Embed Size (px)
Citation preview
Blunt Traumatic Dissection of the Internal Carotid Artery Treated by Balloon Occlusion
Aksel G. Nordestgaard, MD, Geoffrey H. White, MDI, Steven Cobb, MD', Mark Mehringer, MD2, Samuel E. Wilson, MDI, Torrcxncc.. Cdifiirnia.
An extensive traumatic intimal dissection of the internal carotid artery was successfully managed by permanent occlusion of the vessel with percuta- neously-placed, inflatable balloons in a young patient who had suffered transient ischemic neurological attacks despite anticoagulation. This technique has not been previously reported for treatment of dissection. Review of 34 published reports of symptomatic intimal dissection associated wi th non-penetrating trauma to the head and neck revealed that most did not have a direct injury to the carotid region and that development of symptoms was often delayed. Only 50 % of these patients had onset of neurological symptoms within six hours of the episode of trauma, while 33 % remained asymptomatic for more than one week before complications occurred. In 15 patients who were treated surgically, only nine (60 %) achieved full recovery. Operative repair was considered unduly hazardous in our patient because of extension of the spiral dissection to the base of the skull. Successful use of percutaneous balloon occlusion of the carotid in this patient suggests that this technique should be considered a worthy alterna- tive for management of selected cases. (Ann Vasc Surg 1987, 7, (61 0-61 5).
KEY-WORDS : Balloon occlusion. Carotid artery dissection. Carotid artery trauma.
Dissection of the extracranial internal carotid ar- tery (ICA) is an uncommon consequence of blunt head and neck trauma for which there is no agree- ment on definitive treatment. We describe a patient with blunt traumatic dissection of the extracranial ICA, illustrating many of the typical features of this condition. The dissection was
From the Departments of Surgery' and Radiology 2,
Harbor- UCLA Medical Center, Torrance, California.
Presented at the Annual Meeting of the Southern Caltfbr- nia Vascular Surgical Society, Long Beach, California, September 26-28, 1986.
Reprint requests :Samuel E. Wilson, MD, Department of Surgery, Box 25, Harbor- UCLA Medical Center, 1000 West Carson Street, Torrance, California 90509, U.S.A.
treated with a new technique : balloon occlusion of the ICA proximal and distal to the site of intimal tear. Balloon occlusion should be considered as an alternative treatment for selected cases of blunt traumatic dissection of the extracranial ICA are reviewed to place this treatment in
CASE REPORT
perspective.
A 21-year-old male was admitted to Harbor-UCLA Medical Center with transient right facial, arm and leg weakness and sensory loss. Two weeks previously. the patient had been involved in a motorcyle accident with brief loss of consciousness. Examination at another hospital soon after the accident showed superficial lace-
VOLUME 1 No 5 - 1987 B.4LLOON OCCI,C'SION FOR CAROTID TRACM4 61 1
rations of the left foot as the only abnormal finding, and after suturing. the patient was discharged home. Pcrsis- tent right occipital headache and neck pain had been the only subsequent complaint. until development of tran- sient right-sided hemiparesis and sensory loss 24 hours before admission t o our hospital.
