Embed Size (px)
Citation preview

Aoneand Mineral. 9 (1990) 137-152 Elsevier
BAM W269
137
Biochemical responses to sequential human parathyroid hormone (l-38) and calcitonin in
osteoporotic patients
Anthony B. Hodsman and Laurence J. Fraher
Dqorrmenr of Medicine nnd the Lawson Research Iwiture. 3. losephi Heolrh Cewe and rhr Uniwniry of Western Ontario, London. Onmio. Canada
(Received 5 September 1989)
(Accepted 19 January 19-W
Summary
Pamthyroid borm~nc (PTH) has been proposed as a skelaal activator for cyclicat pmocok of ,rea,mem for osteoporosis; among severat potential drugs that might serve to depress the subqusnt phase of as
teoclastic bone resorption, cakitonin is the most selective. Twenty patients aged 5&7S years were eb
rbiled in a stttdg of ttcIr !??rhmical rerposes dur .~ ‘mm * !U?y Wi*&x cyck with synthetic hPT?f
l-38, given as a subctttatteow injection of 4w W/day; half the patients were radmtdy aUocatai to R-
ceive a subsequent 56.day depressor cycle with cakitonin in a dare of 100 U/day, while the remainder re-
ceived no further treatment. All patients received an initial 24-h intravenous infusion of hFTH t-38 (0.5
Ullrgih) to evaluate the fTH-dependent renal synthesis of I,ZS(OH)2D. Serum calcium increated from
2.20 + 0.07 mmolll to 2.56 zt 0.16 (P < O.OOS) during FIN infusion, but was not significantly different
from baseline during intermittent treatment. Baseline concentrations of serum 1,2S(OHkD were 22.8 ?
8.2 pglml, increased to 52.2 f 25. I (P < 0.005) during infusion and remained si@catttly higher than
baseline after 14 days intermittent therapy (33.1 ? 19.4, P < 0.05). Gastrointestinal absorption of*Ca,
as represented by alpha (peak fractional absorptionih), increased from 0.397 * 0.173 to 0.552 f 0.210
(P < 0.01) during hITH 1-38 therapy and was moderately correlated with the innemem in serum
1,25(OH)$I levels (r = 0.5. P < 0.03). Daily cslcium excretion was significantly increased above hasp
lint during hFTH l-38 therapy, but there were no correlations between changes in binary czdcium, al-
pha or semm 1,25(OH)tD levels. Baseline fasting urinary excretion of OH-proline increased during
hkTH l-38 treatment from 30.5 + 13.9 moVmmol ctce*inine to 43.4 + 17.5 immediately after bfTH
l-38 infusion (P < 0.025). and mean excretion was persistxtly higher than baseline during intermittent
treatment: the increased urine calcium and OH-proline excretion are consistent with FfEi-induced aai-
vation of bone resorption. Serum alialine phosphatase and osteocakin lwets incteared signiticantly
during a W-day period of obsewuian after the hP171 L-38 cycle, which ts ccatsistem with increased os-
teoblast activity in association with coupled bone formation. In those patients subsequcatty receiving
catcitonin, biochemical changes in semm alkaline phosphatase and ostecalcin were significantly
blunted in comparison to the findings seen m those treated with hFfH l-38 alone; urine OH-pmline ex-
cretion was 25% lower at the end of cakitonin therapy, compared to the group treatedwith hFTH I-38
Correspondence to: Dr Anthony Lt. Hodsman, The Lawson Research InMute, St. Jowph’s Health
Centre, 268 Grawvcnor Street, Londail, Ontario, C.i,.da h’6.A :Vi.
0169.Mxw19o/$03.50 @11990 Elsevier Science Publishers B.V. (Biomedic21 Pivision)

138
alone. mese preliminary findings may form the basis for designing further ADFR protocols utilizing
FlTl peptides and cakitonin to treat osteapaosir.
Introduction
As our understanding of the physiological cycle of bone remodelling has pro- gressed, it is theoretically possible to exploit the separate hommnal influences gov- erning this cycle. Frost first postulated that bone cell populations might be altered sequentially in such a manner as to lead to reversal of the fundamental bone remod- elling deficit which results in progressive osteoporosis in the later decades of life [l]. This approach has been dubbed ‘ADFR’ therapy, since it requires the sequential treatment with an Activating drug to entrain new bone remodelling units, a Depres- sor drug to limit the initial phase of osteoclastic resorption, followed by a treatment- Free interval to allow unimpeded osteoblastic bone formation, before Repeating the cycie. Initial applicaiions of the ADFR concept, utilizing oral phosphate thera- py as an activator and either sodium etidronate or calcitonin as depressors, re- ported modest increases in bone mass [Z-7], but to date there is little evidence to substantiate a true activation of bone turnover. Recently synthetic amino teminal PTH fragments have been used as anabolic agents to augment trabecular bone mass both in animals [&lo] and osteoporotic patients [II-141. However, in addition to its anabolic action, PTH is probably an important physiological activator of hone remodelliog and turnover [U]. This prompted us to evaluate an ADFR protocol which combined a Zweek phase in which synthetic hPTH 1-38 therapy was used primarily as the activatmn step with a sequential 6-week period of calcitonin as the depressor step within a 3-month repeating treatment cycle. The logistics of such a treatment cycle are similar to earlier reports utilizing oral phosphate and disphos- phonate [Z-7]. We have followed biochemical indicators of the renal and skeletal responses to hPTH 1-38 during this 3 month cycle in 20 osteoporotic patients.
Since the PTH-dependent renal synthesis of 1,25(OH)P may be impaired in el- derly osteoporotic patients [16], we have specifically evaluated this response during an initial intravenous infusion of (l-38)PTH, as well as during the 2-week period of daily subcutaneous hPTH l-38 injections.
Patients and treatment protocol
Twenty patients, aged 50-78, including three men aged 45,50 and 78 and 17 wo- men aged 65.9 * 5.7 (SD) years, were enrolled into the study. The entry criteria for this study were based on a clinical diagnosis of idiopathic osteoporosis in the men and post-menopausal osteoporosis in the women.

