Embed Size (px)
Citation preview
BARIATRIC SURGERY
EMILY SCHWICHTENBERG
CONCORDIA COLLEGEMOORHEAD, MINNESOTA
Objectives
To explain different bariatric procedures Discuss requirements for surgery Explain post-op medical nutrition
therapy Discuss proper and important lifestyle
changes Discuss ethical issues
Obesity
as an Epidemic
Schernthaner, G., & Morton J.M. (2008). Bariatric surgery in patients with morbid obesity and type 2 diabetes. Diabetes Journal, 31, 297-302.
66.3% of United States adults are overweight
32.2% are obese with a BMI >30 kg/m²
4.8% are morbidly obese with a BMI >40 kg/m²
From 1986-2000 BMI >30 kg/m² doubled in the United States
BMI of >40 kg/m² quadrupled BMI of >50 kg/m² increased fivefold
Statistics
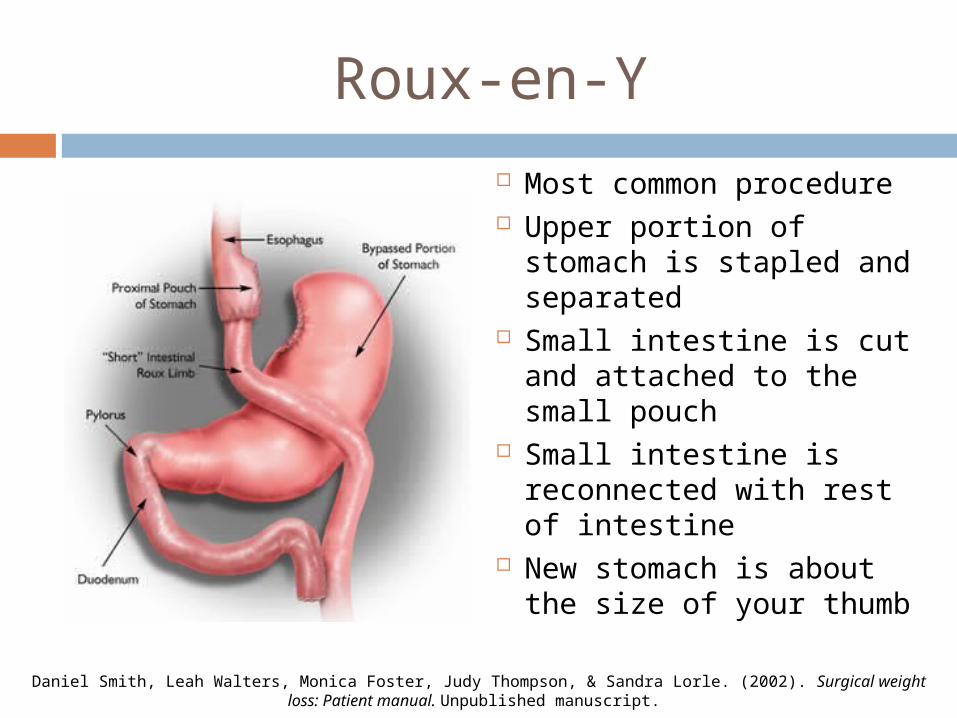
Roux-en-Y
