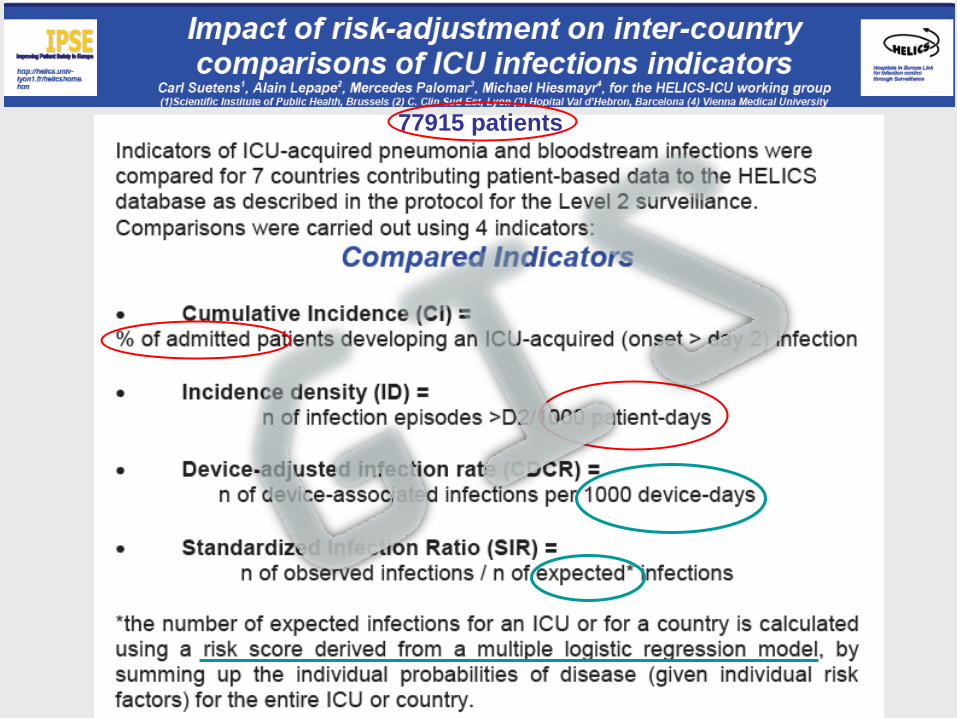
77915 patients


NOSOCOMIAL INFECTIONS
SURVEILLANCE PROGRAMS
• Whatever the detection, registration and reporting method, NI surveillance programs are necessary to establish corrective measures.
• NI-Surveillance Programs are relevant only if they aim at improving care

Technical Workshop on Patient Safety and
Care of Acutely Ill Patients: Changing the Paradigm Friday 22 September 2006, Barcelona



Mean from 7,7 epis/1.000 CVC days
to 1,4 after 18 months (p<0,002).

FROM SURVEILLANCE TO
PREVENTION
FROM ENVIN TO BACTERIEMIA,
PNEUMONIA & RESISTANCE-ZERO


REDUCTION OF CATHETER-RELATED BACTEREMIA IN INTENSIVE CARE
UNITS BY A MULTIFACTORIAL INTERVENTION: PILOT STUDY (2007)
Bacteriemia zero (2009-2010)

GENERAL FRAMEWORK
WHO
SMoH SEMICYUC
HR
(ICU)
BALTIMORE
agreement
agreement
Bacteriemia zero

Quality Agency SMoH
HR Department
HR Cordinating
Team Cordinator, ICU physician
ICU nurse, preventivist
ICU-1 ICU-2 ICU-n
Information, engagement
Managers commitment
Leadership
Organize: Functions
Resources distribution
Training
Monitoring
Evaluation reports: results
Structure & Process evaluation
Physician, Nurse, Executive,
infectious diseases comitee
Training
Implementation
Self-evaluation
Improvement
Cofinancing & coordination
Monitoring & spreading
NATIONAL ORGANIZATION

OBJECTIVES
• Reduce ICU CLABSI (< 4 episodes per 1000 CL days)
• Create through the HR an ICU network to apply
effective Safe Practices
• Promote Safety Culture in the Spanish ICU
• Improve CLABSI information system

