Embed Size (px)
Citation preview
RECENT UPDATE OF BETA-BLOCKERS IN
AMI & HFBeta-blockade today:Beta-blockade today:
the gap between evidence and practicethe gap between evidence and practice
DR A.SAI RAVI SHANKER
MD.DM
INTERVENTIONAL CARDIOLOGIST
SWETHA HOSPITAL
Beta – blockers still WONDER us !!!Beta – blockers still WONDER us !!!
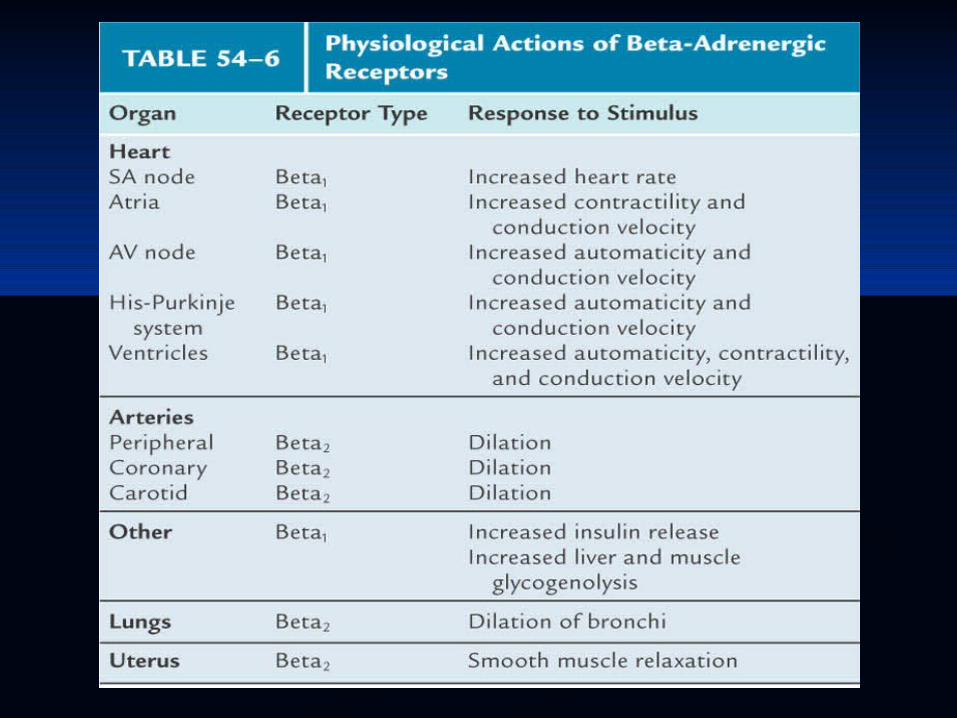
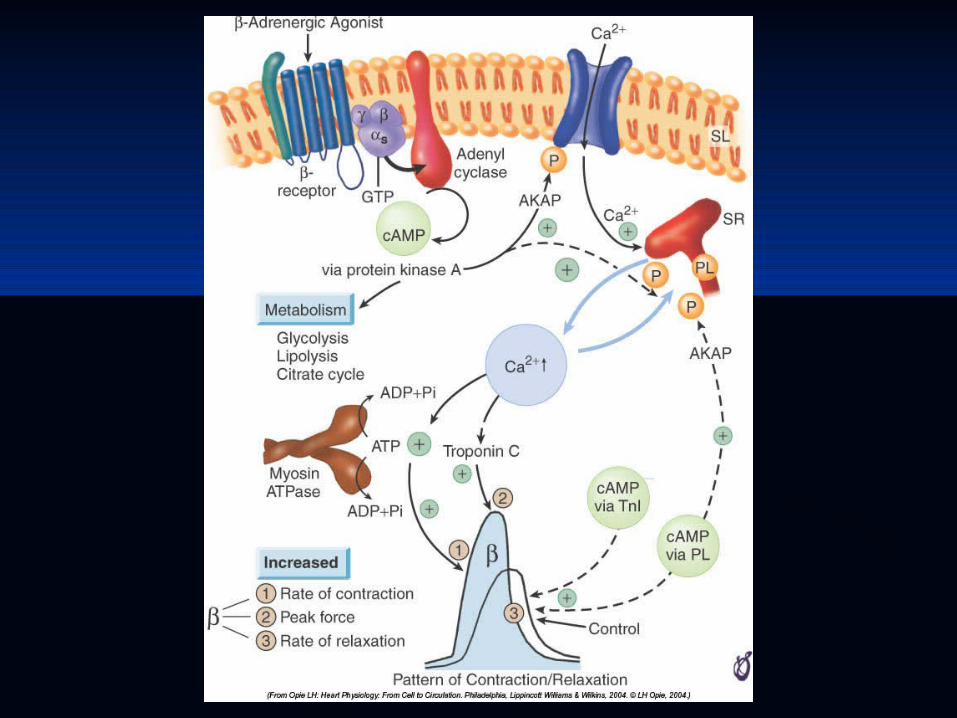
Beta ReceptorsBeta Receptors
Beta 1Beta 1 - on cardiac scarcolemma - on cardiac scarcolemma
- coupled by G protein system - coupled by G protein system
- cAMP activation- cAMP activation
- opening of calcium channels- opening of calcium channels
Positive - inotropic, chronotropic, lusitropic Positive - inotropic, chronotropic, lusitropic effect, dromotropic effecteffect, dromotropic effect
Beta 2Beta 2 – on bronchial and vascular smooth – on bronchial and vascular smooth muscle - relaxationmuscle - relaxation
Increased in heart failureIncreased in heart failure
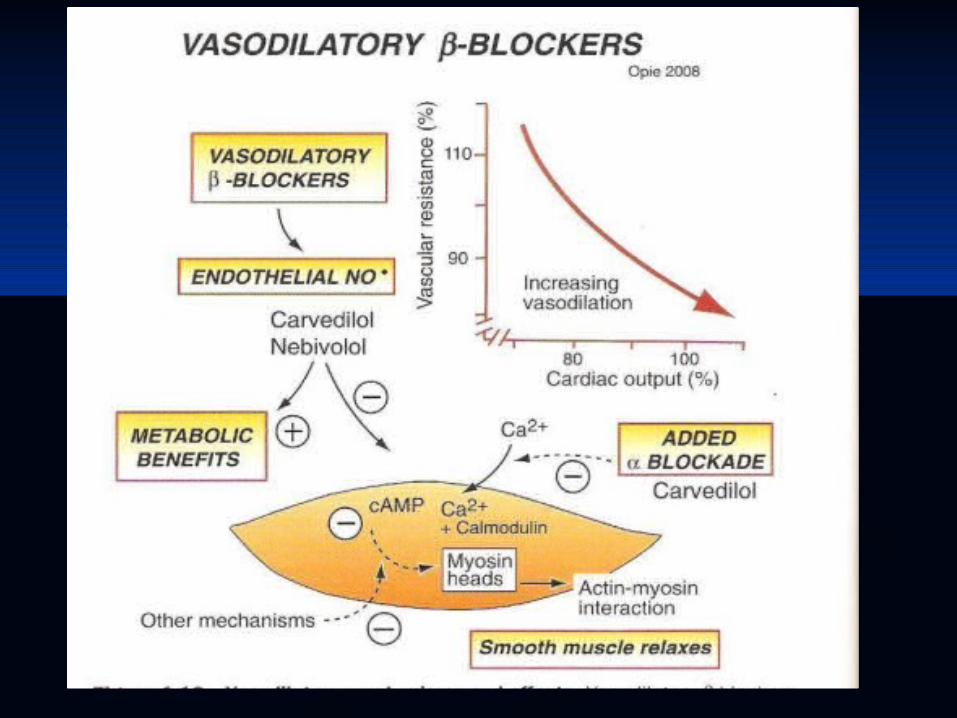
Beta 3Beta 3 – mediate vasodilatation by release of – mediate vasodilatation by release of nitric oxidenitric oxide
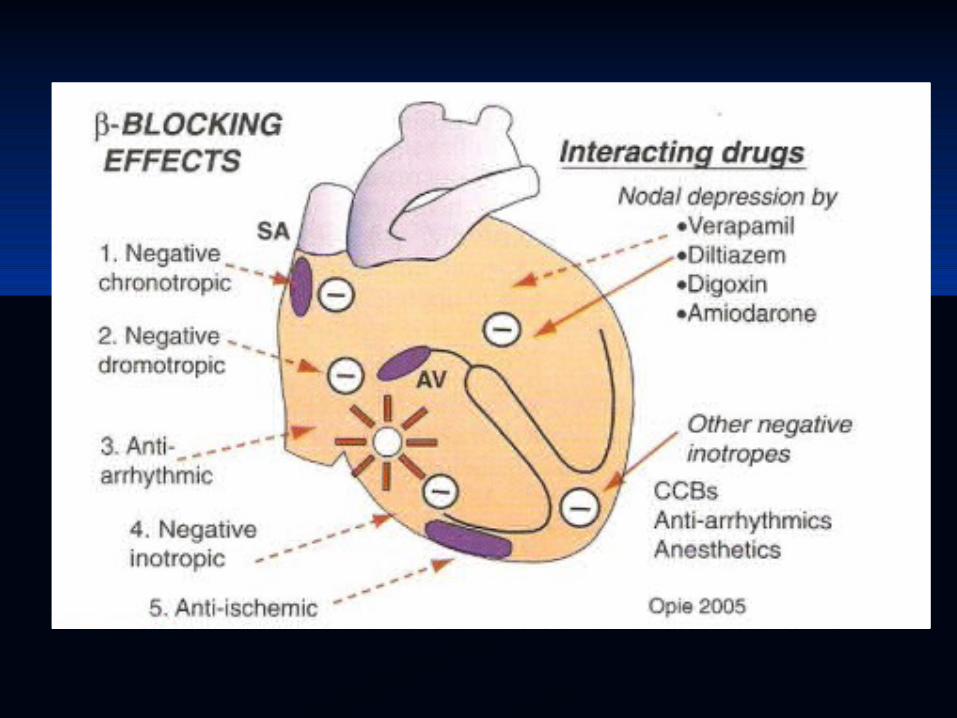
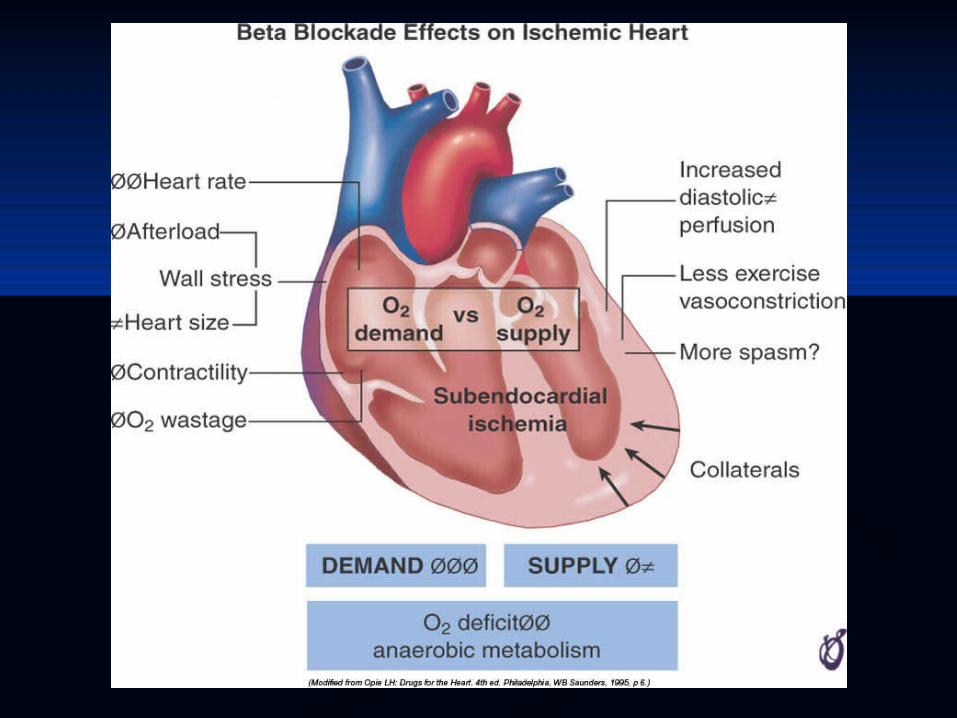
Anti-ischaemic Effects of Anti-ischaemic Effects of betablockadebetablockade
Negative inotropic, chronotropic and Negative inotropic, chronotropic and dromotropic effectdromotropic effect
Decreases myocardial oxygen demandDecreases myocardial oxygen demand Decrease in heart rate – long diastolic Decrease in heart rate – long diastolic
myocardial perfusionmyocardial perfusion
• Background• Tachycardia as an independent risk factor• Beta blocker therapy (angina, post- infarction, heart failure,
hypertension, diabetes)
• Are all beta blockers alike?• Adverse effects (fatigue, CHF, cold feet, diabetes)
• What do the guidelines say?
