Embed Size (px)
Citation preview

This Review is part of a thematic series on the Biology of Cardiac Arrhythmias, which includes the following articles:
Antiarrhythmic Drug Target Choices and Screening
Inherited Arrhythmogenic Diseases: The Complexity Beyond Monogenic Disorders
Genomics in Sudden Cardiac Death
Regulation of Ion Channel Expression
Biology of Cardiac Arrhythmias: Ion Channel Protein Trafficking
Computational Insights: Chaos and Wave Theory
Gene Therapy and Cell Therapy of Cardiac Arrhythmias Eduardo Marban and Gordon Tomaselli, Editors
This series is in honor of Harry A. Fozzard, 8th Editor of Circulation Research.
Biology of Cardiac ArrhythmiasIon Channel Protein Trafficking
Brian P. Delisle,* Blake D. Anson,* Sridharan Rajamani, Craig T. January
Abstract—The mechanisms underlying normal and abnormal cardiac rhythms are complex and incompletely understood.Through the study of uncommon inheritable arrhythmia syndromes, including the long QT and Brugada syndromes, newinsights are emerging. At the cellular and tissue levels, we now recognize that ion channel current is the sum ofbiophysical (gating, permeation), biochemical (phosphorylation, etc), and biogenic (biosynthesis, processing, traffick-ing, and degradation) properties. This review focuses on how heart cells process ion channel proteins and how thisprotein trafficking may be altered in some cardiac arrhythmia diseases. In this review, we honor Dr Harry A. Fozzard,a modern pioneer in cardiac arrhythmias, cell biology, and molecular electrophysiology. As a scientist and physician,his writings and mentorship have served to foster a generation of investigators who continue to bring this complex fieldtoward greater scientific understanding and impact on humankind. (Circ Res. 2004;94:1418-1428.)
Key Words: arrhythmia � ion channels � protein trafficking � cell biology
It is well understood that cardiac arrhythmias are a commonand sometimes lethal manifestation of many acquired and
inherited diseases affecting the cardiovascular system. Elec-trophysiologists have long sought to understand and treat thearrhythmogenic mechanisms of these diseases to sustain lifeand improve its quality. Beginning in 1949 with the firstreports of cardiac action potential recordings,1,2 includingnormal3,4 and diseased5 human heart, extraordinary progresshas been achieved in understanding mechanisms of normaland abnormal cell electrophysiology and heart rhythm gen-eration. The reductionist approach has resulted in the identi-fication of multiple families of ionic currents, their associated
channel and transporter proteins, and the genes encoding theirmultiple subunit structures. Similarly, evolution of knowl-edge about the complex cellular processes that modulate ionchannel function, govern cell-to-cell communication, andgenerate different mechanisms of arrhythmias have added toour understanding of normal and abnormal electrophysiolog-ical properties. From these findings emerged the concept thatabnormalities in surface membrane ion channel function arecentral to arrhythmogenesis. More recent observations thatmutated ion channels identified in patients and studied inexperimental models undergo altered expression or are incor-rectly processed within cells have broadened our view of the
Original received January 20, 2004; resubmission received March 15, 2004; revised resubmission received April 1, 2004; accepted April 2, 2004.From the Section of Cardiovascular Medicine, Departments of Medicine and Physiology, University of Wisconsin-Madison.*Both authors contributed equally to this study.Correspondence to Dr Craig T. January, Room H6/354 Box 3248, Section of Cardiovascular Medicine, CSC, 600 Highland Ave, Madison, WI 53792.
E-mail [email protected]© 2004 American Heart Association, Inc.
Circulation Research is available at http://www.circresaha.org DOI: 10.1161/01.RES.0000128561.28701.ea
1418
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

potential mechanisms underlying changes in ion channelcurrents. Thus, it is now recognized that the macroscopiccurrent in heart and other excitable tissues is the sum of 2processes: (1) biophysical (gating, ion permeation) and bio-chemical (phosphorylation, etc) modulation of surface mem-brane ion channels and (2) biogenic modulation (biosynthe-sis, processing, trafficking, and degradation) of channelprotein. Incorrect processing of mutant proteins within cells,in fact, has become an increasingly important mechanismcausing many diseases, and the potential for correctingdefective protein processing offers novel therapeuticapproaches.
Protein Processing in CellsThe 1972 Nobel Prize for Chemistry was awarded to DrChristian Anfinsen for work suggesting that the primaryamino acid sequence of a protein is sufficient for properfolding in vitro.6 Since that time, it has become apparent thatprotein biogenesis in vivo is more complex, requiring addi-tional proteins that assist with peptide processing and traf-ficking, energy input, posttranslational modification, proteinquality control, and degradation. These processes are outlinedin Table 1. It is important to recognize that the bulk of ourinformation has been derived from lower organisms andexpression studies in heterologous systems.
Transcription and TranslationRegulating the expression of ion channels at the cell surfacebegins at the level of gene transcription and mRNA stability.Genomic DNA contains binding sites for transcriptionalproteins and their regulatory elements (transcriptional activa-tors and repressors). During transcription, RNA polymerasesgenerate long strands of heteronuclear RNA that contain anuntranslated 5� region, multiple exons (amino acid encodingRNA sequences) and introns (noncoding RNA sequences ofincompletely understood function) interspersed among theexons, and an untranslated 3� region. Removal of the intronicsequences (splicing) occurs in the nucleus, creating mRNAconsisting of exons to define the coding region as well as 5�and 3� noncoding regions that promote mRNA translation andstability. Normal mRNA splicing can vary for a single geneproduct, thereby generating multiple transcripts with differentcoding regions and/or differing translation efficiencies. Sim-ilarly, pathogenic nucleotide substitutions, deletions, andinsertions can affect mRNA synthesis and stability, thereby
altering the amount of mRNA available for subsequentpeptide generation.
Messenger RNA is exported from the nucleus to thecytoplasm where ribosomal proteins translate coding regionsinto polypeptide chains. Ribosomal translation begins withthe codon AUG, which encodes the amino acid methionine.This “start” codon is usually preceded by a 6-nucleotideconsensus motif (GCCACC, the Kozak sequence).7 In eu-karyotic cells, translocation of the nascent polypeptide fromthe ribosome into the endoplasmic reticulum (ER) is thoughtto occur cotranslationally and is initiated when specific signalsequences (amino acid motifs) in the elongating polypeptidebind a cytosolic signal recognition particle that then targetsthe complex to receptors within the ER membrane. Forcytosolic proteins, the targeting signal sequence is almostinvariably found within the amino terminal. Ion channels,however, have the added complexity of possessing severaltransmembrane spanning domains. Consequently, these pro-teins contain numerous signal sequences to direct ER (andultimately plasma) membrane crossings that determine thecytoplasmic and extracellular domains, and these signalingsequences are not restricted to the amino terminal. Forexample, in voltage-gated K� channels (Kv1.3), as well as incystic fibrosis transmembrane conductance regulator (CFTR)Cl� channels, the first ER targeting translocation signalsequence is contained within the second transmembranespanning domain, nearly 200 amino acids downstream fromthe amino terminal. Additional transmembrane domains alsointeract with the ER membrane to initiate and terminatetranslocation to allow for complex transmembrane proteinspanning structures.8 Although unknown, the mechanismsdriving translocation of cardiac ion channels are presumed tobe similar.
Posttranslational Modification of ProteinsAs a peptide is inserted into the ER, it is almost immediatelybound by protein chaperones (so termed because they mon-itor immature proteins) that are proposed to facilitate matu-ration and the formation of proper tertiary structure requiredfor protein function. Many chaperone proteins are ATPasesand may have other enzymatic activities as well.9,10 Mostnewly synthesized proteins rapidly undergo core-glycosylation, the site-specific (an amino acid motif usuallycontaining an asparagine) addition and trimming of mannose-rich sugar moieties, which may assist in subsequent proteinfolding, maturation, and stability.11–13
Ion channels exist as large protein complexes with acentrally located pore that allows for ion flow across mem-branes. For most Na� and Ca2� channels, the � (pore-forming) subunit is synthesized as a monomeric proteinderived from a single gene product that has 4 repeatingdomains of similar structure. For K� channels, however, the� subunit is a multimeric protein formed by the coassemblyof multiple peptides either from the same or from relatedgenes. Most voltage-gated cardiac K� channels (Kv) areassumed to require the coassembly of 4 subunit peptides toform a tetrameric protein channel structure. For at least someK� channels, assembly involves the formation of dimers,which then dimerize again to form the tetrameric channel
TABLE 1. Posttranslational Processing of Proteins
A protein, once synthesized on a ribosome, has several outcomes:
● It must fold into a proper tertiary structure● It may assemble with other proteins (similar or not) to form a larger
mature molecule (eg, K� channel oligomerization, accessory subunitaddition, etc)
● It may be cleaved into one or more smaller mature protein molecules(eg, Ca2� channel �2-� subunits)
● It may be transported (traffic) to another intracellular location(s) andbe sorted for delivery to its final destination
● It may be targeted at any stage for degradation (eg, ubiquitin-proteosomes, lysosomes)
Delisle et al Ion Channel Protein Trafficking 1419
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

structure.14 This occurs within the ER membrane15 and ismediated by amino terminal T1 (first tetramerization) do-mains.16 Not all K� channels have T1 domains and additionalpeptide recognition domains within the transmembrane andC-terminal regions have been identified.17 Although yet to befound, mutations within such recognition domains may alteroligomerization and contribute to cardiac ion channel dis-eases. Furthermore, most ion channels have accessory sub-units that serve multiple regulatory roles. Thus, not only mustthe � subunit proteins interact and assume a proper3-dimensional structure but also the accessory subunit pro-teins must assemble correctly to form multimeric macromo-lecular complexes, and for most proteins this is thought tooccur in the ER.18,19
After folding and assembly, the protein is transported outof the ER through vesicle budding where it travels alongcytoskeletal elements to the ER–Golgi intermediate complex(ERGIC).20 Work on KATP ion channels has shown that properprotein folding and assembly results in the masking, orunmasking, of ER retention and export signal sequences, thusproviding a mechanism governing export from the ER.21
From the ERGIC, the peptide travels through the Golgicomplex where residues core-glycosylated in the ER undergofurther processing (“complex glycosylation”). The extent ofglycosylation varies as sugar moieties are added and trimmedrepeatedly during maturation.11 On reaching the trans-Golgi,proteins are sorted based on specific sequences and ear-marked for their final destination, be it other intracellularcompartments, the plasma membrane, or extracellular space.