• The original Keystone ICU project was adapted to fit the organizational and cultural characteristics of the Spanish health care system.
• The model to engage, educate, execute, and evaluate was unchanged and a key element of the study implementation
Bacteriemia zero
Bacteriemia zero
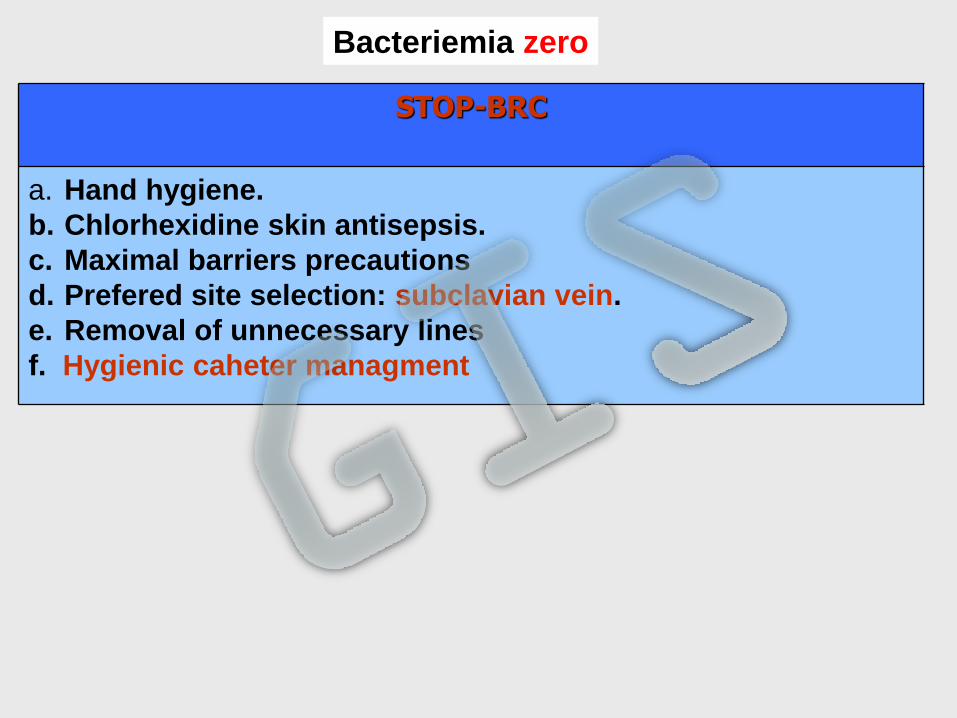
STOP-BRC
a. Hand hygiene.
b. Chlorhexidine skin antisepsis.
c. Maximal barriers precautions
d. Prefered site selection: subclavian vein.
e. Removal of unnecessary lines
f. Hygienic caheter managment
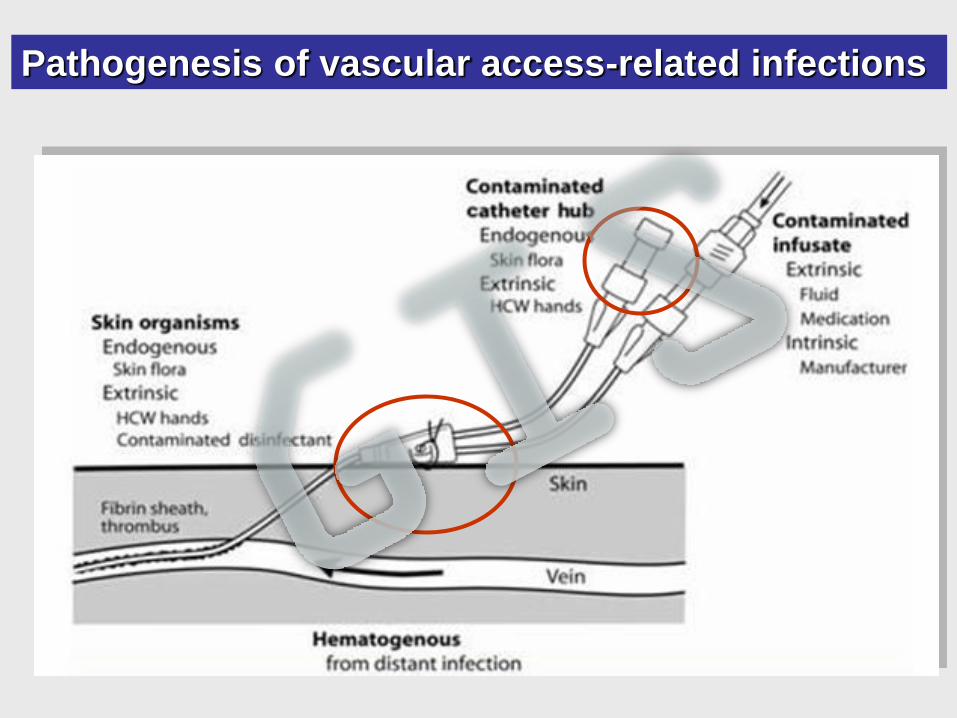
Pathogenesis of vascular access-related infections


