Embed Size (px)
Citation preview
Better Data for Informed Commissioning
Improving data quality: national developments
Dr Masood Nazir
General Practitioner
Clinical Informatics Advisor
NHS England
About us
• The NHS Commissioning Board (NHS CB):
• was established as a special health authority on 31
October 2011 and as an executive non-departmental
public body on 1 October 2012;
• plays a key role in the Government’s vision to modernise
the NHS and secure the best possible outcomes for
patients.
• Renamed to NHS England – 1st April 2013
2
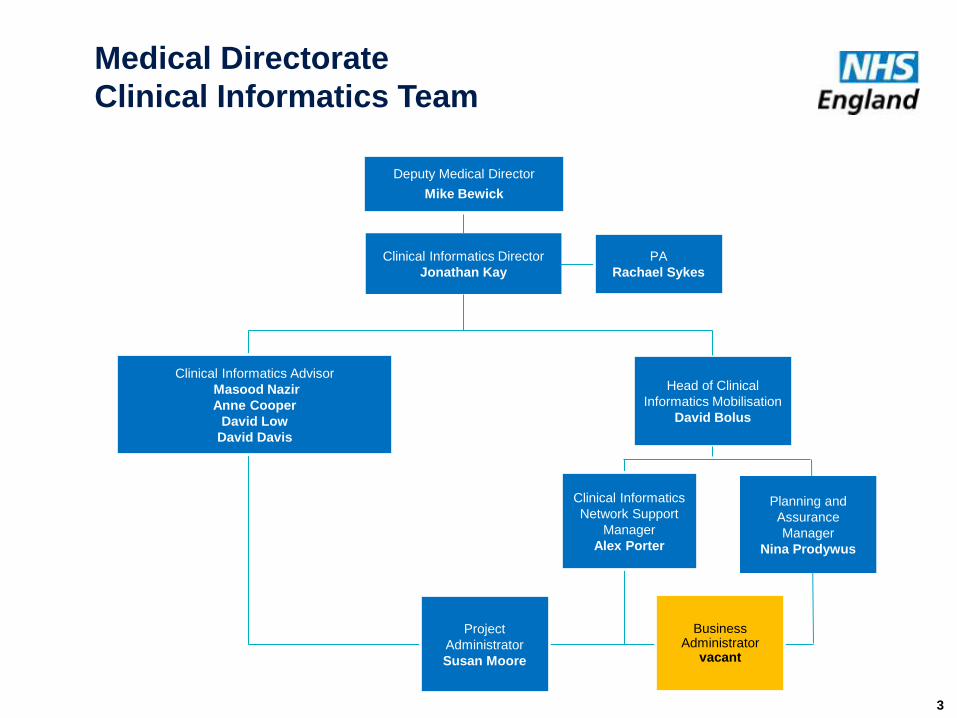
Clinical Informatics Advisor
Masood Nazir
Anne Cooper
David Low
David Davis
Head of Clinical
Informatics Mobilisation
David Bolus
Project
Administrator
Susan Moore
Clinical Informatics
Network Support
Manager
Alex Porter
Clinical Informatics Director
Jonathan Kay
Planning and
Assurance
Manager
Nina Prodywus
3
PA
Rachael Sykes
Medical Directorate
Clinical Informatics Team
Business Administrator
vacant
Deputy Medical Director
Mike Bewick
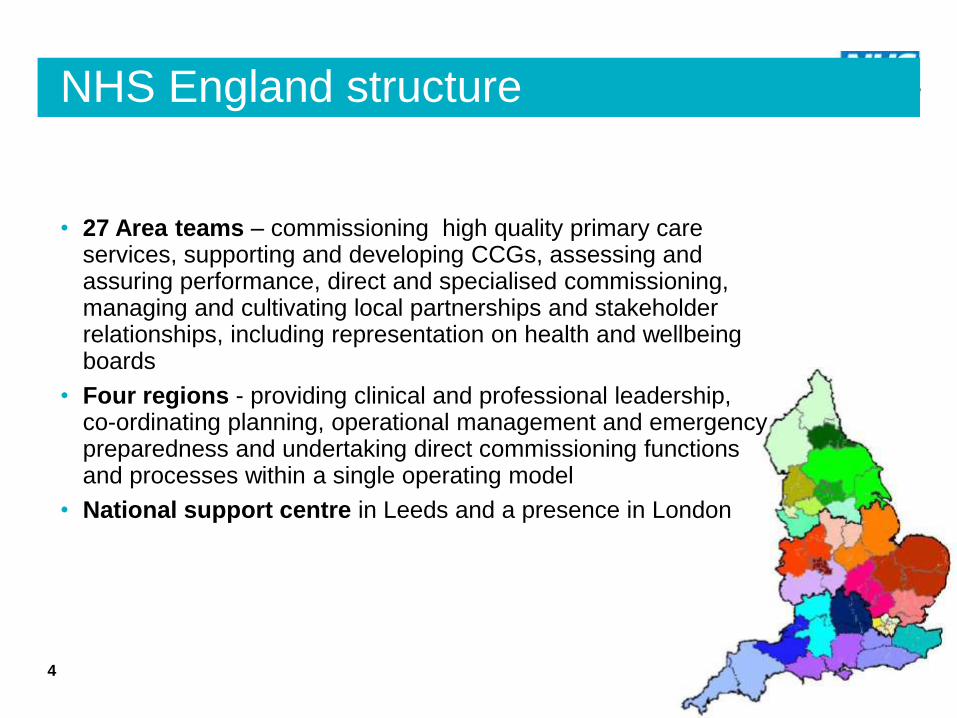
NHS England structure
• 27 Area teams – commissioning high quality primary care services, supporting and developing CCGs, assessing and assuring performance, direct and specialised commissioning, managing and cultivating local partnerships and stakeholder relationships, including representation on health and wellbeing boards
• Four regions - providing clinical and professional leadership, co-ordinating planning, operational management and emergency preparedness and undertaking direct commissioning functions and processes within a single operating model
• National support centre in Leeds and a presence in London
4
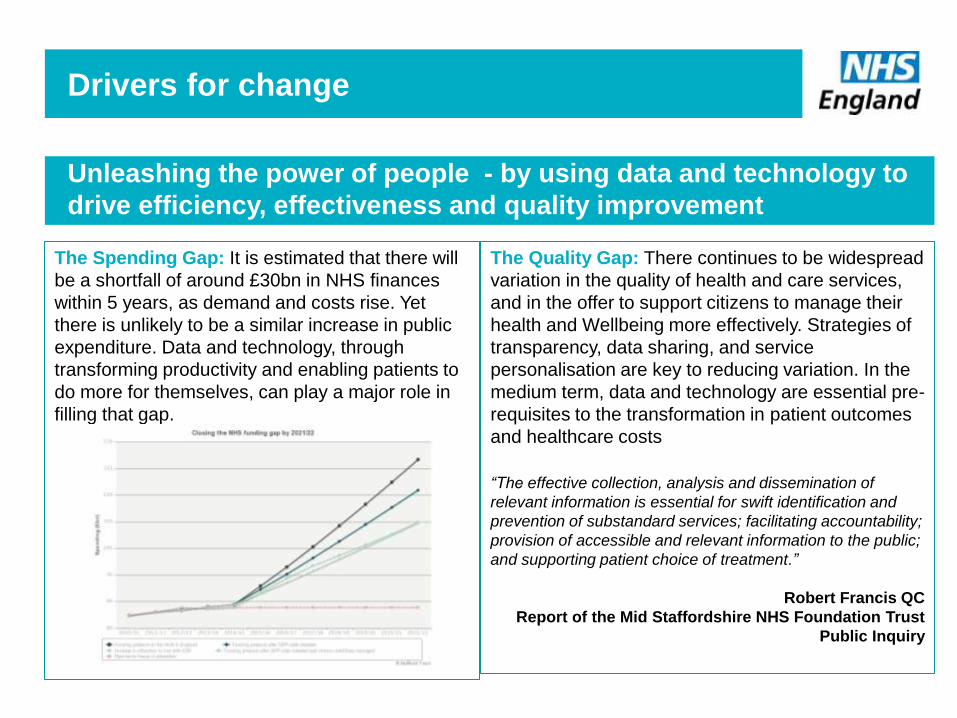
Unleashing the power of people - by using data and technology to
drive efficiency, effectiveness and quality improvement
The Spending Gap: It is estimated that there will
be a shortfall of around £30bn in NHS finances
within 5 years, as demand and costs rise. Yet
there is unlikely to be a similar increase in public
expenditure. Data and technology, through
transforming productivity and enabling patients to
do more for themselves, can play a major role in
filling that gap.