139
All patients were referred because of symptomatic vertebr.J !r xtures and radioi- ogical evidence of osteopenia, although no patients were admitted to the study within 3 months of an acute fracture episode and none were immobilized because of continuing bone pain. Particular care was taken to exclude primary causes for 05- teoporosis in all subjects, including hyperparathymidism, hmhymidism, gluco- wrticoid excess, multiple myeloma and hypogonadism (in the men), by appm- ptiate biochemical screening. None of the female patients were receiving estrogen replacement therapy, and none of the subjects were taking calcium supplements or other therapy known to influence bone metabolism, within 6months prior to entry into the study. All patients had a tram-iliac crest bone biopsy at entry to the study which showed a low bone turnover in all cases (data not shown). Vertebral BMD, measured in all patients at the start of the study, was 0.928 f 0.036 g/d and ranged from 0.841 to 1.047 g/cm’ in the men and 0.683 to 1.120 g/d in the women. Entry criteria for this clinical study did not require confimmtion of osteopenia bv bone histological or densitometric criteria because of the relatively low diagnostic sensitivity of these variables. After signing informed consent, all patients were ini- tially admitted to a Clinical Investigation Unit during the first 4 days of the study protocol for detailed studies of the calcium-bone endocrine axis.
After baseline blood and urine collections the following treatment pmmcol was initiated: ail patients underwent an initial intravenous infusion of synthetic human parathyroid hormone 1-38 (Bissendorf Peptide, WedemarluHaunover, FRG) cm day 1. Each ampoule contained 35 fig pure hPTH l-38 peptide, equivalent to 400 IU, when assayed in a bovine renal adenylate cyctasz system against a FTH stan- dard supplied by the National Institute of Biological Standards and Control. LPTH 1-38 was dissolved in 0.9% NaCl containing 0.1% human serum albumen and in- fused at 43 q g hPTH l-38 peptide (0.5 IU equivalents)/k&h for 24 h. For an aver- age of 60 kg body wt, this amounted to a total dose of 720 IU equivalents PTH. From day 2 to day 14 all patients received a single daily subcutaneousinjection of 35 pg hPTH 1-38 (400 IU equivalents). On day 15 half the patients were randomly al- located to begin daily subcutaneous injections of salmon calcitoniu (Calcimar, Ror- er Pharmaceuticals Ltd., Horsham, PA, USA) for 6 weeks, beginning with 20 units the first week, 50 units the second week and 100 unitslday thereafter. Appropriate blood and urine samples were collected at the following time points during the
study: baseline, day 1 during hFTH l-38 infusion; days 2,7 and 14 during intermit- tent hPTH l-38 injections; days 35 and 56 (during which half the gtoup were re- ceiving daily CT injections); day 100 while off all therapy.
Methods
Fasting blood samples were collected throughout prior to hPTH 1-38 or c&it&n injections. Urine hydroxyproline (OH-Pm) was measured in fasting spot urine samples, but all other urine biochemistry was measured in 24 h collections. Serum and urine calcium (Ca), inorganic phosphate (P,), creatinine and alkaline phospha- tase (AP) were measured by standard automated methodology. Serum ionized cal-

cium (Ca*‘) was measured by ion selective electrode (Ciba Coming Diagnostics Corp., Medfield, MA, USA). Serum vitamin D metabolites, 25(OH)D and 1,25(OH),D were measured by competitive binding assays following isolation by HPLC [17]. Serum osteocalcin (OC) was measured by radioimmunoassay (Incstar Corp., Stillwater, MN, USA), with a normal range of 1.8-6.5 ng/tnl. Serum immu- noreactive parathyroid homtone (CPTH) was measured by a mid-molecule assay (Incstar Corp.), with a normal range of 35-85 pmolk Urinary hydroxyproline (OH-Pro) was measured by a wlotimetric assay [la] in fasting 2-h urine samples af- ter a 12-h overnight fast, thus avoiding the influence of exogenous dietary sources oa OH-Pro extretinn [19]. The normal range was established for 50 healthy young adults, aged i0 to 40 years, as 2.6-40.9pmoYmmol creatinine, and is expected to increase by 30% in post-menopausal women [19]. Urinary cyclic AMP (CAMP) was measured by radioimmunoassay (Immunonuclear Corp., Chicago, IL, USA) with a normal range of ~450 nmoUmmol creatinine. Dietary calcium absorption was as- sessed in the fasting state on days-l and 14 by giving 5&i of “Ca in 20 tng cold ele- mental calcium carrier, as a 100 ml solution of CaCl after Marshall and Nordin [20]. In the original method, 4SCa absorption is indicated by alpha (the fraction of the dose absorbed per hour), which represents the maximal rate of calcium absorption and appearance in the systemic circulation as calculated from a computerized curve-fitting analysis of %a measured in venous blood samples obtained CIWI 4 h after ingestion of the tracer. Normal values for alpha are reported as 0.568 f 0.3% (2 SD) in non-osteoporotic women aged 60-69 1211. In our experience alpha was very strongly correlated with the 60 min appearance of “Ca in venous blood sam- ples (r = 0.95). Since the latter is a simpler laboratory measurement, these results are also reported here, expressed as % total ingested dose per extracellular fluid volume.
Statistical methods
Data presented in the text are means f SD. Statistical comparisons within treat- ment groups were evaluated by Student’s paired t-test and adjusted for multiple comparisons by Bonferroni’s method (i.e., adjusting the significance value for an individual test for the number of tests made on that parameter within the group [22]). Where appropriate, Bartlett’s test was used to test for a normal distribution within data sets [23]. Linear regression analysis was used to test for significant for- relations. Statistical significance between groups and across time was analysed by Analysis of Variance (ANOVA) with repeated measures in BMDP-5V (?XDP Statistical Software, Inc., Los Angeles, CA, USA).
Figure 1 shows the response of serum calcium &a), ionized Ca”, inorganic phos- phate (P,), 1,25(OH),D and endogenous immunoreactive parathyroid hormone (i-

