Embed Size (px)
Citation preview
Technical Proposal
Technical Proposal · November 2009 · Original
Contact Person: Beate Neumeyer · [email protected] · T + 49.(0)7021.970 8718
AGEG Consultants eG · Jesinger Str. 52 · 73230 Kirchheim unter Teck · Germany
German Financial Cooperation with Pakistan
Basic Health Programme in FATA
BMZ Number 2008 66 517
KfW German Development Bank

KfW – Pakistan – Basic Health Programme in FATA 2
Content
List of Abbreviations 3
1 Introduction and Background 4
2 Interpretation of the tasks 6
3 Proposal for the Implementation 15
4. Project Management 21
5 Presentation of the Team 23
Annex: CVs of Professional Staff 25
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 3
List of Abbreviations
CAMP Community Appraisal & Motivation Programme
CDR Case Detection Rate
DHS Directorate of Health of the FATA Secretariat
FATA Federally Administered Tribal Areas
FC Financial Cooperation
FR Frontier Regions”
FR Frontier Region
GTZ Gesellschaft für technische Zusammenarbeit
IDP Internally Displaced People
IEC Information, Education and Communication
LGOs Local Government Ordinances
MALC Marie Adelaide Leprosy Center
NGO Non.governmental Organisation
NWFP North-West Frontier Province
PEA Project Exectuing Agency
PHC Primary Health Care
PIU Project Implementing Unit
SDP Sustainable Development Plan
TC Technical Cooperation

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 4
1 Introduction and Background
1.1 Introduction
In the framework of Financial Cooperation (FC) between the Islamic Republic of Pakistan and Germany, the German Government has offered a grant of EUR 5.38 million for health interventions in the Federally Administered Tribal Areas (FATA) to contribute to improving priority health care services in the underserved and politically unstable target area.
The Programme includes the financing of equipment, infrastructure, consumables, vehicles, drugs, mobile health care, mother and child health care, trainings, and consulting services for the Health Programme FATA. The Programme will be implemented in cooperation with GTZ (Gesellschaft für technische Zusammenarbeit).
1.2 AGEG Expe-rience in Pakis-tan
AGEG has been working in Pakistan for a number of years as the lead consultant for some German TC (Technical Cooperation) and FC projects which relate to the present proposal:
• Strengthening the Tuberculosis Control Program in NWFP/FATA, PN 2000.2247.5, since January 2004, with GTZ (TC)
• Strengthening the Tuberculosis Control Program in NWFP, PN 2000.66.290, since March 2007, with KfW (FC)
• Health Infrastructure AJK, PN 2005 66 398 and PN 2006 70 042, with KfW (FC)
1.3 Proposal De-velopment
In August 2008 a pre-feasibility study was conducted in cooperation with the concerned Health Authorities for the detailed preparation of the Basic Health Programme FATA.
In September 2009, KfW invited AGEG Consultants eG to develop and submit a technical and financial proposal for the Programme FATA” with the BMZ No. 2008 66 517.
The proposal development could not advance as fast as desired, (i) because of the worsening security situation and (ii) because GTZ up to date has not clearly defined its own program design for TB control support in North-West Frontier Province (NWFP) and FATA for the next phase starting January 2010, making a coordinated approach difficult.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 5
1.4 Map of the Region:

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 6
2 Interpretation of the tasks
2.1 Context analysis
Situated midway along Pakistan’s border with Afghanistan, FATA stretches over 450 km and consists of seven “Political Agencies” (Bajaur, Khyber, Kurram, Mohmand, North Waziristan, Orakzai, and South Waziristan) and six smaller zones, called “Frontier Regions” (FR) in the districts of Bannu, Dera Ismail Khan, Kohat, Lakki Marwat, Peshawar and Tank. The region is home to a mainly Pashtun population in more than a dozen major tribes and hundreds of clans and sub-tribes. FATA covers about 27,220 km2 and has about 3,4 million people1. However, there is a strong migration exchange with Afghanistan, and presently the ongoing military activities have caused heavy internal migration with over 100.000 Internally Displaced People (IDP). Bajaur Agency has the highest population with almost 800.000 people and the highest population density with 460 persons/km2.
Under the constitution, FATA is included among the “territories” of Pakistan. It is represented in the National Assembly and the Senate but remains under the direct executive authority of the President. Laws framed by the National Assembly do not apply here unless so ordered by the President, who is also empowered to issue regulations for the “peace and good government” of the tribal areas. Today, FATA continues to be governed primarily through the Frontier Crimes Regulation 1901. It is administered by the Governor of the NWFP in his capacity as an agent to the President of Pakistan, under the overall supervision of the Ministry of States and Frontier Regions in Islamabad. The system of devolution introduced elsewhere in the country in 2001 by means of provincial Local Government Ordinances (LGOs) has not been extended to the tribal areas. Rather, a separate LGO for FATA has been elaborated which works through councillors.
In 2002, a FATA Secretariat was set up, headed by the Secretary FATA. In 2006, the Civil Secretariat FATA was established to watch over decision-making functions, with an Additional Chief Secretary, four secretaries and a number of directors. Project implementation is now carried out by line departments of the Civil Secretariat FATA. The NWFP Governor’s Secretariat plays a coordinating role for the interaction between the federal and provincial governments and the Civil Secretariat FATA.
Each tribal agency is administered by a political agent, assisted by a number of assistant political agents, tehsildars (administrative head of a tehsil) and naib tehsildars (deputy tehsildars), as well as members from various local police (khassadars) and security forces (levies, scouts).
The political agent plays a supervisory role for development projects and chairs an agency development sub-committee. An FR is administered by the district coordination officer of the respective settled district, who exercises the same political power in an FR as the political agent does in a tribal agency.
Interference in local matters is kept to a minimum. The tribes regulate their own affairs in accordance with customary rules and unwritten codes, characterized by collective responsibility for the actions of individual tribe members and territorial responsibility for the area under their control. The
1 FATA MICS Multiple Indicator Cluster Survey 2007

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 7
government functions through local-level tribal intermediaries, the maliks (representatives of the tribes) and lungi holders (representatives of sub-tribes or clans), who are influential members of their respective clan or tribe. All criminal and civil cases in FATA are decided under the Frontier Crimes Regulation 1901 by a jirga. Residents of the tribal areas may, however, approach the Supreme Court of Pakistan and Peshawar High Court.
In the FATA, only 7% of the area is cultivated. Public and private sector development is linked to a small elite, leaving most of the population very poor. The urban population is only around 3%, while 97% live in rural areas. Overall literacy is at 18% (1998), for females from 10 years up just 3%. Those who are able to travel find work in cities across Pakistan as well as in the Middle East, using their earnings to support families at home. The result is an acute shortage of doctors, teachers and skilled workers in general, and in particular a dearth of qualified female teachers and doctors. Around 36% of households receive remittances from other parts of the country. 43.5% of the population listen to Government radio channels. FM radios are listened to by 16.1% of households, TV is watched by 13.6% of households in FATA. Only 41.5% of the population have access to safe water supply.
2.2 Health Indi-cators
Health indictors for FATA are incomplete and in many cases only estimates are available. In line with the FATA Sustainable Development Plan 2006 - 2015 (SDP) objective to obtain better data for informed decision-making, the FATA Secretariat with the financial and technical assistance of UNICEF, have carried out the first population based survey (MICS, Mutliple Indicator Cluster Survey) in 2007 from which many of the following data are taken. Results were published in 2009. While until then very few data with weak validity have been available, these data manifest the political will to advance the development in FATA based on more robust information (despite severe problems in data collection and ana-lysis). Other data sources are the “FATA Sustainable Development Plan (2006 - 2015)” and sporadic data from NGO projects.
The infant mortality rate is estimated to be 87 deaths per 1,000 live births for both sexes, with elevated mortality for males (male 95, female 72). The under-five mortality rate in FATA was 104 per 1,000 live births (male 110, female 80). Maternal mortality is thought to exceed 600 deaths per 100,000 live births2. Using the “Sisterhood Method”, the MICS came up with a rate of 380 per 100,000 live births, which is considerably higher than in Pakistan (276) and NWFP (275).
Of children aged 0-59 months, 33.2% are underweight and 16.3% are severely underweight. Males are more affected than females, rural areas more than urban areas3.
2.3 Health Care System
Health service provision is very limited in FATA. There is only 1 doctor for 7,670 population (Pakistan: 1,226) and 1 hospital bed for 2,179 population (Pakistan: 1,341).
There are no private hospitals in FATA, although services are offered by private medical practitioners. These include doctors qualified in Afghanistan and the former Soviet republics, who are not recognized by the Pakistan
2 FATA SDP 3 FATA MICS 2007
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 8
Medical and Dental Association, as well as local prayer leaders and faith healers.
The first major challenge confronting the health care sector is restricted access to health services, especially for the poorer and more vulnerable segments of the population. Restrictions are physical, cultural (especially for females), administrative (staff absenteeism, staff availability) or financial (unofficial payments and opportunity costs). Modern health care practices like institutional delivery and neonatal care are not generally accepted, due to cultural reluctance.
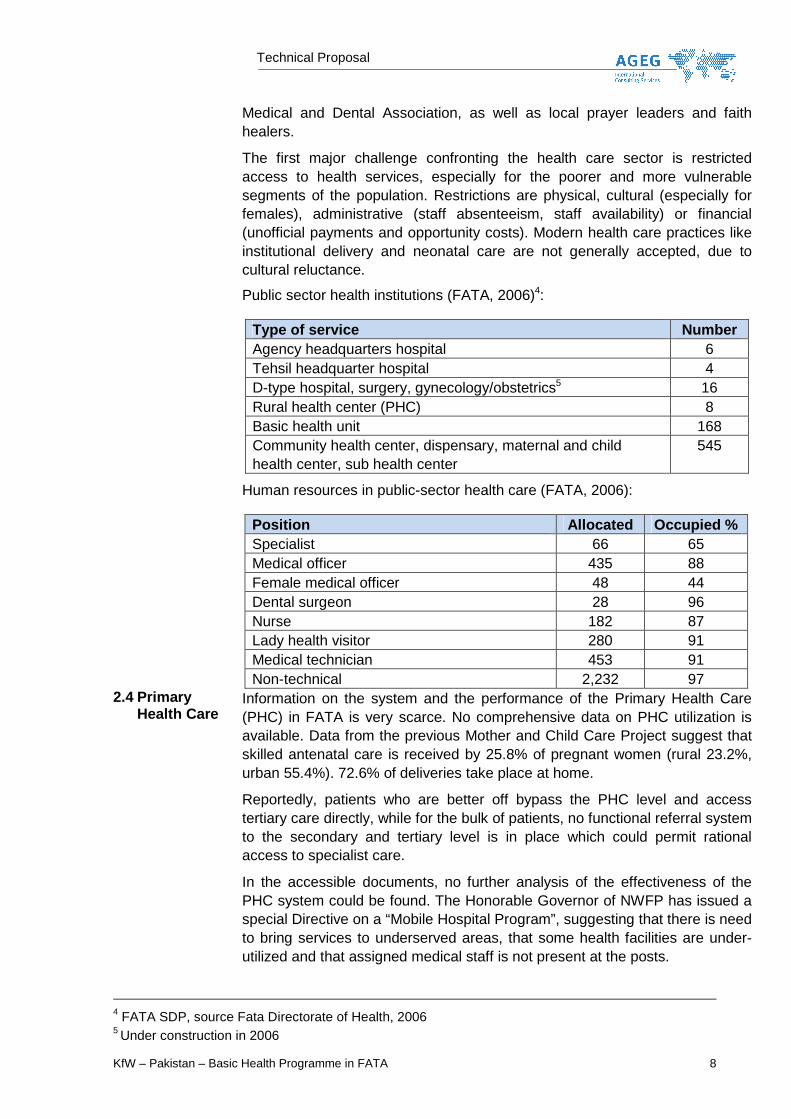
Public sector health institutions (FATA, 2006)4:
Type of service Number Agency headquarters hospital 6 Tehsil headquarter hospital 4 D-type hospital, surgery, gynecology/obstetrics5 16 Rural health center (PHC) 8 Basic health unit 168 Community health center, dispensary, maternal and child health center, sub health center
545
Human resources in public-sector health care (FATA, 2006):
Position Allocated Occupied % Specialist 66 65 Medical officer 435 88 Female medical officer 48 44 Dental surgeon 28 96 Nurse 182 87 Lady health visitor 280 91 Medical technician 453 91 Non-technical 2,232 97
2.4 Primary Health Care
Information on the system and the performance of the Primary Health Care (PHC) in FATA is very scarce. No comprehensive data on PHC utilization is available. Data from the previous Mother and Child Care Project suggest that skilled antenatal care is received by 25.8% of pregnant women (rural 23.2%, urban 55.4%). 72.6% of deliveries take place at home.
Reportedly, patients who are better off bypass the PHC level and access tertiary care directly, while for the bulk of patients, no functional referral system to the secondary and tertiary level is in place which could permit rational access to specialist care.
In the accessible documents, no further analysis of the effectiveness of the PHC system could be found. The Honorable Governor of NWFP has issued a special Directive on a “Mobile Hospital Program”, suggesting that there is need to bring services to underserved areas, that some health facilities are under-utilized and that assigned medical staff is not present at the posts.
4 FATA SDP, source Fata Directorate of Health, 2006 5 Under construction in 2006

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 9
2.5 TB Control in FATA
The TB DOTS programme was started in 2001 in Khyber Agency as pilot project and was implemented in all agencies in 2003. The vision of the FATA TB programme is “TB-free FATA”.
TB Control Programme FATA has an established structure, with a TB Control Programme Manager and his Deputy. At the Agency and FR level, the Programme is supervised by Agency TB Officers. The area has 31 diagnostic centers and 153 treatment centers. The Programme has been supported by the AGEG/GTZ Strengthening Tuberculosis Control Project since 2007.
Although no data on incidence or on prevalence of TB in FATA is available, the following data taken from the AGEG/GTZ Strengthening Tuberculosis Control Project allow to get a picture of the development of TB control in FATA:
FATA
* With effect of 1st quarter 2009, the health services of the Frontier Regions are reporting on
tuberculosis patients. Therefore, the population of the FRs (340,000 people) is included in the denominator for the calculation of the Case Detection Rate (CDR).
** Results of the cohort of 1st quarter 2008 *** For cases detected in 1st quarter of 2009
FATA
* From cases detected in 1st quarter of 2009 ** At the end of 1st quarter 2009
For security reasons, the intra/interagency meetings for 4th quarter 2008 and the 1st quarter 2009 review in FATA scheduled with AGEG/GTZ STCP support were held in Peshawar. All training activities for health staff from FATA have to be conducted in Peshawar for the time being due to the prevailing security situation in FATA. No supervisory visits can be conducted by project staff and even for government employees the movements in FATA are very restricted due to security restrictions. Wherever military operations are launched, access for national staff is either very restricted or impossible.
Nevertheless, the following recent tables with data from FATA give evidence of the possibility to improve TB outcomes (SS = Sputum Smear) even under very difficult conditions.
Indicator 2006 2007 2008 2009 CDR of new pulmonary smear positive case*
36%
37%
38%
51%***
Treatment success rate of new pulmonary smear positive cases
90%
89%
90%**
Indicator 2006 2007 2008 2009 Percentage of new pulmonary smear positive cases out of new pulmonary TB cases registered in a quarter.
45%
41%
49%
51%*
No of reporting diagnostic centres 24 24 29 31**

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 10
CDR All Casess
All Cases, 74%
All Cases, 60%
All Cases, 52%
All Cases, 52%
All Cases, 59%
All Cases, 55%
All Cases, 52%
All Cases, 52%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2002 2003 2004 2005 2006 2007 2008 2nd Q2009
WHO
Target
CDR New SS + %
NSS+, 72%
NSS+, 46%
NSS+, 36%
NSS+, 33%
NSS+, 37%
NSS+, 32%
NSS+, 30%
NSS+, 27%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2002 2003 2004 2005 2006 2007 2008 2nd Q2009
WHO
Target

