Embed Size (px)
Citation preview


Rohan Hall
Goldfields Urology
Bendigo
Full Steam Ahead

Full Stream Ahead

LUTS
Age <45 – 20%
Age 65-79 – 48%
Age 80> - 70%
OAB (urgency, frequency, nocturia, UUI)
BOO (hesitancy,poor flow, incomplete emptying)
BPH
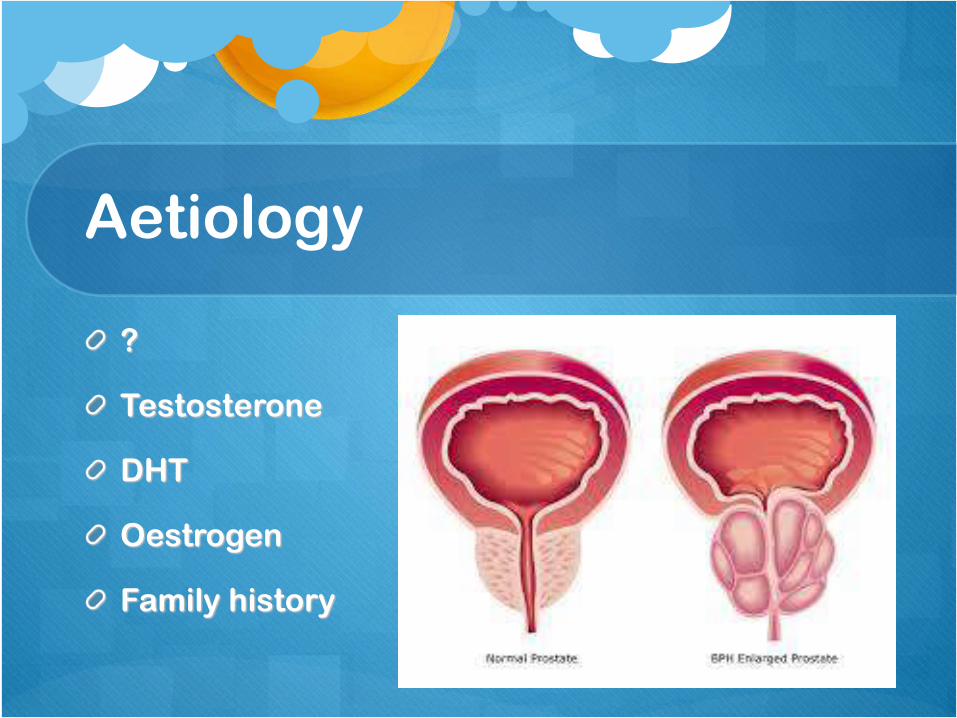
Aetiology
?
Testosterone
DHT
Oestrogen
Family history
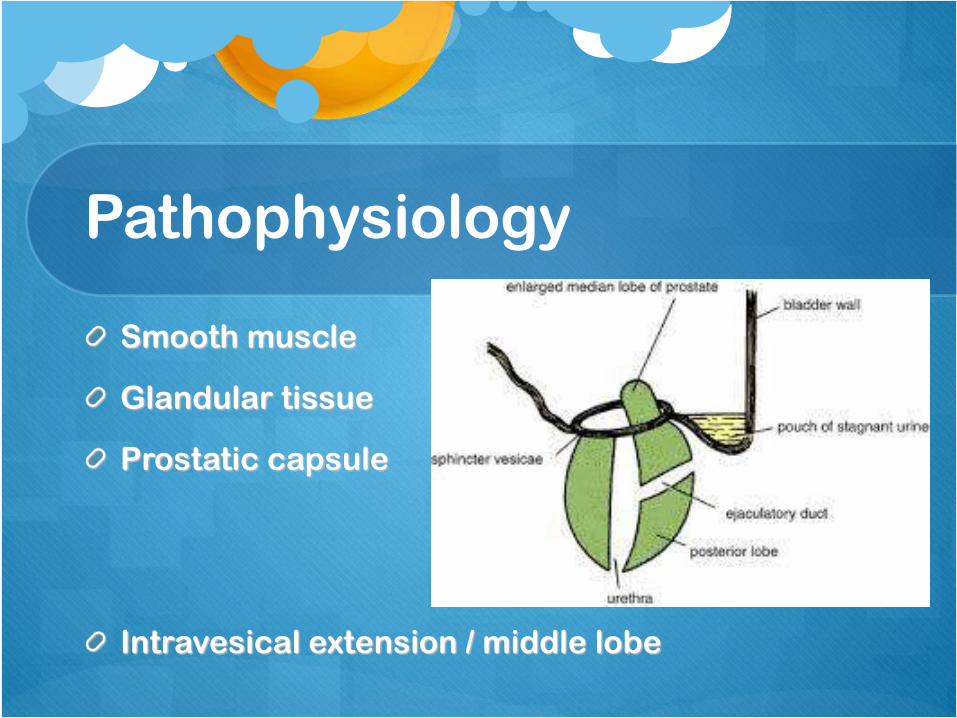
Pathophysiology
Smooth muscle
Glandular tissue
Prostatic capsule
Intravesical extension / middle lobe

