Embed Size (px)
Citation preview

[CANCER RESEARCH 49, 3759-3764. July 15. 1989|
Blood Flow, Metabolism, Cellular Microenvironment, and Growth Rate of HumanTumor Xenografts1
F. Kallinowski,2 K. H. Schlenger, S. Runkel, M. Kloes, M. Stohrer, P. Okunieff, and P. Vaupel
Department of Radiation Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 02114 [F. K., P. O., P. V.], and Department ofApplied Physiology, University of Mainz, D-6500 Mainz, Federal Republic of Germany [K. H. S., S. R., M. K., M. S.J
ABSTRACT
Better understanding of the micromilieu of human tumors in situ ismandatory for further improvement of diagnostic and therapeutic interventions. Since investigations of untreated tumors of a wide size rangeare precluded in humans for ethical reasons, size-dependent changes inthe pathophysiology of primary and metastatic human tumors werestudied using "tissue-isolated" xenografts in nude rats. Tumor types
included lung and breast cancers, ovarian and thyroid carcinomas, uterustumors, and melanomas. A 10-fold variation in weight-adjusted tumorperfusion indicated large variations in angiogenesis which were unrelatedto tumor type. Flow values obtained were consistent with data fromclinical observations and were comparable to that in isografted rodenttumors. Using actual consumption and supply rates, maximum oxygenand glucose uptake rates were calculated for each tumor type. Thecapacity to consume oxygen and glucose varied 9-fold and 4-fold, respectively. However, considering actual consumption rates, blood flow wasthe principal modulator of substrate supply and tumor metabolism inthese human tumor xenografts. Consequently, therapeutically relevantparameters of the metabolic micromilieu largely depended on the efficacyof the tumor circulation. Hereby, high metabolic rates concomitant withhigh flow values coincided with rapid tumor growth. Thus, in order todesign the best individualized therapy, flow-related data should supplement histological classification and clinical staging and grading. Furtherdevelopment of relatively noninvasive technologies (magnetic resonanceimaging, magnetic resonance spectroscopy, or positron emission tomography) might permit such monitoring.
INTRODUCTION
During malignant transformation, genomic changes occur (1,2). As a consequence, the enzymology of cancer cells is altered(3, 4), and inherent resistance to radiation and chemotherapycan increase (5, 6). In vitro, gene expression, growth factorresponse, nutrient supply, cellular proliferation, and treatmentsensitivity are interrelated (7-9).
In vivo, growth of solid tumors requires the formation of newblood vessels (10). It has not yet been conclusively shownwhether or not oncogenesis and angiogenesis are linked (11).Several angiogenic factors, produced by tumor or immune cells,mediate the process of neovascularization (12).
Considering isotransplanted rodent tumors, it is well established that the efficiency of the new vascular network, andconsequently of microcirculation, governs nutritive tumor perfusion (13-15). Within one tumor line, a flow decline per unitweight during growth can lead to the development of hypoxia,acidosis, and substrate depletion in tumor microareas, whichcan markedly alter the tumor response to nonsurgical treatmentmodalities (16-18). Such microareas are heterogeneously distributed within individual tumors due to an anisotropic flowdistribution (13-15).
Received 12/21/88; revised 3/13/89; accepted 4/5/89.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Financial support from the "Gesellschaft der Goenner und Foerderer derGrundlagenforschung des Krebses" (Mainz. FRG) is gratefully acknowledged.
2To whom requests for reprints should be addressed, at Institute of Physiologyand Pathophysiology. University of Mainz, Duesbergweg 6. D-6500 Mainz.Federal Republic of Germany.
Data on primary or metastatic tumors in patients are inconclusive. Repeated investigation of such tumors at differentgrowth stages is usually impossible due to the need for immediate therapeutic intervention. In order to bridge the gap, weinvestigated therapeutically relevant pathophysiological properties of various xenografted human tumors.
MATERIALS AND METHODS
Animals and Tumors. Different primary or metastatic human tumorswere investigated (6 breast cancers, 1 lung cancer, 2 ovarian carcinomas,2 uterine tumors, 2 thyroid cancers, 2 malignant melanomas). Tumortissue was xenografted into athymic mice (NMRI-nu/ni/) without prioradaptation to culture conditions. Details of the breeding and maintenance of immunodeficient rodents were described previously (19). Afterat least four mouse passages, tumors from this "bank" were trans
planted into athymic, T-cell-deficient (WAG/Fra-rnu/rnu) rats. Tissuewas grown either s.c. in the flank or as "tissue-isolated" tumor prepa
rations in the groin (implantation technique described in Refs. 20 and21). In addition, DS-carcinosarcomas in Sprague-Dawley rats werestudied in order to allow a comparison of the results obtained withthose previously reported on isotransplanted rodent tumors.