Most common procedure Upper portion of stomach
is stapled and separated Small intestine is cut and
attached to the small pouch
Small intestine is reconnected with rest of intestine
New stomach is about the size of your thumb
Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
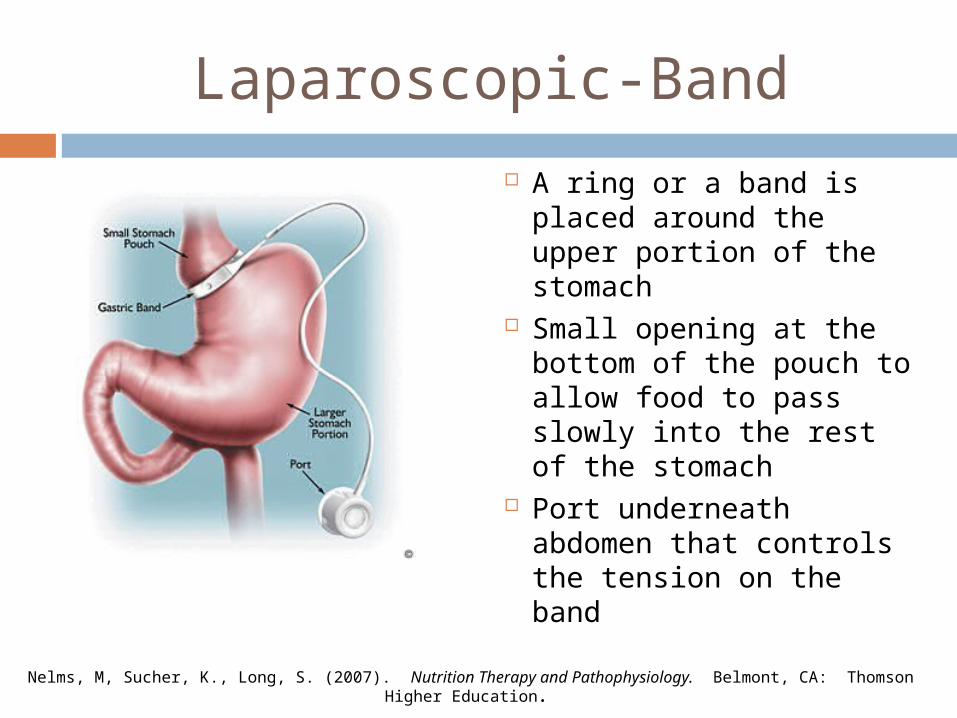
Laparoscopic-Band
A ring or a band is placed around the upper portion of the stomach
Small opening at the bottom of the pouch to allow food to pass slowly into the rest of the stomach
Port underneath abdomen that controls the tension on the band
Nelms, M, Sucher, K., Long, S. (2007). Nutrition Therapy and Pathophysiology. Belmont, CA: Thomson Higher Education.
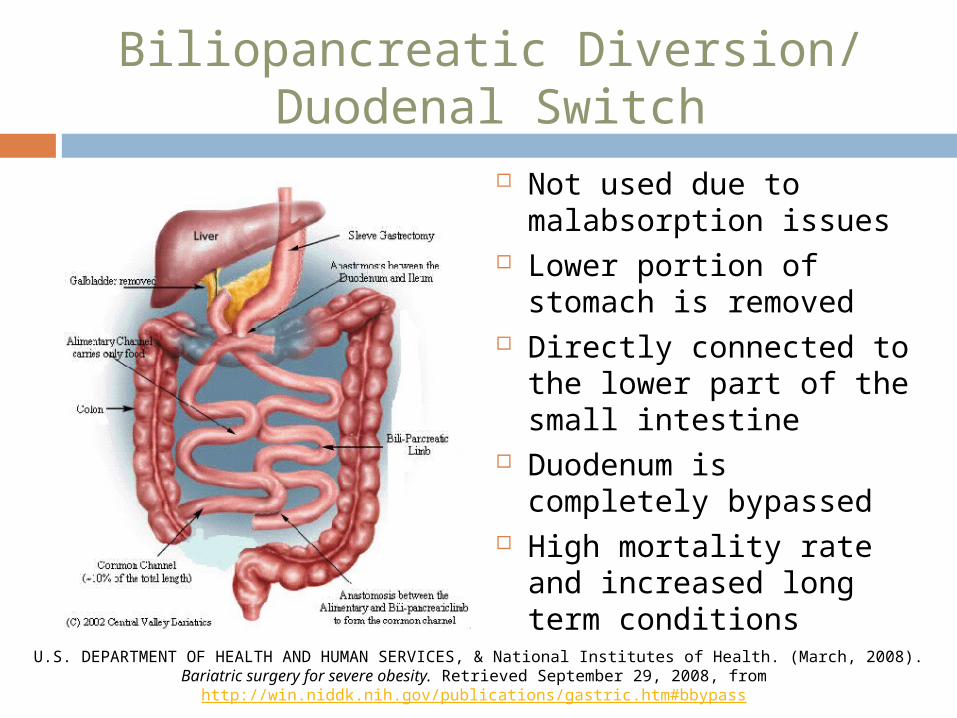
Biliopancreatic Diversion/ Duodenal Switch
Not used due to malabsorption issues