Clinical Sequelae
OAB – Urgency and urge incontinence
Urinary retention
Detrusor failure
UTI
High pressure storage or voiding – renal failure
Ejaculatory dysfunction

Medical Management
Smooth muscle
Alpha blockade
- selective
Glandular tissue
Dutasteride/fina
steride
OAB / detrusor
irritability
Ditropan
Vesicare
Betmiga
Diet

Surgical Management
Divide high bladder neck
Resect intravesical middle lobe
Dilemma:
Retrograde ejaculation
Urethral stricture
Urgency/Urge Urinary Incontinence
Risk of anaesthetic

Open Prostatectomy
Traditional approach prior to endoscopy
Large prostates
Pro’s – tissue for examination, less risk to
urethra
Con’s – surgical risk, incontinence risk,

TURP
“Re-bore”
“ Coring out an apple”
“Gold Standard”
Pro’s – physically remove obstruction, tissue for pathology
Con’s – issues with large glands, retrograde ejaculation, anticoagulation, stricture

Laser Ablation
Vaporisation
Pro’s – anticoagulation, 19Fr sheath
Con’s – anticoagulation, length of operation,
urethral strictures, no tissue for pathology,
depth of ablation, need for second procedure

Urolift
“0% sexual side effects”
Better for smaller gland
Less bleeding
In reality…….
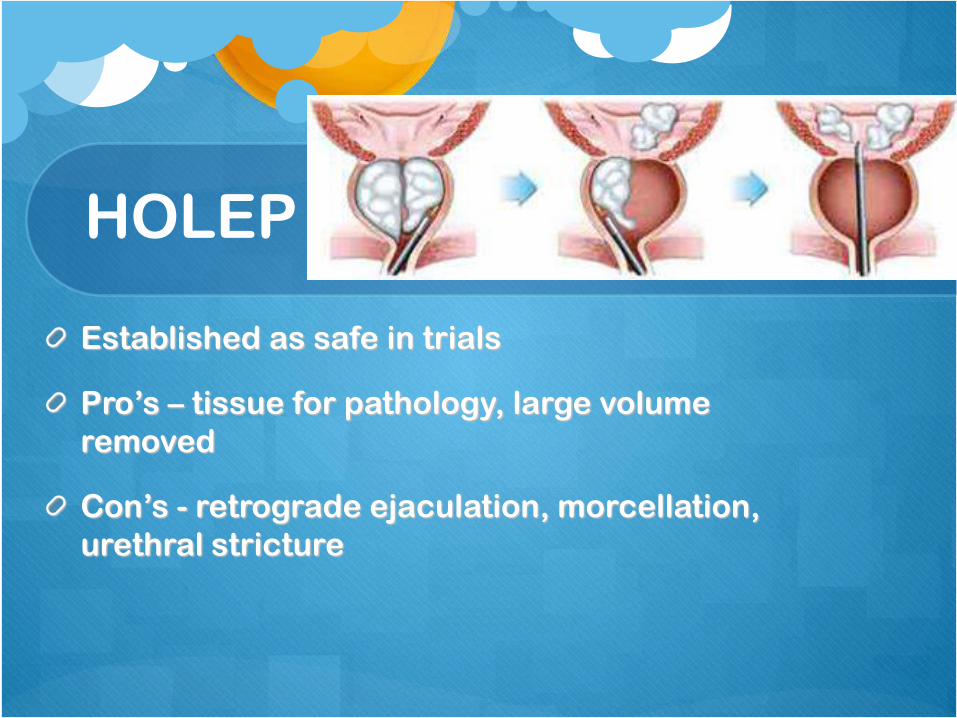
HOLEP
Established as safe in trials
Pro’s – tissue for pathology, large volume
removed
Con’s - retrograde ejaculation, morcellation,
urethral stricture

Hydrodissection
New
Aquablation
Dissection versus ablation

Embolisation
Controversial
Proven for menorrhagia
Erectile dysfunction

CBI
Why?
Virchow’s triad
Solution
2 bags – why
Counting bags
Titration

Recovery – tips
Bladder spasm – ditropan (2.5-5mg prn)
Traction
Manual washout

Questions?