Embed Size (px)
Citation preview

Bleeding Disorders in Congenital SyndromesSusmita N. Sarangi, MD, Suchitra S. Acharya, MD
Bleeding Disorders and Thrombosis Program, Cohen
Children’s Medical Center of New York, New Hyde Park,
New York
Drs Sarangi and Acharya contributed to the
conceptualization, content, and composition of the
manuscript and approved the fi nal manuscript as
submitted.
DOI: 10.1542/peds.2015-4360
Accepted for publication Aug 15, 2016
Address correspondence to Suchitra S. Acharya,
MD, Bleeding Disorders and Thrombosis Program,
Cohen Children’s Medical Center of New York, 269-
01 76th Ave, Suite 255, New Hyde Park, NY 11040.
E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2017 by the American Academy of
Pediatrics
FINANCIAL DISCLOSURE: The authors have
indicated they have no fi nancial relationships
relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors
have indicated they have no potential confl icts of
interest to disclose.
Children with congenital syndromes
with multiple anomalies need a
multidisciplinary approach to
their care, along with continued
surveillance for rare manifestations
such as a bleeding diathesis, which
may not be evident at diagnosis. This
accompanying bleeding diathesis
due to thrombocytopenia or other
coagulation defects may be a part of
the syndrome that is not routinely
addressed. Consequently, this may go
unrecognized in these children until
they face hemostatic challenges, which
is not uncommon (given the number
of corrective surgeries performed
for the congenital defects) in this
population leading to unanticipated
surgical bleeding. Counseling for these
families should include discussions
regarding potential spontaneous or
trauma-related bleeding associated
with these syndromes that can
evolve over time. This review aims
to highlight congenital syndromes
where hemostatic defects have been
reported, aid the treating primary care
physician (PCP) to adequately workup
these patients as part of surveillance
or before scheduled procedures
and recommends guidelines for
appropriate and timely referral to the
hematologist.
Achieving hemostasis is a complex
process starting with endothelial
injury that results in platelet plug
formation, which is then strengthened
by deposition of fibrin formed
by the proteolytic coagulation
cascade. Platelets initially attach
to subendothelial collagen and
von Willebrand factor (vWF) via
glycoproteins VI and 1bα (GPVI,
GPIbα). This leads to activation of
platelets releasing Thromboxane
A2 (TxA2) and conforming the
glycoprotein IIb/IIIa (GPIIb/IIIa)
receptor on the platelet surface into
its high affinity state, which now
binds to fibrinogen and vWF. This
further leads to release of platelet
granule contents (fibrinogen, Factor
V, platelet factor 4, Calcium, ADP,
ATP, serotonin, vWF) leading to an
extremely procoagulant surface and
abstractPediatricians provide a medical home for children with congenital
syndromes who often need complex multidisciplinary care. There are
some syndromes associated with thrombocytopenia, inherited platelet
disorders, factor deficiencies, connective tissue disorders, and vascular
abnormalities, which pose a real risk of bleeding in affected children
associated with trauma or surgeries. The risk of bleeding is not often an
obvious feature of the syndrome and not well documented in the literature.
This makes it especially hard for pediatricians who may care for a handful
of children with these rare congenital syndromes in their lifetime. This
review provides an overview of the etiology of bleeding in the different
congenital syndromes along with a concise review of the hematologic
and nonhematologic clinical manifestations. It also highlights the need
and timing of diagnostic evaluation to uncover the bleeding risk in these
syndromes emphasizing a primary care approach.
STATE-OF-THE-ART REVIEW ARTICLEPEDIATRICS Volume 139 , number 2 , February 2017 :e 20154360
To cite: Sarangi SN and Acharya SS. Bleeding
Disorders in Congenital Syndromes. Pediatrics.
2017;139(2):e20154360
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
platelet aggregation. The stage is
now set for the cascade of serine
proteases (factors V, VII, VIII, IX, X,
XI, XII, XIII) activated by the release
of tissue factor, which culminate in
the cleaving of thrombin to form
an insoluble fibrin mesh leading
to a stable clot at the site of injury.
With the many players involved in
coagulation, it can be seen how the
clinical bleeding phenotype can be
modified by gene–gene interactions
by improving or worsening the
integrity of clot formation directly
or indirectly. Therefore, this review
will focus on congenital syndromes
associated with quantitative
(thrombocytopenia) and qualitative
platelet function defects (ie, defects
in platelet generation or defects at 1
or more levels of platelet activation)
and coagulation factor deficiencies.
It will also highlight congenital
syndromes where bleeding can
result from defects in the underlying
connective tissue or anatomic
malformations that increase
predisposition to bleeding. It will
further discuss basic evaluation of
these patients on the basis of a high
index of suspicion and highlight what
phenotypes need specialist referral
for both health maintenance and
prevention of surgical bleeding and
discuss general treatment principles.
Table 1 and Supplemental Tables 5
and 6 summarize the key features of
the congenital syndromes discussed
in this review.
COMMON CONGENITAL SYNDROMES ASSOCIATED WITH A BLEEDING DIATHESIS
Chromosomal Syndromes
A fault in chromosome distribution
during cell division leads to
aneuploidy, which can be associated
with thrombocytopenia but is rarely
severe. Hohlfeld et al 6 in a study of
5194 fetal blood samples (17 to 41
weeks) reported 4.7% samples (247
samples) with thrombocytopenia
(platelet counts <150 000/μL), out
of which 17% (43 samples) were
due to chromosomal anomalies. The
prevalence was 54% in Trisomy
13, 86% in Trisomy 18, 31% in
Turner syndrome, and 6% in
Trisomy 21–Down syndrome (DS).
However, Hord et al 7 reported mild
to moderate thrombocytopenia
(platelet counts 40 000–100 000/
μL) in 28% of neonates with DS. The
exact mechanism is not known, but
is thought to be due to decreased
platelet production, from chronic
fetal hypoxia, which also leads to
intrauterine growth retardation. 8
DS (Trisomy 21) is also associated
with other hematologic findings,
such as polycythemia, neutropenia,
abnormal circulating blasts,
erythroblastosis, and giant platelets. 9
Approximately 10% of neonates with
DS have transient myeloproliferative
disorder, which can present with
isolated thrombocytopenia or
thrombocytosis, leukocytosis, or
persistent peripheral blood blasts.
These abnormal blood cells will self-
resolve in most infants by 3 months
after birth; however, 20% can have
more progressive disease. Both
transient myeloproliferative disorder
and myeloid leukemia associated
with DS (ML-DS), which presents
at 1 to 4 years of age, have somatic
mutations in the megakaryocyte
erythroid transcription factor
GATA-1. 10, 11 ML-DS has a preceding
myelodysplastic phase with patients
presenting with progressive
anemia and thrombocytopenia,
which then develops into leukemia.
