Embed Size (px)
Citation preview

Basal-Bolus, Insulin Pumps, Carbohydrate
Counting, Combination Therapy
Dr.Ihab TadrosMedical Director
Daisy Care Medical – USAThe Leader in insulin Pump Therapy

Educational Objectives At the completion of this presentation the attendee will
be able to: Describe the principles behind physiologic basal-bolus
insulin therapy. Recite the principles and the indications for CSII
(Insulin pump therapy) in the management of diabetes.
Apply the concepts of counting grams for appropriate insulin therapy and review the Quick-Carb Count system for determining carbohydrate grams.
Discuss the principles and appropriate indications for combination therapy.

4:00
25
50
75
8:00 12:00 16:00 20:00 24:0024:00 4:00
Breakfast Lunch Dinner
Pla
sma
Insu
lin
µU
/ml)
Physiological Insulin Secretion Profile
Time

Comparative Action of Insulins
Onset Peak Duration
Lispro 5-15 min 0.5-1.5 hr 5 hr
Aspart 5-15 min 0.5-1.5 hr 5 hr
Glulisine 5-15 min 0.5-1.5 hr 5 hr
Regular 30-60 min 2-3 hr 6-8 hr
NPH 2-4 hr 4-10 hr 10-16 hr
Glargine 2-4 hr None 20-24 hr
Detemir 2-4 hr None 12-24 hr

Profiles of Human Insulins and Analogs
0 2 4 6 8 10 12 14 16 18 20 22 24
Pla
sma in
sulin
levels
Regular (6–8 h)
NPH (10–16 h)
Hours
Detemir, Glargine (20-24 h)
Aspart, Glulisine, Lispro (4–5 h)

Insulins That Most Closely Match the Physiologic Insulin Profile Bolus (prandial) insulin analogs
Rapid acting When taken ten minutes before eating, most
closely coincides with CHO absorption rate Basal (background) insulin analogs
Long-acting Slow and steady rate of absorption
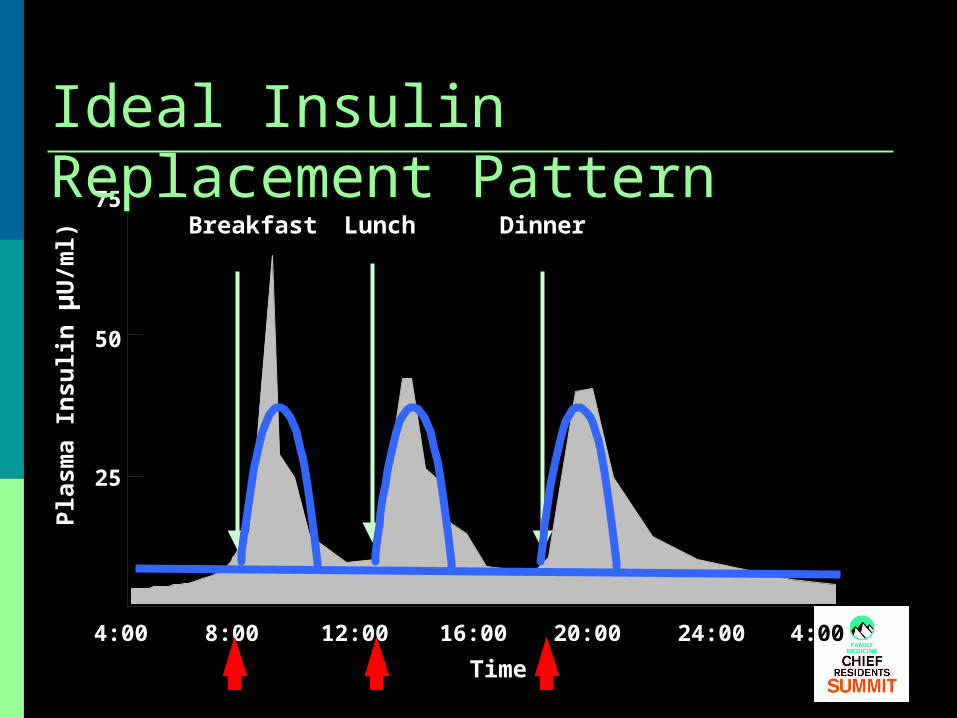
4:00
25
50
75
16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
Pla
sma
Insu
lin
µU
/ml)
Ideal Insulin Replacement Pattern
12:008:00
Time
Augmentation of the Beta-Cell Exogenous insulin administered to
augment endogenous production Often required at about 6 years post
diagnosis Glucose rises in spite of treatment with
oral antidiabetic drug(s)

Mr. Brown 52 yo CM with T2DM for 7 years Treated with SU, metformin, lifestyle
changes Has lost 28 pounds since diagnosis Walks 30-45 minutes 5-6 days per week
Last A1C has increased from 7.2% to 9.3% and HGM has indicated rising values

