Embed Size (px)
Citation preview

BENIGN DISEASES OF THE THYROID
Rivka Dresner Pollak M.D
Endocrinology.

Thyroid gland- anatomyThyroid gland- anatomy

Thyroid gland- anatomyThyroid gland- anatomy
sternocleidomastoidsternocleidomastoid
thyroidthyroid
esophagus
tracheatrachea
jugular v.
carotid a.carotid a.
strap musclesstrap muscles
vertebra


Recommended and Typical Values for Dietary Iodine Intake
Recommended Daily Intake μg I/dayAdults 150During pregnancy 200Children 90-120
Typical Iodine intakesNorth America 75-300Europe (Germany, Belgium) 50-70Switzerland 130-160Chile <50-150


Thyroid secretion
P
ProteinBound
Thyroidhormone
Free T4, T3 Tissue actionTissue action
Hormone metabolismHormone metabolism
Fecal excretionFecal excretion
Serum thyroid hormone bindingSerum thyroid hormone binding
Feedback controlFeedback control

TBG = thyroxine binding globulinTTR = transthyretin% binding- mostly to TBGT4 - 99.5T3- 95
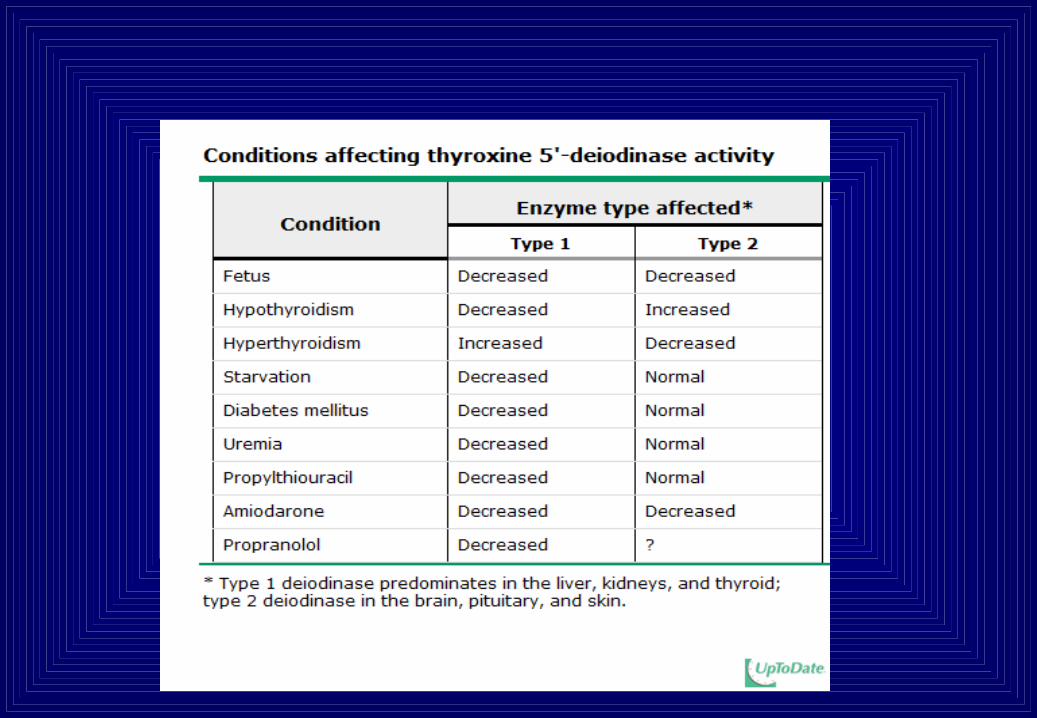
DEIODINASETYPE 1 & 2
THYROXINE BINDING GLOBULIN
Estrogen
Androgen =
Glucocorticoids =
Acute illness N
Chronic illness
Liver dis.
METABOLISM
TRANSPORT
THYROID HORMONES TRANSPORT AND METABOLISM

