Embed Size (px)
Citation preview
Vol. 43. No. 1INFECTION AND IMMUNITY, Jan. 1984, p. 6-100019-9567/84/010006-05$02.00/0Copyright © 1984, American Society for Microbiology
Bacterial Translocation from the Gastrointestinal Tracts of RatsReceiving Thermal Injury
KAZUYOSHI MAEJIMA,'t EDWIN A. DEITCH,' AND RODNEY D. BERG2*Departments of Microbiology and Immunology.2 and Sitrger , 1 Loutisiana State Universitv Medical Center, Shreveport,
Loutisiana 71130
Received 1 August 1983/Accepted 29 September 1983
Rats receiving nonlethal thermal burns over 20 or 40% of their total body surface area were tested atvarious intervals for the translocation of indigenous bacteria from their gastroititestinal tracts to theirmesenteric lymph nodes, peritoneal cavities, and bloodstreams. No indigenous bacteria were cultured fromthese organs of control rats or from rats receiving 20% burns. However, 44%Y of the rats receiving 40% burnsexhibited viable Escherichia coli, Proteus mirabilis, Staphylococcus sp. and Clostridium sp. in theirmesenteric lymph nodes 2 days after thermal injury. Bacterial translocation after burn stress also was testedin antibiotic-decontaminated rats monoassociated with E. coli. E. (oli attained population levels in theseanimals of 108 to 109 per g of cecum. E. (coli translocated to 100% of the mesenteric lymph nodes of both thecontrol and 40% burned rats. However, E. c oli translocated at a greater incidence to the spleens, livers, andperitoneal cavities of the burned rats compared with translocation to these organs in control rats. Thenumbers of E. coli translocating to the mesenteric lymph nodes, spleens, and livers also were greater in the40% burned rats than in control rats. By 14 days after thermal injury, the rats were able to clear E. coli fromtheir spleens and livers, and the infection remained localized in the mesenteric lymph nodes. These resultssupport the concept that the indigenous gastrointestinal flora or exogenous organisms colonizing thegastrointestinal tract are potential sources of septicemia after thermal injury.
Bacterial infection is a frequent and serious problem inpatients who survive the shock phase of thermal injury (17).The unique tendency for burn patients to develop repeatedepisodes of bacteremia is related to a combination of the lossof the skin barrier to bacteria (17) and to an acquiredimpairment of the immune defense system (13, 14). Infec-tions in burn patients generally have been considered to arisefrom exogenous organisms colonizing the burn wound (17).Consequently, therapy of burn patients has emphasized theadoption of strict infection control policies to reduce contactwith exogenous organisms and the use of topical antimicro-bial agents to reduce bacterial colonization of the wound site(17). Very little attention has been directed to the indigenousmicroflora in the gastrointestinal (GI) tract of the burnpatient as a source of bacteremia. Burn stress may allowcertain indigenous bacteria to pass from the GI tract to otherorgans and spread to the bloodstream to cause severeinfection.The passage of viable indigenous bacteria from the GI
tract through the intact epithelial mucosa to the mesentericlymph nodes (MLN) and other organs has been termedbacterial translocation (10, 16, 26). Indigenous bacteria arenot present in the MLN, spleens, livers, or kidneys ofhealthy, specific pathogen-free mice (10). These bacteriaeither do not pass through the GI mucosa, are killed intransit, or are killed in reticuloendothelial organs such as theMLN. Indigenous bacteria translocate from the GI tract,however, when there is overgrowth of certain bacteriapopulating the GI tract (7, 11) or when the host immunedefense mechanisms are compromised (9, 21, 22). For exam-ple, viable aerobic and anaerobic bacteria of the indigenousGI flora translocate to the MLN, spleens, livers, and kidneys
* Corresponding author.t Present address: Laboratory Animal Center. School of Medi-
cine, Keio University, Tokyo 160, Japan.
of athymic (nude) mice to a much greater degree than tothese organs of heterozygous (nu/+)mice (21). Immunosup-pressive agents such as prednisone, cyclophosphamide, 5-fluorouracil, methotrexate, or cytosine arabinoside injectedinto mice also promote the translocation of indigenousbacteria from the GI tract (9). Since thermal injury decreasesthe efficiency of specific and nonspecific defense mecha-nisms (1, 3, 5, 14), it seems likely that patients receivingburns are particularly at risk for infection by indigenousbacteria translocating from their own GI tracts. Further-more, bacteria translocating from the GI tract to the MLN ofburn patients would be more likely to survive and to spreadsystemically due to the immunosuppressed state of thesepatients.Although Howerton and Kolmer (19) demonstrated that
Pseudomonas aeruiginosa can translocate from the GI tractto the MLN of burned rats, it is not known whether thermalinjury will promote the translocation from the GI tract ofindigenous bacteria less virulent than nonindigenous P.aeruginosa. Consequently, we tested whether a nonlethalthermal injury would promote the translocation of indige-nous bacteria from the rat GI tract to the MLN, spleen, liver,or peritoneal cavity. Translocation of facultatively anaerobicand strictly anaerobic bacteria from the GI tract occurred inrats receiving 40% total body area burns. We also testedbacterial translocation from the GI tracts of rats that hadbeen antibiotic decontaminated and colonized with Esche-ric hia c oli before receiving the 40% burns. E. (oli translocat-ed to a much greater extent to the MLN, spleens, livers, andperitoneal cavities of the rats receiving 40% burns than tothese organs of control rats.