ARS Question #1 What do you recommend?
1. Do you add another oral agent?2. Do you consider an alternative agent?3. Do you consider insulin?
Mr. Brown Insulin therapy has the best chance of
achieving target A1C The natural history indicates that insulin is
needed Other agents work in the presence of
adequate insulin—endogenous plus exogenous
Mr. Brown Choices for beginning insulin
Basal insulin each evening Insulin detemir (Levemir) Insulin glargine (Lantus) NPH
Combination (rapid-acting/ intermediate acting) insulin before evening meal
Insulin protaminated aspart/ aspart (NovoLog 70/30) Insulin protaminated lispro/lispro (Humalog 75/25)

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
12:008:00
Time
Detemir, Glargine
Pla
sma
Insu
lin
Basal Insulin Bedtime Only

Analog Mixed Insulin Program
4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
12:00
Time
Pla
sma
Insu
lin
8:00

ARS Question #2 How do you begin insulin therapy?
1. Insulin detemir 0.1-0.2 units/kg or 10-20 units each evening
2. Insulin glargine 0.1-0.2 units/kg or 10-20 units each evening
3. Insulin protaminated aspart/aspart (NovoLog Mix 70/30) 12 units before evening meal
4. Any of the above

24-Hour Plasma Glucose CurveNormal and Type 2 Diabetes
Time of Day
400
300
200
100
0
0600 06001000 1400 1800 2200 0200
NEJM 318: 1231-1239, 1988
Glu
cose
(m
g/d
L) Diabetes
Normal

ARS Question #3 What do you do with the existing
oral agents?1. Continue the SU and metformin2. Continue the SU but not metformin3. Continue metformin but not the SU4. Discontinue the SU and metformin

Mrs. Blue 59 yo AAF with T2DM for 13 years
Currently treated with SU, MF, and insulin detemir once each evening
Recently her A1C has increased from 7.4% to 8.5%

ARS Question #4 What do you now recommend?
1. Continue SU and metformin; give insulin detemir twice daily
2. Discontinue SU and metformin; give insulin detemir twice daily
3. Discontinue SU, add bolus insulin before largest meal (dinner)
4. Discontinue SU, add bolus insulin before breakfast and dinner
5. None of the above

Diabetes 44: 1249-1258, 1995
UKPDS: β-Cell Function over 6 Years
Years After Diagnosis
-C
ell
Funct
ion
(%
)
N=376
51% residual secretion
28% residual insulin secretion
Decline to insulin deficiency ~ 12 yrs after Dx!
Insulin loss starts 10 yrs before Dx.
Half gone by Dx.
Insulin loss is part of T2 DM
10/22/02

Replacement Insulin Therapy Beta cells are now producing very little
insulin She requires a physiologic insulin
replacement regimen Basal-bolus system Similar to a patient with T1DM

4:00
25
50
75
8:00 12:00 16:00 20:00 24:0024:00 4:00
Breakfast Lunch Dinner
Pla
sma
Insu
lin
µU
/ml)
Physiological Insulin Secretion Profile
Time

Mrs. Blue Insulin choices
Basal Insulin detemir Insulin glargine
Bolus Insulin aspart Insulin lispro Insulin glulisine

4:00
25
50
75
16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
Pla
sma
Insu
lin
µU
/ml)
Ideal Insulin Replacement Pattern
12:008:00
Time

As Patients Get Closer to A1C Goal, the Need to Manage PPG Significantly Increases
Adapted from Monnier L, Lapinski H, Collette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of Type 2 diabetic patients: variations with increasing levels of HBA(1c). Diabetes Care. 2003;26:881-885.
Increasing Contribution of PPG as A1C Improves
% C
on
trib
uti
on
A1C Range (%)

4:00 16:00 20:00 24:00 4:00
Breakfast LunchLunch Dinner
12:008:00
TimeTime
Detemir/ Glargine
Basal + Meal-Related Regimen
Pla
sma
Insu
lin
Aspart Aspart, Aspart, Lispro Lispro, Lispro,Glulisine Glulisine Glulisine

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
12:00
Time
Pla
sma
Insu
lin
8:00
Basal Insulin: Twice Daily - AM & Bedtime
Detemir/ Glargine

Mrs. Blue In a person with T2DM
Total daily insulin dose = 1.0 -1.2 units/ kg Divide total daily dose
50% basal insulin (insulin detemir, glargine) Give each evening and adjust based on the fasting
glucose 50% bolus insulin (insulin aspart, glulisine, lispro)
Give pre-meal and adjust based on the next pre-meal glucose or ideally 2 hours post-meal
Goal: 2 h post-meal = pre-meal +/- 40 mg/dL

Mrs. Blue Most patients will require more insulin on
board in the AM (physiologic basis) Start with bolus dose divided pre-meal 1/3, 1/3,
1/3 Adjust based on post-prandial blood glucose
Most patients require: 38% of total bolus dose pre-breakfast 28% of total bolus dose pre-lunch 33% of total bolus dose pre-dinner