Serum protein binding of thyroid hormonesSerum protein binding of thyroid hormones
Total TTotal T44
TBG T4T4T4
TBG T4T4 T4 T4T4
““Pill effect”Pill effect”
BoundBound Free Free
synthesisBy liver

Regulation of Thyroid hormone secretionRegulation of Thyroid hormone secretion
Hypothalamus
TT44, T, T33
TSHTSH(-)(-) (+)(+)
TRHTRH(+)(+)(-)(-)
PituitaryPituitary
Thyroid

Assessment of bioactive thyroid Assessment of bioactive thyroid hormoneshormones
Check free hormone levels:Check free hormone levels:Free TFree T44
Free TFree T33
Check thyroid hormone “biosensor’:Check thyroid hormone “biosensor’:TSH TSH

Thyroid function testsThyroid function tests
Hypo HyperHypo Hyper Hypo HyperHypo Hyper 11oo Hypo 1 Hypo 1oo Hyper Hyper
TSHTSHFTFT33nmol/Lnmol/L
FTFT44
pmol/Lpmol/L
0.15
4
3.0
1.2
21
10

Laboratory tests in thyroid diseaseLaboratory tests in thyroid disease
Anti-thyroid antibodies:Anti-thyroid peroxidase (TPO)
Thyroid stimulating antibodies:TSI-Thyroid stimulating imunoglobulinsTSH receptor Antibody
Thyroglobulin

2. Thyroid scanning2. Thyroid scanning
Radioactive isotopes of I (Radioactive isotopes of I (131131I, I, 123123I)I)PertechnetatePertechnetate
Generates Data on:Generates Data on:- Anatomy- Anatomy- Physiology- Physiology

Normal thyroid scanNormal thyroid scan

““Hot nodule”Hot nodule”

““Cold” noduleCold” nodule

Multinodular goiter (MNG)Multinodular goiter (MNG)
Pertechnetate scanPertechnetate scan CHEST X-RAYCHEST X-RAY

RRadio adio AActive ctive IIodine odine UUptake ptake ((RAIURAIU))
0 6 12 18 240
10
20
30
40
50
Time (hours)
HyperthroidismHyperthroidism
NormalNormal
Hyperthyroidism withHyperthyroidism withRapid turnoverRapid turnover
HypothroidismHypothroidism
2

Thyroid abnormalitiesThyroid abnormalities
FunctionFunctionStructureStructure
Hyperthyroidism Hypothyroidism
EtiologyEtiology
RRXX
ThyroiditisThyroiditisGoiterGoiter
NodularNodular Diffuse Diffuse
BenignBenign MalignantMalignant Function nl Function nl

Hyperthyroidism-EtiologyHyperthyroidism-Etiology
• Diffuse toxic goiter (Graves’ disease)- most common in young people• Toxic adenoma (Plummers’ diesease)• Toxic mulitinodular goiter (MNG)• Subacute thyroiditis-Hyperthyroid phase• Hyperthyroid phase of Hashimotos’ thyroiditis• (“Hashitoxicosis)• Factitious hyperthyroidism• Rare causes: -TSHoma
-Hydatidiform mole/choriocarcinoma- Multiplex pregnancy- Struma ovarii

Graves’ diseaseGraves’ disease• Diffuse toxic goiterDiffuse toxic goiter
• OpthalmopathyOpthalmopathy
• DermopathyDermopathy
•Acropathy Acropathy
(clubbing)(clubbing)Etiology: AutoimmuneAnti-TSH receptor antibodies (stimulating, blocking, neutral)Anti-thyroid antibodies expression of HLA-DR3 association with:
-diabetes mellitus-type 1 myasthenia gravis-Addison’s disease lupus- pernicious anemia

• Epidemiology : incidence 0.3-1.5/1000
• Female: Male 5:1
• Most Common cause of hyperthyroidism
Graves’ diseaseGraves’ disease