MATERIALS AND METHODS
Rats. Specific pathogen free, female, Crl:CDH(SD)BRHoltzman rats (Charles River Breeding Laboratories, Inc.,
6
on May 9, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
INDIGENOUS BACTERIA 7
Wilmington, Mass.), weighing 180 to 210 g. were usedthroughout the experiments. The rats were fed Purina Labo-ratory Chow (Ralston Purina Co., Inc., St. Louis, Mo.) adlibitum. Bedding consisted of San-I-Cel laboratory animalbedding (Paxton Processing Co., Inc., Paxton, Ill.).
Antibiotic decontamination. Specific pathogen-free ratswere given 4 mg of streptomycin sulfate (Pfizer. Inc., NewYork, N.Y.) and 4 mg of bacitracin (The Upjohn Co.,Kalamazoo, Mich.) per ml of drinking water for 4 days aspreviously described (7). The antibiotic-decontaminated ratsthen were inoculated orally by feeding needles (Popper andSons, Inc., New Hyde Park, N.Y.) with 3 x 108 E. coli C25resistant to streptomycin (15. 23). The rats continued toreceive streptomycin and bacitracin in their drinking water.The rats received thermal burns 4 days after oral coloniza-
tion with E. coli C25. Control rats which were antibioticdecontaminated and subsequently colonized with E. coli didnot receive thermal injury. The rats were killed at varioustime intervals after receiving thermal injury, and the organswere cultured for viable E. co/i.Thermal injury. The procedures utilized to burn the rats
were adapted from those described by Walker et al. (25).Rats were anesthetized intraperitoneally with 25 mg ofpentobarbital sodium (Nembutal) per kg of body weight. Thehair was shaved from both the back and abdomen, and therat was placed in a plastic holder containing an opening toexpose the back (20% total body surface area) and anotheropening to expose the abdomen (20% total body surfacearea). The exposed back was immersed in boiling water(100°C) for 10 s. and the exposed abdomen was immersed for3 s. Rats with thermal injury to only the back received 20%total body surface area burns, and rats with thermal injury toboth the back and abdomen received 40% burns. Ratsreceiving 40% burns were injected intraperitoneally with 10ml of sterile normal saline to prevent shock.
Translocation of E. coli C25. Rats were decontaminatedwith streptomycin and bacitracin and subsequently colo-nized with E. coli C25. These rats then received 20 or 40%total body area thermal burns. Burned and control rats atvarious intervals after thermal injury were anesthetized withchloroform (Aldrich Chemical Co., Milwaukee. Wis.), andblood was obtained by heart puncture. The blood wastransferred into 5 ml of brain heart infusion (Difco Labora-tories, Detroit, Mich.) and incubated for 48 h at 37°C. Anincision was then made with sterile instruments through theskin and peritoneum of the abdomen. The exposed viscerawere swabbed with sterile, cotton-tipped applicator stickswhich were cultured in tryptic soy broth (Difco) to detectany bacterial contamination. The caudal and cranial MLN.spleen, and liver were removed, and each was placed in
grinding tubes (Tri-R Instruments. Rockville Centre. N.Y.)containing sterile tryptic soy broth. The ceca were placed in
grinding tubes containing phosphate-buffered saline (pH7.3). The organs were weighed and then homogenized withTeflon grinders (Tri-R Instruments). Portions (0.2 ml) of theMLN. spleen. and liver were cultured on Tergitol-7 agar(Difco) containing 1 mg of streptomycin sulfate per ml. Theplates were incubated for 24 h at 370C. The cecal homoge-nates were diluted serially in phosphate-buffered saline (pH7.3) and cultured on Tergitol-7 containing 1 mg of streptomy-cin sulfate per ml. The plates were incubated for 24 h at37°C. The cecal homogenate was diluted serially in phos-phate-buffered saline (pH 7.3) and cultured on Tergitol-7agar containing streptomycin sulfate. The numbers of viableE. coli C25 were determined per gram of organ or per wholeorgan.
Translocation of indigenous bacteria. Rats receiving 20 or40% burns were anesthetized with chloroform, and bloodwas obtained by heart puncture as described above. Thevarious organs were removed and placed in grinding tubescontaining prereduced, enriched tryptic soy broth with0.05% dithiothreitol (Sigma Chemical Co., St. Louis, Mo.) toreduce any oxygen contamination (6). The grinding tubeswere transferred into an anaerobic glove box (Coy Manufac-turing Co., Ann Arbor, Mich.) (2) maintained at less than 10parts of oxygen per 106 parts of an atmosphere consisting of5% carbon dioxide, 10% hydrogen. and 85% nitrogen. Theoxygen level inside the anaerobic glove box was monitoredwith a Trace Oxygen Analyzer (Lockwood and McLorie,Inc., Horsham, Pa.). The organs were homogenized insidethe glove box with Teflon grinders, and portions werecultured on prereduced, enriched tryptic soy agar (2) de-signed to support the growth of strictly anaerobic bacteria ofthe indigenous microflora. The enriched tryptic soy agarcontained 1 mg of polymyxin B (Pfizer) per ml to inhibit thegrowth of facultatively anaerobic bacteria such as E. (oli.The plates were incubated at 37°C for at least 4 days insidethe anaerobic glove box.