Quality Control and Protein DegradationA protein must attain a correct tertiary or native structure tofunction properly. Cells have evolved a complex set ofquality-control monitoring processes that prevent many non-native or misfolded proteins from reaching their intendeddestinations by tagging such proteins as abnormal and target-ing them for premature degradation. These quality-controlmechanisms, however, remain poorly understood. In mam-malian cells, the majority of the quality control is thought tooccur in the ER.22
Protein degradation is essential for homeostasis becauseeverything a cell synthesizes must ultimately be degraded,secreted, or shed; accumulation of metabolic products usuallyis lethal to a cell. The principal pathways for degradationdepend on the type of protein (membrane, cytosolic, etc) andthe reason for degradation. Once identified by quality-controlmechanisms, most misfolded proteins are retrotranslocatedout of the ER to undergo ATP-dependent ubiquination, whichis followed by degradation within proteasomes.23,24 Proteinsand other cellular components can also be degraded throughautophagic destruction by lysosomes.25,26
Ion Channels in Human Heart DiseaseCardiac action potentials reflect changes in membrane con-ductance governed by dozens of different ion channels andelectrogenic exchangers. Inherited long QT syndrome(LQTS) was recognized 40 years ago as 2 distinct clinicalphenotypes, the Romano-Ward and the Jervell and Lange-Nielsen syndromes.27–29 Elucidating the causes of LQTS has
been central to progress in identifying several human ionchannel genes and in understanding genetic and molecularmechanisms of cardiac ion channel diseases. The manifesta-tions of LQTS arise from polygenic causes, with 7 forms ofinherited LQTS described to date (LQT1–7; Table 2). Thephenotypes are often attributed to “loss of function” or “gainof function” mutations in the affected ion channels. LQT1, 2,5, and 6 are thought to prolong the plateau of cardiac actionpotentials by reducing K� channel currents (loss of function)activated during depolarization. LQT1 and 5 are character-ized by mutations in KCNQ1 (KvLQT1) and KCNE1 (MinK),which encode the � and � subunits, respectively, for theslowly activating delayed rectifier K� current (IKs). LQT2 and6 are characterized by mutations in KCNH2 (human-ethera-go-go-related gene; HERG) and KCNE2 (MiRP1), whichencode the � and putative � subunits, respectively, for therapidly activating delayed rectifier K� current (IKr). LQT7 iscaused by mutations in KCNJ2 (Kir2.1), which reduces theinward rectifier K� channel current (IK1) to slow the return ofthe membrane to the resting potential. LQT4 was recentlyassociated with abnormalities in ankyrin-B protein, whichpromotes the formation of macromolecular signaling com-plexes to reduce repolarizing current. In contrast, LQT3arises from mutations in hNaV1.5 (SCN5a), which encodesthe cardiac Na� channel. These cause failure of normalinactivation to increase late Na� current (gain of function)and prolong action potentials. More than 200 mutations in thegenes encoding for LQT1–7 are known, with LQT1 and 2patients accounting for most of LQTS. Additional congenitalarrhythmia syndromes continue to be described, and these aresummarized in Table 2. Unlike LQTS, some of these involvegain of function mutations in K� channels (short QT syn-drome) and loss of function mutations in Na� channels(Brugada syndrome, cardiac conduction disease, etc).
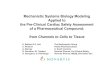
The functional effects of gene mutations are often studiedby expressing appropriately engineered cDNA in heterolo-gous systems. For ion channels, the cellular or macroscopiccurrent (I) is the product of the number of functional channelsin the cell surface membrane (N), the probability that thechannel is open (Po), and the single channel conductance (i).This paradigm is illustrated in Figure 1 for HERG current(IHERG). Changes in Po and i can be detected by measuringmacroscopic and/or single channel currents, whereas under-standing changes in N requires a multifaceted approach ofbiochemical, molecular, immunocytochemical, and electro-physiological techniques.
Protein Trafficking: Lessons From LQT2Nearly 100 LQT2-linked mutations have been identified inHERG channels. The majority of mutations are single nucle-otide changes causing single amino acid substitutions in thechannel protein (missense mutations). Only a small numberof these mutations have been expressed and functionallycharacterized, with the consistent finding that LQT2 muta-tions cause reduced IHERG. A somewhat surprising finding wasthat this occurs by several different cellular mechanisms, asillustrated in Figure 1.30–32 (1) Reduced N arises frommutations that generate a trafficking-defective protein withthe immature channel retained in the ER. A reduced N can
1420 Circulation Research June 11, 2004
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

also arise from nonsense mutations that cause codon deletionsor frame shifts to generate a truncated protein, and recentevidence also suggests that some mutations reduce N bydecreasing gene transcription efficiency.33 (2) Altered Po canarise through mutations affecting a channel’s gating andkinetic properties. (3) Altered i can arise through mutationsaffecting channel permeability/selectivity (typically pore mu-tations). (4) In channels that form as multimeric proteins (ie,
K� channels), dominant-negative interactions between coas-sembled mutant and wild-type (WT) channel subunits canpotentially affect N, Po, or i. Furthermore, a mutation canreduce IHERG by combinations of these cellularmechanisms.32,34–38
Protein trafficking defects reduce the delivery of channelsto the cell surface membrane and have emerged as a commonLQT2 disease mechanism. These mutations are not restricted
TABLE 2. Cardiac Ion Channel Diseases
Disease Current Chromosome Defective Gene Key Reference
Long QT: Romano-Ward (LQT1–6) and AndersenSyndrome (LQT-7)
LQT1 IKs, 2 amplitude 11p15.5 KvLQT1 (KCNQ1) Wang, et al, 199696
LQT2 IKr, 2 amplitude 7q35–36 HERG (KCNH2) Curran et al, 199564
LQT3 INa, 1 late current 3p21–24 SCN5a (hNaV1.5) Wang et al, 199597
LQT4 altered cell Ca2� 4q25–27 ANKB Schott et al, 199598
Mohler et al, 200399
LQT5 IKs, 2 amplitude 21q22.1–22.2 MinK (KCNE1) Splawski et al, 1997100
LQT6 IKr, 1 deactivation 21q22.1–22.2 MiRP1 (KCNE2) Abbott et al, 1999101
LQT7 IK1, 2 amplitude 17q23 Kir2.1 (KCNJ2) Tristani-Firouzi et al, 2002102
Long QT: Jervell and Lange-Nielsen
JLN1 IKs, 2 amplitude 11p15.5 KvLQT1 (KCNQ1) Neyroud et al, 1997103
JLN2 IKs, 2 amplitude 21q22.1–22.2 MinK (KCNE1) Schultze-Bahr et al, 1997104
Sudden infant death syndrome (LQTS in neonates)
IKs, 2 amplitude 11p15.5 KVLQT1 (KCNQ1) Schwartz et al, 2000105
INa, 1 late current 3p21–24 SCN5a (hNaV1.5) Ackerman et al, 2001106
IKr, 2 amplitude 7q35–36 HERG (KCNH2) Lupoglazoff et al, 2004107
Brugada syndrome
BS1 INa, 2 amplitude 3p21–24 SCN5a (hNaV1.5) Chen et al, 1998108
BS2 ? 3p22–25 ? Weiss et al, 2002109
Idiopathic ventricular fibrillation
IVF INa, 2 amplitude 3p21–24 SCN5a (hNaV1.5) Akai et al, 2000110
Catecholaminergic (Biventricular) ventriculartachycardia
CPVT1 1 cell Ca2� 1q42–43 hRyR2 Priori et al, 2001111
Laitinen et al, 2001112
CPVT2 1 cell Ca2� 1p13–21 CASQ2 Postma et al, 2002113
Cardiac conduction disease
CCD INa, 2 amplitude 3p21–24 SCN5a (hNaV1.5) Schott et al, 1999114
Sick sinus syndrome
INa, 2 amplitude 3p21–24 SCN5a (hNaV1.5) Benson et al, 2003115
If, 2 cAMPresponse
15q24–25 HCN4 Schulze-Bahr et al, 2003116
Atrial fibrillation
IKs, 1 amplitude 11p15.5 KvLQT1 (KCNQ1) Chen et al, 2003117
? 10q22–24 ? Brugada et al, 1997118
? 6q14–16 ? Ellinor et al, 2003119
Short QT syndrome
SQT1 IKr, 1 amplitude 7q35–36 HERG (KCNH2) Brugada et al, 200365
SQT2 IKs, 1 amplitude 11p15.5 KvLQT1 (KCNQ1) Bellocq et al, 2004120
Delisle et al Ion Channel Protein Trafficking 1421
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

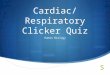
to a single region of the HERG channel (Figure 2); rather,trafficking-defective mutations have been found in severalregions of the protein, including the N-terminus (T65P,threonine to proline at amino acid position 65), transmem-brane regions (N470D, A561V), pore region (G601S,Y611H, V612L, T613M, L615V), and the C-terminus(R752W, N861I) including the cyclic nucleotide-bindingdomain (F805C, V822M, R823W).32,35–37,39–43 These muta-tions can be distinguished from WT and normally traffickingmutant channels because they are minimally present in thecell membrane. Electrophysiologically, there is little or nodetectable current, and on Western blot analysis, immature(135-kD) core-glycosylated protein is present, but the mature(155-kD) complexly glycosylated protein is absent, as dis-cussed. Using immunocytochemistry, several investigatorshave shown directly that trafficking-defective LQT2 channelprotein (for the T65P, A561V, G601S, Y611H, R752W,
V822M, N861I mutations) is located predominantly intracel-lular with a perinuclear pattern,32,35–37,42,44,45 and 2 mutations(T65P and Y611H) have been shown directly to colocalizewith resident ER proteins.32,37 These data suggest thattrafficking-defective mutant channels are retained in the ERas core-glycosylated protein.