Thyroid and pituitary function in Thyroid and pituitary function in Graves’ diseaseGraves’ disease
TT44, , TT33 TSHTSH(+)(+) (-)(-)
(+)(+)
Thyroid Stimulating Thyroid Stimulating Immunoglobulins (TSI)Immunoglobulins (TSI)

Graves’ disease- Graves’ disease- Clinical featuresClinical features
Symptoms:
Fatigue palpitationsWeight lossHeat intoleranceFrequent bowel movementsSweatinghyperkinesia
Signs:
TachycardiaMuscle wasting pulse pressureEye signsDiffuse goiterLymphadenopathySplenomegalyHyperreflexia
In the elderly: cardiovascular symptoms, myopathy

Graves’ Disease- GoiterGraves’ Disease- Goiter

Graves disease- Graves disease- OpthalmopathyOpthalmopathy
Extrathyroidal TSHR is present in retro-orbital adipocytes, muscle cells and fibroblasts

Grave’s Opthalmopathy
• Class 0 — No symptoms or signs • Class I — Only signs, no symptoms (eg, lid
retraction, stare, lid lag) • Class II — Soft tissue involvement • Class III — Proptosis • Class IV — Extraocular muscle involvement • Class V — Corneal involvement • Class VI — Sight loss (optic nerve involvement)

Graves’ disease dermopathyGraves’ disease dermopathy

Graves disease- diagnosisGraves disease- diagnosis
• Clinical hyperthyroidism
• Biochemistry: FT4, TT3 , TSHcholesterol
• Serology: anti-TSH receptor antibodiesanti-thyroid antibodies

Graves’ disease- therapyGraves’ disease- therapy1. Antithyroid drugs:
Thionamides- Propylthiouracil (PTU)Propylthiouracil (PTU)Methimazole (MMI)Methimazole (MMI)-blockers
3. Definitive therapy:131I- side effects:
hypothyroidism
Surgery- subtotal thyroidectomy
side effects: anesthesia morbidityhypoparathyroidismrecurrent laryngeal nerve damagehypothyroidism
Treat for 12 monthsTreat for 12 months
~30%remissionremission70%
RecurrenceOr non-remission
Follow-upFollow-up

Anti-thyroid thionamide drugsAnti-thyroid thionamide drugs
PTU (propylthiouracil) MMI (methimazole)
Dosage: TID Once daily
Effect: T4, T3 synthesis T4, T3 synthesis
inhibits T4→T3(high dose) (slow)
Agranulocytosis*: Non-dose dependent Dose dependent
(> 40 mg/day)
> 40 yrs
Pregnancy: placental transfer placental
transfer
aplasia cutis
*occurrence 0.3-0.6%

Treatment of Graves' Orbitopathy
• Treatment of patients with Graves' orbitopathy has three components:
• Reversal of hyperthyroidism, if present • Symptomatic treatment • Treatment with a glucocorticoid, orbital irradiation,
orbital decompression surgery to reduce inflammation in the periorbital tissues
• Anti thyroid drugs and thyroidectomy are safe; Radioactive iodine may worsen the situation.

The effect of high- dose PTUThe effect of high- dose PTU
0 1 2 3 4 5 620
25
30
35
40
45
50 FT4
FT3
012345678910
Days
12001200 600600PTU dose mg/day:
Upper limit of normal
Normalrange
140
120
100
80
Pulse rate:

Subacute thyroiditisSubacute thyroiditis
Etiology: (Post) viral inflammation of thyroid
Symptoms & signs: HyperthyroidismPainful swelling of thyroidPain irradiation to earFeverSometimes “silent”
Laboratory: ESR acute phase reactants (CRP)


Subacute thyroiditis- therapySubacute thyroiditis- therapy
A self limited disease
Therapy depends on symptoms/signs
Non-steroid anti-inflammatory agents (NSAIDS)
-blockers
Corticosteroids
Outcome - in 6 months 90% euthytroid