141

142
PTH) to intravenous hPTH l-38 (0.5 IU equivalents/kg/h) over 24 h; subsequent responses to intermittent S.C. hPTH l-38 (400 IU equiwlentsfday) are shown in Fig. 2.
As can be seen in Panel A, Fig. 1, serum Ca and Ca*+ were both significantly higher than baseline within 4 h, and increased progressively during hPTH 1-38 in- fusion from 2.20 + 0.07 to 2.59 + 0.16 (PC O.OOS) and from 1.23 f 0.07 to 1.51 f 0.14 (P < 0.00.5), respectively. However, fasting serum Ca levels returned to base- line values during S.C. hPTH l-38 therapy, and by day 14 serum Ca was 2.30 + 0.14 mmol/l (Fig. 2, Panel A). During the infusion serum Pi fell from a baseline of 1.16 + 0.14 mmol/l to 0.96 * 0.17 mmol/l (P < 0.005) (Fig. l), but returned to l.l& 4 0.16 mmoI/l by day 14 (Fig. 2), which was not significantly different from baseline. Se- ram concentration of 1,2S(OH),D was 22.8 + 8.2 pglml at the start of infusion and increased to 52.2 * 25.1 (P < 0.005) after 24 h (Fig. l), and was still significantly higher than baseline on day 7 (35.9 f 16.5 pg/ml, P < 0.05) and day 14 (33.1+ 19.4, P < 0.0s) of hPTH 1-38 therapy (Fii. 2). Endogenous I-PTH levels, as measured by a mid-molecule assay, fell from 56.2 f 18.3 to 39 + 15.7 pmol/I (P c 0.05), dur- ing hPTH l-38 infusion (Fig. l), but increased slightly from this nadir to 44.6 *
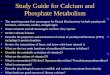
B 1 2 7 14 812 7 14 Days Days
Fig. 3. Sequential urine biochemistry during the total period of hFTH l-38 treatment; vatws arc shown at bareline (6). during 24-h PTH infusion (day 1) and during imermittent FTH treatment (days 2,7.14).
All data are means f SEM and signikant differenosa from baseline are represented by l ‘.P c 0.003,
*,Pc 0.025. The normal range for wine OH-ho acretian isgiven by the bar adjacent to the axis.

143
18.5 by day 14 of intermittent LF’TH 1-38 (Fig. Z), although thiswas still statistical- ly lower than baseline (P < 0.05).
Figure 3 shows the urinary excretion of Ca, Pi, CAMP and OH-Pro, both during hPTH 1-38 infusion (day 1) and subsequently during therapy with ~termitsent hPTH l-38. As can be seen in Panel A, urinary CAMP increased during the infu- sion from 318 k 150 to 544 + 207 nmoVmmol creatinine (P < 0.005) and remained significantly higher than baseline during intermittent hFTH l-38 therapy. Urinary excretion ofPiincreasedfrom 19.9 + 5.1 to34.4 k lOSmmoU24h(PC0.005),cor- responding to an increase in fractional Pi excretion from !S 7 4 4.2 to 26.1 f 8.1%. However, daily Pi excretion was not significantly different from baseline during in- termittent hPTH l-38 therapy. During the infusion, 24 h urine Ca was not signiti- cantly diierent from baseline (4.0 + 2.9 vs. 4.3 i 2.3 mm&day, respectively). However, there was an abrupt increase in mine Ca on day 2 to 7.9 f 4.4 mmoUday (P c 0.005 compared to baseline) and a relative calciurcsir persisied throughout the period of intermittent hPTH l-38 therapy (Fig. 3). Although the magnitttdc of the calciuria parallelled the relative changes observed in scmm 1,25(OI$D levels on days 2,7 and 14, there were no significant correlations between the increaws in serum 1,25(OH)$ over baseline and urine Ca excretion either on day 2 (I = 0.25) or day 14 (I = 0.12). As can be seen in Panel D of Fig. 3, urinary OH-Pro was not significantly different from baseline during the infwioa, but there was a sigttifkmt increase on day 2 to 43.4 f 17.5 pmoVmmo1 creatinine (P < O.Mi compared to baseline. values of 30.5 f 13.9). However, subsequent OH-Pro excretion during in- termittent MTH 1-38 therapy was not significant higher than baseline.
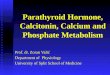
There were no correlations between gastrointestinal “Ca absorption and hase- tine 25(OH)D (I = 0.06) and 1,25(OH),D (I = 0.09) levels. As can he seen in Fig. 4, absorption of “Ca, as represented by alpha (the maximum fractional rate ofab- sorption in the first hour), increased from 0.397 f 0.173 to 0.552 f 0.210 (P -=z 0.01) between the baseline value and the second test after 14 days intermittent
G.I. 45Ca. Absorption
Pre- Post-PTH
Fig. 4. Changes in ga@rointestinal calcium abwrptian pre- and post-WTH I-38 therapy m day 14. Al- pha (solid bars) represents the peak rracttoaal sbwrptiaa of cat&n per how; the [email protected] sormal n~san v&c and the 1 SD range is shown adjacent fotheaxis (after Bullamorestal. [2lj). Akosbovmare changes in the 60 min venm~~ “Ca levels (open bars) expressed BS 96 dosz absorbed pet ECF. Dam arc
means f SEM. **.P<O.Ol.