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 11
Treatment Success Rates
77%
92%94%
85%
100%95%
77%
94%
87%92%93% 93% 94%
97%
90%97%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
110%
2nd Q 2009 93% 93% 94% 97% 90% 97% 77% 0% 0% 0% 92%
2nd Q 2008 94% 85% 100% 95% 77% 94% 87% 0% 0% 0% 92%
Khyber Moh Bajaur Orakzai Kurram NWA SWA FR PeshFR
BannuFR DIK All FATA
Default Rates
7%
0% 0% 0%
3%
2%
0% 0% 0%
11%
3%
8%
0% 0% 0%
3%
0%
7%
2%
3%
0%
2%
-1%
1%
3%
5%
7%
9%
11%
13%
15%
2nd Q 2009 2% 0% 3% 2% 7% 0% 7% 0% 0% 0% 3%
2nd Q 2008 2% 0% 0% 0% 11% 3% 8% 0% 0% 0% 3%
Khyber Moh Bajaur Orakzai Kurram NWA SWA FR PeshFR
BannuFR DIK All FATA
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 12
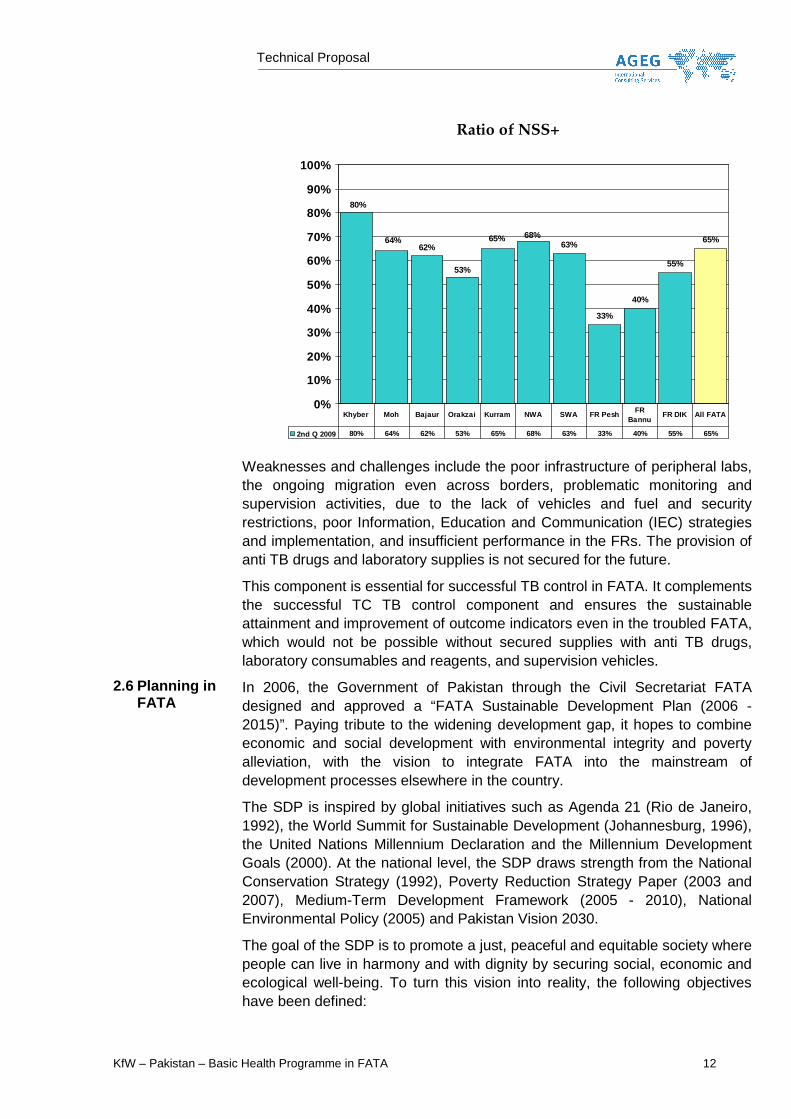
Ratio of NSS+
63%
33%
40%
55%
65%68%65%
53%
62%64%
80%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2nd Q 2009 80% 64% 62% 53% 65% 68% 63% 33% 40% 55% 65%
Khyber Moh Bajaur Orakzai Kurram NWA SWA FR PeshFR
BannuFR DIK All FATA
Weaknesses and challenges include the poor infrastructure of peripheral labs, the ongoing migration even across borders, problematic monitoring and supervision activities, due to the lack of vehicles and fuel and security restrictions, poor Information, Education and Communication (IEC) strategies and implementation, and insufficient performance in the FRs. The provision of anti TB drugs and laboratory supplies is not secured for the future.
This component is essential for successful TB control in FATA. It complements the successful TC TB control component and ensures the sustainable attainment and improvement of outcome indicators even in the troubled FATA, which would not be possible without secured supplies with anti TB drugs, laboratory consumables and reagents, and supervision vehicles.
2.6 Planning in FATA
In 2006, the Government of Pakistan through the Civil Secretariat FATA designed and approved a “FATA Sustainable Development Plan (2006 - 2015)”. Paying tribute to the widening development gap, it hopes to combine economic and social development with environmental integrity and poverty alleviation, with the vision to integrate FATA into the mainstream of development processes elsewhere in the country.
The SDP is inspired by global initiatives such as Agenda 21 (Rio de Janeiro, 1992), the World Summit for Sustainable Development (Johannesburg, 1996), the United Nations Millennium Declaration and the Millennium Development Goals (2000). At the national level, the SDP draws strength from the National Conservation Strategy (1992), Poverty Reduction Strategy Paper (2003 and 2007), Medium-Term Development Framework (2005 - 2010), National Environmental Policy (2005) and Pakistan Vision 2030.
The goal of the SDP is to promote a just, peaceful and equitable society where people can live in harmony and with dignity by securing social, economic and ecological well-being. To turn this vision into reality, the following objectives have been defined:

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 13
• Address basic social needs underlying causes of prevailing disparities within FATA
• Improve institutional and financial capacities to allow a scaling-up of development initiatives being already undertaken
• Explore and diversify available opportunities to make a positive contribution towards the economic uplift of the area
• Manage and maintain ecological and subsistence-support systems to increase livelihood security for ordinary people
• Monitor and evaluate multi-sectoral progress to support, assess and strengthen sustainable development.
The SDP is implemented through Annual Development Programmes. Due to scarce financial resources and increased development costs, most projects lag far behind in schedule and scope. Ongoing and aggravating conflicts are severely hindering all development plans and activities. Travel, productivity, trade and public services are greatly impaired and prices for food, housing, energy and services have multiplied.
2.7 Health Plan-ning
Health planning still focuses on infrastructure and curative services. Many medical students trained elsewhere in Pakistan do not return to FATA for work. The human resource crisis is aggravated by the fact that FATA does not have its own health workforce. All public employees are part of the health cadres of the NWFP (2007). Health facilities and human resources in health tend to concentrate in the area near Peshawar, while the regions further away are depleted. Transferring staff from the settled areas has not proved helpful as they are rarely accepted by the population.
The SDP has a focus on equitable access to health care and guarantee for quality services. All segments of the health sector will be strengthened, including the Health Directorate. Community empowerment and intense IEC plays a key role. Cooperation with the private sector and with the non-government sector is high on the agenda.
The targets of the SDP in Health are:
Sector indicator Baseline
2006 Target 2011
Target 2015
Infant mortality (deaths per 1,000 live births)
87 83 77
Maternal mortality (deaths per 100,000 live births)
600 500 400
Water supply and sanitation NA NA NA Access to improved sources of drinking water (per cent)
54 65 75
Access to improved sanitation (per cent)
10 17 25
2.8 „Critical Ap-praisal” of the ToR and
The Consultant acknowledges that the ToR consider the limitations regarding planning, implementing and monitoring/evaluating health care programmes in the FATA under the present security situation, where access to the FATA
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 14
the meth-odological concept
region is not possible for any non-tribal persons, let alone foreigners. Even access to the capital of NWFP, Peshawar, is largely restricted or impossible. Programme operational planning, monitoring, assessment of results and achieved milestones, and technical and financial steering will need to be handled very flexibly from all partners involved. As clearly stated in the pre-feasibility study, most likely some weaknesses in project management (supervision!) will have to be accepted and modifications will be necessary during the course of the project time.
During the inception phase of the project, the proposed logframe will have to be revised (if the security situation will permit) which will make it redundant commenting on the present inconsistency in the definition of program objectives between the logframe in the Feasibility Study (referred to in the ToR), the Minutes of Meeting (attached to the Feasibility Study) and the objectives defined in the ToR themselves.
The proposed Programme comprises five components:
1. TB Control Programme 2. Mobile Health Care Squads 3. Mother and Child Health Care 4. Emergency Care 5. Disposition Fund for minor infrastructure and equipment measures
The organisational setup, too, has to pay tribute to the security situation in NWFP and in FATA: The components 3 and 4 will be managed completely by national NGOs, component 2 will be managed by the FATA secretariat (supported by the consultant). The Consultant will have quite limited control over the effectiveness and quality of the implementation of these components. The TB control component (1.) will be managed with the same opportunities and threats as presently the FATA TB component of the TC programme. Component 5 will start off as an open programme for which the mode of coordination with GTZ interventions will have to be determined.
For components 3 and 4, Greenstar and Community Appraisal & Motivation Programme (CAMP) have submitted some preliminary documentation. The Consultant assumes that these two NGOs will still be ready for cooperation on the basis of these documents, although these notes are supposedly not binding and the NGOs are not signatories of the Minutes of Meeting attached to the Feasibility Study. The consultant has not received any intervention plan for component 2 from the FATA Secretariat.
As the FATA Secretariat has not submitted a feasibility paper for the “Mobile Health Care Squads” (component 2), there is great need to clarify this component during the inception phase. The indications from the preceding PC1 (2003 - 2007) as well as the report from a meeting and presentation on October 17, 2008 to the Governor of NWFP, do not contain any sound problem analysis or baseline information on the PHC system nor any rationale why the chosen approach with big investments in vehicles would be effective or even feasible.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 15
3 Proposal for the Implementation
3.1 Methodological Approach
The programme methodology has to comply with the given situation in FATA as regards security, mobility, migration, inaccessibility, interference of influences outside the medical framework, scarce human resources, limited planning and implementation capacity, etc. This situation requires a very flexible approach which will have to be reflected in the inception report documents and its time schedules and definition of milestones.
On the other hand, the Consultant has already positive experience in cooperation with the FATA authorities through the TB control component of the GTZ supported project.
The consultant will seek very close cooperation with the FATA Secretariat and with the Department of Health, which will have the overall coordination of the programme through a Project Implementing Unit (PIU) to be nominated by the Project Exectuing Agency (PEA) and supported by the consultant.
Further, programme effectiveness will certainly be strengthened through the contracting of two locally well established NGOs for component 3 and 4. Here, the consultant will follow up on planning, monitoring and reporting only, since the NGOs will carry out their components on their own.
The consultant will make best use of the available synergies arising from its other activities in health in NWFP and in FATA. In particular, the already existing personal relations with representatives of the FATA Department of Health will be used to accelerate the warming up phase during project inception. Project staff will work closely with the project staff of the KfW supported TB control programme in NWFP and share office with them. This will, to some extent, allow to rationalize in equipment and to cooperate in procedures common to both projects. This should permit to implement especially procurement activities with fewer problems as some pitfalls are now already known and can be avoided.
In addition, synergies will be sought also with the GTZ supported NWFP TB control programme and with the new GTZ activities in FATA. They will mainly consist in harmonization of capacity building and training activities for FATA staff in aligning with relevant needs identified in the present FC programme. On the operational level, the programme will greatly benefit from the establishment of the TB reference laboratory in Peshawar.
3.2 TB Control Programme (Component 1)
The TB control Programme will be similar to the one in NWFP and include supply and distribution of drugs, activity and result monitoring, procurement of vehicles, consumables and reagents, and support to IEC activities. During the inception phase, the consultant will analyze the existing system and assess options for cooperation with other actors engaged in TB control like the “Marie Adelaide Leprosy Center” NGO (MALC).
In order to facilitate the import of goods, the consultant will start early
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 16
preparing the necessary steps with government institutions including the Economic Affairs Division (EAD) to obtain tax exemption. Drug needs for an estimated 6.000 patients per year will be calculated and drug orders placed using the same methods as in the NWFP programme. At present, drug procurement through the Global Drug Facility (GDF) appears to be the most feasible and economical mode in order to ensure the supply with quality drugs. A special permit to import these drugs even if produced in India may be required.
Some part of the disposition fund (component 5) may be used for minor repair and equipment supply for peripheral labs and for drug storage facilities if needed. The component will benefit from the quality assurance system for TB smears already in place in NWFP with support from the AGEG/GTZ TB Control Programme and the national NGO Association for Community Development.
The TB component will be planned and implemented in close cooperation and coordination with the ongoing NWFP programmes (KfW and GTZ). Ongoing and planned support by other donors like GFATM will be assessed and considered. Cooperation and coordination with the National TB Control Programme (NTP) and with WHO in Pakistan will be fostered. Further precision for planning will be carried out during the inception phase, once GTZ has decided more in detail on the components and activities of the new FATA Health Programme which will also contain a TB control component. Further, drug procurement will have to take into consideration any new treatment standards and drug combinations which may be recommended by WHO. It will be carried out by the national project manager in cooperation with the procurement officer of the NWFP TB Control project, with support from the management of both projects.
3.3 Mobile Health Care Squads (Component 2)
This component is the continuation and extension of an activity which has already been carried out by the FATA Secretariat since 2004. For this component, the ToR mention the provision of specialized vehicles, equipment for diagnostic (including x-ray), dental, surgical and obstetric care and support units. The consultant will assist the Directorate of Health of the FATA Secretariat (DHS) FATA in updating the situational analysis regarding the provision of PHC services as well as of specialized care and existing mobile health care services in the FATA and in carrying out a rational needs assessment. This will serve to optimize the pre-existing planning for the set-up of new Mobile Health Care Squads as well as to establish a plausible plan for the organisation and the management of the system.
The consultant will have in mind the different roles of the mobile services which include (i) bringing basic care to remote areas, (ii) providing some specialized services to isolated parts of the population, (iii) strengthening services and quality of services in Basic Health Units and Health Centers, and (iv) supporting emergency care where needed. Life saving activities will receive special attention.
This component will be managed by the FATA Secretariat, assisted by the consultant. The input of the consultant will focus on the preparation of
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 17
a work plan and on the procurement of vehicles and equipment and the preparation of relevant specifications. As this component will be quite complex to implement, the international team leader and the national programme manager will spend a considerable share of their time and energy in the assistance to the DHS for this component. Specific input for the technical specifications and the preparation of tender documents, as well as for bid evaluation will be provided by the International Equipment and Procurement Specialist.
Special attention will be given to the operational costs and the proper operation of the component, including human resources problems and staff funding. During the inception phase, the consultant will support the FATA Secretariat in drafting an operational plan and a maintenance concept on which the procurement of the mobile health units will depend.
3.4 Mother and Child Health Care (Compo-nent 3)
Culturally, demand for mother and child care is low but seems to pick up. This component will be implemented by Greenstar on its own. Greenstar activities will include training of providers in mother and child health programmes, upgrading of provider outlets, orientation of traditional birth attendants, the provision of delivery kits, as well as toll-free mother and child health phone hotline advisory services and IEC measures. This component will complement the family planning activities already underway by Greenstar, and are expected to contribute significantly to the attainment of MDC goals.
The Consultant will ensure coordination within the programme components, receive 3-monthly reports and annex them to the general reports. Greenstar has submitted a Pre-concept Note in August 2008, which covers 2 Agencies and 3 FR and will serve as starting point for further planning.
3.5 Emergency Care (Compo-nent 4)
The NGO “Community Appraisal & Motivation Programme” (CAMP) will plan and implement this component on its own. It has submitted a corporate capability statement, but no concept note. In this component, the improvement of emergency care for selected Rural Health Centers, Tehsil Head Quarter Hospitals and Agency Head Quarter Hospitals is targeted. CAMP is already implementing emergency programmes at lower levels including respective training.
During the inception phase, the consultant will ask CAMP to submit a proposal. The Consultant will ensure coordination within the programme components, receive 3-monthly reports and annex them to the general reports.
The needs assessment, the preparation of equipment lists, technical specifications and tender documents will be guided by the International Equipment and Procurement Specialist.
3.6 Disposition Fund
This component will mainly support the activities of GTZ in FATA especially to improve quality management activities in selected health facilities. The fund will be managed by the consultant. The use of funds will be coordinated with GTZ as an ongoing process. Standard operational procedures and formats will be developed for needs assessment, the application for funds, the acceptance of works and
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 18
payments made.
3.7 Work Plan 1. Inception Phase (3-4 months):
After contract signature, the team leader will travel to Islamabad and meet with stakeholders from the FATA Secretariat and the FATA DoH, as well as with NWFP health authorities related to the programme, in particular TB control. Further, first meetings will be held with the KfW and GTZ country staff and with AGEG consultants of other projects in NWFP and FATA. Contact will be established with related NGOs (Greenstar and CAMP, MALC).
The Programme structure will be discussed with the FATA Secretariat regarding the establishment of a PIU in Peshawar. The team leader with support from the KfW TB Control Project will start the search for the local project staff and find agreements with the KfW and GTZ TB projects on sharing office room, equipment and to some extent staff and functions in Peshawar and in Islamabad. The consultant assumes that office rent will be paid by the KfW TB control project.
For local transport, the consultant assumes that one of the vehicles to be procured will be free for use by the consultant. Until this vehicle arrives, the consultant will rent a car at the expense of the disposition fund.
Further activities during the inception phase will include:
• Elaboration of cooperation procedures with the PIU
• Elaboration of concepts and operational plans for each of the components, with time schedules, activities, results, and mile stones, monitoring plan and tools, cost estimates with financing schedule
• Harmonization of procedures and activities with the KfW TB control Project
• Analysis of drug needs and preparation of first lot order at GDF
• Analysis of needs in laboratory supply and preparation of first order if applicable
• Needs assessment for the Mobile Health Care Squads
• Elaboration of an operations and maintenance plan for the Mobile Health Care Squads
• Revision of the logframe, if the security situation allows
2. Implementation Phase
The consultant will ensure the overall Programme coordination and fulfill the requested reporting requirement. Reports will be routed through the DHS FATA. Project funds will be managed according to KfW Guidelines. In as far as data is available, the consultant will follow up on the programme related health situation and monitor the attainment of project mile stones and goals.
The time schedules for each component established during the inception