Lower portion of stomach is removed
Directly connected to the lower part of the small intestine
Duodenum is completely bypassed
High mortality rate and increased long term conditions
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, & National Institutes of Health. (March, 2008). Bariatric surgery for severe obesity. Retrieved September 29, 2008, from http://win.niddk.nih.gov/publications/gastric.htm#bbypass
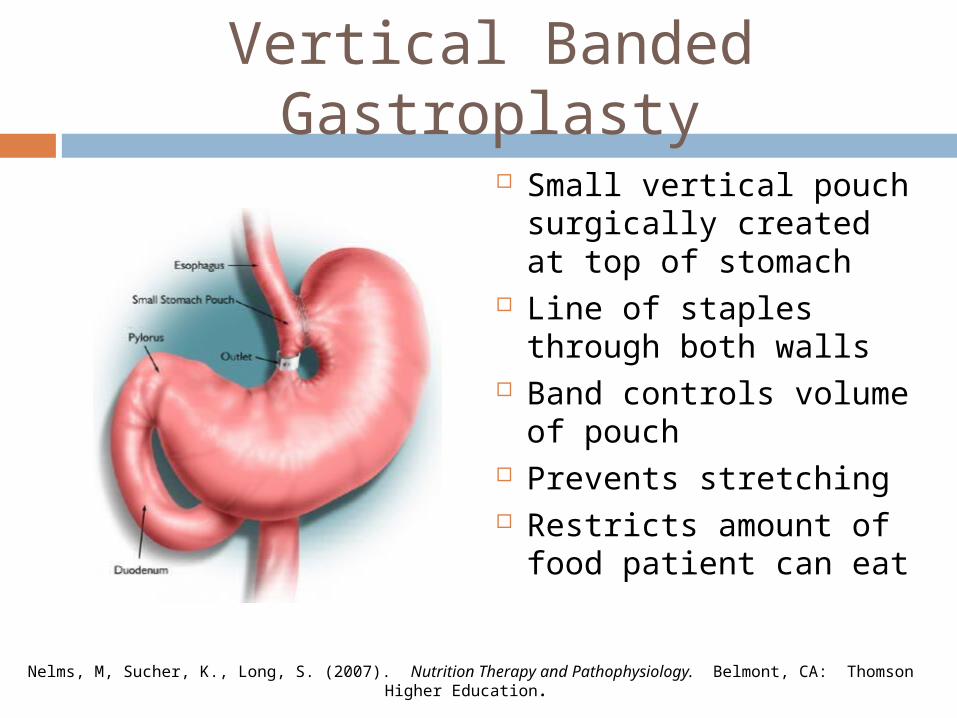
Vertical Banded Gastroplasty
Small vertical pouch surgically created at top of stomach
Line of staples through both walls
Band controls volume of pouch
Prevents stretching Restricts amount of
food patient can eat
Nelms, M, Sucher, K., Long, S. (2007). Nutrition Therapy and Pathophysiology. Belmont, CA: Thomson Higher Education.
