Embed Size (px)
Citation preview

04/12/2016
1
Balloons, Boing-Boings, and Bioreactors
A Story of Knee Osteoarthritis
David Crane MD
Bluetail Medical Group St. Louis, MO; Columbia, MO; Naples, FL
Disclosures
• Consultant for Arthrex
Bluetail Medical Group
• Non-operative sports medicine
• Percutaneous use of biologics
• Collaborate closely with surgeons
– Intra-operative use
– Post-operative use
• Over 24,000 patients treated to date

04/12/2016
2
Biocellular Graft Use
• Follow FDA guidelines
• Minimal manipulation
• Point of care
• Most common treated disease
• Knee Osteoarthritis
• A blind doctor walks into a bar….
• And finds way more than he bargained for!

04/12/2016
3
What I’ve learned since fellowship
There is a
balloon…
What I’ve learned since fellowship
There is a
boing boing…
What I’ve learned since fellowship
There is a
bioreactor

04/12/2016
4
These 3 roughly correlate to;
Mechantransduction of
the joint capsule
And neurohormonal
signalling
And myotendionous
support
These 3 roughly correlate to;
Hoop stress of the
meniscus
AND
mechanotransduction
of cartilage
These 3 roughly correlate to;
Synovium with:
Growth Factors
Progenitor Cells
HA
Chemokines,
Cytokines,
Interleukins
MMP’s

04/12/2016
5
The Capsule
Mechantransduction of
the joint capsule
Capsular Anatomy
Capsular Anatomy

04/12/2016
6
Capsular Anatomy
Transverse section of the
medial joint capsule above
the level of the joint line:
Layers I and II are fused
anteriorly
Layers II and III are fused
posteriorly

04/12/2016
7
Capsular Anatomy
Capsular Anatomy
Capsular Anatomy

04/12/2016
8
Capsular Anatomy
Capsular Anatomy
The Meniscus and Cartilage Interface
Hoop stress of the
meniscus
AND
mechanotransduction
of cartilage
04/12/2016
9
Meniscus Anatomy
• Load and forces are distributed across a much larger surface area because of the menisci, which:
• (1) decrease focal contact pressure by increasing the contact area
• (2) protect the underlying articular cartilage. Resection of 15-34% of a meniscus may increase contact pressure by more than 350%. Normal knees have 20% better shock-absorbing capacity than meniscectomized knees.
Insall JN, Scott WN, eds. Surgery of the Knee. 3rd ed. Philadelphia, Pa: WB Saunders Co; 2001.
Rodkey WG. Basic biology of the meniscus and response to injury. Instr Course Lect. 2000. 49:189-93.
Vaziri A, Nayeb-Hashemi H, Singh A, Tafti BA. Influence of meniscectomy and meniscus replacement on the
stress distribution in human knee joint. Ann Biomed Eng. 2008 May 22. epub ahead of print.
Three layers of the
medial capsule:
I. Crural fascia
II. Superficial portion
of the MCL
III. Deep portion of
the MCL including
the
meniscofemoral
and meniscotibial
extensions of the
deep MCL.
The Synovium and Fat Pad
Synovium with:
Growth Factors
Progenitor Cells
HA
Chemokines,
Cytokines,
Interleukins
MMP’s

