Embed Size (px)
Citation preview

Biology 350:MicrobialDiversity
A Few Words About AntimicrobialTherapy…
Lecture #368 December 2008
-1-

Did you have a nice weekend?
-2-My family and I did….

Handouts and Announcements•Outline of lecture plus questions.•Short essay on bacteriophages in nature.•Blog entry on the “parvome” andantibiotics.•Wednesday: short last lecture plus courseevaluations.•Review session: Thursday 1 PM, in the“regular” classroom (not here in lab).•E-mails up until noon on Sunday?•Final exam on Monday at 8 AM!
-3-

16s rRNA censuses!•Thursday section: barnacle tissue!•Lots of interesting marine bacteria:Xanthobacter, Lewinella, Sulfitobacter,Arcobacter, Lysobacter, cyanobacteria…even asupposedly obligate thiotrophic symbiont!•Sulfur rich environment, filter feeding.•Friday section: kefir grain!•11/16 isolates were Lactobacilluskefiranfaciens or very similar strains.•Plus two Shigella/E. coli, and 3Chromobacterium violaceum isolates.•“Transients,” non pathogenic strains, etc.
-4-
Today’s lecture agenda•Two final examples of pathogenicmechanisms (mysterious) of bacteria.•History of antimicrobial therapy.•Basic concepts in antimicrobial therapy(with some old friends from lab).•The Central Dogma and antibiotics.•Mutations to antibiotic resistance.•Promiscuous HGT and antibiotic resistance.•Two late breaking topics: phage therapyand the actual function of antibiotics.
-5-