DS-associated acute lymphoblastic
leukemia develops after age 4 years,
presenting with cytopenias, and often
lower platelet counts than ML-DS
patients. Therefore, all DS patients
should have a complete blood cell
count at birth and if found to have
any hematologic abnormalities
should be referred to hematology.
Other trisomies such as Trisomy 13
and Trisomy 18 have very distinct
clinical patterns ( Table 1),
and the diagnosis is usually
made soon after birth. Although
survival beyond infancy is rare, life
expectancy is improving. Recognizing
thrombocytopenia is important
because these conditions have
associated cardiac, respiratory, and
craniofacial anomalies that may need
corrective or palliative surgeries.
Surgical planning in these patients
needs a multidisciplinary team with
screening blood work to identify
thrombocytopenia, which if present
will need platelet transfusions pre-
and postoperatively depending upon
the complexity of the surgery guided
by the hematologist.
Turner syndrome (45, X) can
be associated with transient
thrombocytopenia (31% of patients 6)
in the newborn period. Due to the
single functional X chromosome, girls
can inherit X-linked conditions like
hemophilia, but this has only very
rarely been described. 12 Therefore,
prolonged bleeding events warrants
referral to a hematologist for workup.
Gastro-enteral bleeding can occur in
Turner syndrome due to associated
inflammatory bowel disease or
often unrecognized intestinal
telangiectasias (incidence of 7%). 13
DiGeorge syndrome (22q11.2 del)
is the most common micro deletion
syndrome with associated mild
macrothrombocytopenia in 30%
of patients resulting from deletion
of the contiguous GP1BB gene in
the deleted Chromosome 22q11
locus, which codes for the subunit
of the platelet adhesion receptor. 1
Immune dysfunction is common in
these patients and it is estimated
that immune thrombocytopenic
purpura is 200 times more common in
these patients as compared with the
general population. 14, 15 These platelet
abnormalities need to be identified
early on and specifically before
corrective cardiac surgeries. Close
collaboration with a hematologist
before these surgeries will help avert
bleeding complications.
Noonan syndrome is a relatively
common autosomal dominant
2 by guest on July 1, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 139 , number 2 , February 2017
multisystem disorder with
a prevalence of 1 in 1000 to
2500 individuals. Patients with
Noonan syndrome with germ-line
mutations in PTPN11 need to be
monitored for the development
of myeloproliferative disorder or
juvenile myelomonocytic leukemia. 16
Prevalence of bleeding disorders
in Noonan syndrome has been well
described (ranging between 50%
and 89%) if positive bleeding history
or abnormal hemostatic laboratory
values are considered, whereas it
ranges between 10% and 42% if both
history and laboratory values are
considered. 17 – 22 Thrombocytopenia
is not reported as commonly;
however, platelet function defects
are frequent with a prevalence of
27%. 2 Up to 37% of these patients
can have factor XI deficiency while
von Willebrand disease and mixed
factor deficiencies are also reported. 2
Due to the complex phenotype,
a significant proportion of these
patients need surgical procedures.
A reasonable screening process can
begin with obtaining a platelet count,
prothrombin time (PT), activated
partial thromboplastin time (aPTT),
and Factor XI levels at a minimum
even in the absence of bleeding
symptoms and if there is a significant
bleeding history to include platelet
function testing and testing for other
components of the clotting cascade in
consultation with the hematologist.
Connective Tissue Disorders
Easy bruising and bleeding are
prominent manifestations of
heritable collagen disorders
with Ehlers-Danlos syndrome
3
TABLE 1 Features of Congenital Syndromes Associated With Thrombocytopenia
Disorder Incidence Clinical Features Incidence of Thrombocytopenia When to Refer to Hematology
Trisomy 21 1 in 660 Cognitive impairment, hearing
issues, thyroid issues, heart
defects, gastroenteral atresias,
cataracts
7–28%a All patients with any hematologic
abnormalities
Trisomy 13 1 in 5000 Cleft lip and palate, polydactyly,
rocker bottom feet, cutis aplasia,
omphalocele, VSD, PDA, neural
tube defects
54%a (All patients had platelet counts
>100 000/μL)
Platelet count <150 000/μL
Trisomy 18 1 in 5000 Dolichocephaly, micrognathia,
overriding fi ngers, cardiac septal
defects, horse shoe kidney,
psychomotor retardation, feeding
issues
86%a (20% with platelet counts 50 000–
100 000/μL)
Platelet count <150 000/μL
Turner
syndrome
1 in 2500 Coarctation of aorta, aortic stenosis,
short stature, ovarian failure,
horseshoe kidney, cubitus valgus,
low posterior hairline, webbed
neck
31%a (18% with platelet counts 50 000–
100 000/μL)
Platelet count <100 000/μL or between
100 000 and 150 000/μL and needs
surgery
DiGeorge
syndrome
1 in 4000 Typical facies, thymic abnormalities,
hypocalcemia, velopharyngeal
insuffi ciency, conotruncal cardiac
defects, tetralogy of Fallot,
truncus arteriosus, aortic arch
anomalies
30% 1 (Usually mild
macrothrombocytopenia)
Platelet count <150 000/μL and/or
rapidly falling platelet counts in the
context of viral illness should be
referred to rule out ITP
Noonan
syndrome
1 in 1000–2500 Facial dysmorphism, cardiac
anomalies, short stature, bony
and genital anomalies.
6.2% 2 (27% have platelet function defects) Any patient with thrombocytopenia
and all patients before surgery to
evaluate platelet function and other
components of clotting cascade.
Wiskott–Aldrich
syndrome
1 in 4 million Microthrombocytopenia, eczema,
immune defects
Microthrombocytopenia is universal
feature (platelet counts 5000–50 000/
μL) 3
Refer all patients. Also refer to
Immunology.
Cornelia de
Lange
syndrome
1 in 10 000 Growth retardation, synophrys,
limb abnormalities and cognitive
impairment
35% (15/43 patients) with platelet counts
<100 000 4 (16% had ITP with majority
progressing to chronic ITP; 11% had
transient thrombocytopenia)
Check platelet count at diagnosis
and every 5 years if asymptomatic.
Platelet count <100 000 or rapidly
falling platelet count refer to
hematology to rule out ITP
Jacobsen
syndrome
1 in 100 000 Dysmorphogenesis of hands and
feet, frequent cardiac defects and
cognitive impairment
Macrothrombocytopenia (88.5%)
with varying degrees of platelet
function defects (platelets with
giant α granules, storage pool
defects and delayed maturation of
megakaryocytes) 5
Any patient with thrombocytopenia
and all patients before surgery to
evaluate platelet function.
PDA, patent ductus arteriosus; VSD, ventricular septal defect. a Prevalence data from fetal samples (Hohlfeld et al 6).
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
(EDS) being the most prevalent.