04/12/2016
10
Why mixed results with cellular
treatments?
• Many variables exist in product & delivery ere are many variables in product and delivery
Platelet Activation
Activation releases > 1500 proteins
• Alpha granules contain > 300 growth
factors
– PDGF, VEGF, TGF-β1, bFGF, EGF
• Dense granules contain serotonin,
histamine, Ca, adenosine and dopamine
Unactivated platelets
Activated platelets
Growth Factors
• Anti-inflammatory
• Anti-degradative
• Analgesic
• Antimicrobial
• Modulate healing
04/12/2016
11
Rationale for PRP in OA
• PRP Chondrocyte proliferation
Chondrogenic markers
Col 2, PG Synthesis
Cartilage repair- PDGF and TGF
MSC proliferation
Inhibition of pain pathway
Synovial HA Production
Rationale for PRP in OA–ACP
vs HA
• ACP MMP-13
• ACP HAS-2 expression in synoviocytes
• ACP cartilage synthetic activity
➔ACP acts to stimulate endogenous HA production and decrease cartilage catabolism
} Compared with HA
Sundman et al, 2014
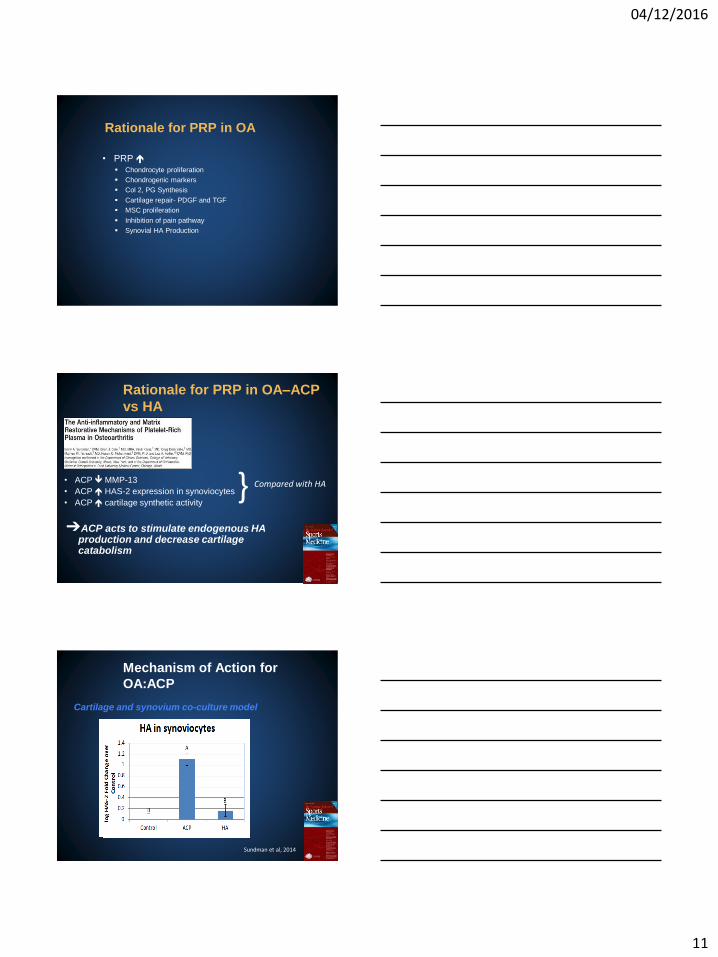
Mechanism of Action for
OA:ACP
Cartilage and synovium co-culture model

04/12/2016
12
Mechanism of Action for
OA:ACP
Cartilage and synovium co-culture model
Sundman et al., 2014
Mechanism of Action for
OA:ACP
• Controlled Laboratory
Study
• Investigated proliferation
of Superficial Zone
Protein (SZP) and cell
proliferation at articular
cartilage after contact with
ACP
Sakata et al, 2015
Level 1 Evidence PRP vs HA for
OA
Plasma based PRP versus HA:
• WBC preparation
• RCT - 176 patients 3 weekly injections
• 38% of patients receiving PRGF had 50% decrease in
WOMAC pain score in 24 weeks vs 24% of patients
receiving HA (p value 0.044)
Sanchez et al, 2012