MEDIDAS DE PREVENCIÓN BRC: EVIDENCIA 1A
1. Higiene de manos adecuada
2. Desinfección de la piel con clorhexidina
3. Máximas barreras de precaución
5. Retirada de CVC no necesarios
4. Preferencia de localización subclavia
6. Mantenimiento higiénico del catéter
Bacteriemia zero

Bacteriemia zero
Comprehensive Safety Plan
1. Evaluate safety culture
2. Education on safety culture
3. Identify defects in clinical practice
4. Establish alliances with Executive Board
5. Learn from defects
STOP-BRC
a. Hand hygiene.
b. Chlorhexidine skin antisepsis.
c. Maximal barriers precautions
d. Prefered site selection: subclavian vein.
e. Removal of unnecessary lines
f. Hygienic caheter managment

“BUNDLES “ PREVENCION BRC + CUSP
PROGRAMA DE MICHIGAN
• Hand hygiene
• Maximal barriers precautions
• Clorhexidine skin antisepsis
• Avoid femoral
• Removal of unnecessary lines
+ +
CUSP
Pronovost Pet al. Improving communication in the ICU using daily goals. J Crit Care 2003
Pronovost P. Implementing and validating a comprehensive unit-based safety program. J Patient Saf 2005.
Pronovost P Senior executive adopt-a-work unit: a model for safety improvement. Jt Cm J Qual Saf 2004.
Pronovost P, Goeschel C. Improving ICU care: it takes a team. Healthc Exec 2005
BZ IMPLEMENTATION
• Engage: local BSI cases, basal rates (locals, nationals, european)
• Educate
• Execute
– Cart line
– Check list at insertion
– Daily goals
– Learning frrom errors
– Nurse empowerment
• Evaluate
– Surveillance and feed-back (rates, check-list, safety clima)
– Consider infections = errors
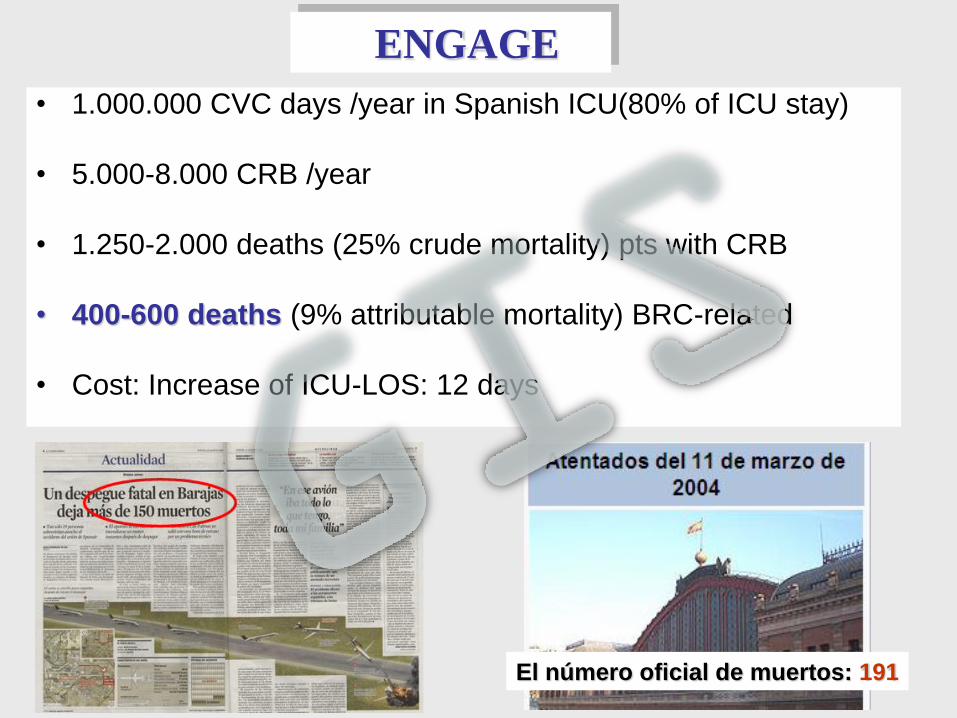
• 1.000.000 CVC days /year in Spanish ICU(80% of ICU stay)
• 5.000-8.000 CRB /year
• 1.250-2.000 deaths (25% crude mortality) pts with CRB
• 400-600 deaths (9% attributable mortality) BRC-related
• Cost: Increase of ICU-LOS: 12 days
ENGAGE
El número oficial de muertos: 191

