Embed Size (px)
Citation preview
th16 Biennial Congress of theAsian Association of Endocrine Surgeons
AsAES 2018Theme: Building Endocrine Surgery of Tomorrow
March 8 (Thurs) - 10 (Sat), 2018
Hotel
Aerocity,New Delhi, IndiaJ W M A R R I O T T
Pre-Congress Workshop, March 6 (Tue) - 7 (Wed), 2018
AIIMS, New Delhi
Organised By:Department of Endocrine SurgerySanjay Gandhi Postgraduate Institute of Medical SciencesRaibareli Road, Lucknow, Uttar Pradesh, India
E-mail : [email protected] www.asaes2018.org Tel. +91-522-2668777 Fax. +91-522-2668777

I n d e x
1. Welcome Message Pg 1-4
2. AsAES Council Pg 5
3. Organising Committee Pg 6
4. Plenary Speakers Pg 7
5. Pre-Congress Event Pg 8
6. Programme at a Glance Pg 9
7. Plenary Speakers Abstracts Pg 10-17
8. Registration Detail Pg 18
9. Contact Us Pg 18

Welcome Message by the
AsAES Chairman
1
Welcome to the 16th Congress of the Asian Association of Endocrine Surgeons
It is my great honor and pleasure to welcome you to the 16th Congress of the Asian Association of Endocrine Surgeons, to be held from March 8 to 10, 2018 at New Delhi, India by Congress President Saroj K. Mishra with the official support of the Indian Association of Endocrine Surgeons. Congress President Saroj K Mishra is Professor and Head of Department of Endocrine Surgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India. He selected judiciously J W Marriott Hotel, NewDelhi Aerocity as the location and venue of the Congress. The venue is very easy to access from the International Airport and to the central area of Delhi City also. Therefore, you can join the Congress without difficulty wherever you live, and you can also enjoy unique traditional Indian cultures before or after the Congress.
Our Association was found in 1986 and the first Congress was held in Tokyo 2 years later, led by first President Yoshihide Fujimoto,sadly, who passed away in July 2016. He wanted to have an association similar to the International Association of Endocrine Surgeons to provide anopportunity for mutual understandings and friendship among endocrine surgeons in Asia. Since then, the meeting is being held biennially in many cities in Asia. The 5th Congress was held in 1996 in Hyderabad, India, led by President Lakshmana Rao. Therefore, the 16th Congress in 2018 is the second Congress to be held in India. Since the Local Organizing Committee is officially supported by the Indian Association of Endocrine Surgeons, I expect that the Congress will be very successful and provide a forum for further exchange of information and the development of new knowledge in the field of endocrine surgery, and that it will be a very good opportunity to expand the spirit of friendship among endocrine surgeons in Asia. As Chairman of the AsAES, I cordially invite all of you to the 16th Congress in 2018.
Akira Miyauchi, MDChairmanAsian Association of Endocrine Surgeons

Dear Friends,Greetings from the Organization Committee of AsAES 2018.It is with great pleasure we wish to invite you to the 16th Biennial Congress of Asian Association of Endocrine Surgeons to be held on March 8th–10th, 2018 at the Hotel J W Merriott, Aerocity, New Delhi, India. This Congress is coinciding with the Silver Jubilee year of the establishment of Indian Association of Endocrine Surgeons (IAES). During the last two decades the speciality of Endocrine Surgery has grown leaps and bound in several parts of our country and Asia Pacific region. Establishment of endocrine surgery units/departments, training opportunities, safe and quality surgical care, adoption of new technology, high quality research publications etc. In spite of financial and logistic constraints the rapid growth of the specialty could be attributed to visionary leadership, strong determination and excellent training opportunities. Endocrine Surgery is a relatively new specialty compared to other specialities of surgery. However, it possesses unique features which others specialities do not have, so it continues to attract new talent. The real challenge for us is to nurture this talent and build the future of endocrine surgery. The theme of 2018 AsAES congress is thus “Building the Endocrine Surgery of Tomorrow”. Besides, the congress will have regular scientific features like Plenary Lectures, Symposia, Panel Discussions, Meet the Professor, Grand Round, Selected Surgical Video demonstration , Satellite Symposia and Poster Presentation in both standard hard copy and Multimedia formats. We are going to have Pre-congress workshop on 6th and 7th March 2018 which will be announced shortly. Plan your abstracts , presentation for the call which will be announced in March. The weather in New Delhi in early March is quite pleasant. You don’t need to carry warm clothes as the spring will be setting in by that time. There are many things to see in New Delhi and nearby cities like Agra (world famous Tajmahal ), and Jaipur (palaces). Our event management team will help you in planning the tour of your choice. Do bring your family to enjoy the best season of India in it’s capital and beyond.
With warm regards
(Saroj K Mishra)Congress PresidentAsAES2018
Message from the desk of
Congress President
2

