Embed Size (px)
Citation preview

Introduction: Benign bone tumors are relatively common. The majority occur in children. Ward published, The Relative Incidence of Benign Bone Tumors in the Burden of Musculoskeletal Diseases in the United States in 2008. Ward determined that the national prevalence of benign bone tumors in rank order was 1,511 osteochondromas, 1,246 unicameral bone cysts, 769 giant cell tumors, 733 enchondromas, 632 aneurysmal bone cysts, and 577 metaphyseal fibrous defects. Benign bone tumors frequently create “contained” osseous defects that can lead to pathological fracture. Treatment is dependent on the aggressiveness of the lesion, location, containment, and bone strength. The Enneking staging system for benign bone tumors characterizes them as “latent”, “active”, or “aggressive”. Latent benign bone tumors remain quiescent or heal spontaneously. Active benign bone tumors progress but are limited by natural barriers such as the bone cortex or periosteum. Aggressive tumors do not respect these natural barriers and will extend into the soft tissues. Latent and even some active benign bone tumors can at times be observed. Most active and almost all aggressive benign bone tumors need to be treated. Tumors of all type that lead to pathological fracture need to be treated. Intralesional excision and grafting is commonly performed. Intralesional excision requires exposure of the entire tumor cavity, excision of all the lesional tissue, extending the margins with adjuvants if necessary, and filling the defect. There are many choices of graft material including autogenous bone graft, allograft, and bone graft substitutes. The defects created by benign bone tumors are contained and are thus good candidates for grafting with a bioceramic. Bone graft substitutes are attractive options because they are reported to be effective, avoid donor site morbidity, and are readily available. These biomaterials can be placed open or injected. Bioceramics are a class of osteoconductive bone graft substitutes that act as a scaffolding material for bone repair. They contain hydroxyapatite, calcium phosphate, calcium sulfate, or composite materials. Some of these are naturally occurring such as coral while others are manufactured. The history of bioceramics dates back to 1892 with the use of calcium sulfate for space occupying lesions by Dr. Dressman and subsequently Dr. Leonard Peltier. The original material was Plaster of Paris which is non-inflammatory and nonreactive and encouraged bone healing in a contained lesion. Subsequently, coralline hydroxyapatite was reported for similar lesions followed by other ceramics. All of these bone graft substitutes have the advantage of being non-immunogenic, non-inflammatory, in an unlimited supply, and packaged sterile. Mechanically, they have variable structural properties. They can be combined with osteoinductive cytokines. The purpose of this exhibit is to review the published pre-clinical and clinical outcomes with various bioceramics for the treatment of benign bone tumors. We will review their chemistry, strength, and biodegradation.
BIOCERAMICS IN THE TREATMENT OF BENIGN BONE TUMORS
Steven Gitelis, MD | Ross Wilkins, MD | Yale Fillingham, MD | Cara Cipriano, MD AAOS Biological Implants Committee
Leonard Peltier, MD Early developer of Plaster of Paris bone
graft substitute

The published literature of the last ten years was reviewed for studies related to the use of
bioceramics as graft material for benign bone lesions. The studies were characterized based
on levels of evidence and evaluated in terms of their methodology and clinical relevance.