Although collagen proteins are
an integral part of capillary
scaffolding, they also contribute
to platelet activation, adhesion,
and aggregation. EDS is a clinically
and genetically heterogeneous
group of conditions with varying
degrees of skin hyperextensibility,
joint hypermobility, delayed
wound healing, and atrophic skin
scarring. There are 5 subtypes with
a combined prevalence rate of 1
in 5000 individuals. Type IV EDS
(vascular type) carries the gravest
prognosis affecting medium and large
sized vessels. It can initially present
as easy bruising and gum bleeding,
but depending on the vessels affected
can have bleeding from every
possible site of the body, including
fatal intraabdominal bleeding. 23 The
other subtypes of EDS manifest with
soft, fragile hyperextensible skin
along with joint dislocations and
bony abnormalities. 23 The diagnosis
is often challenging in children,
especially when there is no family
history and can lead to extensive
hemostasis-related bleeding
workups, which are often normal.
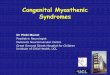
In the office setting, clinicians can
use the Beighton scoring system
( Fig 1) for evaluation of joint
hypermobility and refer patients
with high scores to the geneticist
for further evaluation and
confirmatory genetic testing. 24, 25
Capillary fragility is common among
all subtypes with variable degrees
of platelet function defects and
coagulation factor deficiencies
(factors VIII, IX, XI, XII, and XIII)
being reported. 23 Desmopressin
has been shown to reduce bleeding
risk and postoperative bleeding
in pediatric patients with EDS,
suggesting that a weakened platelet
collagen interaction underlies
the bleeding tendency in EDS. 26
Therefore, individuals with suspected
or confirmed diagnosis of EDS with
any bleeding symptoms or planned
surgical procedures should be
referred to a hematologist.
Abnormalities in Vasculature
Hereditary hemorrhagic
telangiectasia (HHT) or Osler–
Weber–Rendu syndrome is a
common autosomal inherited
disorder with altered defects in
vascular integrity with an incidence
of 1 in 5000 individuals. The
underlying genes ENG, ACVRL1,
SMAD4 encode proteins leading
to elevated expression of vascular
endothelial growth factor. 27 This
leads to characteristic clinical
manifestations of dilated and
tortuous postcapillary venules
(telangiectasias) without intervening
capillaries, which have a higher
propensity to bleed due to inherently
elevated perfusion pressures. In HHT,
telangiectasias can develop in the
nasal mucosa within the first decade
and worsen with age, presenting with
severe and recurrent nosebleeds.
While evaluating significant and
prolonged epistaxis in a pediatric
patient, the PCP should inquire
about bleeding from other sites,
presence of anemia and gastro-
enteral bleeding, and strokes related
to arterio venous malformations
among close family members. It
4
FIGURE 1The Beighton Scoring system for joint hypermobility. Degree of mobility assessed by passive maneuvers in 5 joints. Total score: 0–9. Hypermobility score: ≥5. (Figure reproduced with permission from Arthritis Research UK; http:// www. arthritisresearch uk. org)
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 139 , number 2 , February 2017
might be difficult to make a diagnosis
in childhood as characteristic
telangiectasias are often not present
until later or present as benign-
looking mucocutaneous red spots
that go unnoticed by providers.
The Curacao Criteria ( Table 2) is a
validated scoring system developed
to help elucidate a diagnosis of HHT
as nosebleeds and telangiectasias are
common in the general population. 28, 29
Otorhinolaryngologists should be
consulted early on in a child with
prolonged recurrent nose bleeds to
look for these telangiectasias without
which the diagnosis may be missed
until a later encounter with a life-
threatening bleeding episode.
RARE CONGENITAL SYNDROMES ASSOCIATED WITH A BLEEDING DIATHESIS
Inherited Platelet Disorders
Many of the inherited
thrombocytopenias are clinically
mild and may go unrecognized
unless faced with hemostatic
stressors such as menses, surgery,
trauma, or childbirth. 30 A thorough
bleeding history is a crucial
component in the evaluation of
these patients, including obtaining
previous blood counts if available.
Particularly, time should be devoted
to eliciting the family history with
special attention to hemostatic
stressors, such as menorrhagia,
bleeding after teeth extractions,
blood transfusions after surgery, or
unexplained anemia. Platelet counts
should be determined in family
members with bleeding symptoms.
The pattern of bruising and bleeding
disproportionate to trauma should
raise suspicion for nonaccidental
trauma even in patients in whom
congenital platelet disorders are
suspected. 31 The use of standardized
bleeding assessment tools is very
useful in this setting. The Pediatric
Bleeding Questionnaire identified
high bleeding scores (>96% of
patients) in a cohort of 23 patients
with known inherited platelet
disorders. 32
Supplemental Table 5 outlines
the various features of inherited
thrombocytopenic syndromes. The
underlying molecular defect can be
restricted to platelets alone, or in
some cases can involve other cells
thereby resulting in multisystem
dysfunction. Evaluation of the
patient and the family for presence
of immunodeficiency, hearing loss,
albinism, and renal findings will point
to an underlying syndromic cause of
thrombocytopenia. This is further
complicated by the fact that all
components of the syndrome may not
be present in affected individuals and
therefore a high index of suspicion is
key to their diagnoses. While working
up these patients, it is important
to collect fresh blood samples
with citrate as the anticoagulant
to eliminate the phenomenon
of pseudothrombocytopenia.
Automated platelet counters are not
accurate in the presence of macro
or micro thrombocytopenia and
manual inspection of peripheral
smears under Giemsa or Wright
stain provide important information
regarding platelet number, size, and
granularity. After recognition of
these syndromes, further diagnostic
evaluation of platelet disorders needs
careful preparation (a nontraumatic
blood draw to preserve component
proteins of the coagulation
cascade), specimen handling,
and interpretation and should be
carried out in conjunction with an
experienced hematologist who can
accurately interpret the clinical and
laboratory findings. Although light
transmission aggregometry and
its modification lumiaggregometry
are used for initial screening for
platelet function defects, there are
limitations of standardization and
reproducibility. However, it can
help identify platelet adhesion or
aggregation defects, platelet granule
release defects on the basis of which
further confirmatory testing can be
carried out.
Wiskott–Aldrich syndrome is a
rare autosomal recessive disorder
due to defects in the WASP gene
(Xp 11.22) with an incidence of 4
per million live births. 3 The clinical
features classically include the
triad of microthrombocytopenia
(platelet counts 5000–50 000/
μL) presenting as bruising and
purpura in the neonatal period,
eczema that develops around
infancy and immune defects with
recurrent sinopulmonary infections
in midchildhood. A high index of
suspicion should prompt referral to
a hematologist who may recommend
splenectomy to ameliorate
bleeding symptoms associated with
thrombocytopenia or bone marrow
transplantation, which is usually
curative ( Table 1 and Supplemental
Table 6).
Bone Marrow Failure Syndromes
Thrombocytopenia in inherited
bone marrow failure syndromes
(IBMFS) presents as a component of
progressive marrow failure, which
is the hallmark of these syndromes.