144
6 12 714 35 56 100
hPTH l-38 treatment. Expressed as “Ca in the 60 min venous sample, Ca absorp don increased from 24.1 f 9.6 to 29.7 zk 8.7% per ECF (P 4 0.01). There was a moderately significant correlation between the increment in serum 1,25(OH)$ levels and the increment in alpha bchveen baseline and day 14 (I = 0.5, P < 0.03).
On day 1.5 the 20 patients were randomly allocated to two groups, one of which
received no farther therapy, and one beginning daily S.C. calcitonin injections for 42 days. Figures 5 and 6 show the group comparisons in urinary Ca and OH-Pro excre- tion between the patients receiving q o further treatment and those receiving calci- tonin therapy. It can be seen that urine Ca excretion returned to baseline values af- ter discontinuing hPTH 1-38 therapy by day 35 and remained so thereafter (Fig. SA). After analysis of variance, there was no difference in urinary Ca excretion in the group receiving calcitonin, although the decreased levels observed on day 56 approached significance (P = 0.07) (Fig. 5B). Thus, by the end of the ‘depressor’ phase (day 56) the urine calcium excretion was 4.04 f 2.19 mmoI/day in the group receiving hPTH l-38 alone and 3.02 f 1.76 in the group who had received PTH fol- lowed by calcitonin. Mean urinary OH-Pro excretion was not significantly higher than baseline at any time point other than day 2 of hPTH l-38 therapy (Fig. 6A); similarly, OH-Pro excretion was not significantly lower during calcitonin therapy

145
(Fig. 6B). However, by the end of the depressor phase (day 56), tine OH-Pro ex- cretion was 25% lower in the group receiving calcitonin as wmpared to the group treated with hFTH l-38 alone (25.3 f 9.6 vs. 33.7 f 12.5 ~ol/mmol creatinine, KS.).
Changes in serum alkaline phosphatase and osteocalcin are shown in Fig. 7. Within the group of patients receiving hPTH l-38 therapy alone serum alkaline phosphatase increased from 105 It: 24 IUil to 119 + 34 (P c 0.02) at the end of FTH therapy on day 14, reached a peak of 131 f 39 (P < 0.005) by day 35 and was still significantly (P < 0.01) elevated at the end of the observation period on day 100. Ia an analysis of variance between groups the patients subsequently receiving calcito- nht experienced significantly (P c 0.05) smaller overall increases in alkaline phos- phetase. The increase within thii group was only significantly (P < 0.05) higher
than baseline on day 35. Serum osteocalcht levels increased significantly within the group of patients treated with PTH alone from a baseline of 2.34 + 1.38 to a maxi- mum of 4.03 * 1.94 @ml on day 100 (P c 0.05). As can be seen from Fig. 7, the changes in serum osteocalcin in the group receiving calcitoain were similar, with values increasing from a baseline of 1.97 .t 1.1 to a maximum of 2.M + 1.1 @ml on day 56 (P C 0.05). Although there was a significant change in sermn osteocalcin levels across time by analysis of variance between groups, there were no overall group differences or interactions.

146
Parathyroid hormone is a strong candidate for the role of a remodelling activator in ADFR strategies. In the pathological state of 1” hyperparathyroidism bone remod- elling activity, together with the appearance rate of new remodelling units, is great- ly increased over normal [24-261. There is good reason to believe that PTH is a nat- ural modulator in bone, regulating the birthrate of remodelling units under normal conditions [15]. This fact underscored earlier attempts at ADFR therapy in which inorganic phosphate was used as an activator by way of its ability to induce endoge- nous 2” hypetparathyroidism [2,3,7]. Thus, the availability of synthetic PTH for clinical trials makes possible the design of ADFR protocols incorporating a direct activator of bone remodelling. We chose to use hPTH l-38 in this study because it has been reported to show increased potency over hPTH 1-34 in clinical studies 127). although Zanelli et al. could not confirm this in several in viva and in vitro as- says [28]. A Zweek period of activation utilising 408 IU equivalents of hPTH l-38 per day was selected, based on the work of Hesch et at. [29], who showed significant increases in urinary hydroxyproline excretion without encountering significant