Levels of Evidence for Primary Research Question
Therapeutic Studies—Investigating the Results of Treatment
Level I
• High-quality randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence intervals
• Systematic review2 of Level-I randomized controlled trials (and study results were homogeneous3)
Level II
• Lesser-quality randomized controlled trial (e.g., <80% follow-up, no blinding, or improper randomization)
• Prospective4 comparative study5
• Systematic review2 of Level-II studies or Level-I studies with inconsistent results
Level III
• Case-control study7
• Retrospective6 comparative study5
• Systematic review2 of Level-III studies
Level IV • Case series8
Level V • Expert opinion
• JBJS Author Instructions
SEM composite graft material (calcium sulfate/calcium phosphate)
SEM Bone-apatite appearing grafted with composite material (calcium sulfate/calcium phosphate)
METHODS
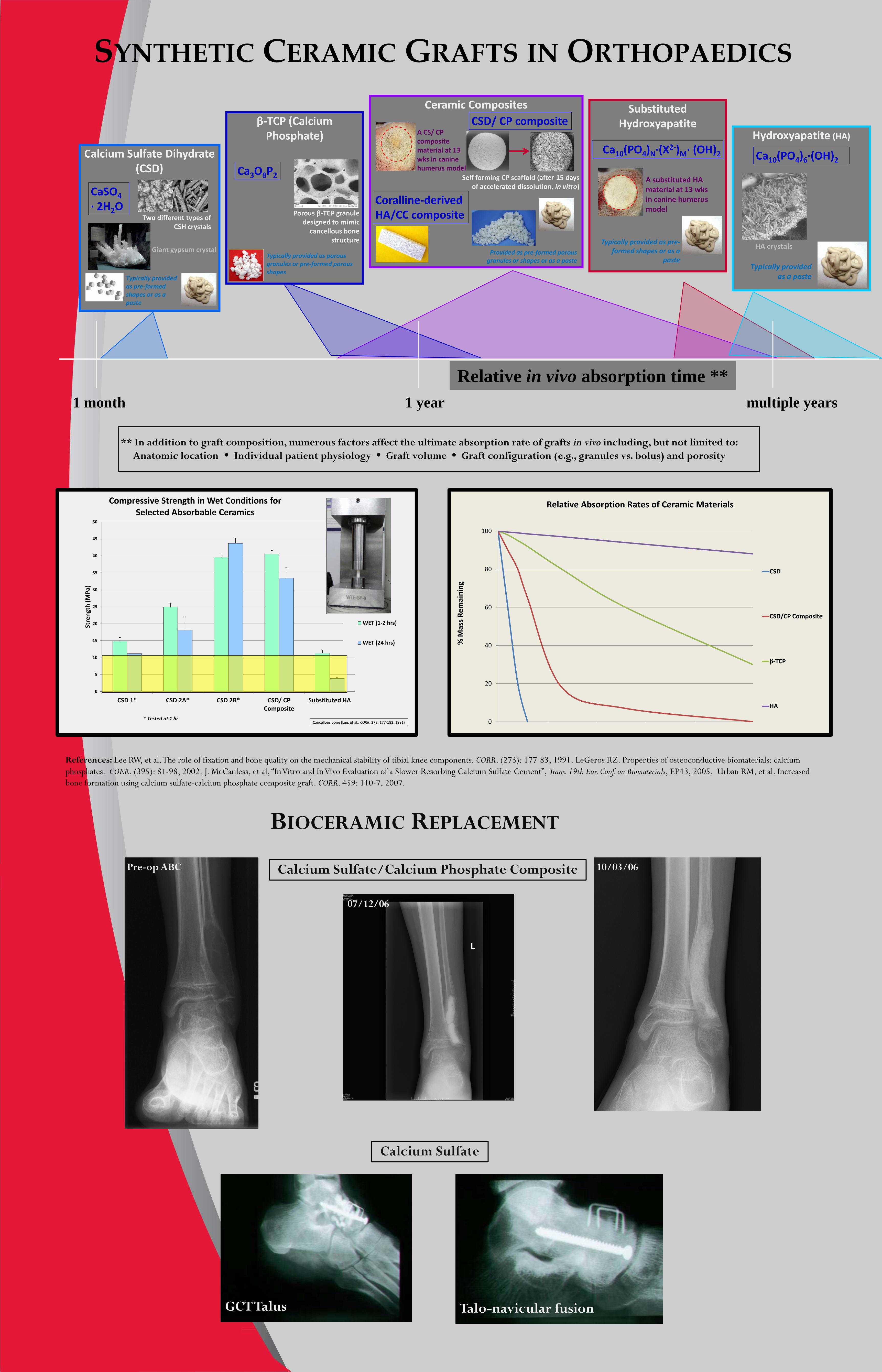
SYNTHETIC CERAMIC GRAFTS IN ORTHOPAEDICS
1 month 1 year multiple years
Relative in vivo absorption time **
References: Lee RW, et al. The role of fixation and bone quality on the mechanical stability of tibial knee components. CORR. (273): 177-83, 1991. LeGeros RZ. Properties of osteoconductive biomaterials: calcium phosphates. CORR. (395): 81-98, 2002. J. McCanless, et al, “In Vitro and In Vivo Evaluation of a Slower Resorbing Calcium Sulfate Cement”, Trans. 19th Eur. Conf. on Biomaterials, EP43, 2005. Urban RM, et al. Increased bone formation using calcium sulfate-calcium phosphate composite graft. CORR. 459: 110-7, 2007.