Re-Exploring the Role of Beta Re-Exploring the Role of Beta Blockers in secondary preventionBlockers in secondary prevention
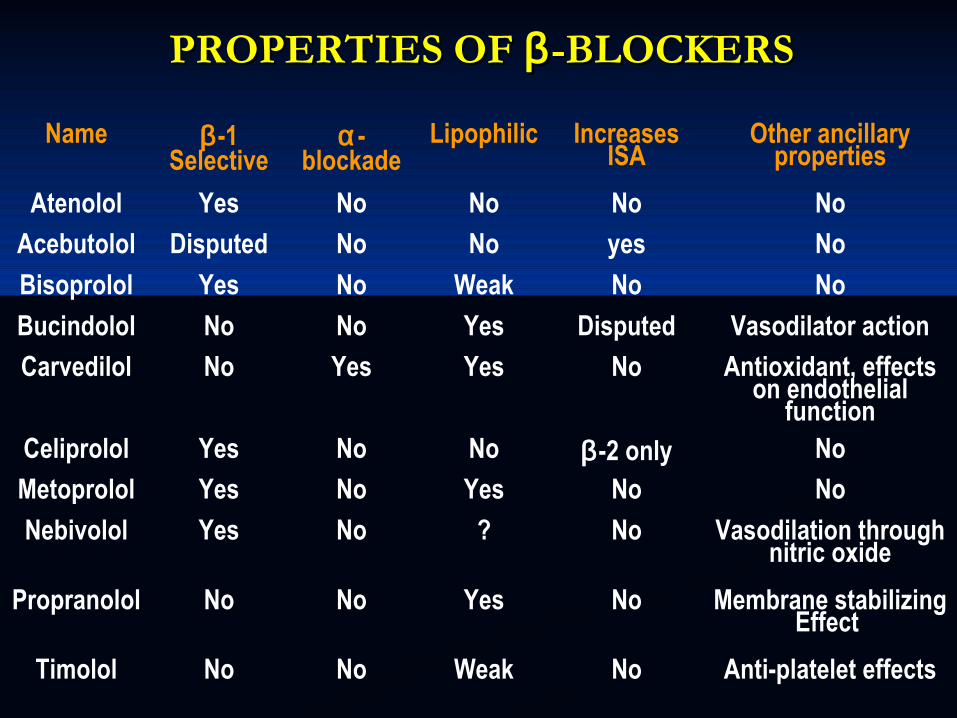
PROPERTIES OF PROPERTIES OF ββ -BLOCKERS-BLOCKERS
Name β -1 Selective
α -blockade
Lipophilic Increases ISA
Other ancillary properties
Atenolol Yes No No No No
Acebutolol Disputed No No yes No
Bisoprolol Yes No Weak No No
Bucindolol No No Yes Disputed Vasodilator action
Carvedilol No Yes Yes No Antioxidant, effects on endothelial
functionCeliprolol Yes No No β -2 only No
Metoprolol Yes No Yes No No
Nebivolol Yes No ? No Vasodilation through nitric oxide
Propranolol No No Yes No Membrane stabilizing Effect
Timolol No No Weak No Anti-platelet effects
Other cardiac indicationsOther cardiac indications
HOCMHOCM Mitral stenosis in sinus rhythmMitral stenosis in sinus rhythm Mitral valve prolapse syndromeMitral valve prolapse syndrome Dissecting aneurysmDissecting aneurysm Neurocardiogenic syncopeNeurocardiogenic syncope Cyanotic spellsCyanotic spells Congenital prolonged QT syndromeCongenital prolonged QT syndrome Catecholaminergic polymorphic VTCatecholaminergic polymorphic VT
Noncardiac indicationsNoncardiac indications
Perioperative hypertension- esmololPerioperative hypertension- esmolol Thyrotoxicosis -propranololThyrotoxicosis -propranolol MigraineMigraine Anxiety statesAnxiety states Open angle Glaucoma –timololOpen angle Glaucoma –timolol Oesophageal varicesOesophageal varices
Side effectsSide effects
BronchospasmBronchospasm Cold extremitiesCold extremities Worsening of claudicationWorsening of claudication Bradycardia, heart blocksBradycardia, heart blocks InsomniaInsomnia DepessionDepession Erectile dysfunction (11-26%) Erectile dysfunction (11-26%) Metabolic side effectsMetabolic side effects
Contraindications Contraindications
Severe bradycardiaSevere bradycardia High degree heart blockHigh degree heart block Cardiogenic shockCardiogenic shock Overt untreated LVFOvert untreated LVF Severe asthmaSevere asthma Severe depressionSevere depression PVD , Raynauds phenomenonPVD , Raynauds phenomenon
• Background• Tachycardia as an independent risk factor• Beta blocker therapy (angina, post- infarction, heart failure,
hypertension, diabetes)
• Are all beta blockers alike?• Adverse effects (fatigue, CHF, cold feet, diabetes)
• What do the guidelines say?
Re-Exploring the Role of Beta Re-Exploring the Role of Beta Blockers in secondary preventionBlockers in secondary prevention
Determinants of resting heart rateDeterminants of resting heart rate
• Circulating hormones • Level of physical fitness • The autonomic nervous system
sympathetic- vagal balance
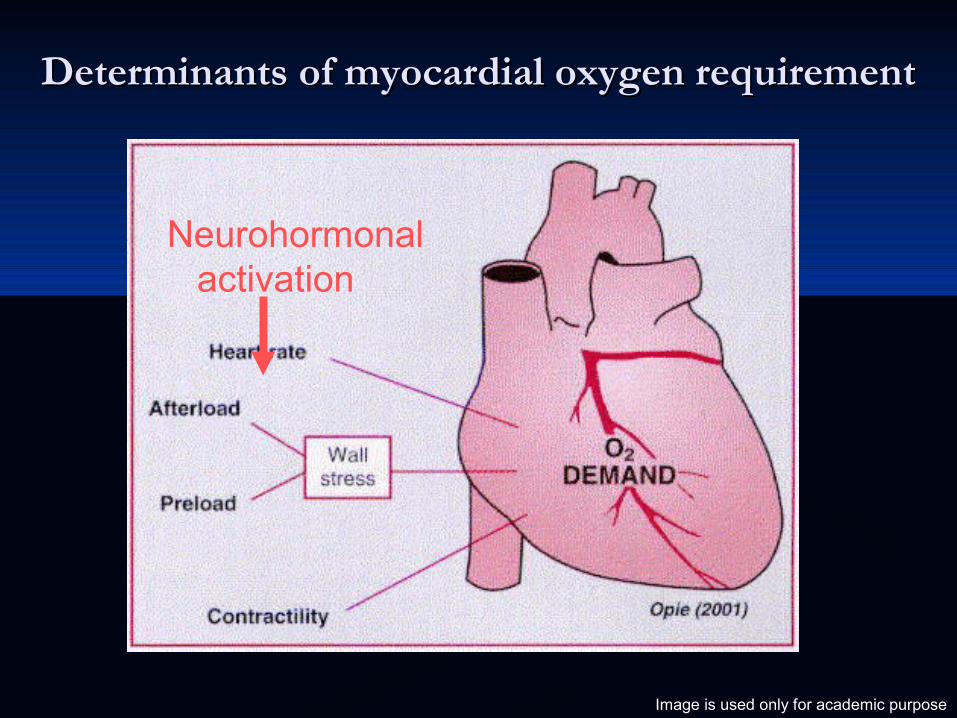
Determinants of myocardial oxygen requirementDeterminants of myocardial oxygen requirement
Neurohormonal activation
Image is used only for academic purpose
Resting heart rate and mortalityResting heart rate and mortalityThe Copenhagen Male StudyThe Copenhagen Male Study
• A low heart rate is associated with a high level of physical fitness
• Resting heart rate is a risk marker for mortality independent of physical fitness
• Resting heart rate above 90 bpm confers a 3 fold increase in mortality compared to men with heart rate ≤50 beats per minute (bpm)
• Elevated resting heart rate is associated with an increased risk• • 16% increase in mortality per 10 bpm increase in resting heart
rate
Jensen MT Heart 2013; 99:882
Tachycardia is a risk factorTachycardia is a risk factor
Heart rate impacts:
-Myocardial oxygen requirement - Myocardial ischemia -Cardiac function
-Coronary plaque stability -Infarct size -Sudden death
ACC 2013: Major ACC 2013: Major Clinical Trials ResultsClinical Trials Results
Beta-Blocker Therapy in Acute Beta-Blocker Therapy in Acute Myocardial Infarction: Myocardial Infarction:
How to Give Good CareHow to Give Good Care
Betablockers in MIBetablockers in MI
� AtenololAtenolol� MetoprololMetoprolol� PropranololPropranolol� CarvedilolCarvedilol� Timolol Timolol
� Reduces myocardial O2 Reduces myocardial O2 consumptionconsumption
� Reduces infarct sizeReduces infarct size� AntiarrhythmicAntiarrhythmic� Decreases catecholamine Decreases catecholamine
induced FFA –reduction in induced FFA –reduction in O2 consumption and O2 consumption and arrhythmiasarrhythmias
Metaanalysis of 26 trials, MIAMI, ISIS, Metaanalysis of 26 trials, MIAMI, ISIS, COMMIT TrialsCOMMIT Trials
� Death 13%Death 13%
� Reinfarction 22%Reinfarction 22%
� Sudden cardiac death 15%Sudden cardiac death 15%
Chadda et al, Circulation 1986; 73:503
Beta Blocker Heart Attack Beta Blocker Heart Attack Trial (BHAT) 1986Trial (BHAT) 1986
� 3,837 patients randomized3,837 patients randomized� Propranolol or placebo and followed for 25 Propranolol or placebo and followed for 25
monthsmonths
– Propranolol significantly reduced:Propranolol significantly reduced:» total mortalitytotal mortality» cardiovascular mortalitycardiovascular mortality» sudden deathsudden death» nonfatal infarctionnonfatal infarction
First ConclusionFirst Conclusion
� Multiple studies for over 20 years have Multiple studies for over 20 years have demonstrated:demonstrated:– Beta-blockers in patients PreThrombolytic Era Beta-blockers in patients PreThrombolytic Era
have a mortality benefit ranging between 10 have a mortality benefit ranging between 10 and 15%and 15%
Freemantle et al. Beta Blockade after Myocardial Infarction: Systematic Review and Meta Regression Analysis. BMJ 1999 318:1730
Beta Blockade after Beta Blockade after Myocardial Infarction - 1999Myocardial Infarction - 1999
� Meta analysis of 31 long-term trials Meta analysis of 31 long-term trials performed during the reperfusion era on performed during the reperfusion era on almost 25,000 patientsalmost 25,000 patients
� 10.1% reduction in overall mortality10.1% reduction in overall mortality
Final ConclusionFinal Conclusion� Large trials have demonstrated that beta-Large trials have demonstrated that beta-
blockers benefit all these AMI patient blockers benefit all these AMI patient groups groups – No reperfusion therapyNo reperfusion therapy– Thrombolytic therapyThrombolytic therapy– Percutaneous coronary interventionPercutaneous coronary intervention– CABGCABG
Caution #1: Caution #1: DocumentationDocumentation
� Failure to give a beta-blocker, with a good clinical Failure to give a beta-blocker, with a good clinical reason, and to then not appropriately document this, reason, and to then not appropriately document this, is often analyzed and publicly interpreted as is often analyzed and publicly interpreted as underuse, a gap in care or poor medical care.underuse, a gap in care or poor medical care.
� The further assumption is that these non- treated The further assumption is that these non- treated patients often suffered a higher unnecessary rate of patients often suffered a higher unnecessary rate of death and complications.death and complications.
The Practice Standard for Beta Blockers The Practice Standard for Beta Blockers makes two measurements and requires two makes two measurements and requires two chart documentations:chart documentations:
� Was it given in the first 24 hours?Was it given in the first 24 hours?
� Was the patient discharged on a BB?Was the patient discharged on a BB?
What are clinical situations where a beta-What are clinical situations where a beta-blocker should not be given and could hurt the blocker should not be given and could hurt the patient?patient?
Caution #2: Caution #2: Do No HarmDo No Harm
Contraindications to Beta-Blocker Use Contraindications to Beta-Blocker Use During Acute Myocardial InfarctionDuring Acute Myocardial Infarction
� Bradycardia -- heart rate less than 50Bradycardia -- heart rate less than 50� PR > . 24PR > . 24� Second or third degree atrioventricular blockSecond or third degree atrioventricular block� Pulmonary edemaPulmonary edema� HypotensionHypotension� ShockShock� Myocardial infarction precipitated by cocaine Myocardial infarction precipitated by cocaine
useuse� Active heart failureActive heart failure
The data of the recently The data of the recently completed COMMIT Trial completed COMMIT Trial reinforces that beta-blocker reinforces that beta-blocker
therapy should be withheld if the therapy should be withheld if the patient is at all unstable.patient is at all unstable.