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 19
phase will be followed during the implementation phase. The main focus for the consultant will be on the support to the FATA Secretariat in the procurement of equipment and vehicles, drugs, laboratory consumables and reagents, and IEC material. This will include preparation of tender documents with lists of equipment and bills of quantities, tendering, bid evaluation, awards of contracts, in close cooperation with DHS FATA. Procurement will be done in line with KfW guidelines and regulations stipulated in the ToR and in the Separate Agreement. The support to the FATA Secretariat for the implementation of component 2 will be an ongoing activity and focus on management issues, once initial procurement is done. Other advisory activities will secure the effectiveness and efficiency of the investment measures.
Where relevant and to the extent possible given the security situation, pre-installation works will be coordinated and the accomplishment will be documented through issuance of a certificate. The consultant will apply the relevant procedure also for the supervision of installation and the acceptance of equipment. The assumption is that national project staff will be free and safe to travel to the concerned places.
Further details of the implementation phase will be documented in the inception report.
3.8 Work Plan and Staffing Sched-ule

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 20

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 21
4. Project Management
4.1 Introduction
The Programme implementation is the responsibility of the following Pro-gramme-Executing Agencies: 1. FATA Secretariat (Component 1 and 2) 2. Greenstar/SMP Ltd. (Component 3) 3. CAMP (Component 4) The DHS FATA, through a new PIU, has the responsibility for the overall coordination between the public and the private sector components and for the implementation of the component 2 (Mobile Health Care).
The consultant assists the DHS in the overall coordination and manage-ment of the programme, gives particular input for components 1 and 2, monitors components 3 and 4, and manages the disposition fund.
4.2 Project Organi-sation and backup
The project organisation is oriented towards the best setting for close co-operation with the PEA and the PIU.
In order to benefit from maximum synergies, the project team will share office with the KfW NWFP TB control team in Peshawar and in Islama-bad. This will allow for easy exchange of experience as well as for mutual support in project activities, such as tendering and procurement, and will keep the costs down.
In the given situation, project management structures need to be flexible and respect security considerations of project and stakeholder personnel. The national project team works in Peshawar, the international team will work from Islamabad and from abroad. During the intermittent visits of the team leader to Islamabad every quarter, he will meet with the project team and the FATA programme partners and monitor project progress, adjust the planning, carry out and/or supervise specific project tasks, and liaise with national and international partners. While working from home, he will be in constant telephone, web-based phone and video connec-tions and Email contact with the team and supervise, guide and support everyday activities. The team leader will be responsible for project result monitoring and reporting.
The team leader will have technical backup support from the project co-ordinator and administrative support from the AGEG headoffice.
The national Programme Manager will be responsible for day-to-day im-plementation of all tasks of the consultant as described in the ToR. He will be supported by the team leader, the project coordinator, the AGEG headoffice, a national Financial and Administrative Officer and the Logis-tics Assistant, who will also be the driver. He will cooperate very closely with the consultant staff of the KfW TB project. His counterparts will be the authorities delegated into the PIU in particular for the implementation of components 1 and 2. He will liaise with Greenstar and CAMP for the purpose of monitoring and reporting, but will provide technical support to CAMP for procurement.
Expertise for Health Center equipment, Hospital equipment, for Mobile

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 22
Health Squads equipment and procurement will be provided by the Inter-national Equipment and Procurement Specialist who will be supported by the local project team and the Team Leader. Procurement for vehicles, drugs and other medical and non-medical supplies for the TB Control Component will be carried out by the project manager in cooperation with the procurement officer of the NWFP TB Control Programme, with sup-port from the management of both projects.
4.3 Results-based
M&E During the inception phase, the consultant will revise the logframe and submit it to the PEA and KfW for approval. Then, suitable tools and pro-cedures will be put in place to allow for constant monitoring of project progress against the planning. It is expected that repeated target adapta-tions may be necessary which will then be communicated to the DHS and to KfW.
4.4 Reporting
After 4 months, the consultant will submit the inception report in the for-mat indicated in the ToR. Then, every 6 months, he will submit a com-prehensive progress report to the DHS and to KfW following the require-ments given in the ToR. Reports from the 2 NGOs will be attached with a brief summary included in the report. Short progress summaries will be submitted quarterly in between.
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 23
5 Presentation of the Team
5.1 Introduction: team composi-tion
The team size has been kept to a minimum because the consultant can draw on staff resources from the KfW TB project to a certain extent in as far as identical tasks are to be fulfilled. The Procurement Expert in the AGEG/KfW TB programme will also take over the supervision of all pro-curement to be undertaken in this programme. The international team leader has very large project management experience himself and will benefit from AGEG experiences in the other health projects in Pakistan and in AJK.
The national team will be recruited during the inception phase. Former recruitment experience in NWFP including the FATA based AGEG/GTZ TB advisor will facilitate the task.
5.2 The project team
Position Person months (pm)
International expert intermittent 14,8 pm (total)
01. Team Leader, Dr. Matthias REINICKE 12 pm
02. Project Coordinator, Dr. Reinhard KOPPENLEITNER
1,8 pm
03. Equipment and Procurement Expert, Dieter NASSLER
1,0 pm
National long term experts/staff 105 pm (total)
03. Programme Manager; NN 35 pm
04. Finance and Administration Officer, NN 35 pm
05. Driver/Logistic Assistant, NN 35 pm
5.3 Profile of the experts
Dr. Matthias REINICKE: Team Leader Dr. Reinicke is a medical doctor with specialization in General Medicine and in Public Health. He has profound project management experience in many countries, recently mainly in the Balkan countries, where he was Health Sector Programme manager and Head of Operations for the Eu-ropean Union (EAR). His experience covers all aspects of public health projects including emergency medicine and procurement of drugs and equipment. He has been involved in several TB control projects and in many Primary Health Care programmes.
As this project covers several aspects of health care, the profile of Dr. Reinicke fits the task perfectly. He will quickly adapt to the particular challenges in Pakistan and in FATA and familiarize himself with the KfW guidelines, supported by the experienced KfW/AGEG TB control team in Peshawar and the project coordinator.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 24
Dr. Reinhard KOPPENLEITNER: Project Coordinator, Ba ckstopping Dr. Koppenleitner is in charge of the Health Department at AGEG. He holds academic degrees in Paediatrics and Public Health. He has gained project management experience with several long term projects in coun-tries like Kyrgyzstan, Pakistan and Haiti and is familiar with KfW pro-curement procedures. In Pakistan, he is also the Project Coordinator of the GTZ and the KfW TB control projects NWFP as well as the KfW AJK Health Infrastructure Project. He is familiar with relevant government au-thorities, with most stakeholders and with relevant programmes of the government and of other donors.
Dr. Koppenleitner will be in charge of the overall coordination and back-stopping of the project. He will ensure the close cooperation between the TC and the FC projects and therefore realize synergy effects. He will be the direct link with relevant experts at KfW and GTZ and guarantee the quality of project reporting. Dieter NASSLER: Equipment and Procurement Specialis t: Director of Mediconsult Planning & Consulting Services Sdn. Bhd. (Medi-consult) holds an MBA from Germany. Prior to setting-up Mediconsult he was the Managing Director of Vamed Engineering Sdn. Bhd., directly in-volved in the establishment of the Institute Jantung Negara (National Cancer Institute, Malaysia). Overall, Mr. Nassler has more than 30 years of experience in healthcare consulting and hospital management both at national and international level. His areas of expertise encompass all fields of healthcare consultancy, including logistic and procurement, maintenance planning, health economics, health system, feasibility stud-ies, market analysis, project management and assessment of healthcare needs of both governmental and non-governmental organisations. He was involved in Project Preparation Study for Post-Earthquake Hospitals Reconstruction in AJK, Pakistan funded by KfW Entwicklungsbank and was involved in Post-tsunami Rehabilitation and Reconstruction of Dr Za-inoel Abidin Hospital, Banda Aceh, Indonesia funded by KfW Entwick-lungsbank & AUSAID amongst others. Further projects which he coordi-nates at present are implemented in China, Malaysia, Thailand, India, Pakistan, Nepal as well as in various African and Middle Eastern coun-tries.
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 25
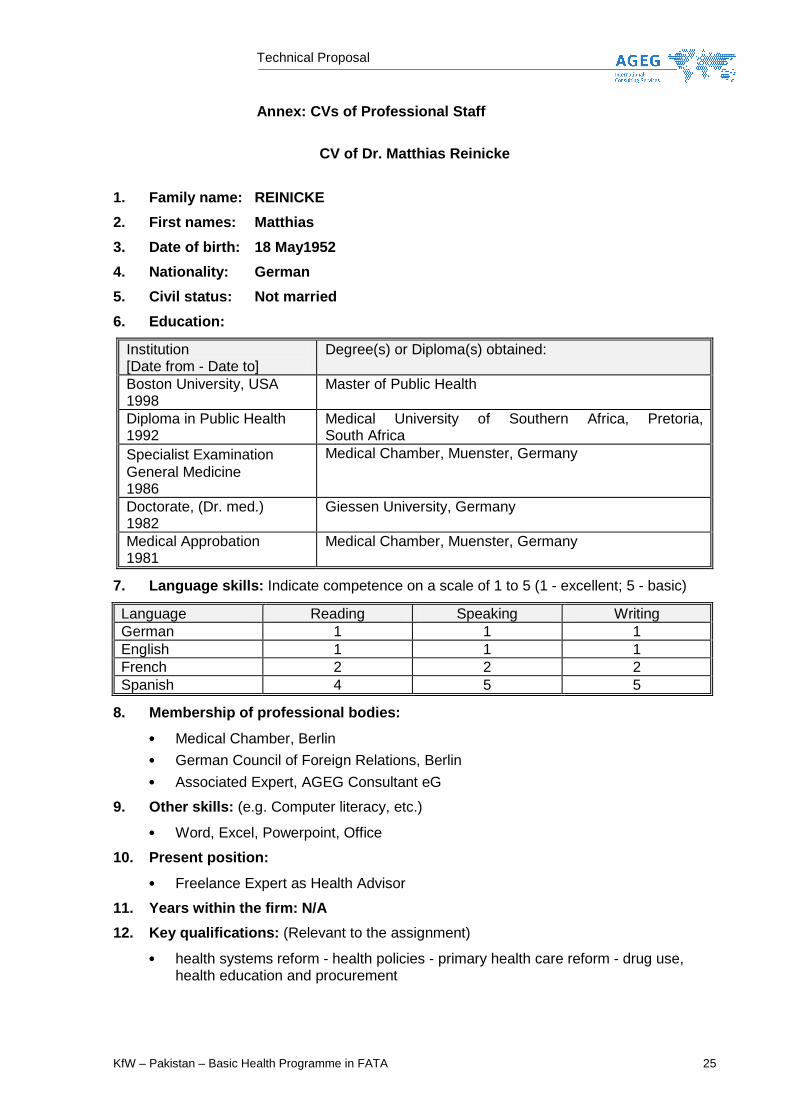
Annex: CVs of Professional Staff
CV of Dr. Matthias Reinicke
1. Family name: REINICKE
2. First names: Matthias
3. Date of birth: 18 May1952
4. Nationality: German
5. Civil status: Not married
6. Education:
Institution [Date from - Date to]
Degree(s) or Diploma(s) obtained:
Boston University, USA 1998
Master of Public Health
Diploma in Public Health 1992
Medical University of Southern Africa, Pretoria, South Africa
Specialist Examination General Medicine 1986
Medical Chamber, Muenster, Germany
Doctorate, (Dr. med.) 1982
Giessen University, Germany
Medical Approbation 1981
Medical Chamber, Muenster, Germany
7. Language skills: Indicate competence on a scale of 1 to 5 (1 - excellent; 5 - basic)
Language Reading Speaking Writing German 1 1 1 English 1 1 1 French 2 2 2 Spanish 4 5 5
8. Membership of professional bodies:
•••• Medical Chamber, Berlin
•••• German Council of Foreign Relations, Berlin
•••• Associated Expert, AGEG Consultant eG
9. Other skills: (e.g. Computer literacy, etc.)
•••• Word, Excel, Powerpoint, Office
10. Present position:
•••• Freelance Expert as Health Advisor
11. Years within the firm: N/A
12. Key qualifications: (Relevant to the assignment)
•••• health systems reform - health policies - primary health care reform - drug use, health education and procurement