So first…
Let’s finish up discussingbacterial diseases and their
strategies…
-6-

•Clostridium botulinum andClostridium tetani.•Tetanus/tetany. Excessive nervesignaling.•Flaccid paralysis. Inhibition ofnerve signaling.•Tetanospasmin versus botulinumtoxins.•Structure of the toxins are very,very similar (40% identical).Analogue of A-B toxin system.•Both toxins encoded byprophages!•Benefit to the pathogens??!!•Commercial use for botulinum:Botox!
Neurotoxins as a virulence factor?…
-7-
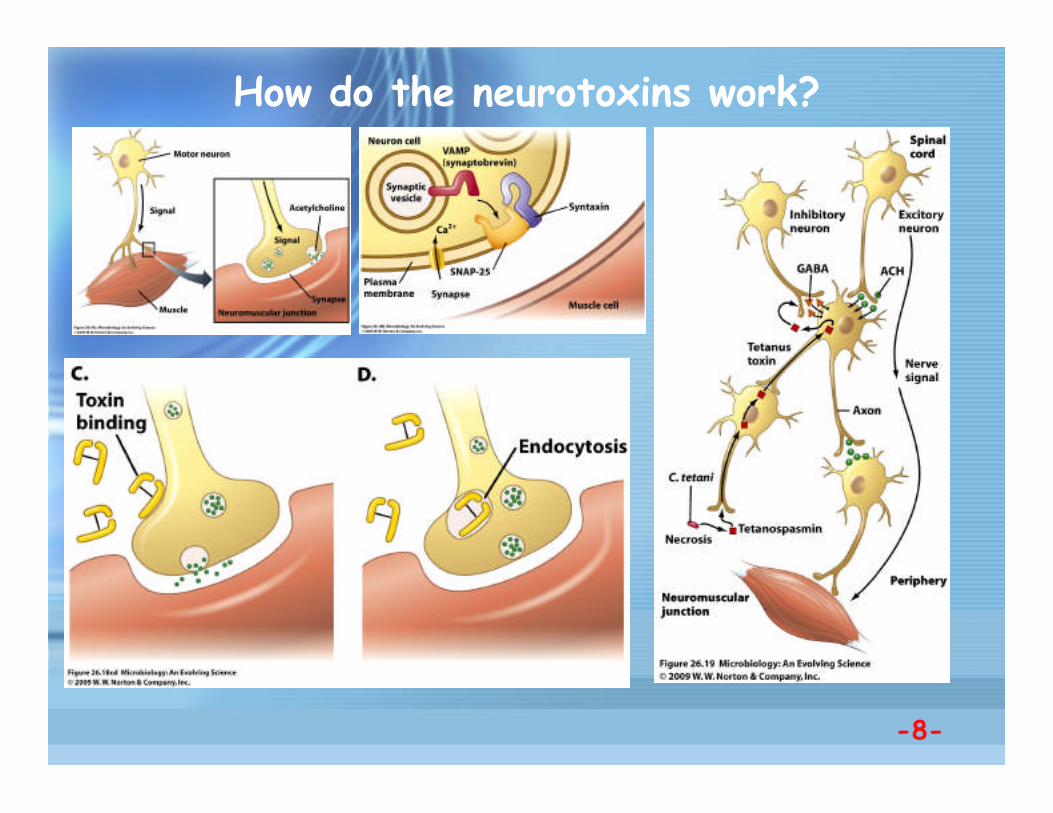
How do the neurotoxins work?
-8-
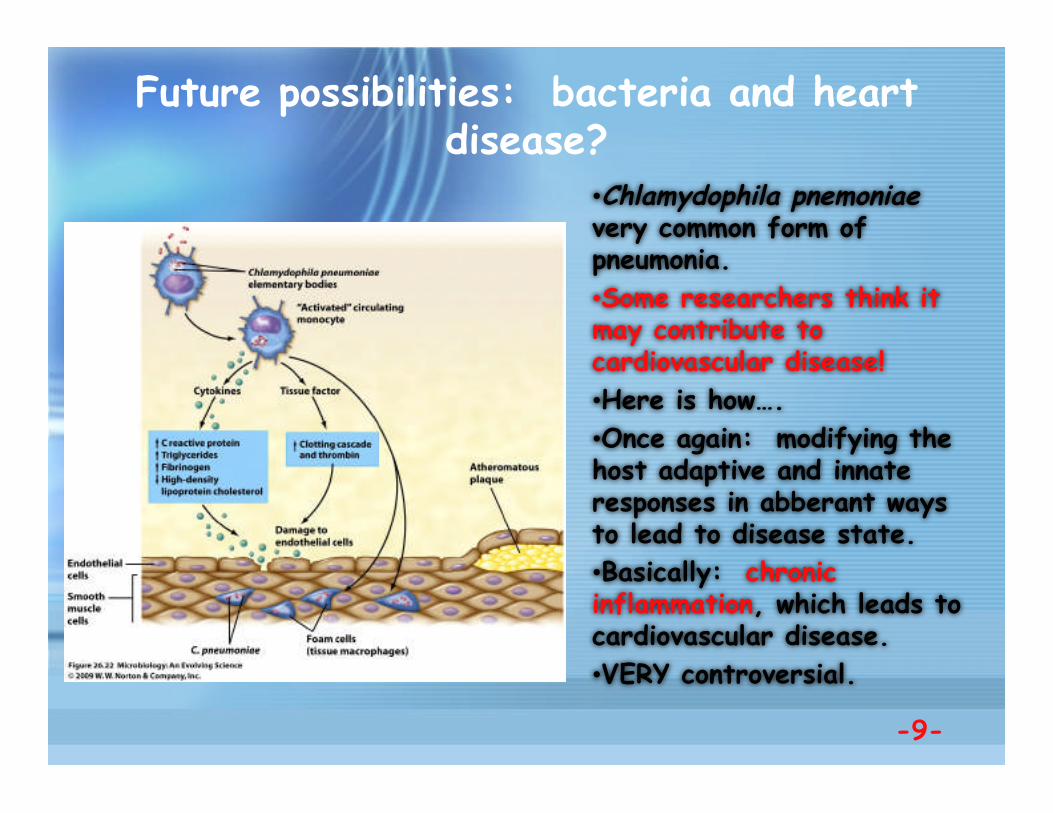
•Chlamydophila pnemoniaevery common form ofpneumonia.•Some researchers think itmay contribute tocardiovascular disease!•Here is how….•Once again: modifying thehost adaptive and innateresponses in abberant waysto lead to disease state.•Basically: chronicinflammation, which leads tocardiovascular disease.•VERY controversial.
Future possibilities: bacteria and heartdisease?
-9-