Caution #3: Caution #3: Do Not Withhold Beta-Do Not Withhold Beta-
Blocker Therapy for Blocker Therapy for Inappropriate ReasonsInappropriate Reasons
� ElderlyElderly� Diabetes MellitusDiabetes Mellitus� NQMINQMI� CardiomyopathyCardiomyopathy� COPDCOPD
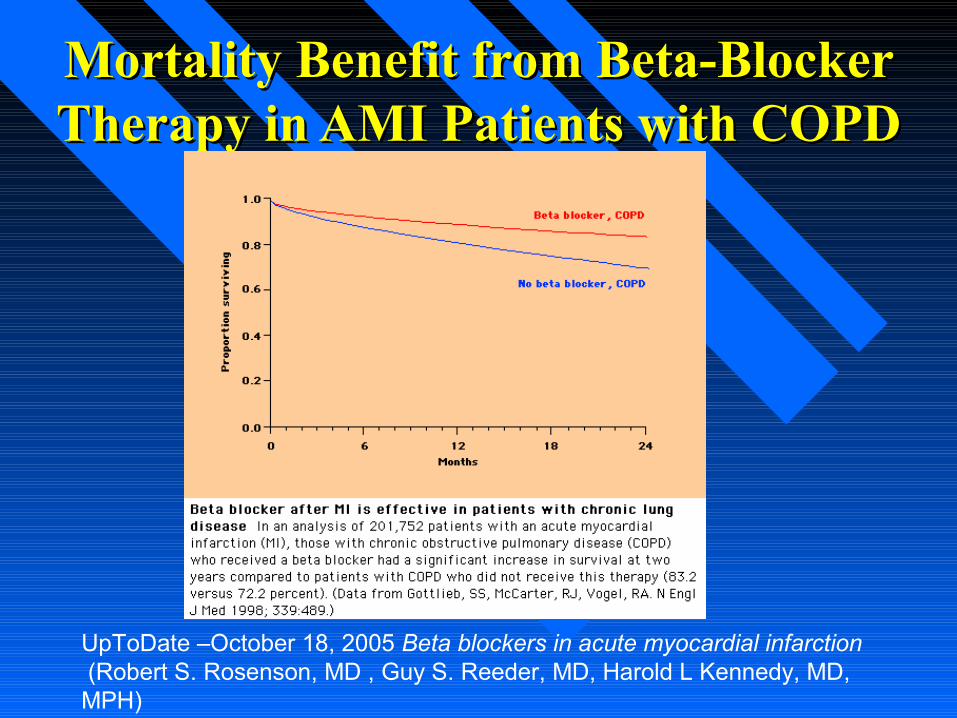
Mortality Benefit from Beta-Blocker Mortality Benefit from Beta-Blocker Therapy in AMI Patients with COPDTherapy in AMI Patients with COPD
UpToDate –October 18, 2005 Beta blockers in acute myocardial infarction (Robert S. Rosenson, MD , Guy S. Reeder, MD, Harold L Kennedy, MD, MPH)
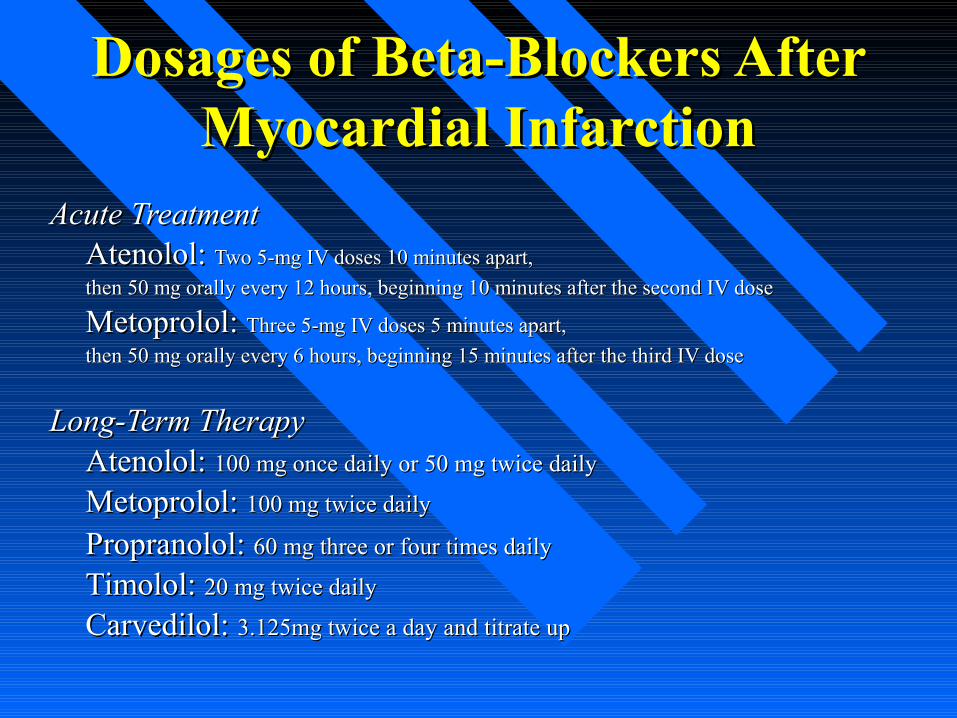
Acute TreatmentAcute Treatment Atenolol: Atenolol: Two 5-mg IV doses 10 minutes apart, Two 5-mg IV doses 10 minutes apart,
then 50 mg orally every 12 hours, beginning 10 minutes after the second IV dosethen 50 mg orally every 12 hours, beginning 10 minutes after the second IV dose
Metoprolol: Metoprolol: Three 5-mg IV doses 5 minutes apart, Three 5-mg IV doses 5 minutes apart,
then 50 mg orally every 6 hours, beginning 15 minutes after the third IV dosethen 50 mg orally every 6 hours, beginning 15 minutes after the third IV dose
Long-Term Therapy Long-Term Therapy Atenolol: Atenolol: 100 mg once daily or 50 mg twice daily100 mg once daily or 50 mg twice daily
Metoprolol: Metoprolol: 100 mg twice daily100 mg twice daily
Propranolol: Propranolol: 60 mg three or four times daily60 mg three or four times daily Timolol: Timolol: 20 mg twice daily20 mg twice daily
Carvedilol: Carvedilol: 3.125mg twice a day and titrate up3.125mg twice a day and titrate up
Dosages of Beta-Blockers After Dosages of Beta-Blockers After Myocardial InfarctionMyocardial Infarction
• Background
• Tachycardia as an independent risk factor• Beta blocker therapy (angina, post- infarction, heart
failure, hypertension, diabetes)
• Are all beta blockers alike?• Adverse effects (fatigue, CHF, cold feet, diabetes)
• What do the guidelines say?
Re-Exploring the Role of Beta Re-Exploring the Role of Beta Blockers in secondary preventionBlockers in secondary prevention
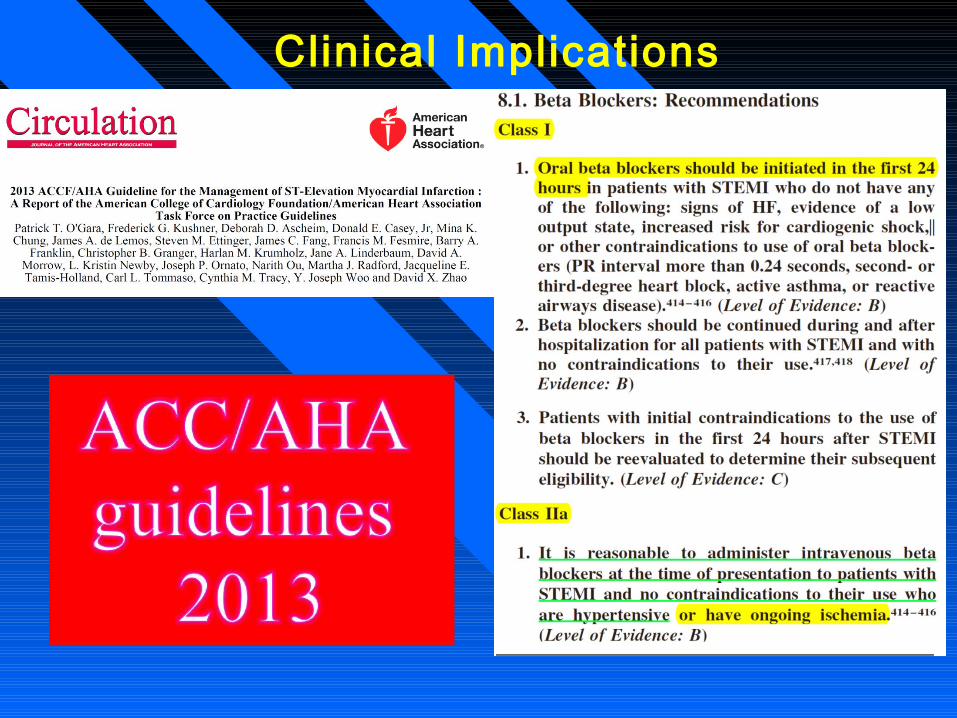
Clinical Implications
Conclusions
In Killip-I-II anterior STEMI patients reperfused by pPCI within 6 hours from symptoms onset, the early pre-reperfusion i.v. metoprolol administration results in:
•Reduced infarct size & slightly increased LVEF at one week.
•Increased long term LVEF (6 months MRI).
•Reduced cases of severely depressed.
•Trend for reduced long-term hard endpoints (driven by reduction of heart failure readmission)..
These results set the basis for a large RCT powered to detect differences in clinical endpoints (MOVE ON! trial).
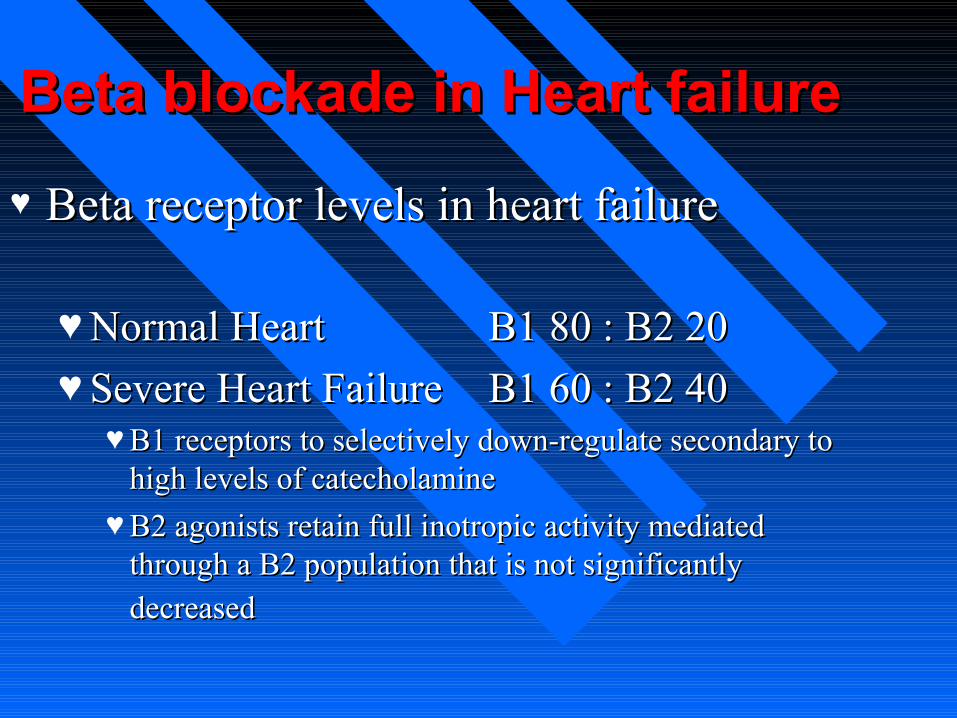
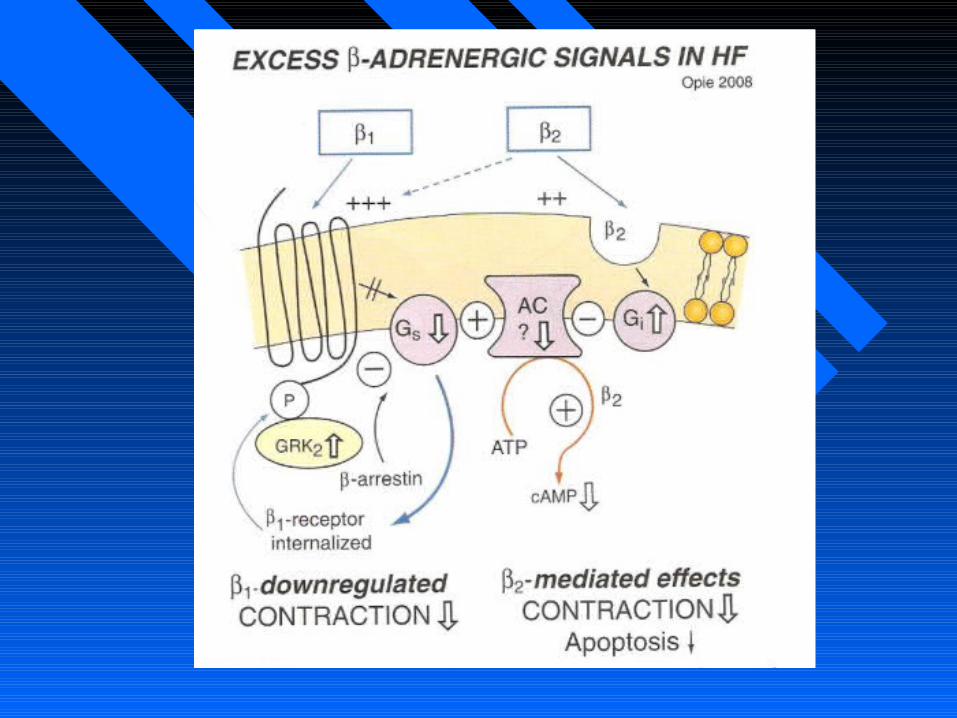
Beta blockade in Heart failureBeta blockade in Heart failure
♥ Beta receptor levels in heart failureBeta receptor levels in heart failure
♥Normal HeartNormal Heart B1 80 : B2 20B1 80 : B2 20
♥Severe Heart FailureSevere Heart Failure B1 60 : B2 40B1 60 : B2 40♥B1 receptors to selectively down-regulate secondary to B1 receptors to selectively down-regulate secondary to
high levels of catecholaminehigh levels of catecholamine
♥B2 agonists retain full inotropic activity mediated B2 agonists retain full inotropic activity mediated through a B2 population that is not significantly through a B2 population that is not significantly
decreaseddecreased
Effects of SNS Activation in Heart Failure
Dysfunction/death of cardiac myocytes
Provokes myocardial ischemia
Provokes arrhythmias
Impairs cardiac performance
These effects are mediated via stimulation
of β and α1 receptors
Am J Hypertens 1998; 11: 23S-37S
Betablocked in HFBetablocked in HF� Time dependant improvement in LV Time dependant improvement in LV
remodellingremodelling� Reduce cetecholamine myocyte toxicityReduce cetecholamine myocyte toxicity� Improved B1 signalingImproved B1 signaling� AntiapoptosisAntiapoptosis� antiarrthymicantiarrthymic� RAAS inhibitionRAAS inhibition� Decreases hyperphosphorylation of calcium Decreases hyperphosphorylation of calcium
release channels of SR and prevents calcium release channels of SR and prevents calcium leak.leak.
