Embed Size (px)
Citation preview
Barriers and FacilitatorsTo making it Happen!
Daren K. HeylandProfessor of Medicine
Queen’s University, Kingston General HospitalKingston, ON Canada

Disclosures
Research Contracts with the Following Companies
• Nestle• Baxter• Fresenius Kabi• Abbott Nutrition

Results of 2007 Results of 2007 International Nutrition International Nutrition
Practice Audit Practice Audit
Cahill N Crit Care Med 2010 (in press)
Average time to start of EN : 46.5 hours (site average range: 8.2-149.1 hours)
In patients with high gastric residual volumes:use of motility agents 58.7% (site average range: 0-100%)
use of small bowel feeding 14.7% (range: 0-100%)

Adequacy of EN: KcalsAdequacy of EN: Kcals

Relationship Between Increased Calories and 60 day Mortality
BMI Group Odds Ratio
95% Confidence
Limits
P-value
Overall 0.76 0.61 0.95 0.014
<20 0.52 0.29 0.95 0.033
20-<25 0.62 0.44 0.88 0.007
25-<30 1.05 0.75 1.49 0.768
30-<35 1.04 0.64 1.68 0.889
35-<40 0.36 0.16 0.80 0.012
>=40 0.63 0.32 1.24 0.180
Legend: Odds of 60-day Mortality per 1000 kcals received per day adjusting for nutrition days, BMI, age, admission category, admission diagnosis and APACHE II score.
Alberda Int Care Med 2009;35:1728


A Qualitative Assessment of A Qualitative Assessment of “Barriers and Facilitators” “Barriers and Facilitators”
to Implementing Nutrition CPGs to Implementing Nutrition CPGs in ICUin ICU
Multiple case study 4 case ICU sites Purposeful sampling
Semi-structured key informant interviews (n=28) Min. 5 years ICU experience Employed at case ICU site May 2004
Document review
Jones NCP 2007;22:449

Potential BarriersPotential Barriers
Resistance to change Patients clinical
condition
Lack of awareness Information overload Weak evidence Resource constraints Slow administrative
process Impractical / Complex Nursing workload Limited critical care
experience

Potential FacilitatorsPotential Facilitators
Agreement of the attending physician & ICU team Part of routine practice Dietitian / Opinion leader Access / Visibility Easy to follow and perform Provision of education Open discussion

Favored Favored Implementation Implementation StrategiesStrategies Informal one-on-one discussions
Academic detailing, ward rounds
ProtocolsPre printed orders, Check-list, algorithms,
Bed-side reminders Feedback and audit
Site reports

The Impact of Enteral Feeding Protocols The Impact of Enteral Feeding Protocols on Enteral Nutrition Delivery:on Enteral Nutrition Delivery:
Results of a multicenter observational Results of a multicenter observational studystudy International, prospective, observational, cohort studies conducted in
2007 and 2008 from 269 Intensive Care Units (ICUs) in 28 countries Included 5497 mechanically ventilated adult patients > 3 days in ICU Sites recorded the presence or absence of a feeding protocol Sites provided selected nutritional data on enrolled patients from ICU
admission to ICU discharge for a maximum of 12 days.
Heyland JPEN 2010 ( in press)
P<0.05
78% of sites reported use of Feeding Protocol


Initial Efficacy and Tolerability of Initial Efficacy and Tolerability of Early Enteral Nutrition with Early Enteral Nutrition with
Immediate or Gradual Introduction in Immediate or Gradual Introduction in Intubated PatientsIntubated Patients
Desachy ICM 2008;34:1054
• This study randomized 100 mechanically ventilated patients (not in shock) to Immediate goal rate vs gradual ramp up (our usual standard).
• The immediate goal group rec’d more calories with no increase in complications

