Embed Size (px)
Citation preview
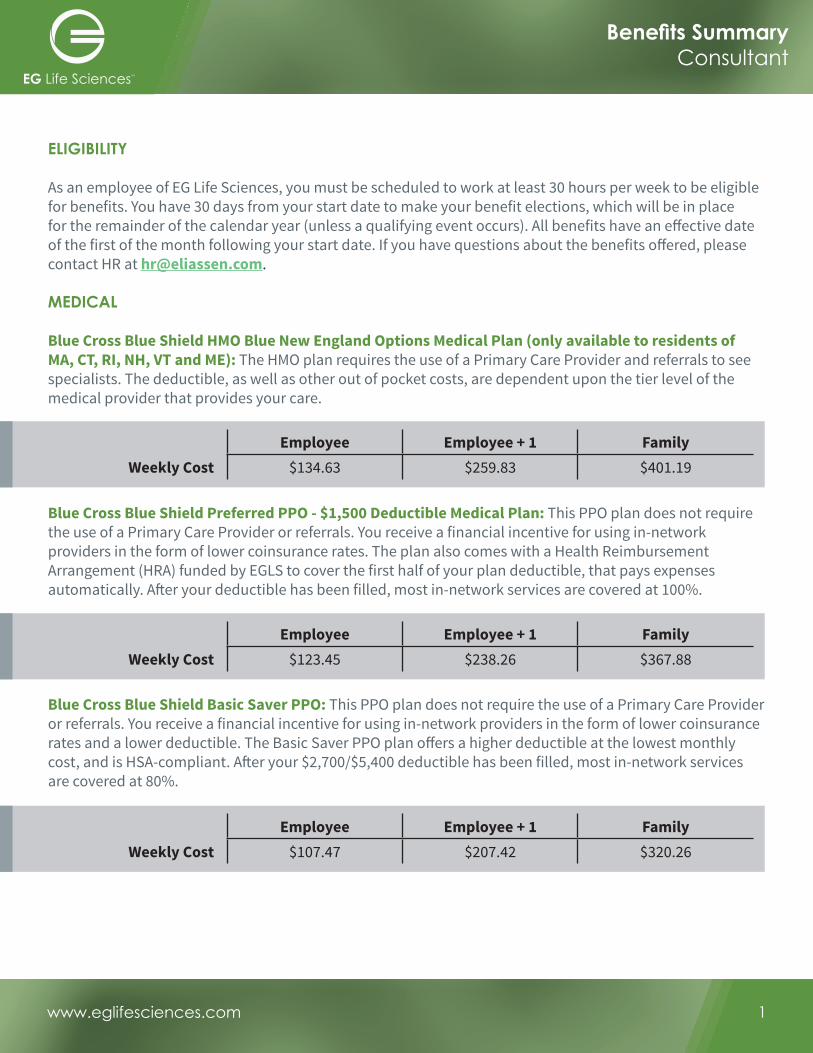
ELIGIBILITY
As an employee of EG Life Sciences, you must be scheduled to work at least 30 hours per week to be eligible for benefits. You have 30 days from your start date to make your benefit elections, which will be in place for the remainder of the calendar year (unless a qualifying event occurs). All benefits have an e� ective date of the first of the month following your start date. If you have questions about the benefits o� ered, please contact HR at [email protected].
MEDICAL
Blue Cross Blue Shield HMO Blue New England Options Medical Plan (only available to residents of MA, CT, RI, NH, VT and ME): The HMO plan requires the use of a Primary Care Provider and referrals to see specialists. The deductible, as well as other out of pocket costs, are dependent upon the tier level of the medical provider that provides your care.
Blue Cross Blue Shield Preferred PPO - $1,500 Deductible Medical Plan: This PPO plan does not require the use of a Primary Care Provider or referrals. You receive a financial incentive for using in-network providers in the form of lower coinsurance rates. The plan also comes with a Health Reimbursement Arrangement (HRA) funded by EGLS to cover the first half of your plan deductible, that pays expenses automatically. A� er your deductible has been filled, most in-network services are covered at 100%.
Blue Cross Blue Shield Basic Saver PPO: This PPO plan does not require the use of a Primary Care Provider or referrals. You receive a financial incentive for using in-network providers in the form of lower coinsurance rates and a lower deductible. The Basic Saver PPO plan o� ers a higher deductible at the lowest monthly cost, and is HSA-compliant. A� er your $2,700/$5,400 deductible has been filled, most in-network services are covered at 80%.
Employee Employee + 1 FamilyWeekly Cost $134.63 $259.83 $401.19
Employee Employee + 1 FamilyWeekly Cost $123.45 $238.26 $367.88
Employee Employee + 1 FamilyWeekly Cost $107.47 $207.42 $320.26
www.eglifesciences.com 1
Benefi ts SummaryConsultant

DENTAL
Blue Cross Blue Shield Dental Blue: The BCBS dental plans allow you to use any dentist that you wish. The Low Plan has a $1,000 annual maximum per person covered under the plan, and the High Plan has a $1,500 annual maximum per person covered under the plan.
VISION
Eyemed Insight: The EyeMed plan provides for annual eye exams and lenses for a $10 copay, and a generous allowance for frames and contacts when using in-network providers.
FLEXIBLE SPENDING ACCOUNTS (FSA)
FSAs allow you to make pre-tax contributions on a per pay period basis toward everyday expenses. This allows you to lower your taxable income. Any money that you contribute to the account that you do not have reimbursed to you is lost, so please estimate your contributions very carefully. For more information on the FSA programs, please contact HR.
Type of Account Eligible Expenses Maximum
Medical FSAOut of pocket medical costs (Rx copays, doctor’s o� ice copays, dental work, glasses, etc.)*
$2,600 per year
Dependent Care FSA Eligible daycare and elder care expenses*
$5,000 per year (or $2,500 per spouse if both are contibuting)
Parking FSA Work-related parking expenses* $255 per month (can be changed on a monthly basis)
Transit FSA Work-related public transportation expenses*
$255 per month (can be changed on a monthly basis)
Employee EE & Spouse/DP EE & Child(ren) FamilyWeekly Cost $1.50 $2.85 $3.01 $4.41
*All FSA claims must be filed within 2.5 months of the end of the plan year or within 60 days of separation from the company.
www.eglifesciences.com 2
Benefi ts SummaryConsultant
Employee EE & Spouse/DP EE & Child(ren) Family$11.62 $23.23 $23.00 $33.91$12.31 $24.63 $24.38 $35.95
Weekly Cost:Low Plan
Weekly Cost:High Plan

FIDELITY INVESTMENTS 401(K) PLAN
EG Life Sciences is proud to partner with Fidelity Investments to provide you with the opportunity to save for your retirement on both a pre-tax and a post-tax, Roth basis. You are eligible to participate in the 401(k) plan beginning the fi rst of the month following your start date. You can enroll in the 401(k) plan at any time – it does not have to be done during the fi rst 30 days of your employment. Please see below for details.
Plan Feature Details
Contribution Amounts Minimum: 1% of pay, Maximum: 90% of pay up to the annual IRS maximum; Contributions may be stopped at any time
Investment Options The EGLS plan o� ers over 30 di� erent investment options, including target date funds; investments can be managed online
Catch-Up ContributionsParticipants age 50 and over by 12/31 of the relevant plan year will be allowed to make a catch-up contribution up to the amount determined by the IRS; please contact HR to authorize these contributions
401(k) MatchEGLS will match 50% of the first $1,500 that you contribute to your own account each calendar year; you must work 1,000 hours in the calendar year to be eligible to receive the match
Vesting Schedule• Year 1 – 0% vested• Year 2 – 50% vested• Year 3 – 100% vested
www.eglifesciences.com 3
Benefi ts SummaryConsultant

1 of 9
HMO Blue New England Options Deductible v.5 Eliassen Group LLC Coverage Period: on or after 01/01/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family | Plan Type: HMO Tiered
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association
Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view theGlossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 to request a copy.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bluecrossma.com/coverage-info or by calling 1-800-358-2227.
Important Questions Answers Why this Matters:What is the overall deductible? $0 See the chart starting on page 2 for your costs for services this plan covers.
Are there other deductibles for specific services?
Yes, for services at a general hospital; $500 member / $1,000 family Standard Benefits Tier; $2,000 member / $4,000 family Basic Benefits Tier. There are no other specific deductibles.
You must pay all of the costs for these services up to the specific deductible amount before this plan begins to pay for these services.
Is there an out–of–pocket limit on my expenses?
Yes. For medical benefits, $5,450 member / $10,900 family; and for prescription drug benefits, $1,000 member / $2,000 family.
The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out–of–pocket limit?
Premiums, balance-billed charges, and health care this plan doesn't cover.
Even though you pay these expenses, they don’t count toward the out-of-pocket limit.
Does this plan use a network of providers?
Yes. See www.bluecrossma.com/findadoctor or call 1-800-821-1388 for a list of network providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? Yes.
This plan will pay some or all of the costs to see a specialist for covered services but only if you have the plan’s permission before you see the specialist.
Are there services this plan doesn’t cover? Yes.
Some of the services this plan doesn’t cover are listed on page 6. See your policy or plan document for additional information about excluded services.
2 of 9
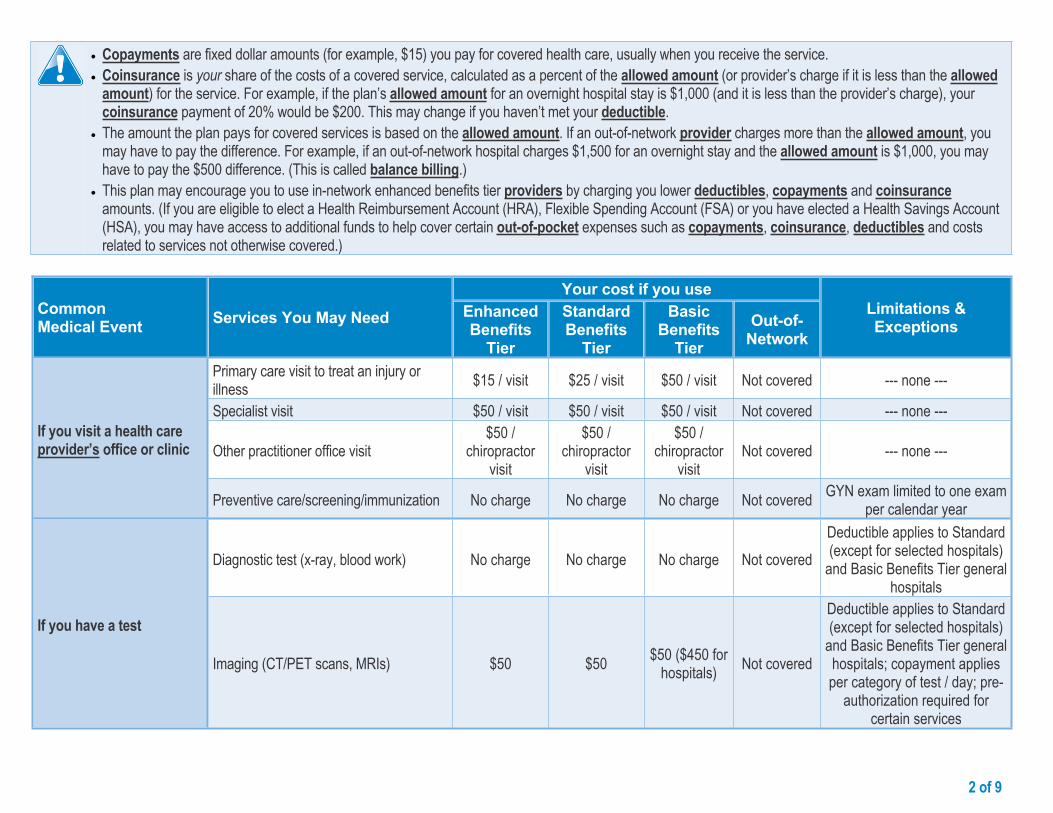
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount (or provider’s charge if it is less than the allowed
amount) for the service. For example, if the plan’s allowed amount for an overnight hospital stay is $1,000 (and it is less than the provider’s charge), your coinsurance payment of 20% would be $200. This may change if you haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use in-network enhanced benefits tier providers by charging you lower deductibles, copayments and coinsurance amounts. (If you are eligible to elect a Health Reimbursement Account (HRA), Flexible Spending Account (FSA) or you have elected a Health Savings Account (HSA), you may have access to additional funds to help cover certain out-of-pocket expenses such as copayments, coinsurance, deductibles and costs related to services not otherwise covered.)
Your cost if you useCommon Medical Event Services You May Need Enhanced
Benefits Tier
Standard Benefits
Tier
Basic Benefits
TierOut-of-
Network
Limitations & Exceptions
Primary care visit to treat an injury or illness $15 / visit $25 / visit $50 / visit Not covered --- none ---
Specialist visit $50 / visit $50 / visit $50 / visit Not covered --- none ---
Other practitioner office visit$50 /
chiropractor visit
$50 / chiropractor
visit
$50 / chiropractor
visitNot covered --- none ---
If you visit a health care provider’s office or clinic
Preventive care/screening/immunization No charge No charge No charge Not covered GYN exam limited to one exam per calendar year
Diagnostic test (x-ray, blood work) No charge No charge No charge Not coveredDeductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals
If you have a test
Imaging (CT/PET scans, MRIs) $50 $50 $50 ($450 for hospitals) Not covered
Deductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals; copayment applies per category of test / day; pre-
authorization required for certain services