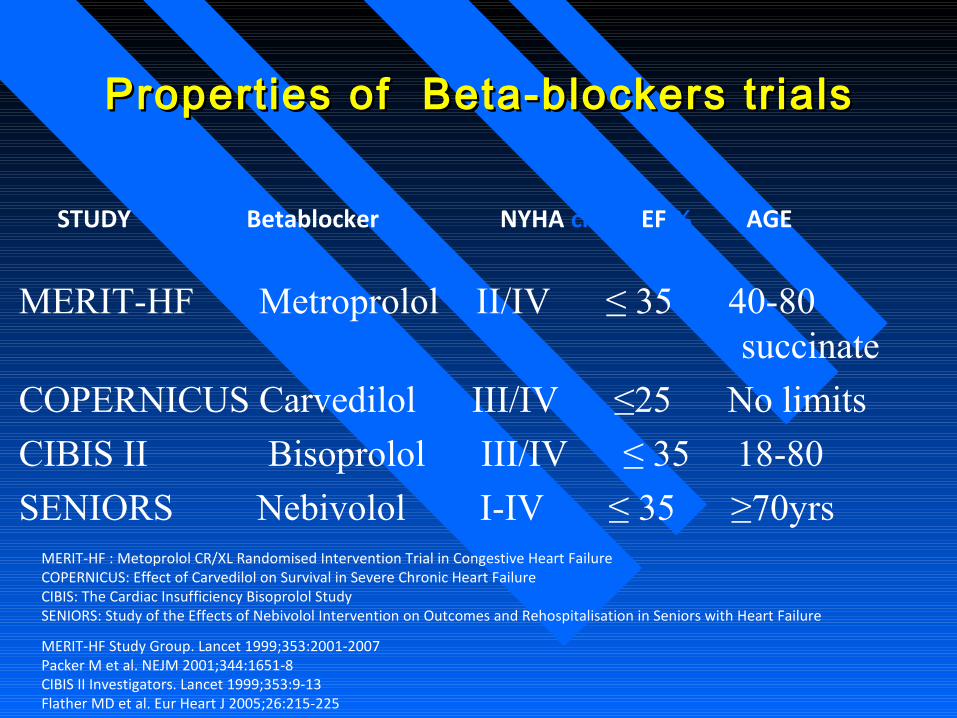
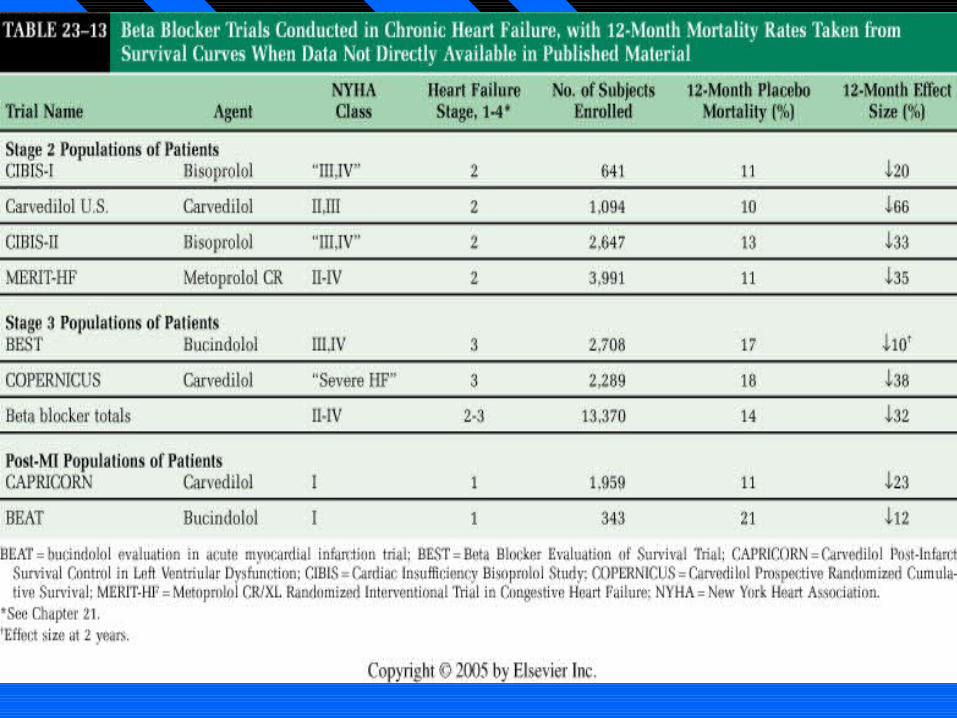
Properties of Beta-blockers trialsProperties of Beta-blockers trials
MERIT-HF Metroprolol II/IV ≤ 35 40-80 succinate
COPERNICUS Carvedilol III/IV ≤25 No limits
CIBIS II Bisoprolol III/IV ≤ 35 18-80
SENIORS Nebivolol I-IV ≤ 35 ≥70yrs
STUDY Betablocker NYHA class EF % AGE
MERIT-HF : Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart FailureCOPERNICUS: Effect of Carvedilol on Survival in Severe Chronic Heart FailureCIBIS: The Cardiac Insufficiency Bisoprolol StudySENIORS: Study of the Effects of Nebivolol Intervention on Outcomes and Rehospitalisation in Seniors with Heart Failure
MERIT-HF Study Group. Lancet 1999;353:2001-2007Packer M et al. NEJM 2001;344:1651-8CIBIS II Investigators. Lancet 1999;353:9-13Flather MD et al. Eur Heart J 2005;26:215-225
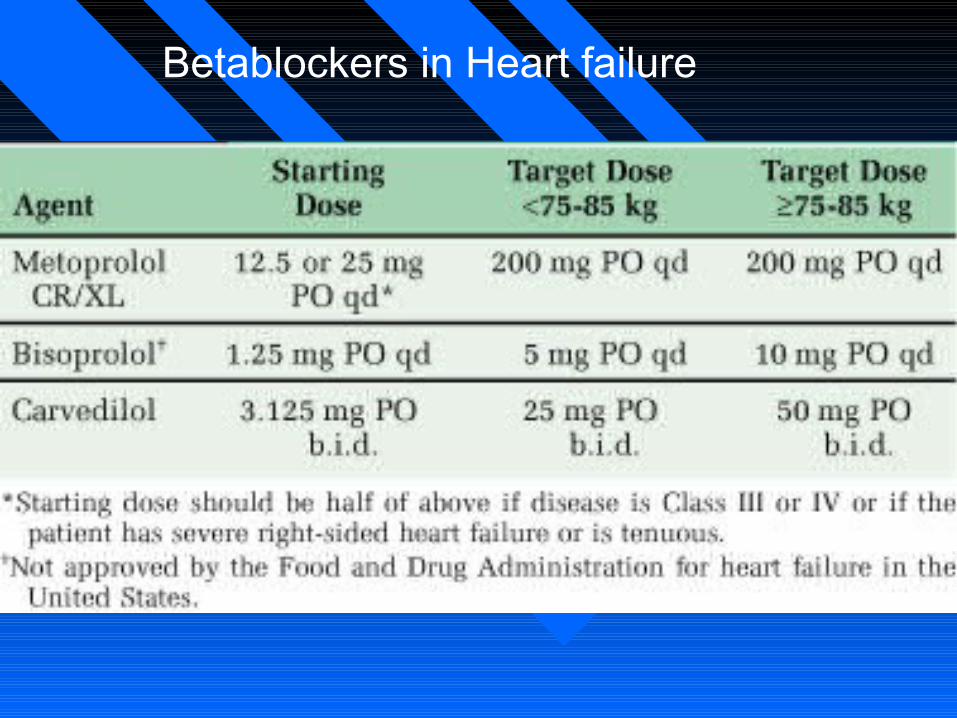
Betablockers in Heart failure
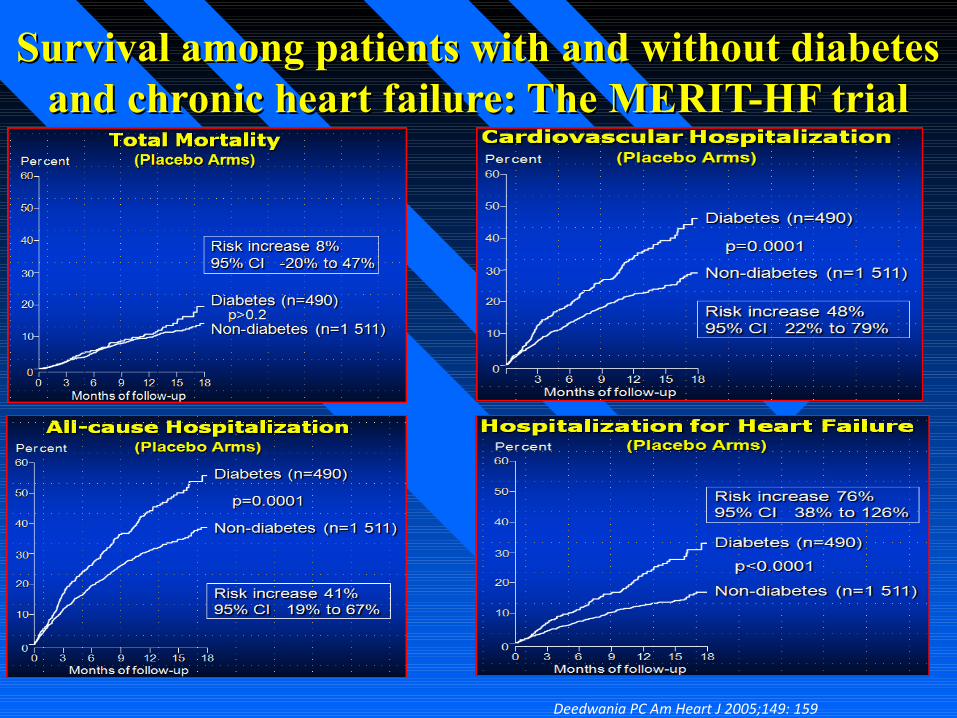
Survival among patients with and without diabetes Survival among patients with and without diabetes and chronic heart failure: The MERIT-HF trialand chronic heart failure: The MERIT-HF trial
Deedwania PC Am Heart J 2005;149: 159
Deedwania PC Am Heart J 2005;149: 159
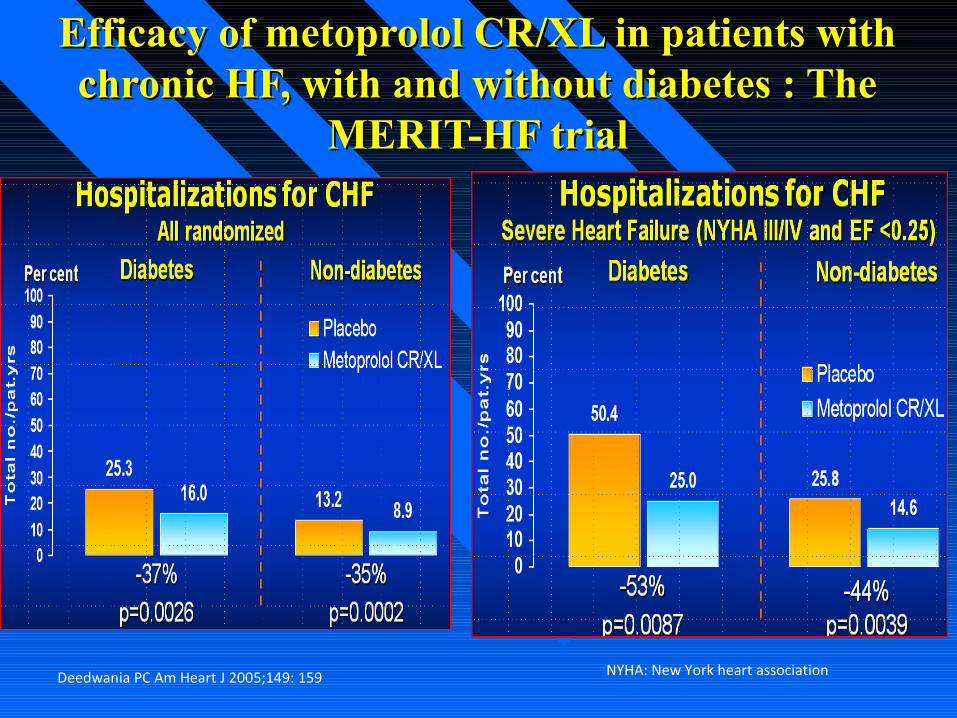
Efficacy of metoprolol CR/XL in patients with Efficacy of metoprolol CR/XL in patients with chronic HF, with and without diabetes : The chronic HF, with and without diabetes : The
MERIT-HF trialMERIT-HF trial
NYHA: New York heart association
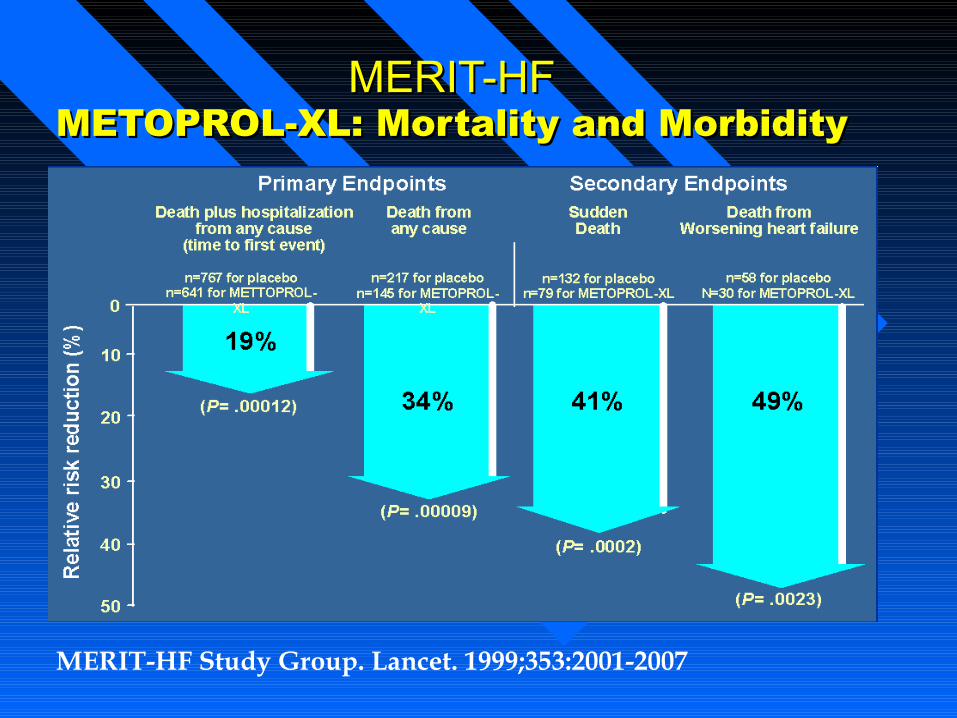
MERIT-HFMERIT-HFMETOPROL-XL: Mortality and MorbidityMETOPROL-XL: Mortality and Morbidity
MERIT-HF Study Group. Lancet. 1999;353:2001-2007
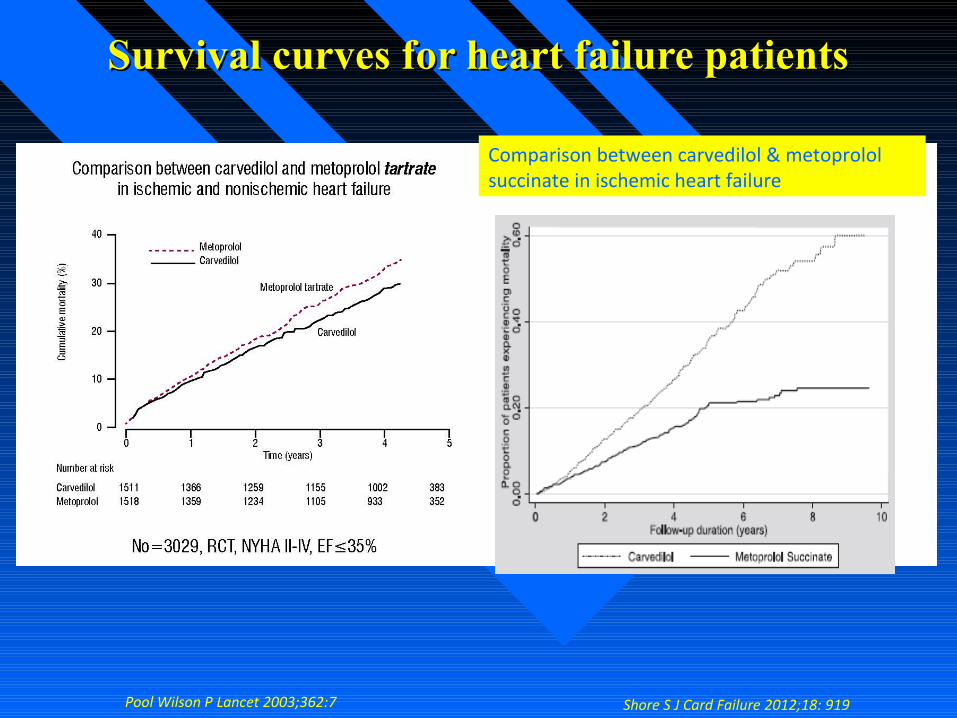
Survival curves for heart failure patientsSurvival curves for heart failure patients
Shore S J Card Failure 2012;18: 919 Pool Wilson P Lancet 2003;362:7
Comparison between carvedilol & metoprolol succinate in ischemic heart failure
• Enrolled 2289 patients with severe HF (LVEF <25%)• Randomized to carvedilol in a target dose of 25 mg bid for up to 29 months
Carvedilol Prospective Randomized Cumulative Survival Trial
(COPERNICUS)
38% reduction in the risk of all-cause mortality among patients with severe congestive heart failure (CHF) treated
with carvedilol compared to placebo
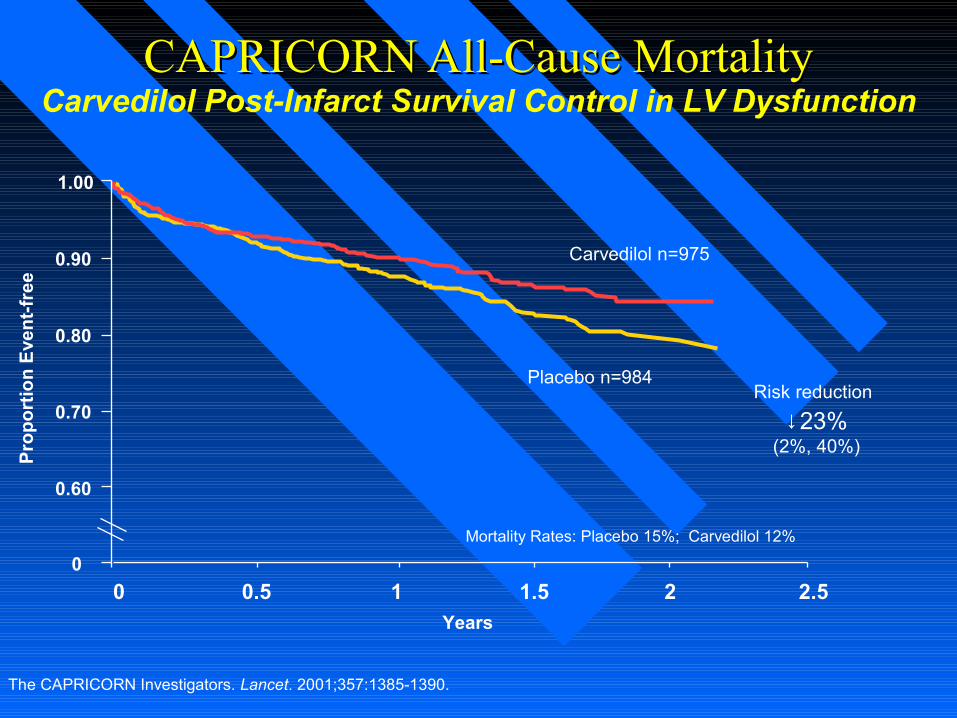
CAPRICORNCAPRICORN All-Cause Mortality All-Cause Mortality
0 0.5 1 1.5 2 2.5
Carvedilol n=975
Placebo n=984
Years
Pro
po
rtio
n E
ven
t-fr
ee
↓23%(2%, 40%)
Risk reduction
0
0.90
0.70
0.60
0.80
The CAPRICORN Investigators. Lancet. 2001;357:1385-1390.
Mortality Rates: Placebo 15%; Carvedilol 12%
Carvedilol Post-Infarct Survival Control in LV Dysfunction
1.00
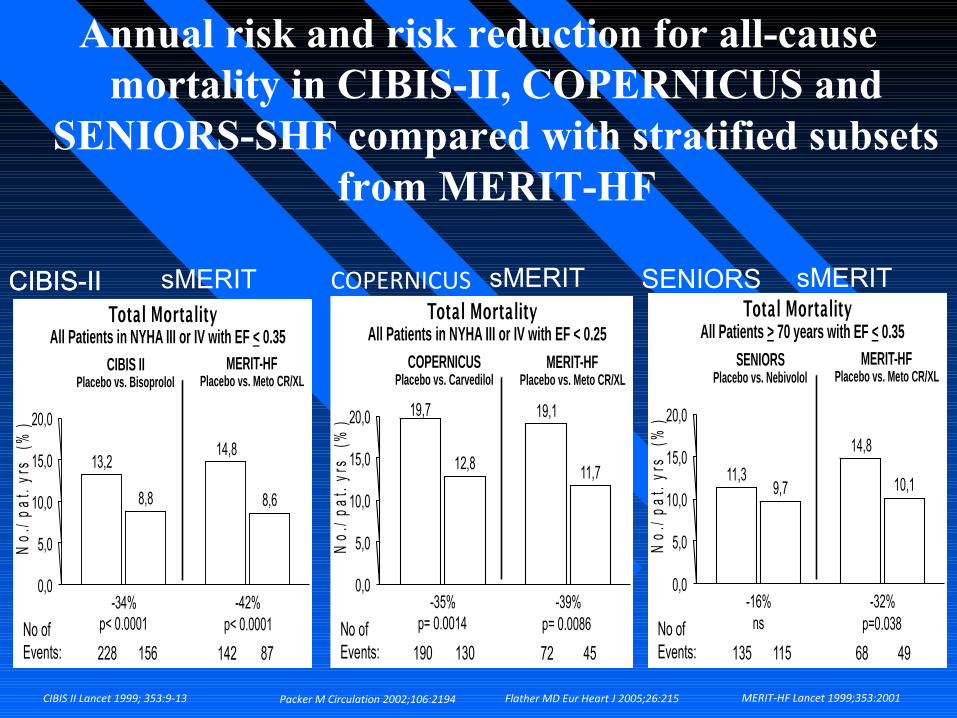
13,2 14,8
8,8 8,6
0,0
5,0
10,0
15,0
20,0
No.
/ pat
. yrs