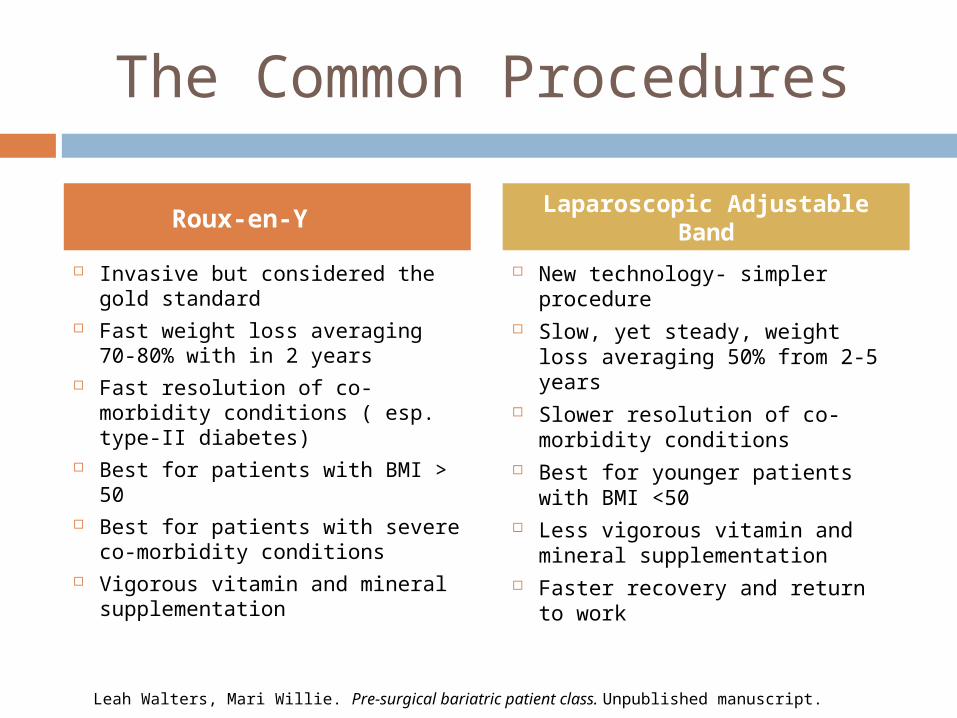
The Common Procedures
Invasive but considered the gold standard
Fast weight loss averaging 70-80% with in 2 years
Fast resolution of co-morbidity conditions ( esp. type-II diabetes)
Best for patients with BMI > 50 Best for patients with severe
co-morbidity conditions Vigorous vitamin and mineral
supplementation
New technology- simpler procedure
Slow, yet steady, weight loss averaging 50% from 2-5 years
Slower resolution of co-morbidity conditions
Best for younger patients with BMI <50
Less vigorous vitamin and mineral supplementation
Faster recovery and return to work