ARS Question #5 What to do with the oral agents?
1. Discontinue the SU and metformin2. Discontinue the SU, continue metformin3. Discontinue metformin, continue the SU4. Continue the SU and metformin

Mrs. Blue1. Discontinue the SU
Very little beta-cell reserve No reason to give an agent to stimulate phase
2 insulin release
2. Continue metformin Improve insulin resistance Lowers total insulin requirement Limits potential weight gain

Continuous Subcutaneous Insulin Infusion (CSII): Insulin Pump Therapy Principles
Allows reproduction of an intact endogenous system of insulin release
Allows variation in the basal infusion rate during the 24-hour period
Allows an immediate insulin bolus with carbohydrate intake
Allows temporary suspension (cessation) of insulin infusion

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Basal infusion
Bolus Bolus Bolus
Pla
sma
insu
lin
Variable Basal Rate: CSII Program

Indications for CSII Elevated A1C Hypoglycemia Exercise Dawn phenomenon Pregnancy Gastroparesis
Changing work schedules
Changing work/ activity demands
Pediatric patients requiring small insulin dosages
Special situations—menstrual cycles

Applications of CSII Any person with diabetes who faces
specific problems or complications Type 1 diabetes Type 2 diabetes
Loss of beta-cell reserve and endogenous insulin production
Requires a “C-peptide of less than 110 percent of the lower limit of normal of the laboratory’s measurement method”
Required by Medicare and many insurance companies
Patient Requirements for Pump Use Motivated to improve control Willingness to monitor BG 4-6 times a day Willingness to do CHO counting Willingness to participate in regular
medical follow-up Covered by insurance or can afford
increased costs

Carbohydrate Counting Insulin dosing (bolus) is based on CHO intake Permits more exact dosing of insulin Carbohydrate content can be easily determined Requires familiarity with CHO vs. proteins or fats Requires familiarity with portion sizes Requires ability to do simple calculations Consider referral to CDE Direct patient to materials on CHO counting

Quick-carb Counting All of the below contain approximately 15
grams of carbohydrate: ½ cup or 4 oz of fruit juice ½ cup canned fruit 1 cup or 8 oz of whole fresh fruit 1 slice of bread, 6 inch tortilla, 2 oz bagel 1 cup of milk ½ cup of potatoes, rice, pasta, beans, peas

Reading Food
Labels

Fat free can be misleading

Quick-carb Counting Dosage of insulin is based on total grams of
carbohydrates Insulin: CHO ratio of 1:15
If the total grams of carbohydrate is 60, then 4.0 units of insulin would be administered.
Insulin: CHO ratio of 1:10 If the total grams of CHO is 60, then 6.0 units of insulin would
be administered. T2DM patients may require 1 unit for each 3-5 grams of CHO
Ex: 60 g 3 units/g = 20 units or 60 g 5 units/g = 12 units
How do you know? Test the blood glucose 2 hours post prandial

Correction Factor Generally 1 unit of insulin will drop blood
glucose by 30-50 points To determine if this is true for your patient
– ask them to test Use either the 1500 or 1800 rule
1500 rule for short-acting insulin (Regular) 1800 rule for rapid-acting insulin
It is an art – not an exact science
Insulin Sensitivity Factor 1800 = Insulin Sensitivity Factor TDD
Example:1800 = 50
36 units
One unit of rapid-acting insulin will affect glucose by 50 mg/dL
TDD = Total Daily Dose of Insulin

Putting it All Together GH is about to eat lunch. His BG is 183. He
is planning to eat a salad, a six inch Subway club sandwich, a small bag of Sunchips and a diet soda.
How many CHO in this meal? How much insulin to cover the CHO?
(Imagine a 1:15 insulin to CHO ratio)
What is target pre-meal BG? How much insulin to correct for 183?
How much total insulin for this meal?

What Does My Patient Need to Know About Using Insulin? Blood glucose goals and testing regimen Insulin action profile and how insulin,
physical activity and food all impact blood glucose
Signs and symptoms of hypoglycemia How to treat How to prevent
Sharps disposal Storage of insulin

Finding the Right Therapy for Your Patient Who is the patient?
BG profile Fairly stable or wide variation?
Psychosocial/cultural factors Dexterity Lifestyle and willingness to adhere to regimen
About the insulin regimen Ability to mimic endogenous insulin secretion Potential adverse effect Cost Complexity

Summary Timely initiation of insulin is critical Insulin analogs most closely match normal
physiology There is a wide variety of insulin regimens and
insulin delivery methods It is important to match the insulin regimen to
patient lifestyle and characteristics When blood glucose goals are not met, titrate
insulin in a timely manner Refer to a Certified Diabetes Educator

Basal-Bolus, Insulin Pumps, Carbohydrate
Counting, Combination Therapy
Dr.Ihab TadrosDaisy Care Medical – USA
The Leader in Insulin Pump TherapyAnd Diabetes Management





