short-term hypercalcemia with such a regimen. Comparable doses of WTH l-34
have been utilized by several grcilps in longer-term studies in which the anabolic ef- fects of continuous hPTH l-34 have been explored as a treatment for osteoporosis [12,13,30]. Calcitonin was selected as a depressor because of its specific action on osteoclast function; the treatment duration of 48 days approximates the resorption phase of bone remodelling seen in post-menopausal women [25,31].
The responses of the bone-endocrine axis to PTH during later decades in life are controversial. The majority of post-menopausal women with osteoporosis have low rates of bone remodelling, including a reduced level of osteocktstic resorption. However, a number of studies suggest that circulating i-PTH levels increase with age, even when the age-related decline in renal function is taken into aewunt [32,33]. Since there is no bone histological evidence for increased PIT-I actitity, this might imply a relative resistance of the skeleton to PTH with aghtg. Similarly, pe- vious studies have found relatively reduced levels of circulating 1,25(OH)p in OS- teoporotic patients, compared to controls [16,34-361 and a blunted response to exogenous hPTH l-34 infusion (16,361. These findings might imply an age-related renal resistance to PTH. Thus, the design of ADF’R protocols utilizing PTH as an activator must take into account a dose that is at least sufficient to overcome rel- ative tissue insensitivity to the hormone throughout the period of therapy.
In this report, the total and ion&d serum Ca rose throughout the 24-h period of hPTH 1-38 infusion, during which time a total of 600-800 IU equivalents were given. As expected, there was a concomitant increase in fractional phosphate ex- cretion and a rise in urinary cyclic AMP excretion. The very low basal 1,25(OH)&l levels seen in our patients are very comparable to those reported in other osteopo rotic patients [35,36]. However, the average increment in 1,25(OH),D ievels dur-
ing hPTH l-38 infusian was 29.4 pdml, more. than twice the baseline. This is corn-- parable to changes reported in normal elderly subjects without osteoporosisby Tsai et al. and discordant with the osteoporotic patients of Tsai et al. [%] and Sltik et al. [16], in whom there was a blunted or absent response to hPTH l-34. The rea sons for the discrepancies between the current study and the two previous reports are unclear; all three have followed a similar protocol with respect to FIT-f dose and duration of infusion. However, our finding of a significant ?,2.5(C@l)aD response to hPTH 1-38 in osteoporotic patients has been reported by others using bolus intra- venous doses of hPTH l-34 [34,35]; moreover, we found that serum lzS(OH)fl levels remained significantly higher than baseline after 14 days intermittent hFTH 1-38 therapy, even though the daily dose was only 400 IU equivalents/day. On bat- ante the degree to which the renal response to PTH is ‘blunted’ in osteoporotic pa- tients may be more apparent than real and, at least in this study, a daily dose of 400 IU equivalents was sufficient to overcome any partial resistance. Since we cannot report on a parallel group of non-osteoporotic controls, the role of impaired renal responsiveness to FTH in the pathophysiology of osteoporosis remains to be de- fined.
Not all of the biochemical changes observed during hPTH l-38 infusion were present during intermittent S.E. injections. Thus, fasting serum calcium and phos- phate levels returned to baseline values, as did the fractional urinary excretion of

148
Pr This may not be surprising, since the biological half-life of tbe peptide at the tis- sue level is probably much shorter than 24 h; indeed, its half-life disappearance from the circulation is less than 5 min [37]. However, significantly increased urinary CAMP excretion persisted throughout the period of intermittent therapy. There was also a significant calciuresis, most marked immediately after hPTH l-38 infu- sion, but present throughout the PTH tredltment period. It is also of interest that there was a small, but sign!ficant, su,7presGon of endogenous i-PTH at the end of the period of exogenous hPTH l-38 therapy. Since there was no detectable in- crease in serum calcium by this point (at least in the fasting state), it is possible that the increased circulating concentrations of 1,2~5(OH)~ were responsible for this endogenous PTH suppression.
The increased urinary calcium and hydroxyproiine excretion might have re- flected increased bone resorption; Hesch et al. reported a modest hydroxyprolinu- ria using the same hPTH l-38 fragment, dose and activation period [ZS] as evi- dence for an increased bone turnover foIlowing PTH therapy. On the other hand, Slovik et al. were only able to detect an increase in hydroxyproline excretion in one of three patients reveiving 750 IU equivalents hPTH l-34 by daily S.C. injection, and no increases were found in the three patients receiving 450 IU equivalents/day [38]. If the fasting urinary OH-proline:creatirtioe index is taken as a measure of bone resorption, then the sequential measurements made from days 1-56 in this study would indicate only a small, and statistically insignificant, increase through- out the whole activation (Fig. 3) and depressor (Fig. 6) phases of the cycle.
After 2 weeks of intermittent hPTH l-38 treatment, serum l,ZS(OH),D levels were still increased by 10.4 pg/ml (45%) over baseline, to levels usually seen in middle-aged, non-osteroporotic adults [34,35]. Although the baseline values are much lower, this increment in serum 1,25(OH)sD is similar to that observed after giving exogenous l,Z(OH),D to healthy young adults [39,40], in whom a large in- crease in urine excretion is seen due to increased dietary calcium absorption. In this report gastrointestinal “Ca absorption also increased significantly, as measured by alpha, the fractional dose absorption per hour and correlated with the increment in serum l,ZS(OH),D levels. This index of calcium absorption has been found to cor- relate well (r = 0.76) with net calcium absorption measured by classical dietary bal- ance techniques [rll]. Slovik et al. Aso reported increased calcium absorption in os- teroporotic subjects treated with intermittent hPTH l-34 [36]. Thus, it would ap- pear that the modest calciuric response to hPTH 1-38 reported in this study might, in part, be explained by the increased circulating levels of l,Z(OH),D leading to increased absorption of dietary calcium. There were, however, no correlations be- tween urine calcium and 45Ca absorption. Since formal calcium balance studies were not performed, there is no way to distinguish between the relative contribu- tions of bone resorption and dietary calcium absorption towards the calciuric re- sponse.
There was a significant increase in serum alkaline phosphatase observed after completion of the 2-week period of intermittent hPTH 1-38 treatment. This was most marked in the patients receiving PTH alone, and persisted until day 100. In the subgroup of patients randomly allocated to receive calcitonin during the depres-