LQT2 mutant subunits differ in their ability to coassemblewith WT channel subunit proteins.34 Coexpression of thetrafficking-defective N470D, A561V, V612L, T613M, andL615M mutations with WT protein results in a variablereduction of IHERG because of a dominant-negative effect ofthe mutant.34,40,46 Ficker et al showed that A561V coas-sembled with WT subunits, trapping most of the HERGprotein in the ER.35 In contrast, the trafficking-defectiveLQT2 mutants G601S and R752W did not cause dominant-negative suppression of IHERG.36,39 Thus, at least sometrafficking-defective LQT2 mutant subunits have dominant-
Figure 1. Macroscopic IHERG depends onthe number of functional channelsinserted in the plasma membrane (N), theopen probability of the channel (Po), andits unitary conductance (i). WT channelprotein is transcribed in the nucleus,synthesized in the ER, exported to theGolgi apparatus, and inserts into theplasma membrane. LQT2 channels mayreduce IHERG by altering gating properties(�Po), altering unitary conductance (�i),by reducing the number of channelsinserted into the plasma membrane(2N), or by combinations of theseeffects.
Figure 2. Trafficking-defective LQT2 muta-tions in the HERG channel. A schematiccartoon representing a single HERG chan-nel �-subunit shows the structuraldomains including 6 transmembrane heli-ces (S1–S6). The cylinders represent puta-tive � helices. The outer pore regionbetween the S5–S6 helices contains com-plex glycosylation (N) and selectivity filter(G-F-G) sites. The C-terminus contains acyclic nucleotide-binding domain (black)and a putative ER retention signal (R-G-R)that can regulate the surface expression ofHERG channel protein. Reportedtrafficking-defective LQT2 mutations(amino acids identified in red) occurthroughout much of the HERG channelprotein.
1422 Circulation Research June 11, 2004
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

negative interactions that suppress the surface expression ofWT subunits. Because little is known about channel multi-merization in myocytes, care must be taken in translatingthese in vitro findings.
HERG Maturation Through theSecretory PathwayAfter synthesis and core-glycosylation in the ER, HERGprotein is exported to the Golgi apparatus for complexglycosylation, sorting, and eventual insertion into the surfacemembrane. As with most large proteins, molecular chaper-ones are assumed to promote the proper folding of newlysynthesized protein and facilitate degradation of misfoldedprotein. Ficker et al identified 2 cytosolic molecular chaper-one proteins, heat conjugate/stress-activated protein 70(Hc/sp 70) and heat shock protein 90 (Hsp 90), that immu-noprecipitated with the core-glycosylated, immature HERGprotein.47 The Hc/sp 70 family of proteins binds to thehydrophobic regions of newly synthesized proteins in thecytosol to stabilize intermediate steps in protein folding. Hsp90 proteins prevent the aggregation of misfolded proteins invitro, but whether it is involved in the normal folding ofproteins remains unclear.9 Inhibition of Hsp 90 with gelde-namycin prevented the maturation of WT HERG channels,reduced the surface expression of IHERG, and promoted theubiquination of the channel protein. These data suggest thatHc/sp 70 and Hsp 90 proteins associate with the cytosolicdomains of immature HERG proteins in the ER membraneand that Hsp 90 promotes HERG channel maturation.
ER resident proteins may avoid forward transport throughthe secretory pathway because they contain amino acidsequences in the lumen (eg, K-D-E-L) or cytosol (K-K-X-Xand R-X-R) that result in their retrograde transport back to theER. Similar sequences have been identified in ion channelproteins, and they are thought to cause the retention ofimproperly assembled/folded channel protein in the ER.48
Once the protein achieves its proper conformation, the signalsequence is masked and the channels are exported out of theER. In HERG channels, Kupershmidt et al identified aputative ER retention signal (R-X-R) at amino acids 1005 to1007 that regulates the surface expression of channel pro-tein.49 They found that deleting the last 147 amino acids(�1012-HERG) from the C-terminal abolished the surfaceexpression of IHERG. Removing the ER retention signal at 1005to 1007 by truncating the last 159 amino acids (�1000-HERG) or mutating the ER retention signal arginines toleucines (R-G-R to L-G-L) increased IHERG. Coexpressing a“decoy” 100-amino acid C-terminal peptide containing theR-G-R retention signal also increased the surface expressionof �1012-HERG. The data suggested that quality-controlcheckpoints regulate HERG trafficking via this ER retentionsignal. Recently, Akhavan et al42 demonstrated that deletingmuch of the C-terminus (�860-HERG) as well as a smaller39-amino acid segment of the C-terminus (�860 to 899-HERG) caused intracellular retention of the protein anddecreased IHERG, suggesting that HERG channels may havemultiple regions that regulate their trafficking out of the ER.
Once in the Golgi apparatus, HERG channels undergocomplex glycosylation. Although HERG protein contains
multiple consensus sites for N-linked glycosylation (N-X-S/T), it is the asparagine at position 598 (N598) that appears toundergo N-linked core- and complex-glycosylation.12 Severalexperimental approaches have shown that HERG subunitprotein is first synthesized as �132-kD peptide in the ER,which rapidly undergoes N-linked core-glycosylation to in-crease the molecular mass to �135-kD. In the Golgi appara-tus, complex glycosylation increases the molecular mass ofeach channel subunit to �155-kD.12,32,44,50 Several biologicalfunctions have been attributed to core- and complex glyco-sylation, including promoting proper protein folding, ERexport, altering protein function, and regulating protein sta-bility. Initially disruption of N-linked glycosylation wasthought to prevent the efficient surface expression of HERGchannels.51 More recent studies have shown thatglycosylation-deficient channels are expressed in the cellsurface membrane and can generate IHERG. However, pulse-chase labeling experiments suggest that the glycosylationdeficient channel protein has a shorter half-life comparedwith WT HERG channels.12
In a yeast 2-hybrid screen of human heart library, aGolgi-resident protein, GM130, interacted with a HERGC-terminal fragment encoding amino acids 667 to 1159.52
However, unlike the Hc/sp 70 and Hsp 90, GM130 coimmu-noprecipitates with both immature core-glycosylated andmature complexly glycosylated HERG protein. CoexpressingGM130 with WT HERG channels reduced functional IHERG,suggesting that GM130 can regulate IHERG. Roti Roti etal52also showed that V822M and R823W, which aretrafficking-defective LQT2 mutations in the nucleotide-binding domain, disrupted the interaction of GM130 with theHERG C-terminal fragment. Given this result, it is temptingto speculate that disruption of the HERG and GM130interaction may contribute to the phenotype of sometrafficking-defective LQT2 mutations.
