Embed Size (px)
DESCRIPTION
James H Bates, MD Associate Professor, CWRU School of Medicine University Hospitals Case Medical Center É 100 minutes experimental complete occlusion in primates É Studies have used 20 hrs- too long É Platelet-fibrin emboli 15%? (TPA should work) É Cholesterol emboli 57-75%? (? Role for TPA) É Calcific emboli (aortic disease) 10%? (TPA worthless) Ò Retinal survival time Ò Lower IOP/dislodge Ò Hemodilution Ò Vasodilation É CO2 inhalation or nitrates
Citation preview

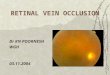
James H Bates, MDAssociate Professor, CWRU School of MedicineUniversity Hospitals Case Medical Center
Ò Occlusion of the central retinal artery at the lamina cribosa , thus causative material not seen in many cases É Platelet-fibrin emboli 15%? (TPA should work)É Cholesterol emboli 57-75%? (? Role for TPA)É Calcific emboli (aortic disease) 10%? (TPA worthless)
Ò Retinal survival timeÉ 100 minutes experimental complete occlusion in
primatesÉ Studies have used 20 hrs- too long


Ò Lower IOP/dislodgeÉGlaucoma dropsÉOcular massageÉ IV Acetazolamide or mannitolÉAnterior chamber paracentesis
Ò VasodilationÉCO2 inhalation or nitrates
Ò Hemodilution

Ò No controlled randomized trials of CRAO and its therapy
Ò Untreated may have 8% chance improvementÒ Conservative therapy may improve it to 15-60%Ò Prior therapy studies were retrospectiveÒ Testing (FA?), outcomes (Va, visual fields)Ò Diagnosing and excluding properly (cilioretinal
artery occlusion or sparing, arteritis)

Ò Therapeutic success may depend on earliest intervention possible
Ò What specialist makes the diagnosis of CRAO and by what means?
Ò How can the ophthalmologist be involved in timely care? Always on site vs telemedicine?
Ò Can ER, Neurology, Interventional Radiology specialists be trained to recognize the entity?

Ò 18/31 patients presented with CRAO within 20 hrs of vision loss
Ò 15/31 saw ophthalmologist within 20 hrs of vision loss, median 3.3 hours till seen
Ò Felt public awareness of entity and its urgency is low
Ò Urged direct referral line to ophthalmology

Ò Photos by Nurses using non-mydriatic cameraÒ Pts c HA, vision loss, neuro sx, diastolic >120Ò Compared to findings by ER doctorsÒ 200 enrolled pts so far- ER examined 33Ò By photos, 31 had urgent finding- ER found 1Ò ER not looking enough, low detection rateÒ ?telemedicine, ER photo training

Ò Review of 7/8 studies trended toward intrarterial therapy
Ò Improvements of vision may have been stat significant, but one line improvements are not a sign of success
Ò 5% adverse event rate cumulativeÒ Criticized studies for comparing heterogeneous
samples

Ò German prospective multicenter study intended to enroll 200 patients
Ò Stopped at 70 due to interim analysis showing no difference in aggressive conservative treatment and IAF
Ò Visual improvement seen in ~60% of both Ò 2 cerebral hemorrhages and overall 37% adverse
event with IAFÒ Criticized for questionable design and exclusion,
still may be best so far

Ò German Study 2008É50 mg rTPA IV over 1 hourÉ28 patients, no adverse eventsÉ32% had significant improvement (3 lines)É41% achieved better than 20/50 if treated within
6.5 hrs of vision loss (7/17)

Ò Illustrative of issues with therapy and studiesÒ 0.9 mg/kg for 1 hour p – CT head and INR<1.6Ò Enrolled 16 patients 8 treated/8 placeboÒ Intracerebral hemorrhage with 8th treated,
severe enough to require rehab, study haltedÒ Patients with less than 6 hours of loss showed
benefit, none over (small n though)Ò Will reconfigure study, shorter time to treat

Ò Natural history and Conservative therapy É poor studies, widely varying outcomes
Ò Interventional with TPAÉSelective intra-arterial by EAGLE is not supportedÉ IV is not clear, but EAGLE conservative is better
Ò Best to do under research protocol, not cowboying it
Ò Time window, complexity of disease, risks may be insurmountable

Ò Exclude patients with vision loss over 6 hoursÒ Devise system that can make a diagnosis
within that time frameÉ Training of non-ophthalmologistsÉ Telemedicine using fundus images
Ò Better studies with intra-arterial vs low-dose IVÒ If benefit found, patient education to drive
treatable patients for therapy

Ò Rudkin, A. K; Lee, A. W.; Chen, C. S. Central retinal artery occlusion: timing and mode of presentation European Journal of Neurology, Volume 16, Number 6, June 2009, pp. 674-677(4)
Ò J Noble, N Weizblit, M O Baerlocher, K T Eng Intra-arterial thrombolysis for central retinal artery occlusion: a systematic review Br J Ophthalmol 2008;92:588-593
Ò Schumacher et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010 Jul;117(7):1367-75. (EAGLE study)
Ò Hattenbach LO, Kuhli-Hattenbach C, Scharrer I, Baatz H. Intravenous thrombolysis with low-dose recombinant tissue plasminogen activator in central retinal artery occlusion Am J Ophthalmol. 2008;146:700-706
Ò Digital Ocular Fundus Photography in the Emergency Department: A New Application for Telemedicine? ClinicalTrials.gov identifier: NCT00873613
Ò Australian Flinders IV study, personal communication with Celia Chen, MD (Ophthalmology)