One-half of each organ homogenate was removed from theanaerobic glove box, and portions were plated on blood agar(Difco) and Tergitol-7 (Difco) to culture aerobic and faculta-tively anaerobic bacteria. These gram-negative enteric bac-teria were identified with the API 20E system (AnalytabProducts. Plainview. N.Y.). Obligately anaerobic bacteriawere identified by the procedures of Holdeman et al. (18).
RESULTSRats receiving thermal burns over 20 or 40% of their total
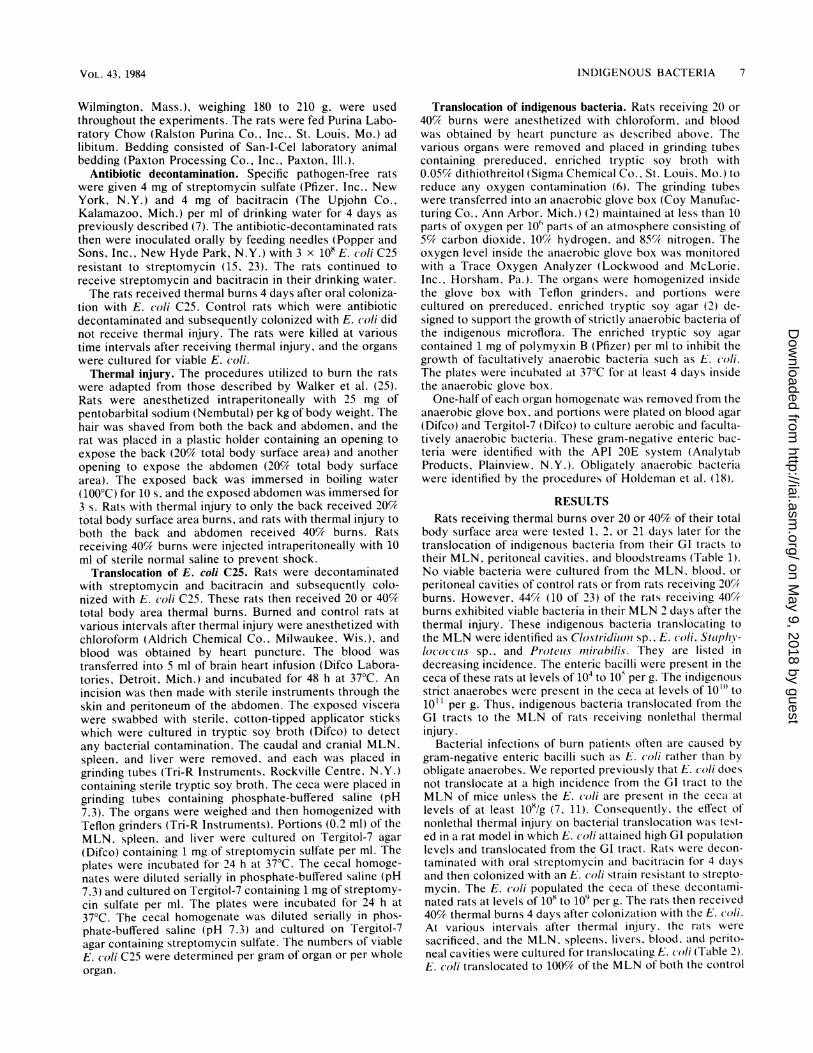
body surface area were tested 1, 2, or 21 days later for thetranslocation of indigenous bacteria from their GI tracts totheir MLN, peritoneal cavities, and bloodstreams (Table 1).No viable bacteria were cultured from the MLN. blood, or
peritoneal cavities of control rats or from rats receiving 20%burns. However, 44% (10 of 23) of the rats receiving 40%burns exhibited viable bacteria in their MLN 2 days after thethermal injury. These indigenous bacteria translocating tothe MLN were identified as Clostridiiuml sp., E. coli. Staphy-lococcus sp., and Pr-oteius miii-bili/s. They are listed in
decreasing incidence. The enteric bacilli were present in thececa of these rats at levels of 104 to 1W per g. The indigenousstrict anaerobes were present in the ceca at levels of 101" to101 l per g. Thus, indigenous bacteria translocated from theGI tracts to the MLN of rats receiving nonlethal thermalinjury.