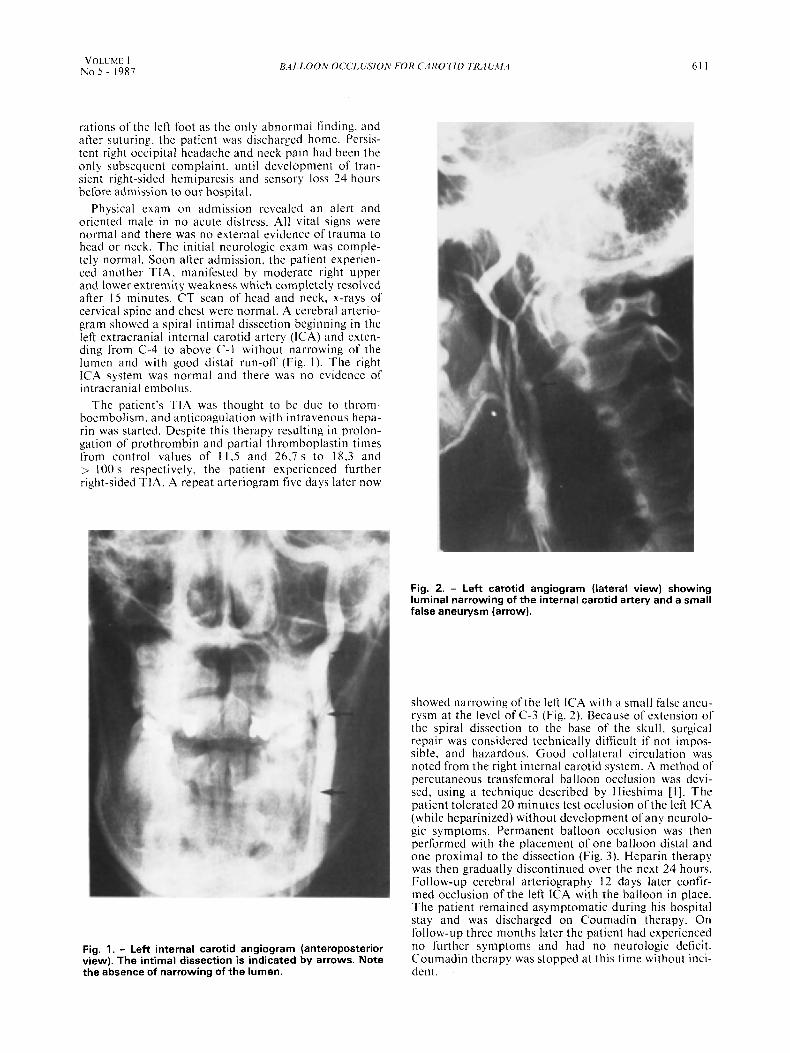
Physical exam on admission revealed an alert and oriented male in no acute distress. All vital signs were normal and there was no external evidence of trauma to head or neck. The initial neurologic exam was comple- tely normal. Soon after admission, the patient experien- ced another TIA. manifested by moderate right upper and lower extremity weakness which completely resolved after 15 minutes. CT scan of head and neck, x-rays of cervical spine and chest were normal. A cerebral arterio- gram showed a spiral intimal dissection beginning in the left extracranial internal carotid artery (ICA) and exten- ding from C-4 to above C-l without narrowing of the lumen and with good distal run-off (Fig. I ) . The right ICA system was normal and there was n o evidence of intracranial embolus.
The patient's TIA was thought to be due to throm- boembolism, and anticoagulation with intravenous hepa- rin was started. Despite this therapy resulting i n prolon- gation of prothrombin and partial thromboplastin times from control values of I1,5 and 26.7 s to 18,3 and > I00 s respectively, the patiel? experienced further right-sided TIA. A repeat arteriogram five days later now
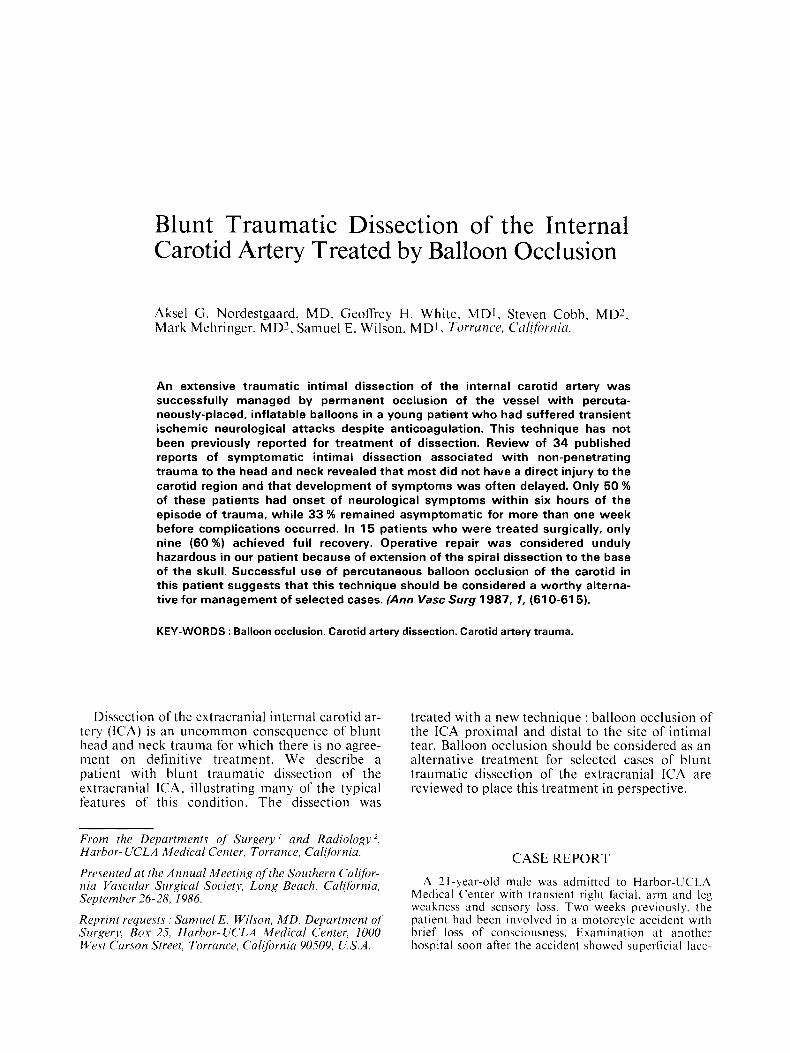
Fig. 2. - Left carotid angiogram (lateral view) showing luminal narrowing of the internal carotid artery and a small false aneurysm (arrow).
showed narrowing of the left ICA with a small false aneu- rysm at the level of C-3 (Fig. 2). Because of extension of the spiral dissection to the base of the skull, surgical repair was considered technically difficult if not impos- sible. and hazardous. Good collateral circulation was noted