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 26
13. Specific experience in the region:
Country Date from - Date to Serbia 2005 - 2008 Kosovo 2000 - 2005 Uganda 1995 - 1997
D. R. Congo November – January 1996/1997 Thailand August – September 1995 Botswana 1989 - 1995
South Africa 1983 - 1985
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 27
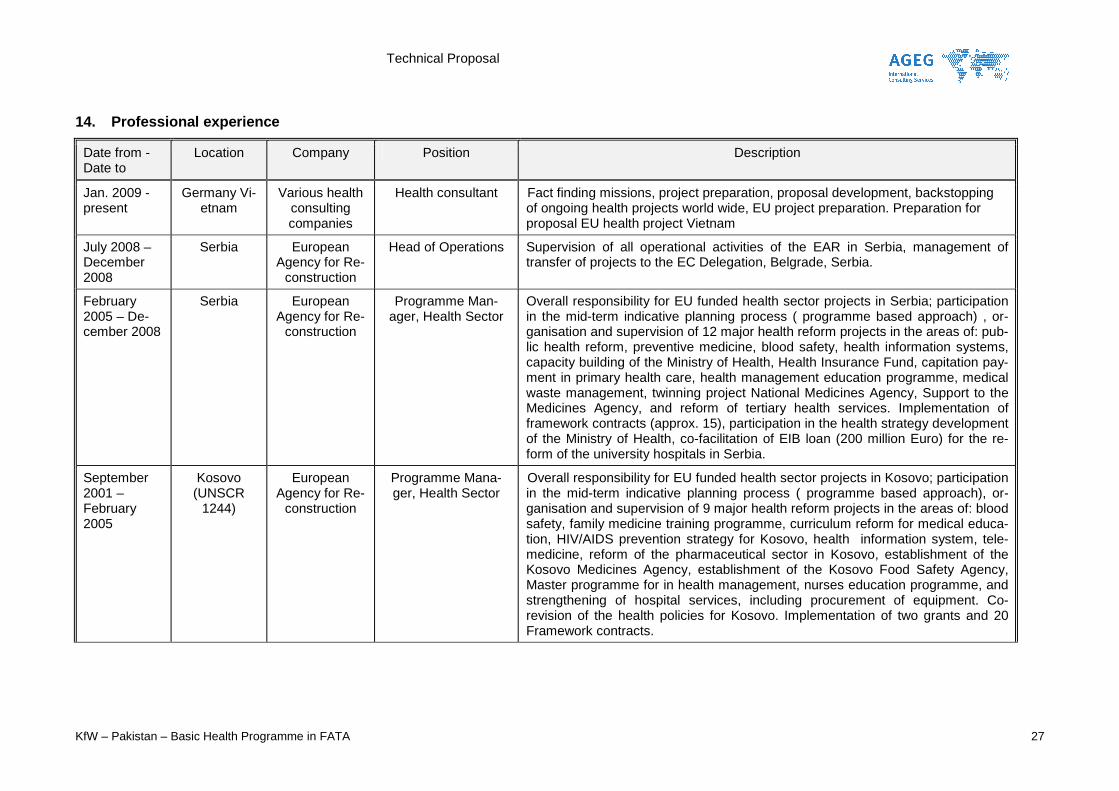
14. Professional experience
Date from - Date to
Location Company Position Description
Jan. 2009 - present
Germany Vi-etnam
Various health consulting companies
Health consultant Fact finding missions, project preparation, proposal development, backstopping of ongoing health projects world wide, EU project preparation. Preparation for proposal EU health project Vietnam
July 2008 – December 2008
Serbia European Agency for Re-
construction
Head of Operations Supervision of all operational activities of the EAR in Serbia, management of transfer of projects to the EC Delegation, Belgrade, Serbia.
February 2005 – De-cember 2008
Serbia European Agency for Re-
construction
Programme Man-ager, Health Sector
Overall responsibility for EU funded health sector projects in Serbia; participation in the mid-term indicative planning process ( programme based approach) , or-ganisation and supervision of 12 major health reform projects in the areas of: pub-lic health reform, preventive medicine, blood safety, health information systems, capacity building of the Ministry of Health, Health Insurance Fund, capitation pay-ment in primary health care, health management education programme, medical waste management, twinning project National Medicines Agency, Support to the Medicines Agency, and reform of tertiary health services. Implementation of framework contracts (approx. 15), participation in the health strategy development of the Ministry of Health, co-facilitation of EIB loan (200 million Euro) for the re-form of the university hospitals in Serbia.
September 2001 – February 2005
Kosovo (UNSCR
1244)
European Agency for Re-
construction
Programme Mana-ger, Health Sector
Overall responsibility for EU funded health sector projects in Kosovo; participation in the mid-term indicative planning process ( programme based approach), or-ganisation and supervision of 9 major health reform projects in the areas of: blood safety, family medicine training programme, curriculum reform for medical educa-tion, HIV/AIDS prevention strategy for Kosovo, health information system, tele-medicine, reform of the pharmaceutical sector in Kosovo, establishment of the Kosovo Medicines Agency, establishment of the Kosovo Food Safety Agency, Master programme for in health management, nurses education programme, and strengthening of hospital services, including procurement of equipment. Co-revision of the health policies for Kosovo. Implementation of two grants and 20 Framework contracts.
Technical Proposal
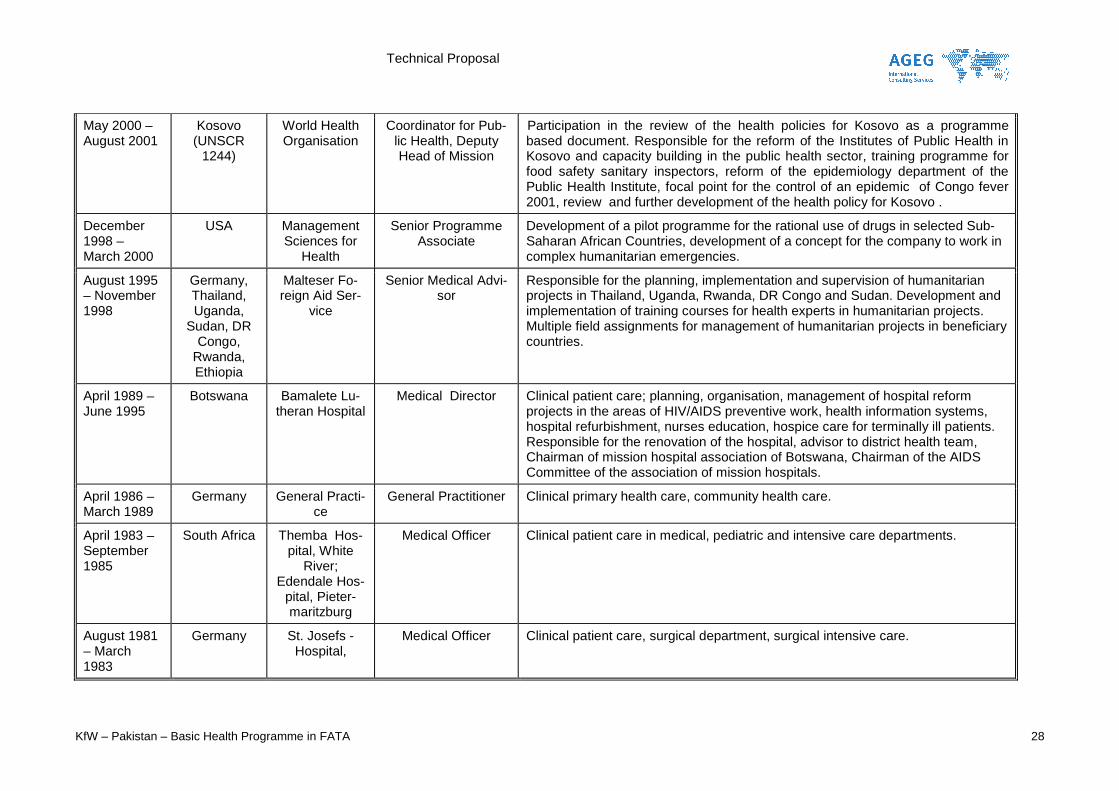
KfW – Pakistan – Basic Health Programme in FATA 28
May 2000 – August 2001
Kosovo (UNSCR
1244)
World Health Organisation
Coordinator for Pub-lic Health, Deputy Head of Mission
Participation in the review of the health policies for Kosovo as a programme based document. Responsible for the reform of the Institutes of Public Health in Kosovo and capacity building in the public health sector, training programme for food safety sanitary inspectors, reform of the epidemiology department of the Public Health Institute, focal point for the control of an epidemic of Congo fever 2001, review and further development of the health policy for Kosovo .
December 1998 – March 2000
USA Management Sciences for
Health
Senior Programme Associate
Development of a pilot programme for the rational use of drugs in selected Sub-Saharan African Countries, development of a concept for the company to work in complex humanitarian emergencies.
August 1995 – November 1998
Germany, Thailand, Uganda,
Sudan, DR Congo,
Rwanda, Ethiopia
Malteser Fo-reign Aid Ser-
vice
Senior Medical Advi-sor
Responsible for the planning, implementation and supervision of humanitarian projects in Thailand, Uganda, Rwanda, DR Congo and Sudan. Development and implementation of training courses for health experts in humanitarian projects. Multiple field assignments for management of humanitarian projects in beneficiary countries.
April 1989 – June 1995
Botswana Bamalete Lu-theran Hospital
Medical Director Clinical patient care; planning, organisation, management of hospital reform projects in the areas of HIV/AIDS preventive work, health information systems, hospital refurbishment, nurses education, hospice care for terminally ill patients. Responsible for the renovation of the hospital, advisor to district health team, Chairman of mission hospital association of Botswana, Chairman of the AIDS Committee of the association of mission hospitals.
April 1986 – March 1989
Germany General Practi-ce
General Practitioner Clinical primary health care, community health care.
April 1983 – September 1985
South Africa Themba Hos-pital, White
River; Edendale Hos-
pital, Pieter-maritzburg
Medical Officer Clinical patient care in medical, pediatric and intensive care departments.
August 1981 – March 1983
Germany St. Josefs - Hospital,
Medical Officer Clinical patient care, surgical department, surgical intensive care.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 29
CV of Dr. Reinhard Koppenleitner 1. Family name: KOPPENLEITNER
2. First names: Reinhard
3. Date of birth: 01.01.1946
4. Nationality: German
5. Civil status: Not married
6. Education:
Institution [Date from - Date to]
Degree(s) or Diploma(s) obtained:
TULANE UNIVERSITY, School of Public Health and Tropical Medicine 08.1996-07.1997
Master of Public Health - specialization: International Health, Program Evaluation, Program Management
Children Hospital Munich 05.1978-08.1982
Board Certified Pediatrician - specialization: Pediatrics
Universities of Munich, Zu-rich and Tuebingen 09.1965-07.1973
Medical Doctor
7. Language skills: Indicate competence on a scale of 1 to 5 (1 - excellent; 5 - basic)
Language Reading Speaking Writing German 1 1 1 English 1 1 1 French 1 2 2 Spanish 2 4 4 Portuguese 3 5 5 Haitian Creole 2 2 3
8. Membership of professional bodies:
•••• Member of the German Society of Tropical Medicine and International Health
•••• Member of the German Society of Pediatrics
•••• Member of the German Association for Tropical Pediatrics
9. Other skills: (e.g. Computer literacy, etc.)
Courses and Training on the following issues:
•••• Health Economics and Public Financing, Pilot Course (GTZ, 2007)
•••• AURA Impact Oriented Proposals (GTZ, 2003)
•••• Project Cycle Management (EU, 2001)
•••• Quality Management for Health (Bavarian Medical Board 2001)
•••• Quality Management for Health (GTZ 2000)
•••• Infectious Disease Epidemiology (School of Public Health Bielefeld, 2000)
•••• Project Cycle Management (GTZ 2000)
•••• Tropical Medicine (Heidelberg 1974, Munich 1994 1995)
•••• Surgery in the Tropics (1994)
•••• Obstetrics (Munich 1974)