Thrombocytopenia may present in
the neonatal period in congenital
amegakaryocytic thrombocytopenia
and thrombocytopenia with
absent radii (TAR) manifesting
as petechial bleeding and rarely
leading to catastrophic intracranial
5
TABLE 2 The Curacao Diagnostic Criteria for
HHT
Criteria Defi nition
Epistaxis Spontaneous, recurrent
nosebleeds
Telangiectasias Multiple, at characteristic
sites (lips, oral cavity,
fi ngers, nose)
Visceral
involvement
Pulmonary, liver, cerebral,
spinal, or gastrointestinal
vascular malformations
Family history A fi rst-degree relative with
defi nite HHT
Diagnostic criteria
Defi nite HHT 3 or 4 criteria are present
Probable HHT 2 criteria are present
HHT unlikely Only 1 criterion is present
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
hemorrhage. Unlike other IBMFS,
the thrombocytopenia in TAR
improves after infancy and may rise
to levels safe to perform surgery,
suggesting that nonlife-threatening
procedures could be delayed until
after infancy. Fanconi anemia
presents with thrombocytopenia as
the first hematologic manifestation
during midchildhood, whereas in
Shwachman–Diamond syndrome it
appears later, having been preceded
by neutropenia for variable amounts
of time. 33 Supplemental Table 6
outlines the various IBMFS that
have thrombocytopenia as part of
the syndrome. The pathognomonic
physical features can aid in
recognizing the underlying IBMFS,
but it is important to realize that
half of these patients may not be
recognized until adulthood. 34
Chromosomal Disorders
Cornelia De Lange syndrome
(heterozygous mutation of NIPBL
gene) is an autosomal dominant
rare inherited disorder that can
have transient thrombocytopenia
at birth. 35 More recently a higher
incidence of chronic immune
thrombocytopenia (ITP) in these
patients has also been described
(see Table 1). 4 Self-injurious
behavior is often a component of
the syndrome that compounded
with thrombocytopenia can lead
to an increased risk of intracranial
bleeding. It has been proposed to
get platelet counts for these patients
at diagnosis, with any unusual
bleeding symptoms and at 5 yearly
intervals if asymptomatic and refer
to hematology for severe bleeding
symptoms. 4
Jacobsen syndrome (11q
syndrome) is perhaps the most well
described congenital syndrome
with thrombocytopenia that
poses significant morbidity to
affected children. The clinical
phenotype is variable with
macrothrombocytopenia a frequent
(88.5% of patients) feature of the
syndrome and a number of other
platelet abnormalities described,
including platelet function defects
( Table 1). 36 – 38 It is important to
recognize that abnormal platelet
function usually persists despite
resolution of thrombocytopenia in
some patients. Therefore, formal
platelet function testing with a plan
for platelet transfusions are indicated
before major procedures despite
normal platelet counts.5
Other Congenital Disorders
Storage disorders such as Gaucher
disease and Niemann–Pick disease
present with splenomegaly either
due to direct splenic infiltration or
portal hypertension. While caring
for these patients, it is important
to keep in mind that platelets can
pool and sequester inside the
abnormally enlarged spleen, which
can lead to acute life-threatening
thrombocytopenia. Von Gierke
disease (glycogen storage disease 1)
has been shown to have associated
platelet function defects. 39 Once
these disorders are diagnosed, it
would be important to obtain a
baseline platelet count and refer to a
hematologist for bleeding symptoms
or before a surgical procedure
for a comprehensive evaluation
of the bleeding phenotype and
recommendations for surgery.
GENERAL GUIDELINES FOR HEALTH MAINTENANCE AND MANAGEMENT OF BLEEDING SYMPTOMS
Newborn Period
Thrombocytopenia is encountered
fairly commonly (up to 25%
of admitted newborns) in the
NICUs with rates increasing with
prematurity. 40 The challenge lies
in identifying which of these can
stem from an underlying inherited
disorder. Fetal platelets are found in
circulation by ∼5 weeks of gestation
and start reaching adult values by
22 weeks. 41 The diagnostic approach
should be based on the gestational
age, onset of thrombocytopenia (<72
hours indicating likely placental,
perinatal factors; >72 hours
indicating postnatally acquired
infections), and the clinical status
of the newborn (sick versus well
appearing). Karyotype testing should
be done in all obviously dysmorphic
infants with thrombocytopenia.
Inherited causes of thrombocytopenia
are in general rare and rarely
present in the newborn period. If a
clear family history is present, the
hematologist should be consulted
to guide appropriate timing of
confirmatory testing and help
manage thrombocytopenia in
the neonatal period. This should
include a comprehensive delivery
plan with contraindication for
instrumental delivery, vacuum,
or use of fetal scalp monitoring.
Early onset thrombocytopenia
<72 hours, presence of macro-
thrombocytes in the smear, limb
abnormalities, and platelet counts
usually >50 000/ μL are good
clues pointing to an underlying
inherited defect. In the setting of a
well appearing infant with isolated
thrombocytopenia and absence of
any other features, it is reasonable
to treat for immune-mediated causes
of thrombocytopenia (neonatal
alloimmune thrombocytopenia)
until platelet antigen incompatibility
can be demonstrated between
mother and infant serologically.
Most allo or auto antibodies against
neonatal platelets clear from the
circulation over time with platelet
counts normalizing within 1 to 2
weeks in most infants. Persistence
of thrombocytopenia beyond 8 to 12
weeks 42 after birth should warrant a
hematology consult especially in the
absence of any immunologic factors
or genetic syndromes.
Infancy and Beyond
The reader is referred to health
supervision guidelines for various
genetic syndromes, which are a
useful resource for physicians
6 by guest on July 1, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 139 , number 2 , February 2017
involved in the care of these
children. 43 – 46 Periodic hematologic
screening has been recommended
in Noonan syndrome, DS, Turner
syndrome, and Jacobsen syndrome as
outlined in previous sections.
The comprehensive care of children
and adolescents with syndromes
mentioned in this review should
include careful attention to oral
hygiene to prevent gum bleeding,
hormonal control of menstrual
bleeding, and avoidance of
medications such as aspirin and
nonsteroidal anti-inflammatory
analgesics. Dental procedures should
ensure good local hemostasis with
fibrillar collagen products along
7
TABLE 3 Management of Common Bleeding Symptoms With Identifi ed Platelet/Coagulation Defects
Symptom General and Preventive
Measures
Associated With Platelet
Defect
Associated With Coagulation
Factor Defi ciency
Interventions Useful for Severe Symptoms
Epistaxis Place patient in sitting
position with neck forward.
Firmly compress tip of nose
for 20 min.
Local application of
hydrophilic powder such
as NasalCeasea
Local application of
hydrophilic powder such
as NasalCeasea
Bleeding lasting >10 min despite hemostatic
measures, >5 episodes per year: refer
to ENT for electrocauterization, nasal
packing for persistent or profuse
bleeding.