(%
)
-34% p< 0.0001
-42% p< 0.0001
Total Mortality
CIBIS II Placebo vs. Bisoprolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.35
No of Events: 228 156 87 142
19,7 19,1
12,8 11,7
0,0
5,0
10,0
15,0
20,0
No.
/ pa
t. y
rs
(%)
-35% p= 0.0014
-39% p= 0.0086
Total Mortality
COPERNICUS Placebo vs. Carvedilol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.25
No of Events: 190 130 45 72
11,3
14,8
9,7 10,1
0,0
5,0
10,0
15,0
20,0
No.
/ pa
t. yr
s (
%)
-16% ns
-32% p=0.038
Total Mortality
SENIORS Placebo vs. Nebivolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients > 70 years with EF < 0.35
No of Events: 135 115 49 68
Annual risk and risk reduction for all-cause mortality in CIBIS-II, COPERNICUS and
SENIORS-SHF compared with stratified subsets from MERIT-HF
COPERNICUSsMERIT SENIORSCIBIS-II sMERIT sMERIT
CIBIS II Lancet 1999; 353:9-13 MERIT-HF Lancet 1999;353:2001Packer M Circulation 2002;106:2194 Flather MD Eur Heart J 2005;26:215
CIBIS-II
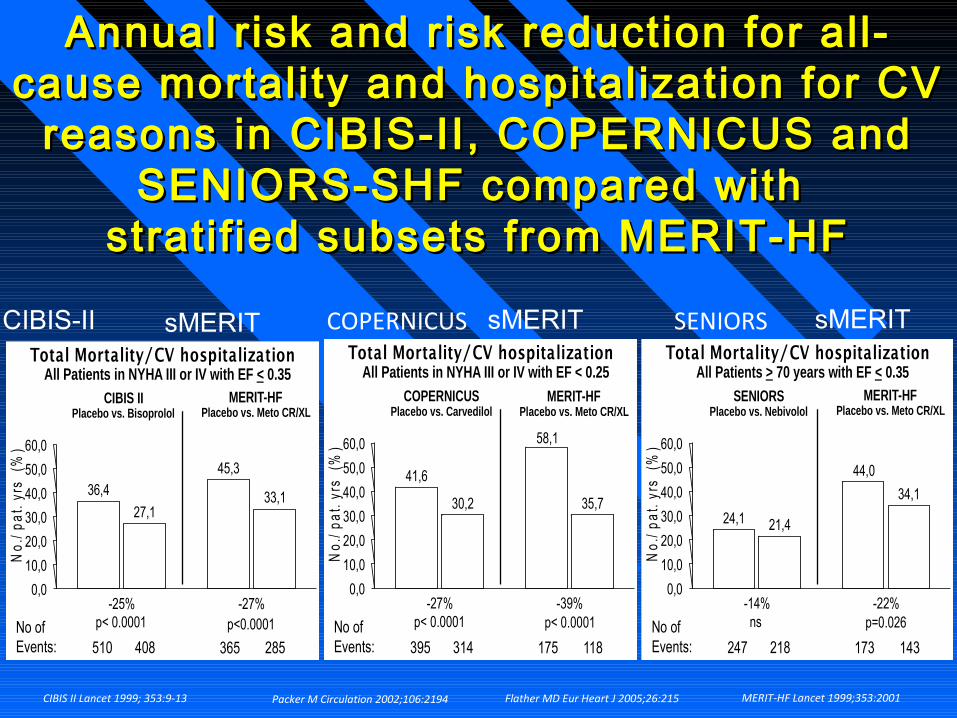
Annual risk and risk reduction for all-Annual risk and risk reduction for all-cause mortality and hospitalization for CV cause mortality and hospitalization for CV
reasons in CIBIS-II, COPERNICUS and reasons in CIBIS-II, COPERNICUS and SENIORS-SHF compared with SENIORS-SHF compared with
stratif ied subsets from MERIT-HFstratif ied subsets from MERIT-HF
36,4
27,1
0,0
10,0
20,0
30,0
40,0
50,0
60,0
No.
/ pat
. yrs
(%
)
-25% p< 0.0001
-27% p<0.0001
Total Mortality/CV hospitalization
CIBIS II Placebo vs. Bisoprolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.35
No of Events: 510 408 285 365
45,3
33,1 41,6
58,1
30,2 35,7
0,0
10,0
20,0
30,0
40,0
50,0
60,0
No.
/ pa
t. yr
s (
%)
-27% p< 0.0001
-39% p< 0.0001
Total Mortality/CV hospitalization
COPERNICUS Placebo vs. Carvedilol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.25
No of Events: 395 314 118 175
24,1
44,0
21,4
34,1
0,0
10,0
20,0
30,0
40,0
50,0
60,0
No.
/ pa
t. yr
s (
%)
-14% ns
-22% p=0.026
Total Mortality/CV hospitalization
SENIORS Placebo vs. Nebivolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients > 70 years with EF < 0.35
No of Events: 247 218 143 173
CIBIS II Lancet 1999; 353:9-13 Packer M Circulation 2002;106:2194 Flather MD Eur Heart J 2005;26:215 MERIT-HF Lancet 1999;353:2001
CIBIS-II sMERIT COPERNICUS sMERIT sMERITSENIORS
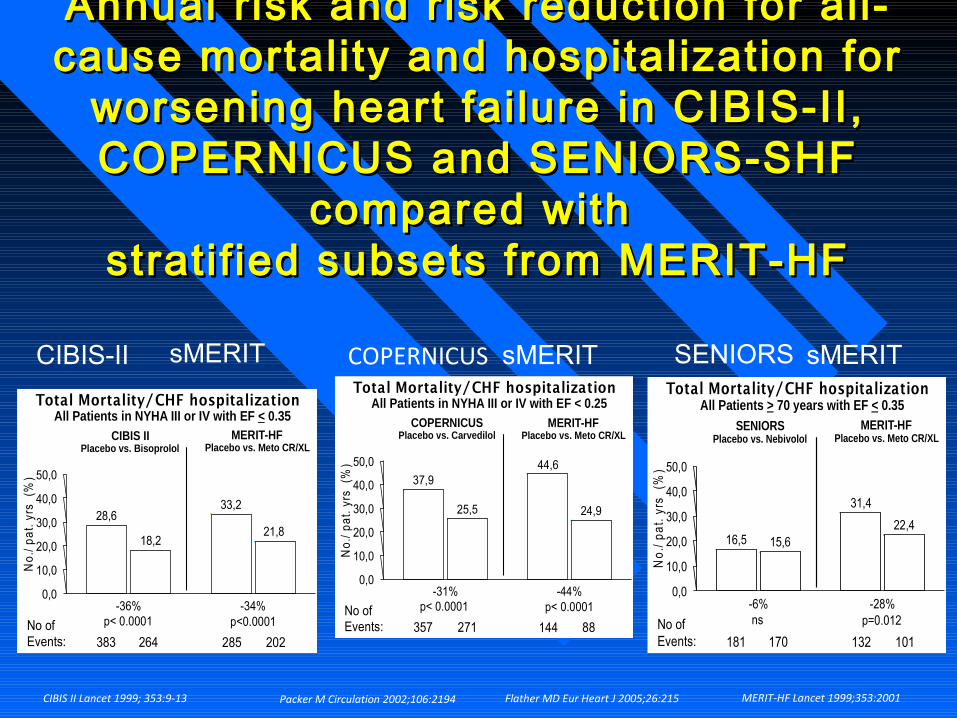
Annual risk and risk reduction for all-Annual risk and risk reduction for all-cause mortality and hospitalization for cause mortality and hospitalization for
worsening heart fai lure in CIBIS-II, worsening heart fai lure in CIBIS-II, COPERNICUS and SENIORS-SHF COPERNICUS and SENIORS-SHF
compared with compared with stratif ied subsets from MERIT-HFstratif ied subsets from MERIT-HF
28,6 33,2
18,2 21,8
0,0
10,0
20,0
30,0
40,0
50,0
No.