Hypothyroidism- classificationHypothyroidism- classification
1. Hashimoto’s thyroiditis2. Post 131I therapy for Grave’s disease3. Post thyroidectomy4. Excessive I intake (amiodarone-procor)
Primary - TSH↑
Secondary TSH ↓ or normal:Hypopituitarism due to adenoma, destructive lesion, ablationTSH↓
Tertiary:Hypothalamic dysfunction (rare)

Hypothyroidism- Hypothyroidism- clinical featuresclinical features
Symptoms:
Fatigue WeaknessWeight gainCold intoleranceConstipationCrampsParesthesias (carpal tunnel)
Signs:
Coarse featuresBradycardiaMyxedemaAnemia
Laboratory: serum thyroid hormones, cholesterolanemia (iron def., megaloblastic)

HypothyroidismHypothyroidism

Hypothyroidism- myxedemaHypothyroidism- myxedema
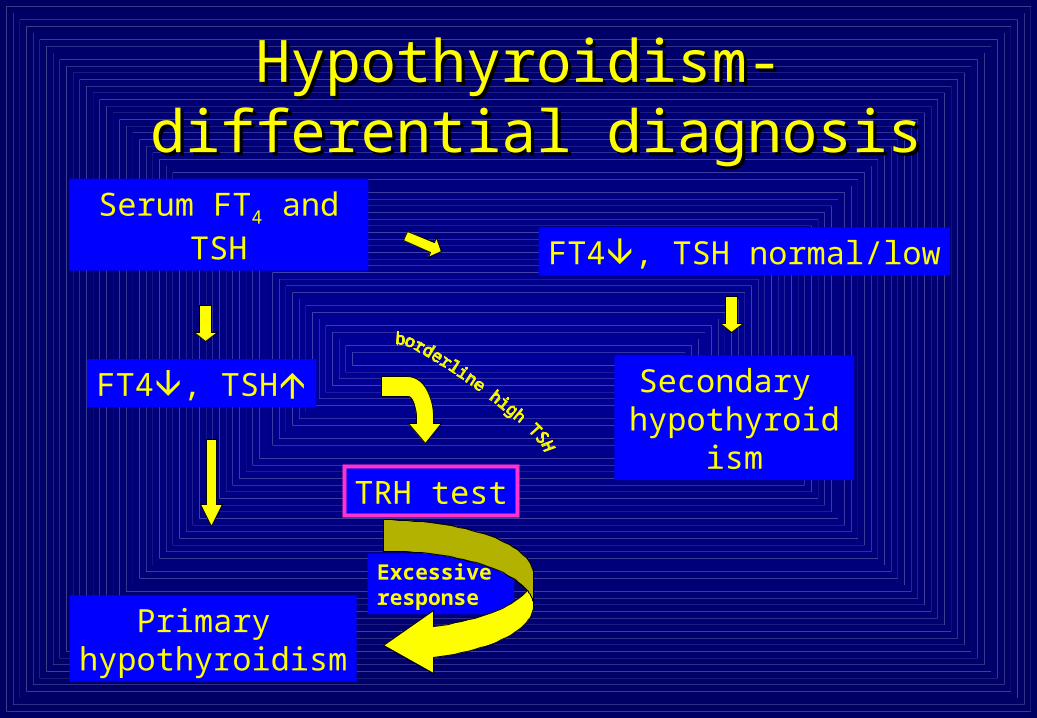
Hypothyroidism-Hypothyroidism- differential diagnosis differential diagnosis
Serum FT4 andTSH
FT4, TSH
Primary hypothyroidism
FT4, TSH normal/low
Secondary hypothyroidism
TRH test
Excessive response