The Quality Gap: There continues to be widespread
variation in the quality of health and care services,
and in the offer to support citizens to manage their
health and Wellbeing more effectively. Strategies of
transparency, data sharing, and service
personalisation are key to reducing variation. In the
medium term, data and technology are essential pre-
requisites to the transformation in patient outcomes
and healthcare costs
“The effective collection, analysis and dissemination of
relevant information is essential for swift identification and
prevention of substandard services; facilitating accountability;
provision of accessible and relevant information to the public;
and supporting patient choice of treatment.”
Robert Francis QC
Report of the Mid Staffordshire NHS Foundation Trust
Public Inquiry
Drivers for change
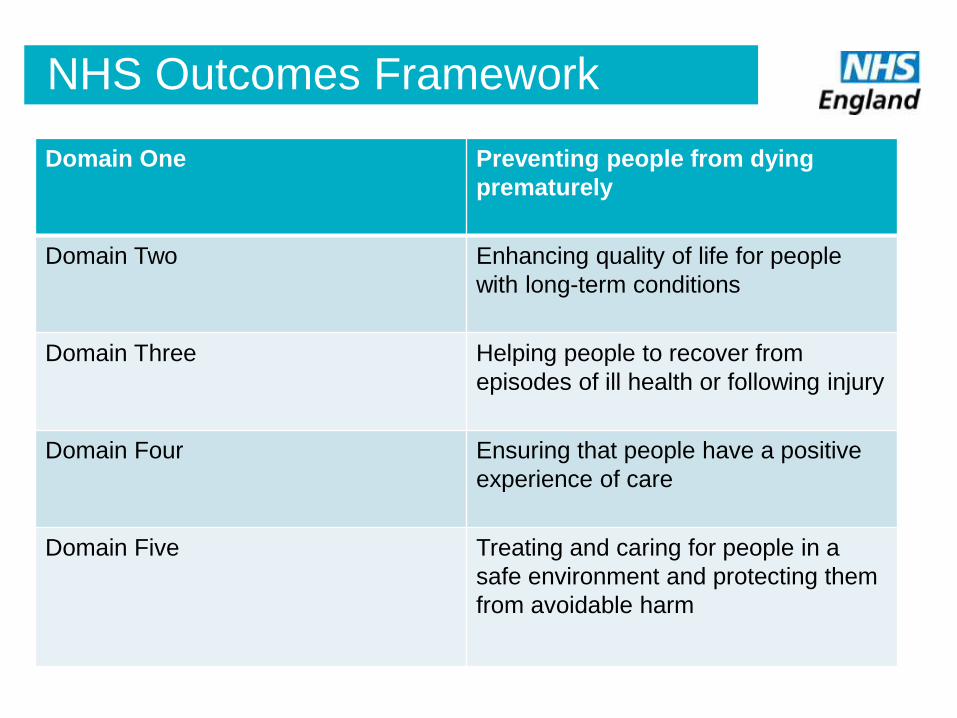
NHS Outcomes Framework
Domain One Preventing people from dying
prematurely
Domain Two Enhancing quality of life for people
with long-term conditions
Domain Three Helping people to recover from
episodes of ill health or following injury
Domain Four Ensuring that people have a positive
experience of care
Domain Five Treating and caring for people in a
safe environment and protecting them
from avoidable harm
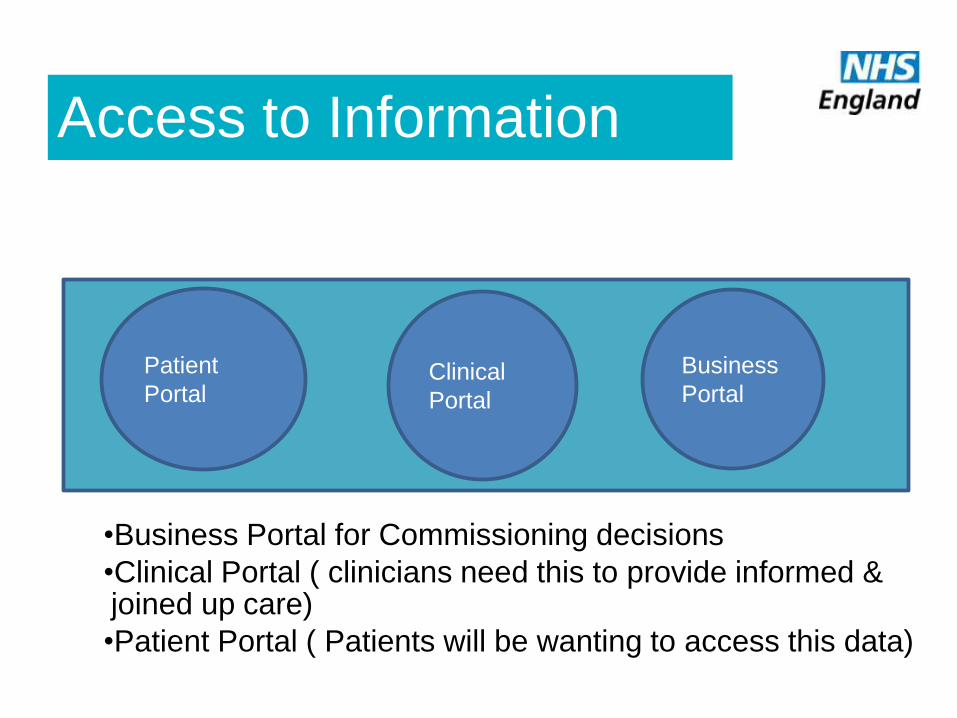
Access to Information
•Business Portal for Commissioning decisions
•Clinical Portal ( clinicians need this to provide informed & joined up care)
•Patient Portal ( Patients will be wanting to access this data)
Clinical
Portal
Business
Portal
Patient
Portal
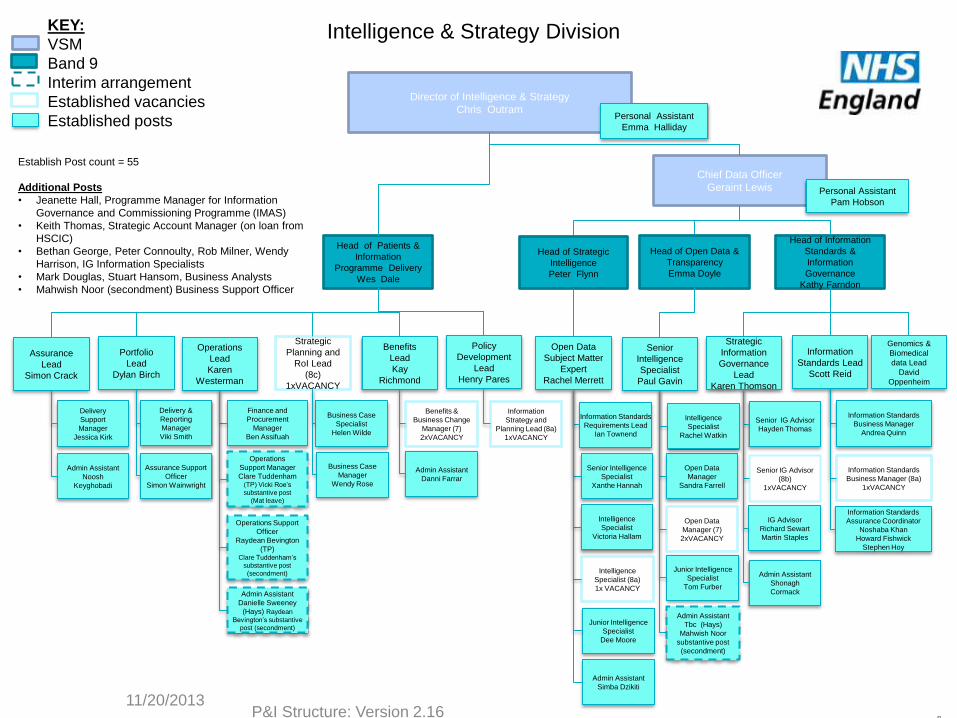
Director of Intelligence & Strategy
Chris Outram Personal Assistant
Emma Halliday
Head of Patients &
Information
Programme Delivery
Wes Dale