Calcium Sulfate Dihydrate (CSD)
CaSO4 · 2H2O
Typically provided as pre-formed shapes or as a paste
Two different types of CSH crystals
Giant gypsum crystal
β-TCP (Calcium Phosphate)
Ca3O8P2
Porous β-TCP granule designed to mimic
cancellous bone structure
Typically provided as porous granules or pre-formed porous shapes
Ceramic Composites CSD/ CP composite
Coralline-derived HA/CC composite
Self forming CP scaffold (after 15 days of accelerated dissolution, in vitro)
Provided as pre-formed porous granules or shapes or as a paste
A CS/ CP composite material at 13 wks in canine humerus model
Substituted Hydroxyapatite
A substituted HA material at 13 wks in canine humerus model
Ca10(PO4)N·(X2-)M· (OH)2
Typically provided as pre-formed shapes or as a
paste
Hydroxyapatite (HA)
Ca10(PO4)6·(OH)2
Typically provided as a paste
HA crystals
0
20
40
60
80
100
0 10 20 30 40 50
CSD
CSD/CP Composite
β-TCP
HA
Relative Absorption Rates of Ceramic Materials
% M
ass R
emai
ning
0
5
10
15
20
25
30
35
40
45
50
CSD 1* CSD 2A* CSD 2B* CSD/ CP Composite
Substituted HA
Stre
ngth
(MPa
)
Compressive Strength in Wet Conditions for Selected Absorbable Ceramics
WET (1-2 hrs)
WET (24 hrs)
* Tested at 1 hr Cancellous bone (Lee, et al., CORR, 273: 177-183, 1991)
** In addition to graft composition, numerous factors affect the ultimate absorption rate of grafts in vivo including, but not limited to: Anatomic location Individual patient physiology Graft volume Graft configuration (e.g., granules vs. bolus) and porosity
Pre-op ABC
07/12/06
10/03/06
BIOCERAMIC REPLACEMENT
Calcium Sulfate/Calcium Phosphate Composite
GCT Talus Talo-navicular fusion
Calcium Sulfate

Results
PRE-CLINICAL TESTING Canine Critical-Size Axial Defect Model A critical-size axial defect model (Figure 1) developed at Rush University has been used successfully for nearly thirty years to perform pre-clinical testing of various bioceramic bone graft substitutes. In this bilateral model, a 13 X 50 mm defect is created in the canine proximal humerus and filled with the test or a control material (Figure 2) such as autologous cancellous bone graft, normal unoperated bone or predicate bioceramics. Untreated, the defects will not heal (Figure 3). The data presented here are from a study comparing a CaSO4/CaPO4 ceramic composite to CaSO4 dihydrate pellets, autologous bone graft and normal canine bone.
Figure 1. Diagram of the critical-size defect (yellow dotted line) created in the canine proximal humerus. The blue lines indicate where transverse sections are taken for histomorphometric analysis. The red box indicates the location of an 8 X 20 mm core for biomechanical compression testing.
Figure 3. Contact x-ray of a transverse section of an untreated defect after 6 weeks. Note that there is only minimal bone formation at the periphery of the defect. Histologically, the center of the untreated defects contained fibrous tissue.[1]
Figure 2. Immediate post-op radiographs of the right and left canine proximal humerus, demonstrating the placement of the composite ceramic (test) and CaSO4 pellets (control) in the 13 X 50 mm defects.
Conclusions
Histomorphometric
Biomechanical
0
5
10
15
20
25
30
35
40
45
50
13 Weeks 26 Weeks Normal Bone
Are
a Fr
actio
n of
New
Bon
e (%
)
Amount of New Bone (%)Composite CeramicCaSO4 PelletsAutograft
Composite Ceramic CaSO4 Pellets Autograft
Figure 8. The area fraction of mineralized new bone was greater in defects treated with the composite ceramic at 13 wks compared to defects treated with CaSO4 pellets, autograft or normal bone (p≤0.025).