Reversing the Trafficking-Defective LQT2Phenotype: New Therapeutic StrategiesIn mammalian cells, reducing the culture temperature canrestore the oligomerization and export of mutant proteins thatare retained in the ER.53,54 Reducing cell culture temperaturealso increases surface expression of several trafficking-defective LQT2 channels. Additional methods that increasethe surface expression of LQT2 trafficking-defective chan-nels have been identified, including incubating cells in: (1)molar concentrations of glycerol; (2) drugs that bind to andcause HERG channel block or their analogues (E4031,cisapride, astemizole, quinidine, fexofenadine); or (3) thesarcoplasmic/endoplasmic reticulum Ca-ATPase (SERCA)inhibitor thapsigargin.31,37–39,43,44,55 The finding that somemutant channels can be “pharmacologically rescued” tofunction in the cell membrane has obvious therapeuticimplications.
Rescue, however, is selective for specific trafficking-defective LQT2 mutations. The T65P, N470D, G601S,R752W, F805C, V822M and R823W mutations are rescuedby lowering incubation temperature, which is thought topromote native protein folding by stabilizing intermediatesteps in the protein-folding pathway. The T65P, N470D, and
Delisle et al Ion Channel Protein Trafficking 1423
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

G601S (but not R752W, F805C, or R823W) are rescued byincubating in HERG channel blocking drugs. Amino acidresidues on the inner portion of the sixth transmembranesegment (S6) of HERG channel protein constitute the drug-binding domain for HERG channel-blocking drugs.56,56a Mu-tating the drug-binding domain minimizes drug block ofHERG channels and prevents the pharmacological rescue ofthe LQT2 trafficking-defective mutant G601S, suggestingthat the inner pore domain may underlie both pharmacolog-ical rescue as well as drug-block of IHERG.43 Although themechanism of pharmacological rescue is incompletely under-stood, binding of HERG channel-blocking drugs may help tostabilize intermediate states of the mutant channel protein thatpromote export of the channel out of the ER. At concentra-tions required for pharmacological rescue most drugs blockIHERG, thereby limiting their therapeutic value.38,43 However,fexofenadine (terfenadine carboxylate) was shown to increasecurrent in the N470D and G601S mutations at drug concen-trations lower than IHERG blocking concentrations, thus uncou-pling channel block from pharmacological rescue.55 Thapsi-gargin, an inhibitor of SERCA channels, can also rescue thetrafficking-defective LQT2 mutations G601S and F805C (butnot N470D). The mechanism of thapsigargin-mediated rescueis distinct from that of rescue by HERG channel blockers for2 reasons. Thapsigargin does not block IHERG at concentrationsthat cause pharmacological rescue, and thapsigargin rescuesLQT2 mutations that HERG channel-blocking drugs do not.44
The mechanism underlying thapsigargin rescue is specula-tive, although it appears to involve alterations in luminal ER[Ca2�] that directly affect protein folding or Ca2�-dependentmolecular chaperones. Interestingly, thapsigargin has alsobeen shown restore surface expression of mutant channels inother diseases that prevent ER export, such as in CFTR.58
The proposed mechanism for trafficking-defective chan-nels is that the protein is incorrectly folded and thereforeearmarked for intracellular retention by cellular quality-control mechanisms. Rescue interrupts this. This postulate issupported by the observation that G601S and R752W haveincreased interactions with Hc/sp 70 and Hsp90 comparedwith WT channels. Rescue reduced these chaperone interac-tions for G601S and R752W.47 It is also important to note thatdifferent methods of rescue do not increase the surfaceexpression of WT channels. Taken together, the data suggestthat rescue by several methods increases the probability thata mutant protein will reach its native conformation. Theobservation that different methods of rescue do not affectsimilarly all LQT2 trafficking-defective channels suggeststhat these mutations differentially affect the protein foldingand oligomerization steps.
Beyond LQT2: Other Proarrhythmic SyndromesLinked to Trafficking-Defective ChannelsTrafficking-defective mutations have been described for thecardiac Na� channel and the inward rectifier K� channelidentified from patients with inherited arrhythmia syndromes.Baroudi et al showed that the Brugada syndrome mutationR1432G and the double mutation R1232W/T1620M reducedINa, and that mutant protein colocalized with the ER residentprotein calnexin, suggesting ER trapping.59,60 Another
trafficking-defective Na� channel mutation, M1766L, wasidentified in an infant with ventricular tachycardia.61,62 Sur-face expression of M1766L increased in mammalian cells byreducing culture temperature, coexpressing the Na� channel�1 subunit, or incubating cells in the Na� channel blockermexiletine.61 Surprisingly, the trafficking-defective pheno-type of the mutation differed depending on the clone of thecardiac Na� channel (hH1, hH1a, or hH1b). The M1776Lmutation prevented the ER export of channel protein in thehH1 and hH1a clones, but not the hH1b clone, which containsa common polymorphism.62 These data suggest that poly-morphisms may modify mutant phenotype expressionthrough unknown intragenic actions.
Multiple mutations in the KCNJ2 gene have been describedin patients with Andersen syndrome. In heterologous expres-sion systems, these mutations cause marked reductions in K�
current. At least some mutations (�95 to 98 and �314 to 315)are reported to be trafficking-defective, with the channelsfailing to reach the surface membrane.63 Both of thesemutations had a dominant-negative effect on surface expres-sion of WT channel protein.
These findings with LQT2, Brugada syndrome, andAndersen syndrome mutations show that defects in proteintrafficking are a relatively common consequence of genemutations and provide one mechanism for loss of ion channelcurrent in inherited arrhythmia syndromes. Given that loss offunction occurs in many of the inherited arrhythmia syn-dromes (Table 2), it is reasonable to speculate that defectiveprotein trafficking will be a common mechanism identified inmany other inherited arrhythmia syndromes and diseasemodels.
A scheme for categorizing alterations in cardiac ion chan-nels in inherited and possibly some acquired arrhythmiadiseases is shown in Table 3 and is in keeping with thenomenclature developed for other inheritable diseases (seelater). Class 1 mutations include abnormalities at the level ofgene transcription or in protein translation that result in no,truncated, nonsense, or altered protein levels. For example,the nucleotide deletion HERG 1261delA leads to an in-framereading abnormality that is thought to result in a truncated,nonfunctional HERG protein.64 Similarly, mutation/polymor-phism in an hNaV1.5 promoter results in altered expression ofNa� channels by altering transcriptional activity to produceloss of functional current.33 Class 2 mutations produceabnormal posttranslational protein processing (protein fold-ing, oligomerization, etc) and lead to defective protein traf-ficking. As discussed, these mutations appear to be common,have been identified in KCNH2, KCNJ2, and hNaV1.5 genes,and span the length and organization of the channel proteins(for HERG, see Figure 2). Multiple intracellular mechanisms
TABLE 3. Classification Scheme for Cardiac IonChannel Mutations
Class 1 Abnormal protein synthesis (altered transcriptionor translation)
Class 2 Defective protein processing/trafficking.
Class 3 Abnormal gating/kinetics
Class 4 Altered or no permeability
1424 Circulation Research June 11, 2004
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

appear to contribute to protein trafficking defects;44 thus,ultimately, subdivisions of class 2 mutation effects mayemerge. Class 3 mutations result in ion channels that havealtered biophysical properties because of changes in channelgating and/or kinetics. Mutations in this class also appear tobe common in LQTS and other arrhythmia syndromes and arefound in different regions and domains of channel proteins.An example is the T474I mutation in HERG channels, wherevoltage-dependent gating is markedly shifted resulting inIHERG activation at more negative voltages, but with decreasedIHERG at more positive voltages.32 A recently described HERGmutation, N588K, which results in failure of the channel toinactivate normally to cause an increase in IHERG during theaction potential plateau, and was identified in 2 families withshort QT syndrome.65 Most LQT3 mutations result in alteredgating of the cardiac Na� channel with marked slowing ofinactivation to increase late INa. Class 4 mutations result inaltered or absent channel selectivity or permeability. Thesegene mutations are located near the ion channel pore regionand have been associated with severe LQTS disease pheno-types.40,41 For example, the G628S mutation in HERG chan-nels results in a normally trafficking protein that insertscorrectly into the cell surface membrane, yet the mutationcauses loss of channel function.32 One amino acid down-stream is the N629D mutation, which causes altered channelinactivation and a reduction in selectivity for K� over Na�.57
The classification scheme shown in Table 3 provides insightinto understanding the impact of ion channel gene mutationson the control of macroscopic current (I); class 1 and 2mutations alter N, class 3 mutations alter Po, and class 4mutations alter i. Clearly, some mutations result in changes inchannel properties that can be attributed to multiple classes.
Defective Protein Trafficking in OtherInheritable Diseases
Defective protein trafficking has emerged as an importantmechanism in many diseases.