Educate (technical)

EDUCATE (PS)

Learning From Defects
Check-list at insertion Daily-goals
IMPLEMENTATION

Protocolo
Manual de aplicación
Checklist inserción
Daily goals Inventario +registro
Safety clima Equipo líder
Aprender de errores
Problemas de seguridad
Definiciones Protocolo inserción
Resumen evidencia
Manual web
Manual Instrumentos
MEDIDAS DE PREVENCIÓN BRC: EVIDENCIA 1A
Bacteriemia zero
1. Higiene de manos adecuada
2. Desinfección de la piel con clorhexidina
3. Máximas barreras de precaución
5. Retirada de CVC no necesarios
4. Preferencia de localización subclavia
6. Mantenimiento higiénico del catéter
MEDIDAS DE PREVENCIÓN BRC: EVIDENCIA 1A
1. Higiene de manos adecuada
2. Desinfección de la piel con clorhexidina
3. Máximas barreras de precaución
5. Retirada de CVC no necesarios
4. Preferencia de localización subclavia
6. Mantenimiento higiénico del catéter
Bacteriemia zero
MEDIDAS DE PREVENCIÓN BRC: EVIDENCIA 1A
1. Higiene de manos adecuada
2. Desinfección de la piel con clorhexidina
3. Máximas barreras de precaución
5. Retirada de CVC no necesarios
4. Preferencia de localización subclavia
6. Mantenimiento higiénico del catéter
Bacteriemia zero
Programa de Seguridad Integral Programa de Seguridad Integral
(PSI)(PSI)
1Evaluación
de cultura
de seguridad
5Aprender
de los
errores
2Formación
en
seguridad
33Identificación
de fallos
4Alianza
con la
Dirección
0
Formación
equipo
seguridad
Bacteriemia zero
BacteriemiaBacteriemia zero
1. Higiene adecuada de manos
2. Desinfección de la piel con clorhexidina
3. Medidas de barrera total durante la inserción
4. Preferencia de localización subclavia
5. Retirada de CVC innecesarios
6. Manejo higiénico de los catéteres
1. Evaluar la cultura de seguridad
2. Formación en seguridad del paciente
3. Identificar errores en la práctica habitual
4. Establecer alianzas con la dirección
5. Aprender de los errores
STOPSTOP--BRCBRC
Equipo Equipo
seguridad seguridad
UCIUCIPlan de seguridad integralPlan de seguridad integral
Resumen STOP-BRC PSI
Curso STOP-BRC
Traducción
PSI In
str
um
en
tos
Mate
rial
form
ació
n
Pó
ste
rs
Do
cu
men
tos
ap
oyo
Test STOP-BRC
Curso PSI
Bacteriemia
zero
+
Guía
de navegación
web web web
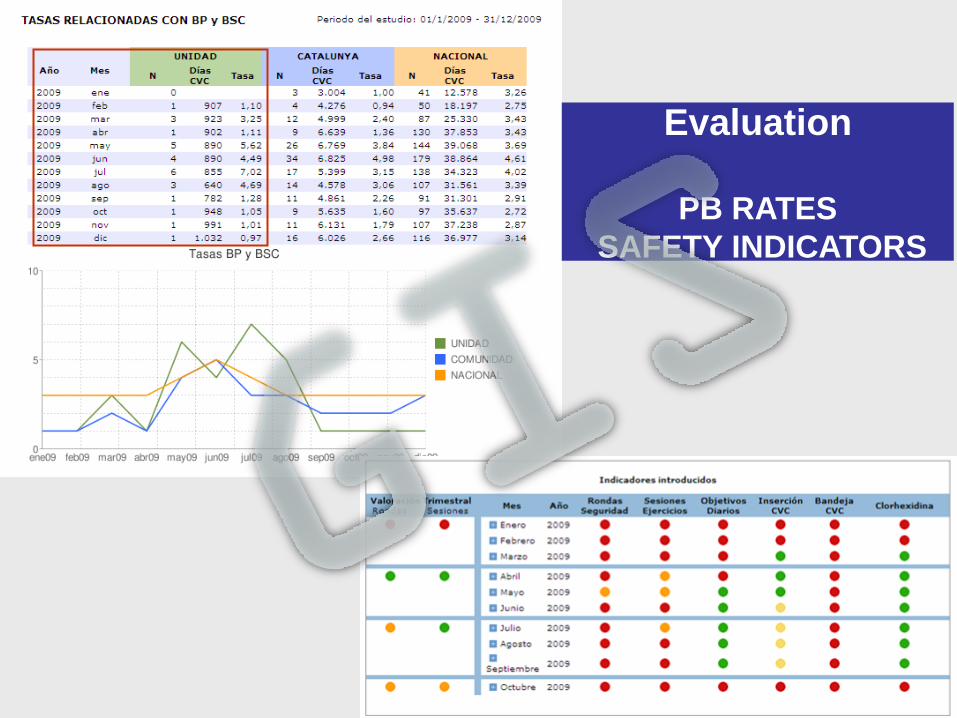
Evaluation
PB RATES
SAFETY INDICATORS