3 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
Enhanced Benefits
Tier
Standard Benefits
Tier
Basic Benefits
TierOut-of-
Network
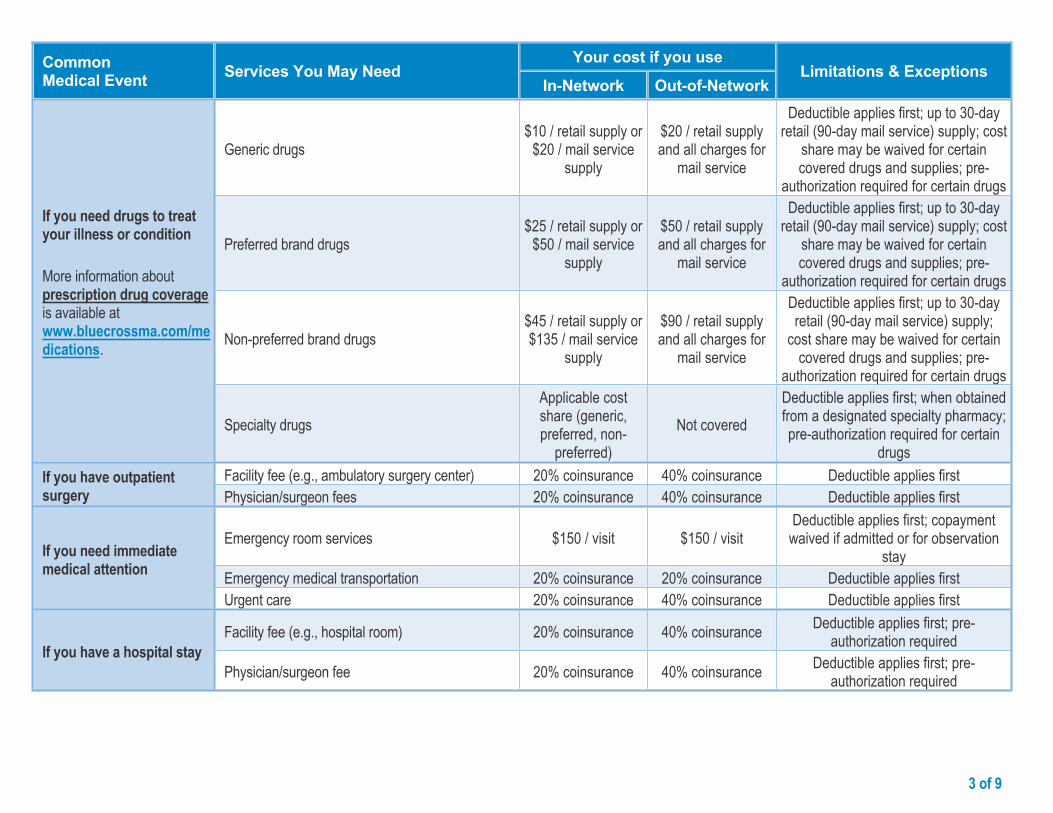
Generic drugs$15 / retail
supply or $30 / mail service
supply
$15 / retail supply or $30 /
mail service supply
$15 / retail supply or $30 / mail service
supplyNot covered
Up to 30-day retail (90-day mail service) supply; cost share may be waived for
certain covered drugs and supplies; pre-authorization required for certain drugs
Preferred brand drugs$30 / retail
supply or $60 / mail service
supply
$30 / retail supply or $60 /
mail service supply
$30 / retail supply or $60 / mail service
supplyNot covered
Up to 30-day retail (90-day mail service) supply; cost share may be waived for
certain covered drugs and supplies; pre-authorization required for certain drugs
Non-preferred brand drugs$50 / retail
supply or $150 / mail service
supply
$50 / retail supply or $150 / mail service
supply
$50 / retail supply or
$150 / mail service supply
Not covered
Up to 30-day retail (90-day mail service) supply; cost share may be waived for
certain covered drugs and supplies; pre-authorization required for certain drugs
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.bluecrossma.com/medications.
Specialty drugs
Applicable cost share (generic, preferred,
non-preferred)
Applicable cost share (generic, preferred,
non-preferred)
Applicable cost share (generic, preferred,
non-preferred)
Not coveredWhen obtained from a designated specialty
pharmacy; pre-authorization required for certain drugs
Facility fee (e.g., ambulatory surgery center)
$150 / admission
$150 / admission ($200 for selected hospitals)
$150 / admission ($1,000 for hospitals)
Not covered
Deductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals; pre-authorization required for certain services
If you have outpatient surgery
Physician/surgeon fees No charge No charge No charge Not covered Pre-authorization required for certain services
4 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
Enhanced Benefits
Tier
Standard Benefits
Tier
Basic Benefits
TierOut-of-
Network
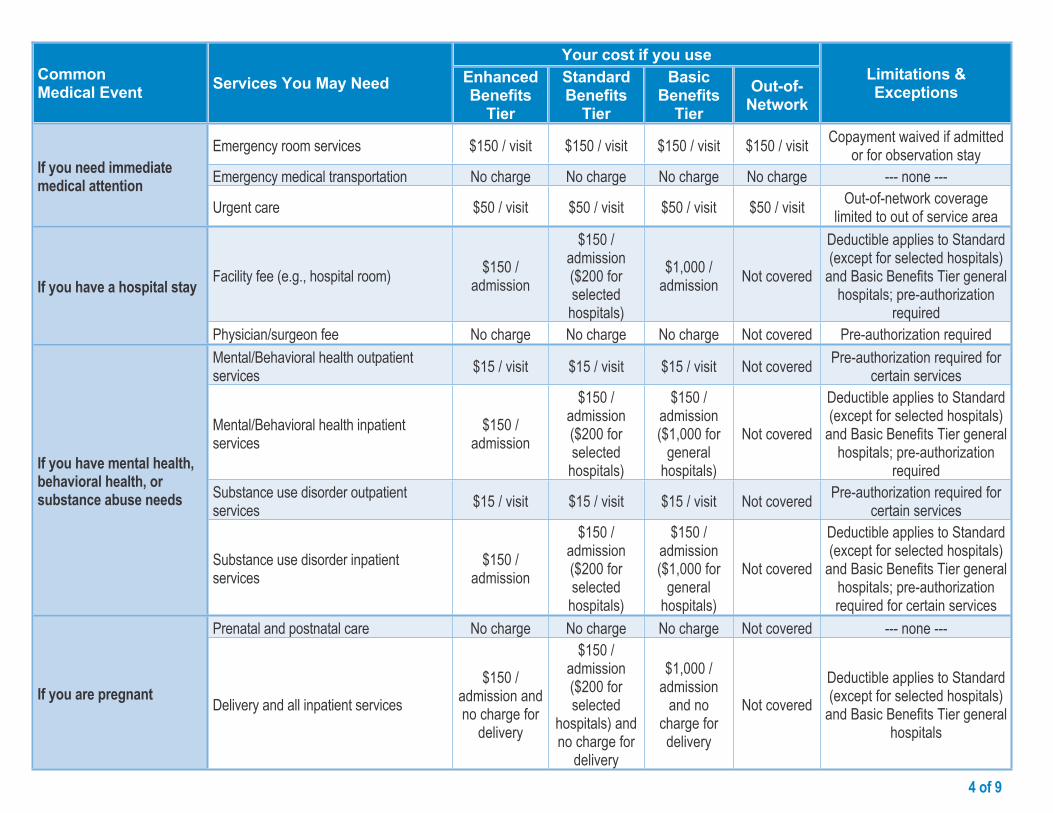
Emergency room services $150 / visit $150 / visit $150 / visit $150 / visit Copayment waived if admitted or for observation stay
Emergency medical transportation No charge No charge No charge No charge --- none ---If you need immediate medical attention
Urgent care $50 / visit $50 / visit $50 / visit $50 / visit Out-of-network coverage limited to out of service area
Facility fee (e.g., hospital room) $150 / admission
$150 / admission ($200 for selected hospitals)
$1,000 / admission Not covered
Deductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals; pre-authorization
requiredIf you have a hospital stay
Physician/surgeon fee No charge No charge No charge Not covered Pre-authorization requiredMental/Behavioral health outpatient services $15 / visit $15 / visit $15 / visit Not covered Pre-authorization required for
certain services
Mental/Behavioral health inpatient services
$150 / admission
$150 / admission ($200 for selected hospitals)
$150 / admission ($1,000 for
general hospitals)
Not covered
Deductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals; pre-authorization
requiredSubstance use disorder outpatient services $15 / visit $15 / visit $15 / visit Not covered Pre-authorization required for
certain services
If you have mental health, behavioral health, or substance abuse needs
Substance use disorder inpatient services
$150 / admission
$150 / admission ($200 for selected hospitals)
$150 / admission ($1,000 for
general hospitals)
Not covered
Deductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals; pre-authorization required for certain services
Prenatal and postnatal care No charge No charge No charge Not covered --- none ---
If you are pregnant Delivery and all inpatient services$150 /
admission and no charge for
delivery
$150 / admission ($200 for selected
hospitals) and no charge for
delivery
$1,000 / admission
and no charge for delivery
Not coveredDeductible applies to Standard (except for selected hospitals)
and Basic Benefits Tier general hospitals

5 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
Enhanced Benefits
Tier
Standard Benefits
Tier
Basic Benefits
TierOut-of-
Network
Home health care No charge No charge No charge Not covered Pre-authorization required
Rehabilitation services$25 / visit 1-20; $50 / visit 21 or more
$25 / visit 1-20; $50 / visit 21 or more
$25 / visit 1-20; $50 / visit 21 or more
Not covered
Limited to 60 visits per calendar year (other than for
autism, home health care, and speech therapy); pre-
authorization required for certain services
Habilitation services$25 / visit 1-20; $50 / visit 21 or more
$25 / visit 1-20; $50 / visit 21 or more
$25 / visit 1-20; $50 / visit 21 or more
Not covered
Rehabilitation therapy coverage limits apply; cost share and coverage limits
waived for early intervention services for eligible children; pre-authorization required for
certain services
Skilled nursing care No charge No charge No charge Not coveredLimited to 100 days per
calendar year; pre-authorization required
Durable medical equipment No charge No charge No charge Not covered --- none ---
If you need help recovering or have other special health needs
Hospice service No charge No charge No charge Not covered Pre-authorization required for certain services
Eye exam No charge No charge No charge Not covered Limited to one exam every 24 months
Glasses Not covered Not covered Not covered Not covered --- none ---If your child needs dental or eye care
Dental check-up
No charge for members with a cleft palate /
cleft lip condition
No charge for members with a cleft palate /
cleft lip condition
No charge for members
with a cleft palate / cleft lip condition
Not covered Limited to members under age 18

6 of 9
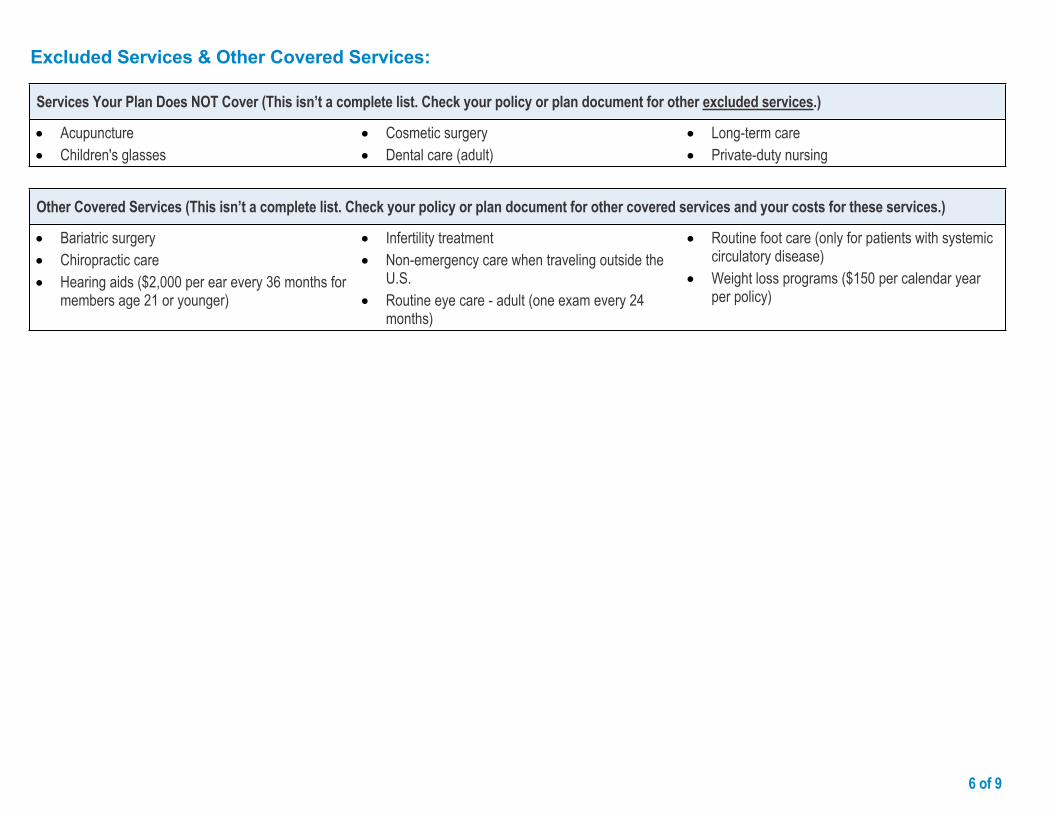
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Children's glasses Cosmetic surgery
Dental care (adult) Long-term care Non-emergency care when traveling outside the
U.S.
Private-duty nursing
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Bariatric surgery Chiropractic care Hearing aids ($2,000 per ear every 36 months for
members age 21 or younger)
Infertility treatment Routine eye care - adult (one exam every 24
months) Routine foot care (only for patients with systemic
circulatory disease)
Weight loss programs ($150 per calendar year per policy)

7 of 9
Your Rights to Continue Coverage:If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.For more information on your rights to continue coverage, contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights:If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact the Member Service number listed on your ID card or contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact The Office of Patient Protection at 1‑800-436-7757 or www.mass.gov/hpc/opp.
Does this Coverage Provide Minimum Essential Coverage?The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard?The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Disclaimer:This document contains only a partial description of the benefits, limitations, exclusions and other provisions of this health care plan. It is not a policy. It is a general overview only. It does not provide all the details of this coverage, including benefits, exclusions and policy limitations. In the event there are discrepancies between this document and the policy, the terms and conditions of the policy will govern.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

8 of 9
Having a baby(normal delivery)
Managing type 2 diabetes(routine maintenance of
a well-controlled condition)
About these Coverage Examples:
These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $6,720 Patient pays $820
Sample care costs:Hospital charges (mother) $2,700Routine obstetric care $2,100Hospital charges (baby) $900Anesthesia $900Laboratory tests $500Prescriptions $200Radiology $200Vaccines, other preventive $40Total $7,540
Patient pays:Deductibles $500Copays $170Coinsurance $0Limits or exclusions $150Total $820
Amount owed to providers: $5,400 Plan pays $4,060 Patient pays $1,340
Sample care costs:Prescriptions $2,900Medical Equipment and Supplies $1,300Office Visits and Procedures $700Education $300Laboratory tests $100Vaccines, other preventive $100Total $5,400
Patient pays:Deductibles $0Copays $1,260Coinsurance $0Limits or exclusions $80Total $1,340
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.
9 of 9Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You canview the Glossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 to request a copy.
® Registered Marks of the Blue Cross and Blue Shield Association.© 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
167788BS3711877
Questions and answers about the Coverage Examples:What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S. Department of Health and Human Services, and aren’t specific to a particular geographic area or health plan.
The patient’s condition was not an excluded or preexisting condition.
All services and treatments started and ended in the same coverage period.
There are no other medical expenses for any member covered under this plan.
Out-of-pocket expenses are based only on treating the condition in the example.
The patient received all care from standard benefits tier providers. If the patient had received care from other in-network or out-of-network providers, costs would have been different.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples. The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not cost estimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary of Benefits and Coverage for other plans, you’ll find the same Coverage Examples. When you compare plans, check the “Patient Pays” box in each example. The smaller that number, the more coverage the plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you’ll pay in out-of-pocket costs, such as copayments, deductibles, and coinsurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses.
MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 158485MB 55-0647 (2/16)
This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect January 1, 2014, as part of the Massachusetts Health Care Reform Law.

Information About the Plan
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 158488MB 55-1252 (2/16)
This health plan includes a tiered provider network called HMO Blue New England Options v.5. Members in this plan pay different levels of cost share (copayments, coinsurance, and/or deductibles) depending on the benefts tier of the provider furnishing the services. A provider’s benefts tier may change. Overall changes to the benefts tiers of providers will happen no more than once each calendar year. For help in fnding the benefts tier of a provider, visit the online provider search tool at www.bluecrossma.com/fndadoctor and search for HMO Blue New England Options v.5.

Nondiscrimination Notice
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164264M 55-1487 (8/16)
Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. It does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Blue Cross Blue Shield of Massachusetts provides:
• Free aids and services to people with disabilities to communicate effectively with us, such as qualifed sign language interpreters and written information in other formats (large print or other formats).
• Free language services to people whose primary language is not English, such as qualifed interpreters and information written in other languages.
If you need these services, call Member Service at the number on your ID card.
If you believe that Blue Cross Blue Shield of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can fle a grievance with the Civil Rights Coordinator by mail at Civil Rights Coordinator, Blue Cross Blue Shield of Massachusetts, One Enterprise Drive, Quincy, MA 02171-2126; phone at 1-800-472-2689 (TTY: 711); fax at 1-617-246-3616; or email at [email protected].
If you need help fling a grievance, the Civil Rights Coordinator is available to help you.
You can also fle a civil rights complaint with the U.S. Department of Health and Human Services, Offce for Civil Rights online at ocrportal.hhs.gov; by mail at U.S. Department of Health and Human Services, 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201; by phone at 1-800-368-1019 or 1-800-537-7697 (TDD).
Complaint forms are available at hhs.gov.