from the right internal carotid system. A method of percutaneous transfemoral balloon occlusion was devi- sed, using a technique described by Hieshima [I]. The patient tolerated 20 minutes test occlusion of the left ICA (while heparinized) without development of any neurolo- gic symptoms. Permanent balloon occlusion was then performed with the placement of one balloon distal and one proximal to the dissection (Fig. 3 ) . Heparin therapy was then gradually discontinued over the next 24 hours. Follow-up cerebral arteriography 12 days later confir- med occlusion of the left ICA with the balloon in place. The patient remained asymptomatic during his hospital stay and was discharged on Coumadin therapy. On follow-up three months later the patient had experienced no further syn1ptoms and had no neurologic deficit. Coumadin therapy was stopped at this time without inci- dent.
Fig. 1. - Left internal carotid angiogram (anteroposterior view). The intimal dissection is indicated by arrows. Note the absence of narrowing of the lumen.
612 ANNALS OF
VASCULAR SURGERY
TABLE I. - Sources of trauma in 3 4 reported patients with blunt traumatic dissection
of the extracranial internal carotid artery
N (%) Sources of Trauma
Motor vehicle accident 23 (68)
Direct blow to neck 3 ( 9) Fall 3 ( 9) Chiropractic manipulation 2 ( 6) Hyperextension of neck during exercise Tonsillectomy Rope around neck
TABLE II. - Associated injuries in 34 reported patients with blunt traumatic dissection of the extracranial
internal carotid artery
Associated injuries N (%) 17 (50) None
Head Facial laceration 5 12 (35) Skull fractures 3 Mandible fractures 2 Nose fracture 1 Subdural hematoma 1 Cerebral laceration 1