Bacterial infections of burn patients often are caused bygram-negative enteric bacilli such as E. coli rather than byobligate anaerobes. We reported previously that E. coli doesnot translocate at a high incidence from the GI tract to theMLN of mice unless the E. coli are present in the ceca atlevels of at least 108/g (7, 11). Consequently. the effect ofnonlethal thermal injury on bacterial translocation was test-ed in a rat model in which E. coli attained high GI populationlevels and translocated from the G6 tract. Rats were decon-taminated with oral streptomycin and bacitracin for 4 daysand then colonized with an E. coli strain resistant to strepto-mycin. The E. coli populated the ceca of these decontami-nated rats at levels of 108 to 109 per g. The rats then received40% thermal burns 4 days after colonization with the E. coli.At variQus intervals after thermal injury. the rtats were
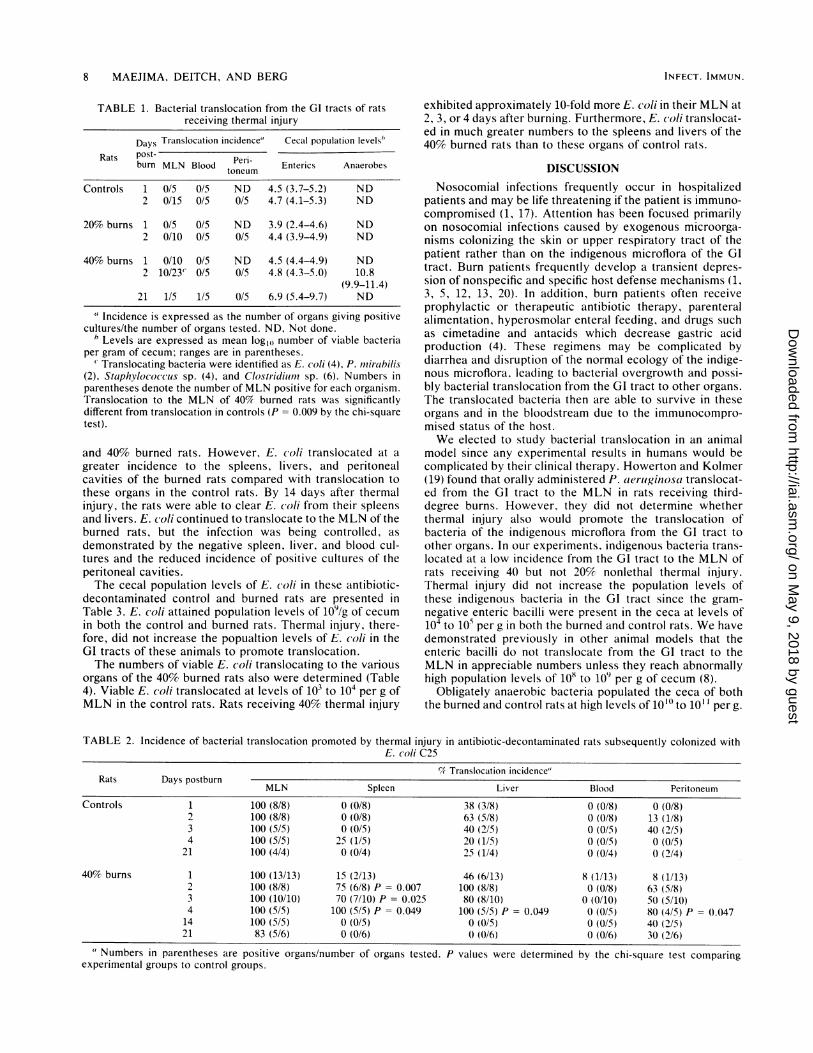
sacrificed, and the MLN, spleens. livers, blood, and perito-neal cavities were cultured for translocating E. coli (Table 2).E. (/li translocated to 100% of the MLN of both the control
VOL. 43, 1984
on May 9, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
8 MAEJIMA, DEITCH, AND BERG
TABLE 1. Bacterial translocation from the GI tracts of ratsreceiving thermal injury
Days Translocation incidence" Cecal population levels'
Rats post- Peri-burn MLN Blood Enterics Anaerobes
Controls 1 0/5 0/5 ND 4.5 (3.7-5.2) ND2 0/15 0/5 0/5 4.7 (4.1-5.3) ND
20% burns 1 0/5 0/5 ND 3.9 (2.4-4.6) ND2 0/10 0/5 0/5 4.4 (3.9-4.9) ND
40% burns 1 0/10 0/5 ND 4.5 (4.4-4.9) ND2 10/23C 0/5 0/5 4.8 (4.3-5.0) 10.8
(9.9-11.4)21 1/5 1/5 0/5 6.9 (5.4-9.7) ND
'Incidence is expressed as the number of organs giving positivecultures/the number of organs tested. ND, Not done.
6 Levels are expressed as mean log1, number of viable bacteriaper gram of cecum; ranges are in parentheses.
' Translocating bacteria were identified as E. coli (4), P. Inirabilis(2), Staphylococcuus sp. (4), and Clostriiduinl sp. (6). Numbers inparentheses denote the number of MLN positive for each organism.Translocation to the MLN of 40W burned rats was significantlydifferent from translocation in controls (P = 0.009 by the chi-squaretest).