Hypothyroidism- therapyHypothyroidism- therapy
• Levothyroxine 0.05-0.3 mg/day
• Combined L-T4 and L-T3 may be beneficial with
respect to well-being
• In elderly patients (at high risk for CVD),
“go low, go slow”
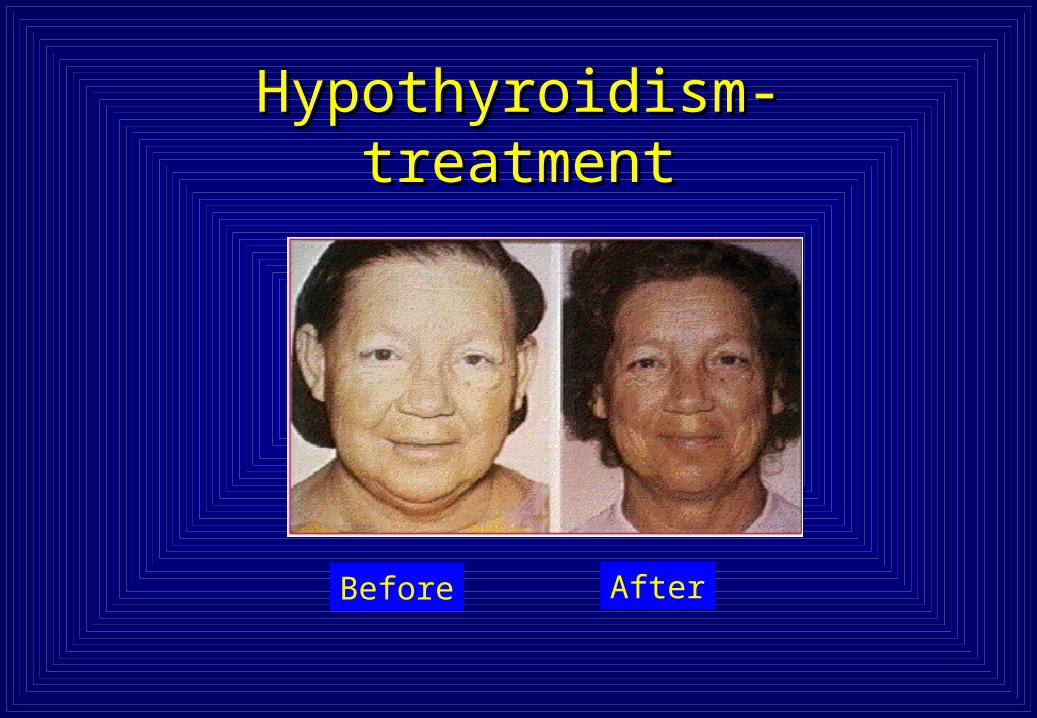
Hypothyroidism- treatmentHypothyroidism- treatment
Before After