Tumor Perfusion and Substrate Turnover. The "tissue-isolated" tu
mors were supplied by a single artery and drained by one vein and thuspermitted the measurement of global tumor blood flow, oxygen consumption, glucose uptake, and lactate release. The techniques used havebeen described previously (21, 22). In brief, cannulas were inserted intothe right jugular vein, the left carotid artery, and the tumor-drainingvein after the animals were anesthetized (sodium pentobarbital, Nem-butal; Ceva, Paris; 35 mg/kg i.p.). Total tumor blood flow was measuredby timed collection of the tumor venous outflow. Arterial and tumorvenous blood samples were obtained, and relevant parameters of therespiratory gas exchange were determined (O2 and CO2 tensions, pH,oxyhemoglobin saturation, hematocrit, hemoglobin concentration).From these data, the O2 content of the blood samples was calculatedassuming maximal oxygen binding by hemoglobin, oxygen dissociationcurves as given by Bork et al. (23) and a constant oxygen solubilitycoefficient as reported by Zander (24). Glucose and lactate concentrations were determined enzymatically. From these data, the respectiveuptake or release rates could be calculated taking into account theactual tumor perfusion rate and the relevant concentration differencesbetween arterial and tumor venous blood. Blood loss due to samplingwas adequately replaced by fresh donor blood. During the experiments,relevant systemic parameters, such as arterial blood pressure, acid-basestatus, and rectal temperature, were monitored.
Measurement of Tumor Tissue Oxygénation.pO2 measurements wereperformed in s.c. tumors with steel-sheathed O2-sensitive needle electrodes (recessed gold-in-glass electrode; outer diameter, 350 MITI;diameter of the cathode, 12 ^m). The electrode was moved through thetissue in steps of 1 mm. The forward motion was immediately followedby a backward step of 0.3 mm in order to relieve tissue pressure. Thelocal oxygen partial pressures were measured l s after the backwardmotion (KIMOC 6650, Sigma pO2 histograph; Eppendorf, Hamburg,Federal Republic of Germany). Several tracks were performed in eachtumor recording a total of 60-120 pO2 values. For comparison, pO2data were also determined in rat liver. Mean arterial blood pressure,rectal temperature, and relevant arterial blood gas parameters weremonitored throughout the experiments.
Theoretical Analysis. From all parameters investigated, descriptivestatistical parameters were calculated. Mean values and standard errors
3759
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN TUMOR XENOGRAFTS
are given in the text if not indicated otherwise. Differences betweengroups were assessed for statistical significance using the Kruskal-Wallis // test, the t test for paired and unpaired observations, and theMann-Whitney U test. Perfusion-related changes were statistically evaluated using least square routines for multiple analysis of variance withinthe framework of general linear models (general linear model procedure,SAS; SAS Institute, Cary, NC). Maximal oxygen and glucose consumption values were estimated with a nonlinear maximum likelihoodleast-squares routine assuming optimum supply conditions (22).
RESULTS
Tumor Perfusion and Metabolism. A total of 294 "tissue-isolated" preparations of the various tumor lines were investi
gated. The xenografts of various tumors types exhibited verydifferent growth properties, reaching tumor sizes between 0.3and 14.6 g after growth periods up to 6 weeks. Perfusion valuesand metabolic rates varied considerably both within and inbetween different tumor lines. In all tumors, blood flow perunit weight was higher in small transplants than at advancedgrowth stages (as an example, see ovarian cancers in Fig. 1,top). The most pronounced flow decline already occurred beforegross tissue necrosis was noted. At relatively constant arterialsubstrate concentrations, the oxygen and glucose supply wasmostly determined by tumor perfusion. The oxygen consumption and glucose uptake rates generally followed the changes inthe respective availabilities. Therefore, the decline of the oxygenconsumption (Fig. 1, top) and glucose uptake with increasing
10
-,*
o.l
0.0110
0.1
0.0 0.5
Glucose uptake(umol/g/min;
100 cË
10
o
</)
ol¡a>D)
0.1 10 100
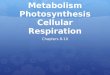
Tumor wet weight (g)Fig. 1. Blood flow and substrale turnover of xenografted ovarian cancers. Top
and bottom, blood flow (•),oxygen consumption ( I ,,.. D), and glucose uptake(Vtt, *) of 48 human ovarian cancer xenografts at various tumor wet weights.Inset, láclaterelease (V,,, O) of the same xenografts as a function of the glucoseuptake. Each data point represents an individual tumor xenograft. Regressionsare: log tumor blood flow = -0.808 log tumor wet weight - 0.436. r - 0.79. P <q.OOUlog KJ; = -0.570 log tumor wet weight - 1.153, r = 0.65, P < 0.001; logy,, = -0.523 log tumor wet weight - 0.462, r = 0.64, P < 0.00 1; log F,. = 0.977log C„+ 0.108. r =0.72, />< 0.001.