Chief Data Officer
Geraint Lewis
Portfolio
Lead
Dylan Birch
Operations
Lead
Karen
Westerman
Assurance
Lead
Simon Crack
Strategic
Planning and
RoI Lead
(8c)
1xVACANCY
Benefits
Lead
Kay
Richmond
Policy
Development
Lead
Henry Pares
Head of Information
Standards &
Information
Governance
Kathy Farndon
Delivery &
Reporting
Manager
Viki Smith
Delivery
Support
Manager
Jessica Kirk
Operations
Support Manager
Clare Tuddenham (TP) Vicki Roe’s
substantive post
(Mat leave)
Assurance Support
Officer
Simon Wainwright
Operations Support
Officer
Raydean Bevington
(TP) Clare Tuddenham’s
substantive post
(secondment)
Admin Assistant
Noosh
Keyghobadi
Admin Assistant
Danni Farrar
Business Case
Manager
Wendy Rose
Information
Strategy and
Planning Lead (8a)
1xVACANCY
Business Case
Specialist
Helen Wilde
Personal Assistant
Pam Hobson
Strategic
Information
Governance
Lead
Karen Thomson
IG Advisor
Richard Sewart
Martin Staples
Information Standards
Business Manager
Andrea Quinn
Admin Assistant
Shonagh
Cormack
Information Standards
Assurance Coordinator
Noshaba Khan
Howard Fishwick
Stephen Hoy
Senior IG Advisor
Hayden Thomas
Genomics &
Biomedical
data Lead
David
Oppenheim
Intelligence & Strategy Division
Admin Assistant
Danielle Sweeney
(Hays) Raydean
Bevington’s substantive
post (secondment)
Information
Standards Lead
Scott Reid
Finance and
Procurement
Manager
Ben Assifuah
Benefits &
Business Change
Manager (7)
2xVACANCY
Information Standards
Business Manager (8a)
1xVACANCY
11/20/2013 P&I Structure: Version 2.16
8
Senior IG Advisor
(8b)
1xVACANCY
Establish Post count = 55
Additional Posts
• Jeanette Hall, Programme Manager for Information
Governance and Commissioning Programme (IMAS)
• Keith Thomas, Strategic Account Manager (on loan from
HSCIC)