Thyroid Storm and Myxedema Coma – rare endocrine emergencies

THYROID STORM
Clinical setting
History of Graves’ disease and discontinuation of medications/
previously undiagnosed hyperthyroidism.
Acute onset of hyperpyrexia (over 40 ˚C)
Sweating
Marked tachycardia, often with atrial fibrillation
Nausea, vomiting, diarrhea
Agitation, tremulousness, delirium
Occasionally “apathetic” – without restlessness and agitation, but with
weakness, confusion, and cardio-vascular dysfunction.
Acute life threatening exacerbation of thyrotoxicosis
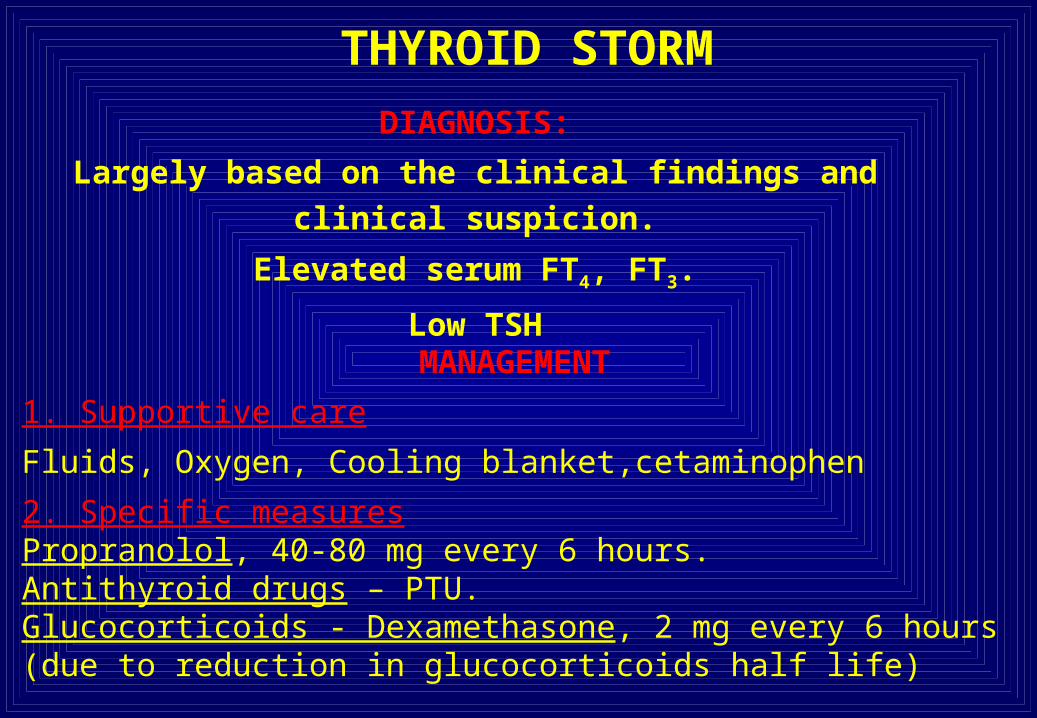
THYROID STORMDIAGNOSIS:
Largely based on the clinical findings and clinical suspicion.
Elevated serum FT4, FT3.
Low TSH
MANAGEMENT
1. Supportive care
Fluids, Oxygen, Cooling blanket,cetaminophen
2. Specific measuresPropranolol, 40-80 mg every 6 hours.Antithyroid drugs – PTU. Glucocorticoids - Dexamethasone, 2 mg every 6 hours (due to reduction in glucocorticoids half life)

Myxedema ComaMyxedema ComaExtreme hypothyroidism:
• Coma• Hypothermia• Hypoventilation• Hypoglycemia• Hyponatremia• Bradycardia
Laboratory: FT4 , FT3, TSHCo2 retention

Myxedema Coma- therapyMyxedema Coma- therapy
Treat:
Ventilation
Precipitating factors
T4 or T3 I.V.Corticosteroids-50-100mg hydrocortisoneevery 8 hours

Subclinical Hypothyroidism
TSH FT4 AND FT3 NORMAL
Biochemical definition
WHEN TO TREAT?WHEN TSH > 10AND WHAT ABOUT 4.5<TSH<10????

TSH 4.5-10

Subclinical hyperthyroidism• TSH below lower limit of normal (<0.3)
• Free T3 & Free T4 – normal
• Make sure not over treatment of hypothyroidism
• Associated with increased risk of atrial fibrillation in subjects > age 60 and accelerated bone loss in postmenopausal women

Always repeat the test
before initiating
therapy!

Amiodarone (Procor)-induced thyroid dysfunction
• Each Procor tablet (200 mg) has 75 mg Iodine• Procor can cause: hypothyroidism- does not require discontinue the
medication (thyroxine can be added)Hyperthyroidism- anti thyroid drugs have limited
efficacy; radioactive iodine doesn’t workThyroiditis- may require steroids
»

















![Max Weber [m. Pollak]](https://img.pdfslide.net/doc/110x75/55cf97af550346d03392ffa1/max-weber-m-pollak.jpg)