Dear Friends
As the past president of the 15th congress of AsAES, it is my great pleasure to send a
good will message for the 16th Congress of AsAES to be held in New Delhi , India. We
know how hard it is to prepare for a successful congress from previous experiences.
So, I would like to express my sincere gratitude and appreciations to Congress
President, Saroj Mishra and the Local Organizing Committee for their endeavor to
make the congress a successful one. Let's not forget that surgical management of
endocrine disease is one of the most common procedures of practice and the
treatment concepts are also rapidly changing. There is no single method or technique
to fit all endocrine treatments, because the cure should be tailored according to
several factors including patients, surgical skill, experience and biomaterial available.
The 16th Congress of AsAES will be a landmark event for all Endocrine surgeons in the
Indian and Asian endocrine society in the diagnosis and management of Endocrine
disease .
I am looking forward to meeting all of the members of AsAES at the 16th Congress in
New Delhi, India.
Euy Young Soh, MD., PhD
Professor, Dept of Thyroid and Endocrine Surgery
Ajou University Hospital
Message from the Past President
3

Dear Friends,Greetings from Indian Association of Endocrine Surgeon
On behalf of the Indian Association of Endocrine Surgeons, I would like to
congratulate you and your team for hosting and making excellent arrangements for
16th Biennial Congress of Asian Association of Endocrine Surgeons at New Delhi. I am
indeed very happy to note that the Congress is coming to India after a long hiatus and
it is only apt that India is hosting it since it is the silver jubilee year of the formation of
Indian Association of Endocrine Surgeons which was the brainchild of our Founder
President Prof S Vittal. I note that eminent faculty from all over the globe will converge
to New Delhi to participate in the academic deliberations which will be of immense
benefit to both practising surgeons and trainees interested in Endocrine Surgery. It is
also a pleasant time to visit Delhi which has numerous places to captivate the interest
of the delegates. I once again extend a warm welcome to all the delegates and faculty
and wish the Conference to be a grand success..
With warm regards
(Prof. S. Babu)
President
Indian Association of Endocrine Surgeons
Message from President,
”Indian Association of Endocrine Surgeons”
4

A SAES 2018 COMMITTE
A SAES COUNCIL MEMBERS
A SAES INTERNATIONAL ADV ISORY COMMITTEE
Akira Miyauchi( Japan )
Chairman
Rohaizak Muhammad( Malaysia)
Secretary Treasurer
Saroj K Mishra( India )
Congress President
Euy-Young Soh( Korea )
Immediate Past Congress President
Julie Miller
Name
Name
Amr Mohsen
Saroj K Mishra
Iwao Sugitani
Cheong Soo Park
CY Lo
Ming-Khoon Yew
Brian Lang
Hisham Abdullah
Amit Agarwal
Radan Dzodic
Soo Khee Chee
Ranil Fernando
Chen-Hsen Lee
Tran Nguc Luong
Robert Parkyn
Ozer Makay
Shin-ichi Suzuki
Imisairi Abd Hadi
Cheah Wei Keat
Imisairi Abd Hadi
B.G Ratnasena
Shih-Ming Huang
Suchart Chantawibul
Chen Guang
Tian Wen
China
China
Australia
Country
Country
Egypt
India
Japan
Korea
Hong Kong
Australia
Hong Kong
India
MalaysiaSerbia
Singapore
Sri Lanka
Taiwan
Vietnam
Australia
Turkey
Japan
Malayasia
Singapore
Malaysia
Sri Lanka
Taiwan
Thailand
5