• Bethan George, Peter Connoulty, Rob Milner, Wendy
Harrison, IG Information Specialists
• Mark Douglas, Stuart Hansom, Business Analysts
• Mahwish Noor (secondment) Business Support Officer
Open Data
Subject Matter
Expert
Rachel Merrett
Head of Open Data &
Transparency
Emma Doyle
Head of Strategic
Intelligence
Peter Flynn
Information Standards
Requirements Lead
Ian Townend
Admin Assistant
Simba Dzikiti
Open Data
Manager
Sandra Farrell
Senior Intelligence
Specialist
Xanthe Hannah
Junior Intelligence
Specialist
Dee Moore
Intelligence
Specialist
Victoria Hallam
Admin Assistant
Tbc (Hays)
Mahwish Noor
substantive post
(secondment)
Senior
Intelligence
Specialist
Paul Gavin
Intelligence
Specialist
Rachel Watkin
Junior Intelligence
Specialist
Tom Furber
Intelligence
Specialist (8a)
1x VACANCY
Open Data
Manager (7)
2xVACANCY
KEY:
VSM
Band 9
Interim arrangement
Established vacancies
Established posts
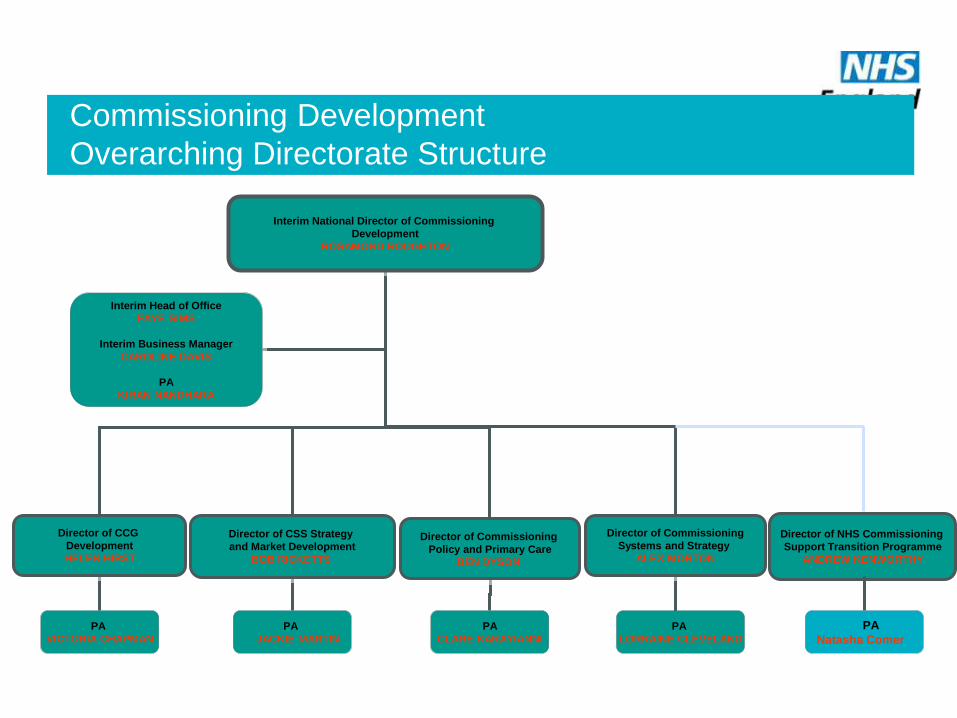
Commissioning Development
Overarching Directorate Structure
Interim National Director of Commissioning
Development
ROSAMOND ROUGHTON
Director of CCG
Development
HELEN HIRST
Director of CSS Strategy
and Market Development
BOB RICKETTS
Director of Commissioning
Policy and Primary Care
BEN DYSON
Interim Head of Office
FAYE SIMS
Interim Business Manager
CAROLINE DAVIS
PA
KIRAN NANDHARA
Director of Commissioning
Systems and Strategy
ALEX MORTON
PA
VICTORIA CHAPMAN
PA
JACKIE MARTIN
PA
CLARE KARAYIANNI
PA
LORRAINE CLEVELAND
Director of NHS Commissioning
Support Transition Programme
ANDREW KENWORTHY
PA
Natasha Comer
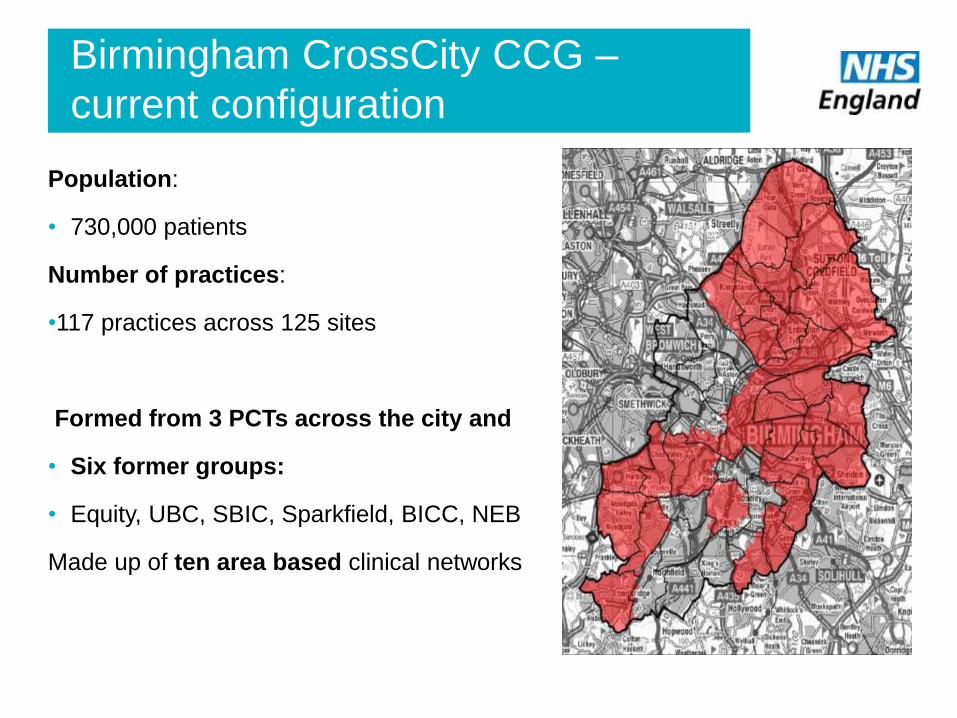
Birmingham CrossCity CCG –
current configuration
Population:
• 730,000 patients
Number of practices:
•117 practices across 125 sites
Formed from 3 PCTs across the city and
• Six former groups:
• Equity, UBC, SBIC, Sparkfield, BICC, NEB
Made up of ten area based clinical networks
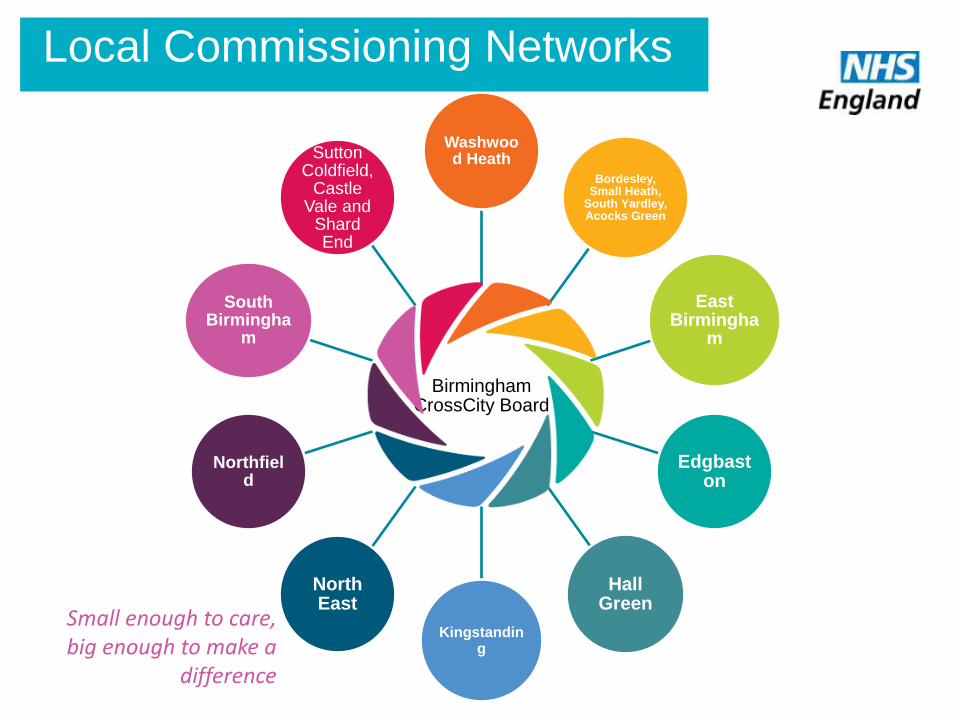
Birmingham CrossCity Board
Washwood Heath
Bordesley, Small Heath,
South Yardley, Acocks Green
East Birmingha
m
Edgbaston
Hall Green
Kingstanding
North East
Northfield
South Birmingha
m
Sutton Coldfield,
Castle Vale and
Shard End
Local Commissioning Networks
Small enough to care, big enough to make a
difference
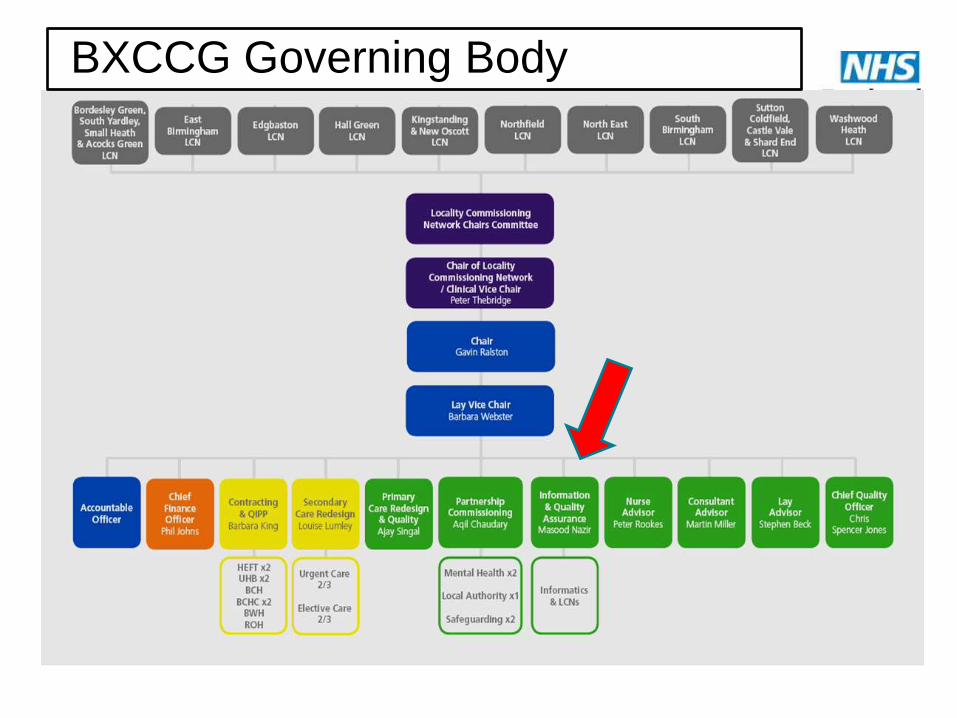
BXCCG Governing Body
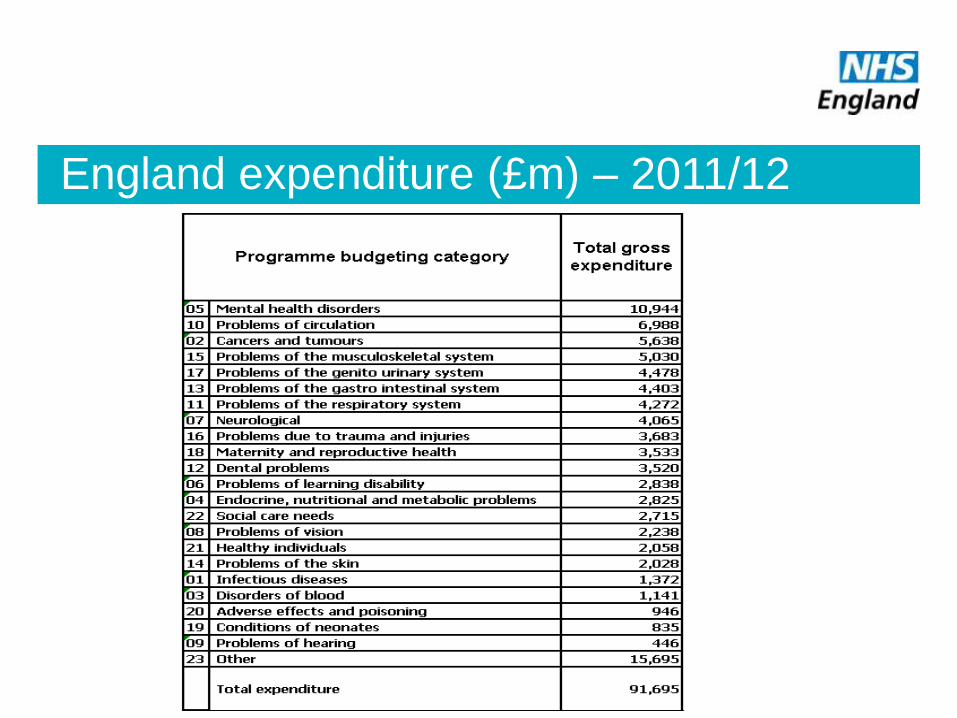
England expenditure (£m) – 2011/12
Key health investment tools
CCG Outcomes Tool – overview of prevalence, demography and outcomes for each CCG (just released – June
2013)
Programme Budgeting Benchmarking Tool – comparative spend data by PCT
Spend and Outcome Tool – looks at spend by programme compared to health outcomes (example on next slide)
Programme Budgeting Atlases – mapping software to illustrate metrics
NHS Comparators – metrics down to practice level – includes inpatients, outpatients, QOF and prescribing data
by spend and volume. Practice level data too
Inpatient Variation Expenditure Tool – comparative spend on high volume HRGs
Patient Reported Outcome Measures Tool – actual health gain from interventions such as hip and knee
replacements
NHS Atlases – tools containing maps showing variation in quality indicators
Primary Care Commissioning Application – QOF tool providing comparative CCG and practice performance
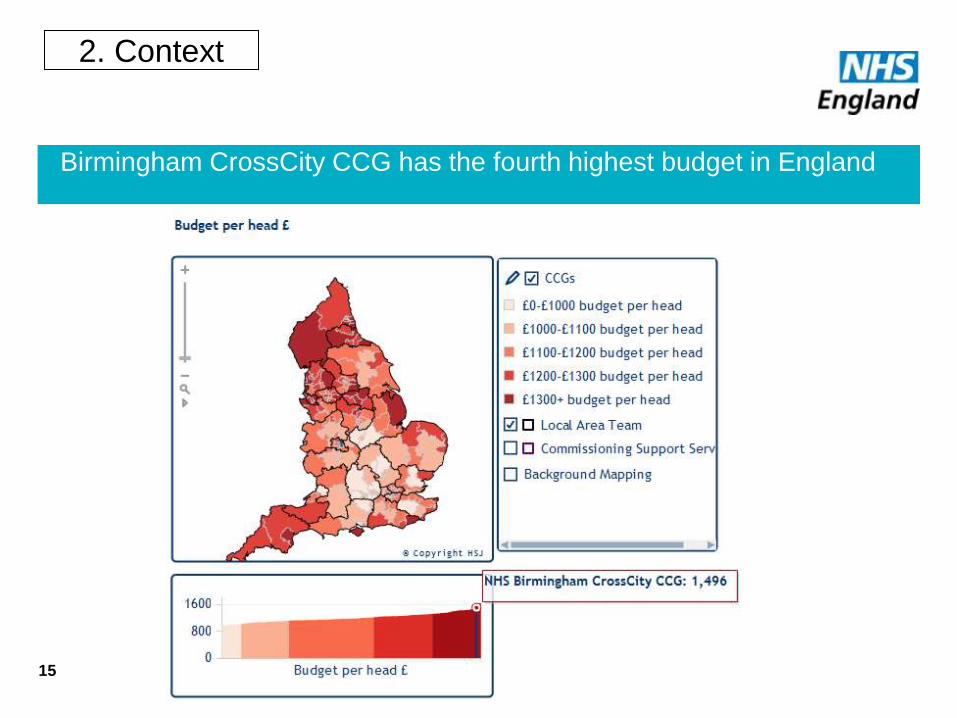
Birmingham CrossCity CCG has the fourth highest budget in England
15
2. Context
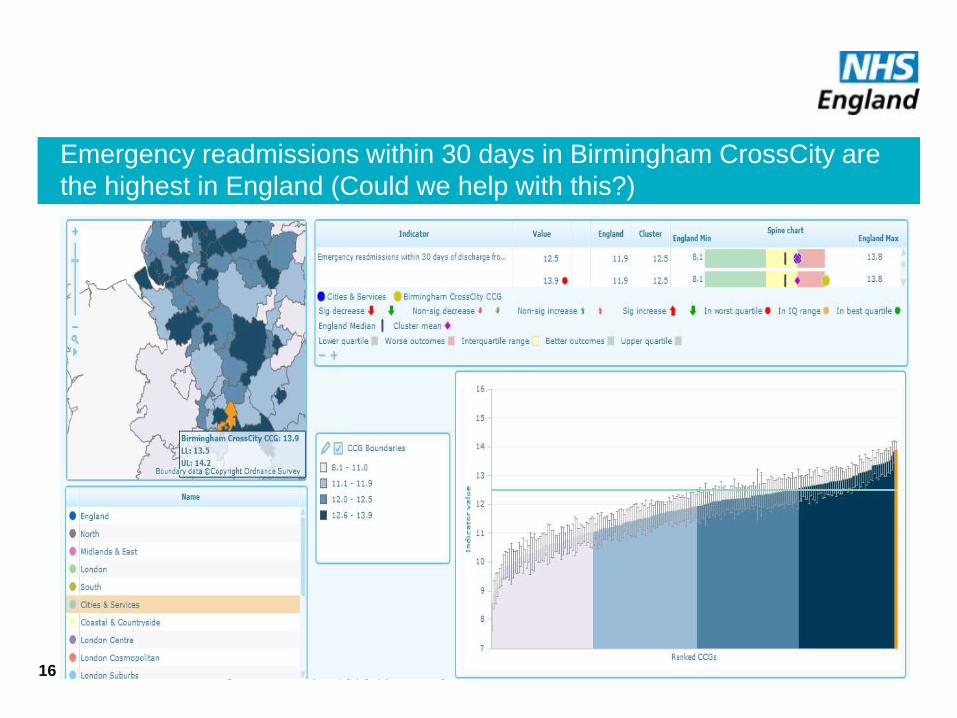
Emergency readmissions within 30 days in Birmingham CrossCity are
the highest in England (Could we help with this?)