/ pa
t. yr
s (
%)
-36% p< 0.0001
-34% p<0.0001
Total Mortality/CHF hospitalization
CIBIS II Placebo vs. Bisoprolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.35
No of Events: 383 264 202 285
37,9 44,6
25,5 24,9
0,0
10,0
20,0
30,0
40,0
50,0
No.
/ pa
t. y
rs
(%)
-31% p< 0.0001
-44% p< 0.0001
Total Mortality/CHF hospitalization
COPERNICUS Placebo vs. Carvedilol
MERIT-HF Placebo vs. Meto CR/XL
All Patients in NYHA III or IV with EF < 0.25
No of Events: 357 271 88 144
16,5
31,4
15,6 22,4
0,0
10,0
20,0
30,0
40,0
50,0
No.
/ pat
. yrs
(%
)
-6% ns
-28% p=0.012
Total Mortality/CHF hospitalization
SENIORS Placebo vs. Nebivolol
MERIT-HF Placebo vs. Meto CR/XL
All Patients > 70 years with EF < 0.35
No of Events: 181 170 101 132
sMERIT sMERIT sMERITCOPERNICUSCIBIS-II SENIORS
CIBIS II Lancet 1999; 353:9-13 Packer M Circulation 2002;106:2194 Flather MD Eur Heart J 2005;26:215 MERIT-HF Lancet 1999;353:2001
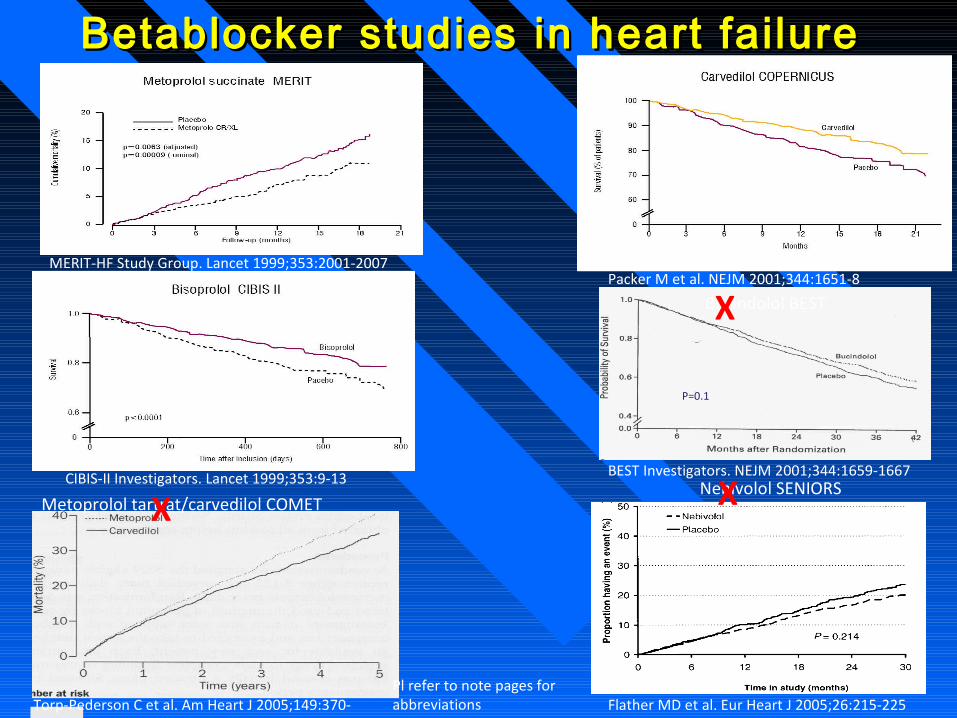
Betablocker studies in heart failureBetablocker studies in heart failure
Bucindolol BEST
P=0.1
Metoprolol tartrat/carvedilol COMETX
X
Nebivolol SENIORSX
Pl refer to note pages for abbreviations
Packer M et al. NEJM 2001;344:1651-8
BEST Investigators. NEJM 2001;344:1659-1667
Torp-Pederson C et al. Am Heart J 2005;149:370-376
Flather MD et al. Eur Heart J 2005;26:215-225
CIBIS-II Investigators. Lancet 1999;353:9-13
MERIT-HF Study Group. Lancet 1999;353:2001-2007
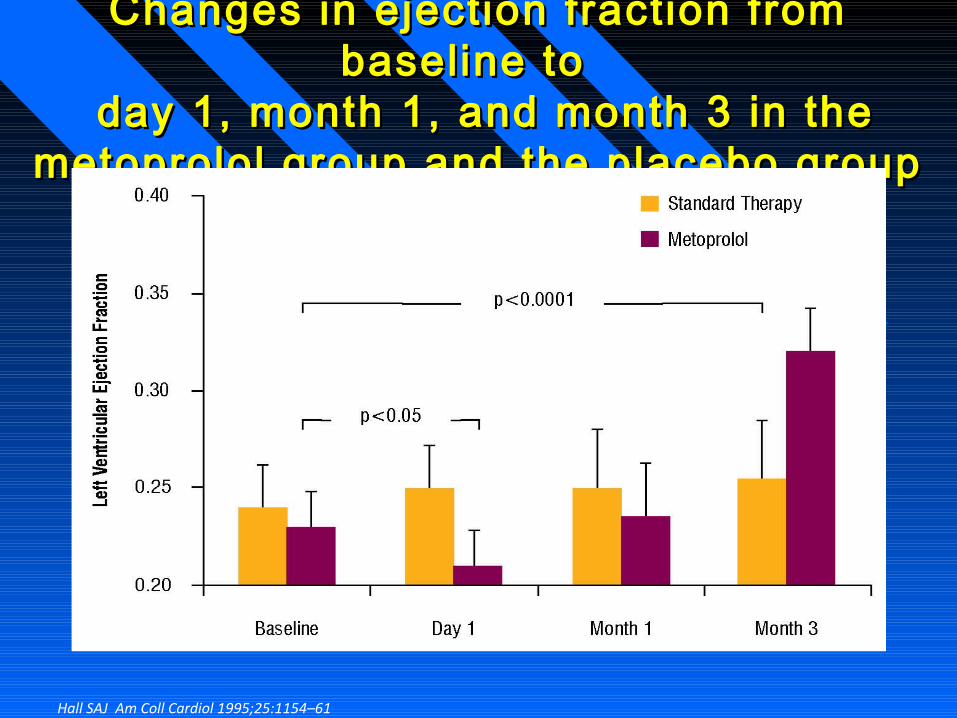
Changes in ejection fraction from Changes in ejection fraction from baseline to baseline to
day 1, month 1, and month 3 in the day 1, month 1, and month 3 in the metoprolol group and the placebo groupmetoprolol group and the placebo group
Hall SAJ Am Coll Cardiol 1995;25:1154–61
ConclusionConclusion ββ -blockers in clinical tr ials-blockers in clinical tr ials
• When adjustments are made for differences between trials the efficacy and tolerability of bisoprolol, carvedilol and metoprolol succinate are similar in patients with systolic heart failure
• Irrespective of NYHA class, ejection fraction and age
• 24 hours β- blockade is important
ConclusionConclusion ββ -blockers in clinical tr ials-blockers in clinical tr ials
The magnitude of heart rate reduction is statistically associated with survival benefit (sudden death) of β-blockers in patients with:
-Hypertension -Post-AMI -Heart failure
-Diabetes mellitus -The effect is independent of β-blocker dose
Deedwania PC Am Heart J 2005;149: 159; Olsson G Am J Hypertens 1991;
Wikstrand J et al, JACC 2002;40:491-8; Cucherat M: Eur Heart J 2007;28:3012-3019 ; McAllister FA Ann Int Med 2009;150:784-794
AMI: acute myocardial infarction
• Background• Tachycardia as an independent risk factor• Beta blocker therapy (angina, post- infarction, heart failure,
hypertension, diabetes)
• Are all beta blockers alike?• Adverse effects (fatigue, CHF, cold feet, diabetes)
• What do the guidelines say?
Re-Exploring the Role of Beta Re-Exploring the Role of Beta Blockers in secondary preventionBlockers in secondary prevention
Relative contraindications to beta-Relative contraindications to beta-blocker treatmentblocker treatment
• Heart rate <60 bpm • Symptomatic hypotension • Greater than minimal evidence of fluid retention • Signs of peripheral hypoperfusion • PR interval >0.24 sec • Second- or third-degree atrioventricular block • History of asthma or reactive airways • Peripheral artery disease with resting limb ischemia
ConclusionConclusion Adverse effects of Adverse effects of ββ -blockers in -blockers in
clinical tr ialsclinical tr ials
• HF patients are more sensitive to dose • Individualized dose-titration is mandated over >3
weeks guided by patient tolerability and the heart rate response
• 24-hour even cardioselective beta-blockade and good
tolerabilty
from 25 mg to 200 mg once daily
• Anti-atherosclerotic effects
• Positive data published from
-Primary prevention in hypertension
-Secondary prevention post-MI
-Secondary prevention in systolic heart failure
Metoprolol Succinate CR/XLA Lipophil ic Beta-blocker with a
High Clinical Cardioselectivity
Long-term benefits s• improved survival• improved control ofheart failure• reduced need forhospitalisation• improved quality of life• improved left ventricularejection fraction
Short-term risks
• worsening heart failure• bradyarrhythmias• prolonged intraventricularconduction• hypotension• worsening renal function
Beta blockers in systolic heart failureIn patients with primarily severe systolic heart failure(low ejection fraction) beta blockade has the following long-term benefits which must be balanced against the short-term risks
2013 ACCF/AHA Guideline for the 2013 ACCF/AHA Guideline for the Management of Heart FailureManagement of Heart Failure
Developed in Collaboration With the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and International Society for Heart and Lung Transplantation
Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation
© American College of Cardiology Foundation and American Heart Association, Inc.
Stages, Phenotypes and Treatment of Stages, Phenotypes and Treatment of HFHF
I.I. Initial and Serial Evaluation of the HF Patient Initial and Serial Evaluation of the HF Patient
(including HFpEF)(including HFpEF)
II. Treatment of Stage A thru D Heart FailureII. Treatment of Stage A thru D Heart Failure
(including HFpEF)(including HFpEF)
III. The Hospitalized PatientIII. The Hospitalized Patient
IV. IV. Surgical/Percutaneous/Transcatheter Interventional TreatmentsSurgical/Percutaneous/Transcatheter Interventional Treatments
V. Coordinating Care for Patients With Chronic HFV. Coordinating Care for Patients With Chronic HF
VI. Quality Metrics/Performance MeasuresVI. Quality Metrics/Performance Measures
OutlineOutline
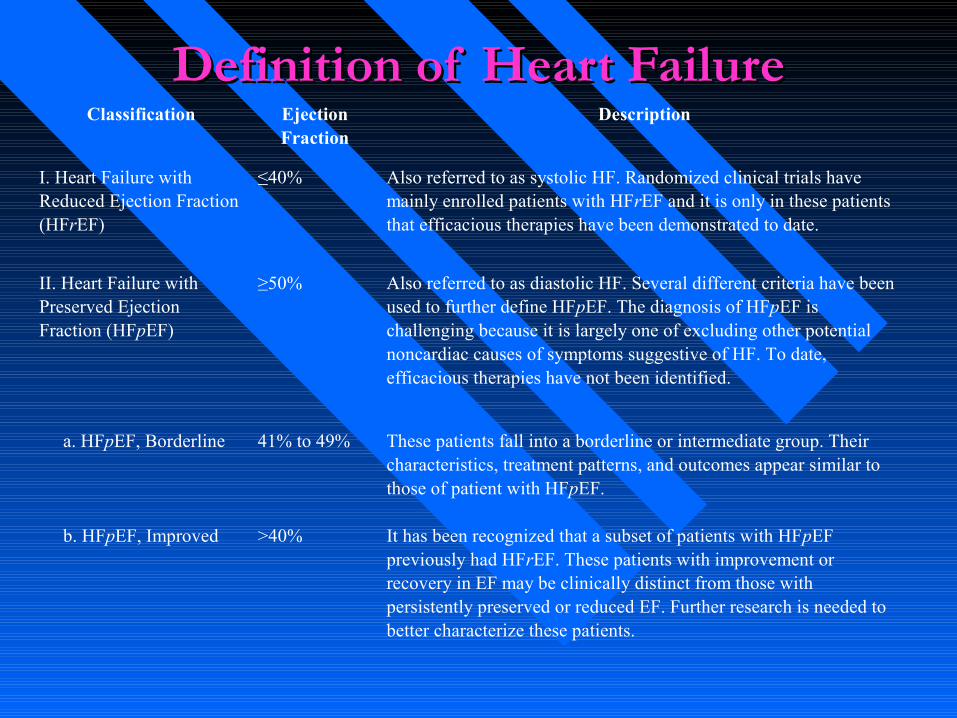
Definition of Heart FailureDefinition of Heart FailureClassification Ejection
FractionDescription
I. Heart Failure with Reduced Ejection Fraction (HFrEF)
≤40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date.