tumor sizes almost paralleled the reduction in tumor perfusion(Fig. 1, bottom). Láclaterelease was mainly determined by theamount of glucose taken up (Fig. 1, inset). From these series ofexperiments, it can be concluded that, within tumors of thesame cell line, tumor size is the primary determinant of tumorblood flow per unit weight at constant arterial blood pressure.Metabolic functions mainly depend on the substrate supply ata given tumor size, which, in turn, is governed by tumorperfusion.
Since tumor size greatly influenced weight-related tumorperfusion and metabolic functions, xenografts from differentcell lines but of similar volumes were compared. The resultspresented hold qualitatively true for every tumor weight. Relevant statistical parameters for tumor masses around 2.5 g aregiven in Table 1.
Considering only tumors of comparable sizes, tumor perfusion varied markedly. The most pronounced variations wereobserved in smaller tumors (wet weights, <2 g) with 10-foldflow differences between the various tumor lines.
Similar to the finding in a single tumor cell line, tumorperfusion was the principal modulator of supply and consumption both of oxygen and glucose (tumor masses, about 2.5 g,i.e., 1% of body weight; Fig. 2, A and E). The amount of oxygenand glucose consumed by various tumors of identical volumeswas largely governed by the substrate availability, which, inturn, was limited by tumor blood flow. Again, lactate releasefrom a variety of human tumor xenografts (about 2.5 g) correlated well with glucose consumption (lactate release = 1.545 *glucose uptake - 0.040, r = 0.888, P < 0.001). Since glucoseconsumption was governed by tumor blood flow, lactate releaseincreased as a function of tumor perfusion (Fig. 2C). In thisstudy, tumor venous pH values close to arterial levels wereobserved in highly perfused tumors despite high lactate releaserates (ApH 0.11; Fig. 2Q. At perfusion rates <0.2 ml/g/min,tumor venous blood was acidified, and pH values as low as 7.1occurred (Fig. 1C). The probability of no overall effect of thecell line on blood flow, oxygen consumption, glucose uptake,lactate release, and tumor venous pH values of different tumorsat identical wet weights was <0.0001 using Wilks', Pillai's,Hostelling-Lawley's, and Roy's criterion. Considering tumor
proliferation, high blood flow rates coincided with rapid growth,whereas low perfusion values were found in tumors with relatively long growth periods (Fig. ID).
The oxygen and glucose uptake values, measured over widesupply ranges, were fitted to a hyperbolic function (22) in orderto gain further insight into intrinsic metabolic properties ofhuman tumor tissue in vivo. The curves were characterized bythe maximum oxygen and glucose uptake at optimum supplyrates (i.e., the respiratory and glycolytic capacities) and by theoxygen and glucose supply at half-maximal substrate uptake.In order to separate tumors with clearly different pathophysi-ological properties, medullary breast cancers with high and lowperfusion rates were considered separately. The estimated consumption values within the supply range investigated are shownin Figs. 3 and 4. It is obvious that the respiratory capacitiesvaried 9-fold (P < 0.001), whereas the glycolytic capacitiesdiffered only 4-fold (value not significant). The substrate availabilities at half-maximal consumption rates were significantlydifferent for both oxygen and glucose (P < 0.001). The respiratory and glycolytic capacities were very high reflecting therelatively rapid growth rates of the tumors investigated. It wasfound that the capacity of human tumor xenografts to consumesubstrates was unrelated to their actual perfusion rates in situ,i.e., tumors with high or low blood flow do not necessarily
3760
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN TUMOR XENOGRAFTS
Table l Growth, perfusion, and metabolism ofxenografled human tumors"
TumortypeNo.
oftransplantsTumorgrowthperiod(days)Tumor
bloodflow(/il/g/min)Oxygen
supply(n\02/g/min)Oxygen
consumption(fi\Oi/g/min)OxygenutilizationGlucose
supply(^mol/g/min)Glucose
consumption(ÿmol/g/min)Glucose
utilizationLáclate
release(^mol/g/min)Arterial
pHTumorvenouspHNo.