EZCOLLAB
This community based service allows you to exchange
resources, research papers, guidelines and other publications, to
share your own knowledge, experiences, and lessons learned.
Participate in online communities and discuss technical and
programmatic issues related to your work


Patients with BSI and CRBSI (%)
2,76
2,12
2,552,28
2,41
1,852,051,95
1,321,59
1,3 1,3
0,93 0,97
0
1
2
3
4
Basel
ine
Imple
m 0
-3m
4-6
m7-
9m
10-1
2m
13-1
5m
16-1
8m
%
BSI CRBSI

12,3
8,417,93
6,397,42
3,283,77
0
2
4
6
8
10
12
14
16
%
Bas
elin
e
Imple
m 0
-3m
4-6
m7-
9m
10-1
2m
13-1
5m
16-1
8m
Patients with >1 CRBSI

CRBSI: Incidence rate (Median)
3,07
2,08
2,5
2,06 2,1
0,861,12
0
1
2
3
4
5
Bas
elin
e
Imple
m 0
-3m
4-6
m7-
9m
10-1
2m
13-1
5m
16-1
8m
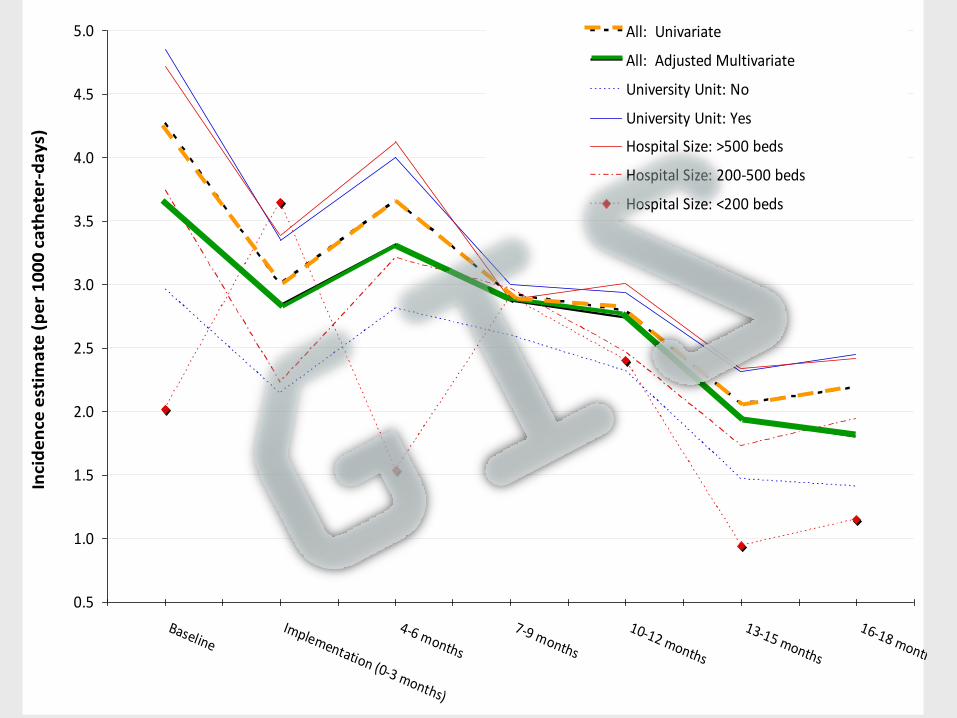
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
BaselineImplementation (0-3 months)
4-6 months
7-9 months
10-12 months
13-15 months
16-18 months
Inci
de
nce
est
ima
te (
pe
r 1
00
0 c
ath
ete
r-d
ays
)
All: Univariate
All: Adjusted Multivariate
University Unit: No
University Unit: Yes
Hospital Size: >500 beds
Hospital Size: 200-500 beds
Hospital Size: <200 beds