OFF ICE BEARERS
LOC AL ADV ISORY COMMITTEE
SC IENT IF IC COMMITTEE
EXECUTIVE COMMITTEE
Anil K. Sarda( New Delhi )
ChairmanOrganising Committe
Aravindan Nair( Vellore )Chairman
Scientific Committee
Saroj Mishra( Lucknow)President
AsAES2018
Anjali Mishra( Lucknow)Secretary General
Gyan Chand(Lucknow)Treasurer
Position Name CountryName Place Name Place
S Vittal Chennai R N Katariya Chandigarh
M M Kapur New Delhi L K Sharma New Delhi
Jothi Ramlingam Madurai K D Varma Lucknow
Ramakant Lucknow N Dorairajan Chennai
M Chandrasekaran Chennai Gopalkrishnan Nair Chennai
R V Suresh Chennai Santosh John Abraham Cochin
Abhaya Dalvi Mumbai
Name Place Name Place
Aravindan Nair Vellore (Chair) Venkatesh PV Rao Bangalore
Anurag Srivastava New Delhi Arunansu Chandigarh
Sunil Chumber New Delhi M J Paul Vellore
Deepak Abraham Vellore N Dorairajan Chennai
Anand Mishra Lucknow Gaurav Agarwal Lucknow
P R K Bhargav Vijaywada Santosh John Abraham Cochin
Pooja Ramakant Lucknow SaiKrishna Vittal Chennai
Divya Dahiya Chandigarh P V Pradeep Kozhikode
Kulranjan Singh Lucknow Prateek Mehrotra Lucknow
S Dhalapathy Chennai Sabaretnam M Lucknow
Name Place Name Place
Anil K Sarda (Chair) New Delhi Anjali Mishra (Secretary General) Lucknow
Gyan Chand (Treasurer) Lucknow B N Mohanty Cuttuck
A K Mohanty Cuttuck Ritesh Agarwal Mumbai
Chitresh Kumar New Delhi N Dorairajan Chennai
Naval Bansal Chandigarh Amit Agarwal Lucknow
Anurag Srivastava (New Delhi)
Workshop Patron
6

