Embed Size (px)
Citation preview

BASH GPwSI Group Audit: what do we image and why?Steven Elliot
GPwSI Tier 2 Neurology Salford
Aim
Assess adherence to and relevance of
the BASH guidelines on imaging patients with suspected brain tumour
Objectives
Record all patients seen Record numbers of patients scanned Record reasons for scans Reflect on non-guideline scans

Standards
95% of scans would be red or orange flags as stipulated by guidelines

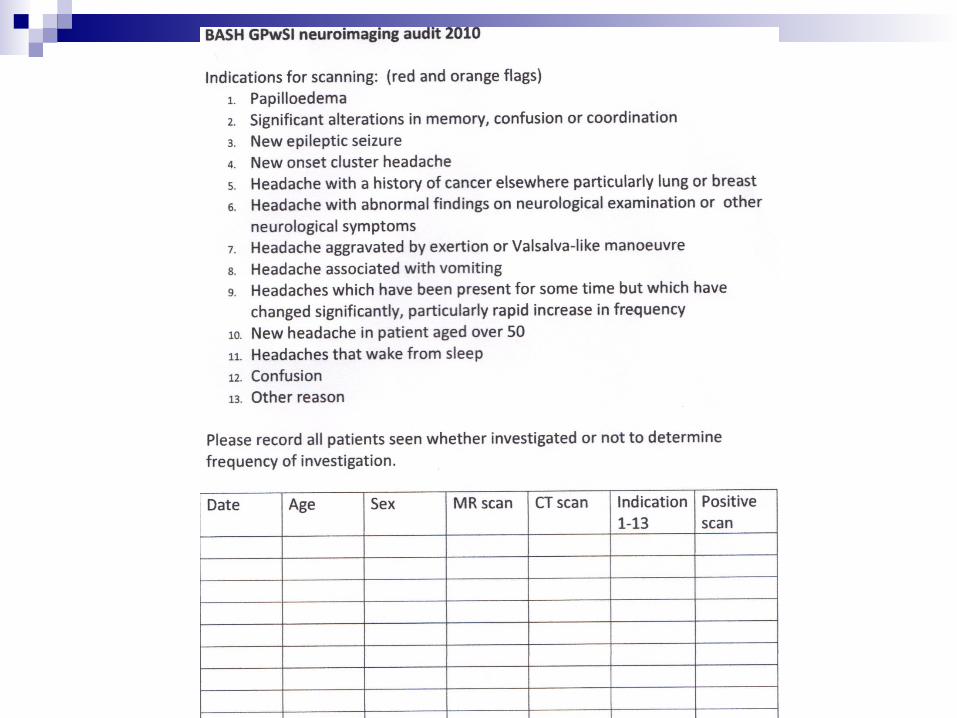
Red flags
Papilloedema New epileptic seizure New onset cluster headache Abnormal findings on examination/neurological
symptoms History of cancer especially lung/breast Significant alteration consciousness, memory,
confusion or co-ordination.

Orange flags
Aggravated by exertion/Valsalva Headache associated with vomiting Headache which has increased in
frequency New onset >50 Headache waking from sleep Confusion

Methods
3 month baseline measurement 2010 Standard audit tool Anonymised collated analysis Reflection and recommendation Personal and/or group re-audit 2011
Baseline results
14 GPwSIs 3month period 895 patients 270 scans (30.16%) 173 (64%) Red or orange flags 54 red flags 16/270 “positive” (5.6%) Average scan rate 32.86%

0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12 13
% scan
Seen
Positive
Scanned
Activity

0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12 13
Indication
Positive
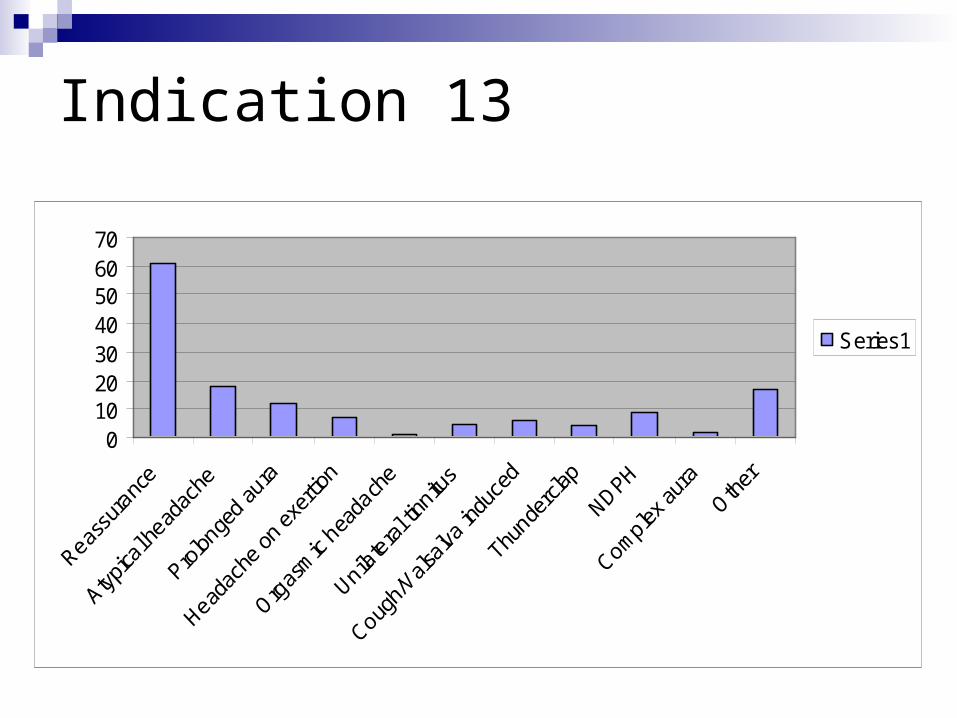
Indication for scan
010203040506070
Series1
Indication 13

Positive scansIndication 7 Intracranial hypotension Bilateral subdurals Grade 1 Chiari Left orbital abnormality Mild Chiari ChiariIndication 8 Sinus thickeningIndication 9 1cm lesion right temporal lobe Aneurysm Indication 13 CVST Multiple emboli Frontal lobe infarct Aneurysm Infarct left parietal lobe Left parietal infarct Glioma

Conclusions
Not adherent Need for personal reflection Need for group reflection Not clear that guidelines are relevant Need for non-cancer indications What do we do about the anxious patient? True positive rate 1.5%


Planning re-audit
Change scanning habits? Change criteria? Give up!

Suggested criteria 1

New criteria 2 New undifferentiated headache where a pattern
has not emerged after 8 weeks Headache aggravated or precipitated by exertion
or Valsalva manoevre, cough or sex and not migraine
Headache associated with vomiting and not migraine
Headache which has increased in frequency/severity in the last six months despite appropriate treatment

New criteria 3
New headache in age >50 whose onset is less than 6 months ago
Headache that wakes from sleep that is not migraine
Thunderclap headache Patient whose anxiety is not relieved by
explanation and is aware of the implications of incidental findings

New criteria 4
New daily persistent headache Headache suggestive of low intracranial
pressure Recent onset headache in HIV or
immmunocompromised

Re-audit
Suggestions? Agree criteria Repeat recording of activity in January to
March 2012 Any volunteers?