Incidence-rate ratio estimated
1
1,231,18
1,36
1,16
1,47
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
Imp
l(0-
3m)
4-6m
7-9m
10-1
2m
13-1
5m
16-1
8m
n/1
000
d s
tay
P = 0.013
P=0,022
NS NS NS
BSI-Secondary to other Infection Sites

CHARACTERISTICS OF PATIENTS WITH PB
BPSC (1.594 patients) ENVIN 2009 (14.984 patients)
• APACHE II 19,7 14, 3
• Age (years) 60,9 62,2
• Males (%) 68,7 64,4
• UD (%)
-Coronary 6,1 22,1
-Médical 55,8 42,7 - -Sched. surg 26,2 28,1
-Trauma 11,9 6,9
• Emerg surgery(%) 31,6 15,1
• ERD (%) 20,7 5,1
• TPN (%) 45,0 12,2
• ICU LOS (days) 33,9 7,7
• Mortality (%) 32,0 11,1

BZ BARRIERS
Barriers to use Chlorhexidine :
-Not believe in its effectiveness
-Difficulties to get it.
-Dislike colorless
-Do not know the standard
Daily goals
-Difficulties to find the usefull model (Type of ICU)
-Not believe in its effectiveness
-No time to meet nurses/physicians
Safety rounds :
-Difficulties to find the useful model
-Not executive's collaboration
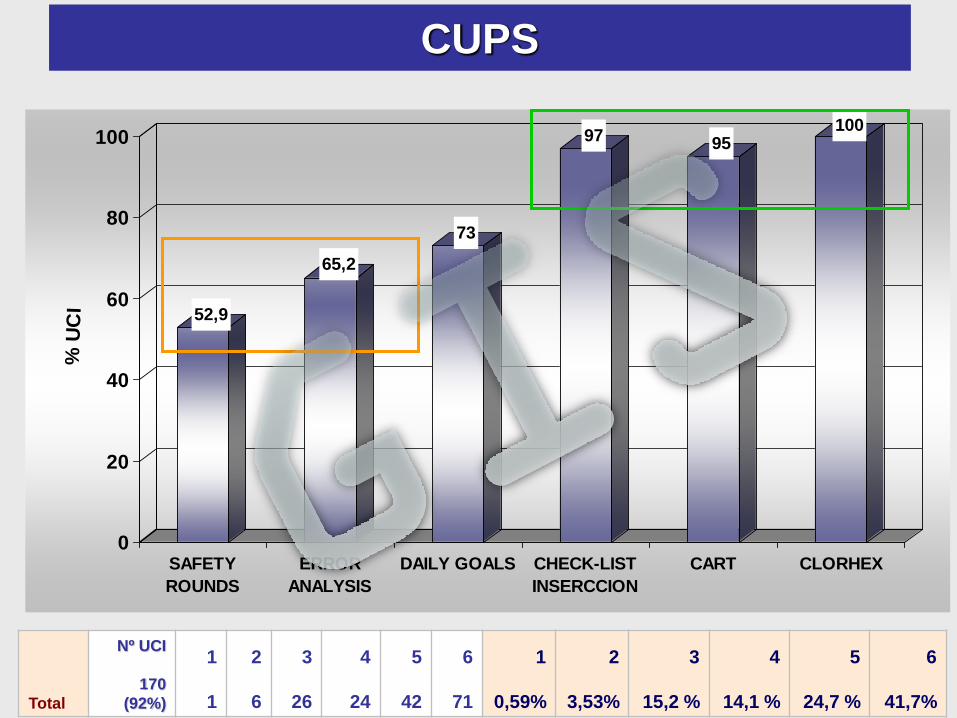
52,9
65,2
73
97 95100
0
20
40
60
80
100
% U
CI
SAFETY
ROUNDS
ERROR
ANALYSIS
DAILY GOALS CHECK-LIST
INSERCCION
CART CLORHEX
CUPS
Total
Nº UCI
170
(92%)
1
1
2
6
3
26
4
24
5
42
6
71
1
0,59%
2
3,53%
3
15,2 %
4
14,1 %
5
24,7 %
6
41,7%

CHANGES IN THE MANAGMENT
OF CRITICALLY ILL PATIENT
LERN FROM
ERRORS
IMPROVEMENT
GOALS
COMUNICATION
IMPROVEMENT
FROM SURVEILLANCE TO PREVENTION