Daily saline nasal lubrication
and humidifi cation of room
air.
Aminocaproic acid 50–100
mg/kg/dose every 6 h
× 7 d
Aminocaproic acid 100 mg/
kg/dose every 6 h × 7 d
HHT patients may need laser ablation or
embolization
Do not: Stick toilet paper,
cotton balls in nose as can
dislodge clot
Desmopressinb intranasal
spray 150 μg/dose: 2
sprays for adult, and 1
spray for <50 kg child
rVIIa (used in Glanzmann thrombasthenia
refractory to platelet transfusions)—
referral to hematology dose: 90 μg/kg
with dose repeated every 2–6 h 3Do not: squeeze bony part of
nose as no blood vessels
here
Oral mucosal
bleeding
(spontaneous)
Ensure good dental hygiene
and periodic dental
cleanings
Oral and/or systemic
aminocaproic acid. Can
use oral swish for 2
min and spit but not as
effective
Oral and/or systemic
aminocaproic acid. Can
use oral swish for 2
min and spit but not as
effective
Platelet and/or blood transfusions as
indicated for platelet defect
Compression with gelatin
sponge
Compression with gelatin
sponge
For coagulopathy: Factor concentrates (FI,
II, VII, VIII, IX, XIII defi ciencies) or FFP or
cryoprecipitat (rich in FVIII, FI, VWF, and
FXIII)
FFP only choice for FV, FXI defi ciencies in the
United States.
Menorrhagia Hormonal regulation Tranexamic acid orally
15–25 mg/kg TID or 10
mg/kg IV TID for serious
bleedingc
Factor concentrates (FI, II,
VII, VIII, IX, XIII defi ciencies)
or FFP or cryoprecipitate
(rich in FVIII, FI, VWF, and
FXIII)
Co-manage with gynecology
Platelet and/or blood
transfusions
FFP only choice for FV, FXI
defi ciencies in the United
States
High dose estrogen therapyc until bleeding
ceases followed by taper and oral
contraception
Blood transfusion Progesterone impregnated intrauterine
devices (eg, Mirenad)
Bruising/minor
lacerations
Protective cushions/pads
as indicated. Rarely if
compromising may need
specifi c treatment
Use of tropical thrombin for oozing and
minor lacerations.
Life-threatening
bleeding (CNS, GI
bleeding)
Avoid contact sports, wear
helmets/protective devices
as indicated in conditions
with severe defi ciencies.
Platelet and/or blood
transfusions
Factor concentrates (FI, II,
VII, VIII, IX, XIII defi ciencies)
or FFP or cryoprecipitate
(rich in FVIII, FI, VWF, and
FXIII)
Refer to hematology to help guide use
of various products like rVIIa and
concentrates
Immediate evaluation to rule
out intracerebral bleeding.
Treat fi rst, image once
stabilized.
FFP only choice for FV, FXI
defi ciencies in the United
States
Blood transfusion
CNS, central nervous system; GI, gastrointestinal; IV, intravenously; TID, 3 times per day.a Catalina Healthcare, Mendon, NY.b Also useful in connective tissue disorders.c Concomitant use of estrogen and tranexamic acid carries a black box warning due to increased risk of thrombosis and if used should be separated by 4 hours.d Bayer Healthcare Pharmaceuticals, Whippany, NJ.
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
with other indicated systemic
hemostatic therapy because of
abundance of fibrinolysis in the
mouth. Children with a high risk of
bleeding should avoid contact sports,
heavy exercise, or isometric exercise
and wear protective pads to avoid
deep hematomas and bruising. 26
Nonweight bearing exercises such as
aqua therapy should be encouraged
to promote a healthy lifestyle. Some
of these children can have restrictive
diets and vitamin K and vitamin C
may need to be supplemented, the
deficiencies of which can aggravate
the underlying bleeding disorder.
Common bleeding symptoms and
their management are addressed in
Table 3.
Antifibrinolytic agents (ε amino
caproic acid and tranexamic acid)
inhibit plasmin activity, thereby
strengthening clot formation and
can be used for prevention of minor
trauma-induced or minor surgical
bleeding especially involving mucosal
surfaces that are rich in fibrinolytic
enzymes in areas such as the mouth,
nose, uterus, and gastrointestinal
tract. Desmopressin (1-deamino-
8-D arginine vasopressin) increases
platelet aggregation by increasing
plasma levels of vWF and factor VIII,
thus improving platelet adhesion
and function. It has been shown
to be useful in various platelet
secretion and granule defects, EDS
and Noonan syndromes, where it
can improve platelet function and
promote hemostasis. 26, 47 – 49 Both
1-deamino-8-D arginine vasopressin
and/or antifibrinolytic agents
can be used as monotherapy or
adjuvant therapies to more definitive
treatment. Hemostasis therapy
should be tailored on the basis of
the underlying hemostatic defect,
severity of bleeding symptoms, or
hemostatic challenge of planned
surgery and results of the bleeding
evaluation. Although platelet
transfusion seems straightforward,
the development of alloantibodies
may cause platelet refractoriness
and therefore should be reserved
for serious bleeding symptoms.
In some cases, judicious and
tailored use of fresh-frozen plasma
(FFP), cryoprecipitate, and rVIIa
may be indicated. The use of
rVIIa is approved in Glanzmann’s
thrombasthenia where it improves
platelet aggregation and fibrin and
thrombin generation.50 Point of care
devices, such as thromboelastogram,
which can quantify global hemostasis
and monitor response to therapeutic
agents, are increasingly being
explored in clinical settings such as
trauma and surgery, 51 which can
provide improved bleed management
and patient outcomes. Further
studies are needed to evaluate
the impact of thromboelastogram
to improve patient outcomes in
bleeding disorders.
GUIDELINES FOR MANAGEMENT BEFORE SURGICAL PROCEDURES
Patients suspected to have a
congenital syndrome with a
bleeding diathesis (symptomatic
or asymptomatic) must have a
sequential evaluation at least 2 to 4
weeks before a scheduled surgical
procedure as proposed in Fig 2.
Bleeding assessment tools are useful
to get a standardized bleeding
history and calculate bleeding scores,
8
FIGURE 2Suggested approach to sequential presurgical evaluation for children with congenital syndromes with known or suspected bleeding diathesis. The laboratory workup should start with an initial screen and a more exhaustive workup can be done in conjunction with the hematologist on the basis of known hemostatic defects for the specifi c congenital syndrome and the bleeding phenotype of the individual patient. aBleeding phenotype: prolonged (>10 min), persistent (>5 episodes/year) nose bleeds, petechiae with minor trauma, bleeding while brushing teeth, heavy menstrual bleeding, prolonged bleeding after tooth eruption or extractions; prolonged bleeding after a procedure requiring a red cell transfusion, >1 cm bruises especially palpable in nature after minor trauma. bHigh risk procedures: craniosynostosis surgery, multiple teeth extraction especially wisdom teeth, plastic or vascular procedures, cardiac procedures, scoliosis surgery, neurosurgery, liver or kidney biopsy. cLow risk procedures: simple dental extraction, bronchoscopy, central venous catheter removal, cutaneous biopsy, GI endoscopy with biopsy, laparoscopic abdominal surgery. dInclude factor XI levels in patients with Noonan syndrome.