Orthopedic 10 (29) Thoracic 7 (21) Abdominal 5 (15) Cervical 4 (121
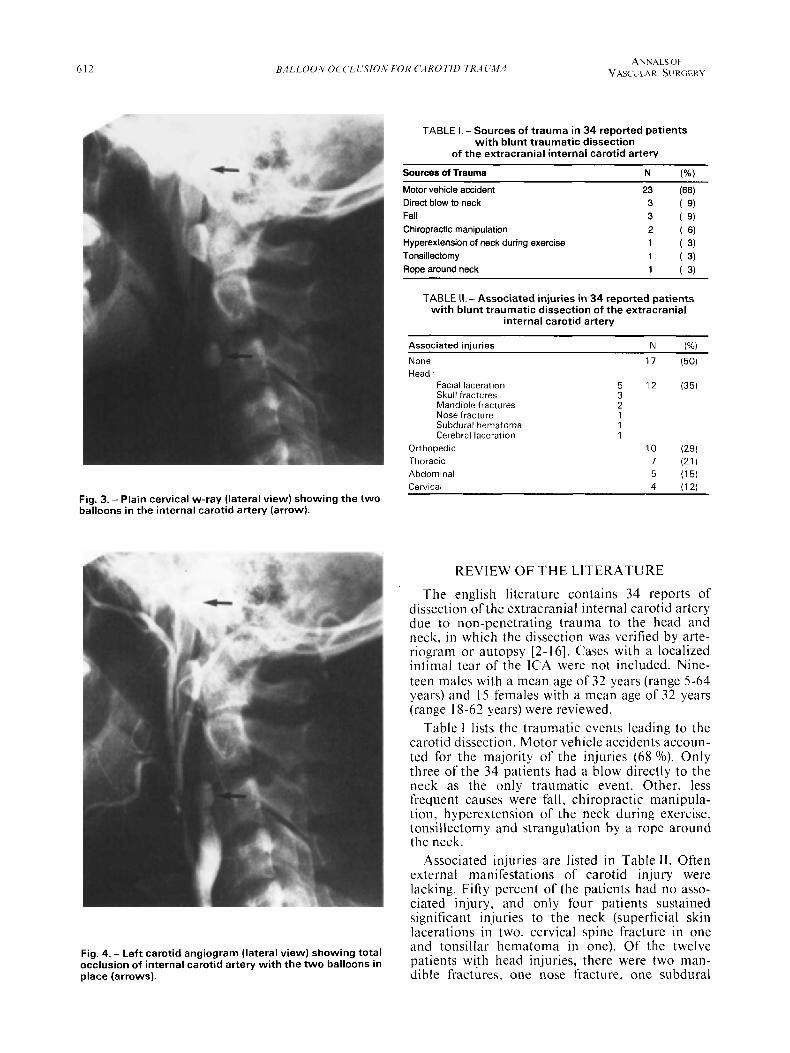
Fig. 3. - Plain cervical w-ray (lateral view) showing the two balloons in the internal carotid artery (arrow).
REVIEW O F THE LITERATURE
The english literature contains 34 reports of dissection of the extracranial internal carotid artery due to non-penetrating trauma to the head and neck, in which the dissection was verified by arte- riogram or autopsy [2-161. Cases with a localized intimal tear of the ICA were not included. Nine- teen males with a mean age of 32 years (range 5-64 years) and 15 females with a mean age of 32 years (range 18-62 years) were reviewed.
Table 1 lists the traumatic events leading to the carotid dissection. Motor vehicle accidents accoun- ted for the majority of the injuries (68 O/O). Only three of the 34 patients had a blow directly to the neck as the only traumatic event. Other, less frequent causes were fall, chiropractic manipula- tion, hyperextension of the neck during exercise, tonsillectomy and strangulation by a rope around the neck.
Associated injuries are listed in Table 11. Often external manifestations of carotid injury were lacking. Fifty percent of the patients had no asso- ciated injury, and only four patients sustained significant injuries to the neck (superficial skin lacerations in two, cervical spine fracture in one and tonsillar hematoma in one). Of the twelve patients with head injuries? there were two man- dible fractures, one nose fracture, one subdural
Fig. 4. - Left carotid angiogram (lateral view) showing total occlusion of internal carotid artery with the two balloons in place (arrows).