149
sor phase, this effect was significantly blunted (Fig. 7). Increases in serum alkaline phosphatae have previously been observed with prolonged intermittent F’l’H treatment, {both hPTH l-34 and hPTH l-38) ir. which the anabolic action of the peptide has been utilized to increase trabecular bone mass in greyhound dogs, ovariectomircd rats and in osteoporotic patients (8,11,12,14~. However, this is the first report in which prolonged changes in alkaline phosphatase oceurwd after a short course of intermittent hlTH 1-34 therapy, in which the dreg was primarily used as an activation agent. In the patients receiving calcitonin therapy, the @tern
pret this difference, shtce the baseline levels were significantly different between the two groups, despite randomization of the patients at the start of the protocol. The increases in alkaline phosphatase reported here for the group receiving hPTH l-38 alone are comparable to those recently published by Heszh et al., although there are important differences between the design of the two studies [14]. Hescb et al. treated eight osteoporotic patients with four cycles of hFTH t-38 and caIcitonin over 14 months. Within each 105 day cycle, all patients received ItPTH l-38 (720 IU equivalents/day) for the first 70 days, and intermittent caicitonin (200 U/&y, in- irattasally) over three 14day intervals within the cycle [14]; seruttt aIk&ne phos- phatase levels increased to 155 IUil by the end of the first cycle and continued to rise with successive ~cycles. The attenuation of the alkaline phosphatase response in the current report within the group receiving sequential treatment with hF’TH 1-38 and calcitonin contrasts with the findings of Hesch et al. Although the differences between the cycle designs in the two studies make it impossible to spectdate about the nature of the alkaline phosphatase response, they serve to emphaaise how IIttIe is currently known about skeletal responses to ADFR protocols. As can be seen in Fig. 7, there was also a trend for serum osteocalcin levels to Increase after hP’TH 1-38 therapy, with significant increments over baseline seen between 56 and 100 days. Taken together, the delayed increases in aikaline phosphatase and osteocal- tin levels suggest the possibility that coupled bone formation foiIowed a period of F’CH-induced skeletal activation.
Other sequential changes in serum and urine biochemistry induced by calcitonin during the depressor phase of the cycle were not impressive. There were no signi& cant differences in serum calcium or phosphate between the calcitonin-treated group and the patients who had received hFTH l-38 aione. As can be seen in Figs. S and 6, the mean urinary calcium and hydroxyproline excretion was lower during calcitonin treatment, but these results were not significantly different at any time point during the depressor phase when compared to the patients not receiving c&i- tonin. However, the sample sire available in this study had only a limited power to detect significant differences between the two groups. Thus, baseline urine OH- proiiie excretion was identical in the two groups; however, at the end of the deprea- sor phase the mean value for the group receiving both hFTH l-38 and calcitonin was reduced by 25% compared to the group not receiving calcitonin. Conventional power analysis indicated that significant differences between the two groups might only have been detected had this reduction exceded 45%. Even so, we believe that the tninimal biochemical changes seen during calcitonin treatment may be the re-

150
sult of an insufficient activation phase with hPTH I-38, either too small a dose, too short a treatment period or both. Thus, Reeve et al., using very short treatment cycles (hPTH l-34, 1 week and calcitriol, 3 weeks), found no evidence of skeletal activation [42]. On the other hand, Hesch et al., using more prolonged cycle times with hPTH 1-38 (70 days), together with concurrent calcitonin, recently reported striking improvements in vertebral bone mass [14]; unfortunateiy the latter report contained no details of urinary calcium or OH-proline excretion.
In summary, intermittent daily injections of hPTH l-38 have been used over a 2- week cycle, followed by 6 weeks of calcitooin as part of the development of an ADFR treatment protocol for osteoporosis. The biochemical responses included a sustained increase in serum 1,2S(OH),D levels during the period of hPTH 1-38 treatment, and increases in dietary “Ca absorption, without significant changes in serum calcium. A modest, but sustained, increase in urinary calcium excretion was seen which may, in part, have reflected increased dietary calcium absorption or al- ternatively increased bone resorption since a brief increment in fasting urinary by- droxyproiine was also seen. The latter would be a reflection of activated bone tum- over. However, the subsequent biochemical changes observed during calcitonitt treatment were insignificant, suggesting that the activation stbntths was, at best, weak. Nonetheless, hPTH 1-38 treatment resulted in sustained increases in serum alkaline phosphatase and osteocalcin which are consistent with coupled bone for- mation, as has been observed in other treatment protocols utihzbtg PTH as an ana- bolic agent in osteoporotic patients [11,12,14]. We conclude that the utilization of PTH in the development of ADFR protocols is feasible, but that future experience might benefit from choosing both a larger dose and longer activation period.
The authors wish to thank MS L. Froste, RN, and MS F. O’Brien, RN, for their in- valuable assistance in patient education and supervision of the protocol and Mrs A. Cavattey for her expert laboratory assistance. Without their help it would not have been possible to carry out this study. The authors also wish to thank MS B. Keys for her help with the preparation of the manuscript. L.J.F. is a National Institute of Nu- trition scholar and A.B.H. is an Ontario Ministry of Health Career Scientist. This study was supported in part by the Ontario Ministry of Health, Canada and the Na- tional Institute of Nutrition. Canada.
1 Frost HM. Coherence treatmenlofastwporosis. OnhopClin N Am 1981:t2:649-669. 2 Rasmwen H, Bordier P. Marie P, Auquier L. Eisinger JB, Kuntz D, et al. Effect of combined ther-
spy with phosphate and cakitonin cm bone volume in osteopomsis. Metab Bone Dis Rel l&s 1980;2:107-111.
3 Anderson C, Cape RDT, Chilly RG, Hodwaan AB, Wolfe BMJ. Preliminary observations af a form of coherence therapy for osteoporosis. CalcifTissue Int 1984,36:341-343.