NHS | Presentation to [XXXX Company] | [Type Date] 16
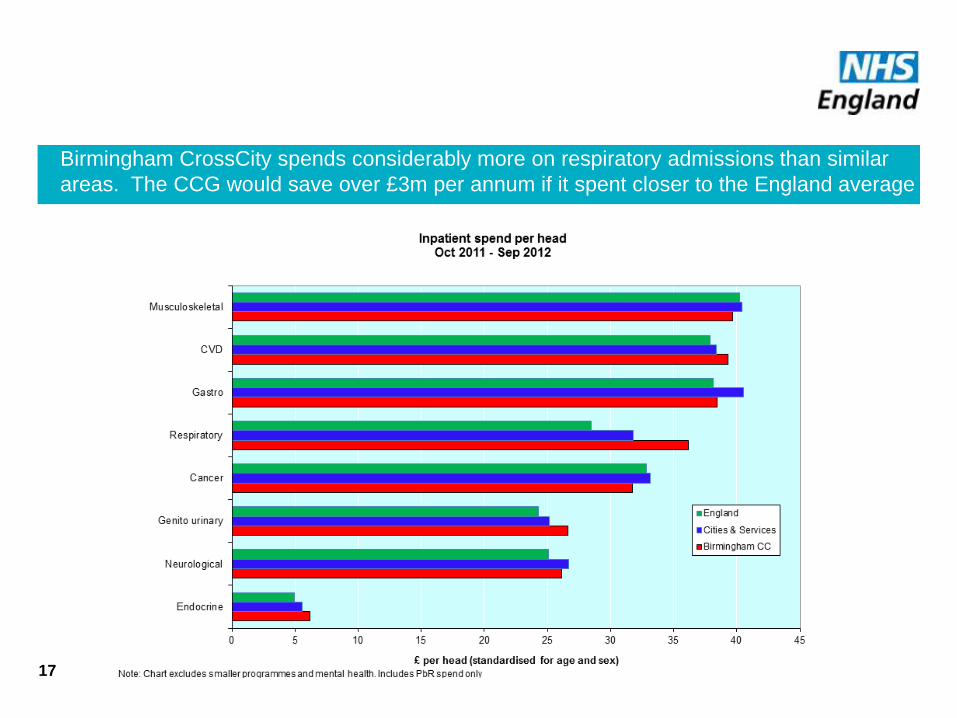
Birmingham CrossCity spends considerably more on respiratory admissions than similar
areas. The CCG would save over £3m per annum if it spent closer to the England average
17
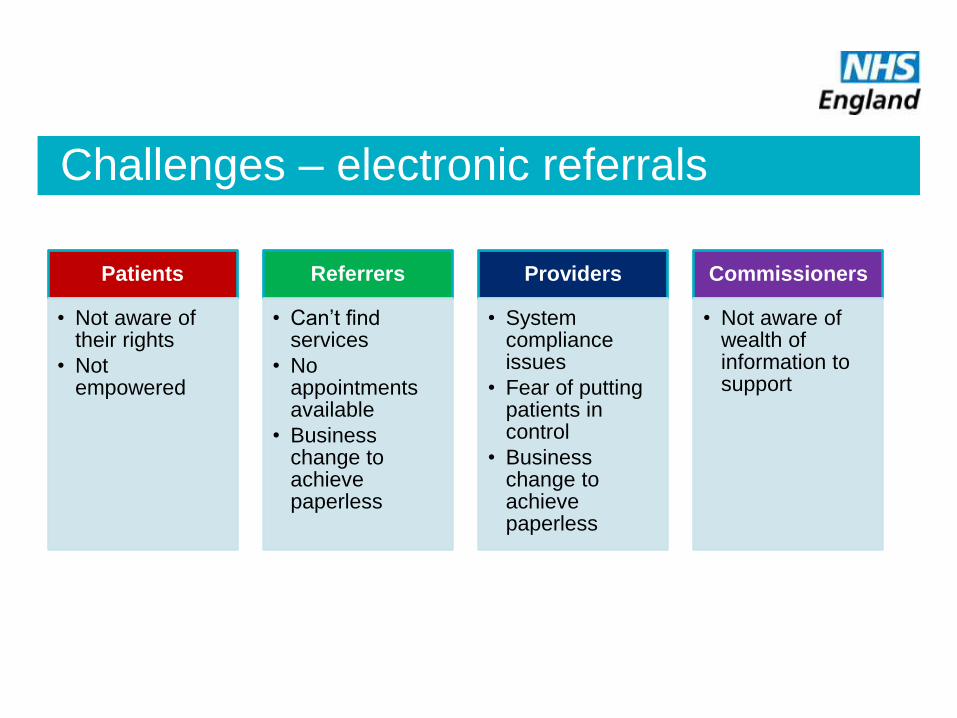
Challenges – electronic referrals
Patients
• Not aware of their rights
• Not empowered
Referrers
• Can’t find services
• No appointments available
• Business change to achieve paperless
Providers
• System compliance issues
• Fear of putting patients in control
• Business change to achieve paperless
Commissioners
• Not aware of wealth of information to support
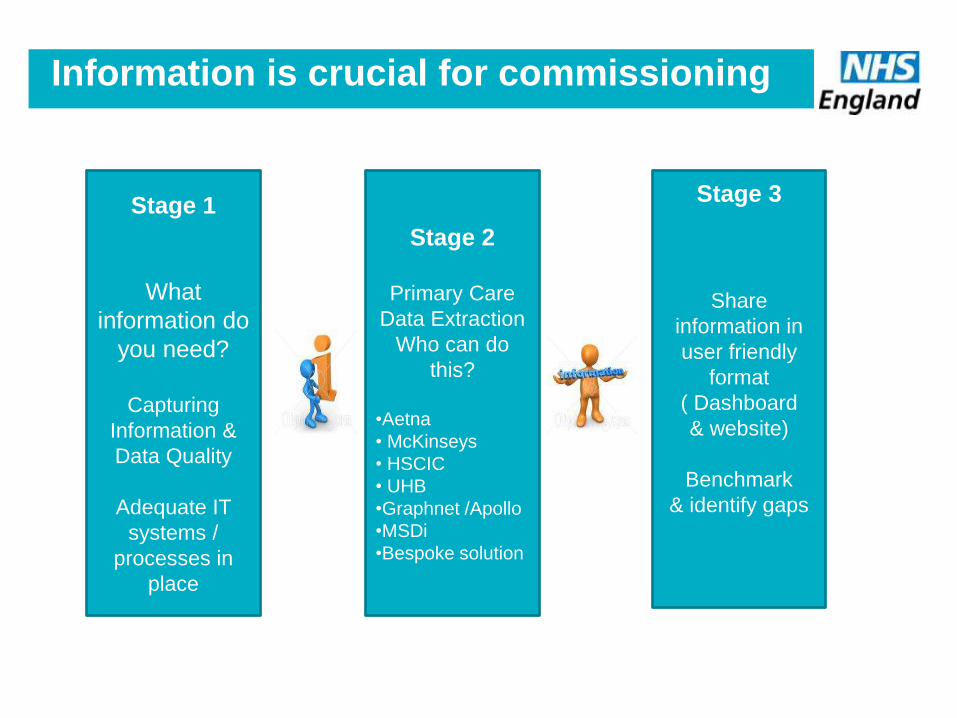
Information is crucial for commissioning
Stage 1
What
information do
you need?
Capturing
Information &
Data Quality
Adequate IT
systems /
processes in
place
Stage 2
Primary Care
Data Extraction
Who can do
this?
•Aetna
• McKinseys
• HSCIC
• UHB
•Graphnet /Apollo
•MSDi
•Bespoke solution
Stage 3
Share
information in
user friendly
format
( Dashboard
& website)
Benchmark
& identify gaps
What is Information Specification about?