Leah Walters, Mari Willie. Pre-surgical bariatric patient class. Unpublished manuscript.
Roux-en-YLaparoscopic Adjustable
Band
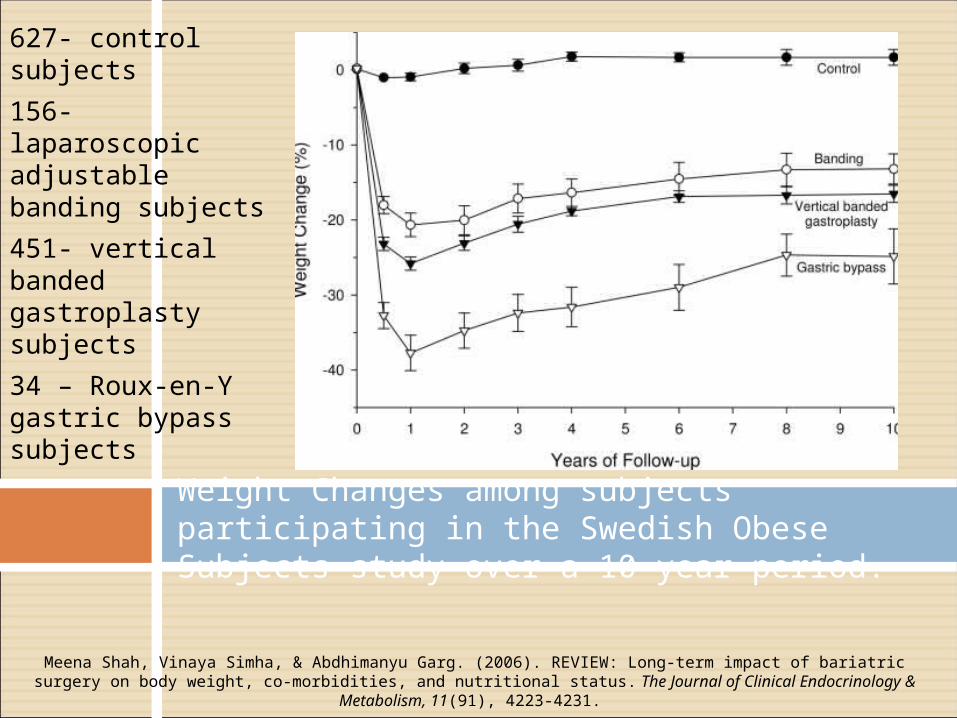
627- control subjects
156- laparoscopic adjustable banding subjects
451- vertical banded gastroplasty subjects
34 – Roux-en-Y gastric bypass subjects
Weight Changes among subjects participating in the Swedish Obese Subjects study over a 10-year period.
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
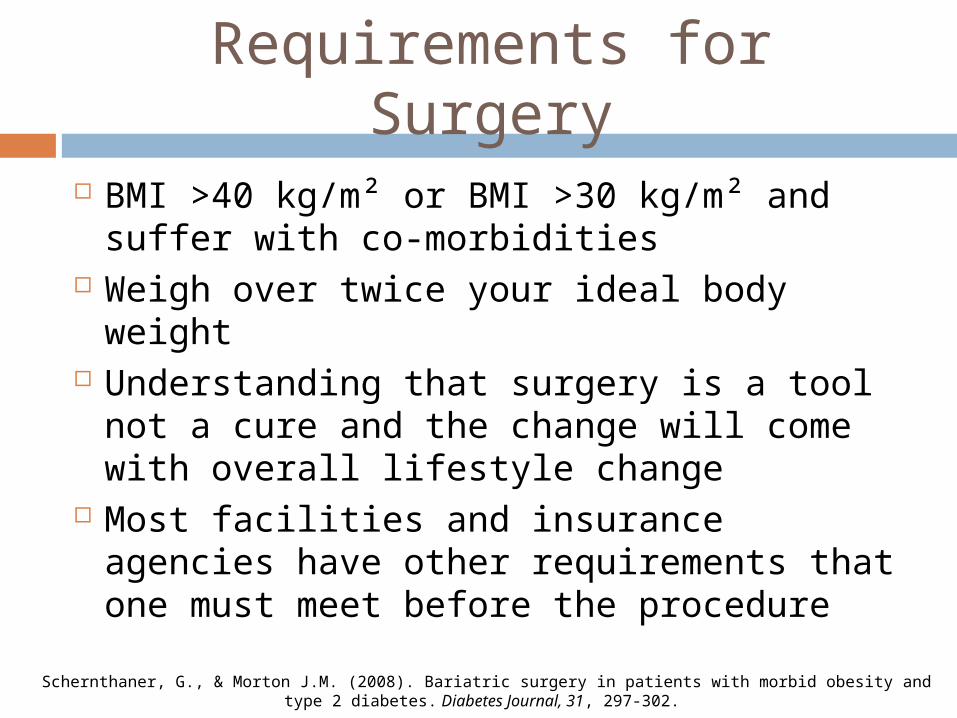
Requirements for Surgery
Schernthaner, G., & Morton J.M. (2008). Bariatric surgery in patients with morbid obesity and type 2 diabetes. Diabetes Journal, 31, 297-302.