and 40% burned rats. However, E. (oli translocated at agreater incidence to the spleens, livers, and peritonealcavities of the burned rats compared with translocation tothese organs in the control rats. By 14 days after thermalinjury, the rats were able to clear E. (oli from their spleensand livers. E. co/li continued to translocate to the MLN of theburned rats, but the infection was being controlled, asdemonstrated by the negative spleen, liver, and blood cul-tures and the reduced incidence of positive cultures of theperitoneal cavities.The cecal population levels of E. coli in these antibiotic-
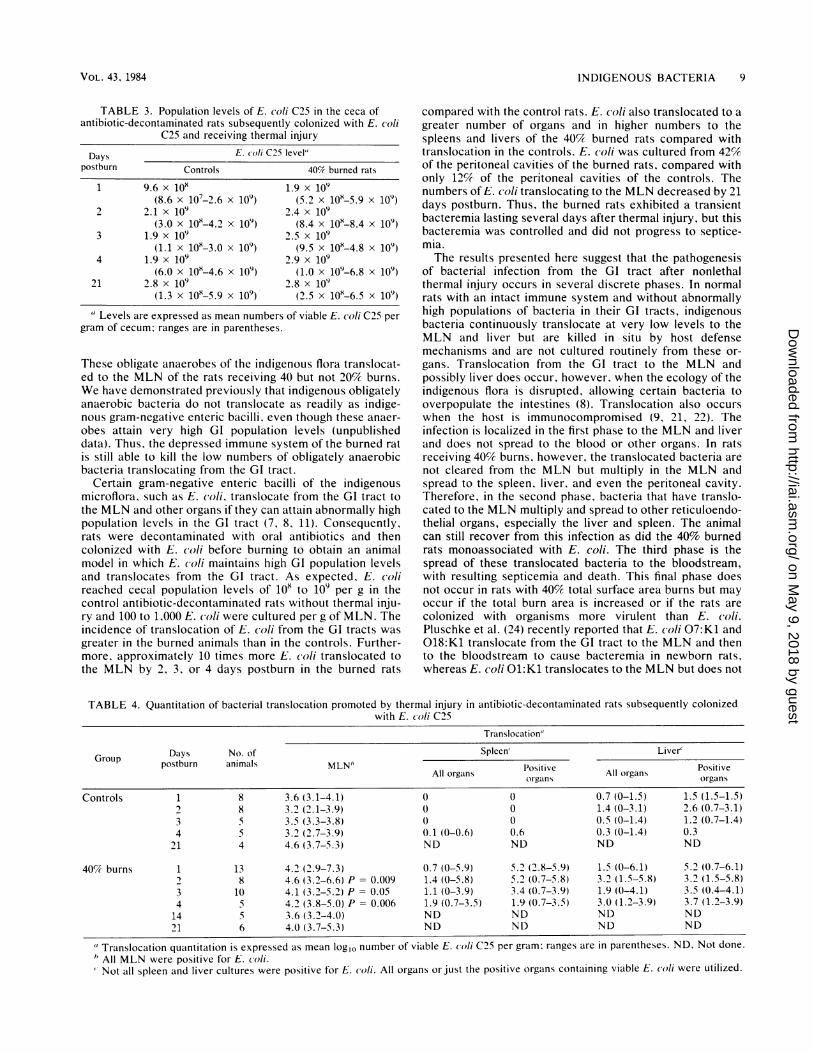
decontaminated control and burned rats are presented inTable 3. E. coli attained population levels of 109/g of cecumin both the control and burned rats. Thermal injury, there-fore, did not increase the popualtion levels of E. (oli in theGI tracts of these animals to promote translocation.The numbers of viable E. coli translocating to the various
organs of the 40% burned rats also were determined (Table4). Viable E. c oli translocated at levels of 103 to 104 per g ofMLN in the control rats. Rats receiving 40% thermal injury
exhibited approximately 10-fold more E. coli in their MLN at2, 3, or 4 days after burning. Furthermore, E. coli translocat-ed in much greater numbers to the spleens and livers of the40% burned rats than to these organs of control rats.
DISCUSSIONNosocomial infections frequently occur in hospitalized
patients and may be life threatening if the patient is immuno-compromised (1, 17). Attention has been focused primarilyon nosocomial infections caused by exogenous microorga-nisms colonizing the skin or upper respiratory tract of thepatient rather than on the indigenous microflora of the GItract. Burn patients frequently develop a transient depres-sion of nonspecific and specific host defense mechanisms (1,3, 5, 12, 13, 20). In addition, burn patients often receiveprophylactic or therapeutic antibiotic therapy, parenteralalimentation, hyperosmolar enteral feeding, and drugs suchas cimetadine and antacids which decrease gastric acidproduction (4). These regimens may be complicated bydiarrhea and disruption of the normal ecology of the indige-nous microflora, leading to bacterial overgrowth and possi-bly bacterial translocation from the GI tract to other organs.The translocated bacteria then are able to survive in theseorgans and in the bloodstream due to the immunocompro-mised status of the host.We elected to study bacterial translocation in an animal
model since any experimental results in humans would becomplicated by their clinical therapy. Howerton and Kolmer(19) found that orally administered P. aeruitginosa translocat-ed from the G6 tract to the MLN in rats receiving third-degree burns. However, they did not determine whetherthermal injury also would promote the translocation ofbacteria of the indigenous microflora from the GI tract toother organs. In our experiments, indigenous bacteria trans-located at a low incidence from the GI tract to the MLN ofrats receiving 40 but not 20% nonlethal thermal injury.Thermal injury did not increase the population levels ofthese indigenous bacteria in the GI tract since the gram-negative enteric bacilli were present in the ceca at levels ofi04 to i05 per g in both the burned and control rats. We havedemonstrated previously in other animal models that theenteric bacilli do not translocate from the GI tract to theMLN in appreciable numbers unless they reach abnormallyhigh population levels of 108 to 109 per g of cecum (8).