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 139 , number 2 , February 2017 9
TABL
E 4
The
Com
pon
ents
an
d S
cori
ng
of t
he
Ped
iatr
ic B
leed
ing
Qu
esti
onn
aire
Sym
pto
m/S
core
–1
01
23
4
Epis
taxi
s—
No
or t
rivi
al (
≤5 p
er y
ear)
>5
per
yea
r or
>10
min
du
rati
on
Con
sult
atio
n o
nly
Pac
kin
g, c
aute
riza
tion
, or
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Cu
tan
eou
s—
No
or t
rivi
al (
≤5 p
er y
ear)
>1
cm a
nd
on
tra
um
aC
onsu
ltat
ion
on
ly—
—
Min
or w
oun
ds
—N
o or
tri
vial
(≤5
per
yea
r)>
5 p
er y
ear
or >
5 m
in
du
rati
on
Con
sult
atio
n o
nly
or
ster
i-
stri
ps
Su
rgic
al h
emos
tasi
s or
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Ora
l cav
ity
—N
oR
epor
ted
at
leas
t on
ceC
onsu
ltat
ion
on
lyS
urg
ical
hem
osta
sis
or
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Gas
troi
nte
stin
al t
ract
—N
oId
enti
fi ed
cau
seC
onsu
ltat
ion
or
spon
tan
eou
s
Su
rgic
al h
emos
tasi
s,
anti
fi b
rin
olyt
ics,
blo
od
tran
sfu
sion
, rep
lace
men
t
ther
apy
or d
esm
opre
ssin
—
Toot
h e
xtra
ctio
nN
o b
leed
ing
in a
t le
ast
2 ex
trac
tion
s
Non
e d
one
or n
o b
leed
ing
in 1
ext
ract
ion
Rep
orte
d, n
o co
nsu
ltat
ion
Con
sult
atio
n o
nly
Res
utu
rin
g, r
epac
kin
g, o
r
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Su
rger
yN
o b
leed
ing
in a
t le
ast
2 su
rger
ies
Non
e d
one
or n
o b
leed
ing
in 1
Rep
orte
d, n
o co
nsu
ltat
ion
Con
sult
atio
n o
nly
Su
rgic
al h
emos
tasi
s or
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Men
orrh
agia
—N
oR
epor
ted
or
con
sult
atio
n
only
Anti
fi b
rin
olyt
ics
or
con
trac
epti
ve p
ill u
se
D&
C o
r ir
on t
her
apy
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
des
mop
ress
in, o
r
hys
tere
ctom
y
Pos
tpar
tum
No
ble
edin
g in
at
leas
t
2 d
eliv
erie
s
No
del
iver
ies
or n
o
ble
edin
g in
1 d
eliv
ery
Rep
orte
d o
r co
nsu
ltat
ion
only
D&
C, i
ron
th
erap
y or
anti
fi b
rin
olyt
ics
Blo
od t
ran
sfu
sion
,
rep
lace
men
t th
erap
y, o
r
des
mop
ress
in
—
Mu
scle
hem
atom
a—
Nev
erP
ostt
rau
ma,
no
ther
apy
Sp
onta
neo
us,
no
ther
apy
Sp
onta
neo
us
or t
rau
mat
ic,
req
uir
ing
rep
lace
men
t
ther
apy
or d
esm
opre
ssin
Sp
onta
neo
us
or t
rau
mat
ic r
equ
irin
g
surg
ical
inte
rven
tion
or
blo
od
tran
sfu
sion
Hem
arth
rosi
s—
Nev
erP
ostt
rau
ma,
no
ther
apy
Sp
onta
neo
us,
no
ther
apy
Sp
onta
neo
us
or t
rau
mat
ic,
req
uir
ing
rep
lace
men
t
ther
apy
or d
esm
opre
ssin
Sp
onta
neo
us
or t
rau
mat
ic r
equ
irin
g
surg
ical
inte
rven
tion
or
blo
od
tran
sfu
sion
Cen
tral
ner
vou
s sy
stem
—N
ever
——
Su
bd
ura
l, an
y in
terv
enti
onIn
trac
ereb
ral,
any
inte
rven
tion
Oth
era
—N
oR
epor
ted
Con
sult
atio
n o
nly
Su
rgic
al h
emos
tasi
s,
anti
fi b
rin
olyt
ics
or ir
on
ther
apy
Blo
od t
ran
sfu
sion
, rep
lace
men
t
ther
apy,
or
des
mop
ress
in
Rep
rin
ted
wit
h p
erm
issi
on f
rom
Bow
man
M, R
idd
el J
, Ran
d M
L, T
oset
to A
, Silv
a M
, Jam
es P
D. E
valu
atio
n o
f th
e d
iagn
osti
c u
tilit
y fo
r vo
n W
illeb
ran
d d
isea
se o
f a
ped
iatr
ic b
leed
ing
qu
esti
onn
aire
. J T
hro
mb
Ha
emos
t. 2
009;
7(8)
: Tab
le S
1. —
, sco
re n
ot
avai
lab
le f
or t
his
par
ticu
lar
syst
em.
a In
clu
des
pos
tcir
cum
cisi
on, u
mb
ilica
l stu
mp
, cep
hal
hem
atom
a, m
acro
scop
ic h
emat
uri
a, p
ostv
enip
un
ctu
re, a
nd
con
jun
ctiv
al h
emor
rhag
e.
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
which can help recognize individual
bleeding risk. The components of the
Pediatric Bleeding Questionnaire are
presented in Table 4 for review. 52
A thorough head to toe physical
examination to identify and uncover
bleeding risk should focus on
hyperextensibility, telangiectasias,
palpable bruises, splenomegaly,
ecchymoses, and petechiae. All
medications and alternative therapies
(including herbal preparations)
should be carefully reviewed, and
any medications known to affect
hemostasis should be discontinued or
substituted. A basic workup should
include a complete blood count,
PT, and aPTT with mixing studies
(when PT/aPTT are prolonged),
which helps distinguish a clotting
factor deficiency from nonspecific
coagulation inhibitors. In syndromes
with known qualitative platelet
defects, platelet function analysis
(PFA-100), which has replaced the
bleeding time, should be included as
part of the initial workup if available.
Further testing should be guided by
a pediatric hematologist who can
then order confirmatory testing.