of transplantsBreastcarcinoma831
+172
±1811.3
±3.74.5+
1.539
±70.65
+0.230.25
+0.0936
+40.24
+0.067.40
±0.027.14±0.03Thyroidcarcinoma519
±3242±7644.8±14.310.8+3.126+51.33+0.380.19
±0.0918+70.44+0.157.42±0.037.29+ 0.02Breastcarcinoma1227
±187
±2215.9
+3.97.1
±1.352
+50.78
±0.160.26
±0.0438
+40.35
+0.077.32
±0.027.10+0.04Melanoma98±
1289±6252.2±9.317.8+3.636
±41.73±0.370.37
±0.0821+20.48
±0.097.47+0.017.37±0.01Breastcarcinoma334
±1143
±3825.6
+7.58.3
+3.630
+40.81
±0.260.22
+0.0529
±50.39
±0.157.41
±0.037.27±0.03Uterinesarcoma423
±5304+11951.3
±19.412.4±5.123
±21.54±0.400.29
±0.1020±20.71±0.157.40
+0.017.28±0.02Breastcarcinoma1033
+1145
+3520.9
±5.26.9+
1.440
±51.22
+0.210.43
±0.0938
±30.35
±0.097.35
±0.017.16±0.02Uterinecarcinoma1021
±2309+7352.5+
11.110.1±1.030
±61.85±0.470.26
±0.0318±30.42
+0.097.39+0.027.28±0.02Breastcarcinoma935+
1156
+2625.7
±4.611.8
±2.646
±61.21
+0.230.43
+0.1134
±50.34
±0.127.32
±0.037.14±0.04Thyroidcarcinoma515
±1552±168106.2+32.520.2±7.322
±53.12±0.890.55
±0.0923±40.66
±0.137.46±0.017.37+ 0.02Ovariancarcinoma935
+1179
+4630.8
±7.611.3
+2.343
+71.19
+0.260.25
±0.0725
+40.26
±0.067.41
±0.027.28±0.02Lungcarcinoma118±
1573+6894.8±12.023.0±6.328
±63.31±0.380.78±0.0726
±31.13±O.IO7.44
±0.027.35±0.03Ovariancarcinoma225
±1214
+5240.3
±9.39.4+
1.424
+31.05
±0.290.23
±0.0323
+40.32
±0.027.43
±0.027.35±0.01Breastcarcinoma108+
1578±25286.8+
11.024.1+3.129+33.21±0.530.71
±0.1124±31.03±0.147.44±0.017.32
+ 0.02Melanoma319+
1233
±3242.9
±6.415.7
+5.135
±81.43
±0.230.31
±0.0423
+30.52
±0.037.45
±0.017.32±0.01Rattumor*1010+
1539±9891.5±18.024.4±4.830+32.82+0.520.85+0.1434+31.57+0.257.42+0.017.27±0.02
" Tumor sizes around 2.5 g; values are means ±SE.* Rat tumor (DS-carcinosarcoma) included for comparison.
exhibit comparatively high or low respiratory or glycolyticcapacities, respectively. Furthermore, the actual supply rates,especially at larger tumor sizes and in tumors with low perfusionrates, were generally below the availabilities required for half-maximal substrate consumptions.
Tissue Oxygénation.Oxygen partial pressure distributionswere measured in s.c. xenografts of breast and lung cancerswith high or low perfusion rates. Tissue pO2 distributions ofhuman tumor xenografts with low perfusion rates were generally shifted to lower values; i.e., the pO2 histograms were tiltedto the left and were less variable than that of normal tissues. Attumor wet weights of 2.5 g, 50-60% of the values were obtainedfrom tissue areas with pO2 levels <5 mm Hg (Fig. 5/1). Decreased radiosensitivity is expected to occur in these areas. Incontrast, the tissue oxygénationof human tumor xenograftswith relatively high blood flow values was comparable to thatof normal liver (Fig. 5/4). In these latter tumors, less than 10%of the pO2 readings were <5 mm Hg, i.e., in tissue areas withdecreased radiation sensitivity.
Considering oxygen levels in well perfused tumors as a function of size, a worsening of the tissue oxygénationwas noted atadvanced growth stages (Fig. 5B). This is concomitant with thedecrease in tumor perfusion reported above. However, "hyp-oxic" tumor areas in these well perfused xenografts did not
exceed 7% of the measured tumor volume even when tumorsizes exceeding 5% of the body mass were investigated. Hereby,values below 3 mm Hg, i.e., below those necessary for half-maximal radiation sensitivity, are regarded hypoxic. This is incontrast to findings in poorly perfused tumors, where "hypoxic"
pO2 readings were already detected in more than one-half ofthe tissue mass at much smaller volumes.