Obligately anaerobic bacteria populated the ceca of boththe burned and control rats at high levels of 10"' to 1011 per g.
TABLE 2. Incidence of bacterial translocation promoted by thermal injury in antibiotic-decontaminated rats subsequently colonized withE. coli C25
% Translocation incidence"Rats Days postburn MNSleRatsDayspostburn
MLN Spleen Liver Blood Peritoneum
Controls 1 100 (8/8) 0 (0/8) 38 (3/8) 0 (0/8) 0 (0/8)2 100 (8/8) 0 (0/8) 63 (5/8) 0 (0/8) 13 (1/8)3 100 (5/5) 0 (0/5) 40 (2/5) 0 (0/5) 40 (2/5)4 100 (5/5) 25 (1/5) 20 (1/5) 0 (0/5) 0 (0/5)
21 100 (4/4) 0 (0/4) 25 (1/4) 0 (0/4) 0 (2/4)
40% burns 1 100 (13/13) 15 (2/13) 46 (6/13) 8 (1/13) 8 (1/13)2 100 (8/8) 75 (6/8) P = 0.007 100 (8/8) 0 (0/8) 63 (5/8)3 100 (10/10) 70 (7/10) P = 0.025 80 (8/10) 0 (0/10) 50 (5/10)4 100 (5/5) 100 (5/5) P = 0.049 100 (5/5) P = 0.049 0 (0/5) 80 (4/5) P = 0.04714 100 (5/5) 0 (0/5) 0 (0/5) 0 (0/5) 40 (2/5)21 83 (5/6) 0 (0/6) 0 (0/6) 0 (0/6) 30 (2/6)
Numbers in parentheses are positive organs/number of organs tested. P values were determined by the chi-square test comparingexperimental groups to control groups.
INFECT. IMMUN.
on May 9, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
INDIGENOUS BACTERIA 9
TABLE 3. Population levels of E. coli C25 in the ceca ofantibiotic-decontaminated rats subsequently colonized with E. coli
C25 and receiving thermal injury
Days E. coli C25 level"postburn Controls 40% burned rats
1 9.6 x 10 .9 x O(8.6 x 107-2.6 x 109) (5.2 x 10"-5.9 x 109)
2 2.1 x 109 2.4x 109(3.0 x 10-4.2 x 109) (8.4 x 10"-8.4 x 109)
3 1.9 x 109 2.5 x 109(1.1 x 10-3.0 x 109) (9.5 x 108-4.8 x 109)
4 1.9 x 109 2.9 x 109(6.0 x 10"-4.6 x 109) (1.0 x 109-6.8 x 109)
21 2.8 x 109 2.8 x 109(1.3 x 10"-5.9 x 109) (2.5 x 10"-6.5 x 109)
Levels are expressed as mean numbers of viable E. coli C25 pergram of cecum; ranges are in parentheses.
These obligate anaerobes of the indigenous flora translocat-ed to the MLN of the rats receiving 40 but not 20% burns.We have demonstrated previously that indigenous obligatelyanaerobic bacteria do not translocate as readily as indige-nous gram-negative enteric bacilli, even though these anaer-obes attain very high GI population levels (unpublisheddata). Thus, the depressed immune system of the burned ratis still able to kill the low numbers of obligately anaerobicbacteria translocating from the GI tract.