Figure 10. The typical nature of new bone in the defects after 13 weeks. (A) Defects treated with the composite ceramic showed new bone with incorporation of the CaSO4/CaPO4 matrix (dark stained) and TCP granules (gray). (B) Defects with CaSO4 pellets and (C) autograft contained new bone without residual material. (D) Normal bone of the canine proximal humerus. (Undecalcified ground sections; stain, basic fuchsine and toluidine blue; original magnification, ×100). [2]
A B C D
13 week Composite Ceramic
13 week CaSO4 Pellets 13 week Autograft Normal Bone
Figure 11. The typical nature of bone in a defect treated with composite ceramic (A) at 26 weeks with few TCP granules (gray) and a trabecular architecture resembling normal bone (Figure 10-D). (B) Defects treated with conventional CaSO4 pellets with no pellets remaining and (C )defect treated with autograft. (Undecalcified ground sections; stain, basic fuchsine and toluidine blue; original magnification, ×100). [2]
A B C
26 week Composite Ceramic
26 week CaSO4 Pellets 26 week Autograft
Composite Ceramic • Superior to conventional CaSO4 pellets and autograft bone
More bone and increased strength at 13 weeks Normal architecture and strength at 26 weeks
• Exploits the different resorption rates of CaSO4 and CaPO4
CaSO4/CaPO4 matrix: early resorption and vascular infiltration TCP granules: scaffold for bone formation and early strength
Canine Critical-Size Axial Defect Model • Successful model to study various bone graft substitutes
• Can follow healing of defects of over time radiographically and histologically
• Allows for histomorphometric and mechanical data from same animals
0
1
2
3
4
5
6
7
8
9
13 Weeks 26 Weeks Normal Bone
Ulti
mat
e C
ompr
essi
ve S
tres
s (M
pa)
Strength of New Bone (MPa)Composite CeramicCaSO4 PelletsAutograft
Composite Ceramic CaSO4 Pellets Autograft
Figure 12. The ultimate compressive stress of the cored bone samples was greater in defects treated with the composite ceramic than in defects treated with CaSO4 pellets, autograft or normal bone at both 13 and 26 weeks (p ≤ 0.047).
0
100
200
300
400
500
600
13 Weeks 26 Weeks Normal Bone
Elas
tic M
odul
uls
(Mpa
)
Stiffness of New Bone (MPa)Composite CeramicCaSO4 PelletsAutograft
Composite Ceramic CaSO4 Pellets Autograft
Figure 13. The elastic modulus of defects treated with the composite ceramic was several fold greater (p ≤0.025) than defects treated with CaSO4 pellets after 13 and 26 wks. There was no difference in modulus between the composite ceramic-treated defects compared to normal bone at either time period.
Figure 14. Typical stress-strain curves for composite ceramic (red), CaSO4 pellets (blue) and normal bone (black) at 26 weeks.
Strain (%)
Stre
ss (M
Pa)
Ceramic composite
Normal Bone
CaSO4 Pellets
Yield
0
5
10
15
20
25
30
35
40
45
A B C D Pellets Composite Ceramic
Autograft Normal Bone
Perc
ent
Area Fraction of New Bone at 13 Weeks
CaSO4 Pellets
Figure 15. Bar graph comparing data on the area fraction of restored bone from the present study with data from previous studies of other bone graft materials using this critical-sized defect model at the 13-week evaluation time point. A-D represent data for other CaSO4-based bone graft substitutes.[2]
Area Fraction of New Bone
0
10
20
30
40
0 5 10 15 20 25 30
Weeks
Per
cent
PRO-DENSEAutograft
Area Fraction of Normal Bone
Ceramic composite
Autograft
Figure 16. Line graph of amount of new bone filling defects treated with the ceramic composite (blue line) and autograft (green line) over time (2, 3, 4, 6, 8, 13 and 26 weeks). The data are compared to the amount of bone found in a normal canine humerus (red dashed line).
Methods of Analysis 1. Serial clinical radiographs Rate of implant material resorption
and replacement with new bone
2. Stained histological sections Area fraction of new bone and
residual implant material
3. Biomechanical compression
testing Strength and stiffness of new bone
Figure 5. (A) Mechanical test specimens (yellow dashed lines) are cored from the center of each defect (black dashed lines). (B) The resultant mechanical test cylinders are 8 mm X 20 mm. (C) Unconfined, uniaxial compression tests are performed on each core (arrow) using a modified compression subpress (ASTM D695) and a servo hydraulic mechanical testing system with a 1000N Dynacell Dynamic Load Cell (Instron Corp).