Familial Hypercholesterolemia and theLow-Density Lipoprotein ReceptorCholesterol, although a small molecule, plays a vital role inbiology. Familial hypercholesterolemia is one of several geneticcauses of an elevated low-density lipoprotein (LDL) concentra-tion in plasma. In pioneering work, Brown and Goldsteinidentified mutations in the gene encoding the LDL receptor thatcaused defective protein trafficking, as well as affecting LDLreceptor internalization, ligand-binding, and appropriate target-ing of the LDL receptor in hepatocytes.66–69 More than 700mutations have been identified in the gene encoding the LDLreceptor protein (http://www.ucl.ac.uk/fh/). These mutationsusually are grouped functionally according to the pattern ofdisruption of the structure and function of LDL receptor. Class Imutations have no receptors synthesized. Class II mutationshave LDL receptor protein synthesized, but it is trafficking-defective and is retained in the ER. Class III mutations result inreceptor protein that traffics to reach the cell surface but fails tobind LDL normally. Class IV mutations result in receptors thatreach the cell surface and bind LDL, but fail to cluster in coatedpits for subsequent internalization. It is interesting that �50% of
LDL receptor mutations act to disrupt receptor protein traffick-ing from the ER to the Golgi complex.70,71
Cystic Fibrosis and CFTRCystic fibrosis is a monogenic recessive disease caused bymutations in the gene encoding for the CFTR protein.72 It is animportant disease in protein trafficking. CFTR is a cAMP-dependent Cl� channel that regulates fluid composition acrossthe epithelial cell membranes. More than 1000 mutations in thegene have been described (http://www.genet.sickkids.on.ca/cgi-bin/WebObjects/MUTATION). Similar to the LDL receptormutations, CFTR mutations are usually grouped according to thepattern of disruption of the CFTR protein. Class I mutationsresult in failed synthesis of CFTR protein. Class II mutationscause defective protein trafficking with the CFTR proteinretained in the ER. Class III mutations cause defective regulationof normally trafficking CFTR protein. Class IV mutations causean abnormal channel conductance. The most common mutationin cystic fibrosis is the deletion of the codon for a phenylalanineat position 508 (�F508) of CFTR protein and is found in 70% ofaffected patients. This mutation is thought to cause the CFTRprotein to fold incorrectly and be retained in the ER, thus failingto traffic to the plasma membrane.73 It is then retrotranslocatedfrom the ER to undergo ubiquitination and proteosomal degra-dation.74,75 The �F508 CFTR protein is particularly interestingbecause it is capable of forming functional channels underexperimental conditions. In both heterologous expression andepithelial tissue systems, the protein trafficking defect can be“corrected” by reducing incubation temperature (�30°C) and byincubation with a variety of chemical agents such as glycerol,trimethylamine N-oxide, sodium 4-phenylbutyrate, and deuter-ated water, which are proposed to act as pharmacologicalchaperones to cause misfolded CFTR protein to assume aconfiguration that permits trafficking to the surface mem-brane.76–78 These findings have driven the search for newpharmacological strategies for the treatment of patients withcystic fibrosis.
Charcot-Marie-Tooth Disease and ConnexinsCharcot-Marie-Tooth disease (CMTX) is a complex polygenicneuropathic disorder that constitutes the most common form ofinheritable disease in the peripheral nervous system. Connexinsare a family of homologous integral gap junction membraneproteins that form channels for the transmission of electricalsignals and diffusion of small ions and molecules betweencoupled cells.79 One form of CMTX results from mutations inthe gap junction protein �1 gene (GJB1), which encodesconnexin 32 (Cx32).80–83 More than 200 mutations throughoutGJB1 have been identified.80,84–88 Several molecular mecha-nisms have been proposed for Cx32 mutations to cause CMTX,including: (1) mRNA for Cx32 is not transcribed; (2) mRNA isnormally transcribed but little protein is produced; (3) Cx32protein is synthesized but not properly transported to the plasmamembrane; (4) the Cx32 protein is transported normally to theplasma membrane but does not form functional channels; and(5) the Cx32 protein inserts in the surface membrane and formsgap junction channels that function abnormally.
Delisle et al Ion Channel Protein Trafficking 1425
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

Nephrogenic Diabetes Insipidus andAquaporin ChannelsNephrogenic diabetes insipidus (NDI) is characterized by theinability to concentrate the urine resulting in excessive urineproduction and thirst. The genetic basis of NDI is multifac-torial and includes mutations in the aquaporin-2 channel(AQP2) gene. This channel is vasopressin-regulated and isfound in the kidney at distinct sites along nephrons andcollecting ducts.89 More than 20 mutations in AQP2 havebeen identified in patients with autosomal-recessive NDI.Functional expressions of several AQP2 mutations haveshown that some result in nonfunctional channel proteins,whereas others produce a small increase in osmotic waterpermeability.90–93 Several AQP2 mutant proteins show im-paired transport from the ER. Interestingly, Tamarappoo andVerkman93 found that the trafficking defect of several AQP2mutations was corrected by incubation in glycerol to rescuefunctional channels, and immunostaining confirmed theirredistribution from ER to the cell surface.
The diseases described are but a few examples of patho-logical conditions caused by gene mutations that may resultin failure of proteins to traffic normally through the ER toreach their intended destinations. Presently, nearly 100 dis-eases have been reported that involve abnormal proteintrafficking or “traffic jams” within cells.94,95 Furthermore, itis clear that while some mutations interfere with the ability ofa protein to undergo normal processing and intracellulartrafficking, the same mutation may have minimal or no effecton the protein’s function provided it reaches its intendedtarget. Thus, therapeutic strategies to correct or restoreprotein trafficking, even partially, may have important clini-cal benefits.
Summary: Genomics and ProteomicsThe study of inherited arrhythmia syndromes is one area inwhich human genomics has led to new information andinsight into the polygenic nature of some cardiac arrhythmias.Undoubtedly, more genes and mutations for cardiac arrhyth-mia diseases await discovery. Concomitantly, proteomics isresulting in the identification of multiple molecular andcellular mechanisms that underlie the phenotypic expressionof gene mutations. These discoveries potentially may lead tonew proteomic-based, as well as gene-based, therapies inmany diseases. Presently, molecular models do not exist thataccurately predict the functional consequences of most ionchannel gene mutations on biogenic or biophysical function.Whereas the identification of new genes and gene mutationsremains an essential component for progress in understandingdisease mechanisms, this must be accompanied by functionalexpression studies to identify the mechanisms for molecularand cellular dysfunction of the encoded proteins.
AcknowledgmentsThis work is supported in part by National Heart Lung and BloodInstitute grant R01 HL60723 (C.T.J.) and National Research ServiceAward Postdoctoral Fellowship Award F32 HL071476 (B.P.D.). Theauthors thank Drs Eugenia M.C. Jones and Gail A. Robertson forhelpful scientific comments, and Thankful Sanftleben for superbassistance with the preparation of the manuscript.
References1. Corabouef E, Weidmann S. Potentiel de repos et potentiels d’action du
muscle cardiaque mesures a l’aide d’electrodes intracellulaires. C R SocBiol. 1949;143:1329–1331.
2. Corabouef E, Weidmann S. Potentiel du muscle cardiaque obtebus al’aide de microelectrodes intracellulaires. C R Soc Biol. 1949;143:1361-
3. Woodbury JW, Lee J, Brady AJ, Merendino KA. Transmembranalpotentials from the human heart. Circ Res. 1957;5:179.
4. Bromberger-Barnea B, Caldini P, Wittenstein GJ. Transmembrane potentials ofthe normal and hypothermic human heart. Circ Res. 1959;7:138–140.
5. Trautwein W, Kassebaum DG, Nelson RM, Hecht H. Electrophysiolog-ical study of human heart muscle. Circ Res. 1962;10:306–312.
6. Anfinsen CB, Haber E, Sela M, White FH, Jr. The kinetics of formationof native ribonuclease during oxidation of the reduced polypeptide chain.Proc Natl Acad Sci U S A. 1961;47:1309–1314.
7. Kozak M. Interpreting cDNA sequences: some insights from studies ontranslation. Mamm Genome. 1996;7:563–574.
8. Tu L, Wang J, Helm A, Skach WR, Deutsch C. Transmembrane bio-genesis of Kv1.3. Biochemistry. 2000;39:824–836.
9. Fewell SW, Travers KJ, Weissman JS, Brodsky JL. The action ofmolecular chaperones in the early secretory pathway. Annu Rev Genet.2001;35:149–191.
10. Walter S, Buchner J. Molecular chaperones–cellular machines for proteinfolding. Angew Chem Int Ed Engl. 2002;41:1098–1113.
11. Helenius A, Aebi M. Intracellular functions of N-linked glycans. Science.2001;291:2364–2369.
12. Gong Q, Anderson CL, January CT, Zhou Z. Role of glycosylation in cellsurface expression and stability of HERG potassium channels. Am JPhysiol Heart Circ Physiol. 2002;283:H77–H84.
13. Schrag JD, Procopio DO, Cygler M, Thomas DY, Bergeron JJ. Lectincontrol of protein folding and sorting in the secretory pathway. TrendsBiochem Sci. 2003;28:49–57.