Quan-Yang Duh,USA
Tsuneo Imai, Japan
Anders Bergenfelz, Sweden
Richard Prinz, USA
Herbert Chen, USA
Akira Miyaychi, Japan
C S PandavIndia
Yoshihiro TominagaJapan
PLENARY SPEAKERS7
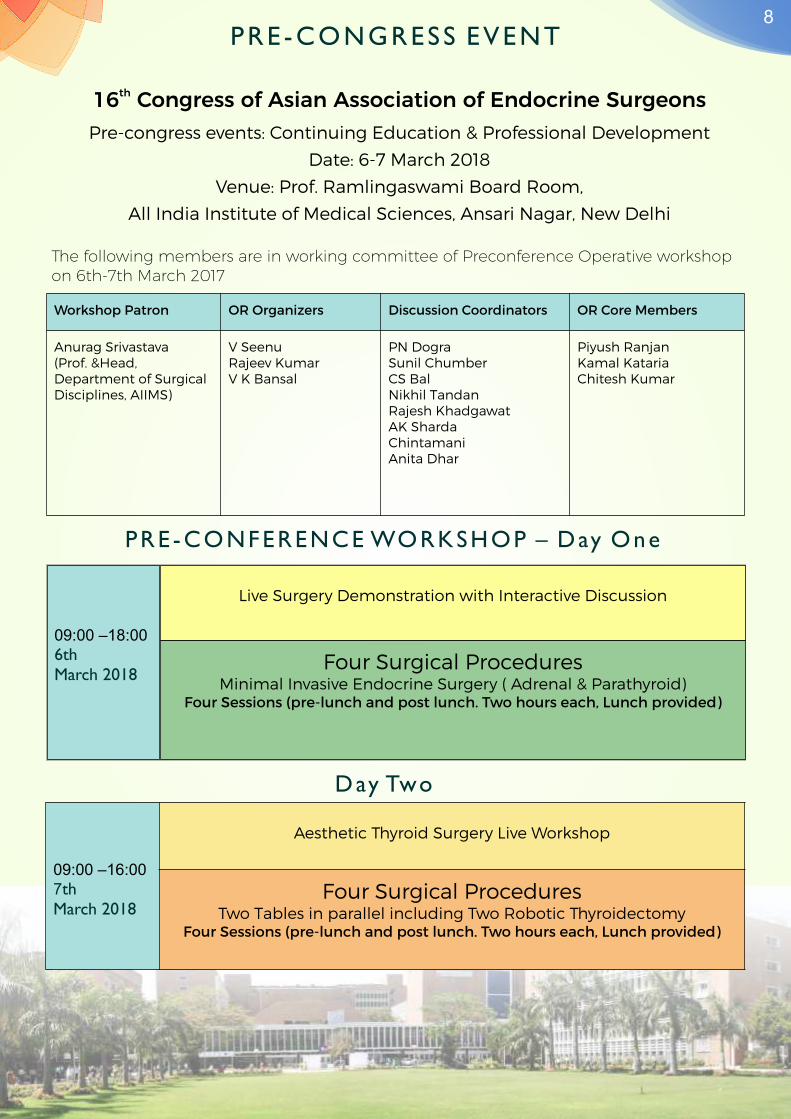
PRE -CONGRESS EVENT
PRE -CONFERENCE WORKSHOP – Day One
Day Two
Workshop Patron OR Organizers Discussion Coordinators OR Core Members
Anurag Srivastava(Prof. &Head, Department of Surgical Disciplines, AIIMS)
V SeenuRajeev KumarV K Bansal
PN DograSunil ChumberCS BalNikhil TandanRajesh KhadgawatAK ShardaChintamaniAnita Dhar
Piyush RanjanKamal KatariaChitesh Kumar
th16 Congress of Asian Association of Endocrine SurgeonsPre-congress events: Continuing Education & Professional Development
Date: 6-7 March 2018
Venue: Prof. Ramlingaswami Board Room,
All India Institute of Medical Sciences, Ansari Nagar, New Delhi
The following members are in working committee of Preconference Operative workshop on 6th-7th March 2017
09:00 –18:006th March 2018
Live Surgery Demonstration with Interactive Discussion
Four Surgical ProceduresMinimal Invasive Endocrine Surgery ( Adrenal & Parathyroid)
Four Sessions (pre-lunch and post lunch. Two hours each, Lunch provided)
09:00 –16:007th
March 2018
Aesthetic Thyroid Surgery Live Workshop
Four Surgical ProceduresTwo Tables in parallel including Two Robotic Thyroidectomy
Four Sessions (pre-lunch and post lunch. Two hours each, Lunch provided)
8

PROGRAMME AT A GLANCE9
Pre-congressWorkshop AsAES 2018
TimeDay 1
March 6Day 2
March 7Day 1
March 8, 2018Day 2
March 9, 2018Day 3
March 10, 2018
07:30-08:20 Meet the Professor Meet the Professor
08:30-09:00 Opening CeremonyPlenary Session 3 : State-of-the-Art LectureQuan Yang Duh (USA)
Meet The Professor
09:00-10:30
Plenary Session 1Historical Lecture:Chandrakant S. Pandav India
Opening Plenary Lecture:Richard Prinz, USA
Key Note Lecture:Akira Miyauchi, Japan
Plenary Session 4: Theme SymposiumBuilding Endocrine Surgery of Tomorrow
Free paper Session 7-9
Clinical Grand Round-3 Presenta�on of Interes�ng Cases
10:30-11:00 Coffee Break, Poster Walk & Networking
11:00-12:30
Free Paper Award Sessions
1.Fujimoto Best Research Paper
2.LOC Best Oral Paper
3. LOC Best Poster-Podium Presentation
Continuing Endocrine Surgery Education & Professional Skill Development
Thyroid and ParathyroidUSG Course
Symposium 7Special Situations in Endocrine Surgery
Symposium 8Neuro-endocrine Tumors of GI Tract & Pancreas
Symposium 9Contemporary Issues in Endocrine Pathology
Continuing Endocrine Surgery Education & Professional Skill DevelopmentMaster Video Demonstration by Experts
Endocrine Surgery Practice in Low Resource Settings PanelSouth Asia, Central & West Asia, Gulf, CIS, ASEAN (CLMV), Africa, Latin America, Eastern Europe & Balkan Countries
12:30-13:30 Council MeetingLuncheon SatelliteSymposium
Luncheon SatelliteSymposium
Endocrine Surgery Quiz
Closing Ceremony followed by Lunch& City Site-Seeing
13:30-14:00 Business Meeting
14:00-15:30
Symposium 1Management of Benign Goitres
Symposium 2Differentiated Thyroid Carcinoma
Symposium 3Functional Thyroid Disease
Continuing Endocrine Surgery Education & Professional Skill Development
Clinical Grand Round 1
Plenary Session 5:Guest Lecture 2Herbert Chen (USA)
Special Lecture 2Yoshiriro Tominaga (Japan)
Coffee Break, Poster Walk & Networking
15:30-16:00 Coffee Break, Poster Walk & NetworkingSymposium 10Pheochromocytoma & Paraganglionoma
Symposium 11Management of Adrenal Cortical Neoplasms
Symposium 12Functional disorders of Parathyroid Glands
Endocrine Surgery Video Award Session
Plenary Session 2Guest Lecture 1: Anders Bergenfelz, Sweden
Special Lecture 1:Tsuneo Imai, Japan
16:00-17:00
17:00-18:30
Symposium 4Medullary Thyroid CarcinomaSymposium 5Technology in Endocrine SurgerySymposium 6Management of Advanced Thyroid Cancer
Continuing Endocrine Surgery Education & Professional Skill Development Clinical Grand Round 2
Free paper 4-6
Multi-Disciplinary
Endocrine Tumor
Board
19:00 onward
Presidential Welcome Dinner Cultural Programme & Gala Dinner
Hotel
Aerocity,New Delhi, IndiaJ W M A R R I O T T
Venue:

The National Cancer Database and the Treatment of Thyroid CancerRichard Prinz,
Clinical Professor of Surgery, Department of SurgeryNorth Shore University Health System
University of Chicago Pritzker School of Medicine, United States of America
The National Cancer Database [NCDB] is a nationwide oncology database. It documents 70% of all newly
diagnosed cancers in the USA. Data from the NCDB has had and continues to have a major influence on the
ATA Guidelines for the surgical management of differentiated thyroid cancer. The findings of the 2007
Bilimoria et al paper and the 2014 Adam et al paper will be reviewed and their impact on the 2009 and 2015 ATA
guidelines respectively delineated. Recent work by our group has shown that the large increase in the diagnosis
of follicular variant of papillary cancer among patients with papillary thyroid cancer affects the findings in the
Adam paper. There is an increase in overall survival in patients with classical papillary cancer 2-4 cm in size
having total thyroidectomy versus lobectomy. This difference is not seen with FVPTC. Our use of NCDB data
has shown that the 2015 ATA guideline change in patients age from 45 to 55 years as a factor in the staging of
follicular thyroid cancer may not be as appropriate as for papillary thyroid cancer. Survival for papillary thyroid
cancer decreases incrementally with increasing age, and age 55 seems appropriate as a cut off for a change that
effects overall the survival of papillary thyroid cancer. However, the survival for follicular cancer has a sharp
decrease at age 45 so the increase to age 55 as a change in age effecting T category and ultimately stage is not
appropriate. We have also used NCDB data to show that radioiodine therapy has the same beneficial effect on
survival whether administered within 3 months of thyroidectomy or after 3 to 12 months showing that delayed
therapy if necessary is not detrimental. In conclusion this large database will continue to be a useful tool to
answer new questions concerning thyroid cancer and the answers it provides will affect the staging and
management of it.
10PLENARY SPEAKERS ABSTRACT