A B
C
Figure 4. New bone and residual implanted materials are quantified by superimposing a point-counting grid on digital images of the central 12-mm diameter of the defect area. The data are expressed as the percent area fraction.
Test Control
Radiographic
Figure 7. Transverse section radiographs of restored defects that had been treated with the composite ceramic after 13 (A) and 26 (B) weeks and autologous bone graft after 13 weeks (C). Black circles define the area of the bone defect. D: Transverse section of an unoperated canine humerus demonstrating normal trabecular architecture.[2]
A B
C D
Post-op 2 Weeks 6 Weeks 13 Weeks 26 Weeks
Composite Ceramic
CaSO4 Pellets
Autograft
Figure 6. Serial radiographs of bone defects treated with equal volumes of composite ceramic, CaSO4 pellets or autologous bone graft. Replacement of the composite ceramic with new mineralized bone was apparent, beginning at 2 weeks and continued until 26 weeks when replacement with new bone was nearly complete. Resorption of CaSO4 pellets was essentially complete by 6 weeks.
13 wk Composite 26 wk Composite
13 wk Autograft Normal canine bone
Figure 9. Defect treated with composite ceramic at 6 weeks. The majority of the CaSO4/CaPO4 matrix had been resorbed, allowing deep infiltration of capillaries (black arrows) and venules (V). Newly formed bone lined with osteoblasts covered the surfaces of the remaining CaSO4/CaPO4 matrix (white arrows) and the TCP granules (TCP) (Undecalcified ground sections; stain, basic fuchsine and toluidine blue; original magnification, ×154).[2]
References [1] Turner TM, J Bone Joint Surg Am. 2001; [2] Urban RM, CORR 2007
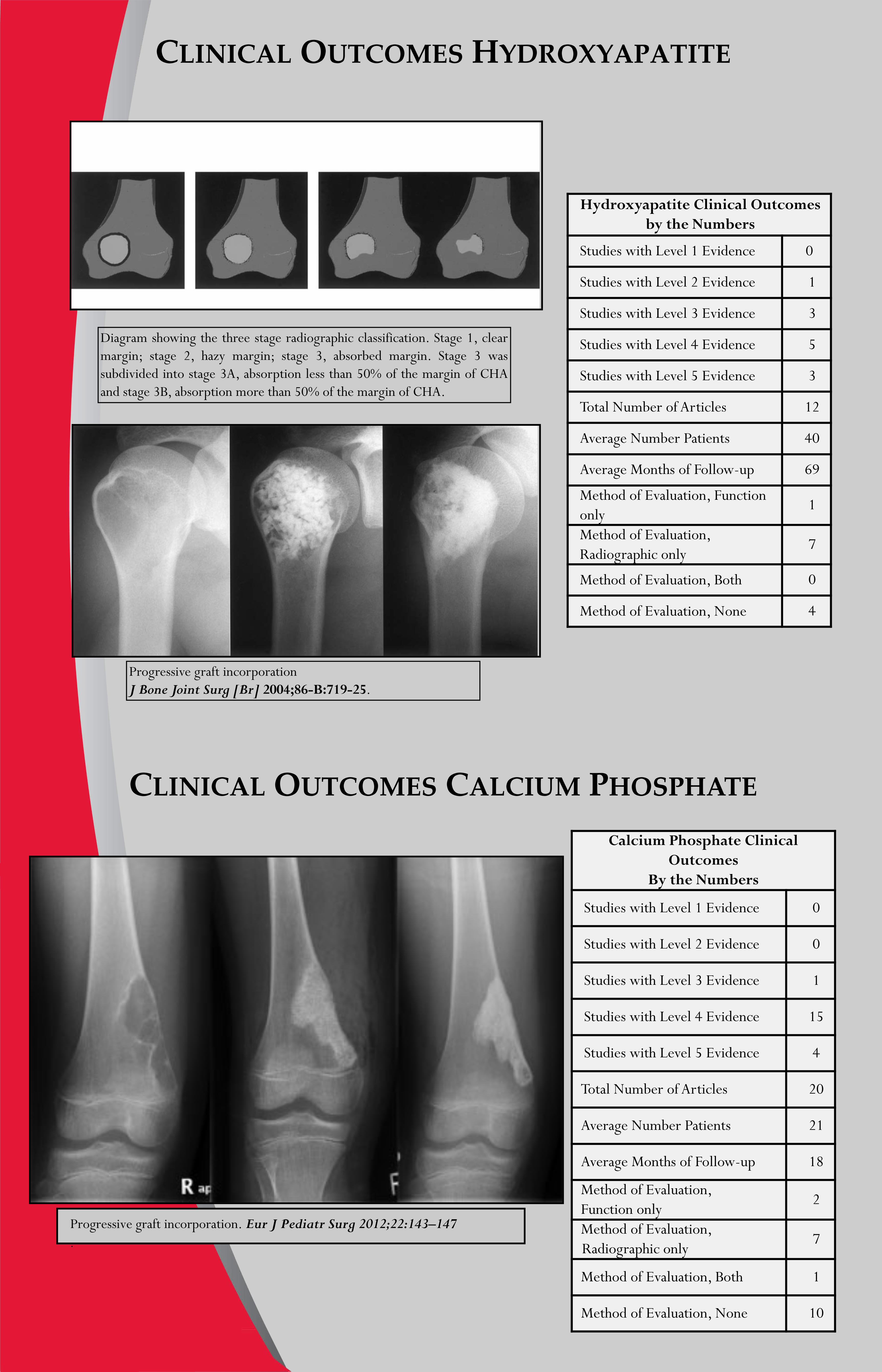
CLINICAL OUTCOMES HYDROXYAPATITE
Progressive graft incorporation. Eur J Pediatr Surg 2012;22:143–147 .
Hydroxyapatite Clinical Outcomes by the Numbers
Studies with Level 1 Evidence 0
Studies with Level 2 Evidence 1
Studies with Level 3 Evidence 3
Studies with Level 4 Evidence 5
Studies with Level 5 Evidence 3
Total Number of Articles 12
Average Number Patients 40
Average Months of Follow-up 69
Method of Evaluation, Function only
1
Method of Evaluation, Radiographic only
7
Method of Evaluation, Both 0
Method of Evaluation, None 4
Diagram showing the three stage radiographic classification. Stage 1, clear margin; stage 2, hazy margin; stage 3, absorbed margin. Stage 3 was subdivided into stage 3A, absorption less than 50% of the margin of CHA and stage 3B, absorption more than 50% of the margin of CHA.
Progressive graft incorporation J Bone Joint Surg [Br] 2004;86-B:719-25.
CLINICAL OUTCOMES CALCIUM PHOSPHATE Calcium Phosphate Clinical
Outcomes By the Numbers
Studies with Level 1 Evidence 0
Studies with Level 2 Evidence 0
Studies with Level 3 Evidence 1
Studies with Level 4 Evidence 15
Studies with Level 5 Evidence 4
Total Number of Articles 20
Average Number Patients 21
Average Months of Follow-up 18
Method of Evaluation, Function only
2