Translation ResourcesProfciency of Language Assistance Services
Spanish/Español: ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que fgura en su tarjeta de identifcación (TTY: 711).
Portuguese/Português: ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711).
Chinese/简体中文: 注意:如果您讲中文,我们可向您免费提供语言协助服务。请拨打您 ID 卡上的号码联系会员服务部(TTY 号码:711)。
Haitian Creole/Kreyòl Ayisyen: ATANSYON: Si ou pale kreyòl ayisyen, sèvis asistans nan lang disponib pou ou gratis. Rele nimewo Sèvis Manm nan ki sou kat Idantitifkasyon w lan (Sèvis pou Malantandan TTY: 711).
Vietnamese/Tiếng Việt: LƯU Ý: Nếu quý vị nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ được cung cấp cho quý vị miễn phí. Gọi cho Dịch vụ Hội viên theo số trên thẻ ID của quý vị (TTY: 711).
Russian/Русский: ВНИМАНИЕ: если Вы говорите по-русски, Вы можете воспользоваться бесплатными услугами переводчика. Позвоните в отдел обслуживания клиентов по номеру, указанному в Вашей идентификационной карте (телетайп: 711).
Arabic/ةيب:انتباه: إذا كنت تتحدث اللغة العربية، فتتوفر خدمات الساعدة اللغوية مجانا بالنسبة لك. اتصل بخدمات العضاء عل الرقم الوجود عل بةاقة هويتك (جهاز الهاتف
.(711 :”TTY“ النص للصم والبكم
Mon-Khmer, Cambodian/ខមែរ: ការជនដណង៖ បរសនបរើអនកនយាយភាសា ខមែរ បសវាជនយភាសាឥតគតថលៃ គអាចរកបានសបរារអនក។ សមទរសពទបៅខនកបសវាសរាជកតាមបេបៅបេើរណណ សរាគា េលៃនររសអនក (TTY: 711)។
French/Français: ATTENTION : si vous parlez français, des services d’assistance linguistique sont disponibles gratuitement. Appelez le Service adhérents au numéro indiqué sur votre carte d’assuré (TTY : 711).
Italian/Italiano: ATTENZIONE: se parlate italiano, sono disponibili per voi servizi gratuiti di assistenza linguistica. Chiamate il Servizio per i membri al numero riportato sulla vostra scheda identifcativa (TTY: 711).
Korean/한국어: 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 귀하의 ID 카드에 있는 전화번호(TTY: 711)를 사용하여 회원 서비스에 전화하십시오.
Greek/λληνικά: ΠΡΟΣΟΧΗ: Εάν μιλάτε Ελληνικά, διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε την Υπηρεσία Εξυπηρέτησης Μελών στον αριθμό της κάρτας μέλους σας (ID Card) (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association

Polish/Polski: UWAGA: Osoby posługujące się językiem polskim mogą bezpłatnie skorzystać z pomocy językowej. Należy zadzwonić do Działu obsługi ubezpieczonych pod numer podany na identyfkatorze (TTY: 711).
Hindi/हिदी: धयान द: दद आप दिनददी बोलत ि, तो भयाषया सियातया सवयाए, आप क ललए नन:शलक उपलबध ि। सदस सवयाओ को आपक आई.डी. कयाडड पर ददए गए नबर पर कॉल कर (टदी.टदी.वयाई.: 711).
Gujarati/ગજરાતી: ધયાન આપો: જો તમ ગજરયાતી બોલતયા હો, તો તમન ભયાષયાકી સહયાતયા સવયાઓ વવનયા મલ ઉપલબધ છ. તમયારયા આઈડી કયાડડ પર આપલયા નબર પર Member Service ન કૉલ કરો (TTY: 711).
Tagalog/Tagalog: PAUNAWA: Kung nagsasalita ka ng wikang Tagalog, mayroon kang magagamit na mga libreng serbisyo para sa tulong sa wika. Tawagan ang Mga Serbisyo sa Miyembro sa numerong nasa iyong ID Card (TTY: 711).
Japanese/日本語: お知らせ:日本語をお話しになる方は無料の言語アシスタンスサービスをご利用いただけます。IDカードに記載の電話番号を使用してメンバーサービスまでお電話ください(TTY: 711)。
German/Deutsch: ACHTUNG: Wenn Sie Deutsche sprechen, steht Ihnen kostenlos fremdsprachliche Unterstützung zur Verfügung. Rufen Sie den Mitgliederdienst unter der Nummer auf Ihrer ID-Karte an (TTY: 711).
Persian/پارسیان:شناسایی کارت روی بر مندرج تلفن شمار گیرد. با می قرار شما اختیار در رایگان صورت ب بانی ز کمک شما فارسی است، خدمات بان ز توج: اگر
.(TTY: 711) ید بگیر اعضا« تماس بخش »خدمات با خود
Lao/ພາສາລາວ: ຂ ຄວນໃສໃຈ: ຖາເຈ າເວ າພາສາລາວໄດ, ມ ການບ ລ ການຊວຍເຫ ອດານພາສາໃຫທານໂດຍບ ເສຍຄາ. ໂທ ຫາ ຝາຍບ ລ ການສະ ມາ ຊ ກທ ໝາຍເລກໂທລະສບຢໃນບດຂອງທານ (TTY: 711).
Navajo/Diné Bizaad: BAA !KOHWIINDZIN DOO&G&: Din4 k’ehj7 y1n7[t’i’go saad bee y1t’i’ 47 t’11j77k’e bee n7k1’a’doowo[go 47 n1’ahoot’i’. D77 bee an7tah7g7 ninaaltsoos bine’d44’ n0omba bik1’7g7ij8’ b44sh bee hod77lnih (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164711MB 55-1493 (8/16)

1 of 9
Preferred Blue PPO Saver $1500 Eliassen Group LLC Coverage Period: on or after 01/01/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family | Plan Type: PPO
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association ssociaion
Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 to request a copy.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bluecrossma.com/coverage-info or by calling 1-800-358-2227.
Important Questions Answers Why this Matters:
What is the overall deductible?
$1,500 individual contract / $3,000 family contract. Does not apply to in-network prenatal care; preventive care. The family deductible can be met by eligible costs incurred by any combination of members enrolled under the same family plan. But, the entire amount of the family deductible must be met before benefits will be provided for any one member.
You must pay all the costs up to the deductible amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the deductible starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the deductible.
Are there other deductibles for specific services?
No.You don’t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
Is there an out–of–pocket limit on my expenses?
Yes. $6,450 member / $12,900 family.The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out–of–pocket limit?
Premiums, balance-billed charges, and health care this plan doesn't cover.
Even though you pay these expenses, they don’t count toward the out-of-pocket limit.
Does this plan use a network of providers?
Yes. See www.bluecrossma.com/findadoctor or call 1-800-821-1388 for a list of preferred providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? No. You can see the specialist you choose without permission from this plan.
Are there services this plan doesn’t cover? Yes.
Some of the services this plan doesn’t cover are listed on page 6. See your policy or plan document for additional information about excluded services.

2 of 9
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount (or provider’s charge if it is less than the allowed
amount) for the service. For example, if the plan’s allowed amount for an overnight hospital stay is $1,000 (and it is less than the provider’s charge), your coinsurance payment of 20% would be $200. This may change if you haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use in-network providers by charging you lower deductibles, copayments and coinsurance amounts. (If you are eligible to elect a Health Reimbursement Account (HRA), Flexible Spending Account (FSA) or you have elected a Health Savings Account (HSA), you may have access to additional funds to help cover certain out-of-pocket expenses such as copayments, coinsurance, deductibles and costs related to services not otherwise covered.)
Your cost if you useCommon Medical Event Services You May Need
In-Network Out-of-NetworkLimitations & Exceptions
Primary care visit to treat an injury or illness No charge 20% coinsurance Deductible applies firstSpecialist visit No charge 20% coinsurance Deductible applies first
Other practitioner office visit No charge / chiropractor visit
20% coinsurance / chiropractor visit Deductible applies firstIf you visit a health care
provider’s office or clinic
Preventive care/screening/immunization No charge 20% coinsurance Limited to age-based schedule and / or frequency
Diagnostic test (x-ray, blood work) No charge 20% coinsurance Deductible applies firstIf you have a test Imaging (CT/PET scans, MRIs) No charge 20% coinsurance Deductible applies first

3 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
Generic drugs$10 / retail supply or
$20 / mail service supply
$20 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply; cost
share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
Preferred brand drugs$25 / retail supply or
$50 / mail service supply
$50 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply; cost
share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
Non-preferred brand drugs$45 / retail supply or $135 / mail service
supply
$90 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply;
cost share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.bluecrossma.com/medications.
Specialty drugs Applicable cost share (generic, preferred, non-
preferred)Not covered
Deductible applies first; when obtained from a designated specialty pharmacy; pre-authorization required for certain
drugsFacility fee (e.g., ambulatory surgery center) No charge 20% coinsurance Deductible applies firstIf you have outpatient
surgery Physician/surgeon fees No charge 20% coinsurance Deductible applies first
Emergency room services $150 / visit $150 / visitDeductible applies first; copayment waived if admitted or for observation
stayEmergency medical transportation No charge No charge Deductible applies first
If you need immediate medical attention
Urgent care No charge 20% coinsurance Deductible applies first
Facility fee (e.g., hospital room) No charge 20% coinsurance Deductible applies first; pre-authorization requiredIf you have a hospital stay
Physician/surgeon fee No charge 20% coinsurance Deductible applies first; pre-authorization required

4 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
Mental/Behavioral health outpatient services No charge 20% coinsuranceDeductible applies first; pre-
authorization required for certain services
Mental/Behavioral health inpatient services No charge 20% coinsurance Deductible applies first; pre-authorization required
Substance use disorder outpatient services No charge 20% coinsuranceDeductible applies first; pre-
authorization required for certain services
If you have mental health, behavioral health, or substance abuse needs
Substance use disorder inpatient services No charge 20% coinsuranceDeductible applies first; pre-
authorization required for certain services
Prenatal and postnatal care No charge 20% coinsuranceDeductible applies first for in-network
postnatal care and out-of-network prenatal and postnatal careIf you are pregnant
Delivery and all inpatient services No charge 20% coinsurance Deductible applies first
5 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
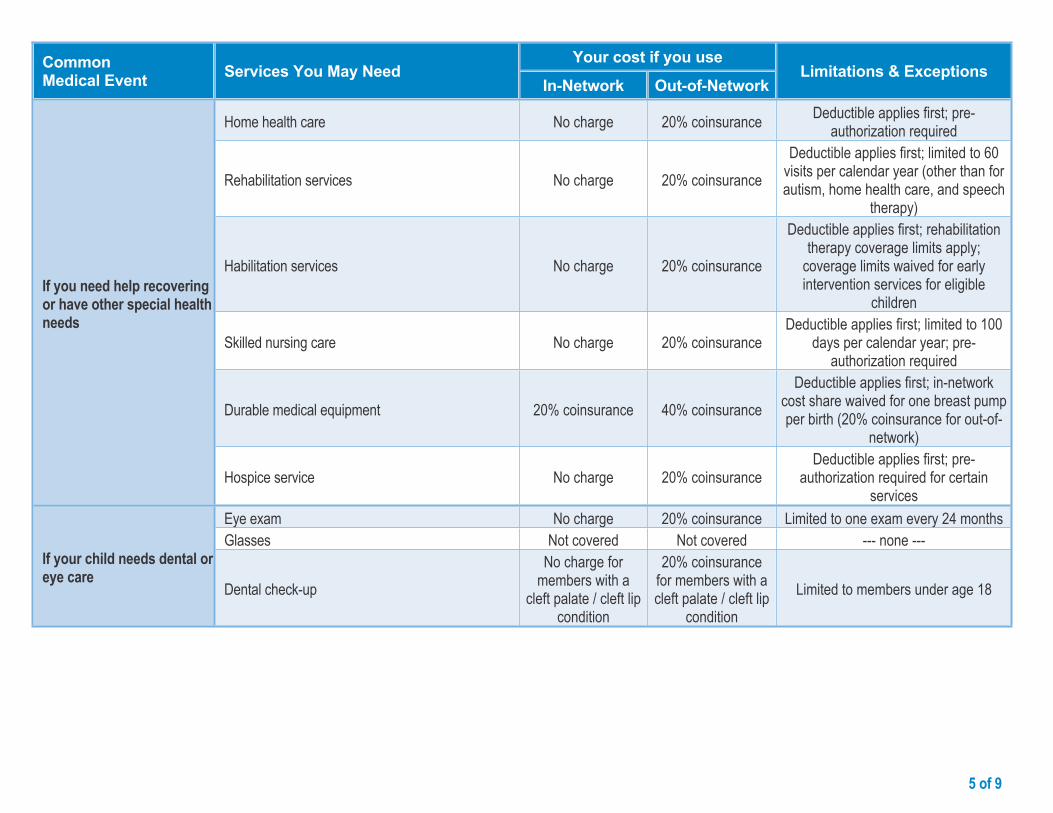
Home health care No charge 20% coinsurance Deductible applies first; pre-authorization required
Rehabilitation services No charge 20% coinsuranceDeductible applies first; limited to 60
visits per calendar year (other than for autism, home health care, and speech
therapy)
Habilitation services No charge 20% coinsurance
Deductible applies first; rehabilitation therapy coverage limits apply;
coverage limits waived for early intervention services for eligible
children
Skilled nursing care No charge 20% coinsuranceDeductible applies first; limited to 100
days per calendar year; pre-authorization required
Durable medical equipment 20% coinsurance 40% coinsuranceDeductible applies first; in-network
cost share waived for one breast pump per birth (20% coinsurance for out-of-
network)
If you need help recovering or have other special health needs
Hospice service No charge 20% coinsuranceDeductible applies first; pre-
authorization required for certain services
Eye exam No charge 20% coinsurance Limited to one exam every 24 monthsGlasses Not covered Not covered --- none ---
If your child needs dental or eye care
Dental check-upNo charge for
members with a cleft palate / cleft lip
condition
20% coinsurance for members with a cleft palate / cleft lip
conditionLimited to members under age 18

6 of 9
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Children's glasses
Cosmetic surgery Dental care (adult)
Long-term care Private-duty nursing
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Bariatric surgery Chiropractic care Hearing aids ($2,000 per ear every 36 months for
members age 21 or younger)
Infertility treatment Non-emergency care when traveling outside the
U.S. Routine eye care - adult (one exam every 24
months)
Routine foot care (only for patients with systemic circulatory disease)
Weight loss programs ($150 per calendar year per policy)

7 of 9
Your Rights to Continue Coverage:If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.For more information on your rights to continue coverage, contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights:If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact the Member Service number listed on your ID card or contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact The Office of Patient Protection at 1‑800-436-7757 or www.mass.gov/hpc/opp.
Does this Coverage Provide Minimum Essential Coverage?The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard?The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Disclaimer:This document contains only a partial description of the benefits, limitations, exclusions and other provisions of this health care plan. It is not a policy. It is a general overview only. It does not provide all the details of this coverage, including benefits, exclusions and policy limitations. In the event there are discrepancies between this document and the policy, the terms and conditions of the policy will govern.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

8 of 9
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.
Having a baby(normal delivery)
Managing type 2 diabetes(routine maintenance of
a well-controlled condition)
About these Coverage Examples:
These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $4,370 Patient pays $3,170
Sample care costs:Hospital charges (mother) $2,700Routine obstetric care $2,100Hospital charges (baby) $900Anesthesia $900Laboratory tests $500Prescriptions $200Radiology $200Vaccines, other preventive $40Total $7,540
Patient pays:Deductibles $3,000Copays $20Coinsurance $0Limits or exclusions $150Total $3,170
Amount owed to providers: $5,400 Plan pays $1,440 Patient pays $3,960
Sample care costs:Prescriptions $2,900Medical Equipment and Supplies $1,300Office Visits and Procedures $700Education $300Laboratory tests $100Vaccines, other preventive $100Total $5,400
Patient pays:Deductibles $3,000Copays $880Coinsurance $0Limits or exclusions $80Total $3,960

9 of 9Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You canview the Glossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 torequest a copy.
® Registered Marks of the Blue Cross and Blue Shield Association.© 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
167795BS3712955
Questions and answers about the Coverage Examples:What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S. Department of Health and Human Services, and aren’t specific to a particular geographic area or health plan.
The patient’s condition was not an excluded or preexisting condition.
All services and treatments started and ended in the same coverage period.
There are no other medical expenses for any member covered under this plan.
Out-of-pocket expenses are based only on treating the condition in the example.
The patient received all care from in-network providers. If the patient had received care from out-of-network providers, costs would have been higher.
The patient is enrolled in a family contract.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples. The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not cost estimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary of Benefits and Coverage for other plans, you’ll find the same Coverage Examples. When you compare plans, check the “Patient Pays” box in each example. The smaller that number, the more coverage the plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you’ll pay in out-of-pocket costs, such as copayments, deductibles, and coinsurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses.
MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 158485MB 55-0647 (2/16)
This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect January 1, 2014, as part of the Massachusetts Health Care Reform Law.