Active surveillance as the first-line management for patients with low-risk papillary microcarcinoma of the thyroid
Akira Miyauchi, MD, PhDKuma Hospital, Center for Excellence in Thyroid Care, Kobe, Japan
Background
The incidence of thyroid cancer is increasing globally. This is mainly due tothe increase indetection of small
papillary carcinomas, including papillary microcarcinomas (PMCs). Overdiagnosis and overtreatment of
PMCs are suggested.
Methods
In 1993, Miyauchi proposed a clinical trial to compare surgery and active surveillancefor low-risk PMCs
atKuma Hospital, which was approved and the trial started in the same year. Patients choseactive
surveillance or immediate surgery. At the lecture, I will shares our 25-year experience and the outcomes of
these managements on more than2,000 patients with low-risk PMCs.
Results
The oncological outcomes of these management groups were similarly excellent. At 10 years of active
surveillance on 1,235 patients, 8 % and 3.8% of the patients showed tumor enlargement by 3 mm or more
and novel appearance of lymph node metastasis, respectively.Younger patients tended to show disease
progression more often than older patients did. Patients with these slight progressions of the disease were
successfullytreated with a rescue surgery. None of the patients in both study groups died of the disease or
had severe disease conditions. However, incidences ofunfavorable events, such as vocal cord paralysis,
hypoparathyroidism or patients on L-thyroxine,were significantly higher in the immediate surgery group
than in active surveillance group.Cost analyses showed that the total cost for immediate surgery with 10-
year follow-up was 4.1 the total cost of 10-year active surveillance. One might think that active surveillance
is merely procrastinating surgery. However, our estimation of lifetime probability of the disease progression
showed that the vast majority of the patients on active surveillance would not require surgery for their
lifetime.
Conclusions
With these experiences and accumulated evidences, at Kuma Hospital, we currently recommend the active
surveillance as the first-line management for patients with low-risk PMCs.
11

12
My life time work on management of secondary HPT
Yoshihiro Tominaga MD PhDDepartment of thyroid,parathyroid,bone metabolism
Noa Imaike Clinic, Nagoya, Japan
After internship I had been training at Department of Kidney Transplant Surgery also, I was taking care of
dialysis patients. The number of dialysis patients who could survive for long period has been gradually
increased. SHPT was one of serious complications in dialysis patients and some patients required for
parathyoidectomy(PTx).
At that time in our country, we could not acquire enough experience of PTx, then I visited Uppsala University
Hospital, Sweden to study operative procedure and parathyroid pathology. When I visited Uppsala 1989 they
performed bilateral neck exploration in all cases with HPT and total PTx with forearm atograft and resection of
thymic tissue from cervical incision. Their operative procedure for SHPT was same as our strategy. I learned
many things at Uppsala. The number of PTx for SHPT increased in our institute and the number exceeded 3000
cases at June 2013.
Based on pathological evaluation of removed glands we hypothesize that parathyroid glands transform from
diffuse hyperplasia to nodular hyperplasia in CKD and we confirmed that parathyroid cells consisted in nodule
proliferate monoclonally with high growth potential
and decreased expression of VDR and CaSR. To detect nodular gland by ultrasonography, predict resistant to
medical treatment and surgical indication.
Recently new medical treatments; VDR activator, calcimimetics and new phosphate binders
have been available in Japan and the number of PTx for SHPT remarkably decreased. However point of view
concerning, mortality, QOL, symptoms, bone status, nutrition,
cost effectiveness etc. many papers reported that PTx could be superior than medical treatment. PTx for SHPT
should be important role for endocrine surgeons.

Quan-Yang Duh, MD Professor and Chief, Section of Endocrine Surgery, UCSF
Technical and Technological Advances in Thyroid Surgery
Credible surgical treatment of thyroid diseases has been reported since the 10th Century in China and the
Middle East, but it was most well documented by Roger Frugardi of the School of Salerno in Italy in 1170.
Thyroid surgery remained dangerous and rare until late 19th Century. The “Magnificent Seven” of Theodor
Bilroth, Thedor Kocher, William Halsted, Charles Mayo, George Crile, Thomas Dunhill and Frank Lahey,
advanced the technique of thyroid surgery and defined the standard of modern thyroid surgery for most of
20th Century. Improved techniques and technological innovations helped solve problems that plagued
thyroid surgeons and their patients: infection, bleeding, hypothyroidism, hypoparathyroidism, recurrent
nerve injury, etc. Thyroid surgery for Graves' disease, large goiters and thyroid cancer became safe and
effective and was appropriately called “The supreme triumph of surgeon's art”. Currently, new approaches
in thyroid surgery are being developed to allow for better cosmetic result by avoiding anterior neck incision.
Such remote access surgery approaches the thyroid from the chest, axilla, and breast; some approach the
thyroid from behind the ear, and even from the mouth. Advances in endoscopy, energy devices, nerve
monitoring devices, intraoperative parathyroid imaging and robotic assistance lead to a dizzying array of
remote access techniques of so-called “scar-free” thyroid surgery. Advances in molecular genetics testing aid
surgical decision, both in diagnosis and in prognosis. A contemporary thyroid surgeon not only needs to be
an expert on the time-tested technique of Kocher but also to be able to select and use various techniques and
technologies to provide appropriate and individualized care for the patients with thyroid diseases
13