Knowledge of the underlying platelet
abnormality can guide further
platelet function testing because the
use of specific platelet agonists can
limit the amount of blood drawn in
pediatric patients. A multidisciplinary
team involving the surgeon,
hematologist, and anesthesiologist
should tailor a treatment plan before
surgery for these patients with the
judicious use of platelets and other
blood components to avoid allo-
immunization especially because
patients with clinical syndromes
may require more than 1 corrective
procedure. The risk of bleeding due
to any underlying thrombocytopenia
in part depends upon the nature
of the surgery, critical need
for maintaining postoperative
hemostasis and promoting healing,
and individualized target platelet
count depending upon the type
of surgery. Regional anesthesia
and epidural catheters may be
contraindicated depending on the
level of thrombocytopenia and other
hemostatic defects.
CONCLUSIONS
Abnormalities in hemostasis
leading to clinical bleeding are an
often unidentified component of
many congenital syndromes. These
abnormalities are important for the
PCP to recognize and anticipate,
thereby prompting timely referral
to the hematologist to adequately
manage these patients to prevent
catastrophic bleeding.
ABBREVIATIONS
aPTT: activated partial thrombo-
plastin time
DS: Down syndrome
EDS: Ehlers-Danlos syndrome
FFP: fresh-frozen plasma
HHT: hereditary hemorrhagic
telangiectasia
IBMFS: inherited bone marrow
failure syndromes
ITP: immune thrombocytopenia
ML-DS: myeloid leukemia associ-
ated with Down
syndrome
PCP: primary care physician
PT: prothrombin time
TAR: thrombocytopenia with
absent radii
vWF: von Willebrand factor
REFERENCES
1. Budarf ML, Konkle BA, Ludlow LB,
et al. Identifi cation of a patient with
Bernard-Soulier syndrome and a
deletion in the DiGeorge/velo-cardio-
facial chromosomal region in 22q11.2.
Hum Mol Genet. 1995;4(4):763–766
2. Briggs BJ, Dickerman JD. Bleeding
disorders in Noonan syndrome. Pediatr
Blood Cancer. 2012;58(2):167–172
3. Bolton-Maggs PHB, Chalmers EA,
Collins PW, et al; UKHCDO. A review
of inherited platelet disorders with
guidelines for their management on
behalf of the UKHCDO. Br J Haematol.
2006;135(5):603–633
4. Lambert MP, Jackson LG, Clark D,
Kaur M, Krantz ID, Deardorff MA.
The incidence of thrombocytopenia
in children with Cornelia de Lange
syndrome. Am J Med Genet A.
2011;155A(1):33–37
5. Mattina T, Perrotta CS, Grossfeld P.
Jacobsen syndrome. Orphanet J Rare
Dis. 2009;4:9
6. Hohlfeld P, Forestier F, Kaplan C, Tissot
JD, Daffos F. Fetal thrombocytopenia:
a retrospective survey of 5, 194
fetal blood samplings. Blood.
1994;84(6):1851–1856
7. Hord JD, Gay JC, Whitlock JA.
Thrombocytopenia in neonates with
trisomy 21. Arch Pediatr Adolesc Med.
1995;149(7):824–825
8. Watts TL, Roberts IAG. Haematological
abnormalities in the growth-restricted
infant. Semin Neonatol. 1999;4:41–54
9. Webb D, Roberts I, Vyas P. Haematology
of Down syndrome. Arch Dis Child
Fetal Neonatal Ed. 2007;92(6):
F503–F507
10. Lange BJ, Kobrinsky N, Barnard
DR, et al. Distinctive demography,
biology, and outcome of acute myeloid
leukemia and myelodysplastic
syndrome in children with Down
syndrome: Children’s Cancer Group
Studies 2861 and 2891. Blood.
1998;91(2):608–615
11. Rainis L, Bercovich D, Strehl S, et al.
Mutations in exon 2 of GATA1 are early
events in megakaryocytic malignancies
associated with trisomy 21. Blood.
2003;102(3):981–986
12. Panarello C, Acquila M, Caprino
D, Gimelli G, Pecorara M, Mori PG.
Concomitant Turner syndrome
and hemophilia A in a female with
an idic(X)(p11) heterozygous at
locus DXS52. Cytogenet Cell Genet.
1992;59(4):241–242
13. Eroglu Y, Emerick KM, Chou PM,
Reynolds M. Gastrointestinal bleeding
in Turner’s syndrome: a case report
and literature review. J Pediatr
Gastroenterol Nutr. 2002;35(1):84–87
14. Akar NA, Adekile AD. Chromosome
22q11.2 deletion presenting with
immune-mediated cytopenias,
macrothrombocytopenia and platelet
dysfunction. Med Princ Pract.
2007;16(4):318–320
10 by guest on July 1, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 139 , number 2 , February 2017
15. Liang HP, Morel-Kopp MC, Curtin
J, et al. Heterozygous loss of
platelet glycoprotein (GP) Ib-V-IX
variably affects platelet function
in velocardiofacial syndrome
(VCFS) patients. Thromb Haemost.
2007;98(6):1298–1308
16. Strullu M, Caye A, Lachenaud J, et al.
Juvenile myelomonocytic leukaemia
and Noonan syndrome. J Med Genet.
2014;51(10):689–697
17. de Haan M, vd Kamp JJ, Briët E,
Dubbeldam J. Noonan syndrome:
partial factor XI defi ciency. Am J Med
Genet. 1988;29(2):277–282
18. Sharland M, Burch M, McKenna
WM, Paton MA. A clinical study of
Noonan syndrome. Arch Dis Child.
1992;67(2):178–183
19. Massarano AA, Wood A, Tait RC,
Stevens R, Super M. Noonan syndrome:
coagulation and clinical aspects. Acta
Paediatr. 1996;85(10):1181–1185
20. Sharland M, Patton MA, Talbot S,
Chitolie A, Bevan DH. Coagulation-factor
defi ciencies and abnormal bleeding
in Noonan’s syndrome. Lancet.
1992;339(8784):19–21
21. Bertola DR, Carneiro JDA, D’Amico EA,
et al. Hematological fi ndings in Noonan
syndrome. Rev Hosp Clin Fac Med Sao
Paulo. 2003;58(1):5–8
22. Sharland M, Patton M, Chittolie A,
et al. Coagulation factor abnormalities
in Noonan syndrome. J Med Genet.
1990;27:646
23. De Paepe A, Malfait F. Bleeding and
bruising in patients with Ehlers-
Danlos syndrome and other collagen
vascular disorders. Br J Haematol.
2004;127(5):491–500
24. O’Brien SH. An update on pediatric
bleeding disorders: bleeding scores,
benign joint hypermobility, and platelet
function testing in the evaluation of the
child with bleeding symptoms. Am J
Hematol. 2012;87(suppl 1):S40–S44
25. Beighton P, Solomon L, Soskolne
CL. Articular mobility in an African
population. Ann Rheum Dis.