Nondiscrimination Notice
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164264M 55-1487 (8/16)
Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. It does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Blue Cross Blue Shield of Massachusetts provides:
• Free aids and services to people with disabilities to communicate effectively with us, such as qualifed sign language interpreters and written information in other formats (large print or other formats).
• Free language services to people whose primary language is not English, such as qualifed interpreters and information written in other languages.
If you need these services, call Member Service at the number on your ID card.
If you believe that Blue Cross Blue Shield of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can fle a grievance with the Civil Rights Coordinator by mail at Civil Rights Coordinator, Blue Cross Blue Shield of Massachusetts, One Enterprise Drive, Quincy, MA 02171-2126; phone at 1-800-472-2689 (TTY: 711); fax at 1-617-246-3616; or email at [email protected].
If you need help fling a grievance, the Civil Rights Coordinator is available to help you.
You can also fle a civil rights complaint with the U.S. Department of Health and Human Services, Offce for Civil Rights online at ocrportal.hhs.gov; by mail at U.S. Department of Health and Human Services, 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201; by phone at 1-800-368-1019 or 1-800-537-7697 (TDD).
Complaint forms are available at hhs.gov.

Translation ResourcesProfciency of Language Assistance Services
Spanish/Español: ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que fgura en su tarjeta de identifcación (TTY: 711).
Portuguese/Português: ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711).
Chinese/简体中文: 注意:如果您讲中文,我们可向您免费提供语言协助服务。请拨打您 ID 卡上的号码联系会员服务部(TTY 号码:711)。
Haitian Creole/Kreyòl Ayisyen: ATANSYON: Si ou pale kreyòl ayisyen, sèvis asistans nan lang disponib pou ou gratis. Rele nimewo Sèvis Manm nan ki sou kat Idantitifkasyon w lan (Sèvis pou Malantandan TTY: 711).
Vietnamese/Tiếng Việt: LƯU Ý: Nếu quý vị nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ được cung cấp cho quý vị miễn phí. Gọi cho Dịch vụ Hội viên theo số trên thẻ ID của quý vị (TTY: 711).
Russian/Русский: ВНИМАНИЕ: если Вы говорите по-русски, Вы можете воспользоваться бесплатными услугами переводчика. Позвоните в отдел обслуживания клиентов по номеру, указанному в Вашей идентификационной карте (телетайп: 711).
Arabic/ةيب:انتباه: إذا كنت تتحدث اللغة العربية، فتتوفر خدمات الساعدة اللغوية مجانا بالنسبة لك. اتصل بخدمات العضاء عل الرقم الوجود عل بةاقة هويتك (جهاز الهاتف
.(711 :”TTY“ النص للصم والبكم
Mon-Khmer, Cambodian/ខមែរ: ការជនដណង៖ បរសនបរើអនកនយាយភាសា ខមែរ បសវាជនយភាសាឥតគតថលៃ គអាចរកបានសបរារអនក។ សមទរសពទបៅខនកបសវាសរាជកតាមបេបៅបេើរណណ សរាគា េលៃនររសអនក (TTY: 711)។
French/Français: ATTENTION : si vous parlez français, des services d’assistance linguistique sont disponibles gratuitement. Appelez le Service adhérents au numéro indiqué sur votre carte d’assuré (TTY : 711).
Italian/Italiano: ATTENZIONE: se parlate italiano, sono disponibili per voi servizi gratuiti di assistenza linguistica. Chiamate il Servizio per i membri al numero riportato sulla vostra scheda identifcativa (TTY: 711).
Korean/한국어: 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 귀하의 ID 카드에 있는 전화번호(TTY: 711)를 사용하여 회원 서비스에 전화하십시오.
Greek/λληνικά: ΠΡΟΣΟΧΗ: Εάν μιλάτε Ελληνικά, διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε την Υπηρεσία Εξυπηρέτησης Μελών στον αριθμό της κάρτας μέλους σας (ID Card) (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association

Polish/Polski: UWAGA: Osoby posługujące się językiem polskim mogą bezpłatnie skorzystać z pomocy językowej. Należy zadzwonić do Działu obsługi ubezpieczonych pod numer podany na identyfkatorze (TTY: 711).
Hindi/हिदी: धयान द: दद आप दिनददी बोलत ि, तो भयाषया सियातया सवयाए, आप क ललए नन:शलक उपलबध ि। सदस सवयाओ को आपक आई.डी. कयाडड पर ददए गए नबर पर कॉल कर (टदी.टदी.वयाई.: 711).
Gujarati/ગજરાતી: ધયાન આપો: જો તમ ગજરયાતી બોલતયા હો, તો તમન ભયાષયાકી સહયાતયા સવયાઓ વવનયા મલ ઉપલબધ છ. તમયારયા આઈડી કયાડડ પર આપલયા નબર પર Member Service ન કૉલ કરો (TTY: 711).
Tagalog/Tagalog: PAUNAWA: Kung nagsasalita ka ng wikang Tagalog, mayroon kang magagamit na mga libreng serbisyo para sa tulong sa wika. Tawagan ang Mga Serbisyo sa Miyembro sa numerong nasa iyong ID Card (TTY: 711).
Japanese/日本語: お知らせ:日本語をお話しになる方は無料の言語アシスタンスサービスをご利用いただけます。IDカードに記載の電話番号を使用してメンバーサービスまでお電話ください(TTY: 711)。
German/Deutsch: ACHTUNG: Wenn Sie Deutsche sprechen, steht Ihnen kostenlos fremdsprachliche Unterstützung zur Verfügung. Rufen Sie den Mitgliederdienst unter der Nummer auf Ihrer ID-Karte an (TTY: 711).
Persian/پارسیان:شناسایی کارت روی بر مندرج تلفن شمار گیرد. با می قرار شما اختیار در رایگان صورت ب بانی ز کمک شما فارسی است، خدمات بان ز توج: اگر
.(TTY: 711) ید بگیر اعضا« تماس بخش »خدمات با خود
Lao/ພາສາລາວ: ຂ ຄວນໃສໃຈ: ຖາເຈ າເວ າພາສາລາວໄດ, ມ ການບ ລ ການຊວຍເຫ ອດານພາສາໃຫທານໂດຍບ ເສຍຄາ. ໂທ ຫາ ຝາຍບ ລ ການສະ ມາ ຊ ກທ ໝາຍເລກໂທລະສບຢໃນບດຂອງທານ (TTY: 711).
Navajo/Diné Bizaad: BAA !KOHWIINDZIN DOO&G&: Din4 k’ehj7 y1n7[t’i’go saad bee y1t’i’ 47 t’11j77k’e bee n7k1’a’doowo[go 47 n1’ahoot’i’. D77 bee an7tah7g7 ninaaltsoos bine’d44’ n0omba bik1’7g7ij8’ b44sh bee hod77lnih (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164711MB 55-1493 (8/16)
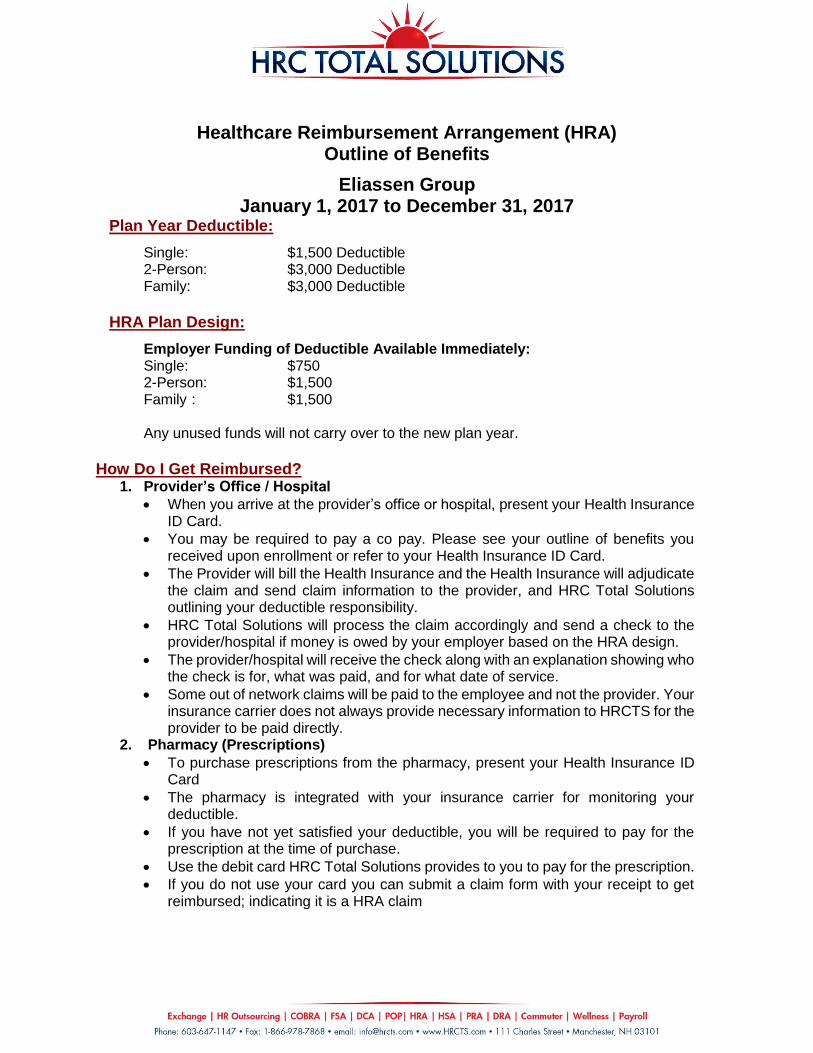
Healthcare Reimbursement Arrangement (HRA) Outline of Benefits
Eliassen Group January 1, 2017 to December 31, 2017
Plan Year Deductible:
Single: $1,500 Deductible 2-Person: $3,000 Deductible Family: $3,000 Deductible
HRA Plan Design:
Employer Funding of Deductible Available Immediately: Single: $750 2-Person: $1,500 Family : $1,500 Any unused funds will not carry over to the new plan year.
How Do I Get Reimbursed?
1. Provider’s Office / Hospital
When you arrive at the provider’s office or hospital, present your Health Insurance ID Card.
You may be required to pay a co pay. Please see your outline of benefits you received upon enrollment or refer to your Health Insurance ID Card.
The Provider will bill the Health Insurance and the Health Insurance will adjudicate the claim and send claim information to the provider, and HRC Total Solutions outlining your deductible responsibility.
HRC Total Solutions will process the claim accordingly and send a check to the provider/hospital if money is owed by your employer based on the HRA design.
The provider/hospital will receive the check along with an explanation showing who the check is for, what was paid, and for what date of service.
Some out of network claims will be paid to the employee and not the provider. Your insurance carrier does not always provide necessary information to HRCTS for the provider to be paid directly.
2. Pharmacy (Prescriptions)
To purchase prescriptions from the pharmacy, present your Health Insurance ID Card
The pharmacy is integrated with your insurance carrier for monitoring your deductible.
If you have not yet satisfied your deductible, you will be required to pay for the prescription at the time of purchase.
Use the debit card HRC Total Solutions provides to you to pay for the prescription.
If you do not use your card you can submit a claim form with your receipt to get reimbursed; indicating it is a HRA claim

Frequently Asked Questions
What is an HRA? A Healthcare Reimbursement Arrangement-Typically, your employer provides a high deductible medical plan and establishes an HRA in your name to help pay for your eligible out-of-pocket medical expenses. The HRA is funded by your employer. You may not contribute to the funding of your HRA. An HRA is an IOU – you have no claim to the money unless you incur eligible expenses. Do I pay deductible expenses at the time of service?
In most cases, you will not need to pay at the time of the appointment for procedures that are subject to your deductible. Please contact your insurance carrier with further questions.
Prescriptions subject to your deductible are paid by your HRCTS card when purchased.
How do I know where I am in my deductible? Please contact your Health Insurance Carrier What expenses are eligible through my HRA? Deductible Expenses per summary of benefits provided by your health insurance carrier. How may I receive my reimbursement? Reimbursements for medical deductible expenses are sent directly to your provider/hospital after HRCTS processes the claim submitted via the weekly Claims File Feed submitted to HRCTS from your health insurance carrier. You should not have to submit a manual claim for reimbursement for any medical deductible expenses. Prescription deductible expenses should be paid using your HRCTS Visa Card or you may submit manually the receipt indicating the purchase and will be reimbursed via check or direct deposit according to the plan design outlined above. How do I know if a claim was received, processed and paid to my provider/hospital?
a) You can log onto the online account you set up to view the date the check was sent, how much the check was for as well as the address of the provider/hospital it was sent to.
b) You can call HRCTS Account Holder Services Monday-Friday 8:30am-7:30pm EST. at 603-647-1147 ext.1 or email [email protected] and request information on claims submitted to HRCTS from your health insurance carrier and were paid to your provider directly
What if Health Insurance Carrier reverses claim? HRCTS will be notified of reversal, the claim will be denied and you will receive a repayment request. You are responsible to remit the repayment amount to HRCTS. What if I receive a bill from my provider/hospital?
1. Your provider bill may not reflect the payment made by HRCTS if sent to you before they processed payment received.
2. Please refer to “How do I know if a claim was received, processed and paid to my provider/hospital?” above.
3. If check was issued for payment sent to provider and not reflected on your bill please contact your provider.

1 of 9
Preferred Blue PPO Saver $2700 Eliassen Group LLC Coverage Period: on or after 01/01/2017Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family | Plan Type: PPO
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association ssociaion
Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 to request a copy.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bluecrossma.com/coverage-info or by calling 1-800-358-2227.
Important Questions Answers Why this Matters:
What is the overall deductible?
$2,700 individual contract / $5,400 family contract. Does not apply to in-network prenatal care; preventive care. The family deductible can be met by eligible costs incurred by any combination of members enrolled under the same family plan. But, the entire amount of the family deductible must be met before benefits will be provided for any one member.
You must pay all the costs up to the deductible amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the deductible starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the deductible.
Are there other deductibles for specific services?
No.You don’t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
Is there an out–of–pocket limit on my expenses?
Yes. $6,450 member / $12,900 family.The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses.
What is not included in the out–of–pocket limit?
Premiums, balance-billed charges, and health care this plan doesn't cover.
Even though you pay these expenses, they don’t count toward the out-of-pocket limit.
Does this plan use a network of providers?
Yes. See www.bluecrossma.com/findadoctor or call 1-800-821-1388 for a list of preferred providers.
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist? No. You can see the specialist you choose without permission from this plan.
Are there services this plan doesn’t cover? Yes.
Some of the services this plan doesn’t cover are listed on page 6. See your policy or plan document for additional information about excluded services.