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 30
•••• Disaster Relief (Bonn Red Cross 1995)
•••• HIV/AIDS (Munich 1998)
•••• Psychotherapy (Munich 1981 - 1987)
•••• Computer skills: MS Office, Statistic packages, Internet
10. Present position:
•••• Member of Directorate of AGEG Consultants eG
•••• Head of Health Department at AGEG since 1999
•••• Public Health Consultant – since 1982
•••• Pediatrician - since 1981
11. Years within the firm: 11
12. Key qualifications: (Relevant to the assignment)
Health Planning and Evaluation - PCM – Hospital Planning - Hospital Management - Quality Management - Tropical Medicine - Family Planning/Reproductive Health - HIV/AIDS/STD Management - Primary Health Care Systems - District Health Care - Environmental Health - Health Care Financing
13. Specific experience in the region:
Country Date from - Date to Cambodia 8/2009 - 4/2010 Pakistan 2003 - 2009
Kyrgyzstan 2001 - 2009 Rwanda 2004 - 2006 Lao PDR 11/2005 - 9/2006
Cameroon 3/2005 - 4/2005 + 4/2008 Kenya 9/2002 - 10/2002, + 6/2009
Madagascar 2001 - 2003 + 12/2007 Ethiopia 8/1999 - 9/1999
Botswana 3/1999 - 4/1999 Palestine Terr. 2/1998 - 12/1998
Nigeria 10/1998 - 11/1998 Azerbaijan 4/1998
Uganda 7/1997 - 9/1997 Guinea 1/1996 - 6/1996
Haiti 1975 - 2007
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 31
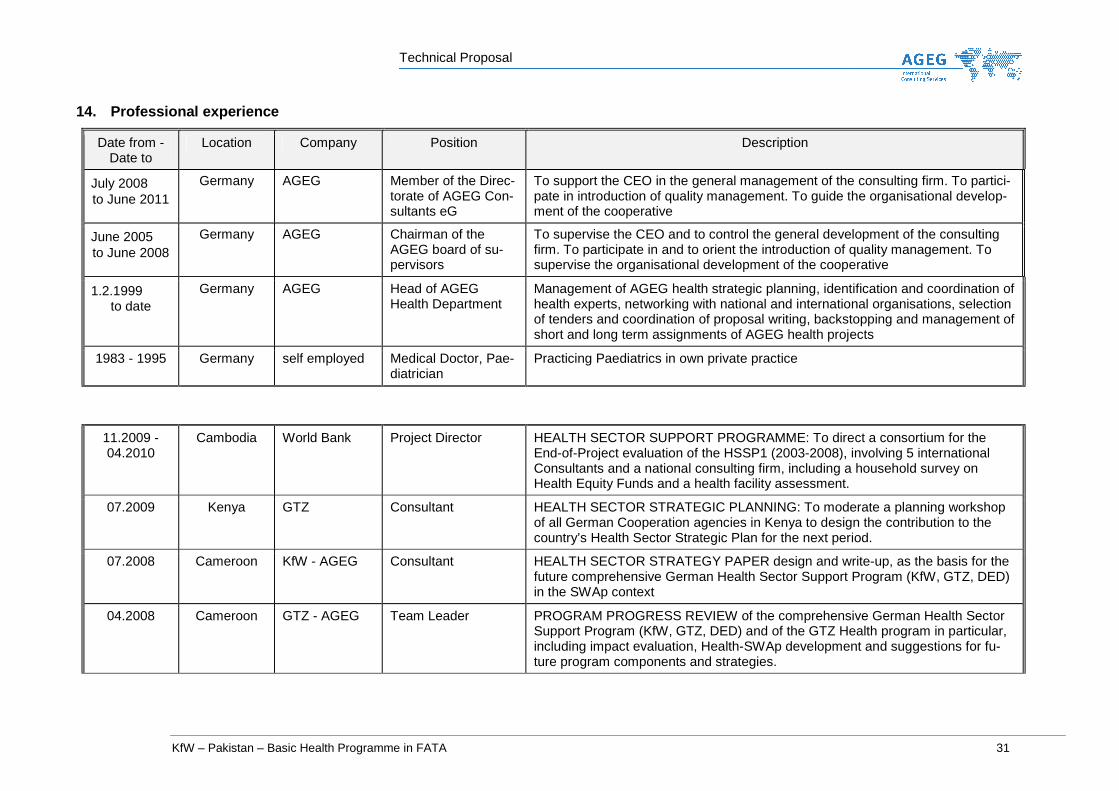
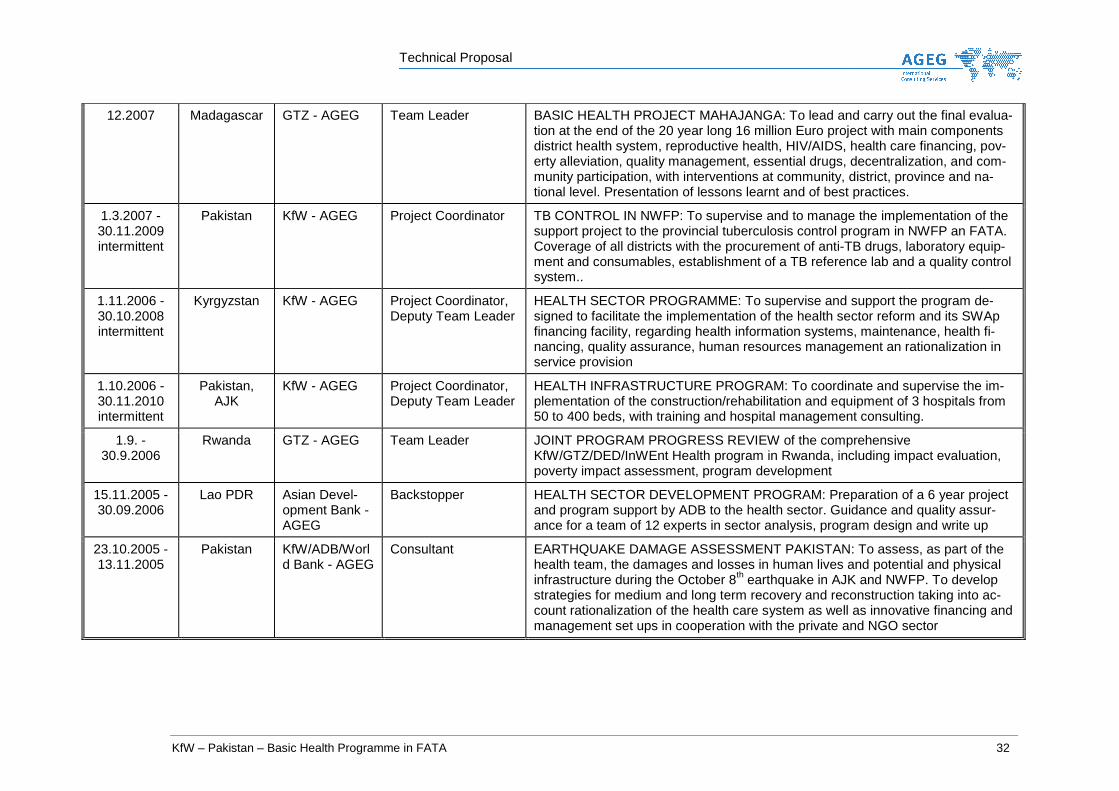
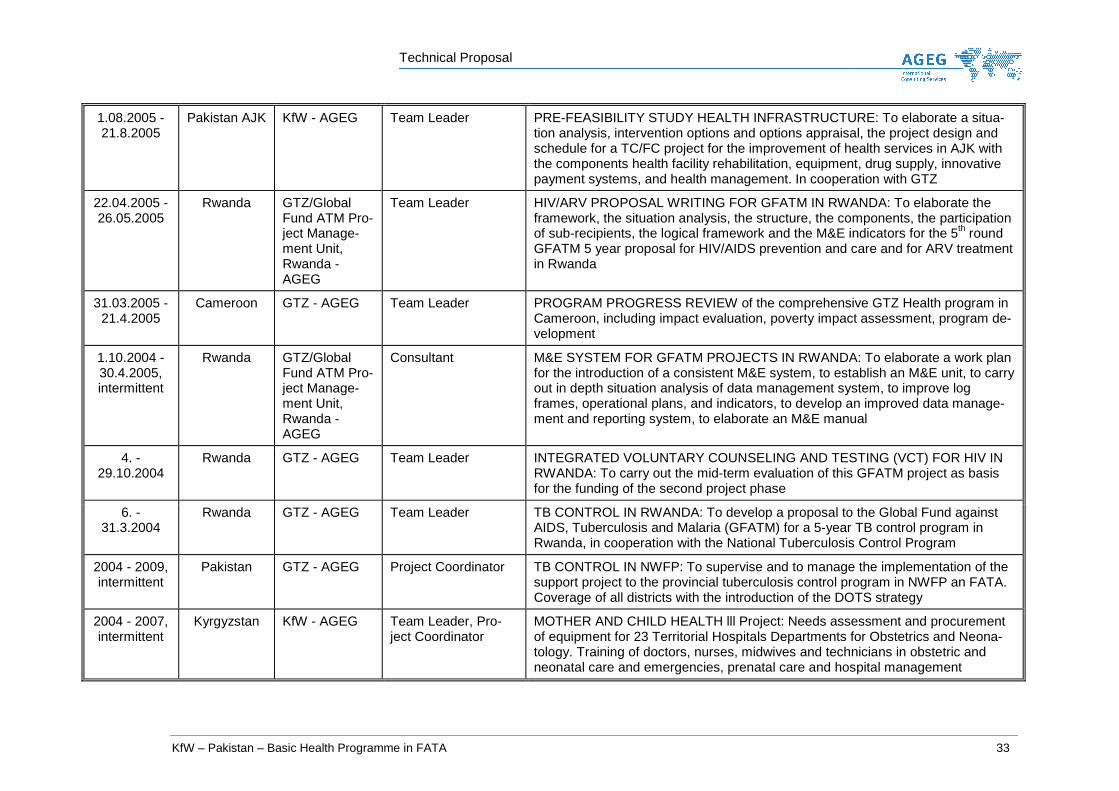
14. Professional experience
Date from - Date to
Location Company Position Description
July 2008 to June 2011
Germany AGEG Member of the Direc-torate of AGEG Con-sultants eG
To support the CEO in the general management of the consulting firm. To partici-pate in introduction of quality management. To guide the organisational develop-ment of the cooperative
June 2005 to June 2008
Germany AGEG Chairman of the AGEG board of su-pervisors
To supervise the CEO and to control the general development of the consulting firm. To participate in and to orient the introduction of quality management. To supervise the organisational development of the cooperative
1.2.1999 to date
Germany AGEG Head of AGEG Health Department
Management of AGEG health strategic planning, identification and coordination of health experts, networking with national and international organisations, selection of tenders and coordination of proposal writing, backstopping and management of short and long term assignments of AGEG health projects
1983 - 1995 Germany self employed Medical Doctor, Pae-diatrician
Practicing Paediatrics in own private practice
11.2009 - 04.2010
Cambodia World Bank Project Director HEALTH SECTOR SUPPORT PROGRAMME: To direct a consortium for the End-of-Project evaluation of the HSSP1 (2003-2008), involving 5 international Consultants and a national consulting firm, including a household survey on Health Equity Funds and a health facility assessment.
07.2009 Kenya GTZ Consultant HEALTH SECTOR STRATEGIC PLANNING: To moderate a planning workshop of all German Cooperation agencies in Kenya to design the contribution to the country’s Health Sector Strategic Plan for the next period.
07.2008 Cameroon KfW - AGEG Consultant HEALTH SECTOR STRATEGY PAPER design and write-up, as the basis for the future comprehensive German Health Sector Support Program (KfW, GTZ, DED) in the SWAp context
04.2008 Cameroon GTZ - AGEG Team Leader PROGRAM PROGRESS REVIEW of the comprehensive German Health Sector Support Program (KfW, GTZ, DED) and of the GTZ Health program in particular, including impact evaluation, Health-SWAp development and suggestions for fu-ture program components and strategies.
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 32
12.2007 Madagascar GTZ - AGEG Team Leader BASIC HEALTH PROJECT MAHAJANGA: To lead and carry out the final evalua-tion at the end of the 20 year long 16 million Euro project with main components district health system, reproductive health, HIV/AIDS, health care financing, pov-erty alleviation, quality management, essential drugs, decentralization, and com-munity participation, with interventions at community, district, province and na-tional level. Presentation of lessons learnt and of best practices.
1.3.2007 - 30.11.2009 intermittent
Pakistan KfW - AGEG Project Coordinator TB CONTROL IN NWFP: To supervise and to manage the implementation of the support project to the provincial tuberculosis control program in NWFP an FATA. Coverage of all districts with the procurement of anti-TB drugs, laboratory equip-ment and consumables, establishment of a TB reference lab and a quality control system..
1.11.2006 - 30.10.2008 intermittent
Kyrgyzstan KfW - AGEG Project Coordinator, Deputy Team Leader
HEALTH SECTOR PROGRAMME: To supervise and support the program de-signed to facilitate the implementation of the health sector reform and its SWAp financing facility, regarding health information systems, maintenance, health fi-nancing, quality assurance, human resources management an rationalization in service provision
1.10.2006 - 30.11.2010 intermittent
Pakistan, AJK
KfW - AGEG Project Coordinator, Deputy Team Leader
HEALTH INFRASTRUCTURE PROGRAM: To coordinate and supervise the im-plementation of the construction/rehabilitation and equipment of 3 hospitals from 50 to 400 beds, with training and hospital management consulting.
1.9. - 30.9.2006
Rwanda GTZ - AGEG Team Leader JOINT PROGRAM PROGRESS REVIEW of the comprehensive KfW/GTZ/DED/InWEnt Health program in Rwanda, including impact evaluation, poverty impact assessment, program development
15.11.2005 - 30.09.2006
Lao PDR Asian Devel-opment Bank - AGEG
Backstopper HEALTH SECTOR DEVELOPMENT PROGRAM: Preparation of a 6 year project and program support by ADB to the health sector. Guidance and quality assur-ance for a team of 12 experts in sector analysis, program design and write up
23.10.2005 - 13.11.2005
Pakistan KfW/ADB/World Bank - AGEG
Consultant EARTHQUAKE DAMAGE ASSESSMENT PAKISTAN: To assess, as part of the health team, the damages and losses in human lives and potential and physical infrastructure during the October 8th earthquake in AJK and NWFP. To develop strategies for medium and long term recovery and reconstruction taking into ac-count rationalization of the health care system as well as innovative financing and management set ups in cooperation with the private and NGO sector
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 33
1.08.2005 - 21.8.2005
Pakistan AJK KfW - AGEG Team Leader PRE-FEASIBILITY STUDY HEALTH INFRASTRUCTURE: To elaborate a situa-tion analysis, intervention options and options appraisal, the project design and schedule for a TC/FC project for the improvement of health services in AJK with the components health facility rehabilitation, equipment, drug supply, innovative payment systems, and health management. In cooperation with GTZ
22.04.2005 - 26.05.2005
Rwanda GTZ/Global Fund ATM Pro-ject Manage-ment Unit, Rwanda - AGEG
Team Leader HIV/ARV PROPOSAL WRITING FOR GFATM IN RWANDA: To elaborate the framework, the situation analysis, the structure, the components, the participation of sub-recipients, the logical framework and the M&E indicators for the 5th round GFATM 5 year proposal for HIV/AIDS prevention and care and for ARV treatment in Rwanda
31.03.2005 - 21.4.2005
Cameroon GTZ - AGEG Team Leader PROGRAM PROGRESS REVIEW of the comprehensive GTZ Health program in Cameroon, including impact evaluation, poverty impact assessment, program de-velopment
1.10.2004 - 30.4.2005, intermittent
Rwanda GTZ/Global Fund ATM Pro-ject Manage-ment Unit, Rwanda - AGEG
Consultant M&E SYSTEM FOR GFATM PROJECTS IN RWANDA: To elaborate a work plan for the introduction of a consistent M&E system, to establish an M&E unit, to carry out in depth situation analysis of data management system, to improve log frames, operational plans, and indicators, to develop an improved data manage-ment and reporting system, to elaborate an M&E manual
4. - 29.10.2004
Rwanda GTZ - AGEG Team Leader INTEGRATED VOLUNTARY COUNSELING AND TESTING (VCT) FOR HIV IN RWANDA: To carry out the mid-term evaluation of this GFATM project as basis for the funding of the second project phase
6. - 31.3.2004
Rwanda GTZ - AGEG Team Leader TB CONTROL IN RWANDA: To develop a proposal to the Global Fund against AIDS, Tuberculosis and Malaria (GFATM) for a 5-year TB control program in Rwanda, in cooperation with the National Tuberculosis Control Program
2004 - 2009, intermittent
Pakistan GTZ - AGEG Project Coordinator TB CONTROL IN NWFP: To supervise and to manage the implementation of the support project to the provincial tuberculosis control program in NWFP an FATA. Coverage of all districts with the introduction of the DOTS strategy
2004 - 2007, intermittent
Kyrgyzstan KfW - AGEG Team Leader, Pro-ject Coordinator
MOTHER AND CHILD HEALTH lll Project: Needs assessment and procurement of equipment for 23 Territorial Hospitals Departments for Obstetrics and Neona-tology. Training of doctors, nurses, midwives and technicians in obstetric and neonatal care and emergencies, prenatal care and hospital management

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 34
March - Sep-tember 2003 intermittent
Pakistan ADB - AGEG Project Coordinator EARLY CHILDHOOD DEVELOPMENT Project, Project Preparation TA, back-stopping the international and the domestic team of experts, in the field of child health (0 to 8 years), nutrition, early education, community based initiatives, child care, capacity building of local governments
22.9. - 4.10.2002
Kenya GTZ - AGEG Consultant REPRODUCTIVE HEALTH: midterm evaluation of the Reproductive Health Pro-ject Kenya
2001 - 2004, intermittent
Kyrgyzstan KfW - AGEG Team Leader, project coordinator
MOTHER AND CHILD HEALTH II Project: Needs assessment and procurement of equipment for 28 Rayon Hospitals Departments for Obstetrics and Neonatol-ogy. Training of doctors, nurses, midwives and technicians in obstetric and neo-natal care and emergencies, prenatal care and hospital management.
2001 - 2007, intermittent
Haiti GTZ - AGEG Project Coordinator REPRODUCTIVE HEALTH. Design and supervision of implementation of a re-gional HIV/AIDS/STI/FP project. Steering of long- and short-term experts. Techni-cal backstopping for project staff. Strong focus on community-based organisa-tions (CBO).
2001 - 2003 intermittent
Madagascar European Commission - AGEG
Consultant HOSPITAL PLANNING. Designed a format and methodology for strategic plan-ning for 14 district hospitals. Advocated for decentralized hospital planning au-thority. Corrected and validated the floor plans and functional paths of a district hospital.
19.3. – 1.4.2001
Kyrgyzstan KfW - AGEG Consultant HIV/AIDS: Designed concept and strategic planning, based on needs assess-ment, of a new project for HIV/AIDS prevention, nation-wide.
18.5. - 10.6.2000
Haiti CARITAS Suisse - AGEG
Consultant HOSPITAL EQUIPMENT: Established a surgical department in a district hospital, including procurement of equipment, design of procedures and standards, draft of manuals and training of personnel.
24.4. - 18.5.2000
Haiti German Agro-Action - AGEG
Consultant HEALTH and FOOD SECURITY: Assessed the nutrition and health education needs in the North-West of Haïti, evaluated previous experiences and elaborated strategies for a food security program in the field of nutrition education, nutrition surveillance, family planning and primary health care
02.1999-11.1999
and 2.2000
Haiti Caritas Suisse - AGEG
Consultant HOSPITAL MANAGEMENT: Evaluation of district hospital management and comprehensive support to develop sustainable management structures including financing and cost recovery

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 35
08.1999-09.1999
Ethiopia EZE - AGEG Consultant REPRODUCTIVE HEALTH: Evaluated a program of Reproductive Health, Family Planning and Adolescent Health in several parts of the country. The program in-cluded strategies like community-based distribution of contraceptives, peer edu-cator approach, IEC, counseling training and management of STD/HIV/AIDS pre-vention and treatment.
03.1999-04.1999
Botswana BMZ - AGEG Consultant PHC INFRASTRUCTURE: In the framework of a series of world-wide ex-post evaluations, assessing the impact of KfW PHC/health infrastructure project that had been completed in 1995, through standardized impact evaluation tool
2.1998 and 11.1998-12.1998
Palestinian Territories
GTZ - AGEG Team Leader REPRODUCTIVE HEALTH: Fact finding and project planning mission to the Pal-estinian territories for a new GTZ program in Reproductive Health and Family Planning
10.1998-11.1998
Nigeria Misereor - AGEG
Consultant HOSPITAL MANAGEMENT: Evaluation and consultancy for a second level hospi-tal. Analysis of structural, operational and financial management. Support in man-agement planning aiming at PHC approach, effective referral functions, appropri-ate teaching and supervisory activities, quality management and sustainability of services
04.1998-04.1998
Azerbaijan GTZ - AGEG Consultant TRAINING: Training and continuing education for pediatricians, gynecologists and obstetricians. Quality assessment in government hospitals
07.1997-09.1997
Uganda DED Team Leader DISTRICT HEALTH: Evaluated different approaches of German Development Service (DED) involvement in two health districts in Uganda. Assessed the effec-tiveness of expatriate health advisers and the quality of health services and de-fined anticipated needs using quantitative and qualitative evaluation tools. As-sisted in strategic planning, concept development and design of future interven-tions
01.1996-07.1996
Guinea DED Program Coordinator REGIONAL HEALTH and PHC: Evaluated, modified and implemented the first phase of a KfW financed regional health program in Upper Guinea. Set up the or-ganisational structure for the German Development Service (DED) in Guinea. De-signed a comprehensive project of technical assistance for the regional health system including PHC at Kankan. Elaborated job descriptions and work plans. Performed situation analysis in 5 health district hospitals