Universal Salt Iodization (USI) and elimination of Iodine Deficiency Disorders (IDD): A global public health success story
1 2 3Pandav SC , Sirohi A , Yadav K
Background
Dietary iodine intake is essential for production of thyroid hormones. Deficiency of iodine can lead to
goiter, mental impairment, growth retardation, increased pregnancy loss and infant mortality. USI was
adopted as a strategy for elimination of IDDs in World Health Assembly in 1993.
Objective
To assess current status of USI and Iodine nutrition and consequent decline of IDDs globally from available
evidence.
Methods: Online literature review was done to gather data regarding countries who have adopted USI,
Household level utilization of adequately iodized salt and Median Urinary Iodine Concentration (mUIC)
levels.
Results
World'spopulation having access to iodized salt increased from <20% in 1990 to 86% in 2017. In 1993, 93%
(113 out of 121) countries had insufficient iodine intake while 7% (8/121) had sufficient intake. None of the
countries reported excess iodine intake. In 2016, countries having insufficient intake reduced to 12%
(15/127)while countries with sufficient iodine intake increased to 80% (102/127). Ten countries (8%) were
found to be having excess iodine intake.
Discussion
USI has been proven to be effective strategy to deliver sufficient iodine to most population groups and
eliminate IDDs. Some of the key determinants to sustain and achieve USI are making salt iodization a
global industry norm, public education and social mobilization, supporting small scale producers, engaging
the processed food industry, regular and timely surveys and maintaining international support and
partnerships.
14

Eurocrine: an international endocrine surgical registry for quality control, benchmarking and research
Anders Bergenfelz Sweden
Background
With the growing economic pressure on the health care sector, it is of utmost importance to monito quality
control in general, and complications in particular. Further, the introduction of new technologies needs to
be evaluated. Research is preferably performed as randomized controlled trials (RCT). However, when
expected differences are small and for rare events and diagnosis, large prospective observational studies may
be preferred. RCTs may be considered as an experimental situation, whereas large observational studies,
national and international, should ideally mirror the “real world” situation more closely.
Methods
Eurocrine©, is an international registry for endocrine surgery, initially funded by a grant from the Health
Program of the European Union 2014-2017, which is now open for international participation. The content
of the registry covers the entire spectrum of endocrine surgery: thyroid, parathyroid, adrenal-
paraganglioma, and GEP-NET. Data is easy to download in Excel format. The registry has several user
friendly features: dashboards for comparisons between departments, national data and countries, on-line
graphs through Microsoft Power BI, and “My Eurocrine”, a flexible tool for local variables, observational
studies and RCTs.
Results
At present, December 2017, almost 90 departments and 12 societies of endocrine surgery, covering 20
countries, are participating in the database. Almost 22 000 operations have been registered. Some interesting
results will be presented. Several prospective trials are planned for 2018 and further.
Conclusion
By a dedicated collaborative of societies and with initial funding by the EU, an international database for
endocrine surgery, Eurocrine©, is now operational, and has already showed its usefulness for evaluating
outcomes and for research.
15
Long term outcome of adrenal surgery for the adrenal malignancy
Tsuneo ImaiNational Hospital Organization, Higashinagoya National Hospital
Introduction
Surgical treatment of adrenal tumors has evolved substantially over the past 40 years. However, non-
surgical treatments for malignant adrenal tumors have not been fairly developed. Complete surgical
resection is a treatment of choice for malignant adrenal tumor. Long-term outcomes of patients with
surgically treated malignant adrenal tumor are reported.
Materials & Methods
This study is retrospective analysis operated at a single institution from 1979 to 2012. The patients were
eligible for malignant adrenal tumor when the operation was primary, and macroscopic radical
adrenalectomy was performed (R0 or R1). Those patients who had retroperitoneal miscellaneous
malignancy involving adrenal gland, or malignant lymphoma treated as adrenal tumor, were excluded.
Diagnoses of adrenocortical carcinoma and metastatic carcinoma were confirmed by pathology. Malignant
pheochromocytoma was defined when distant metastases were proved or combined resections of adjacent
organs were necessary.
Results
There were 874 adrenal surgeries during the above period and 39 patients (4.5%) were eligible for the
criteria. The patients were13-73 year-old, median age was 43, and 18 male, 21 female. Adrenocortical
carcinoma: 11 (Cushing and subclinical Cushing: 5, non-functioning: 6), pheochromocytoma and
functioning paraganglioma: 17 (11 adrenal pheochromocytoma, 6 retroperitoneal paraganglioma), and
metastatic adrenal tumor: 11 (primary site: lung 6, gastric 1, rectal 1, kidney 1, cervix 1, pancreatic islet cell
1). Overall survival was 8.5 years; metastatic: 3.3, adrenocortical carcinoma: 13.3, pheochromocytoma:
17.9 years respectively. Combined resection was performed in 14 patients, which included kidney, liver,
pancreas, inferior vena cava, spleen, and colon.
Conclusion
Many patients with malignant primary adrenal tumor can be expected to have long-term survival after
thorough removal of the tumor, although surgical procedure is sometimes challenging. However, patients
with metastatic adrenal tumor have shorter prognosis, so we need to carefully consider surgical indication
for them
16