And now…
Let’s move onto antimicrobialtherapies…
-10-

Basic thoughts about antimicrobial therapy•The challenge: killing a pathogen without killingthe host.•Similarities and differences between the two arethus crucial.•An “arms race” between host and pathogenquickly develops.•Don’t forget differences between bacteriostatic,bacteriocidal, disinfection, antisepsis.•We have learned a great deal about the basicbiology of microbes (and host cells) due to thisarea of study!
-11-

Paul Ehrlich: Father of Antimicrobial therapy
-12-
•Paul Ehrlich andsyphilis.•Syphilis caused byTreponema pallidum.•Spirochaete motilityreminder?•Ehrlich, syphilis, andstaining.•Salvarsan (#606) thefirst specific treatmentfor syphilis that was notVERY dangerous for thepatient.•“Prodrug” idea.•The first rational useof chemotherapy.

More history of antimicrobial research•Fleming and penicillin.•Florey and Chain made it practical!•Domagk and Prontosil (sulfanilamide drugs)---difference between in vivo and in vitrostudies. Metabolic inhibitor (sulfa looks likePABA, so folate is not made, and thus nonucleic acids).•Waksman and streptomycin: the beginning ofthe antibiotic commercialization period(microbiological safaris).•Limits today!
-13-

•Some simple techniquesYOU have learned in thelab!•MIC analysis---can youdescribe how to set up andanalyze?•Kirby-Bauer analysis.Ditto the earlier question.
Simple tools of the trade…
-14-

Antibiotics interfere with “Central Dogma”phenomena and other characteristics of bacteria
•DNA replication,RNA synthesis,protein synthesis.
•Cell wall synthesis.
•Membrane integrity.
•Focus oncharacteristics NOTfound in eukaryoticcells like us.
•Specific forbacteria!
-15-

Some antibiotics “broader spectrum” than others
•Some antibiotics only inhibit one type of bacterium.
•Others are widely useful against a number of pathogens.
•Depends on mode of action of the antibiotic!
•Also effectiveness in vivo, in tissues, etc.
•But a Golden Age of Antibiotics seemed to dawn… -16-

Then something unpleasant happened….
•Call it the “Dead Hand ofDarwin.”
•Bacteria started becomeresistant to antibiotics.
•Not a surprise, really. Aresistant bacterium wouldbe successful in thepresence of that antibiotic.
•Resistance caused bymutation?
-17-