DISCUSSION
The perfusion of human tumor xenografts varied markedlyeven if tumors of the same cell line, of comparable sizes, andat the same implantation site were considered (Figs. 1 and 2).These differences indicate large variations in angiogenesis,blood vessel morphology, and tumor microcirculation. Thisfinding is in good agreement with previous data on primary andmetastatic human tumors (25-28) and on human tumor xeno
grafts (29). The flow variations were within the range previouslyobserved for tumors in patients (21) and for isotransplantedrodent tumors (30). Comparison of the perfusion of xenograftedand patient tumors shows that the blood flow through humantumors lies within the range ofthat of normal tissue at differentstages of activity (Fig. 6). Preliminary histológica! data indicatethat the mean intercapillary distance in small xenografts ofhighly perfused tumor lines was generally <100 urn whereasmean distances >200 urn were usually observed in poorly perfused transplants. However, the tumor microvessels were nothomogeneously distributed throughout the tumor mass butdensely vascularized areas were often adjacent to hypovascular-ized areas (31, 32).
With increasing tumor sizes, tumor perfusion declined dueto severe morphological and functional alterations of the tumormicrocirculation (14). As a consequence, the substrate availability is reduced in all tumor lines (Fig. 1). In order to assessthe impact of the implantation site on the results obtained (33),data from DS-carcinosarcomas implanted as a "tissue-isolated"preparation into the groin are compared with those from "tissue-isolated" kidney tumors (34). It is obvious that the groin
tumors have an approximately 2 times higher perfusion rate3761
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN TUMOR XENOGRAFTS
020
il-
Loctote Release
O O1 02 03 O« 05 06 07
TUMORBLOOD FLOW (ml/g/min)
Fig. 2. Supply and uptake of oxygen and glucose, láclaterelease, tumor venouspH values, and growth period of various human tumor xenografts at comparatalisizes as a function of tumor blood flow (tumor wet weights around 2.5 g;C7,medullary breast cancers lines with low perfusión; O, •¿�,squamous cell breastcancers; Q, «k,medullary breast cancer line with high perfusion; V, Y, lungcancer; A, A, ovarian carcinoma; D, •¿�uterine tumor , *, thyroid cancer; <, ^,malignant melanoma; >, rat DS t> carcinosarcoma for comparison). Values aremeans ±SE (bars). Lines of best fit: oxygen supply = 169.0 X tumor blood flow+ 1.1, r = 0.99, />< 0.001; PO, = 34.3 x tumor blood How + 3.8, r = 0.93, /><0.001; glucose supply = 5.1 x tumor blood + 0.2, r = 0.99, P< 0.001; F., = 1.0x tumor blood flow + 0. l, r = 0.83, P< 0.001; (-',. = 1.8 X tumor blood flow +0.06. r = 0.85. P < 0.001 ; tumor venous pH (tumor blood flow < 0.23 ml/g/min)= 1.232 X tumor blood flow + 7.026, r = 0.86, P < 0.001; tumor venous pH(tumor blood flow (TBF) > 0.23 ml/g/min] = 0.031 x tumor blood flow + 7.308,r = 0.13, value not significant; tumor growth period = 7.085 x TBp-0704, r =
0.80. P< 0.001).
leading to significantly higher oxygen and glucose supply rates.However, the kidney tumors achieve a comparable oxygenuptake by doubling the oxygen utilization. In contrast, theglucose uptake and the lactate release are low in kidney tumorsdue to relatively low glucose extraction ratios. Based on theflow data it can be concluded that the fat pedicle in the groin isa better "soil" for the implantation of "tissue-isolated" tumors
than the renal site despite the high kidney perfusion.It has been estimated that the maximal respiratory and gly-
colytic metabolism by the xenografted human tumors variedindependently of their actual substrate delivery (Figs. 3 and 4).However, under in vivo conditions, the substrate supply and not
Oxygen supply (ul 02/g/min)
Fig. 3. Oxygen consumption of xenografted human tumors as a function ofthe oxygen supply. Rat DS-carcinosarcomas are included for comparison. Calculated lines represent (lop to bottom) squamous cell breast cancers, melanomas,ovarian cancers, rat DS-carcinosarcomas, lung cancers, medullary breast cancerswith high perfusion rates, thyroid cancers, uterine tumors, and medullary breastcancers with poor blood flow.
EO)"5
coS.E
o>cooo2O
Glucose supply (iimol/g/min)
Fig. 4. Glucose uptake of xenografted human tumors at different glucoseavailabilities. Calculated lines represent (top to bottom) melanomas, lung cancers,medullary breast cancers with high blood flow rates, poorly perfused medullarybreast cancers, uterine tumors, rat DS-carcinosarcomas, ovarian cancers, thyroidcarcinomas, and squamous cell cancers.
the metabolic demand of the cancer cells limited the oxygenand glucose uptake by the xenografts. This is probably due tothe fact that the high intratumor flow resistance even of themost highly vascularized tumors permitted usually less thanhalf-maximal substrate uptake due to restricted supply rates.This finding infers steep gradients for glucose, lactate, and ATPin the intercapillary space of human tumor xenografts (22).Furthermore, glutaminolysis can be expected only in the closevicinity of tumor microvessels (35).