II. Heart Failure with Preserved Ejection Fraction (HFpEF)
≥50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified.
a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF.
b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients.
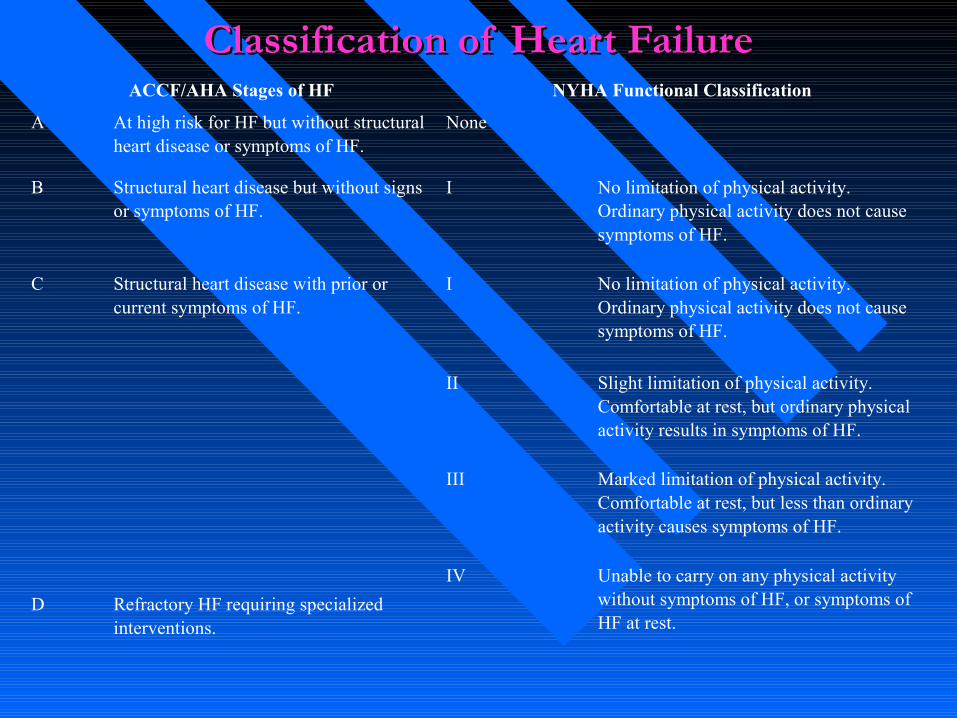
Classification of Heart FailureClassification of Heart FailureACCF/AHA Stages of HF NYHA Functional Classification
A At high risk for HF but without structural heart disease or symptoms of HF.
None
B Structural heart disease but without signs or symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
C Structural heart disease with prior or current symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
II Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF.
III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF.
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
D Refractory HF requiring specialized interventions.
Treatment of Stages A to D
Guideline for HF
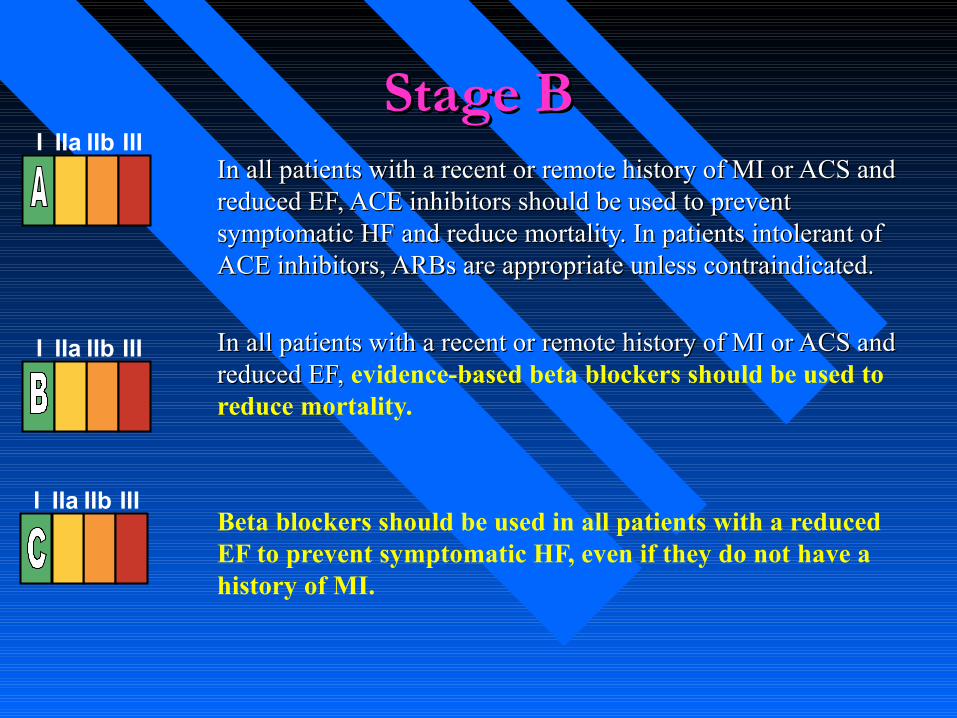
Stage BStage BIn all patients with a recent or remote history of MI or ACS and In all patients with a recent or remote history of MI or ACS and reduced EF, ACE inhibitors should be used to prevent reduced EF, ACE inhibitors should be used to prevent symptomatic HF and reduce mortality. In patients intolerant of symptomatic HF and reduce mortality. In patients intolerant of ACE inhibitors, ARBs are appropriate unless contraindicated.ACE inhibitors, ARBs are appropriate unless contraindicated.
In all patients with a recent or remote history of MI or ACS and In all patients with a recent or remote history of MI or ACS and reduced EF, reduced EF, evidence-based beta blockers should be used to reduce mortality.
Beta blockers should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do not have a history of MI.
I IIa IIb III
I IIa IIb III
I IIa IIb III
Stage C
Treatment of Stages A to D
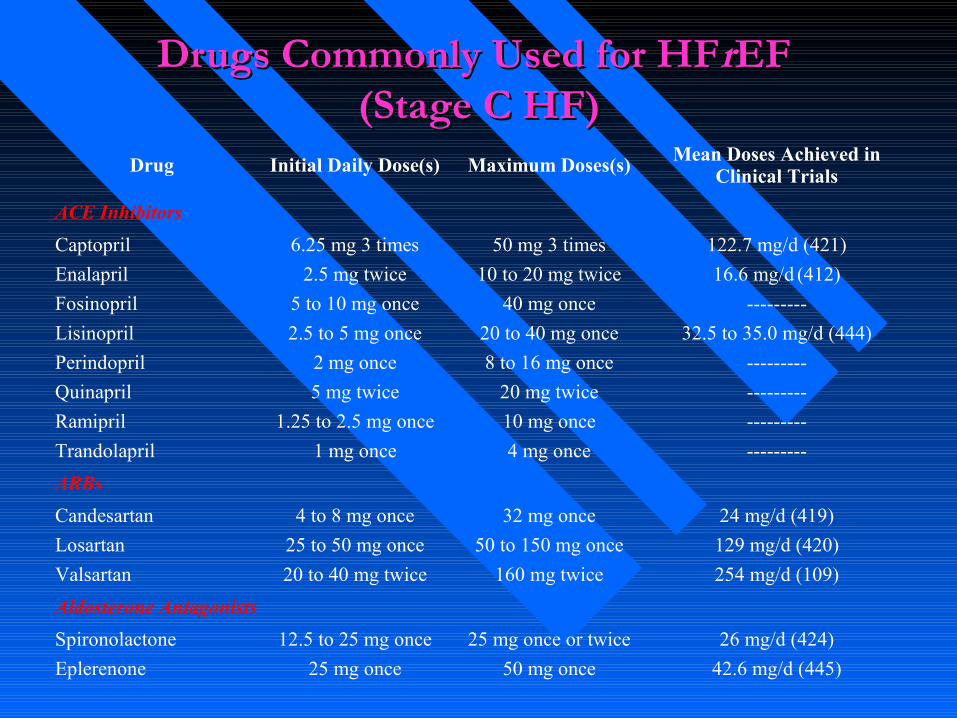
Drugs Commonly Used for HFDrugs Commonly Used for HFrrEF EF (Stage C HF)(Stage C HF)
Drug Initial Daily Dose(s) Maximum Doses(s) Mean Doses Achieved in Clinical Trials
ACE Inhibitors
Captopril 6.25 mg 3 times 50 mg 3 times 122.7 mg/d (421)
Enalapril 2.5 mg twice 10 to 20 mg twice 16.6 mg/d (412)
Fosinopril 5 to 10 mg once 40 mg once ---------
Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35.0 mg/d (444)
Perindopril 2 mg once 8 to 16 mg once ---------
Quinapril 5 mg twice 20 mg twice ---------
Ramipril 1.25 to 2.5 mg once 10 mg once ---------
Trandolapril 1 mg once 4 mg once ---------
ARBs
Candesartan 4 to 8 mg once 32 mg once 24 mg/d (419)
Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d (420)
Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d (109)
Aldosterone Antagonists
Spironolactone 12.5 to 25 mg once 25 mg once or twice 26 mg/d (424)
Eplerenone 25 mg once 50 mg once 42.6 mg/d (445)
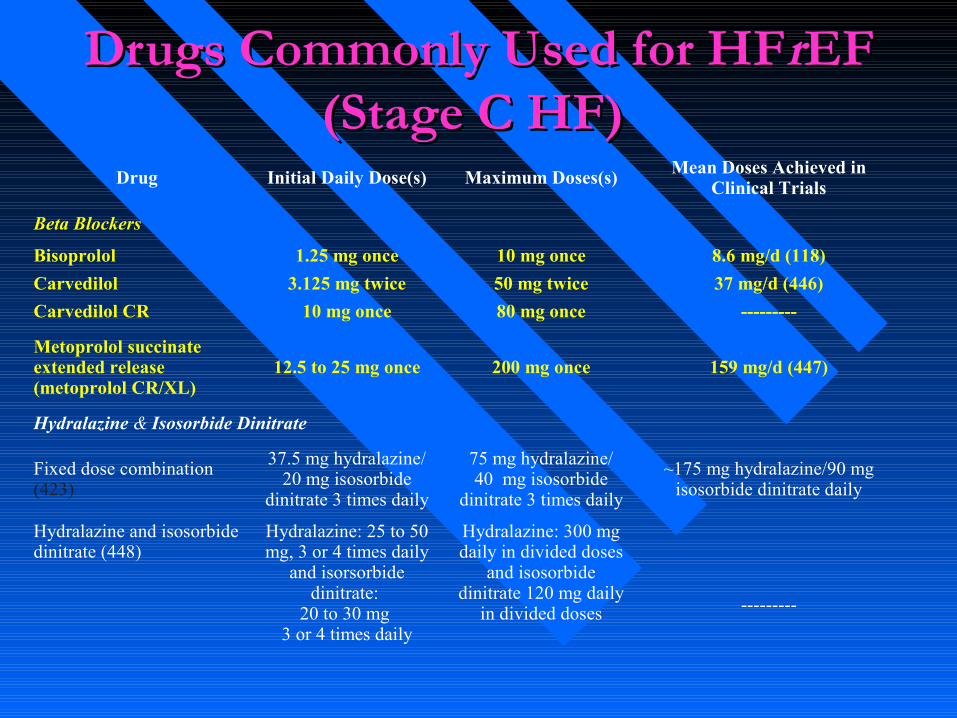
Drugs Commonly Used for HFDrugs Commonly Used for HFrrEF EF (Stage C HF) (Stage C HF)
Drug Initial Daily Dose(s) Maximum Doses(s) Mean Doses Achieved in Clinical Trials
Beta Blockers
Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d (118)
Carvedilol 3.125 mg twice 50 mg twice 37 mg/d (446)
Carvedilol CR 10 mg once 80 mg once ---------
Metoprolol succinate extended release (metoprolol CR/XL)
12.5 to 25 mg once 200 mg once 159 mg/d (447)
Hydralazine & Isosorbide Dinitrate
Fixed dose combination (423)
37.5 mg hydralazine/20 mg isosorbide
dinitrate 3 times daily
75 mg hydralazine/40 mg isosorbide
dinitrate 3 times daily
~175 mg hydralazine/90 mg isosorbide dinitrate daily
Hydralazine and isosorbide dinitrate (448)
Hydralazine: 25 to 50 mg, 3 or 4 times daily
and isorsorbide dinitrate:
20 to 30 mg 3 or 4 times daily
Hydralazine: 300 mg daily in divided doses
and isosorbide dinitrate 120 mg daily
in divided doses ---------
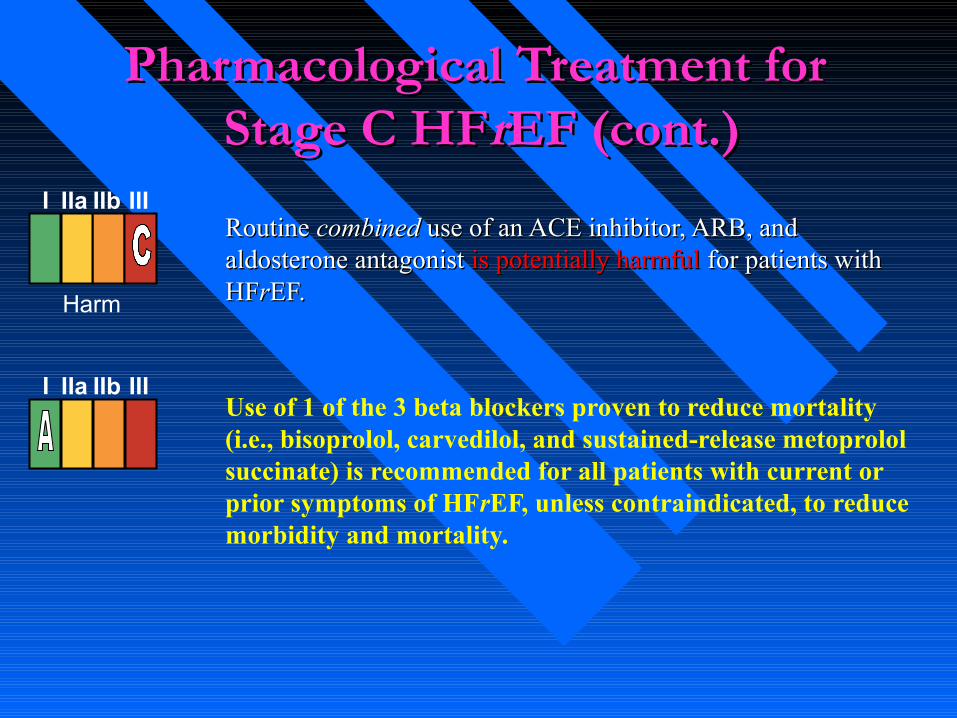
Pharmacological Treatment for Pharmacological Treatment for Stage C HFStage C HFrrEF (cont.)EF (cont.)