1973;32(5):413–418
26. Shovlin CL, Nunes ME, Ruymann
FB, et al. Hereditary haemorrhagic
telangiectasia: pathophysiology,
diagnosis and treatment. Blood Rev.
2010;24(6):203–219
27. Shovlin CL. Hereditary haemorrhagic
telangiectasia: pathophysiology,
diagnosis and treatment. Blood Rev.
2010;24(6):203–219
28. Shovlin CL, Guttmacher AE, Buscarini E,
et al. Diagnostic criteria for hereditary
hemorrhagic telangiectasia (Rendu-
Osler-Weber syndrome). Am J Med
Genet. 2000;91(1):66–67
29. Van Gent MWF, Post MC, Mager JJ,
et al. Diagnostic Curacao Criteria for
HHT; are they still valid? Hematology
Meeting Rep. 2009;3(4):13
30. Drachman JG. Inherited
thrombocytopenia: when a low platelet
count does not mean ITP. Blood.
2004;103(2):390–398
31. Carpenter SL, Abshire TC, Anderst JD;
Section on Hematology/Oncology and
Committee on Child Abuse and Neglect
of the American Academy of Pediatrics.
Evaluating for suspected child abuse:
conditions that predispose to bleeding.
Pediatrics. 2013;131(4). Available at:
www. pediatrics. org/ cgi/ content/ full/
131/ 4/ e1357
32. Biss TT, Blanchette VS, Clark DS,
Wakefi eld CD, James PD, Rand ML.
Use of a quantitative pediatric
bleeding questionnaire to assess
mucocutaneous bleeding symptoms
in children with a platelet function
disorder. J Thromb Haemost.
2010;8(6):1416–1419
33. Alter BP. Inherited bone marrow failure
syndromes. In: Nathan DG, Orkin SH,
Ginsburg D, Loot AT, eds. Nathan and
Oski’s Hematology of Infancy and
Childhood. Vol. 1. 6th ed. Philadelphia,
PA: WB Saunders; 2003:281–365
34. Alter BP. Diagnosis, genetics,
and management of inherited
bone marrow failure syndromes.
Hematology (Am Soc Hematol Educ
Program). 2007;1:29–39
35. Fryns JP, Vinken L. Thrombocytopenia
in the Brachmann-de Lange syndrome.
Am J Med Genet. 1994;49(3):360
36. Gangarossa S, Schiliró G,
Mattina T, Scardilli S, Mollica F,
Cavallari V. Dysmegakaryopoietic
thrombocytopenia in patients with
distal chromosome 11q deletion.
Blood. 1996;87(11):4915–4916
37. Breton-Gorius J, Favier R,
Guichard J, et al. A new
congenital dysmegakaryopoietic
thrombocytopenia (Paris-Trousseau)
associated with giant platelet alpha-
granules and chromosome 11 deletion
at 11q23. Blood. 1995;85(7):1805–1814
38. White JG. Platelet storage pool
defi ciency in Jacobsen syndrome.
Platelets. 2007;18(7):522–527
39. Czapek EE, Deykin D, Salzman EW.
Platelet dysfunction in glycogen
storage disease type I. Blood.
1973;41(2):235–247
40. Roberts I, Stanworth S, Murray NA.
Thrombocytopenia in the neonate.
Blood Rev. 2008;22(4):173–186
41. Sola-Visner M. Platelets in the neonatal
period: developmental differences
in platelet production, function,
and hemostasis and the potential
impact of therapies. Hematology
(Am Soc Hematol Educ Program).
2012;2012:506–511
42. Chakravorty S, Roberts I. How I
manage neonatal thrombocytopenia.
Br J Haematol. 2012;156(2):155–162
43. Bull MJ; Committee on Genetics.
Health supervision for children
with Down syndrome. Pediatrics.
2011;128(2):393–406
44. Frías JL, Davenport ML; Committee on
Genetics and Section on Endocrinology.
Health supervision for children
with Turner syndrome. Pediatrics.
2003;111(3):692–702
45. Romano AA, Allanson JE, Dahlgren
J, et al. Noonan syndrome:
clinical features, diagnosis, and
management guidelines. Pediatrics.
2010;126(4):746–759
46. Bassett AS, McDonald-McGinn DM,
Devriendt K, et al; International 22q11.2
Deletion Syndrome Consortium. Practical
guidelines for managing patients with
22q11.2 deletion syndrome. J Pediatr.
2011;159(2):332–9.e1
47. Stine KC, Becton DL. DDAVP therapy
controls bleeding in Ehlers-Danlos
syndrome. J Pediatr Hematol Oncol.
1997;19(2):156–158
48. Grange CS, Heid R, Lucas SB, Ross
PL, Douglas MJ. Anaesthesia in a
parturient with Noonan’s syndrome.
Can J Anaesth. 1998;45(4):332–336
49. Nurden AT, Freson K, Seligsohn
U. Inherited platelet disorders.
11 by guest on July 1, 2020www.aappublications.org/newsDownloaded from

SARANGI and ACHARYA
Haemophilia. 2012;18(4 suppl
4):154–160
50. Rajpurkar M, Chitlur M, Recht M,
Cooper DL. Use of recombinant
activated factor VII in patients with
Glanzmann’s thrombasthenia: a
review of the literature. Haemophilia.
2014;20(4):464–471
51. Jeger V, Zimmermann H, Exadaktylos
AK. The role of thrombelastography
in multiple trauma. Emerg Med Int.
2011;2011:895674
52. Bowman M, Riddel J, Rand ML, Tosetto
A, Silva M, James PD. Evaluation of the
diagnostic utility for von Willebrand
disease of a pediatric bleeding
questionnaire. J Thromb Haemost.
2009;7(8):1418–1421
12 by guest on July 1, 2020www.aappublications.org/newsDownloaded from

originally published online January 6, 2017; Pediatrics Susmita N. Sarangi and Suchitra S. Acharya
Bleeding Disorders in Congenital Syndromes
ServicesUpdated Information &
015-4360http://pediatrics.aappublications.org/content/early/2017/01/04/peds.2including high resolution figures, can be found at:
References
015-4360#BIBLhttp://pediatrics.aappublications.org/content/early/2017/01/04/peds.2This article cites 52 articles, 15 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/blood_disorders_subBlood Disorderssubhttp://www.aappublications.org/cgi/collection/hematology:oncology_Hematology/Oncologyg_-_development_subhttp://www.aappublications.org/cgi/collection/practice-based_learninPractice-Based Learning & Development_management_subhttp://www.aappublications.org/cgi/collection/administration:practiceAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 1, 2020www.aappublications.org/newsDownloaded from

originally published online January 6, 2017; Pediatrics Susmita N. Sarangi and Suchitra S. Acharya
Bleeding Disorders in Congenital Syndromes
http://pediatrics.aappublications.org/content/early/2017/01/04/peds.2015-4360located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2017/01/04/peds.2015-4360.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2017has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 1, 2020www.aappublications.org/newsDownloaded from