LESSONS FROM BZ
BUNDLE
SAFETY PROGRAM
ICU LEADERS
INSTITUTIONAL
COMINMENT

“NZ RZ” PROJECTS
“BZ” PROJECT
STRUCTURE PARTNERS NZ
SPECIFIC BUNDLE
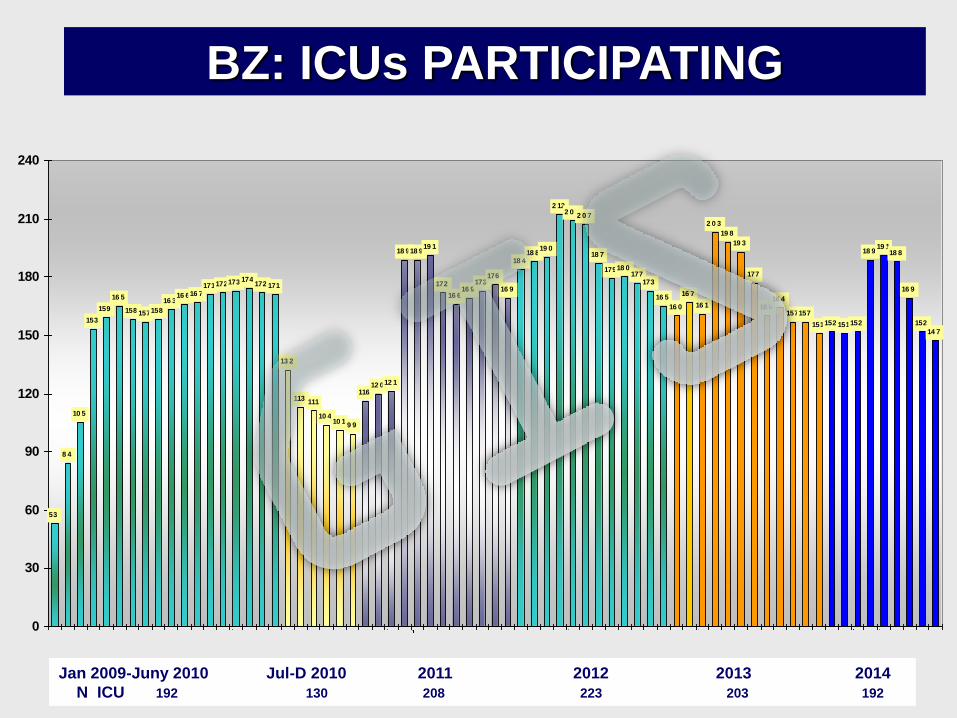
BZ: ICUs PARTICIPATING
53
8 4
10 5
153
159
16 5
158 157158
16 316 616 7
171172173 174172 171
13 2
113111
10 410 1
9 9
11612 012 1
18 918 919 1
172
16 616 9
173176
16 9
18 418 8
19 0
2 122 0 9
2 0 7
18 7
17918 0177
173
16 5
16 0
16 7
16 1
2 0 3
19 8
19 3
177
16 016 4
157157
151152 151152
18 919 1
18 8
16 9
152
14 7
0
30
60
90
120
150
180
210
240
Jan 2009-Juny 2010 Jul-D 2010 2011 2012 2013 2014
N ICU 192 130 208 223 203 192