2 of 9
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount (or provider’s charge if it is less than the allowed
amount) for the service. For example, if the plan’s allowed amount for an overnight hospital stay is $1,000 (and it is less than the provider’s charge), your coinsurance payment of 20% would be $200. This may change if you haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use in-network providers by charging you lower deductibles, copayments and coinsurance amounts. (If you are eligible to elect a Health Reimbursement Account (HRA), Flexible Spending Account (FSA) or you have elected a Health Savings Account (HSA), you may have access to additional funds to help cover certain out-of-pocket expenses such as copayments, coinsurance, deductibles and costs related to services not otherwise covered.)
Your cost if you useCommon Medical Event Services You May Need
In-Network Out-of-NetworkLimitations & Exceptions
Primary care visit to treat an injury or illness 20% coinsurance 40% coinsurance Deductible applies firstSpecialist visit 20% coinsurance 40% coinsurance Deductible applies first
Other practitioner office visit 20% coinsurance / chiropractor visit
40% coinsurance / chiropractor visit Deductible applies firstIf you visit a health care
provider’s office or clinic
Preventive care/screening/immunization No charge 20% coinsurance Limited to age-based schedule and / or frequency
Diagnostic test (x-ray, blood work) 20% coinsurance 40% coinsurance Deductible applies firstIf you have a test Imaging (CT/PET scans, MRIs) 20% coinsurance 40% coinsurance Deductible applies first
3 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
Generic drugs$10 / retail supply or
$20 / mail service supply
$20 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply; cost
share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
Preferred brand drugs$25 / retail supply or
$50 / mail service supply
$50 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply; cost
share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
Non-preferred brand drugs$45 / retail supply or $135 / mail service
supply
$90 / retail supply and all charges for
mail service
Deductible applies first; up to 30-day retail (90-day mail service) supply;
cost share may be waived for certain covered drugs and supplies; pre-
authorization required for certain drugs
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.bluecrossma.com/medications.
Specialty drugs Applicable cost share (generic, preferred, non-
preferred)Not covered
Deductible applies first; when obtained from a designated specialty pharmacy; pre-authorization required for certain
drugsFacility fee (e.g., ambulatory surgery center) 20% coinsurance 40% coinsurance Deductible applies firstIf you have outpatient
surgery Physician/surgeon fees 20% coinsurance 40% coinsurance Deductible applies first
Emergency room services $150 / visit $150 / visitDeductible applies first; copayment waived if admitted or for observation
stayEmergency medical transportation 20% coinsurance 20% coinsurance Deductible applies first
If you need immediate medical attention
Urgent care 20% coinsurance 40% coinsurance Deductible applies first
Facility fee (e.g., hospital room) 20% coinsurance 40% coinsurance Deductible applies first; pre-authorization requiredIf you have a hospital stay
Physician/surgeon fee 20% coinsurance 40% coinsurance Deductible applies first; pre-authorization required

4 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
Mental/Behavioral health outpatient services 20% coinsurance 40% coinsuranceDeductible applies first; pre-
authorization required for certain services
Mental/Behavioral health inpatient services 20% coinsurance 40% coinsurance Deductible applies first; pre-authorization required
Substance use disorder outpatient services 20% coinsurance 40% coinsuranceDeductible applies first; pre-
authorization required for certain services
If you have mental health, behavioral health, or substance abuse needs
Substance use disorder inpatient services 20% coinsurance 40% coinsuranceDeductible applies first; pre-
authorization required for certain services
Prenatal and postnatal careNo charge for
prenatal care; 20% coinsurance for postnatal care
20% coinsurance for prenatal care; 40% coinsurance for postnatal care
Deductible applies first for in-network postnatal care and out-of-network
prenatal and postnatal careIf you are pregnant
Delivery and all inpatient services 20% coinsurance 40% coinsurance Deductible applies first

5 of 9
Common Medical Event Services You May Need
Your cost if you useLimitations & Exceptions
In-Network Out-of-Network
Home health care 20% coinsurance 40% coinsurance Deductible applies first; pre-authorization required
Rehabilitation services 20% coinsurance 40% coinsuranceDeductible applies first; limited to 60
visits per calendar year (other than for autism, home health care, and speech
therapy)
Habilitation services 20% coinsurance 40% coinsurance
Deductible applies first; rehabilitation therapy coverage limits apply;
coverage limits waived for early intervention services for eligible
children
Skilled nursing care 20% coinsurance 40% coinsuranceDeductible applies first; limited to 100
days per calendar year; pre-authorization required
Durable medical equipment 20% coinsurance 40% coinsuranceDeductible applies first; in-network
cost share waived for one breast pump per birth (20% coinsurance for out-of-
network)
If you need help recovering or have other special health needs
Hospice service 20% coinsurance 40% coinsuranceDeductible applies first; pre-
authorization required for certain services
Eye exam No charge 20% coinsurance Limited to one exam every 24 monthsGlasses Not covered Not covered --- none ---
If your child needs dental or eye care
Dental check-upNo charge for
members with a cleft palate / cleft lip
condition
20% coinsurance for members with a cleft palate / cleft lip
conditionLimited to members under age 18
6 of 9
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture Children's glasses
Cosmetic surgery Dental care (adult)
Long-term care Private-duty nursing
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
Bariatric surgery Chiropractic care Hearing aids ($2,000 per ear every 36 months for
members age 21 or younger)
Infertility treatment Non-emergency care when traveling outside the
U.S. Routine eye care - adult (one exam every 24
months)
Routine foot care (only for patients with systemic circulatory disease)
Weight loss programs ($150 per calendar year per policy)

7 of 9
Your Rights to Continue Coverage:If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.For more information on your rights to continue coverage, contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights:If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact the Member Service number listed on your ID card or contact your plan sponsor. Note: A plan sponsor is usually the member’s employer or organization that provides group health coverage to the member. You may also contact The Office of Patient Protection at 1‑800-436-7757 or www.mass.gov/hpc/opp.
Does this Coverage Provide Minimum Essential Coverage?The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard?The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides.
Disclaimer:This document contains only a partial description of the benefits, limitations, exclusions and other provisions of this health care plan. It is not a policy. It is a general overview only. It does not provide all the details of this coverage, including benefits, exclusions and policy limitations. In the event there are discrepancies between this document and the policy, the terms and conditions of the policy will govern.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

8 of 9
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.
Having a baby(normal delivery)
Managing type 2 diabetes(routine maintenance of
a well-controlled condition)
About these Coverage Examples:
These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays $3,750 Patient pays $3,790
Sample care costs:Hospital charges (mother) $2,700Routine obstetric care $2,100Hospital charges (baby) $900Anesthesia $900Laboratory tests $500Prescriptions $200Radiology $200Vaccines, other preventive $40Total $7,540
Patient pays:Deductibles $3,640Copays $0Coinsurance $0Limits or exclusions $150Total $3,790
Amount owed to providers: $5,400 Plan pays $50 Patient pays $5,350
Sample care costs:Prescriptions $2,900Medical Equipment and Supplies $1,300Office Visits and Procedures $700Education $300Laboratory tests $100Vaccines, other preventive $100Total $5,400
Patient pays:Deductibles $5,270Copays $0Coinsurance $0Limits or exclusions $80Total $5,350

9 of 9Questions: Call 1-800-358-2227 or visit us at www.bluecrossma.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You canview the Glossary at www.bluecrossma.com/sbcglossary or call 1-800-358-2227 torequest a copy.
® Registered Marks of the Blue Cross and Blue Shield Association.© 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
168041BS3719854
Questions and answers about the Coverage Examples:What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums. Sample care costs are based on national
averages supplied by the U.S. Department of Health and Human Services, and aren’t specific to a particular geographic area or health plan.
The patient’s condition was not an excluded or preexisting condition.
All services and treatments started and ended in the same coverage period.
There are no other medical expenses for any member covered under this plan.
Out-of-pocket expenses are based only on treating the condition in the example.
The patient received all care from in-network providers. If the patient had received care from out-of-network providers, costs would have been higher.
The patient is enrolled in a family contract.
What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples. The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not cost estimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary of Benefits and Coverage for other plans, you’ll find the same Coverage Examples. When you compare plans, check the “Patient Pays” box in each example. The smaller that number, the more coverage the plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you’ll pay in out-of-pocket costs, such as copayments, deductibles, and coinsurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses.

MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 158485MB 55-0647 (2/16)
This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect January 1, 2014, as part of the Massachusetts Health Care Reform Law.

Nondiscrimination Notice
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164264M 55-1487 (8/16)
Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. It does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Blue Cross Blue Shield of Massachusetts provides:
• Free aids and services to people with disabilities to communicate effectively with us, such as qualifed sign language interpreters and written information in other formats (large print or other formats).
• Free language services to people whose primary language is not English, such as qualifed interpreters and information written in other languages.
If you need these services, call Member Service at the number on your ID card.
If you believe that Blue Cross Blue Shield of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can fle a grievance with the Civil Rights Coordinator by mail at Civil Rights Coordinator, Blue Cross Blue Shield of Massachusetts, One Enterprise Drive, Quincy, MA 02171-2126; phone at 1-800-472-2689 (TTY: 711); fax at 1-617-246-3616; or email at [email protected].
If you need help fling a grievance, the Civil Rights Coordinator is available to help you.
You can also fle a civil rights complaint with the U.S. Department of Health and Human Services, Offce for Civil Rights online at ocrportal.hhs.gov; by mail at U.S. Department of Health and Human Services, 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201; by phone at 1-800-368-1019 or 1-800-537-7697 (TDD).
Complaint forms are available at hhs.gov.

Translation ResourcesProfciency of Language Assistance Services
Spanish/Español: ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que fgura en su tarjeta de identifcación (TTY: 711).
Portuguese/Português: ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711).
Chinese/简体中文: 注意:如果您讲中文,我们可向您免费提供语言协助服务。请拨打您 ID 卡上的号码联系会员服务部(TTY 号码:711)。
Haitian Creole/Kreyòl Ayisyen: ATANSYON: Si ou pale kreyòl ayisyen, sèvis asistans nan lang disponib pou ou gratis. Rele nimewo Sèvis Manm nan ki sou kat Idantitifkasyon w lan (Sèvis pou Malantandan TTY: 711).
Vietnamese/Tiếng Việt: LƯU Ý: Nếu quý vị nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ được cung cấp cho quý vị miễn phí. Gọi cho Dịch vụ Hội viên theo số trên thẻ ID của quý vị (TTY: 711).
Russian/Русский: ВНИМАНИЕ: если Вы говорите по-русски, Вы можете воспользоваться бесплатными услугами переводчика. Позвоните в отдел обслуживания клиентов по номеру, указанному в Вашей идентификационной карте (телетайп: 711).
Arabic/ةيب:انتباه: إذا كنت تتحدث اللغة العربية، فتتوفر خدمات الساعدة اللغوية مجانا بالنسبة لك. اتصل بخدمات العضاء عل الرقم الوجود عل بةاقة هويتك (جهاز الهاتف
.(711 :”TTY“ النص للصم والبكم
Mon-Khmer, Cambodian/ខមែរ: ការជនដណង៖ បរសនបរើអនកនយាយភាសា ខមែរ បសវាជនយភាសាឥតគតថលៃ គអាចរកបានសបរារអនក។ សមទរសពទបៅខនកបសវាសរាជកតាមបេបៅបេើរណណ សរាគា េលៃនររសអនក (TTY: 711)។
French/Français: ATTENTION : si vous parlez français, des services d’assistance linguistique sont disponibles gratuitement. Appelez le Service adhérents au numéro indiqué sur votre carte d’assuré (TTY : 711).
Italian/Italiano: ATTENZIONE: se parlate italiano, sono disponibili per voi servizi gratuiti di assistenza linguistica. Chiamate il Servizio per i membri al numero riportato sulla vostra scheda identifcativa (TTY: 711).
Korean/한국어: 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 귀하의 ID 카드에 있는 전화번호(TTY: 711)를 사용하여 회원 서비스에 전화하십시오.
Greek/λληνικά: ΠΡΟΣΟΧΗ: Εάν μιλάτε Ελληνικά, διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε την Υπηρεσία Εξυπηρέτησης Μελών στον αριθμό της κάρτας μέλους σας (ID Card) (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association

Polish/Polski: UWAGA: Osoby posługujące się językiem polskim mogą bezpłatnie skorzystać z pomocy językowej. Należy zadzwonić do Działu obsługi ubezpieczonych pod numer podany na identyfkatorze (TTY: 711).
Hindi/हिदी: धयान द: दद आप दिनददी बोलत ि, तो भयाषया सियातया सवयाए, आप क ललए नन:शलक उपलबध ि। सदस सवयाओ को आपक आई.डी. कयाडड पर ददए गए नबर पर कॉल कर (टदी.टदी.वयाई.: 711).
Gujarati/ગજરાતી: ધયાન આપો: જો તમ ગજરયાતી બોલતયા હો, તો તમન ભયાષયાકી સહયાતયા સવયાઓ વવનયા મલ ઉપલબધ છ. તમયારયા આઈડી કયાડડ પર આપલયા નબર પર Member Service ન કૉલ કરો (TTY: 711).
Tagalog/Tagalog: PAUNAWA: Kung nagsasalita ka ng wikang Tagalog, mayroon kang magagamit na mga libreng serbisyo para sa tulong sa wika. Tawagan ang Mga Serbisyo sa Miyembro sa numerong nasa iyong ID Card (TTY: 711).
Japanese/日本語: お知らせ:日本語をお話しになる方は無料の言語アシスタンスサービスをご利用いただけます。IDカードに記載の電話番号を使用してメンバーサービスまでお電話ください(TTY: 711)。
German/Deutsch: ACHTUNG: Wenn Sie Deutsche sprechen, steht Ihnen kostenlos fremdsprachliche Unterstützung zur Verfügung. Rufen Sie den Mitgliederdienst unter der Nummer auf Ihrer ID-Karte an (TTY: 711).
Persian/پارسیان:شناسایی کارت روی بر مندرج تلفن شمار گیرد. با می قرار شما اختیار در رایگان صورت ب بانی ز کمک شما فارسی است، خدمات بان ز توج: اگر
.(TTY: 711) ید بگیر اعضا« تماس بخش »خدمات با خود
Lao/ພາສາລາວ: ຂ ຄວນໃສໃຈ: ຖາເຈ າເວ າພາສາລາວໄດ, ມ ການບ ລ ການຊວຍເຫ ອດານພາສາໃຫທານໂດຍບ ເສຍຄາ. ໂທ ຫາ ຝາຍບ ລ ການສະ ມາ ຊ ກທ ໝາຍເລກໂທລະສບຢໃນບດຂອງທານ (TTY: 711).
Navajo/Diné Bizaad: BAA !KOHWIINDZIN DOO&G&: Din4 k’ehj7 y1n7[t’i’go saad bee y1t’i’ 47 t’11j77k’e bee n7k1’a’doowo[go 47 n1’ahoot’i’. D77 bee an7tah7g7 ninaaltsoos bine’d44’ n0omba bik1’7g7ij8’ b44sh bee hod77lnih (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164711MB 55-1493 (8/16)

DENTAL LOW - $1,000 Max

Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association
SUMMARY OF BENEFITS
Eliassen Group LLC
Dental Blue Program 2®
(with Orthodontics)