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 36
01.1996-12.1997
Haiti NGO Consultant DISTRICT HEALTH: Initiated and participated in the reorganisation of District Health Services in the Commune de Gros Morne/Haiti and in the reorganisation and reconstruction of the Alma Mater Hospital in Gros Morne. Composed the steering committee, coordinated funding and technical teams. Participated in the design of studies for outcome assessment, needs assessment and feasibility for the hospital and the district health system. Promoted the integration in the Na-tional Health Policy and in the UCS-Program (Unité Communautaire de Santé).
06.1975-04.1978
Haiti Misereor - AGEH
Hospital Director HOSPITAL AND DISTRICT MANAGEMENT: Directed and developed a District Hospital. Trained paramedical personnel. Initiated nutrition education, under-fives clinics, prenatal clinics, health education, immunization and family planning pro-grams. Trained and supervised traditional birth attendants. Installed accounting and administration. Introduced standardized treatments, the use of essential drugs, and mobile clinics. Initiated the "Gros Morne Integrated Rural Development Project"
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA
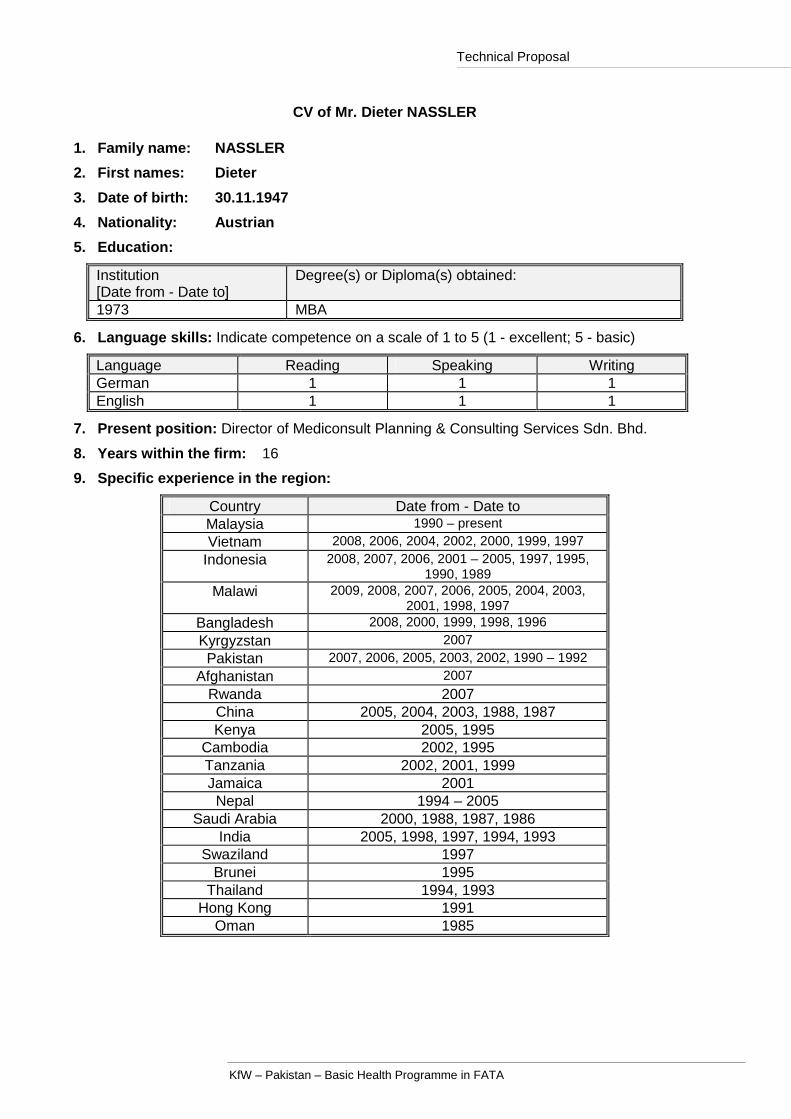
CV of Mr. Dieter NASSLER 1. Family name: NASSLER
2. First names: Dieter
3. Date of birth: 30.11.1947
4. Nationality: Austrian
5. Education:
Institution [Date from - Date to]
Degree(s) or Diploma(s) obtained:
1973 MBA
6. Language skills: Indicate competence on a scale of 1 to 5 (1 - excellent; 5 - basic)
Language Reading Speaking Writing German 1 1 1 English 1 1 1
7. Present position: Director of Mediconsult Planning & Consulting Services Sdn. Bhd.
8. Years within the firm: 16
9. Specific experience in the region:
Country Date from - Date to Malaysia 1990 – present Vietnam 2008, 2006, 2004, 2002, 2000, 1999, 1997
Indonesia 2008, 2007, 2006, 2001 – 2005, 1997, 1995, 1990, 1989
Malawi 2009, 2008, 2007, 2006, 2005, 2004, 2003, 2001, 1998, 1997
Bangladesh 2008, 2000, 1999, 1998, 1996
Kyrgyzstan 2007 Pakistan 2007, 2006, 2005, 2003, 2002, 1990 – 1992
Afghanistan 2007
Rwanda 2007 China 2005, 2004, 2003, 1988, 1987 Kenya 2005, 1995
Cambodia 2002, 1995 Tanzania 2002, 2001, 1999 Jamaica 2001 Nepal 1994 – 2005
Saudi Arabia 2000, 1988, 1987, 1986 India 2005, 1998, 1997, 1994, 1993
Swaziland 1997 Brunei 1995
Thailand 1994, 1993 Hong Kong 1991
Oman 1985

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 38
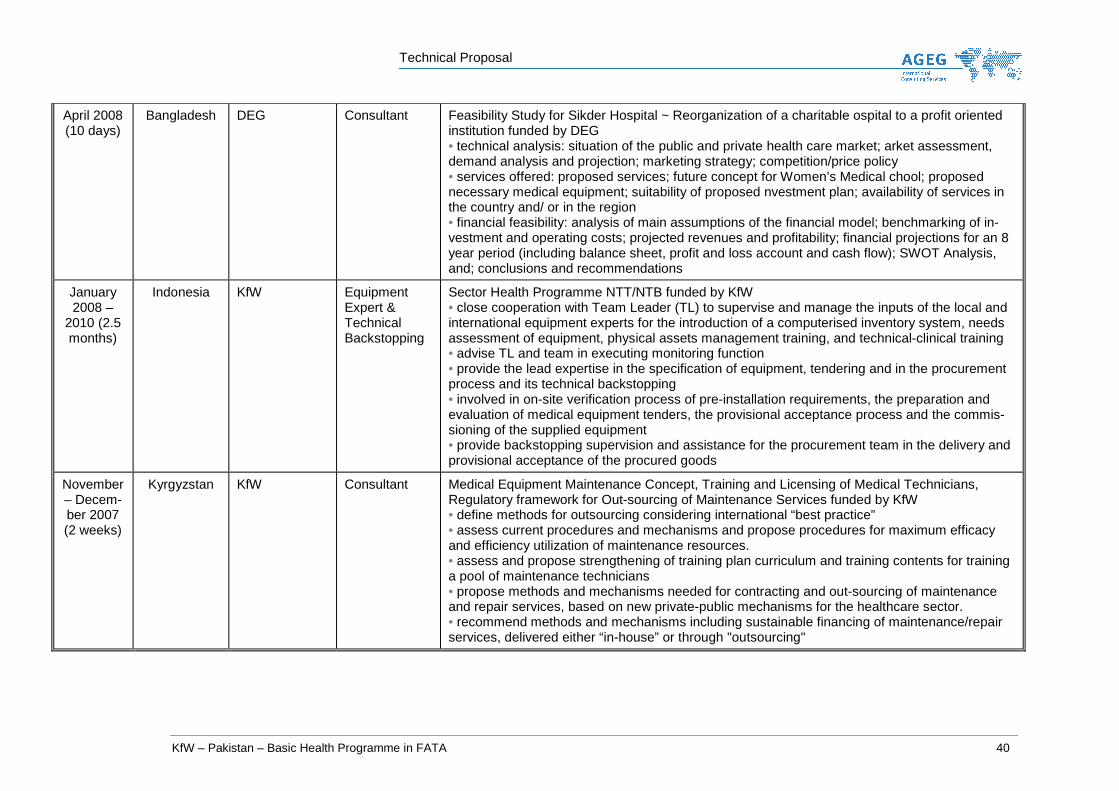
10. Professional experience
Date from - Date to
Location Company Position Description
1993 – present
Malaysia Mediconsult Planning & Consulting Services
Director Director of Mediconsult Planning & Consulting Services Sdn. Bhd.
1990 – 1992
Malaysia VAMED Engi-neering
Managing Di-rector
Managing Director of VAMED Engineering Malaysia
1986 – 1990
Austria VAMED Engi-neering
Director, Hos-pital Manage-ment and Consulting
• Participation and project management in numerous international health care projects. (Refer to list of projects) • Acquisition and negotiations for contracts related to hospital projects and health consulting. • Fact finding missions and project appraisals. • Recruiting of medical staff for foreign hospitals.
1978 – 1985
Austria AGIPLAN Be-triebplanungs-gesellschaft M.B.H., Vienna
Chief of the Department of Health Care Projects
Chief of the Department of Health Care Projects • Participation and project management in numerous health care projects (refer to list of projects)
1973 – 1978
Germany VEB Gebaude-verwaltung, Leipzig
Finance Man-ager
Finance Manager • Materials management, cost accounting, financial project evaluation, financial reporting
October to December 2008 (20
days)
Vietnam Johns Hopkins University School of Public Health
Team Leader Business Plan for the Center for Community Health Research and Development (CCRD), funded through Johns Hopkins University School of Public Health CCRD is one of the first non-governmental and nonprofit Vietnamese organizations specialized in research and interventions for community health promotion, and has been supported by Johns Hopkins’ Center for Com-munication for the past years to be developed into the leading health communication centre. A Business Plan was requested by the funding agency, the main task therefore was to assess the current strengths of CCRD within the existing environment in Vietnam and to develop both a 5 year strategic and a 5 year business plan for the sustainability and future growth of CCRD as the leading center for health and development communication in Vietnam.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 39
June 2008 to Febru-ary 2009
Malawi MoH/KfW Consultant / Procurement agent
Strengthening of Public Financing System with a focus on SWAp procedures, procurement agent for MoH/KfW • Assessment of hardware needs for district cost centres and MoH; • Procurement agent for consulting services to improve the accounting capacity of the Cost Cen-tres through Financial Management Coaches; • Procurement agent for the provision of computers for selected cost centres;
April 2008 – Febru-ary 2009 (45 days)
Vietnam Finnish Concessional Credits Pro-gramme
International Expert
Feasibility Study for ODA support through Finland, funded by the Finnish Concessional Credits Programme The programme included general hospitals of the provinces in Da Nang, Ha Nam and Nghe An • Assessment and analysis of the health system in Vietnam • Assess market feasibility based on health indicators, hospital performance and management capacity • Compilation of demand determination • Establishing preliminary cost estimation of medical equipment to be procurement • Develop the concept and implementation strategy • Needs Assessment for capacity building and training.
April – May 2008 (10 days)
Indonesia KfW Medical Equip-ment Special-ist
Pre-feasibility Study for Capacity Improvement of Animal Health Laboratories for HPAI diagnosis and vaccine quality control funded by KfW • provide overview of the existing veterinary laboratory in AI prevention and ontrol • design a feasible programme concept for appropriately upgrading the eterinary laboratory sys-tem for AI prevention and control matching the funds vailable • estimate the operational cost of the upgraded laboratories • estimate the required maintenance services and cost of the laboratory quipment procured • suggest meaningful accompanying TA measures with particular attention to raining activities on laboratory equipment • elaborate a draft plan for implementation of the project including an estimate f duration for the execution of the programme
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 40
April 2008 (10 days)
Bangladesh DEG Consultant Feasibility Study for Sikder Hospital ~ Reorganization of a charitable ospital to a profit oriented institution funded by DEG • technical analysis: situation of the public and private health care market; arket assessment, demand analysis and projection; marketing strategy; competition/price policy • services offered: proposed services; future concept for Women’s Medical chool; proposed necessary medical equipment; suitability of proposed nvestment plan; availability of services in the country and/ or in the region • financial feasibility: analysis of main assumptions of the financial model; benchmarking of in-vestment and operating costs; projected revenues and profitability; financial projections for an 8 year period (including balance sheet, profit and loss account and cash flow); SWOT Analysis, and; conclusions and recommendations
January 2008 –
2010 (2.5 months)
Indonesia KfW Equipment Expert & Technical Backstopping
Sector Health Programme NTT/NTB funded by KfW • close cooperation with Team Leader (TL) to supervise and manage the inputs of the local and international equipment experts for the introduction of a computerised inventory system, needs assessment of equipment, physical assets management training, and technical-clinical training • advise TL and team in executing monitoring function • provide the lead expertise in the specification of equipment, tendering and in the procurement process and its technical backstopping • involved in on-site verification process of pre-installation requirements, the preparation and evaluation of medical equipment tenders, the provisional acceptance process and the commis-sioning of the supplied equipment • provide backstopping supervision and assistance for the procurement team in the delivery and provisional acceptance of the procured goods
November – Decem-ber 2007 (2 weeks)
Kyrgyzstan KfW Consultant Medical Equipment Maintenance Concept, Training and Licensing of Medical Technicians, Regulatory framework for Out-sourcing of Maintenance Services funded by KfW • define methods for outsourcing considering international “best practice” • assess current procedures and mechanisms and propose procedures for maximum efficacy and efficiency utilization of maintenance resources. • assess and propose strengthening of training plan curriculum and training contents for training a pool of maintenance technicians • propose methods and mechanisms needed for contracting and out-sourcing of maintenance and repair services, based on new private-public mechanisms for the healthcare sector. • recommend methods and mechanisms including sustainable financing of maintenance/repair services, delivered either “in-house” or through "outsourcing"
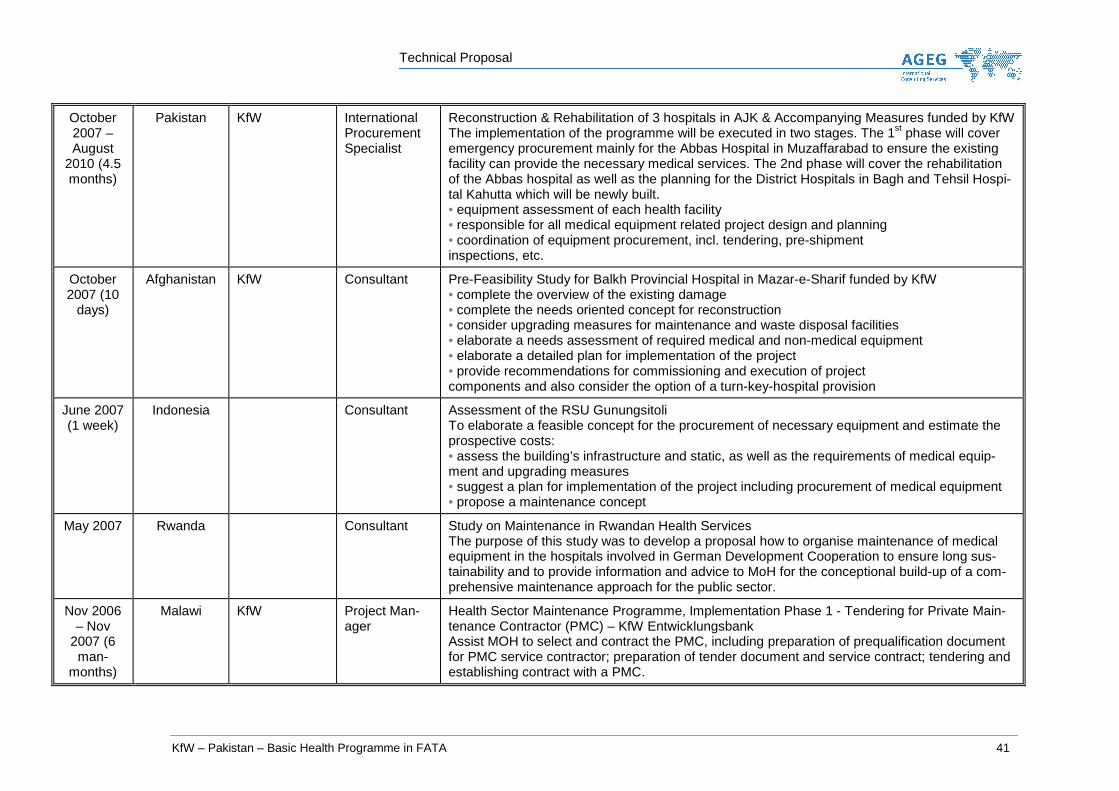
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 41
October 2007 – August
2010 (4.5 months)
Pakistan KfW International Procurement Specialist
Reconstruction & Rehabilitation of 3 hospitals in AJK & Accompanying Measures funded by KfW The implementation of the programme will be executed in two stages. The 1st phase will cover emergency procurement mainly for the Abbas Hospital in Muzaffarabad to ensure the existing facility can provide the necessary medical services. The 2nd phase will cover the rehabilitation of the Abbas hospital as well as the planning for the District Hospitals in Bagh and Tehsil Hospi-tal Kahutta which will be newly built. • equipment assessment of each health facility • responsible for all medical equipment related project design and planning • coordination of equipment procurement, incl. tendering, pre-shipment inspections, etc.
October 2007 (10
days)
Afghanistan KfW Consultant Pre-Feasibility Study for Balkh Provincial Hospital in Mazar-e-Sharif funded by KfW • complete the overview of the existing damage • complete the needs oriented concept for reconstruction • consider upgrading measures for maintenance and waste disposal facilities • elaborate a needs assessment of required medical and non-medical equipment • elaborate a detailed plan for implementation of the project • provide recommendations for commissioning and execution of project components and also consider the option of a turn-key-hospital provision
June 2007 (1 week)
Indonesia Consultant Assessment of the RSU Gunungsitoli To elaborate a feasible concept for the procurement of necessary equipment and estimate the prospective costs: • assess the building’s infrastructure and static, as well as the requirements of medical equip-ment and upgrading measures • suggest a plan for implementation of the project including procurement of medical equipment • propose a maintenance concept
May 2007 Rwanda Consultant Study on Maintenance in Rwandan Health Services The purpose of this study was to develop a proposal how to organise maintenance of medical equipment in the hospitals involved in German Development Cooperation to ensure long sus-tainability and to provide information and advice to MoH for the conceptional build-up of a com-prehensive maintenance approach for the public sector.
Nov 2006 – Nov
2007 (6 man-
months)
Malawi KfW Project Man-ager
Health Sector Maintenance Programme, Implementation Phase 1 - Tendering for Private Main-tenance Contractor (PMC) – KfW Entwicklungsbank Assist MOH to select and contract the PMC, including preparation of prequalification document for PMC service contractor; preparation of tender document and service contract; tendering and establishing contract with a PMC.
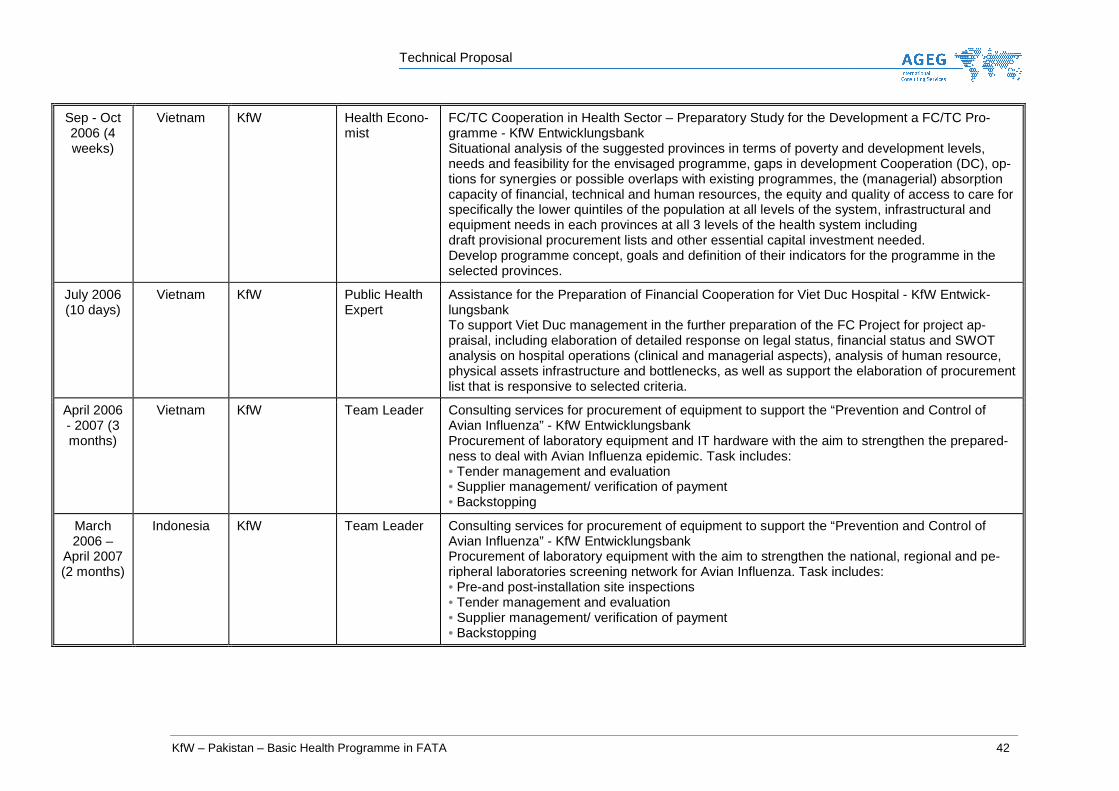
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 42
Sep - Oct 2006 (4 weeks)
Vietnam KfW Health Econo-mist
FC/TC Cooperation in Health Sector – Preparatory Study for the Development a FC/TC Pro-gramme - KfW Entwicklungsbank Situational analysis of the suggested provinces in terms of poverty and development levels, needs and feasibility for the envisaged programme, gaps in development Cooperation (DC), op-tions for synergies or possible overlaps with existing programmes, the (managerial) absorption capacity of financial, technical and human resources, the equity and quality of access to care for specifically the lower quintiles of the population at all levels of the system, infrastructural and equipment needs in each provinces at all 3 levels of the health system including draft provisional procurement lists and other essential capital investment needed. Develop programme concept, goals and definition of their indicators for the programme in the selected provinces.
July 2006 (10 days)
Vietnam KfW Public Health Expert
Assistance for the Preparation of Financial Cooperation for Viet Duc Hospital - KfW Entwick-lungsbank To support Viet Duc management in the further preparation of the FC Project for project ap-praisal, including elaboration of detailed response on legal status, financial status and SWOT analysis on hospital operations (clinical and managerial aspects), analysis of human resource, physical assets infrastructure and bottlenecks, as well as support the elaboration of procurement list that is responsive to selected criteria.
April 2006 - 2007 (3 months)
Vietnam KfW Team Leader Consulting services for procurement of equipment to support the “Prevention and Control of Avian Influenza” - KfW Entwicklungsbank Procurement of laboratory equipment and IT hardware with the aim to strengthen the prepared-ness to deal with Avian Influenza epidemic. Task includes: • Tender management and evaluation • Supplier management/ verification of payment • Backstopping
March 2006 –
April 2007 (2 months)
Indonesia KfW Team Leader Consulting services for procurement of equipment to support the “Prevention and Control of Avian Influenza” - KfW Entwicklungsbank Procurement of laboratory equipment with the aim to strengthen the national, regional and pe-ripheral laboratories screening network for Avian Influenza. Task includes: • Pre-and post-installation site inspections • Tender management and evaluation • Supplier management/ verification of payment • Backstopping