• ISP is getting the right information into the right peoples hands in the format that allows them to understand the data quickly
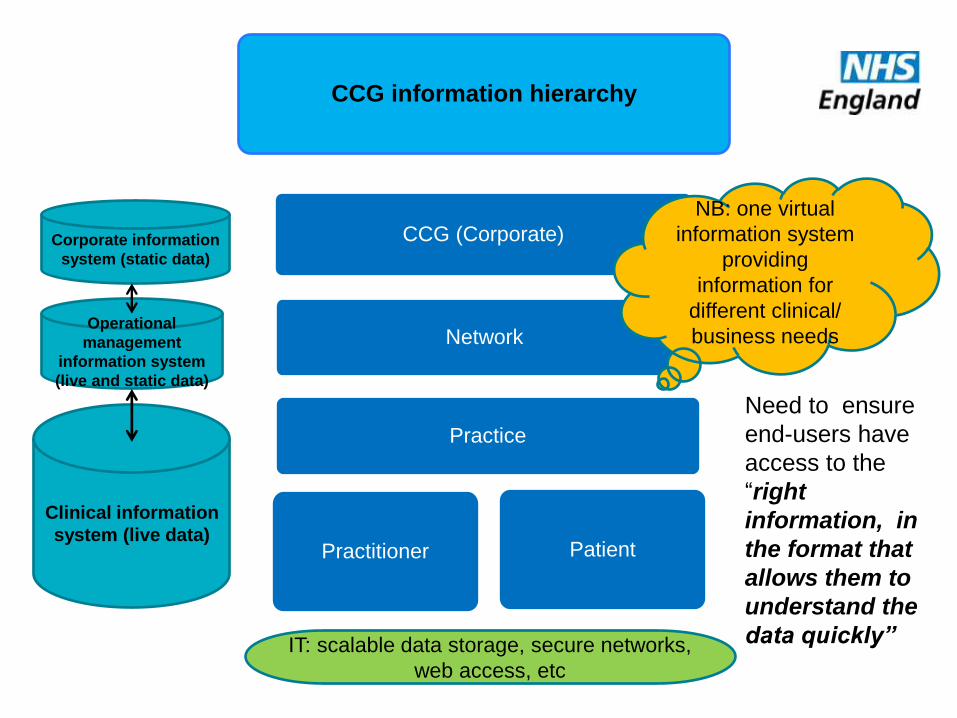
CCG information hierarchy
Practice
Practitioner Patient
CCG (Corporate)
Network
Clinical information
system (live data)
Operational
management
information system
(live and static data)
Corporate information
system (static data)
IT: scalable data storage, secure networks,
web access, etc
NB: one virtual
information system
providing
information for
different clinical/
business needs
Need to ensure
end-users have
access to the
“right
information, in
the format that
allows them to
understand the
data quickly”
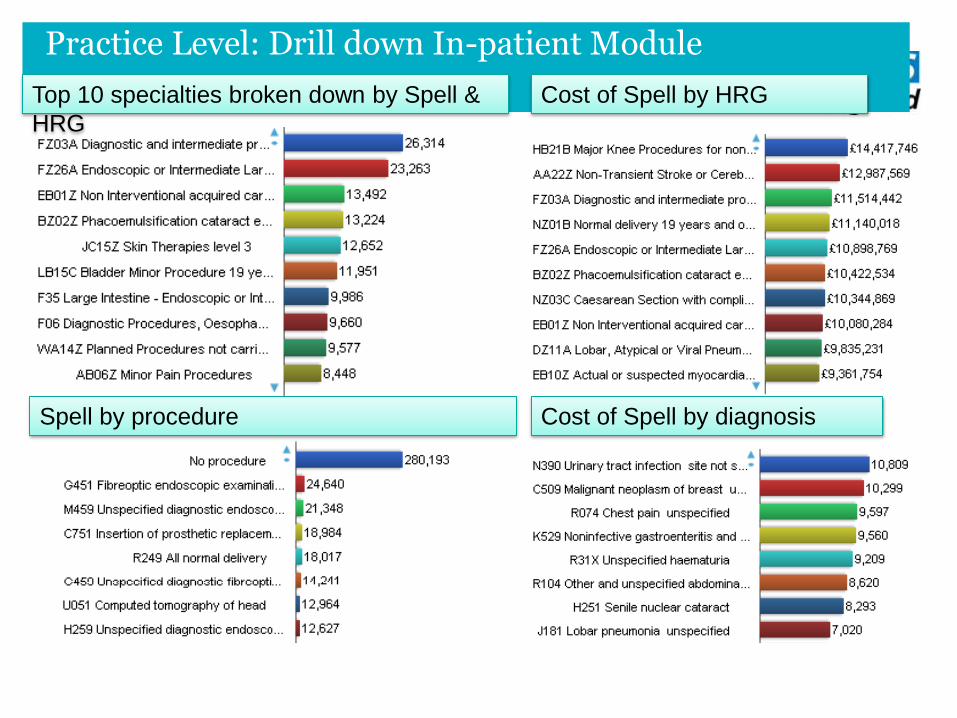
Practice Level: Drill down In-patient Module Top 10 specialties broken down by Spell &
HRG
Cost of Spell by HRG
Cost of Spell by diagnosis Spell by procedure
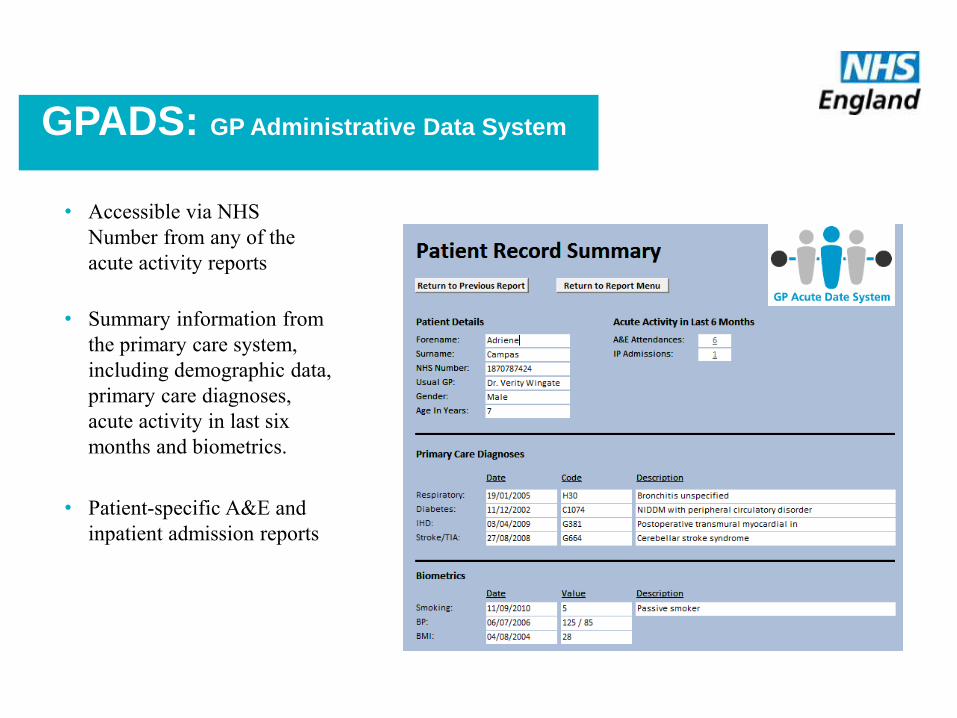
GPADS: GP Administrative Data System
• Accessible via NHS
Number from any of the
acute activity reports
• Summary information from
the primary care system,
including demographic data,
primary care diagnoses,
acute activity in last six
months and biometrics.