Certain gram-negative enteric bacilli of the indigenousmicroflora, such as E. (/li, translocate from the GI tract tothe MLN and other organs if they can attain abnormally highpopulation levels in the GI tract (7, 8, 11). Consequently,rats were decontaminated with oral antibiotics and thencolonized with E. coli before burning to obtain an animalmodel in which E. coli maintains high GI population levelsand translocates from the GI tract. As expected, E. (olireached cecal population levels of 108 to 109 per g in thecontrol antibiotic-decontaminated rats without thermal inju-ry and 100 to 1,000 E. oli were cultured per g of MLN. Theincidence of translocation of E. (oli from the GI tracts wasgreater in the burned animals than in the controls. Further-more, approximately 10 times more E. (coli translocated tothe MLN by 2, 3, or 4 days postburn in the burned rats
compared with the control rats. E. coli also translocated to a
greater number of organs and in higher numbers to thespleens and livers of the 40% burned rats compared withtranslocation in the controls. E. coli was cultured from 42%of the peritoneal cavities of the burned rats, compared withonly 12%. of the peritoneal cavities of the controls. Thenumbers of E. c(li translocating to the MLN decreased by 21days postburn. Thus, the burned rats exhibited a transientbacteremia lasting several days after thermal injury, but thisbacteremia was controlled and did not progress to septice-mia.The results presented here suggest that the pathogenesis
of bacterial infection from the GI tract after nonlethalthermal injury occurs in several discrete phases. In normalrats with an intact immune system and without abnormallyhigh populations of bacteria in their GI tracts, indigenousbacteria continuously translocate at very low levels to theMLN and liver but are killed in situ by host defensemechanisms and are not cultured routinely from these or-
gans. Translocation from the GI tract to the MLN andpossibly liver does occur, however, when the ecology of theindigenous flora is disrupted, allowing certain bacteria tooverpopulate the intestines (8). Translocation also occurswhen the host is immunocompromised (9, 21, 22). Theinfection is localized in the first phase to the MLN and liverand does not spread to the blood or other organs. In ratsreceiving 40% burns, however, the translocated bacteria are
not cleared from the MLN but multiply in the MLN andspread to the spleen, liver, and even the peritoneal cavity.Therefore, in the second phase, bacteria that have translo-cated to the MLN multiply and spread to other reticuloendo-thelial organs, especially the liver and spleen. The animalcan still recover from this infection as did the 40% burnedrats monoassociated with E. coli. The third phase is thespread of these translocated bacteria to the bloodstream,with resulting septicemia and death. This final phase doesnot occur in rats with 40%5 total surface area burns but mayoccur if the total burn area is increased or if the rats arecolonized with organisms more virulent than E. coli.Pluschke et al. (24) recently reported that E. coli 07:K1 and018:K1 translocate from the GI tract to the MLN and thento the bloodstream to cause bacteremia in newborn rats,whereas E. coli 01:K1 translocates to the MLN but does not
TABLE 4. Quantitation of bacterial translocation promoted by thermal injury in antibiotic-decontaminated rats subsequently colonizedwith E. coli C25
Translocation"
Group Days No. of Spleen' Liver'postburn animals MLN" Positive Positive
All organs organsanorgans organs
Controls 1 8 3.6 (3.1-4.1) 0 0 0.7 (0-1.5) 1.5 (1.5-1.5)2 8 3.2 (2.1-3.9) 0 0 1.4 (0-3.1) 2.6 (0.7-3.1)3 5 3.5 (3.3-3.8) 0 0 0.5 (0-1.4) 1.2 (0.7-1.4)4 5 3.2 (2.7-3.9) 0.1 (0-0.6) 0.6 0.3 (0-1.4) 0.3
21 4 4.6 (3.7-5.3) ND ND ND ND
40% burns 1 13 4.2 (2.9-7.3) 0.7 (0-5.9) 5.2 (2.8-5.9) 1.5 (0-6.1) 5.2 (0.7-6.1)2 8 4.6 (3.2-6.6) P = 0.009 1.4 (0-5.8) 5.2 (0.7-5.8) 3.2 (1.5-5.8) 3.2 (1.5-5.8)3 10 4.1 (3.2-5.2) P = 0.05 1.1 (0-3.9) 3.4 (0).7-3.9) 1.9 (0-4.1) 3.5 (0.4-4.1)4 5 4.2 (3.8-5.0) P = 0.006 1.9 (0.7-3.5) 1.9 (0.7-3.5) 3.0 (1.2-3.9) 3.7 (1.2-3.9)14 5 3.6 (3.2-4.0) ND ND ND ND21 6 4.0 (3.7-5.3) ND ND ND ND
"Translocation quantitation is expressed as mean log,0 number of viable E. coli C25 per gram; ranges are in parentheses. ND, Not done.h All MLN were positive for E. coli.Not all spleen and liver cultures were positive for E. coli. All organs or just the positive organs containing viable E. coli were utilized.
VOL. 43, 1984
on May 9, 2018 by guest
http://iai.asm.org/
Dow
nloaded from

10 MAEJIMA, DEITCH, AND BERG
cause bacteremia. Thus, virulence properties of the translo-cating bacteria are important in the pathogenesis of bacte-remia.The animal model used in our study differs in several
respects from previous models employed to relate burnstress to susceptibility to infectious disease. The oral routeof bacterial infection in our model is natural, as comparedwith an artificial intravenous or intraperitoneal route. Impor-tantly, the thermal injury is nonlethal and highly reproduc-ible. Finally, the bacteria translocating from the GI tract tocause infection are indigenous to these animals and are notvirulent exogenous organisms.Our results support the concept that the indigenous GI
flora is an important source of potential septicemia in burnpatients. These patients are at even greater risk of septice-mia if the ecology of the indigenous bacterial flora has beendisrupted by oral antibiotic treatment allowing (i) intestinalovergrowth by certain indigenous bacteria or (ii) the coloni-zation of the intestines by exogenous pathogens, such asCandida sp., P. aeruiginosa, or Staphy/o(o((is sp. Furtherstudies with this burn model should provide information asto the specific immunodeficiencies occurring during burnstress that allow indigenous bacteria to translocate from theGI tract and cause life-threatening infections.
LITERATURE CITED
1. Alexander, J. W., C. K. Ogle, J. D. Stinnett, and B. G. Macmil-lian. 1978. A sequential, prospective analysis of immunologicabnormalities and infection following severe thermal injury.Ann. Surg. 181:809-816.
2. Aranki, A., and R. Freter. 1972. Use of anaerobic glove boxesfor the cultivation of strictly anaerobic bacteria. Am. J. Clin.Nutr. 25:1329-1334.