Method of Evaluation, Radiographic only
7
Method of Evaluation, Both 1
Method of Evaluation, None 10

CLINICAL OUTCOMES CALCIUM SULFATE
Calcium Sulfate Clinical Outcomes by the Numbers
Studies with Level 1 Evidence 0
Studies with Level 2 Evidence 2
Studies with Level 3 Evidence 1
Studies with Level 4 Evidence 11
Studies with Level 5 Evidence 1
Total Number of Articles 15
Average Number Patients 32
Average Months of Follow-up 28
Method of Evaluation, Function only 2
Method of Evaluation, Radiographic only
6
Method of Evaluation, Both 4
Method of Evaluation, None 3 Graft dissolution and bone healing. Clin Orthop Relat Res (2009) 467:2949–2954
CLINICAL OUTCOMES COMPOSITE GRAFT
ABC bone repair and remodeling. Clin Orthop Relat Res (2012) 470:2014–2020
Progressive graft dissolution and bone repair in Unicameral Bone Cyst Computed tomogram of composite graft revealing cyst repair
Composite Graft Clinical Outcomes by the Numbers
Studies with Level 1 Evidence 0
Studies with Level 2 Evidence 0
Studies with Level 3 Evidence 0
Studies with Level 4 Evidence 6
Studies with Level 5 Evidence 0
Total Number of Articles 6
Average Number Patients 32
Average Months of Follow-up 37
Method of Evaluation, Function only
3
Method of Evaluation, Radiographic only
1
Method of Evaluation, Both 1
Method of Evaluation, None 0

SUMMARY AND CONCLUSIONS
After reviewing the literature regarding bioceramics for benign bone tumors, most of the articles suggest that these bone graft substitutes are an acceptable alternative to autogenous bone graft. Pre-clinical animal modeling is helpful but does not eliminate the need for sound clinical studies. Animal testing, however, offers quantitative mechanical and histological data. Clinical articles, however, suffer from the same major weaknesses. The studies are generally Level III or Level IV evidence and relatively small. The measured outcomes are inconsistent. Some of the studies look at function, while others look at x-rays. Some of the studies report on the oncological outcome, most notably local recurrence. When treating benign bone tumors it is hard to conclude that a local recurrence has anything to do with the bone graft substitute. It has more to do with the biology of the bone tumor and the adequacy of excision. Radiological assessment is also inconsistent in most of these studies. Plain radiographs are used which do not accurately determine the amount of bone repair. Computed tomography would be a more accurate method. It can be difficult to determine new bone formation from residual radio-opaque bioceramic. One important question is whether it makes any difference at all. In a contained osseous defect, is it critical to form bone in the medullary space, or is it more important to thicken the cortical margin previously thinned by the tumor? The radiographs can show dissolution of the bioceramic. What we really don’t know is whether dissolution is critical for a successful outcome. Some of these materials completely dissolve while others dissolve very little over many years.