Antibiotic resistance can happen quickly!
•Undetectable to30% of isolates inhospitals resistantin only 20 years!
•This is a recentexample, but thisphenomenon startedimmediately afterpenicillin wasintroduced in the1940s.
-18-
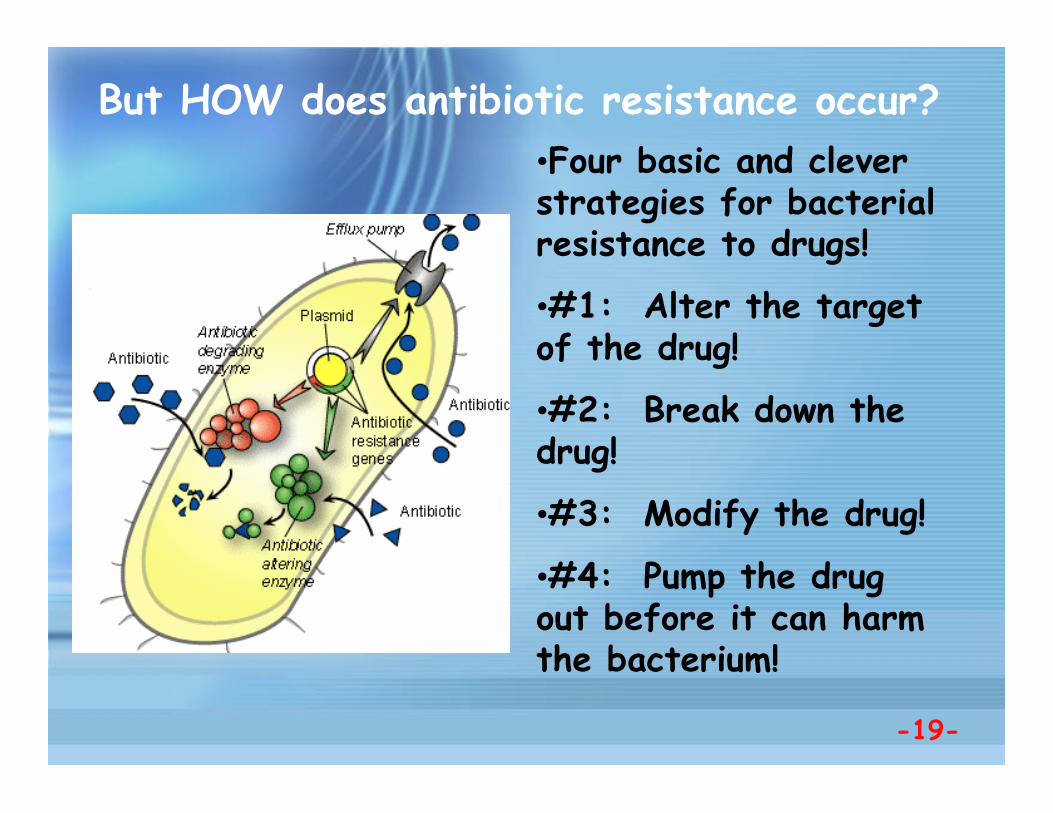
But HOW does antibiotic resistance occur?•Four basic and cleverstrategies for bacterialresistance to drugs!
•#1: Alter the targetof the drug!
•#2: Break down thedrug!
•#3: Modify the drug!
•#4: Pump the drugout before it can harmthe bacterium!
-19-
The real problem emerges…•Antibiotic resistant pathogens wereexpected. The solution? Use >1 type ofantibiotic!
•Chances of simultaneous resistance to twoantibiotics VERY low: 10-9 x 10-9 - 10-18!
•Except, starting in the 1960s, multiplyresistant pathogens began to appear…MROs.
•Pathogens appeared that were resistant tofour or five drugs simultaneously!
•What was going on??!!-20-

Rampant bacterialpromiscuity was the culprit!
•It turns out that bacteriawere swapping genes not onlywith related bacteria, but evenunrelated bacteria!
•Puts Hollywood to shame!
•Like you sharing genes withyour Caesar salad, folks!
•Pathogens were “collecting”drug resistance genes frommany sources!
-21-