The surgical management of hyperparathyroidism has evolved over the last 20 years, transitioning from routine
bilateral neck exploration to frequently a minimally invasive approach. Adjuncts which have made this
transition possible include advancements in imaging techniques which allow the pre-operative localization of
adenomatous glands, the rapid parathyroid hormone assay and the use of 99m technetium sestamibi injections
the day of surgery to allow for gamma probe detection of abnormal glands. The gamma probe can help with
gland localization, which can be particularly useful in a re-operative field or with glands in ectopic locations. It
is also helpful in confirming that excised tissue is abnormal parathyroid tissue, alleviating the need for frozen
sections during surgery. In this talk, we will discuss parathyroidectomy in the year 2018.
17
Hyperparathyroidism and Parathyroid Surgery: where are we in 2018?
Herbert Chen
Chairman, Department of Surgery, University of Alabama at BirminghamSchool of Medicine, Birmingham, AL

Congress SecretariatDepartment of Endocrine SurgerySanjay Gandhi Postgraduate Institute of Medical SciencesRaibareli Road, Lucknow, Uttar Pradesh, India-226014
Tel. +91-522-2668777 Fax. +91-522-2668777
E-mail : [email protected] www.asaes2018.org
Meetings And More
56, Institutional Area,Sector 44,
Gurgaon, Haryana
Phone: +91-124-4534500
Fax: +91-124-4534585
MAIL US
CALL US
EMAIL US
For Registration, Accomodation,Visa Assistance, Site Seeing Tours
RegularDec 2017 - Jan 2018
On-siteFeb 2018 onwards
Overseas Delegates (Member ASAES) USD 600 USD 700
Overseas Delegates (Non-members) USD 700 USD 800
Overseas Delegates (Low & Middle Income Countries) USD 300 USD 350
Overseas Trainee* USD 250 USD 300
LMIC (Low & Middle Income Countries) Trainee* USD 125 USD 150
Indian Trainee* INR 8000 INR 10000
Nurse & Technician USD 50 USD 50
Accompanying Person** USD 50 USD 50
Members of Indian Association of Endocrine Surgeons (IAES)*** INR 12000 INR 15000
India & SAARC INR 17000 INR 20000
Gala Dinner USD 20INR 1,500
USD 20INR 1,500
- Trainee/Students are required to send a certificate from Head of the Department / competent authority to the Secretariat by e-mail.- Accompanying Person refers to a family member of participant.- Members of Indian Association of Endocrine Surgeons (IAES) are required to quote the IAES membership number.
Note:
1.Demad Draft should be made in the name of “Asian Association of Endocrine Surgeons”, payable at Lucknow.
2. For E-banking/ RTGS - Account Name : Asian Association of Endocrine Surgeons
Account Number : 36738319035 Bank Name : State Bank of India Bank Branch : SGPGIMS, Lucknow
IFSC Code : SBIN0007789 Swift Code : SBININBB500
REGISTRATION DETAILS18