In s.c. xenografts of highly perfused tumors, tissue oxygénation is comparable to that of normal liver (Fig. 5). This is mostprobably due to an even better vascularization of s.c. implantsas compared with "tissue-isolated" preparations (33). At larger
sizes, the tumor outgrows its vasculature (36) and hypoxic andanoxic tissue areas develop (37). In poorly perfused tumors,such areas are already present at early growth stages (Fig. 5)and enlarge with tumor growth (21). In such tissue areas,decreased radiation response and altered sensitivity towardssome antiproliferative drugs have to be expected (7, 16-18).There is no evidence for tissue acidosis even at high lactate
3762
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN TUMOR XENOGRAFTS
100
25 50 75 100
TISSUE p02 VALUE (mmHg)
Fig. 5. Frequency distributions of O2 partial pressure in (A) medullary( ) and squamous cell breast cancer xenografts ( ), xenografted lungcancers ( ) and normal rat liver ( ); (B) lung cancer xenografts of differentsizes ( 1.8 ±0.3 g, ; 3.2 ±0.9 g, ; 13.0 ±3.3 g ).
10 -3
el"M
1 -
.1 -
•¿�BO
£tt
.01
Normal Tissue
Tumors in Patients
Xenografts
Breast UterusFig. 6. Range of blood flow values in normal female reproductive organs
(breast tissue during pre- and postmenopause and during lactation (41. 44, 45);basal flow rates in the uterus, perfusion of the pregnant uterus (46-49); malignanttumors of these organs in patients and comparable xenografted human tumors(weight approximately 2.5 g).
production rates as long as tumor perfusion is adequate for theremoval of metabolic waste products (Fig. 1C). At low perfusionrates, however, tumor venous pH distinctly drops. This is inagreement with pH electrode measurements in poorly perfusedmedullary and squamous cell breast cancers (22). Perfusiondifferences could further explain inconsistencies observed during pH measurements in human tumors /// sil u (17). Besidesflow-related variations in removal of metabolic waste products,histology-related pH differences might be important (38).
The better neovascularization, the higher perfusion, and moreadequate substrate supply in some tumor lines coincide withhigher proliferation rates as compared with poorly perfusedtumors. This indicates that the proliferation rate of these tu
mors is limited by the substrate delivery leading to a high cellloss factor in poorly perfused tumors (39). At the moment, theexperimental data are derived from relatively fast-growing tumors transplanted into rodents. However, both local progression and therapeutic response of tumors with the same histologyand similar clinical grading and staging might also depend onperfusion-related parameters (40, 41). In order to individualizetreatment, the assessment of substrate delivery or turnover byhuman tumors should supplement histological and clinical information. Further development of relatively noninvasive technology (magnetic resonance imaging, magnetic resonance spec-troscopy, or positron emission tomography) might permit suchmonitoring (42-44).
ACKNOWLEDGMENTS
The authors are very pleased to thank H. P. Fortmeyer for theimmunodeficient animals, H. Gabbert for the histological classificationof the human tumor xenografts, and S. Skates for expert statisticaladvice.
REFERENCES
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Weinberg. R. A. The genetic origins of human cancer. Cancer (Phila.). 61:1963-1968, 1988.Harris, H. The analysis of malignancy by cell fusion: the position in 1988.Cancer Res., 48: 3302-3306. 1988.Eigenbrodt, E., Fister, P., and Reinacher, P. New perspectives on carbohydrate metabolism in tumor cells. In: R. Beitner (ed.). Regulation of Carbohydrate Metabolism, pp. 141-179. Boca Raton. FL: CRC Press, 1985.White, M. K.. and Weber. M. J. Transformation by the src oncogene altersglucose transport into rat and chicken cells by different mechanisms. Mol.Cell. Biol.. 8: 138-144, 1988.Sklar, M. D. The ras oncogenes increase the intrinsic resistance of NIH 3T3cells (o ionizing radiation. Science (Wash. DC), 239: 645-647, 1988.Sklar, M. D. Increased resistance to m-diamminedichloroplatinum(H) inNIH 3T3 cells transformed by ras oncogenes. Cancer Res., 48: 793-797,1988.Rice, G. C.. Hoy, C., and Schimke, R. T. Transient hypoxia enhances thefrequency of dihydrofolate reducÃasegene amplification in Chinese hamsterovary cells. Proc. Nati. Acad. Sci. USA, 83: 5978-5982, 1986.Sutherland. R. M. Cell and environment interactions in tumor microregions:the multiceli spheroid model. Science (Wash. DC). 