Dental Blue Program 2 with OrthodonticsPreventive Benefit Group Basic Benefit Group Major Benefit Group
No Deductible $50 Per Member/$150 Per Family Calendar Year Deductible
Full Coverage 80% Coverage 50% Coverage
$1,000 Calendar-Year Benefit MaximumDiagnostic• One complete initial oral exam, including initial
dental history and charting of the teeth and supporting structures
• Full mouth X-rays, seven or more films, or panoramic X-ray with bitewing X-rays once each 60 months
• Bitewing X-rays once each six months• Single tooth X-rays as needed• Study models and casts used in planning
treatment once each 60 months• Periodic or routine oral exams once each
six months• Emergency exams
Preventive• Routine cleaning, scaling, and polishing of the
teeth once each six months• Fluoride treatment once each six months
(members under age 19) • Sealants on permanent pre-molar and
molar surfaces (members under age 14)Benefits are provided for one application per bicuspid or molar surface each 48 months
• Space maintainers needed due to premature tooth loss (members under age 19)
Restorative• Amalgam (silver) fillings (limited to one filling
for each tooth surface in a 12-month period)• Composite resin (tooth color) fillings (limited
to one filling for each tooth surface in a 12-month period)
• Pin retention for fillings• Stainless steel crowns on baby teeth and on
first permanent adult molars (members under age 16)
Oral Surgery• Tooth extraction• Root removal• Biopsies
Periodontics (gum and bone)• Periodontal scaling and root planing once per
quadrant each 24 months• Periodontal surgery once per quadrant each
36 months• Periodontal maintenance following active
periodontal therapy once each three months
Endodontics (roots and pulp)• Root canal therapy (permanent teeth, once per
lifetime per tooth)• Retreatment root canal therapy on permanent
teeth, once in a lifetime for each tooth• Therapeutic pulpotomy on primary or
permanent teeth (members under age 16)• Other endodontic surgery to treat or remove
the dental root
Prosthetic Maintenance• Repair of partial or complete dentures,
crowns, and bridges once each 12 months• Adding teeth to an existing complete or
partial denture• Rebase or reline of dentures once each
36 months• Recementing of crowns, inlays, onlays, and
fixed bridgework once each 12 months
Other Services• Occlusal adjustments once each 24 months• Services to treat root sensitivity• Emergency dental care to treat acute pain or
to prevent permanent harm to a member• General anesthesia when administered in
conjunction with covered surgical services
Prosthodontics (teeth replacement)• Complete or partial dentures (including
services to fabricate, measure, fit, and adjust them) once each 60 months for each arch
• Fixed bridges (including services to fabricate, measure, fit, and adjust them) once each 60 months for each tooth
• Replacement of dentures and bridges once each 60 months when the existing appliance can’t be made serviceable
• Adding teeth to an existing bridge• Temporary partial dentures to replace any of
the six upper or six lower front teeth (only covered if they are installed immediately following the loss of teeth and during the period of healing)
Major Restorative (members age 16 or older)• Crowns, once each 60 months for each tooth• Metallic, porcelain, and composite resin inlays.
Benefits are provided for an amalgam filling toward the cost of a metallic, porcelain, or composite resin inlay, once each 60 months for each tooth. You pay any balance.
• Metallic, porcelain, and composite resin onlays, once each 60 months for each tooth
• Replacement of crowns, once each 60 months for each tooth
• Replacement of metallic, porcelain, and composite resin inlays. Benefits are provided for an amalgam filling toward the cost of a metallic, porcelain, or composite resin inlay, once each 60 months for each tooth. You pay any balance.
• Replacement of metallic, porcelain, and composite resin onlays, once each 60 months for each tooth
• Post and core or crown buildup, once each 60 months for each tooth
• Single tooth dental endosteal implants (the fixture and abutment portion) in addition to the allowance for the crown for the implant, once each 60 month period, when the implant replaces permanent teeth through the second molars
Orthodontic Benefit Group
50% coverage for all members No deductible• Complete orthodontic exam• Comprehensive or limited active orthodontic
treatment, including appliances
$1,000 Lifetime Benefit Maximum

Welcome to Dental Blue, a comprehensive dental plan that provides a wide range of benefits to meet your dental care needs.
Your DentistDental Blue offers an extensive network of dentists. Over 90 percent of dentists in Massachusetts and New Hampshire participate with Blue Cross Blue Shield of Massachusetts. Dentists who participate with Blue Cross Blue Shield of Rhode Island and out-of-area dentists who participate in the DenteMax Network of Dentists are also available to Dental Blue members.
If you already have a dentist and you want to know if she or he participates with Blue Cross Blue Shield of Massachusetts, you can call the dentist, look at the current dental provider directory, or call Member Service at the toll-free phone number shown on your Dental Blue ID card.
If you would like help choosing a dentist, you can call the Physician Selection Service at 1-800-821-1388. You can also access the online dental provider directory at www.bluecrossma.com.
Your BenefitsThe dental benefits your plan covers are subject to the deductible and coinsurance (if applicable), and benefit maximum amounts shown in the chart. The chart also shows the percentage of costs your plan will pay for covered dental services. Many of the covered services have specific time or age limits.
For example:
• Cleanings are provided only once each six months.
• Fluoride treatments are provided only for members under age 19.
Pre-Treatment EstimatesIf your dentist expects that your dental treatment will involve covered services that will cost more than $250, Blue Cross Blue Shield recommends that your dentist send a copy of the “treatment plan” to Blue Cross Blue Shield before services are provided. A treatment plan is a detailed description of the procedures that the dentist plans to perform and includes an estimate of the charge for each service. Once the treatment plan is reviewed, you and your dentist will be notified of the benefits available.
Remember, the payment estimate is based on your eligibility status and the amount of your calendar-year or lifetime benefit maximum at the time the estimate is received and reviewed. (The actual payment may differ if your available calendar-year or lifetime benefit maximum or eligibility status has changed.)
Multi-Stage ProceduresYour dental plan provides benefits for multi-stage procedures (procedures that require more than one visit, such as crowns, dentures and root canals) as long as you are enrolled in the plan on the date that the multi-stage procedure is completed. A participating dentist will send a claim for a multi-stage procedure to Blue Cross Blue Shield only after the completion date of the procedure. You will be responsible for all charges for multi-stage procedures if your plan has been cancelled before the completion date of the procedure.
How Dentists Are PaidParticipating DentistsDentists that participate with Blue Cross Blue Shield of Massachusetts, Blue Cross Blue Shield of Rhode Island, or out-of-area dentists that are in the DenteMax Network of Dentists, accept the lesser of either the dentist’s actual charge or the allowed charge as payment in full for covered services. You pay only your deductible and coinsurance (if applicable), and charges beyond your calendar-year or lifetime benefit maximum.
In Massachusetts, benefits are usually only provided when covered services are furnished by a participating dentist. The exceptions are described in your plan description.
Non-participating Dentists Outside of Massachusetts Benefits for covered services by a non-participating dentist outside of Massachusetts are provided based on the 90th percentile of the Dental Prevailing Healthcare Charges in the zip code region where the services are furnished, but no more than the dentist’s actual charge. This amount is sometimes less than the dentist’s actual charge. In this case, you must pay the amount of the actual charge that is in excess of the allowed charge. This is in addition to the amount you would normally pay for covered services.
How Orthodontic Benefits Are PaidYour plan includes orthodontic coverage. The lifetime benefit maximum is not part of your calendar-year benefit maximum; it applies only to orthodontic services. You are responsible for your coinsurance and any charges beyond your lifetime benefit maximum. Benefits are available on your effective date. If your orthodontic treatment began before you were covered under Dental Blue, a monthly fee will be paid for your remaining orthodontic visits until either your treatment is completed or the lifetime benefit maximum is exhausted, whichever comes first.

When Coverage BeginsYou are covered, without a waiting period, from the date you enroll in the plan.
Dependent BenefitsThis plan covers dependents until the end of the calendar month in which they turn age 26, regardless of their financial dependency, student status, or employment status. Please see your plan description (and riders, if any) for exact coverage details.
Accumulated Maximum Rollover BenefitsThis portion of the dental plan includes an Accumulated Maximum Rollover Benefit. This rollover benefit allows you to roll over a certain dollar amount of your unused annual dental benefits for use in the future. There are limits and restrictions on this benefit. Refer to the Accumulated Dental Maximum Rollover brochure for further information.
Enhanced Dental BenefitsEnhanced Dental Benefits for certain dental care services are available for members who have been diagnosed with diabetes, coronary artery disease, oral cancer, or who are pregnant. Contact Member Service for more information.
If You Have to File a ClaimParticipating dentists will send claims directly to Blue Cross Blue Shield. All you have to do is show them your Dental Blue ID card. The payment will be sent directly to your dentist as long as the claims are received within one year of the completed service.
If you receive care from a non-participating dentist, you will typically need to submit the claim yourself. Before submitting your claim, get an Attending Dentist’s Statement form from Member Service.
After your dentist fills out the form, send it and your original itemized bills to Blue Cross Blue Shield of Massachusetts, P. O. Box 986030, Boston, MA 02298. All member-submitted claims must be submitted within two years of the date of service.
If you have a grievance, see your plan description for instructions on how to file a grievance.
Other InformationCoordination of benefits applies to plan members who are covered by another plan for health care expenses. Coordination of benefits ensures that payments from other insurance or health care plans do not exceed the total charges billed for covered services.
Your plan description has a subrogation clause, which means that Blue Cross Blue Shield can recover payments if a member has already been paid for the same claim by a third party.
Questions? For questions about Blue Cross Blue Shield of Massachusetts, call 800-358-2227, or visit us online at www.bluecrossma.com.Interested in receiving information from us via e-mail? Go to www.bluecrossma.com/email to sign up.
Limitations and Exclusions. These pages summarize the benefits of your dental plan. Your plan description and riders define the full terms and conditions in greater detail. Should any questions arise concerning benefits, the plan description and riders will govern. For a complete list of limitations and exclusions, refer to your plan description and riders.
Note: Blue Cross and Blue Shield of Massachusetts, Inc., is the administrator of the benefits described in this summary. Blue Cross and Blue Shield of Massachusetts, Inc., administers claims payments only and does not assume financial risk for claims.
November 2016
® Registered Marks of the Blue Cross and Blue Shield Association. © 2017 Blue Cross and Blue Shield of Massachusetts, Inc.
Printed at Blue Cross and Blue Shield of Massachusetts, Inc.
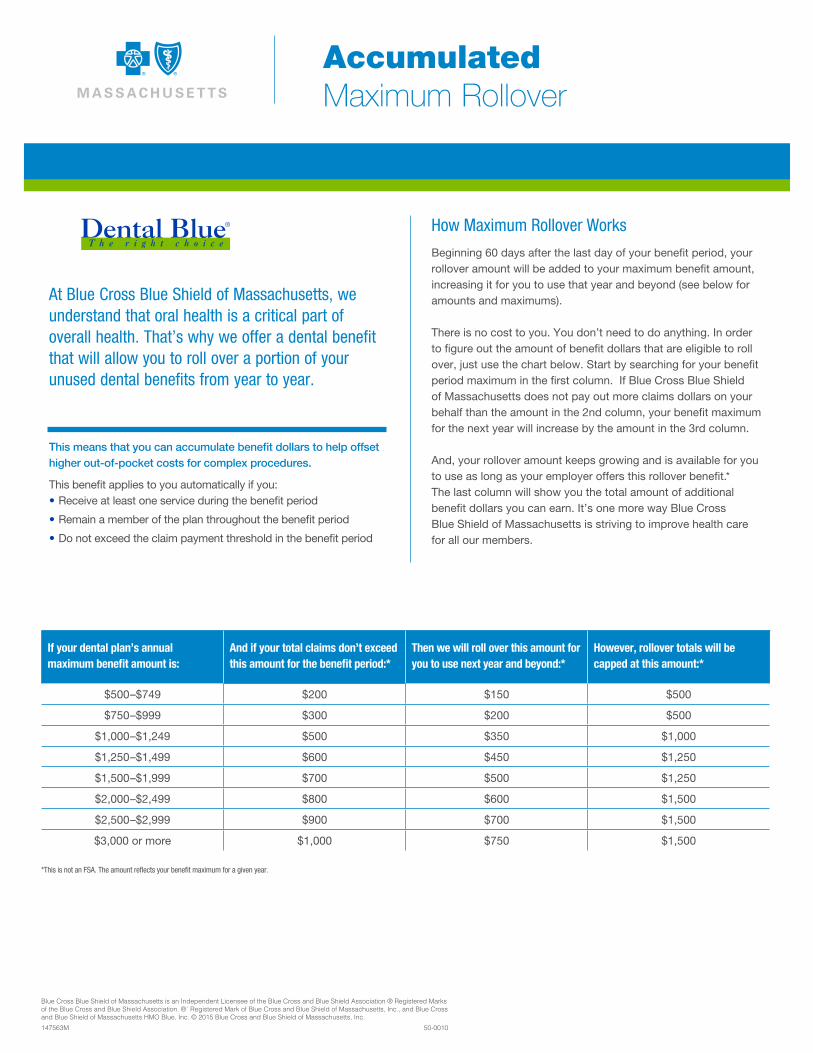
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association ® Registered Marks of the Blue Cross and Blue Shield Association. ®´ Registered Mark of Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. © 2015 Blue Cross and Blue Shield of Massachusetts, Inc.
147563M 50-0010
At Blue Cross Blue Shield of Massachusetts, we understand that oral health is a critical part of overall health. That’s why we offer a dental benefit that will allow you to roll over a portion of your unused dental benefits from year to year.
This means that you can accumulate benefit dollars to help offset higher out-of-pocket costs for complex procedures.
This benefit applies to you automatically if you:•Receive at least one service during the benefit period
•Remain a member of the plan throughout the benefit period
•Do not exceed the claim payment threshold in the benefit period
How Maximum Rollover Works
Beginning 60 days after the last day of your benefit period, your rollover amount will be added to your maximum benefit amount, increasing it for you to use that year and beyond (see below for amounts and maximums).
There is no cost to you. You don’t need to do anything. In order to figure out the amount of benefit dollars that are eligible to roll over, just use the chart below. Start by searching for your benefit period maximum in the first column. If Blue Cross Blue Shield of Massachusetts does not pay out more claims dollars on your behalf than the amount in the 2nd column, your benefit maximum for the next year will increase by the amount in the 3rd column.
And, your rollover amount keeps growing and is available for you to use as long as your employer offers this rollover benefit.* The last column will show you the total amount of additional benefit dollars you can earn. It’s one more way Blue Cross Blue Shield of Massachusetts is striving to improve health care for all our members.
Accumulated Maximum Rollover
If your dental plan’s annual maximum benefit amount is:
And if your total claims don’t exceed this amount for the benefit period:*
Then we will roll over this amount for you to use next year and beyond:*
However, rollover totals will be capped at this amount:*
$500–$749 $200 $150 $500
$750–$999 $300 $200 $500
$1,000–$1,249 $500 $350 $1,000
$1,250–$1,499 $600 $450 $1,250
$1,500–$1,999 $700 $500 $1,250
$2,000–$2,499 $800 $600 $1,500
$2,500–$2,999 $900 $700 $1,500
$3,000 or more $1,000 $750 $1,500
*This is not an FSA. The amount reflects your benefit maximum for a given year.

Nondiscrimination Notice
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164264M 55-1487 (8/16)
Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. It does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Blue Cross Blue Shield of Massachusetts provides:
• Free aids and services to people with disabilities to communicate effectively with us, such as qualified sign language interpreters and written information in other formats (large print or other formats).
• Free language services to people whose primary language is not English, such as qualified interpreters and information written in other languages.
If you need these services, call Member Service at the number on your ID card.
If you believe that Blue Cross Blue Shield of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can file a grievance with the Civil Rights Coordinator by mail at Civil Rights Coordinator, Blue Cross Blue Shield of Massachusetts, One Enterprise Drive, Quincy, MA 02171-2126; phone at 1-800-472-2689 (TTY: 711); fax at 1-617-246-3616; or email at [email protected].
If you need help filing a grievance, the Civil Rights Coordinator is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights online at ocrportal.hhs.gov; by mail at U.S. Department of Health and Human Services, 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201; by phone at 1-800-368-1019 or 1-800-537-7697 (TDD).
Complaint forms are available at hhs.gov.