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 43
March 2006 (2 months)
Vietnam World Bank Consultant Health Funds for the Poor – World Bank To improve the equity and efficiency in the financing and delivery of health care in seven North-ern Uplands Provinces (Bac Kan, Cao Bang, Ha Giang, Lao Cai, Son La, Lai Chau & Dien Bien) • Conduct overall assessment of the health care & hospital system. • Assess the roles and potential contributions of private health sector Participate in seminars & workshops.
Jan-Feb 2006 (2 weeks)
Pakistan KfW Consultant Project Preparation Study for Post-Earthquake Hospitals Reconstruction in AJK - KfW Situation analysis on the aftermath of earthquake in health sector to determine the needs for re-construction. Prepare project proposal including project components, results, and cost estimate.
Jan 2006 (1 week)
Vietnam Lux-Development
Consultant Project Implementation Review for Hung Yen Provincial Health Assistance Project - Lux-Development Review implementation status and prepare work-plan for the completion of project, including the Annual Work-Plan and Budget.
August 2005 (4 weeks)
Pakistan KfW Consultant Feasibility Study for Health Infrastructure in Azad Jammu Kashmir (AJK) - KfW The study examines the structure and condition of health sector; develops and evaluates feasi-ble interventions; conceptual final project proposal with justification of selected interventions, project impact and risk assessment.
May 2005 (3 weeks)
China DEG / KfW Consultant Feasibility Study for the Establishment of an International Heart Hospital - DEG KfW-Bankengruppe The study examines the financial feasibility and the technical as well as management capacity for the operation of an 80-bed international heart hospital in Beijing.
March 2005
(3weeks)
Kenya KfW Logistic Con-sultant
Commodity Audit for Contraceptives - KfW Entwicklungsbank Review of the logistic system for the distribution of contraceptives, and conducting a simplified commodity audit in all levels of the distribution system.
January 2005 (on-
going)
Indonesia KfW / AUSAID Backstopper/ Technical Ad-visor
Post-tsunami Rehabilitation and Reconstruction of Dr Zainoel Abidin Hospital, Banda Aceh – KfW Entwicklungsbank & AUSAID Provides backstopping and technical advisory services for the rehabilitation, reconstruction mas-ter-planning of the hospital, as well as maintenance and procurement of equipment.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 44
Jan – April 2004 &
Septem-ber 2004 (4 weeks)
Vietnam MOH/World Bank
Team Leader Project Preparation Study for Mekong Health Support Project & Project Design – MOH/WB The project attempts to explore regionalisation of health system in Mekong Delta Region. The project covers all 13 provinces in the Region, the tasks performed are to: • Conduct a situational analysis on the health status, organisation of health system, health provi-sion and utilisation, health prospects focusing on equity, health seeking behaviour, quality of services, curative and preventive medicine, role and function of a regional hospital; • Health financing and spending analysis, source of funding, health care fees and health care fund for the poor as well as analysis of the future challenges in health financing; • Develop strategic options for management considerations for issues associated with curative and preventive health, in particular the feasibility of establishing a regional hospital and the as-sociating aspects in organisation, financial, training, monitoring & evaluation and; • Prepare budget estimation for the project. • Synthesize the issues within the strategic context such as the main sector issues, government strategy, sector issues that will be addressed by the project and its strategic choice.
Dec 2003 – Jan 2004
China KfW Team Leader Feasibility Study for Health Sector II & III / HIV Preventive Programme – KfW The study assesses the provincial and prefecture Centre for Disease Control and Prevention (CDC) in 8 provinces, with the objectives to: • Validate the role, services and capacity of the CDCs, • Assess the needs and benefits of equipment upgrading, • Harmonise the proposed equipment list of all CDCs, • Develop framework for implementation covering schedule, planning stages and recommendations for implementation process of the programme.
2005/ 2004/
2003 (4 months)
Malawi KfW Team Leader Health Sector Maintenance Programme (KfW) Framework development for contracting out maintenance services for medical equipment to the private sector based on a Public-Private Partnership approach, among others, delineation of roles & responsibilities, scope of contracting out services, service contract, and preliminary budget estimate. Preparation of the nationwide inventory for medical equipment and monitoring of survey.
2003 (3 weeks)
Pakistan KfW Consultant Basic Healthcare Programme, Northern Area (KfW) Sector analysis related to health financing, structure of delivery system and condition of facilities to obtain approval of the project and define accompanying measures related to facility planning and mapping of healthcare facilities.
2002 (3 months)
Vietnam KfW Team Leader Provincial Hospital Development I (KfW) –2003 to 2005 Medical equipment and maintenance planning for 5 provincial hospitals, tendering assistance and supervision of installation and training as well as evaluation of equipment needs related to the hospital development plans for the three years programme.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 45
2002 (3 weeks)
Cambodia KfW Consultant Reproductive Health Project Cambodia (KfW) Situation analysis of reproductive health related to contraceptive availability and demand, pro-curement and distribution as well as qualification of health personnel. Development of project proposal to assure contraceptive coverage and proper distribution.
2002 (1 month)
Pakistan KfW Consultant Basic Health Care Programme – North-West Frontier Province (KfW) Project evaluation for the final approval of project financing for the supply of medical equipment for district hospitals, health centers and accompanying and mapping of health care facilities of district level.
2002 (6 weeks)
Vietnam KfW Consultant Provincial Hospital Development II (KfW) Feasibility study for the provincial hospital development for four provinces, covering the opera-tional, economic and equipment as well as maintenance aspects. The study developed the framework for the implementation including medical equipment supply, hospital information sys-tem, training and management support.
2002 (3 weeks)
Tanzania KfW Consultant Tanga Region – Health Development Programme (KfW) Assessment of operational and economic aspects as well as equipment and development of a strategic framework to support the Region health delivery system over a period of 10 years. The study included management capacity, operating cost, financing and catchment analysis.
2001 (3 weeks)
Malawi IFC Team Leader Operational Review of Mwaiwathu private Hospital, Blantyre (IFC) Operational review of the private hospital in relation to services, manpower, cost structure, profit and loss account for three years and recommendations for the improvement of overall hospital performance.
2001 (3 weeks)
Tanzania KfW Consultant Commodity Audit for Contraceptives (KfW) Commodity audit for the logistics system and supply of injectables funded by KfW at all levels of the distribution system and recommendation for improvement and implementation.
2001 (3 weeks)
Jamaica KfW Consultant Post Rehabilitation Audit of Two Hospitals (KfW) Post rehabilitation audit study for the two hospitals rehabilitated under the Health Service Ra-tionalisation Projects related to utilisation of medical services, financing, equipment and overall hospital performance.
6 months between 2001 and
2005
Indonesia KfW Team Leader Rehabilitation of Dr. Kariadi Hospital, Semarang (KfW) - 2001 to 2005 • Preparation of functional programme and schedule of accommodation for the 600-bed teaching hospital as basis for the masterplan; • Management of measures to improve the management skills (quality management, accounting & finance as well as human resource development) of the hospital personnel; • Procurement assistance for medical equipment and supervision of installation and training; • Review of existing maintenance organisation and development of a maintenance concept.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 46
2001 (4 months)
Nepal GTZ Team Leader Community Based Drug Management (CBDM), (GTZ) • Assistance to the government of Nepal, Department of Health Services in the procurement of contraceptives and monitoring of distribution. • Implementation of community based drug programmes, review material and monitoring training programmes at district and village level. • Assessment and analysis of logistic issues related to the Community Drug Programme
2000 (2 weeks)
Bangladesh World Bank Consultant Participation in the Midterm Review of the Health and Population Sector Programme (HPSP) re-lated to procurement and logistics.
2000 (2 weeks)
Saudi Arabia Islamic Deve-lopment Bank (IDB)
Consultant Appraisal of feasibility study for a 500-bed private hospital in Al-kober including assessment of management capacity of the future operator.
2000 (3 weeks)
Vietnam KfW Consultant Development of project proposal for the upgrading of 5 provincial hospitals in Vietnam funded by KfW.
2000 (3 weeks)
Bangladesh World Bank Consultant Assessment of procurement capacity for the Health and Population Sector Programme and de-velop a proposal for the procurement structure to improve the quality and organisation of pro-curement.
1999 (2 months)
Vietnam European Uni-on
Consultant Assessment of requirements of medical equipment for Provincial and District Hospitals in 3 prov-inces. Planning of medical equipment to be provided through the project, which is funded by the European Commission.
1999 (7 months)
Bangladesh (KfW)/EPOS Consultant Kreditanstalt fur Wiederaufbau (KfW)/EPOS Procurement assistance comprising of tender preparation, tendering and supervision of supply for contraceptives funded by KfW.
1999 (2 months)
Tanzania KfW Consultant Kreditanstalt fur Wiederaufbau (KfW) Involved in verification of quantities for the procurement of medical equipment and essential drugs for the Commodity Aid Programme financed by KfW. Preparation of specification and ten-der documents, tendering as well as supervision of installation and distribution
1998 (2 months)
Bangladesh KfW Consultant Kreditanstalt fur Wiederaufbau (KfW) Tasks Assessment of logistic and distribution of contraceptives under the Health and Population Programme (HAPP4) to improve quality assurance for contraceptives and monitoring of distribu-tion to reduce system losses.
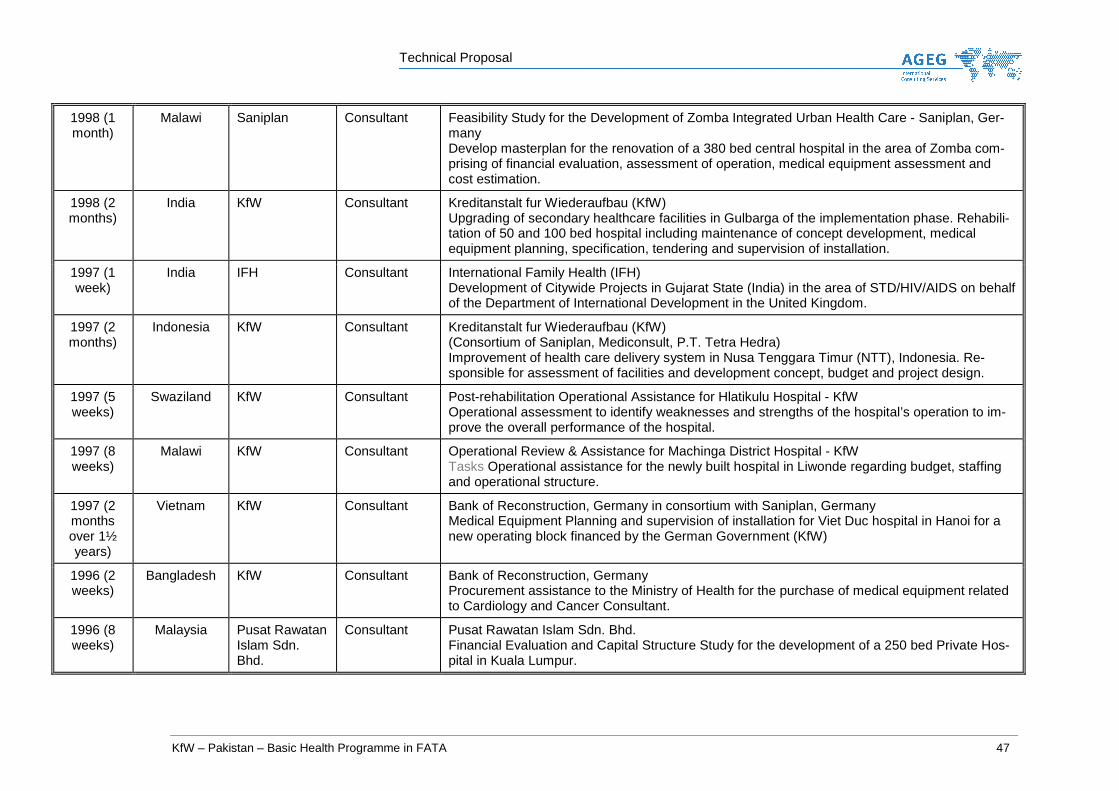
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 47
1998 (1 month)
Malawi Saniplan Consultant Feasibility Study for the Development of Zomba Integrated Urban Health Care - Saniplan, Ger-many Develop masterplan for the renovation of a 380 bed central hospital in the area of Zomba com-prising of financial evaluation, assessment of operation, medical equipment assessment and cost estimation.
1998 (2 months)
India KfW Consultant Kreditanstalt fur Wiederaufbau (KfW) Upgrading of secondary healthcare facilities in Gulbarga of the implementation phase. Rehabili-tation of 50 and 100 bed hospital including maintenance of concept development, medical equipment planning, specification, tendering and supervision of installation.
1997 (1 week)
India IFH Consultant International Family Health (IFH) Development of Citywide Projects in Gujarat State (India) in the area of STD/HIV/AIDS on behalf of the Department of International Development in the United Kingdom.
1997 (2 months)
Indonesia KfW Consultant Kreditanstalt fur Wiederaufbau (KfW) (Consortium of Saniplan, Mediconsult, P.T. Tetra Hedra) Improvement of health care delivery system in Nusa Tenggara Timur (NTT), Indonesia. Re-sponsible for assessment of facilities and development concept, budget and project design.
1997 (5 weeks)
Swaziland KfW Consultant Post-rehabilitation Operational Assistance for Hlatikulu Hospital - KfW Operational assessment to identify weaknesses and strengths of the hospital’s operation to im-prove the overall performance of the hospital.
1997 (8 weeks)
Malawi KfW Consultant Operational Review & Assistance for Machinga District Hospital - KfW Tasks Operational assistance for the newly built hospital in Liwonde regarding budget, staffing and operational structure.
1997 (2 months over 1½ years)
Vietnam KfW Consultant Bank of Reconstruction, Germany in consortium with Saniplan, Germany Medical Equipment Planning and supervision of installation for Viet Duc hospital in Hanoi for a new operating block financed by the German Government (KfW)
1996 (2 weeks)
Bangladesh KfW Consultant Bank of Reconstruction, Germany Procurement assistance to the Ministry of Health for the purchase of medical equipment related to Cardiology and Cancer Consultant.
1996 (8 weeks)
Malaysia Pusat Rawatan Islam Sdn. Bhd.
Consultant Pusat Rawatan Islam Sdn. Bhd. Financial Evaluation and Capital Structure Study for the development of a 250 bed Private Hos-pital in Kuala Lumpur.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 48
1995 Cambodia KfW Consultant Bank of Reconstruction, Germany Study on Mother-Child Health, Birth Spacing, STD/HIV/AIDS Prevention in Cambodia and pro-ject development for financial assistance related to improvement of Birth Spacing and Mother-Child Health
1995 Indonesia Kumpulan Pe-rangsang Se-langor Berhad
Consultant Kumpulan Perangsang Selangor Berhad Tasks Feasibility Study for a 200-bed private hospital. This feasibility study composed of a mar-ket analysis, physical planning and determination of investment cost and financial structure of the project.
1995 Brunei ATH-Niagabena Sdn. Bhd.
Consultant ATH-Niagabena Sdn. Bhd. Tasks Feasibility study for an 80-bed private hospital. This feasibility study comprised of a mar-ket analysis, physical planning and determination of investment cost and financial structure of the project.
1995 Kenya International Family Health, London
Consultant International Family Health, London Tasks Team member for the development of project concept to strengthen the Reproductive Health with the Government and N.G.O.
1994 to 2005
(about 12 months)
Nepal EPOS Consul-tant, Germany
Procurement and Logistics Consultant
Supervision of procurement for basic medical equipment and essential drug supply for primary health centres financed by the German Government, introduction of pull system for the distribu-tion of drugs and contraceptives.
1994 / 2005
India KfW Team Leader Bank of Reconstruction, Germany Upgrading Secondary Level Hospitals in Karnataka, India Concept development for upgrading of secondary level hospitals in consideration of cost recov-ery and operating budget constraints.
1994 Thailand Consultant 200 bed hospital, Siamdol, Thailand Feasibility study comprises of market analysis including room and space programme and all fi-nancial aspects
1993 India KfW Consultant Bank of Reconstruction, Germany (Family planning and rehabilitation of health facilities in Maharashtra) Project Appraisal related to the rehabilitation of health facilities in respect of requirements and budget