VOLUME 1 NO 5 - 1987 BALLOON OCCLUSION FOR CAROTID TRAUMA 613
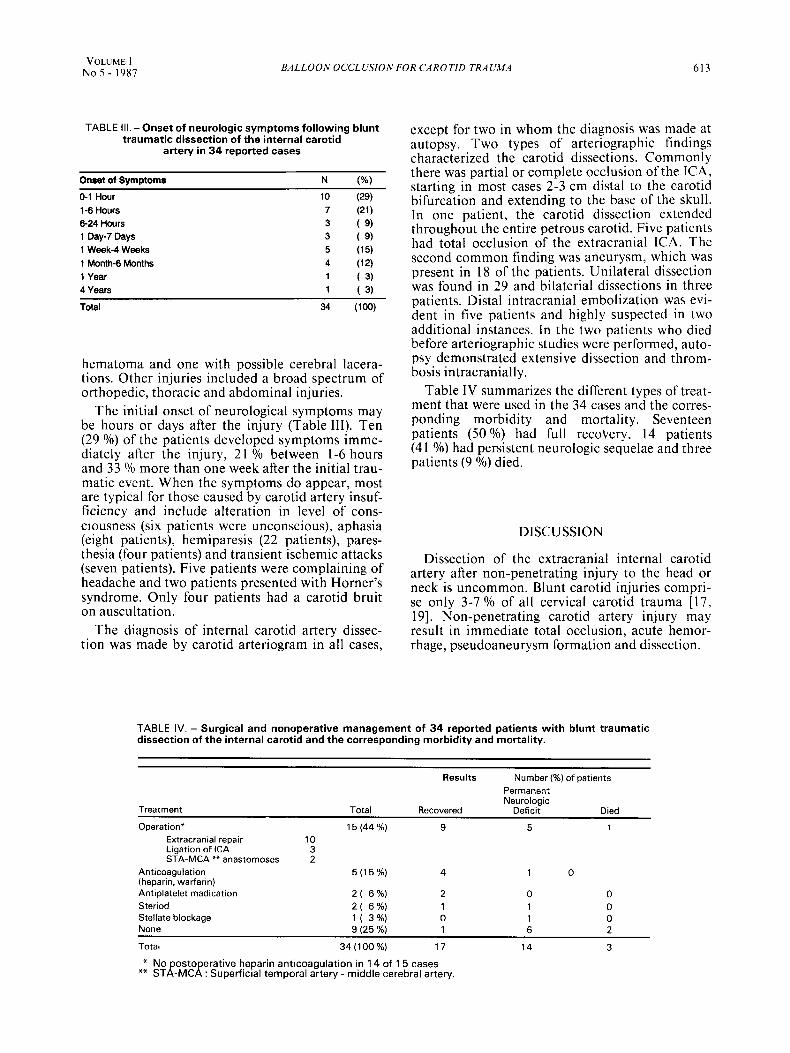
TABLE Ill. - Onset of neurologic symptoms following blunt traumatic dissection of the internal carotid
artery in 34 reported cases
Onset of Symptoms N (%)
0-1 Hour 10 (29) 1-6 Hours 7 (21) 6-24 Hours 3 ( 9) 1 Qay-7 Days 3 ( 9) 1 Week-4 Weeks 5 (15) 1 Month-6 Months 4 (12) I Year 1 ( 3) 4 Years 1 ( 3) Total 34 (100)
hematoma and one with possible cerebral lacera- tions. Other injuries included a broad spectrum of orthopedic, thoracic and abdominal injuries.
The initial onset of neurological symptoms may be hours or days after the injury (Table 111). Ten (29 O/o) of the patients developed symptoms imme- diately after the injury, 21 O/o between 1-6 hours and 33 O/o more than one week after the initial trau- matic event. When the symptoms do appear, most are typical for those caused by carotid artery insuf- ficiency and include alteration in level of cons- ciousness (six patients were unconscious), aphasia (eight patients), hemiparesis (22 patients), pares- thesia (four patients) and transient ischemic attacks (seven patients). Five patients were complaining of headache and two patients presented with Horner’s syndrome. Only four patients had a carotid bruit on auscultation.
The diagnosis of internal carotid artery dissec- tion was made by carotid arteriogram in all cases,
except for two in whom the diagnosis was made at autopsy. Two types of arteriographic findings characterized the carotid dissections. Commonly there was partial or complete occlusion of the ICA, starting in most cases 2-3 cm distal to the carotid bifurcation and extending to the base of the skull. In one patient, the carotid dissection extended throughout the entire petrous carotid. Five patients had total occlusion of the extracranial ICA. The second common finding was aneurysm, which was present in 18 of the patients. Unilateral dissection was found in 29 and bilaterial dissections in three patients. Distal intracranial embolization was evi- dent in five patients and highly suspected in two additional instances. In the two patients who died before arteriographic studies were performed, auto- psy demonstrated extensive dissection and throm- bosis intracranially.
Table IV summarizes the different types of treat- ment that were used in the 34 cases and the corres- ponding morbidity and mortality. Seventeen patients (50 O/o) had full recovery, 14 patients (4 I O/o) had persistent neurologic sequelae and three patients (9 Yo) died.