Translation ResourcesProficiency of Language Assistance Services
Spanish/Español: ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que figura en su tarjeta de identificación (TTY: 711).
Portuguese/Português: ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711).
Chinese/简体中文: 注意:如果您讲中文,我们可向您免费提供语言协助服务。请拨打您 ID 卡上的号码联系会员服务部(TTY 号码:711)。
Haitian Creole/Kreyòl Ayisyen: ATANSYON: Si ou pale kreyòl ayisyen, sèvis asistans nan lang disponib pou ou gratis. Rele nimewo Sèvis Manm nan ki sou kat Idantitifkasyon w lan (Sèvis pou Malantandan TTY: 711).
Vietnamese/Tiếng Việt: LƯU Ý: Nếu quý vị nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ được cung cấp cho quý vị miễn phí. Gọi cho Dịch vụ Hội viên theo số trên thẻ ID của quý vị (TTY: 711).
Russian/Русский: ВНИМАНИЕ: если Вы говорите по-русски, Вы можете воспользоваться бесплатными услугами переводчика. Позвоните в отдел обслуживания клиентов по номеру, указанному в Вашей идентификационной карте (телетайп: 711).
Arabic/ةيرب:انتباه: إذا كنت تتحدث اللغة العربية، فتتوفر خدمات املساعدة اللغوية مجانا بالنسبة لك. اتصل بخدمات األعضاء عىل الرقم املوجود عىل بطاقة هويتك (جهاز الهاتف
.(711 :”TTY“ النيص للصم والبكم
Mon-Khmer, Cambodian/ខមែរ: ការជនដណង៖ បរសនបរើអនកនយាយភាសា ខមែរ បសវាជនយភាសាឥតគតថលៃ គអាចរកបានសបរារអនក។ សមទរសពទបៅខនកបសវាសរាជកតាមបេបៅបេើរណណ សរាគា េលៃនររសអនក (TTY: 711)។
French/Français: ATTENTION : si vous parlez français, des services d’assistance linguistique sont disponibles gratuitement. Appelez le Service adhérents au numéro indiqué sur votre carte d’assuré (TTY : 711).
Italian/Italiano: ATTENZIONE: se parlate italiano, sono disponibili per voi servizi gratuiti di assistenza linguistica. Chiamate il Servizio per i membri al numero riportato sulla vostra scheda identificativa (TTY: 711).
Korean/한국어: 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 귀하의 ID 카드에 있는 전화번호(TTY: 711)를 사용하여 회원 서비스에 전화하십시오.
Greek/λληνικά: ΠΡΟΣΟΧΗ: Εάν μιλάτε Ελληνικά, διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε την Υπηρεσία Εξυπηρέτησης Μελών στον αριθμό της κάρτας μέλους σας (ID Card) (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association

Polish/Polski: UWAGA: Osoby posługujące się językiem polskim mogą bezpłatnie skorzystać z pomocy językowej. Należy zadzwonić do Działu obsługi ubezpieczonych pod numer podany na identyfikatorze (TTY: 711).
Hindi/हिदी: धयान द: दद आप दिनददी बोलत ि, तो भयाषया सियातया सवयाए, आप क ललए नन:शलक उपलबध ि। सदस सवयाओ को आपक आई.डी. कयाडड पर ददए गए नबर पर कॉल कर (टदी.टदी.वयाई.: 711).
Gujarati/ગજરાતી: ધયાન આપો: જો તમ ગજરયાતી બોલતયા હો, તો તમન ભયાષયાકી સહયાતયા સવયાઓ વવનયા મલ ઉપલબધ છ. તમયારયા આઈડી કયાડડ પર આપલયા નબર પર Member Service ન કૉલ કરો (TTY: 711).
Tagalog/Tagalog: PAUNAWA: Kung nagsasalita ka ng wikang Tagalog, mayroon kang magagamit na mga libreng serbisyo para sa tulong sa wika. Tawagan ang Mga Serbisyo sa Miyembro sa numerong nasa iyong ID Card (TTY: 711).
Japanese/日本語: お知らせ:日本語をお話しになる方は無料の言語アシスタンスサービスをご利用いただけます。IDカードに記載の電話番号を使用してメンバーサービスまでお電話ください(TTY: 711)。
German/Deutsch: ACHTUNG: Wenn Sie Deutsche sprechen, steht Ihnen kostenlos fremdsprachliche Unterstützung zur Verfügung. Rufen Sie den Mitgliederdienst unter der Nummer auf Ihrer ID-Karte an (TTY: 711).
Persian/پارسیان:شناسایی کارت روی بر مندرج تلفن شمار گیرد. با می قرار شما اختیار در رایگان صورت ب بانی ز کمک شما فارسی است، خدمات بان ز توج: اگر
.(TTY: 711) ید بگیر اعضا« تماس بخش »خدمات با خود
Lao/ພາສາລາວ: ຂ ຄວນໃສໃຈ: ຖາເຈ າເວ າພາສາລາວໄດ, ມ ການບ ລ ການຊວຍເຫ ອດານພາສາໃຫທານໂດຍບ ເສຍຄາ. ໂທ ຫາ ຝາຍບ ລ ການສະ ມາ ຊ ກທ ໝາຍເລກໂທລະສບຢໃນບດຂອງທານ (TTY: 711).
Navajo/Diné Bizaad: BAA !KOHWIINDZIN DOO&G&: Din4 k’ehj7 y1n7[t’i’go saad bee y1t’i’ 47 t’11j77k’e bee n7k1’a’doowo[go 47 n1’ahoot’i’. D77 bee an7tah7g7 ninaaltsoos bine’d44’ n0omba bik1’7g7ij8’ b44sh bee hod77lnih (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164711MB 55-1493 (8/16)

DENTAL HIGH - $1,500 Max

Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association
SUMMARY OF BENEFITS
Eliassen Group LLC
Dental Blue Program 2®
(with Orthodontics)

Dental Blue Program 2 with OrthodonticsPreventive Benefit Group Basic Benefit Group Major Benefit Group
No Deductible $50 Per Member/$150 Per Family Calendar Year Deductible
Full Coverage 80% Coverage 50% Coverage
$1,500 Calendar-Year Benefit MaximumDiagnostic• One complete initial oral exam, including initial
dental history and charting of the teeth and supporting structures
• Full mouth X-rays, seven or more films, or panoramic X-ray with bitewing X-rays once each 60 months
• Bitewing X-rays once each six months• Single tooth X-rays as needed• Study models and casts used in planning
treatment once each 60 months• Periodic or routine oral exams once each
six months• Emergency exams
Preventive• Routine cleaning, scaling, and polishing of the
teeth once each six months• Fluoride treatment once each six months
(members under age 19) • Sealants on permanent pre-molar and
molar surfaces (members under age 14)Benefits are provided for one application per bicuspid or molar surface each 48 months
• Space maintainers needed due to premature tooth loss (members under age 19)
Restorative• Amalgam (silver) fillings (limited to one filling
for each tooth surface in a 12-month period)• Composite resin (tooth color) fillings (limited
to one filling for each tooth surface in a 12-month period)
• Pin retention for fillings• Stainless steel crowns on baby teeth and on
first permanent adult molars (members under age 16)
Oral Surgery• Tooth extraction• Root removal• Biopsies
Periodontics (gum and bone)• Periodontal scaling and root planing once per
quadrant each 24 months• Periodontal surgery once per quadrant each
36 months• Periodontal maintenance following active
periodontal therapy once each three months
Endodontics (roots and pulp)• Root canal therapy (permanent teeth, once per
lifetime per tooth)• Retreatment root canal therapy on permanent
teeth, once in a lifetime for each tooth• Therapeutic pulpotomy on primary or
permanent teeth (members under age 16)• Other endodontic surgery to treat or remove
the dental root
Prosthetic Maintenance• Repair of partial or complete dentures,
crowns, and bridges once each 12 months• Adding teeth to an existing complete or
partial denture• Rebase or reline of dentures once each
36 months• Recementing of crowns, inlays, onlays, and
fixed bridgework once each 12 months
Other Services• Occlusal adjustments once each 24 months• Services to treat root sensitivity• Emergency dental care to treat acute pain or
to prevent permanent harm to a member• General anesthesia when administered in
conjunction with covered surgical services
Prosthodontics (teeth replacement)• Complete or partial dentures (including
services to fabricate, measure, fit, and adjust them) once each 60 months for each arch
• Fixed bridges (including services to fabricate, measure, fit, and adjust them) once each 60 months for each tooth
• Replacement of dentures and bridges once each 60 months when the existing appliance can’t be made serviceable
• Adding teeth to an existing bridge• Temporary partial dentures to replace any of
the six upper or six lower front teeth (only covered if they are installed immediately following the loss of teeth and during the period of healing)
Major Restorative (members age 16 or older)• Crowns, once each 60 months for each tooth• Metallic, porcelain, and composite resin inlays.
Benefits are provided for an amalgam filling toward the cost of a metallic, porcelain, or composite resin inlay, once each 60 months for each tooth. You pay any balance.
• Metallic, porcelain, and composite resin onlays, once each 60 months for each tooth
• Replacement of crowns, once each 60 months for each tooth
• Replacement of metallic, porcelain, and composite resin inlays. Benefits are provided for an amalgam filling toward the cost of a metallic, porcelain, or composite resin inlay, once each 60 months for each tooth. You pay any balance.
• Replacement of metallic, porcelain, and composite resin onlays, once each 60 months for each tooth
• Post and core or crown buildup, once each 60 months for each tooth
• Single tooth dental endosteal implants (the fixture and abutment portion) in addition to the allowance for the crown for the implant, once each 60 month period, when the implant replaces permanent teeth through the second molars
Orthodontic Benefit Group
50% coverage for all members No deductible• Complete orthodontic exam• Comprehensive or limited active orthodontic
treatment, including appliances
$1,500 Lifetime Benefit Maximum

Welcome to Dental Blue, a comprehensive dental plan that provides a wide range of benefits to meet your dental care needs.
Your DentistDental Blue offers an extensive network of dentists. Over 90 percent of dentists in Massachusetts and New Hampshire participate with Blue Cross Blue Shield of Massachusetts. Dentists who participate with Blue Cross Blue Shield of Rhode Island and out-of-area dentists who participate in the DenteMax Network of Dentists are also available to Dental Blue members.
If you already have a dentist and you want to know if she or he participates with Blue Cross Blue Shield of Massachusetts, you can call the dentist, look at the current dental provider directory, or call Member Service at the toll-free phone number shown on your Dental Blue ID card.
If you would like help choosing a dentist, you can call the Physician Selection Service at 1-800-821-1388. You can also access the online dental provider directory at www.bluecrossma.com.
Your BenefitsThe dental benefits your plan covers are subject to the deductible and coinsurance (if applicable), and benefit maximum amounts shown in the chart. The chart also shows the percentage of costs your plan will pay for covered dental services. Many of the covered services have specific time or age limits.
For example:
• Cleanings are provided only once each six months.
• Fluoride treatments are provided only for members under age 19.
Pre-Treatment EstimatesIf your dentist expects that your dental treatment will involve covered services that will cost more than $250, Blue Cross Blue Shield recommends that your dentist send a copy of the “treatment plan” to Blue Cross Blue Shield before services are provided. A treatment plan is a detailed description of the procedures that the dentist plans to perform and includes an estimate of the charge for each service. Once the treatment plan is reviewed, you and your dentist will be notified of the benefits available.
Remember, the payment estimate is based on your eligibility status and the amount of your calendar-year or lifetime benefit maximum at the time the estimate is received and reviewed. (The actual payment may differ if your available calendar-year or lifetime benefit maximum or eligibility status has changed.)
Multi-Stage ProceduresYour dental plan provides benefits for multi-stage procedures (procedures that require more than one visit, such as crowns, dentures and root canals) as long as you are enrolled in the plan on the date that the multi-stage procedure is completed. A participating dentist will send a claim for a multi-stage procedure to Blue Cross Blue Shield only after the completion date of the procedure. You will be responsible for all charges for multi-stage procedures if your plan has been cancelled before the completion date of the procedure.
How Dentists Are PaidParticipating DentistsDentists that participate with Blue Cross Blue Shield of Massachusetts, Blue Cross Blue Shield of Rhode Island, or out-of-area dentists that are in the DenteMax Network of Dentists, accept the lesser of either the dentist’s actual charge or the allowed charge as payment in full for covered services. You pay only your deductible and coinsurance (if applicable), and charges beyond your calendar-year or lifetime benefit maximum.
In Massachusetts, benefits are usually only provided when covered services are furnished by a participating dentist. The exceptions are described in your plan description.
Non-participating Dentists Outside of Massachusetts Benefits for covered services by a non-participating dentist outside of Massachusetts are provided based on the 90th percentile of the Dental Prevailing Healthcare Charges in the zip code region where the services are furnished, but no more than the dentist’s actual charge. This amount is sometimes less than the dentist’s actual charge. In this case, you must pay the amount of the actual charge that is in excess of the allowed charge. This is in addition to the amount you would normally pay for covered services.
How Orthodontic Benefits Are PaidYour plan includes orthodontic coverage. The lifetime benefit maximum is not part of your calendar-year benefit maximum; it applies only to orthodontic services. You are responsible for your coinsurance and any charges beyond your lifetime benefit maximum. Benefits are available on your effective date. If your orthodontic treatment began before you were covered under Dental Blue, a monthly fee will be paid for your remaining orthodontic visits until either your treatment is completed or the lifetime benefit maximum is exhausted, whichever comes first.

When Coverage BeginsYou are covered, without a waiting period, from the date you enroll in the plan.
Dependent BenefitsThis plan covers dependents until the end of the calendar month in which they turn age 26, regardless of their financial dependency, student status, or employment status. Please see your plan description (and riders, if any) for exact coverage details.
Accumulated Maximum Rollover BenefitsThis portion of the dental plan includes an Accumulated Maximum Rollover Benefit. This rollover benefit allows you to roll over a certain dollar amount of your unused annual dental benefits for use in the future. There are limits and restrictions on this benefit. Refer to the Accumulated Dental Maximum Rollover brochure for further information.
Enhanced Dental BenefitsEnhanced Dental Benefits for certain dental care services are available for members who have been diagnosed with diabetes, coronary artery disease, oral cancer, or who are pregnant. Contact Member Service for more information.
If You Have to File a ClaimParticipating dentists will send claims directly to Blue Cross Blue Shield. All you have to do is show them your Dental Blue ID card. The payment will be sent directly to your dentist as long as the claims are received within one year of the completed service.
If you receive care from a non-participating dentist, you will typically need to submit the claim yourself. Before submitting your claim, get an Attending Dentist’s Statement form from Member Service.
After your dentist fills out the form, send it and your original itemized bills to Blue Cross Blue Shield of Massachusetts, P. O. Box 986030, Boston, MA 02298. All member-submitted claims must be submitted within two years of the date of service.
If you have a grievance, see your plan description for instructions on how to file a grievance.
Other InformationCoordination of benefits applies to plan members who are covered by another plan for health care expenses. Coordination of benefits ensures that payments from other insurance or health care plans do not exceed the total charges billed for covered services.
Your plan description has a subrogation clause, which means that Blue Cross Blue Shield can recover payments if a member has already been paid for the same claim by a third party.
Questions? For questions about Blue Cross Blue Shield of Massachusetts, call 800-358-2227, or visit us online at www.bluecrossma.com.Interested in receiving information from us via e-mail? Go to www.bluecrossma.com/email to sign up.
Limitations and Exclusions. These pages summarize the benefits of your dental plan. Your plan description and riders define the full terms and conditions in greater detail. Should any questions arise concerning benefits, the plan description and riders will govern. For a complete list of limitations and exclusions, refer to your plan description and riders.
Note: Blue Cross and Blue Shield of Massachusetts, Inc., is the administrator of the benefits described in this summary. Blue Cross and Blue Shield of Massachusetts, Inc., administers claims payments only and does not assume financial risk for claims.
November 2016
® Registered Marks of the Blue Cross and Blue Shield Association. © 2017 Blue Cross and Blue Shield of Massachusetts, Inc.
Printed at Blue Cross and Blue Shield of Massachusetts, Inc.

Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association ® Registered Marks of the Blue Cross and Blue Shield Association. ®´ Registered Mark of Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. © 2015 Blue Cross and Blue Shield of Massachusetts, Inc.
147563M 50-0010
At Blue Cross Blue Shield of Massachusetts, we understand that oral health is a critical part of overall health. That’s why we offer a dental benefit that will allow you to roll over a portion of your unused dental benefits from year to year.
This means that you can accumulate benefit dollars to help offset higher out-of-pocket costs for complex procedures.
This benefit applies to you automatically if you:•Receive at least one service during the benefit period
•Remain a member of the plan throughout the benefit period
•Do not exceed the claim payment threshold in the benefit period
How Maximum Rollover Works
Beginning 60 days after the last day of your benefit period, your rollover amount will be added to your maximum benefit amount, increasing it for you to use that year and beyond (see below for amounts and maximums).
There is no cost to you. You don’t need to do anything. In order to figure out the amount of benefit dollars that are eligible to roll over, just use the chart below. Start by searching for your benefit period maximum in the first column. If Blue Cross Blue Shield of Massachusetts does not pay out more claims dollars on your behalf than the amount in the 2nd column, your benefit maximum for the next year will increase by the amount in the 3rd column.
And, your rollover amount keeps growing and is available for you to use as long as your employer offers this rollover benefit.* The last column will show you the total amount of additional benefit dollars you can earn. It’s one more way Blue Cross Blue Shield of Massachusetts is striving to improve health care for all our members.
Accumulated Maximum Rollover
If your dental plan’s annual maximum benefit amount is:
And if your total claims don’t exceed this amount for the benefit period:*
Then we will roll over this amount for you to use next year and beyond:*
However, rollover totals will be capped at this amount:*
$500–$749 $200 $150 $500
$750–$999 $300 $200 $500
$1,000–$1,249 $500 $350 $1,000
$1,250–$1,499 $600 $450 $1,250
$1,500–$1,999 $700 $500 $1,250
$2,000–$2,499 $800 $600 $1,500
$2,500–$2,999 $900 $700 $1,500
$3,000 or more $1,000 $750 $1,500
*This is not an FSA. The amount reflects your benefit maximum for a given year.

Nondiscrimination Notice
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164264M 55-1487 (8/16)
Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. It does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Blue Cross Blue Shield of Massachusetts provides:
• Free aids and services to people with disabilities to communicate effectively with us, such as qualified sign language interpreters and written information in other formats (large print or other formats).
• Free language services to people whose primary language is not English, such as qualified interpreters and information written in other languages.
If you need these services, call Member Service at the number on your ID card.
If you believe that Blue Cross Blue Shield of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can file a grievance with the Civil Rights Coordinator by mail at Civil Rights Coordinator, Blue Cross Blue Shield of Massachusetts, One Enterprise Drive, Quincy, MA 02171-2126; phone at 1-800-472-2689 (TTY: 711); fax at 1-617-246-3616; or email at [email protected].
If you need help filing a grievance, the Civil Rights Coordinator is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights online at ocrportal.hhs.gov; by mail at U.S. Department of Health and Human Services, 200 Independence Avenue, SW Room 509F, HHH Building Washington, DC 20201; by phone at 1-800-368-1019 or 1-800-537-7697 (TDD).
Complaint forms are available at hhs.gov.
Translation ResourcesProficiency of Language Assistance Services
Spanish/Español: ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que figura en su tarjeta de identificación (TTY: 711).
Portuguese/Português: ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711).
Chinese/简体中文: 注意:如果您讲中文,我们可向您免费提供语言协助服务。请拨打您 ID 卡上的号码联系会员服务部(TTY 号码:711)。
Haitian Creole/Kreyòl Ayisyen: ATANSYON: Si ou pale kreyòl ayisyen, sèvis asistans nan lang disponib pou ou gratis. Rele nimewo Sèvis Manm nan ki sou kat Idantitifkasyon w lan (Sèvis pou Malantandan TTY: 711).
Vietnamese/Tiếng Việt: LƯU Ý: Nếu quý vị nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ được cung cấp cho quý vị miễn phí. Gọi cho Dịch vụ Hội viên theo số trên thẻ ID của quý vị (TTY: 711).
Russian/Русский: ВНИМАНИЕ: если Вы говорите по-русски, Вы можете воспользоваться бесплатными услугами переводчика. Позвоните в отдел обслуживания клиентов по номеру, указанному в Вашей идентификационной карте (телетайп: 711).
Arabic/ةيرب:انتباه: إذا كنت تتحدث اللغة العربية، فتتوفر خدمات املساعدة اللغوية مجانا بالنسبة لك. اتصل بخدمات األعضاء عىل الرقم املوجود عىل بطاقة هويتك (جهاز الهاتف
.(711 :”TTY“ النيص للصم والبكم
Mon-Khmer, Cambodian/ខមែរ: ការជនដណង៖ បរសនបរើអនកនយាយភាសា ខមែរ បសវាជនយភាសាឥតគតថលៃ គអាចរកបានសបរារអនក។ សមទរសពទបៅខនកបសវាសរាជកតាមបេបៅបេើរណណ សរាគា េលៃនររសអនក (TTY: 711)។
French/Français: ATTENTION : si vous parlez français, des services d’assistance linguistique sont disponibles gratuitement. Appelez le Service adhérents au numéro indiqué sur votre carte d’assuré (TTY : 711).
Italian/Italiano: ATTENZIONE: se parlate italiano, sono disponibili per voi servizi gratuiti di assistenza linguistica. Chiamate il Servizio per i membri al numero riportato sulla vostra scheda identificativa (TTY: 711).
Korean/한국어: 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 귀하의 ID 카드에 있는 전화번호(TTY: 711)를 사용하여 회원 서비스에 전화하십시오.
Greek/λληνικά: ΠΡΟΣΟΧΗ: Εάν μιλάτε Ελληνικά, διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε την Υπηρεσία Εξυπηρέτησης Μελών στον αριθμό της κάρτας μέλους σας (ID Card) (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association

Polish/Polski: UWAGA: Osoby posługujące się językiem polskim mogą bezpłatnie skorzystać z pomocy językowej. Należy zadzwonić do Działu obsługi ubezpieczonych pod numer podany na identyfikatorze (TTY: 711).
Hindi/हिदी: धयान द: दद आप दिनददी बोलत ि, तो भयाषया सियातया सवयाए, आप क ललए नन:शलक उपलबध ि। सदस सवयाओ को आपक आई.डी. कयाडड पर ददए गए नबर पर कॉल कर (टदी.टदी.वयाई.: 711).
Gujarati/ગજરાતી: ધયાન આપો: જો તમ ગજરયાતી બોલતયા હો, તો તમન ભયાષયાકી સહયાતયા સવયાઓ વવનયા મલ ઉપલબધ છ. તમયારયા આઈડી કયાડડ પર આપલયા નબર પર Member Service ન કૉલ કરો (TTY: 711).
Tagalog/Tagalog: PAUNAWA: Kung nagsasalita ka ng wikang Tagalog, mayroon kang magagamit na mga libreng serbisyo para sa tulong sa wika. Tawagan ang Mga Serbisyo sa Miyembro sa numerong nasa iyong ID Card (TTY: 711).
Japanese/日本語: お知らせ:日本語をお話しになる方は無料の言語アシスタンスサービスをご利用いただけます。IDカードに記載の電話番号を使用してメンバーサービスまでお電話ください(TTY: 711)。
German/Deutsch: ACHTUNG: Wenn Sie Deutsche sprechen, steht Ihnen kostenlos fremdsprachliche Unterstützung zur Verfügung. Rufen Sie den Mitgliederdienst unter der Nummer auf Ihrer ID-Karte an (TTY: 711).
Persian/پارسیان:شناسایی کارت روی بر مندرج تلفن شمار گیرد. با می قرار شما اختیار در رایگان صورت ب بانی ز کمک شما فارسی است، خدمات بان ز توج: اگر
.(TTY: 711) ید بگیر اعضا« تماس بخش »خدمات با خود
Lao/ພາສາລາວ: ຂ ຄວນໃສໃຈ: ຖາເຈ າເວ າພາສາລາວໄດ, ມ ການບ ລ ການຊວຍເຫ ອດານພາສາໃຫທານໂດຍບ ເສຍຄາ. ໂທ ຫາ ຝາຍບ ລ ການສະ ມາ ຊ ກທ ໝາຍເລກໂທລະສບຢໃນບດຂອງທານ (TTY: 711).
Navajo/Diné Bizaad: BAA !KOHWIINDZIN DOO&G&: Din4 k’ehj7 y1n7[t’i’go saad bee y1t’i’ 47 t’11j77k’e bee n7k1’a’doowo[go 47 n1’ahoot’i’. D77 bee an7tah7g7 ninaaltsoos bine’d44’ n0omba bik1’7g7ij8’ b44sh bee hod77lnih (TTY: 711).
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2016 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.164711MB 55-1493 (8/16)

Hello,Neighbor
More,for less. . .
Eliassen Group
• You’re on the INSIGHTNetwork
• For a complete list ofproviders near you, useour Provider Locator onwww.eyemed.com andchoose the INSIGHTnetwork or call1-866-804-0982.
• For Lasik providers, call1-877-5LASER6 orvisit eyemedlasik.com.
40%Complete pairof prescriptioneyeglasses
20%Non-prescriptionsunglasses
20%Remaining balancebeyond plan coverage
These discounts are forin-network providers only
Vision Care In-Network Out-of-NetworkServices Member Cost Reimbursement
OFF
OFF
OFF
ExamWith Dilation as Necessary $10 Copay Up to $50
Contact Lens Fit and Follow-Up (Contact lens fit and two follow up visits are available once a comprehensive eye exam has been completed)
Standard Contact Lens Fit & Follow-Up Up to $55 N/APremium Contact Lens Fit & Follow-Up 10% off retail N/A
Retinal Imaging Up to $39 N/A
Frames $0 Copay; $130 allowance; 80% of charge over $130 Up to $74
Standard Plastic LensesSingle Vision $10 Copay Up to $42Bifocal $10 Copay Up to $78Trifocal $10 Copay Up to $130Standard Progressive Lens $75 Up to $78Premium Progressive Lens $95 - $120Tier 1 $95 Up to $78Tier 2 $107 Up to $78Tier 3 $120 Up to $78Tier 4 $75, 80% of charge less $120 Allowance Up to $78
Lenticular $10 Copay Up to $130
Lens Options (paid by the member and added to the base price of the lens)UV Treatment $15 N/ATint (Solid and Gradient) $15 N/AStandard Plastic Scratch Coating $0 Up to $12Standard Polycarbonate $40 N/AStandard Polycarbonate - Kids under 19 $40 N/AStandard Anti-Reflective Coating $45 N/APremium Anti-Reflective Coating N/ATier 1 $57 N/ATier 2 $68 N/ATier 3 80% of charge N/A
Photochromic/Transitions $75 N/APolarized 20% off retail price N/AOther Add-Ons and Services 20% off retail price N/A
Contact LensesConventional $0 Copay; $105 allowance; 15% off retail price over $105 Up to $84Disposable $0 Copay; $105 allowance; plus balance over $105 Up to $84Medically Necessary $0 copay, Paid in Full Up to $210
Laser Vision CorrectionLasik or PRK from U.S. Laser Network 15% off the retail price or 5% off the promotional price N/A
FrequencyExamination Once every 12 monthsLenses or Contact Lenses Once every 12 monthsFrame Once every 24 months
Premium progressives and premium anti-reflective designations are subject to annual review by EyeMed’s Medical Director and are subject to change based on marketconditions. Fixed pricing is reflective of brands at the listed product level . All providers are not required to carry all brands at all levels.
_____________________________ _________________________________________ _________________

What’s in it for me? Options. It’s simple really. We love our members—that’s why we are dedicated to helping you see clearly and we’ve built a network that gives you lots of choices and flexibility. You can choose from independent doctors and retail providers to find the one that best fits your needs and schedule. No matter which one you choose, our plan is designed to be easy to use and to save you money. Welcome to EyeMed.
And now it’s time for the breakdown . . . Here’s an example of what you might pay for a pair of glasses vs. what you’d pay without vision coverage. So, let’s say you get an eye exam and choose a frame that costs $163 with single vision lenses that have UV and scratch protection. Now let’s see the difference . . .
eyemed.com
Out-of-NetworkReimbursementWith UsBenefits Snapshot
Exam with dilation as necessary (Once every 12 months)
Exam $10 Copay Exam $106
Lens $10 Copay Lens $78$15 UV treatment add-on $23 UV treatment add-on
+$0 Scratch coating add-on +$25 Scratch coating add-on
$25 $126
Benefits are not provided from services or materials arising from: 1) Orthoptic or vision training, subnormal vision aids and any associated supplemental testing; Aniseikonic lenses; 2)Medical and/or surgical treatment of the eye, eyes or supporting structures; 3) Any eye or Vision Examination, or any corrective eyewear required by a Policyholder as a condition ofemployment; Safety eyewear; 4) Services provided as a result of any Workers’ Compensation law, or similar legislation, or required by any governmental agency or program whetherfederal, state or subdivisions thereof; 5) Plano (non-prescription) lenses and/or contact lenses; 6) Non-prescription sunglasses; 7) Two pair of glasses in lieu of bifocals; 8) Services ormaterials provided by any other group benefit plan providing vision care 9) Services rendered after the date an Insured Person ceases to be covered under the Policy, except whenVision Materials ordered before coverage ended are delivered, and the services rendered to the Insured Person are within 31 days from the date of such order. 10) Lost or broken lenses,frames, glasses, or contact lenses will not be replaced except in the next Benefit Frequency when Vision Materials would next become available. Benefits may not be combined with anydiscount, promotional offering, or other group benefit plans. Standard/Premium Progressive lens not covered-fund as a Bifocal lens. Standard Progressive lens covered-fund PremiumProgressive as a Standard. Premium progressives and premium anti-reflective designations are subject to annual review by EyeMed’s Medical Director and are subject to change based onmarket conditions. Fixed pricing is reflective of brands at the listed product level. All providers are not required to carry all brands at all levels. Underwritten by Fidelity Security Life InsuranceCompany of Kansas City, Missouri, except in New York. This is a snapshot of your benefits. The Certificate of Insurance is on file with your employer. Benefit allowance provides no remainingbalance for future use within the same benefit year. **Based on industry averages.
85%SAVINGSwith us
With Us Without Insurance**
Frame $163 Frame $163
-$130 allowance
$33
-$6.60 (20% discount off balance)
$26.40
Total $61.40 Total $395
$10 Copay Up to $50
$0 Copay; $130 allowance; 80% of charge over $130 Up to $74
$10 Copay Up to $42
$0 Copay; $105 allowance; plus balance over $105 Up to $84
Frames (Once every 24 months)
Or
Single Vision Lenses (Once every 12 months)
Contacts (Once every 12 months)


![Uniform Medical Plan coverage limits€¦ · The Uniform Medical Plan (UMP) ... Uniform Medical Plan [UMP], Medicare Advantage) and the Blue Cross and Blue Shield Federal Employee](https://img.pdfslide.net/doc/110x75/5f96691c9c795f3a6a6c7606/uniform-medical-plan-coverage-limits-the-uniform-medical-plan-ump-uniform.jpg)


