The true test of a successful outcome for grafting a benign bone tumor comes down to two clinical factors. First, has the patient recovered to full function without limitations?; and second, has the bone repair process been adequate enough to avoid fracture? These two factors are far more important than the x-ray appearance but, unfortunately, are not reported in most of the published literature. The ideal study would be a prospective randomized trial comparing bioceramic to autogenous bone graft. The patients would be assessed radiographically using computed tomography and a functional evaluation done to determine if the patients have returned to normal activity level. This study should include complications such as infection, drainage, and, most notably, fracture as adverse outcomes. Ideally, the study would be performed on a single diagnosis such as unicameral bone cyst. The tumors have to be consistently treated either open or percutaneously. The above-described study, however, would be extremely difficult to complete by a single institution. Ward noted the relative infrequency of these tumors, and it would take a great deal of time to accrue a population with ample power to answer the question regarding outcomes with bioceramics versus autogenous bone graft. Almost by necessity a multi-institutional study would have to be conducted and only one type of bioceramic utilized. Despite these shortcomings, bioceramics for contained osseous defects is a promising technique. They avoid the morbidity of autogenous bone graft and may even be applied percutaneously by injection. One added potential value is their ability to carry pharmaceuticals. In the future, combination products including a bioceramic combined with inductive proteins, mesenchymal stem cells, or pharmaceuticals may help diminish the risk of local tumor recurrence. Currently these combined products are under investigation by numerous manufacturers and laboratories, and more will become available in the future.
Author disclosures are in the Final Program
and in the AAOS Orthopaedic Disclosure program

REFERENCES AND REFERENCE ANNOTATIONS
1. AAOS, The Burden of Musculoskeletal Diseases in the
United States: Prevalence, Societal and Economic Cost. 1st
ed. 2008. 247.
2. Enneking, W.F., S.S. Spanier, and M.A. Goodman, Current
concepts review. The surgical staging of musculoskeletal
sarcoma. J Bone Joint Surg Am, 1980. 62(6): p. 1027-30.
3. Boone, D.W., Complications of iliac crest graft and bone
grafting alternatives in foot and ankle surgery. Foot Ankle
Clin, 2003. 8(1): p. 1-14.
4. Urban, R.M., et al., Increased bone formation using
calcium sulfate-calcium phosphate composite graft. Clin
Orthop Relat Res, 2007. 459: p. 110-7.
5. Urban, R.M., et al., Healing of large defects treated with
calcium sulfate pellets containing demineralized bone
matrix particles. Orthopedics, 2003. 26(5 Suppl): p. s581-5.