DISCUSSION
Dissection of the extracranial internal carotid artery after non-penetrating injury to the head or neck is uncommon. Blunt carotid injuries compri- se only 3-7 O/o of all cervical carotid trauma [17, 191. Non-penetrating carotid artery injury may result in immediate total occlusion, acute hemor- rhage, pseudoaneurysm formation and dissection.
TABLE IV. - Surgical and nonoperative management of 34 reported patients with blunt traumatic dissection of the internal carotid and the corresponding morbidity and mortality.
Results Number (%) of patients Permanent Neurologic
Treatment Total Recovered Deficit Died
Operation, 15 (44 %) 9 5 1 Extracranial repair 10 Ligation of ICA 3 STA-MCA ** anastomoses 2
Anticoagulation 5 ( 1 5 % ) 4 1 0 (heparin, warfarin) Antiplatelet madication 2 ( 6%) 2 0 0 Steriod 2 ( 6%) 1 1 0 Stellate blockage 1 ( 3%) 0 1 0 None 9 (25 %) 1 6 2
Total 34(100%) 17 14 3
** STL-MCA : Superficial temporal artery - middle cerebral artery. * No ostoperative heparin anticoagulation in 14 of 15 cases
614 BALL00111 OCCLWION POR CAKOTID TRAUWA ANNALS OF
VASCULAR SURGERY
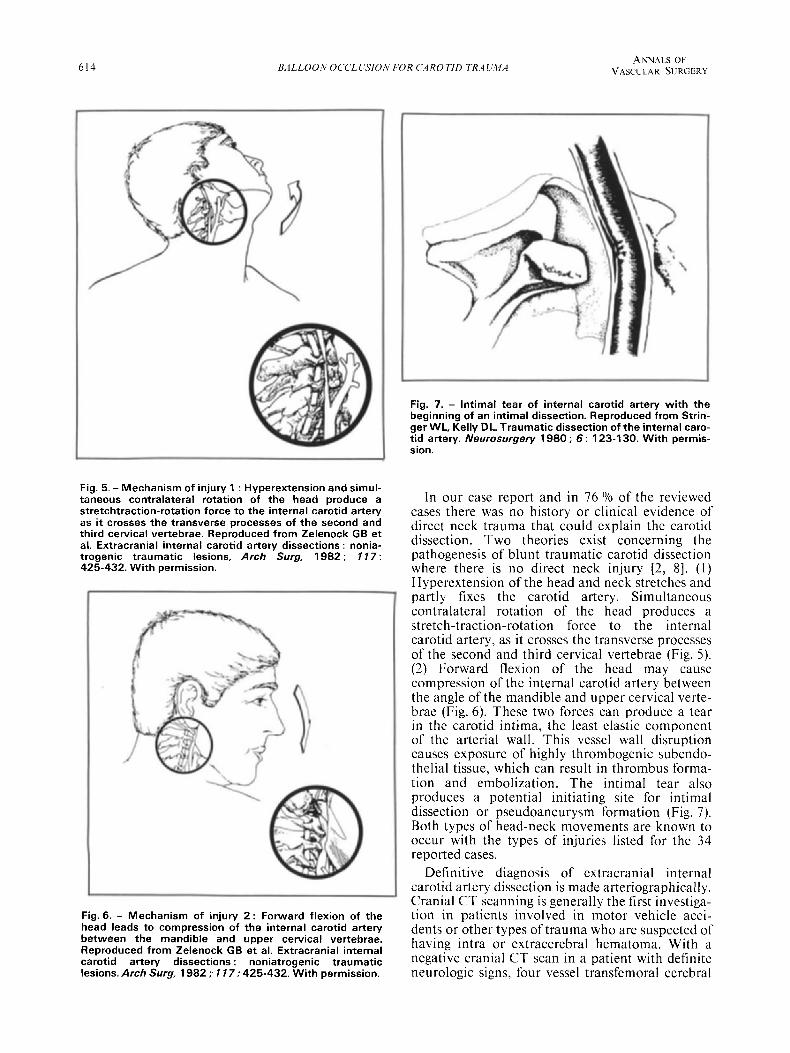
Fig. 5. - Mechanism of injury 1 : Hyperextension and simul- taneous contralateral rotation of the head produce a stretchtraction-rotation force to the internal carotid artery as it crosses the transverse processes of the second and third cervical vertebrae. Reproduced from Zelenock GB et al. Extracranial internal carotid artery dissections : nonia- trogenic traumatic lesions, Arch Surg, 1982 ; 1 17 : 425-432. With permission.