14. Deutsch C. The birth of a channel. Neuron. 2003;40:265–276.15. Rosenberg RL, East JE. Cell-free expression of functional Shaker
potassium channels. Nature. 1992;360:166–169.16. Shen NV, Chen X, Boyer MM. Pfaffinger PJ. Deletion analysis of K�
channel assembly. Neuron. 1993;11:67–76.17. Deutsch C. Potassium channel ontogeny. Annu Rev Physiol. 2002;64:19–46.18. McDonald TV, Yu Z, Ming Z, Palma E, Meyers MB, Wang KW,
Goldstein SA, Fishman GI. A minK-HERG complex regulates the cardiacpotassium current I(Kr). Nature. 1997;388:289–292.
19. Nagaya N, Papazian DM. Potassium channel alpha and beta subunitsassemble in the endoplasmic reticulum. J Biol Chem. 1997;272:3022–3027.
20. Lippincott-Schwartz J, Roberts TH, Hirschberg K. Secretory proteintrafficking and organelle dynamics in living cells. Annu Rev Cell DevBiol. 2000;16:557–589.
21. Ma D, Jan LY. ER transport signals and trafficking of potassium channelsand receptors. Curr Opin Neurobiol. 2002;12:287–292.
22. Ellgaard L, Molinari M, Helenius A. Setting the standards: quality controlin the secretory pathway. Science. 1999;286:1882–1888.
23. Schwartz AL, Ciechanover A. The ubiquitin-proteasome pathway andpathogenesis of human diseases. Annu Rev Med. 1999;50:57–74.
24. Kostova Z, Wolf DH. For whom the bell tolls: protein quality control ofthe endoplasmic reticulum and the ubiquitin-proteasome connection.EMBO J. 2003;22:2309–2317.
25. Cuervo AM, Dice JF. Age-related decline in chaperone-mediatedautophagy. J Biol Chem. 2000;275:31505–31513.
26. Klionsky DJ, Emr SD. Autophagy as a regulated pathway of cellulardegradation. Science. 2000;290:1717–1721.
27. Jervell A, Lange-Nielsen F. Congenital deaf-mutism, functional heartdisease with prolongation of the Q-T interval and sudden death. AmHeart J. 1957;54:59–68.
28. Romano C, Gremme G, Pongiglione R. Aritmie cardiache rare dell’ etapediatrica. II. Accessi sincopali per fibrillazione ventricolare parossistica.Clinica Pediatrica, Bologna. 1963;45:656–683.
29. Ward OC. A new familial cardiac syndrome in children. J Ir Med Assoc.1964;54:103–106.
30. Keating MT, Sanguinetti MC. Molecular genetic insights into cardiovas-cular disease. Science. 1996;272:681–685.
31. January CT, Gong Q, Zhou Z. Long QT syndrome: cellular basis and arrhythmiamechanism in LQT2. J Cardiovasc Electrophysiol. 2000;11:1413–1418.
32. Zhou Z, Gong Q, Epstein ML, January CT. HERG channel dysfunction inhuman long QT syndrome. Intracellular transport and functional defects.J Biol Chem. 1998;273:21061–21066.
1426 Circulation Research June 11, 2004
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

33. Yang P, Bezzina C, Zhou B, Baldwin HSS, Liu K, Kupershmidt S, RodenDM. Regulation of cardiac sodium channel transcription in vitro and invivo. Circulation. 2003;108:IV-75–IV-76.
34. Sanguinetti MC, Curran ME, Spector PS, Keating MT. Spectrum ofHERG K�-channel dysfunction in an inherited cardiac arrhythmia. ProcNatl Acad Sci U S A. 1996;93:2208–2212.
35. Ficker E, Dennis AT, Obejero-Paz CA, Castaldo P, Taglialatela M,Brown AM. Retention in the endoplasmic reticulum as a mechanism ofdominant-negative current suppression in human long QT syndrome. JMol Cell Cardiol. 2000;32:2327–2337.
36. Ficker E, Thomas D, Viswanathan PC, Dennis AT, Priori SG, NapolitanoC, Memmi M, Wible BA, Kaufman ES, Iyengar S, Schwartz PJ, Rudy Y,Brown AM. Novel characteristics of a misprocessed mutant HERGchannel linked to hereditary long QT syndrome. Am J Physiol Heart CircPhysiol. 2000;279:H1748–H1756.
37. Paulussen A, Raes A, Matthijs G, Snyders DJ, Cohen N, Aerssens J. Anovel mutation (T65P) in the PAS domain of the human potassiumchannel HERG results in the long QT syndrome by trafficking deficiency.J Biol Chem. 2002;277:48610–48616.
38. Zhou Z, Gong Q, January CT. Correction of defective protein trafficking ofa mutant HERG potassium channel in human long QT syndrome. Pharma-cological and temperature effects. J Biol Chem. 1999;274:31123–31126.
39. Furutani M, Trudeau MC, Hagiwara N, Seki A, Gong Q, Zhou Z,Imamura S, Nagashima H, Kasanuki H, Takao A, Momma K, JanuaryCT, Robertson GA, Matsuoka R. Novel mechanism associated with aninherited cardiac arrhythmia: defective protein trafficking by the mutantHERG (G601S) potassium channel. Circulation. 1999;99:2290–2294.
40. Huang FD, Chen J, Lin M, Keating MT, Sanguinetti MC. Long-QTsyndrome-associated missense mutations in the pore helix of the HERGpotassium channel. Circulation. 2001;104:1071–1075.
41. Moss AJ, Zareba W, Kaufman ES, Gartman E, Peterson DR, Benhorin J,Towbin JA, Keating MT, Priori SG, Schwartz PJ, Vincent GM, RobinsonJL, Andrews ML, Feng C, Hall WJ, Medina A, Zhang L, Wang Z.Increased risk of arrhythmic events in long-QT syndrome with mutationsin the pore region of the human ether-a-go-go-related gene potassiumchannel. Circulation. 2002;105:794–799.
42. Akhavan A, Atanasiu R, Shrier A. Identification of a COOH-terminalsegment involved in maturation and stability of human ether-a-go-go-related gene potassium channels. J Biol Chem. 2003;278:40105–40112.
43. Ficker E, Obejero-Paz CA, Zhao S, Brown AM. The binding site for channelblockers that rescue misprocessed human long QT syndrome type 2 ether-a-gogo-related gene (HERG) mutations. J Biol Chem. 2002;277:4989–4998.
44. Delisle BP, Anderson CL, Balijepalli RC, Anson BD, Kamp TJ, JanuaryCT. Thapsigargin selectively rescues the trafficking defective LQT2channels G601S and F805C. J Biol Chem. 2003;278:35749–35754.
45. Cui J, Kagan A, Qin D, Mathew J, Melman YF, McDonald TV. Analysisof the cyclic nucleotide binding domain of the HERG potassium channeland interactions with KCNE2. J Biol Chem. 2001;276:17244–17251.
46. Kagan A, Yu Z, Fishman GI, McDonald TV. The dominant negativeLQT2 mutation A561V reduces wild-type HERG expression. J BiolChem. 2000;275:11241–11248.
47. Ficker E, Dennis AT, Wang L, Brown AM. Role of the cytosolic chap-erones Hsp70 and Hsp90 in maturation of the cardiac potassium channelHERG. Circ Res. 2003;92:e87–100.
48. Zerangue N, Schwappach B, Jan YN, Jan LY. A new ER traffickingsignal regulates the subunit stoichiometry of plasma membrane K(ATP)channels. Neuron. 1999;22:537–548.
49. Kupershmidt S, Yang T, Chanthaphaychith S, Wang Z, Towbin JA,Roden DM. Defective human Ether-a-go-go-related gene traffickinglinked to an endoplasmic reticulum retention signal in the C terminus.J Biol Chem. 2002;277:27442–27448.
50. Zhou Z, Gong Q, Ye B, Fan Z, Makielski JC, Robertson GA, January CT.Properties of HERG channels stably expressed in HEK 293 cells studiedat physiological temperature. Biophys J. 1998;74:230–241.
51. Petrecca K, Atanasiu R, Akhavan A, Shrier A. N-linked glycosylationsites determine HERG channel surface membrane expression. J Physiol.1999;515(Pt 1):41–48.
52. Roti Roti EC, Myers CD, Ayers RA, Boatman DE, Delfosse SA, ChanEK, Ackerman MJ, January CT, Robertson GA. Interaction with GM130during HERG ion channel trafficking. Disruption by type 2 congenitallong QT syndrome mutations. Human Ether-a-go-go-Related Gene. J BiolChem. 2002;277:47779–47785.
53. Bergmann JE, Singer SJ. Immunoelectron microscopic studies of the intracellulartransport of the membrane glycoprotein (G) of vesicular stomatitis virus ininfected Chinese hamster ovary cells. J Cell Biol. 1983;97:1777–1787.
54. Kreis TE, Lodish HF. Oligomerization is essential for transport of vesicularstomatitis viral glycoprotein to the cell surface. Cell. 1986;46:929–937.
55. Rajamani S, Anderson CL, Anson BD, January CT. Pharmacologicalrescue of human K(�) channel long-QT2 mutations: human ether-a-go-go-related gene rescue without block. Circulation. 2002;105:2830–2835.