192
130
208
223
203192
0
50
100
150
200
250
n
2009-2010 Jl-D 2010 2011 2012 2013 2014
BZ NZ RZ
BZ: ICUs PARTICIPATING

HEALTH REGIONS PB RATES 2012- 2013
2,72
2,37
2,78
2,26
1,9
1,42
2,05
1,55
1,87
1,47
2,45
2,4
3,96
3,59
1,87
1,56
3,33
2,61
2,36
2,27
2,34
1,28
1,79
2,66
1,53
3,16
2,36
1,56
5,95
3
2,67
1,8
0 1 2 3 4 5 6
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
2013
2012
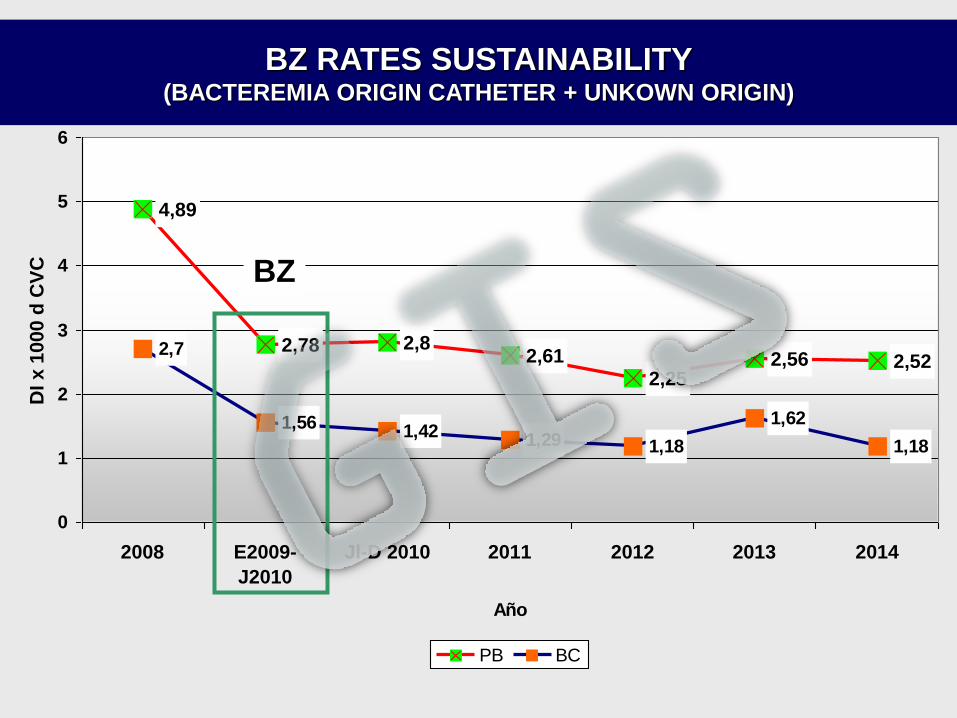
4,89
2,78 2,82,61
2,252,56 2,52
2,7
1,561,42
1,29 1,18
1,62
1,18
0
1
2
3
4
5
6
2008 E2009-
J2010
Jl-D 2010 2011 2012 2013 2014
Año
DI x 1
000 d
CV
C
PB BC
BZ
BZ RATES SUSTAINABILITY (BACTEREMIA ORIGIN CATHETER + UNKOWN ORIGIN)

HOSPITAL SIZE AND PB RATES
3,053,092,98
2,57
2,782,81
2,42,35
2,01
1,781,9
2,14
2,78
2,51
1,541,62
1,511,61
0
1
2
3
4
DI n
º B
RC
x 1
00
0 d
CV
C
>500 beds 201-500 <200 beds
BZ Jl-D 2010 2011 2012 2013 2014

1,5
1,7 1,64
1,461,33
1,24
0
0,5
1
1,5
2
2,5
2008 BZ 2011 2012 2013 2014
BZ: 1330 BSOF , 784.580 days of stay
2011: 863 BSOF, 527.414 days of stay
2012: 825 BSOF, 620.413 days of stay
2013: 789 BSOF, 541.943 days of stay
2014: 651 BSOF, 524.455 days of stay
BSI-Secondary to other Infection Sites

0
10
20
30
40
50
Subc Fem Yug Basil Axilar Otr
2009 2010 2011 2012 2013 2014

EPINE

ESTUDIO EPINE PREVALENCIA DE INFECCIÓN EN PACIENTES CRÍTICOS
37,2
26,8
30,7
24,05
32,9
25,3
28,7
22,41
0
5
10
15
20
25
30
35
40
%
2008 2009 2010 2011
Infect
Pts

EPINE STUDY
BACTERIEMIA PREVALENCE IN ICU
0,25
0,2 0,19 0,18
0
0,2
0,4
%
2008 2009 2010 2011



Time from ICU admission to onset of bloodstream infection
by country/network, 2008-2012 (n=26 815 BSI episodes)



Consider HCAI as an avoidable error,
is the first step to eradicate.
Surveillance is needed to quantify the
HCAI as to monitor the prevention
interventions.
BZ and NZ have promoted a culture of
safety, including training, teamwork
and implementation of guidelines and
bundles, which has helped to reduce
the risk.
Education, analysis and
dissemination of conclusions and
agreements, require technical and
financial resources


![Biomarkers for diagnosing serious bacterial infections in older ......bacteraemia in older adults [+ve LR range 1.50 to 2.60]. A CRP≥50mg/L only raises the probability of bacteraemia](https://img.pdfslide.net/doc/110x75/60b29041652da54ccf7015a6/biomarkers-for-diagnosing-serious-bacterial-infections-in-older-bacteraemia.jpg)


