Fig. 6. - Mechanism of injury 2 : Forward flexion of the head leads to compression of the internal carotid artery between the mandible and upper cervical vertebrae. Reproduced from Zelenock GB et al. Extracranial internal carotid artery dissections : noniatrogenic traumatic lesions. Arch Surg, 1982 ; 1 17 : 425-432. With permission.
Fig. 7. - lntimal tear of internal carotid artery with the beginning of an intimal dissection. Reproduced from Strin- ger WL, Kelly DL. Traumatic dissection of the internal caro- tid artery. Neurosurgery 1980 ; 6 : 123-1 30. With permis- sion.
In our case report and in 76 Yo of the reviewed cases there was no history or clinical evidence of direct neck trauma that could explain the carotid dissection. Two theories exist concerning the pathogenesis of blunt traumatic carotid dissection where there is no direct neck injury [2, 81. ( I ) Hyperextension of the head and neck stretches and partly fixes the carotid artery. Simultaneous contralateral rotation of the head produces a stretch-traction-rotation force to the internal carotid artery, as it crosses the transverse processes of the second and third cervical vertebrae (Fig. 5). (2) Forward flexion of the head may cause compression of the internal carotid artery between the angle of the mandible and upper cervical verte- brae (Fig. 6). These two forces can produce a tear in the carotid intima, the least elastic component of the arterial wall. This vessel wall disruption causes exposure of highly thrombogenic subendo- thelial tissue, which can result in thrombus forma- tion and embolization. The intimal tear also produces a potential initiating site for intimal dissection or pseudoaneurysm formation (Fig. 7). Both types of head-neck movements are known to occur with the types of injuries listed for the 34 reported cases.
Definitive diagnosis of extracranial internal carotid artery dissection is made arteriographically. Cranial C T scanning is generally the first investiga- tion in patients involved in motor vehicle acci- dents or other types of trauma who are suspected of having intra or extracerebral hematoma. With a negative cranial CT scan in a patient with definite neurologic signs, four vessel transfemoral cerebral

VOLUME I NO 5 - 1987 BALLOON OCCLUSION FOR CAROTID TRAUMA 615
arteriography is then indicated to rule out signifi- cant cervical vascular injury. The arteriographic studies should include demonstration of both extracranial and intracranial carotid and vertebral arteries, with evaluation of collateral circulation, whether there are intracranial emboli and the size of the superficial temporal artery if an extracra- nial-intracranial anastomosis is planned. The importance of follow-up arteriogram has been stressed by several authors [6, 101 to evaluate the progression of healing of the dissection.
The natural history of these dissections and proper treatment have not been established because of the scarcity of cases. Patients who have a completed hemiplegic deficit and necrosis of brain tissue would reasonably be treated without operation or anticoagulation, because of the possi- bility of converting an ischemic infarct into a hemorrhagic one. Surgical intervention should be considered for patients with ischemic symptoms felt to be secondary to hypoperfusion resulting from high grade stenosis or occlusion without completed stroke. If the ischemic symptoms are secondary to emboli from the damaged carotid artery, then antiplatelet or anticoagulation therapy should be instituted. Failure of either of these two
1.
2.
3.
4.
5.
6.
7.
8.
medical therapies, as in our patient, necessitates surgical intervention. However with extension of the carotid dissection to the base of the skull, surgi- cal repair is often impossible and ligation of the internal carotid artery (sometimes inferior to the distal extent of dissection) has previously been the unsatisfactory option.
Therapeutic balloon occlusion has become a relatively safe method for managing many cases of vascular trauma of the head and neck [20]. We have successfully used this new technique in the treatment of a patient with blunt traumatic dissec- tion of the internal carotid artery. The procedure is performed under local anesthesia with minimal discomfort to the patient. Before permanent balloon occlusion is performed, a 15-20 minute balloon test occlusion is performed with the patient heparinized, during which the neurological status is constantly evaluated. Tolerance of the test occlusion and arteriographic evidence of good collateral cerebral circulation have been shown to be strong predictors for uncomplicated permanent carotid balloon occlusion [21]. Should there be either intolerance to the balloon occlusion test or insufficient collateral circulation on arteriogram, intracranial-extracranial anastomosis with occlu- sion of the internal carotid.artery should be consi- dered.