BMI >40 kg/m² or BMI >30 kg/m² and suffer with co-morbidities
Weigh over twice your ideal body weight Understanding that surgery is a tool not
a cure and the change will come with overall lifestyle change
Most facilities and insurance agencies have other requirements that one must meet before the procedure
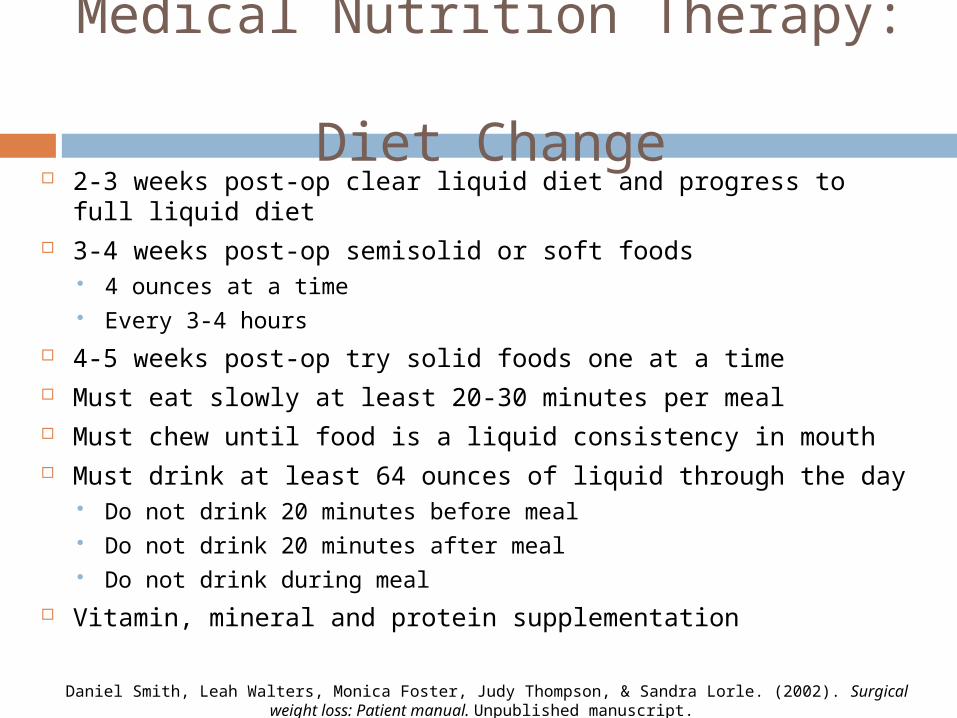
Medical Nutrition Therapy: Diet Change
Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
2-3 weeks post-op clear liquid diet and progress to full liquid diet
3-4 weeks post-op semisolid or soft foods 4 ounces at a time Every 3-4 hours
4-5 weeks post-op try solid foods one at a time Must eat slowly at least 20-30 minutes per meal Must chew until food is a liquid consistency in mouth Must drink at least 64 ounces of liquid through the day
Do not drink 20 minutes before meal Do not drink 20 minutes after meal Do not drink during meal
Vitamin, mineral and protein supplementation
Supplementation
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
With the limited diet patients will not get RDA for certain vitamins and minerals Vitamin B12, Iron, Folate, Calcium, Vitamin
D, Vitamin A Adequate protein intake is crucial for
healing post-op Can be taken in a multi-vitamin or
separate daily Make sure all supplements are chewable Must have correct dosage in multi-vitamin
Supplementation: B12 300-500µg/d Sublingual form (under the
tongue) Deficiency seen in 64% of
Roux-en-Y patients (Shah et al, 2006).