240: 177-184. 1988.Moscow, J. A., and Cowan. K. H. Mullidrug resistance. J. Nati. Cancer Inst..80: 14-20, 1988.Gimbrone, M. A., Leapman. S. B., Cotran, R. S., and Folkman, J. Tumordormancy in vivo by prevention of neovascularization. J. Exp. Med., 136:261-276. 1972.Cullino. P. M. Angiogenesis and oncogenesis. J. Nati. Cancer Inst.. 61:639-643, 1978.Folkman. J.. and Klagsbrun. M. Angiogenic factors. Science (Wash. DC),235: 442-446. 1987.Cullino. P. M. Extracellular compartments of solid tumors. In: F. F. Becker,Cancer 3. pp. 327-354. New York: Plenum Publishing Corp., 1975.Vaupel, P.. Frinak, S.. and Bicher. H. I. Heterogeneous oxygen partialpressure and pH distribution in C3H mouse mammary adenocarcinoma.Cancer Res., 41: 2008-2013, 1981.Jain, R. K. Determinants of tumor blood flow: a review. Cancer Res.. 48:2641-2658, 1988.Moulder, J. E.. and Rockwell, S. Tumor hypoxia: its impact on cancertherapy. Cancer Metastasis Rev., S: 313-341, 1987.Wike-Hooley, J. L., Haveman. J., and Reinhold. H. S. The relevance oftumor pH to the treatment of malignant disease. Radiother. Oncol.. 2: 343-366, 1984.Teicher, B. A., Lazo. J. S., and Sartorelli, A. C. Classification of antineo-plastic agents by their selective toxicities toward oxygenated and hypoxictumor cells. Cancer Res., 41: 73-81. 1981.Fortmeyer. H. P., and Basiert. G. Breeding and maintenance of nu/nu miceand rnu/rnu rats. In: G. B. Basten. H. P. Fortmeyer. and H. Schmidt-Matthicscn (eds.), Thymusaplastic Nude Mice and Rats in Clinical Oncology,pp. 25-37. New York: Fischer, 1981.Kallinowski, F., Fortmeyer, H. P., Runkel, S., and Vaupel, P. Substrateutilization of human tumor xenografts in vivo. J. Nutr. Growth Cancer, 4:155-166. 1987.Vaupel, P., Forlmeyer, H. P., Runkel. S.. and Kallinowski. F. Blood flow,oxygen consumption and tissue oxygénationof human breast cancer xenografts in nude rats. Cancer Res., 47: 3496-3503. 1987.Kallinowski. F.. Vaupel. P.. Runkel. S.. Berg, G.. Fortmeyer, H. P.. Baessler,K. H., Wagner, K., Mueller-Klieser, W., and Walenta, S. Glucose uptake,láclaterelease, ketone body turnover, metabolic micromilieu and pH distri-
3763
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN TUMOR XENOGRAFTS
butions ¡nhuman breasl cancer xenografts in nude rats. Cancer Res., 48:7264-7272, 1988.
23. Bork, R., Vaupcl. P., Guenther. H., and Thews, G. Atemgas-pH-Nomo-gramme fuer das Rattenblut bei 37'C. Anaesthesist. 24: 84-90, 1975.
24. Zander, R. Oxygen solubility in normal human blood. Adv. Physiol. Sci., 25:331-332. 198Õ.
25. Brem, S.. Cotran. R., and Folkman, J. Tumor angiogenesis: a quantitativemethod for histologie grading. J. Nati. Cancer Inst.. 48: 347-356, 1972.
26. Brem, S., Jensen. H. M., and Cullino, P. M. Angiogenesis as a marker ofprcneoplastic lesions of the human breast. Cancer (Phila.), 41: 239-244,1978.
27. Chodak, G. W., Haudcnschild. C., Gittes, R. F., and Folkman. J. Angiogenicactivity as a marker of ncoplastic and preneoplastic lesions of the humanbladder. Ann. Surg., 192: 762-771. 1980.
28. Jensen. H. M., Chen, I., DeVault, M. R.. and Lewis, A. E. Angiogenesisinduced by "normal" human breast tissue: a probable marker for precancer.Science (Wash. DC), 218: 293-295, 1982.
29. Solesvik, O. V., Rofstad, E. K., and Brustad. T. Vascular structure of fivehuman malignant melanomas grown in athymic nude mice. 111.J. Cancer,46: 557-567. 1982.
30. Jain, R. K., and Ward-Hartley. K. A. Tumor blood flow: characterization,modifications and role in hyperthermia. IEEE Trans., SU-31:504-526. 1984.