56. Lees-Miller JP, Duan Y, Teng GQ, Duff HJ. Molecular determinant ofhigh-affinity dofetilide binding to HERG1 expressed in Xenopus oocytes:involvement of S6 sites. Mol Pharmacol. 2000;57:367–374.
56a. Mitcheson JS, Chen J, Lin M, Culberson C, Sanguinetti MC. A structural basisfor drug-induced long QT syndrome. Proc Natl Acad Sci U S A. 2000;97:12329–12333.
57. Lees-Miller JP, Duan Y, Teng GQ, Thorstad K, Duff HJ. Novel gain-of-functionmechanism in K(�) channel-related long-QT syndrome: altered gating andselectivity in the HERG1 N629D mutant. Circ Res. 2000;86:507–513.
58. Egan ME, Glockner-Pagel J, Ambrose C, Cahill PA, Pappoe L, BalamuthN, Cho E, Canny S, Wagner CA, Geibel J, Caplan MJ. Calcium-pumpinhibitors induce functional surface expression of Delta F508-CFTRprotein in cystic fibrosis epithelial cells. Nat Med. 2002;8:485–492.
59. Baroudi G, Acharfi S, Larouche C, Chahine M. Expression and intra-cellular localization of an SCN5A double mutant R1232W/T1620Mimplicated in Brugada syndrome. Circ Res. 2002;90:E11–E16.
60. Baroudi G, Pouliot V, Denjoy I, Guicheney P, Shrier A, Chahine M.Novel mechanism for Brugada syndrome: defective surface localizationof an SCN5A mutant (R1432G). Circ Res. 2001;88:E78–E83.
61. Valdivia CR, Ackerman MJ, Tester DJ, Wada T, McCormack J, Ye B,Makielski JC. A novel SCN5A arrhythmia mutation, M1766L, withexpression defect rescued by mexiletine. Cardiovasc Res. 2002;55:279–289.
62. Ye B, Valdivia CR, Ackerman MJ, Makielski JC. A common humanSCN5A polymorphism modifies expression of an arrhythmia causingmutation. Physiol Genomics. 2003;12:187–193.
63. Bendahhou S, Donaldson MR, Plaster NM, Tristani-Firouzi M, Fu YH,Ptacek LJ. Defective potassium channel Kir2.1 trafficking underliesAndersen-Tawil syndrome. J Biol Chem. 2003;278:51779–51785.
64. Curran ME, Splawski I, Timothy KW, Vincent GM, Green ED, KeatingMT. A molecular basis for cardiac arrhythmia: HERG mutations causelong QT syndrome. Cell. 1995;80:795–803.
65. Brugada R, Hong K, Dumaine R, Cordeiro J, Gaita F, Borggrefe M,Menendez TM, Brugada J, Pollevick GD, Wolpert C, Burashnikov E,Matsuo K, Sheng WY, Guerchicoff A, Bianchi F, Giustetto C, Schimpf R,Brugada P, Antzelevitch C. Sudden death associated with short-QTsyndrome linked to mutations in HERG. Circulation. 2003;109:30–35.
66. Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterolhomeostasis. Science. 1986;232:34–47.
67. Funahashi T, Miyake Y, Yamamoto A, Matsuzawa Y, Kishino B.Mutations of the low density lipoprotein receptor in Japanese kindredswith familial hypercholesterolemia. Hum Genet. 1988;79:103–108.
68. Hobbs HH, Brown MS, Goldstein JL. Molecular genetics of the LDL receptorgene in familial hypercholesterolemia. Hum Mutat. 1992;1:445–466.
69. Koivisto UM, Hubbard AL, Mellman I. A novel cellular phenotype forfamilial hypercholesterolemia due to a defect in polarized targeting ofLDL receptor. Cell. 2001;105:575–585.
70. Hobbs HH, Russell DW, Brown MS, Goldstein JL. The LDL receptorlocus in familial hypercholesterolemia: mutational analysis of amembrane protein. Annu Rev Genet. 1990;24:133–170.
71. Goldstein JL, Brown MS. Molecular medicine. The cholesterol quartet.Science. 2001;292:1310–1312.
72. Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z,Zielenski J, Lok S, Plavsic N, Chou JL. Identification of the cysticfibrosis gene: cloning and characterization of complementary DNA.Science. 1989;245:1066–1073.
73. Cheng SH, Gregory RJ, Marshall J, Paul S, Souza DW, White GA,O’Riordan CR, Smith AE. Defective intracellular transport and pro-cessing of CFTR is the molecular basis of most cystic fibrosis. Cell.1990;63:827–834.
74. Yang Y, Janich S, Cohn JA, Wilson JM. The common variant of cysticfibrosis transmembrane conductance regulator is recognized by hsp70 anddegraded in a pre-Golgi nonlysosomal compartment. Proc Natl Acad SciU S A. 1993;90:9480–9484.
75. Pind S, Riordan JR, Williams DB. Participation of the endoplasmic reticulumchaperone calnexin (p88, IP90) in the biogenesis of the cystic fibrosis trans-membrane conductance regulator. J Biol Chem. 1994;269:12784–12788.
76. Cheng SH, Fang SL, Zabner J, Marshall J, Piraino S, Schiavi SC,Jefferson DM, Welsh MJ, Smith AE. Functional activation of the cysticfibrosis trafficking mutant delta F508-CFTR by overexpression. Am JPhysiol. 1995;268:L615–L624.
Delisle et al Ion Channel Protein Trafficking 1427
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

77. Sato S, Ward CL, Krouse ME, Wine JJ, Kopito RR. Glycerol reversesthe misfolding phenotype of the most common cystic fibrosis mutation.J Biol Chem. 1996;271:635–638.
78. Brown CR, Hong-Brown LQ, Biwersi J, Verkman AS, WelchWJ. Chemical chaperones correct the mutant phenotype of the deltaF508 cystic fibrosis transmembrane conductance regulator protein. CellStress Chaperones. 1996;1:117–125.
79. Zhou L, Griffin JW. Demyelinating neuropathies. Curr Opin Neurol.2003;16:307–313.
80. Bergoffen J, Scherer SS, Wang S, Scott MO, Bone LJ, Paul DL, ChenK, Lensch MW, Chance PF, Fischbeck KH. Connexin mutations inX-linked Charcot-Marie-Tooth disease. Science. 1993;262:2039–2042.
81. Ionasescu VV. Charcot-Marie-Tooth neuropathies: from clinicaldescription to molecular genetics. Muscle Nerve. 1995;18:267–275.
82. Fischbeck KH, Deschenes SM, Bone LJ, Scherer SS. Connexin32 andX-linked Charcot-Marie-Tooth disease. Cold Spring Harb Symp QuantBiol. 1996;61:673–677.
83. Bone LJ, Deschenes SM, Balice-Gordon RJ, Fischbeck KH, Scherer SS.Connexin32 and X-linked Charcot-Marie-Tooth disease. Neurobiol Dis.1997;4:221–230.
84. Hahn AF, Bolton CF, White CM, Brown WF, Tuuha SE, Tan CC,Ainsworth PJ. Genotype/phenotype correlations in X-linked dominantCharcot-Marie-Tooth disease. Ann N Y Acad Sci. 1999;883:366–382.
85. Abrams CK, Oh S, Ri Y, Bargiello TA. Mutations in connexin 32: themolecular and biophysical bases for the X-linked form of Charcot-Marie-Tooth disease. Brain Res Brain Res Rev. 2000;32:203–214.
86. Krutovskikh V, Yamasaki H. Connexin gene mutations in humangenetic diseases. Mutat Res. 2000;462:197–207.
87. Ressot C, Bruzzone R. Connexin channels in Schwann cells and thedevelopment of the X-linked form of Charcot-Marie-Tooth disease.Brain Res Brain Res Rev. 2000;32:192–202.
88. Hanemann CO, Bergmann C, Senderek J, Zerres K, Sperfeld AD.Transient, recurrent, white matter lesions in X-linked Charcot-Marie-Tooth disease with novel connexin 32 mutation. Arch Neurol.2003;60:605–609.
89. Nielsen S, Frokiaer J, Marples D, Kwon TH, Agre P, Knepper MA.Aquaporins in the kidney: from molecules to medicine. Physiol Rev.2002;82:205–244.
90. Deen PM, Croes H, van Aubel RA, Ginsel LA, van Os CH. Water channelsencoded by mutant aquaporin-2 genes in nephrogenic diabetes insipidus areimpaired in their cellular routing. J Clin Invest. 1995;95:2291–2296.
91. Mulders SM, Knoers NV, Van Lieburg AF, Monnens LA, Leumann E,Wuhl E, Schober E, Rijss JP, van Os CH, Deen PM. New mutations inthe AQP2 gene in nephrogenic diabetes insipidus resulting in functionalbut misrouted water channels. J Am Soc Nephrol. 1997;8:242–248.