REFERENCES
HIESHIMA GB, MEHRINGER CM, GRINNELL VS, et al. Emergency occlusive techniques. Surg Neurol 1978 ; 9 :
ZELENOCK GB, KAZMERS A, WHITEHOUSE WM, et al. Extracranial internal carotid arterv dissections : nonia-
293-302.
trogenic traumatic lesions. Arch Surg (982 : 117: 425-432. PELLEGRINI RV. MANZETTI GW. DIMARCO RF. et al. The direct surgical management of lesions of the high in- ternal carotid artery. J Cardiovasc Surg 1984 ; 25 : 29-35. CHAKERA TMH. Bilateral extracranial internal carotid artery injury due to nonpenetrating trauma - report of three cases. Br J Radio1 1979 ; 52 : 704-708. BEATTY RA. Dissecting hematoma of the internal carotid arterv following chiromactic cervical maniodation. J Traima 1977 : 77 : 248-i49. BERGOUIST BJ. BOONE SC. WHALEY RA. Traumatic dissection of the internal carotid artery treated by EClC anastomosis. Stroke 198 1 ; 12 : 73-76. STRINGER WL, KELLY DL. Traumatic dissection of the internal carotid artery. Neurosurgery 1980 ; 6 : 123- 130. NEW PF, MOMOSE KJ. Traumatic dissection ofthe inter- nal carotid arterv at the atlantoaxial level. secondarv to nonpenetrating injury. Radiology 1969 ; 93 : 41-49.
. 9. DRAGON R, SARANCHAK H. LAKIN R. STRAUCH
G. Blunt injuries to the carotid and vertebral arteries. Am J Surg 1981 ; 141 : 497-550.
10. SULLIVAN HG, VINES FS, BECKER DP. Sequelae of in- direct internal carotid injury. Radiology 1973 ; 109: 9 1-98.
I I . LlTTLE JM, VANDERFIELD GK, MAY J, LAMOND S. Traumatic thrombosis of the internal carotid artery. Lancet I969 : 2 : 926-930.
12. LA1 MD. HOFFMAN HG, ADAMKlEWlCZ JJ. Dissec- ting aneurysms of internal carotid artery after nonpenetrat- ing neck injury. Acta Radiol.1966 ; 5 : 290-294.
13. NORTHCROFT CGB, MORGAN CAD. A fatal case of traumatic thrombosis of the internal carotid artery. Br J
14. MILLER JDR, AYERS TN. Post-traumatic changes in the internal carotid artery and its branches : an arteriographic study. Radiology 1967 ; 8 9 : 95-100.
MAS LM. Closed cervical cranial trauma associated with involvement of carotid and vertebral arteries. J Neurosurg
16. DRATZ HM, WOODHALL B. Traumatic dissecting aneu- rysms of left internal carotid, anterior cerebral and middle cerebral arteries. J Neuropathol Exp ilieurol 1947 ; 6 : 286-291.
17. RUB10 PA, REUL GH, BEALL AC. Acute carotid artery injury : 25 years’experience. J Trauma 1974 ; 14 : 967-973.
18. HARDY JD, RAJU S, NEELY WA, BERRY DM. Aortic and other arterial injuries. Ann Surg 1975 ; 181 : 640-653.
19. THAL ER, SNYDER WH, HAYS RJ. Management of carotid artery injuries. Surgery 1974 ; 76 : 955-962.
20. MEHRINGER CM, HlESHIMA GB, GRINNEL VS et al. Therapeutic embolization for vascular trauma of the head and neck. A J N R 1983 ; 4 : 437-442.
21. CHOLIS, BERNSTEIN A, ESKRlDGE J, FLAMME. Value of temporary balloon occlusion test of major cerebral arteries in predicting tolerance. The American Society of Neuroradiology, 24th Annual Meeting, January, 1986, Abstract Brook, s79.
SUQ 1944 ; 3 2 : 105-107.
15. GURDJIAN ES, HARDY WC, LINDNER DW, THO-
1963 ; 20 : 4 18-422.