• Patient-specific A&E and
inpatient admission reports
PRIMIS Data Quality Indicator (PDQI)
• Updates the existing IM&T DES tools
• (IM&T DES - >7,200 practices uploaded results to CHART Online – comparative database)
• Uses MIQUEST data extraction & CHART tool for patient level analysis in practice
• Uses new version of CHART online to compare practice & CCG level data
• Uses some existing queries but also introduces new topics
©University of Nottingham 2013
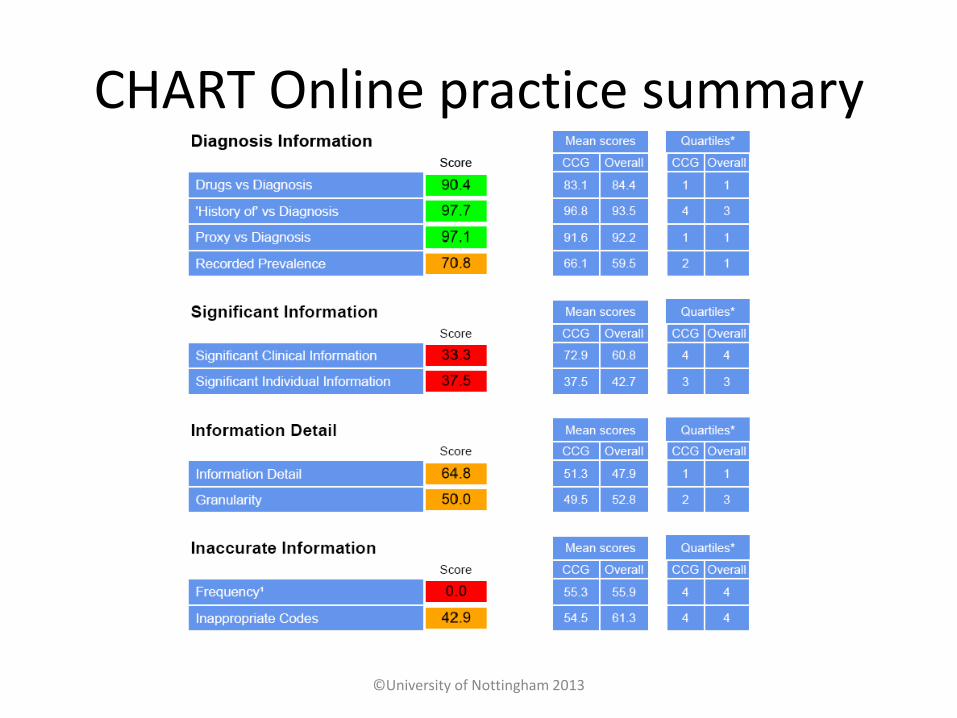
CHART Online practice summary
©University of Nottingham 2013
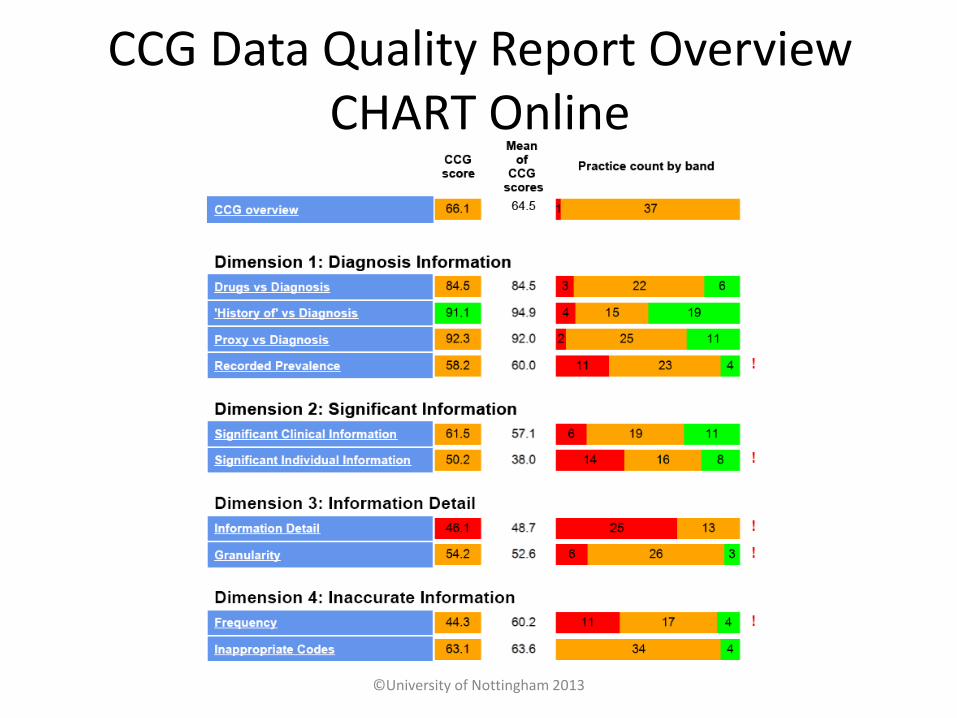
CCG Data Quality Report Overview CHART Online
©University of Nottingham 2013
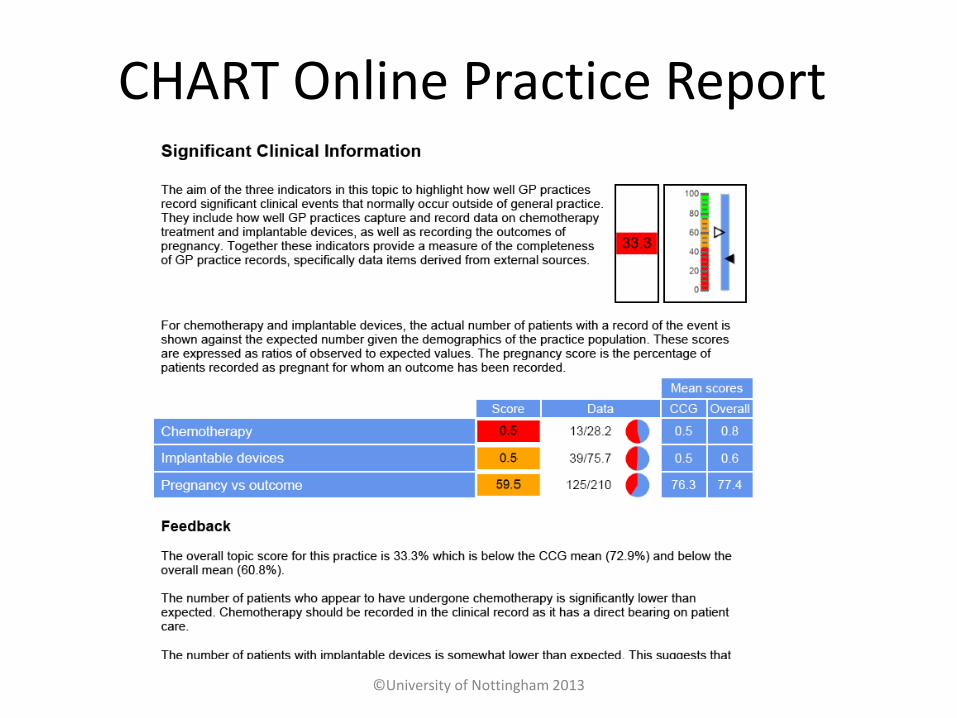
CHART Online Practice Report
©University of Nottingham 2013
28
NHS | Presentation to [XXXX Company] | [Type Date] 29
NHS | Presentation to [XXXX Company] | [Type Date] 30
NHS | Presentation to [XXXX Company] | [Type Date] 31
NHS | Presentation to [XXXX Company] | [Type Date] 32
How does a commissioning body
influence anything?
•Mandatory elements in contracts
•Funding projects
• National
• Local
•Transfer of good practice
• Galley of examples Awards
• “Do once and share”
•Influence by… influence
33
“Know where to find the information and how to use it – That’s the secret of success”
35
36
The challenge
• Implementing commissioning intelligence solutions is a challenge, a major project and a substantial change to the way care is delivered
• But it is achievable, and others have achieved it and gained many benefits
• Achieving good data quality remains a challenge, but sharing of data is one of the first steps on the road to achieving

Give me a kick
when it’s all sorted
Dr Masood Nazir:
How can we help?





