Important for protection of the nerve cells. Needed for cell synthesis and helps break down some fatty acids and proteins
Deficiency causes anemia, fatigue, degeneration of peripheral nervesMeena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight,
co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson
Wadsworth
Supplementation: Iron
Deficiency seen in 52% of Roux-en-Y patients (Shah et al, 2006)
Take with vitamin C to increase absorption
320 mg daily Prevents anemia Iron carries oxygen to
cells importantly muscle cells
Deficiency causes anemia
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Folate
Deficiency seen in 34% of Roux-en-Y patients (Shah et al, 2006)
400-1000 µg/d daily intake
Increased rate of neural defects in children born to Roux-en-Y mothers
Helps with protein synthesis
Deficiency causes anemia, weakness, confusion Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Calcium Deficiency seen in 10% of
surgical patients Recommended intake 1200-
1500 mg/d Take twice daily 500-600 mg/d
due to absorption rate Deficiency is not always
apparent at first because of calcium releasing from the bone
calcium citrate supplement more effective than calcium carbonate
Deficiency is seen as stunted growth in children and osteoporosis in adults
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Vitamin D
Deficiency seen in 51% of patients
Recommended supplementation is 400 IU/d
Recommended to take separate than iron supplement due to absorption
Important for bone health Deficiency is seen as
rickets in children and osteomalacia in adults
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson Wadsworth
Supplementation: Vitamin A 10% of Roux-en-Y patients
adapt vitamin A deficiencies It is recommended to have
supplementation as needed based on physician monitoring
Deficiency is due to some fat malabsorption
Important for sight and skin health
Deficiencies include: decreased immune function, blindness, night blindness, and some skin conditionsMeena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight,
co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231. Whitney E, & Rolfes S. R. (2005). In Elizabeth Howe (Ed.), Understanding nutrition (10th ed.). Belmont, CA: Thomson
Wadsworth
Supplementation: Protein
Protein is important post-op to help heal the surgical wound
Recommended 65 grams per day
Supplementation should be 200 calories with 15 grams of protein
High Protein Foods Fish Lean cuts of beef or
pork Skinless chicken or
turkey Dry beans/legumes Egg whites Non-fat or low-fat milk
and milk products Nuts and peanut
butter
Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Nutrition Care Process
Assessment Age, weight and
height BMI, and IBW Nutrient intake
Diagnosis Co-morbidities Obesity
Intervention Weight loss
program Bariatric surgery
Vitamin regimens Exercise regimens
Monitor Follow-up
appointments Vitamin regimens Exercise regimens
Lifestyle Change
Meena Shah, Vinaya Simha, & Abdhimanyu Garg. (2006). REVIEW: Long-term impact of bariatric surgery on body weight, co-morbidities, and nutritional status. The Journal of Clinical Endocrinology & Metabolism, 11(91), 4223-4231.
Exercise 30-6o minutes 3-5 days a week
Weight loss changed from 70% baseline to 90% baseline with exercise (Shah et al, 2006).
Strength training 2-3 times per week Positive attitude
Surround yourself with a positive social support group
Easier to manage stress
Ethical Issue: Overall Cost
Daniel Smith, Leah Walters, Monica Foster, Judy Thompson, & Sandra Lorle. (2002). Surgical weight loss: Patient manual. Unpublished manuscript.
Approximately $30,000-$50,000 for the surgery alone Can vary depending on health care facility
Approximately $100 monthly for vitamin supplements Can vary on brand and purchase company
$250-$300 for protein supplements Dependent on brand
Ethical Issue: Insurance Coverage
Insurance will cover surgery Insurance will not cover preventative care
Dietetic counseling before obesity gets out of control
Personal training sessions Insurance will not cover vitamin
supplementation This is a huge cost post-op Due to surgery supplementation is crucial
Ethical Issue: Surgical Requirements
The strict requirements may lead patients to gain weight before applying for insurance
Some facilities require weight loss before surgery Insures seriousness of patient Provides positive feedback for patient
Learn new lifestyle If gaining weight to meet BMI requirements
patient is not learning the new lifestyle Find a workout routine that works for them
Questions?