31. Warren, B. A. The vascular morphology of tumors. In: H. 1. Peterson (ed.).Tumor Blood Circulation: Angiogenesis, Vascular Morphology and BloodFlow of Experimental and Human Tumors. Boca Raton, FL: CRC Press,1979.
32. Vaupel. P., and Hammersen. F. (eds.), Mikrozirkulation in malignen Tumoren. Basel: S. Karger AG, 1983.
33. Vaupel. P.. and Mucller-Klieser. W. Cell line and growth site as relevantparameters governing tumor tissue oxygénation.Adv. Exp. Med. Biol., 200:633-643, 1986.
34. Vaupel, P. Alemgaswechsel und Glukosestoffwechsel von Implantationstumoren (DS-Carcinosarkom) in vivo. Funktionsanalyse Biol. Syst.. /: 1-138.1974.
35. Kallinowski. F., Runkel, S., Fortmeyer, H. P.. Foerster, H., and Vaupel, P.i -Glulamine: a major substrate for tumor cells in viro"!J. Cancer Res. Clin.
Oncol., 113: 208-215. 1987.36. Tannock, I. F. Population kinetics of carcinoma cells, capillary endothelial
cells, and fibroblasts in a transplanted mouse mammary tumor. Cancer Res.,JO: 2470-2476, 1970.
37. Vaupel, P. Hypoxia in neoplastic tissue. Microvasc. Res.. 13: 399-408. 1977.38. Kallinowski, F., and Vaupel. P. pH distributions in spontaneous and iso-
transplanted rat tumors. Br. J. Cancer, 58: 314-321, 1988.39. Rofstad, E. Growth and vascular structure of human melanoma xenografts.
Cell Tissue Kinet., / 7: 91-101, 1984.40. DiChiro, G., Hatazawa, J., Katz, D. A., Rizzoli, H. V., and DeMichele, D.
J. Glucose utilization by intracranial meningiomas as an index of tumoraggressivity and probability of recurrence: a PET study. Radiology, 164: 521-526, 1987.
41. Gatenby, R. A., Kessler, H. B., Rosenblum, J. S., Coia, L. R., Moldofsky, P.J., Hartz, W. H., and Broder, G. J. Oxygen distribution in squamous cellcarcinoma métastasesand its relationship to outcome of radiation therapy.Int. J. Radiât.Oncol. Biol. Phys., 74:831-838, 1988.
42. Beaney, R. P., Lammertsma, A. A.. Jones, T., McKenzie, C. G.. and Hainan,K. E. Positron emission tomography for in viro measurements of regionalblood flow, oxygen utilization, and blood volume in patients with breastcarcinoma. Lancet, /: 131-134, 1984.
43. Kim, S. G., and Ackerman, J. J. H. Quantitative determination of tumorblood flow and perfusion via deuterium nuclear magnetic resonance spec-troscopy in mice. Cancer Res.. 48: 3449-3453, 1988.
44. Okunieff, P., Ramsay, J., Tokuhiro. T., Hitzig, B. M., Rummeny, E., Mc-Farland, E., Neuringer, L. J., and Suit, H. Estimation of tumor oxygénationand metabolic rate using "P MRS: correlation of longitudinal relaxationwith tumor growth rate and DNA synthesis. Int. J. Radial. Oncol. Biol.Phys., 14: 1185-1195, 1988.
45. Vorherr. H. The Breast. New York: Academic Press, 1974.46. Johnson, R. A thermodynamic method for investigation of radiation induced
changes in the microcirculation of human tumors. Int. J. Radiât.Oncol. Biol.Phys., /: 659-670, 1976.
47. Nystroem, C., Forssman, L., and Roos, B. Myometrical blood flow studiesin carcinoma of the corpus uteri. Acta Radio!. Ther. Phys. Biol.. 8: 193-198,1969.
48. U. Stave (ed.). Perinatal Physiology. New York: Plenum Publishing Corp.,1978.
49. Meschia, G. Circulation to female reproductive organs. In: Handbook ofPhysiology. The Cardiovascular System, Sect. 3, Vol. 1, Chap. 8, p. 241-269. Rockville, MD: American Physiological Society, 1981.
3764
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1989;49:3759-3764. Cancer Res F. Kallinowski, K. H. Schlenger, S. Runkel, et al. Growth Rate of Human Tumor XenograftsBlood Flow, Metabolism, Cellular Microenvironment, and
Updated version
http://cancerres.aacrjournals.org/content/49/14/3759
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/49/14/3759To request permission to re-use all or part of this article, use this link
on June 25, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

















![Cellular Metabolism [Autosaved]](https://img.pdfslide.net/doc/110x75/577c86241a28abe054bffe38/cellular-metabolism-autosaved.jpg)