At least three mechanisms ofgene transfer were involved
•Pathogens taking up“naked DNA” from otherbacteria:transformation.
•Pathogens having“bacterial sex” withother bacteria viaplasmids: conjugation.
•Pathogens being infectedby viruses carrying genesfrom other bacteria:transduction.
-22-
So now you know…we have anemerging and serious problem!
•Antibiotics don’tchange, butbacteria can!
•Many millions ineconomic costs.
•We misuseantibiotics andmake it easier!
•Agricultural misusea MAJOR problem!
-23-
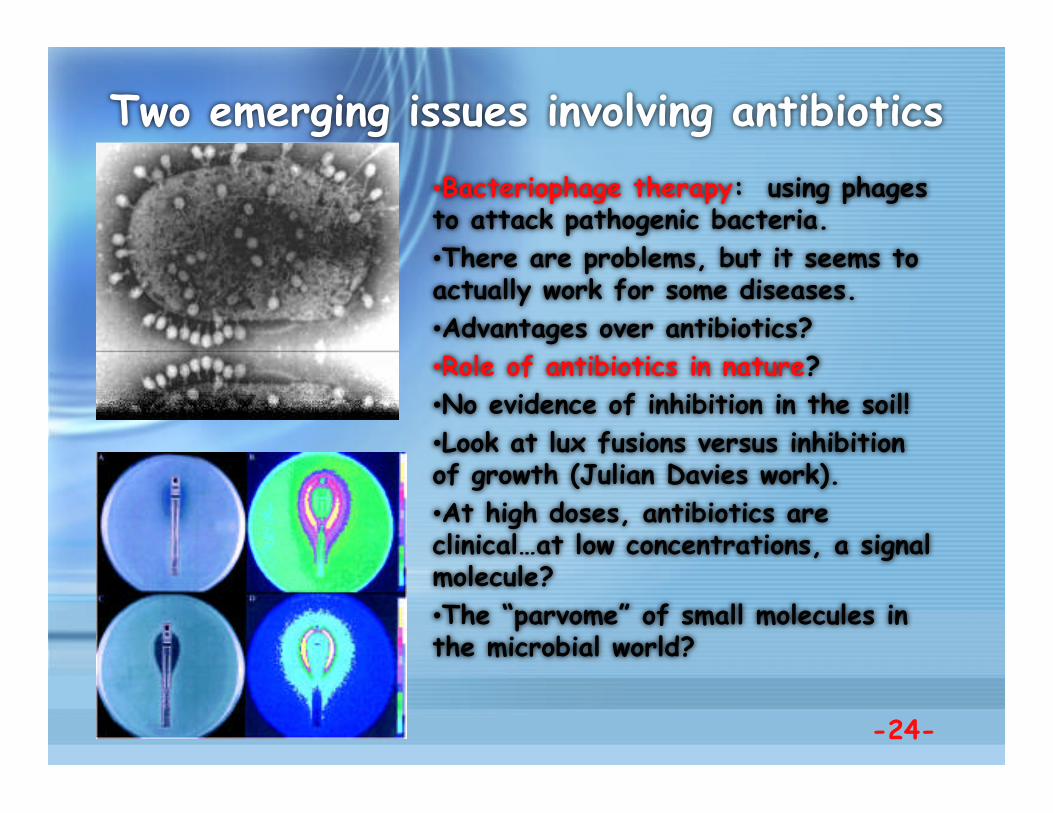
Two emerging issues involving antibiotics•Bacteriophage therapy: using phagesto attack pathogenic bacteria.•There are problems, but it seems toactually work for some diseases.•Advantages over antibiotics?•Role of antibiotics in nature?•No evidence of inhibition in the soil!•Look at lux fusions versus inhibitionof growth (Julian Davies work).•At high doses, antibiotics areclinical…at low concentrations, a signalmolecule?•The “parvome” of small molecules inthe microbial world?
-24-
Summary of today’s lecture•It is not always simple to see the benefit of a virulence factoras an advantage to the pathogen!•Antibiotics are based upon the metabolism of the bacterium,and have taught us a great deal about them…and about hostcells.•Bacteria become resistant to antibiotics via at least fourdifferent pathways.•Bacteria exchange drug resistance genes by severalmechanisms, creating MROs of great clinical importance.•Our habits with antibiotics make the spread of MROs possible.•Phage therapy may be a useful tool in our disease-fightingarsenal.•Antibiotics may have VERY different effects at lowconcentrations, and thus serve a different function in naturethan in the clinic!
-25-

Next time:
A short overview of the course!
-26-
No reading (well, plenty ofreading, actually)---we are
cruising toward the Final Exam…





