Routine Routine combinedcombined use of an ACE inhibitor, ARB, and use of an ACE inhibitor, ARB, and aldosterone antagonist aldosterone antagonist is potentially harmful is potentially harmful for patients with for patients with HFHFrrEF. EF.
Use of 1 of the 3 beta blockers proven to reduce mortality (i.e., bisoprolol, carvedilol, and sustained-release metoprolol succinate) is recommended for all patients with current or prior symptoms of HFrEF, unless contraindicated, to reduce morbidity and mortality.
I IIa IIb III
I IIa IIb III
Harm
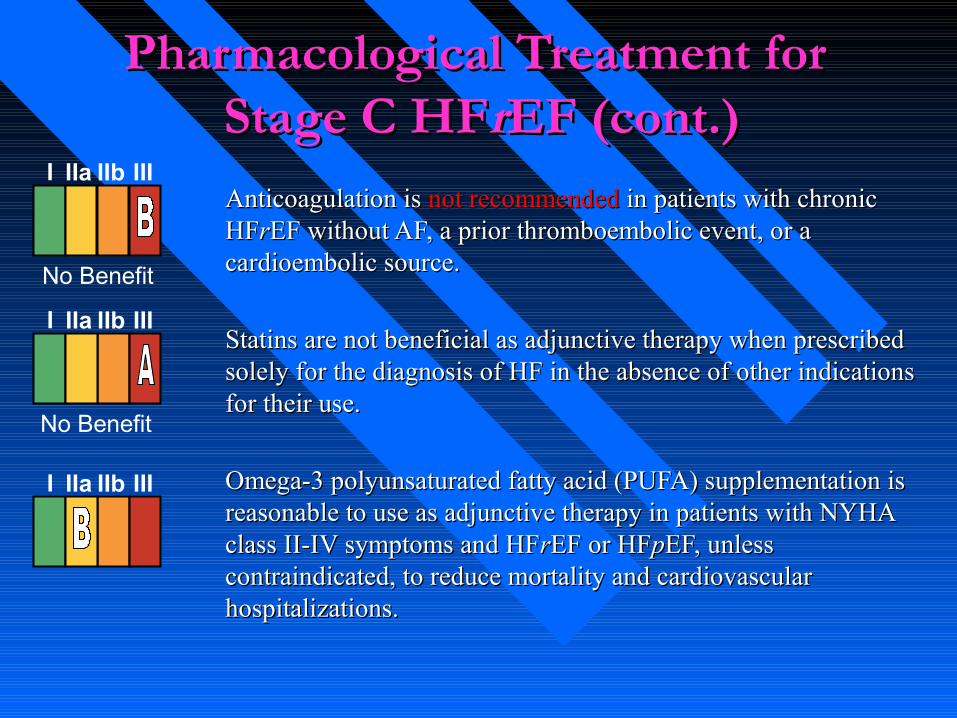
Pharmacological Treatment for Pharmacological Treatment for Stage C HFStage C HFrrEF (cont.)EF (cont.)
Anticoagulation is Anticoagulation is not recommended not recommended in patients with chronic in patients with chronic HFHFrrEF without AF, a prior thromboembolic event, or a EF without AF, a prior thromboembolic event, or a cardioembolic source.cardioembolic source.
Statins are not beneficial as adjunctive therapy when prescribed Statins are not beneficial as adjunctive therapy when prescribed solely for the diagnosis of HF in the absence of other indications solely for the diagnosis of HF in the absence of other indications for their use.for their use.
Omega-3 polyunsaturated fatty acid (PUFA) supplementation is Omega-3 polyunsaturated fatty acid (PUFA) supplementation is reasonable to use as adjunctive therapy in patients with NYHA reasonable to use as adjunctive therapy in patients with NYHA class II-IV symptoms and HFclass II-IV symptoms and HFrrEF or HFEF or HFppEF, unless EF, unless contraindicated, to reduce mortality and cardiovascular contraindicated, to reduce mortality and cardiovascular hospitalizations.hospitalizations.
I IIa IIb III
No Benefit
I IIa IIb III
No Benefit
I IIa IIb III
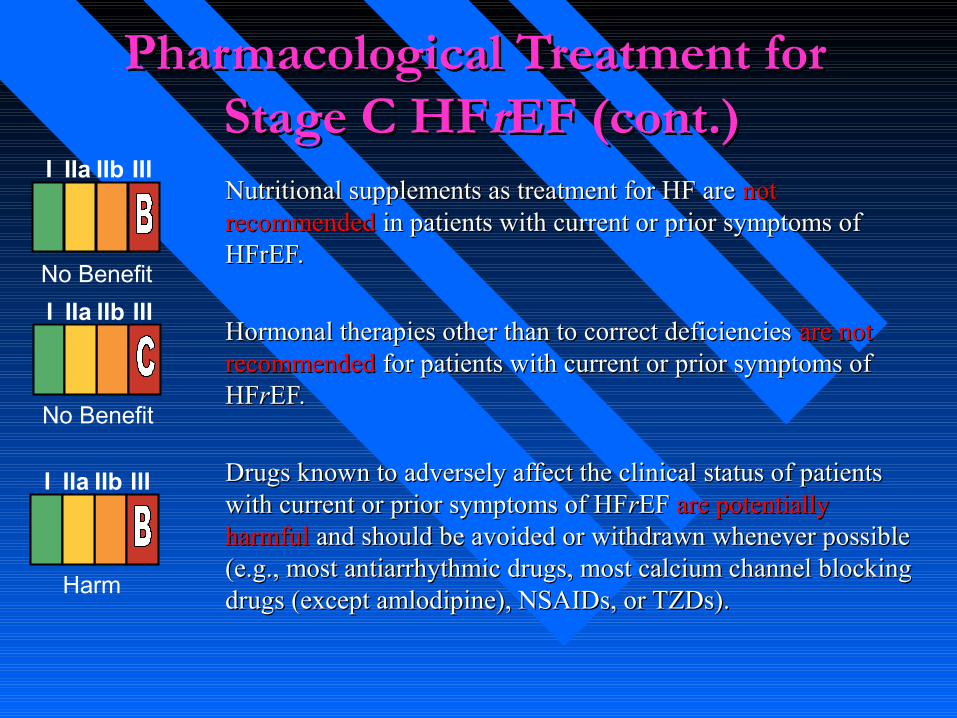
Pharmacological Treatment for Pharmacological Treatment for Stage C HFStage C HFrrEF (cont.)EF (cont.)Nutritional supplements as treatment for HF are Nutritional supplements as treatment for HF are not not recommended recommended in patients with current or prior symptoms of in patients with current or prior symptoms of HFrEF.HFrEF.
Hormonal therapies other than to correct deficiencies Hormonal therapies other than to correct deficiencies are not are not recommendedrecommended for patients with current or prior symptoms of for patients with current or prior symptoms of HFHFrrEF. EF.
Drugs known to adversely affect the clinical status of patients Drugs known to adversely affect the clinical status of patients with current or prior symptoms of HFwith current or prior symptoms of HFrrEF EF are potentially are potentially harmful harmful and should be avoided or withdrawn whenever possible and should be avoided or withdrawn whenever possible (e.g., most antiarrhythmic drugs, most calcium channel blocking (e.g., most antiarrhythmic drugs, most calcium channel blocking drugs (except amlodipine), NSAIDs, or TZDs).drugs (except amlodipine), NSAIDs, or TZDs).
No Benefit
I IIa IIb III
I IIa IIb III
I IIa IIb III
No Benefit
Harm
Pharmacological Treatment for Pharmacological Treatment for Stage C HFStage C HFrrEF (cont.)EF (cont.)
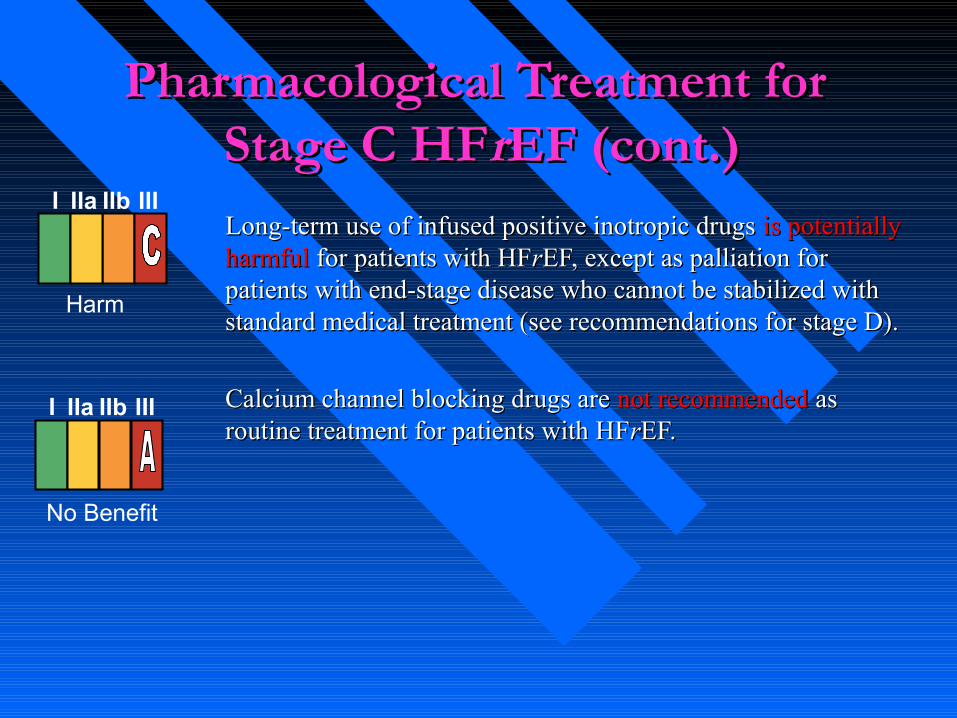
Long-term use of infused positive inotropic drugs Long-term use of infused positive inotropic drugs is potentially is potentially harmfulharmful for patients with HFfor patients with HFrrEF, except as palliation for EF, except as palliation for patients with end-stage disease who cannot be stabilized with patients with end-stage disease who cannot be stabilized with standard medical treatment (see recommendations for stage D).standard medical treatment (see recommendations for stage D).
Calcium channel blocking drugs are Calcium channel blocking drugs are not recommended not recommended as as routine treatment for patients with HFroutine treatment for patients with HFrrEF.EF.
Harm
I IIa IIb III
I IIa IIb III
No Benefit
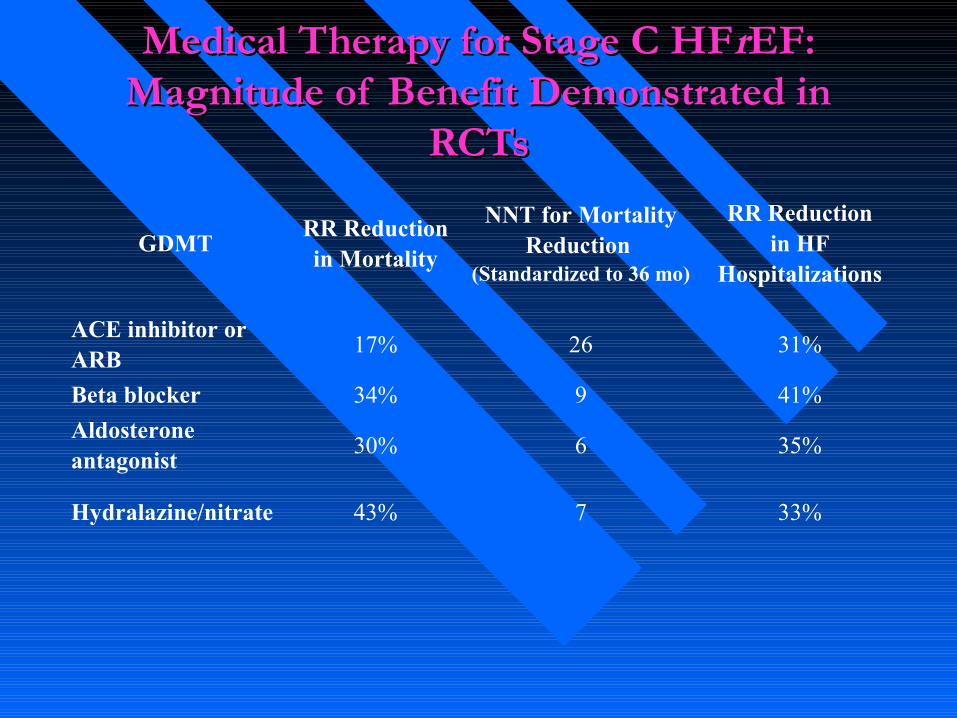
Medical Therapy for Stage C HFMedical Therapy for Stage C HFrrEF: EF: Magnitude of Benefit Demonstrated in Magnitude of Benefit Demonstrated in
RCTsRCTs
GDMTRR Reduction in Mortality
NNT for Mortality Reduction
(Standardized to 36 mo)
RR Reductionin HF
Hospitalizations
ACE inhibitor or ARB
17% 26 31%
Beta blocker 34% 9 41%
Aldosterone antagonist
30% 6 35%
Hydralazine/nitrate 43% 7 33%