92. Canfield MC, Tamarappoo BK, Moses AM, Verkman AS, Holtzman EJ.Identification and characterization of aquaporin-2 water channelmutations causing nephrogenic diabetes insipidus with partial vaso-pressin response. Hum Mol Genet. 1997;6:1865–1871.
93. Tamarappoo BK, Verkman AS. Defective aquaporin-2 trafficking innephrogenic diabetes insipidus and correction by chemical chaperones.J Clin Invest. 1998;101:2257–2267.
94. Aridor M, Hannan LA. Traffic jam: a compendium of human diseasesthat affect intracellular transport processes. Traffic. 2000;1:836–851.
95. Aridor M, Hannan LA. Traffic jams II: an update of diseases of intra-cellular transport. Traffic. 2002;3:781–790.
96. Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, VanRaayTJ, Shen J, Timothy KW, Vincent GM, de Jager T, Schwartz PJ, ToubinJA, Moss AJ, Atkinson DL, Landes GM, Connors TD, Keating MT.Positional cloning of a novel potassium channel gene: KVLQT1mutations cause cardiac arrhythmias. Nat Genet. 1996;12:17–23.
97. Wang Q, Shen J, Splawski I, Atkinson D, Li Z, Robinson JL, Moss AJ,Towbin JA, Keating MT. SCN5A mutations associated with an inheritedcardiac arrhythmia, long QT syndrome. Cell. 1995;80:805–811.
98. Schott JJ, Charpentier F, Peltier S, Foley P, Drouin E, Bouhour JB, Donnelly P,Vergnaud G, Bachner L, Moisan JP. Mapping of a gene for long QT syndrometo chromosome 4q25–27. Am J Hum Genet. 1995;57:1114–1122.
99. Mohler PJ, Schott JJ, Gramolini AO, Dilly KW, Guatimosim S, duBell WH,Song LS, Haurogne K, Kyndt F, Ali ME, Rogers TB, Lederer WJ, Escande D,Le Marec H, Bennett V. Ankyrin-B mutation causes type 4 long-QT cardiacarrhythmia and sudden cardiac death. Nature. 2003;421:634–639.
100. Splawski I, Timothy KW, Vincent GM, Atkinson DL, Keating MT.Molecular basis of the long-QT syndrome associated with deafness.N Engl J Med. 1997;336:1562–1567.
101. Abbott GW, Sesti F, Splawski I, Buck ME, Lehmann MH, Timothy KW,Keating MT, Goldstein SA. MiRP1 forms IKr potassium channels withHERG and is associated with cardiac arrhythmia. Cell. 1999;97:175–187.
102. Tristani-Firouzi M, Jensen JL, Donaldson MR, Sansone V, Meola G,Hahn A, Bendahhou S, Kwiecinski H, Fidzianska A, Plaster N, Fu YH,Ptacek LJ, Tawil R. Functional and clinical characterization of KCNJ2mutations associated with LQT7 (Andersen syndrome). J Clin Invest.2002;110:381–388.
103. Neyroud N, Tesson F, Denjoy I, Leibovici M, Donger C, Barhanin J,Faure S, Gary F, Coumel P, Petit C, Schwartz K, Guicheney P. A novelmutation in the potassium channel gene KVLQT1 causes the Jervell andLange-Nielsen cardioauditory syndrome. Nat Genet. 1997;15:186–189.
104. Schulze-Bahr E, Wang Q, Wedekind H, Haverkamp W, Chen Q, Sun Y,Rubie C, Hordt M, Towbin JA, Borggrefe M, Assmann G, Qu X,Somberg JC, Breithardt G, Oberti C, Funke H. KCNE1 mutations causeJervell and Lange-Nielsen syndrome. Nat Genet. 1997;17:267–268.
105. Schwartz PJ, Priori SG, Dumaine R, Napolitano C, Antzelevitch C,Stramba-Badiale M, Richard TA, Berti MR, Bloise R. A molecular linkbetween the sudden infant death syndrome and the long-QT syndrome.N Engl J Med. 2000;343:262–267.
106. Ackerman MJ, Siu BL, Sturner WQ, Tester DJ, Valdivia CR, MakielskiJC, Towbin JA. Postmortem molecular analysis of SCN5A defects insudden infant death syndrome. JAMA. 2001;286:2264–2269.
107. Lupoglazoff JM, Denjoy I, Villain E, Fressart V, Simon F, Bozio A, BerthetM, Benammar N, Hainque B, Guicheney P. Long QT syndrome in neo-nates: conduction disorders associated with HERG mutations and sinusbradycardia with KCNQ1 mutations. J Am Coll Cardiol. 2004;43:826–830.
108. Chen Q, Kirsch GE, Zhang D, Brugada R, Brugada J, Brugada P,Potenza D, Moya A, Borggrefe M, Breithardt G, Ortiz-Lopez R, WangZ, Antzelevitch C, O’Brien RE, Schulze-Bahr E, Keating MT, TowbinJA, Wang Q. Genetic basis and molecular mechanism for idiopathicventricular fibrillation. Nature. 1998;392:293–296.
109. Weiss R, Barmada MM, Nguyen T, Seibel JS, Cavlovich D, KornblitCA, Angelilli A, Villanueva F, McNamara DM, London B. Clinical andmolecular heterogeneity in the Brugada syndrome: a novel gene locus onchromosome 3. Circulation. 2002;105:707–713.
110. Akai J, Makita N, Sakurada H, Shirai N, Ueda K, Kitabatake A,Nakazawa K, Kimura A, Hiraoka M. A novel SCN5A mutation asso-ciated with idiopathic ventricular fibrillation without typical ECGfindings of Brugada syndrome. FEBS Lett. 2000;479:29–34.
111. Priori SG, Napolitano C, Tiso N, Memmi M, Vignati G, Bloise R,Sorrentino V, Danieli GA. Mutations in the cardiac ryanodine receptorgene (hRyR2) underlie catecholaminergic polymorphic ventriculartachycardia. Circulation. 2000;102:r49–r53.
112. Laitinen PJ, Brown KM, Piippo K, Swan H, Devaney JM, Brahmbhatt B,Donarum EA, Marino M, Tiso N, Viitasalo M, Toivonen L, Stephan DA,Kontula K. Mutations of the cardiac ryanodine receptor (RyR2) gene in familialpolymorphic ventricular tachycardia. Circulation. 2001;103:485–490.
113. Postma AV, Denjoy I, Hoorntje TM, Lupoglazoff JM, Da Costa A,Sebillon P, Mannens MM, Wilde AA, Guicheney P. Absence of calse-questrin 2 causes severe forms of catecholaminergic polymorphic ven-tricular tachycardia. Circ Res. 2002;91:e21–e26.
114. Schott JJ, Alshinawi C, Kyndt F, Probst V, Hoorntje TM, Hulsbeek M,Wilde AA, Escande D, Mannens MM, Le Marec H. Cardiac conductiondefects associate with mutations in SCN5A. Nat Genet. 1999;23:20–21.
115. Benson DW, Wang DW, Dyment M, Knilans TK, Fish FA, Strieper MJ,Rhodes TH, George AL, Jr. Congenital sick sinus syndrome caused byrecessive mutations in the cardiac sodium channel gene (SCN5A). J ClinInvest. 2003;112:1019–1028.
116. Schulze-Bahr E, Neu A, Friederich P, Kaupp UB, Breithardt G, PongsO, Isbrandt D. Pacemaker channel dysfunction in a patient with sinusnode disease. J Clin Invest. 2003;111:1537–1545.
117. Chen YH, Xu SJ, Bendahhou S, Wang XL, Wang Y, Xu WY, Jin HW,Sun H, Su XY, Zhuang QN, Yang YQ, Li YB, Liu Y, Xu HJ, Li XF, MaN, Mou CP, Chen Z, Barhanin J, Huang W. KCNQ1 gain-of-functionmutation in familial atrial fibrillation. Science. 2003;299:251–254.
118. Brugada R, Tapscott T, Czernuszewicz GZ, Marian AJ, Iglesias A, MontL, Brugada J, Girona J, Domingo A, Bachinski LL, Roberts R. Identi-fication of a genetic locus for familial atrial fibrillation. N Engl J Med.1997;336:905–911.
119. Ellinor PT, Shin JT, Moore RK, Yoerger DM, MacRae CA. Locus for atrialfibrillation maps to chromosome 6q14–16. Circulation. 2003;107:2880–2883.
120. Bellocq C, van Ginneken A, Bezzina CR, Escande D, Mannens M, BaroI, Wilde AA. Mutation in the KCNQ1 gene leading to the short intervalsyndrome. Circulation. 2004. In press.
1428 Circulation Research June 11, 2004
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from

Brian P. Delisle, Blake D. Anson, Sridharan Rajamani and Craig T. JanuaryBiology of Cardiac Arrhythmias: Ion Channel Protein Trafficking
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2004 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.0000128561.28701.ea2004;94:1418-1428Circ Res.
http://circres.ahajournals.org/content/94/11/1418World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 14, 2018
http://circres.ahajournals.org/D
ownloaded from