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 49
1993 Thailand Hospital Pibul Song Gram Hospital Bang-kok
Consultant Feasibility study for investment decision
1993 Thailand Consultant 350 bed Private Hospital, Mahawogse Feasibility study comprises of market analysis including room and space programme and all fi-nancial aspects
1993 Malaysia Seremban Ge-neral Hospital
Consultant Feasibility study for 120 bed in Seremban
1992 / 1993
Malaysia ADB Consultant Masterplanning of 7 hospitals in Malaysia (ADB Project) Tasks Project Consultant of overall administration and financial duties related to the Masterplan Project
1990 - 1992
Pakistan / Malaysia / Thailand
ADB Managing Di-rector
Project acquisition and project negotiations for health care projects ADB-Project in Malaysia for upgrading of 7 hospitals • various feasibility studies in Malaysia; • design, engineering and Project management of a Paediatric hospital in Quetta, Pakistan • medical equipment planning and functional concept for a 450 bed private hospital in Bangkok
1991 Hong Kong Project Man-ager
Feasibility Study Private Hospital Feasibility study comprises of market analysis including room and space programme and all fi-nancial aspects.
1990 - 1992
Malaysia Cardio Tho-racic Centre Kuala Lumpur
Managing Di-rector
Monitoring of the planning stage and the implementation of the turnkey project.
1990 Indonesia KfW Project Man-ager
Bank of Reconstruction, Germany Assistance in elaboration of the Masterplan of 4 hospitals in South Kalimantan to the local con-sultant.
1989 Indonesia KfW Project Man-ager
Appraisal mission South Kalimantan for Bank of Reconstruction (KFW), Germany Appraisal mission for the upgrading of 4 hospitals and various health centres in South Kaliman-tan
1988 – 1989
Hungary Project Man-ager
200 bed Rehabilitation Centre Budapest Feasibility study comprises of market analysis including international patient sourcing room and space programme, investment cost and financing.
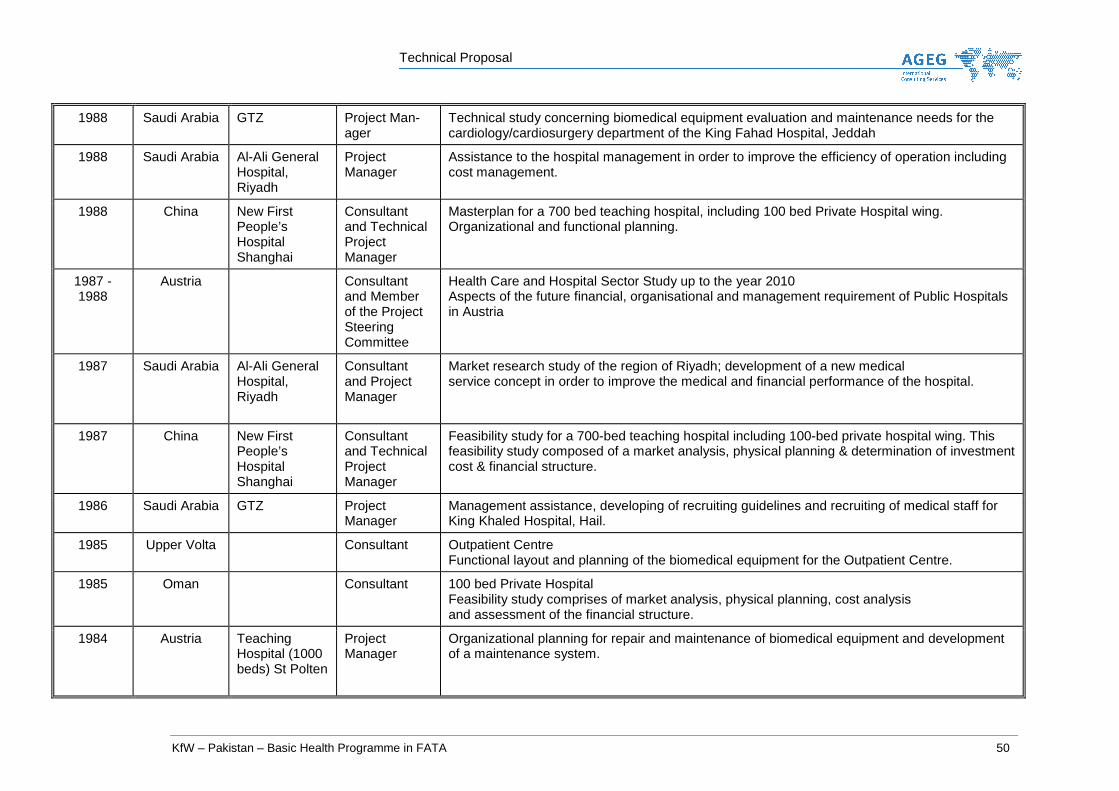
Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 50
1988 Saudi Arabia GTZ Project Man-ager
Technical study concerning biomedical equipment evaluation and maintenance needs for the cardiology/cardiosurgery department of the King Fahad Hospital, Jeddah
1988 Saudi Arabia Al-Ali General Hospital, Riyadh
Project Manager
Assistance to the hospital management in order to improve the efficiency of operation including cost management.
1988 China New First People’s Hospital Shanghai
Consultant and Technical Project Manager
Masterplan for a 700 bed teaching hospital, including 100 bed Private Hospital wing. Organizational and functional planning.
1987 - 1988
Austria Consultant and Member of the Project Steering Committee
Health Care and Hospital Sector Study up to the year 2010 Aspects of the future financial, organisational and management requirement of Public Hospitals in Austria
1987 Saudi Arabia Al-Ali General Hospital, Riyadh
Consultant and Project Manager
Market research study of the region of Riyadh; development of a new medical service concept in order to improve the medical and financial performance of the hospital.
1987 China New First People’s Hospital Shanghai
Consultant and Technical Project Manager
Feasibility study for a 700-bed teaching hospital including 100-bed private hospital wing. This feasibility study composed of a market analysis, physical planning & determination of investment cost & financial structure.
1986 Saudi Arabia GTZ Project Manager
Management assistance, developing of recruiting guidelines and recruiting of medical staff for King Khaled Hospital, Hail.
1985 Upper Volta Consultant Outpatient Centre Functional layout and planning of the biomedical equipment for the Outpatient Centre.
1985 Oman Consultant 100 bed Private Hospital Feasibility study comprises of market analysis, physical planning, cost analysis and assessment of the financial structure.
1984 Austria Teaching Hospital (1000 beds) St Polten
Project Manager
Organizational planning for repair and maintenance of biomedical equipment and development of a maintenance system.

Technical Proposal
KfW – Pakistan – Basic Health Programme in FATA 51
1984 Austria Industrial Medical Centre, Lenzing
Consultant Requirement assessment for medical and non-medical facilities, physical and organizational planning.
1983 Austria Regional Hospital Lilienfeld
Project Manager
• Requirement assessment with bed capacity evaluation • Supervision of the functional layout • Organizational planning for patient administration • Planning of nursing management and relevant documentation
1983 Austria Regional Hospital/Stockerau
Project Manager
• Supply analysis and determination of the capacity • Investigation concerning the comprehensive organizational and medical cooperation of hospitals • Organizational and structural planning • Physical and functional planning
1978 – 1982
Austria Gen Hospital Vienna/University Clinics (2,000 beds)
Supervisor Coordination, control and evaluation of all organizational and functional services, including cost analysis