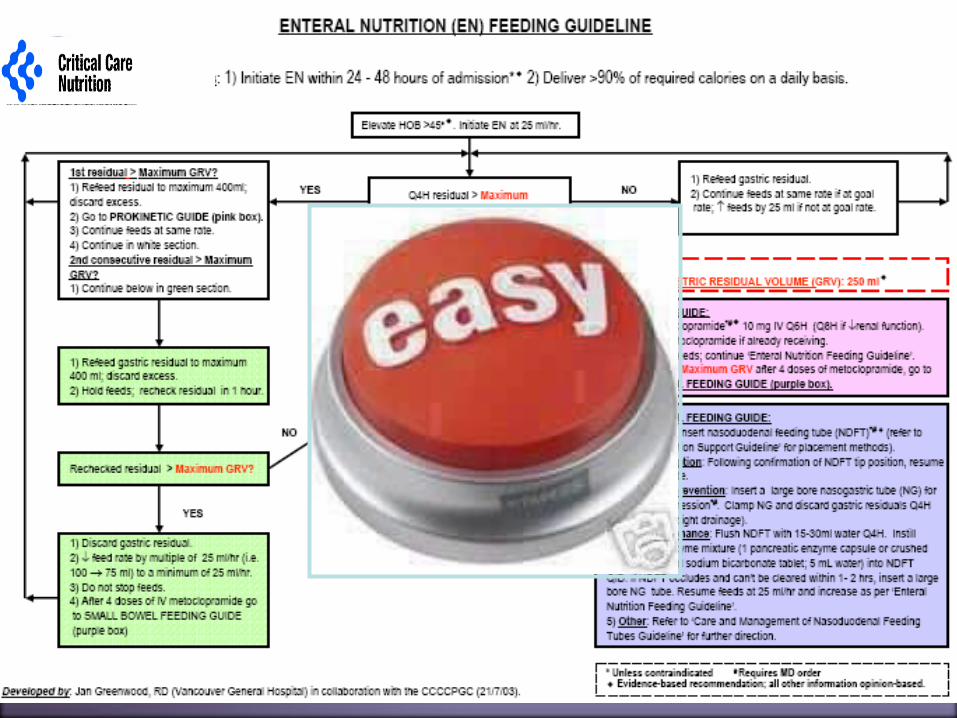
Not all critically ill patients are the same; we have different feeding options based on hemodynamic stability and suitability for high volume intragastric feeds.
Use semi elemental solution In select patients, we start the EN immediately at goal rate,
not at 25 ml/hr. We target a 24 hour volume of EN rather than an hourly
rate and provide the nurse with the latitude to increase the hourly rate to make up the 24 hour volume.
Tolerate higher GRV threshold (250 ml or more) Motility agents and protein supplements are started
immediately, rather than started when there is a problem.
The Efficacy of Enhanced The Efficacy of Enhanced PProtein-rotein-EEnergy nergy PProvision via the Enteral Rorovision via the Enteral Rouute in Critically Ill te in Critically Ill
PPatients: atients: The PEP uP Protocol!The PEP uP Protocol!
A Major Paradigm Shift in How we Feed Enterally

The Efficacy of Enhanced The Efficacy of Enhanced PProtein-rotein-EEnergy nergy PProvision via the Enteral Rorovision via the Enteral Rouute in Critically Ill te in Critically Ill
PPatients: atients: The PEP uP Protocol!The PEP uP Protocol!
Figure 2.1 Adequacy of Calories from EN (Before Group vs. After Group on Full Volume Feeds)
PLOT Before Group After Group
% calories received/prescribed
0
10
20
30
40
50
60
70
80
90
100
ICU Day
1 2 3 4 5 6 7
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Total P-value 0.049 0.0005 0.17 0.31 0.60 0.34 0.20 0.015
Heyland (in submission)

The Efficacy of Enhanced The Efficacy of Enhanced PProtein-rotein-EEnergy nergy PProvision via the Enteral Rorovision via the Enteral Rouute in Critically Ill te in Critically Ill
PPatients: atients: The PEP uP Protocol!The PEP uP Protocol!
Heyland (in submission)
Figure 2.2 Adequacy of Protein from EN (Before Group vs. After Group on Full Volume Feeds)
PLOT Before Group After Group
% protein received/prescribed
0
10
20
30
40
50
60
70
80
90
100
110
120
ICU Day
1 2 3 4 5 6 7
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Total P-value 0.014 <0.0001 0.0015 0.13 0.57 0.62 0.34 0.002

Need for Constant Need for Constant RemindersReminders

PosterPoster

ReminderHOB
sticker
ReminderHOB
sticker
Reminderscreensavers
Reminderscreensavers

Early Enteral Nutrition in the ICU:Early Enteral Nutrition in the ICU:The Clock Is Ticking!The Clock Is Ticking!
Daren K. Heyland, MD, FRCPC, MScProfessor of MedicineQueen’s University Kingston, Ontario
Special DVD presentation

www.criticalcarenutrition.com


Overall Site PerformanceOverall Site Performance

Protocolize/automate care Improve organizational cultureDevelop Dietitian and other KOL as local opinion
leaders Audit and feedback with bench-marked site reports Assess barriers and have interactive workshops with
small group problem solving Implement strategies with rapid cycle change
(PDSA)Educational reminders (manuals, posters, pocket
cards) One on one academic detailing
Practice Changing Practice Changing InterventionsInterventions

What works best at your site?
(barriers and enablers will vary site to site)
What is already working well at your site?
(strengths and weakness are different across sites)
ConclusionsConclusions
Long way to go to narrow the quality gap Need to enrich our understanding on how best to
achieve that; but in the mean time, act now! With our emerging understanding of the problems, we
need to develop more targeted or strategic solutions.Strengths & weaknesses; barriers & enablers vary across
sites. Stay tuned…