6. Leupold, J.A., et al., A comparison of ProOsteon, DBX,
and collagraft in a rabbit model. J Biomed Mater Res B
Appl Biomater, 2006. 79(2): p. 292-7.
7. Giannoudis, P.V., H. Dinopoulos, and E. Tsiridis, Bone
substitutes: an update. Injury, 2005. 36 Suppl 3: p. S20-7.
8. Irwin, R.B., M. Bernhard, and A. Biddinger, Coralline
hydroxyapatite as bone substitute in orthopedic oncology.
Am J Orthop, 2001. 30(7): p. 544-50.
9. Shibuya, K., et al., The medium-term results of treatment
with hydroxyapatite implants. J Biomed Mater Res B Appl
Biomater, 2005. 75(2): p. 405-13.
10. Matsumine, A., et al., Calcium hydroxyapatite ceramic
implants in bone tumour surgery. A long-term follow-up
study. J Bone Joint Surg Br, 2004. 86(5): p. 719-25.

11. Ogose, A., et al., Comparison of hydroxyapatite and beta
tricalcium phosphate as bone substitutes after excision of
bone tumors. J Biomed Mater Res B Appl Biomater, 2005.
72(1): p. 94-101.
12. Csizy, M., R.E. Buckley, and C. Fennell, Benign calcaneal
bone cyst and pathologic fracture--surgical treatment with
injectable calcium-phosphate bone cement (Norian): a case
report. Foot Ankle Int, 2001. 22(6): p. 507-10.
13. Welkerling, H., et al., Painful soft-tissue reaction to
injectable Norian SRS calcium phosphate cement after
curettage of enchondromas. J Bone Joint Surg Br, 2003.
85(2): p. 238-9.
14. Thawrani, D., et al., Successful treatment of unicameral
bone cyst by single percutaneous injection of alpha-BSM. J
Pediatr Orthop, 2009. 29(5): p. 511-7.

15. Matsumine, A., et al., Calcium phosphate cement in
musculoskeletal tumor surgery. J Surg Oncol, 2006. 93(3):
p. 212-20.
16. Yasuda, M., K. Masada, and E. Takeuchi, Treatment of
enchondroma of the hand with injectable calcium
phosphate bone cement. J Hand Surg Am, 2006. 31(1): p.
98-102.
17. Yajima, H., et al., Treatment of intraosseous ganglia and
bone cysts of the carpal bones with injectable calcium
phosphate bone cement. Hand Surg, 2008. 13(3): p. 167-73.
18. Hirata, M., et al., Use of purified beta-tricalcium phosphate
for filling defects after curettage of benign bone tumours.
Int Orthop, 2006. 30(6): p. 510-3.
19. Vigler, M., et al., Subtrochanteric femoral fractures due to
simple bone cysts in children. J Pediatr Orthop B, 2006.
15(6): p. 439-42.

20. Gitelis, S., et al., Use of a calcium sulfate-based bone graft
substitute for benign bone lesions. Orthopedics, 2001.
24(2): p. 162-6.
21. Kelly, C.M. and R.M. Wilkins, Treatment of benign bone
lesions with an injectable calcium sulfate-based bone graft
substitute. Orthopedics, 2004. 27(1 Suppl): p. s131-5.
22. Dormans, J.P., et al., Percutaneous intramedullary
decompression, curettage, and grafting with medical-grade
calcium sulfate pellets for unicameral bone cysts in
children: a new minimally invasive technique. J Pediatr
Orthop, 2005. 25(6): p. 804-11.
23. Clayer, M., Injectable form of calcium sulphate as
treatment of aneurysmal bone cysts. ANZ J Surg, 2008.
78(5): p. 366-70.

24. Mirzayan, R., et al., The use of calcium sulfate in the
treatment of benign bone lesions. A preliminary report. J
Bone Joint Surg Am, 2001. 83-A(3): p. 355-8.
25. Schindler, O.S., et al., Composite ceramic bone graft
substitute in the treatment of locally aggressive benign
bone tumours. J Orthop Surg (Hong Kong), 2008. 16(1): p.
66-74.
26. Gitelis, S., et al., Outcomes in the treatment of benign bone
lesions using an engineered bioceramic: Preclinical and
clinical results. RUSH Orthopedics Journal, 2009: p. 37-
43.