151
4 Woodson GC. Coherence therapy with phosphate and etidronatc for orteopaosis: preliminaq re- subs. In: Christianwt C. Johansen IS. Riis 81, edr. Osteopair 1987. Viborg. Denmarlt: Norhaven A/S, 19*7:11**-1189.
5 Millet PD. Neal BJ. Mclntvre DO. Yanover MJ. Kowalski L. The effect of coherence fADFRI tber- apy with phosphate and e&Jronate on axial bone mineral density ir. post ~‘&Q&Ni,. In: Christiansen C, Johansen JS, Riis BJ. CL. Ostcoporosir 1987. Vib-xg, DenmarL: Norhaven AIS, 1987:8ed-885.
6 Mallette LE, LeBlanc AD. Cyclic therapy of ortcoporti we of a brief, hi&dose pulse ofetidro- “ate as a terminator of ~~teoclast activity. In: ChristianJen C, Johacsen IS, m BJ. eds. Osleopme- sir 1987. Viborg, Denmark Norhaven AIS, 1987$&l-946.
7 Hodmum AB. Effects of cyclical therapy of osteoporosis using an oral regimee of iaorganie pbw phate and sodium etidronate: a clinical and bone histomorphomctrlc study. Bane M&ml 1989:5:201-212.
8 Podbesek RD. Stevenson R, Zxtelli GD, Edouard C, Meuniet PJ, Reeve 1, et al. Treatment with human pamthyroid hormone fragmmt (bFl’H l-34) stimulates bone fonaatlott and intestinal caki-
urn absotption in the greyhound: compatiron with data from the ortcopormb trial. In: Cohn DV. Talmage RV. Matthews JL, edo. Homxmal control of calcium metabolism. Proceeding of the ti venth International Conference on Calcium Regulating Hormones. New York: Excerpta Media. 1981;118-123.
9 Tan: CS, Heersche JNM, Murray TM, Parsons JA. Parathytoid hotmaze stlmnlstes the bate appo- sitian rate independently of its rewrptive action; differential &cc@ of intent&em and mailrmms administration. Endocrinology 1982;110:506-512.
IO Hori M. Uzaw T. Morita L, Noda T, Takahssbi H, Isaee J. Effect of human paratbyrokl bnmocK (PTH(l-34)) on experimental osteopettla of rats induced by ovaieetomy. Bae Mineral 1988:3:193-199.
11 Reeve J. Hesp R. Williams D. Hulme P. Klenc- L, Zanelli JM, et al. Aeabolie ef6cn of Imr doses af a fragment of human paratbyroid hormone on the skeleton in ~usatostwPormi3. Lancet 1976d:lO35-1038.
12 Reeve J, Meunier PJ, Parsms JA. Anabolic effect of human pamthymid fragment on trabcmdar bate in involutional mteoporasisz a multicentre trial. Br Med J 1980;$0:1340-f34.4.
I3 SlovikDM. RosenthalDI. Dowelt S. PottsJTJr. Daly MA. Campbell JA.dal. Ratomtionofs~& nal bate ii osteoporotic men-iy tre&ent with h&an parethyroid hornme (l-34) and 1,2& hydtoxyvitamin D. J Bone Mitt Res 1986;1:377-381.
14 Hescb R-D, Busch U,PmkopM, Dellittg G, Rittit~ghattse E-F. Incteaseofvettebraldensitybyc.x~
bination therapy with pulsatilc l-38bPTI-l and sequential addition of caleitottin naal spray ie as.
teopuroticpatients. CtifTirsueInt 1989:44376-180.
15 Partitt AM. The actions of parethyroid hormone on bate: relation to bate remodeling and tumover. calcium homeostasis. and metabolic butte discase. Part 2 of 4 parts. PTH and boas &k&me turn-- over and plasma calcium regulalion. Metabolism 1976Zi:%9-955.
!6 Slovik DM, AdamsJS, Neet RM, Hotick MF, PottsJT. Deficient prodwtion of 1,2Qlibydmxyvita- min D in elderly ostec~ptotic patiettts. N Engl J Med 1981;MS:372-374.
I7 Fraher I.J. Adami S. Clemens TL, JonerG, OXiotdan JL. Radioimmutma%a~ of l~xlibvdmmi-
tattdn 4: &dies on’the metabolism of vitamin Dz in man. CIia Ettdcaiool198&9:151-I&. _
18 Clcary J. Saunders RA. A simplified ptofedure for the ~.teasurement of total bydmxypr&ne in urine. Clin Chim Acta 197437:217-W.
19 Hodgkimora. A, Thompson T. Measurement of the fasting winary bydmxypmliw cmatbdw ratio in notmal adults and its variation with age and sex. J Clin Path01 1982P5:807-811.
20 Mat&all DH, Notdin BEC. Kinetic analysis of plasma radioacti”ity after oral ingcstioo ofradiocaki- am,. Nature 1%9$22:797.
21 B,d,amore JR,GaUagber JC, Wilkitwn R,NardinBEC,Marsb~DH.Effcaof~egeon~~~* sorption. LatKa 1970@535-537.
22 Sncdecar GW, Cochran WG. The binomial distribution. In: Statistical analysis (7th Edn.), Iowc Tbe Iowa State University Pterr, 1980;116.
23 Snedewr GW, Cochran WG. The random effects tttadel. In: Statistical analysis (7tb Edn.). Iowa:

152
Tbe IowaState University Press. 1980;116. 24 Charboo SA, Edooard CM, Arlot MF, Flewtier PJ. Effects of parathyroid hormone on remodelling
of iliac trabecolar bone packets in patients with priotaty hypxparathyroidirm. Clin Orthop Rel Res 1982$62:255-263.
25 Eriksen EF. Nonoel and pathological remodelhog of human trabecular bone: three dimensional re- coostroctioo of the remodcllina xooence in normal and in metabolic bone disease. Endoctinol Rev _ 19%7:379-408.
26 Etiksen EF. Mosekilde L, Melsen F. Trabeculta bone remodeling and balance in primary hypetpa- thymidirm. Bone 1986:7:213-221.
27 Hesch RD. Heck 1, AuFmkolk 8. Fin, clinical obsetvations with hFTH (l-38). a more potent ho- man pantymid hormone peptide. Harm Metab Res 1984:16:559-560.
28 Z&Iii JM, Auk’mkolk B, Lane E, Ball C. The biological activity of the syotbetic l-38 sequence of human pamthyroid hormone in in viva and in vitro bioassay systems. In: Cohn DV. Manin TJ, Mew nier PI. eds. Calcium regulation and bone metabolism. Basic and clinical aspects. Amsterdato: Ex-
cetpta Media, 1987;9:561. 29 Hesch RD, Heck J, Schettler T. Human panthyroid hormone for coherence therapy of o~eopo~e-
sis. Acta Endocrino11985:108:171-172.
30 Reeve J, Treeear GW. Pamms JA. Preliminary trial of low doses of human parathvroid hommne I-34peptideintteatmentofosteoporosi.x Clin &tdocdool1976:21:469-477. _
31 Reeker RR, Kimmel DB, Partilt AM, Davies KM, Keshawaa N, Hinders 5. Static and tetraevcline- based bone histomorphomettic data from 34 normal postmenopausal females. J Bane h&t Res 1988:3:133-144.
32 Forem MS, Klein RF, Nissenson RA. Nelson K. Heath H, Amaod CD, et al. Effect of age on circu- tatiog immoooreactive and bioactive parsthyroid hormone levels in wmen. J Bone Min Res 1987;2:363-365.
33 Young G, Marcus R. Minkoff JR, Kim LY, Sogre GV. Age-related rise in pamthyroid hormone in man: the use of intact and midmolecule antisera to distinguish hormone scmtioo from retention. J Bone Mio Res 1987;2:%7-374.
34 Riggs L, Hamstra A, DeLoca HF. Assessment of%hydmryvitamin D-l alpha-hydmxylase reserve in postmenopausal osteoporosis by administration of pamthyroid extract. J CJio Ettdnctinol Metab 1981;53:833-815.
35 Soreosen OH, Lumholtz B, Lund B, Hjelmstrand IL, Mosekilde L, Melsen F. et al. Acute effects of parothymid hormone on vitamin D metabolism in patients with the bone loss of aging. J Clitt Endo-
crinol Metab 1982;54:1258-1261.
36 Tsai Keh-Sung. Heath H, Kumar R, Riggs BL. Impaired vitamin D metabolism with aging in WD
men: possible role in pathogenesisof senile osteoporosis. J Clin Invest 19&1,73:1668-1672. 37 Kent GN. Loveridge. N, Reeve I, Zanelli J. Phatmamkinetirs of synthetic human parethyroid bor-
mone l-34 in man measured by cytochcmical bioassay sod radioimmuooassay. Cfio Sci 1985:9:171-177.
38 Slovik DM. Neer RM, Potts JT. Short-term effects of synthetic human parathymid hormone-(l-34) administration on bone mineral metabolism in osteopmotic patients. J Clip Invest
1981;68:i261-1271.
39 Adams ND, Gray RW, Lemaoo J, Cheoog HS. Bffects of calcitriol administrationan calcium metab- olism in healthy men. Kidney for 1982:21:40-97.
40 Smothers RL. Levine BS, Singer FR, Bryce GF, Melton JP, Miller ON. Relationship between uri- naq calcium and calcium intake during calcitriol adntistmtion. Kidney fnt 1986;29:578-583.
41 Marshall DH, Nordin BEC. A comparison of radioactive calcium absorption tests with oet calciom absorption Clin Sci 1981;61:477-481.
42 Reeve J, Arlot M, Price TE, Edouard C, Heap R, Huime P, et al. Periodic MU~SCS of human l-34 pamthyroid peptide alternating with calcittial paradoxically reduce bone remodelliog in spinal os- teoparosis. EurJ Clin lnvest 1987;17:421-428,