3. Arturson, G., C. F. Hogman, G. 0. Johansson, and J. Killander.1969. Changes in immunoglobulin levels in severely burnedpatients. Lancet i:546-548.
4. Artz, C. P., J. A. Moncrief, and B. A. Pruitt. 1979. Burns. Ateam approach. The W. B. Saunders Co., Philadelphia.
5. Baker, C. C., C. L. Miller, and D. D. Trunkey. 1979. Predictingfatal sepsis in burn patients. J. Trauma 19:641-648.
6. Berg, R. D. 1978. Antagonism among the normal anaerobicbacteria of the mouse gastrointestinal tract determined byimmunofluorescence. Appl. Environ. Microbiol. 35:1066-1073.
7. Berg, R. D. 1980. Inhibition of Escherichia coli translocationfrom the gastrointestinal tract by normal cecal flora in gnotobi-otic or antibiotic-decontaminated mice. Infect. Immun.29:1073-1081.
8. Berg, R. D. 1981. Promotion of the translocation of entericbacteria from the gastrointestinal tracts of mice by oral treat-ment with penicillin. clindamycin, or metronidazole. Infect.Immun. 33:854-861.
9. Berg, R. D. 1983. Bacterial translocation from the gastrointesti-
nal tracts of mice receiving immunosuppressive chemothera-peutic agents. Curr. Microbiol. 8:285-292.
10. Berg, R. D., and A. W. Garlington. 1979. Translocation ofcertain indigenous bacteria from the gastrointestinal tract to themesenteric lymph nodes and other organs in a gnotobioticmouse model. Infect. Immun. 23:403-411.
11. Berg, R. D., and W. E. Owens. 1979. Inhibition of translocationof viable Escheric/ia c o/i from the gastrointestinal tract of miceby bacterial antagonism. Infect. Immun. 25:820-827.
12. Bjornson, A. B., W. H. Altemeier, and H. S. Bjornson. 1977.Changes in humoral components of host defense following burntrauma. Ann. Surg. 186:88-96.
13. Deitch, E. A., F. Gelder, and J. C. McDonald. 1982. The rela-tionship between CIG depletion and peripheral neutrophil func-tion in rabbits and man. J. Trauma 22:469-475.
14. Deitch, E. A., F. Gelder, and J. C. McDonald. 1982. Prognosticsignificance of abnormal neutrophil chemotaxis after thermalinjury. J. Trauma 22:199-204.
15. Freter, R. 1962. In vivo and in vitro antagonism of intestinalbacteria against S/hige//aflcexneri. J. Infect. Dis. 110:38-46.
16. Fuller, R., and D. J. Jayne-Williams. 1970. Resistance of thefowl (Gallits domnesticis) to invasion by its intestinal flora. II.Clearance of translocated intestinal bacteria. Res. Vet. Sci.11:368-374.
17. Hartford, C. E. 1981. The bequests of Moncrief and Moyer: anappraisal of topical therapy of burns-1981 American BurnAssociation presidental address. J. Trauma 21:827-834.
18. Holdeman, L. V., E. Cato, and W. E. C. Moore (ed.). 1977.Anaerobe laboratory manual. 4th ed. Virginia Polytechnic Insti-tute and State University. Blacksburg.
19. Howerton, E. E., and S. N. Kolmer. 1972. The intestinal tract asa portal of entry of Pseudomionas in burned rats. J. Trauma12:335-350.
2t). Munster, A. M., R. A. Winchurch, W. I. Birmingham, and P.Keeling. 1980. Longitudinal assay of lymphocyte responsive-ness in patients with major burns. Ann. Surg. 192:772-775.
21. Ownens, W. E., and R. D. Berg. 1980. Bacterial translocationfrom the gastrointestinal tract of athymic (nu/nu) mice. Infect.Immun. 27:461-467.
22. Owens, W. E., and R. D. Berg. 1982. Bacterial translocationfrom the gastrointestinal tracts of thymectomized mice. Curr.Microbiol. 7:169-174.
23. Ozawa, A., and R. Freter. 1964. Ecological mechanism control-ling growth of Esc/eric/ia coli in continuous flow cultures andin the mouse intestine. J. Infect. Dis. 114:235-242.
24. Pluschke, G., A. Mercer, B. Kusecek, A. Pohl, and M. Achtman.1983. Induction of bacteremia in newborn rats by Eshe/ichia(o/i Kl is correlated with only certain 0 (lipopolysaccharide)antigen types. Infect. Immun. 39:599-608.
25. Walker, H. L., A. D. Mason, Jr., and G. L. Raluston. 1964.Surface infections with Pseuidomonoas aeruginosa. Ann. Surg.160:297-305.
26. Wolochow, H., G. J. Hildebrand, and C. Lamanna. 1966. Trans-location of microorganisms across the intestinal wall of the rat:effect of microbiail size and concentration. J. Infect. Dis.116:523-528.
INFECT. IMMUN.
on May 9, 2018 by guest
http://iai.asm.org/
Dow
nloaded from





