04/12/2016
13
96 patients:
PRGF 3 injections vs 1 injection HA
PRGF (Plasma Rich in Growth Factors- WBC) vs HA:
PRP Superior to HA for up to 12 months
Level 1 Evidence PRP vs HA for
OA
Vaquerizo et al, 2013
ACP Superior to HA for up to 6 months
Level 1 Evidence ACP vs. HA for
OA
Cerza et. al, 2012
Double Blind Level 1 ACP vs HA
0
10
20
30
40
50
60
70
1 2 3 4 5 6
IKD
C S
core
Visit
IKDC*
ACP
HA
ACP Clinically Superior to HA at 6 months
0
1
2
3
4
5
6
7
1 2 3 4 5 6
VA
S Pa
in S
core
Visit
VAS Pain*
ACP
HA
Cole BJ, Fortier L, Karas V, Merkow D, Stuckey A, Butty D, Verma N, Preliminary Data, 2014
04/12/2016
14
Double Blind Level 1 ACP vs HA
ACP Biologically Superior to HA at 6 months
0
0.05
0.1
0.15
0.2
0.25
1 2 3 5 6
Co
nce
ntr
atio
n
Visit
TNF-α
ACP
HA
0
2
4
6
8
10
12
14
16
18
20
1 2 3 5 6
Co
nce
ntr
atio
n
Visit
IL-6*
ACP
HA
Cole BJ, Fortier L, Karas V, Merkow D, Stuckey A, Butty D, Verma N, Preliminary Data, 2014
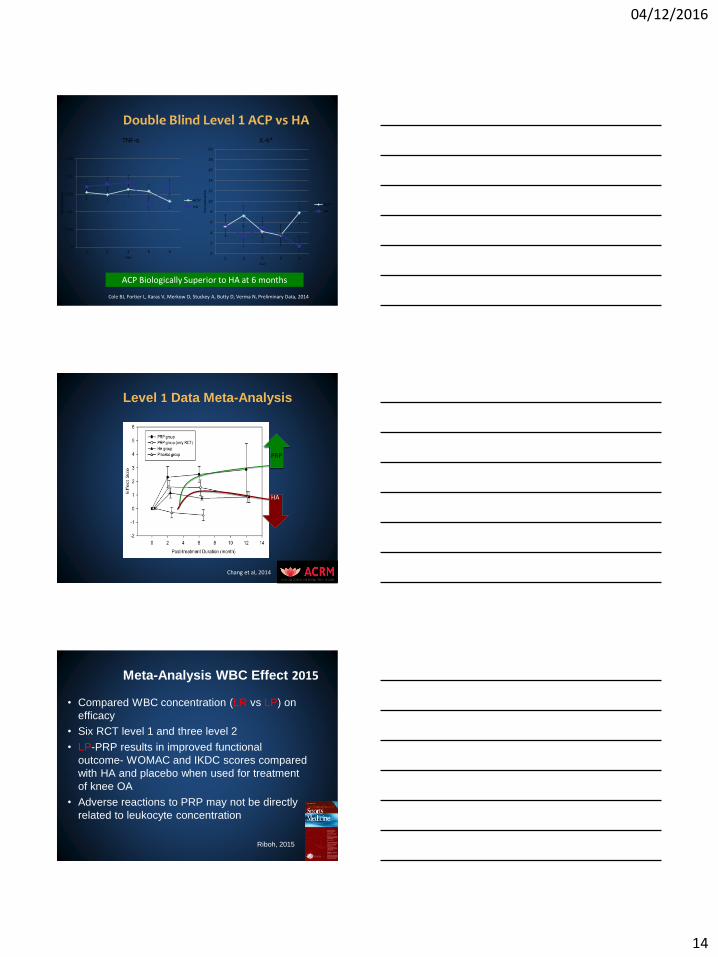
Level 1 Data Meta-Analysis
Chang et al, 2014
HA
PRP
Meta-Analysis WBC Effect 2015
• Compared WBC concentration (LR vs LP) on
efficacy
• Six RCT level 1 and three level 2
• LP-PRP results in improved functional
outcome- WOMAC and IKDC scores compared
with HA and placebo when used for treatment
of knee OA
• Adverse reactions to PRP may not be directly
related to leukocyte concentration
Riboh, 2015
04/12/2016
15
Systematic Review PRP for OA
• Six Level 1 Studies- 739 patients (817 knees)
• PRP showed significant clinical improvements compared to HA/saline up to 12 months
• WOMAC significantly better for PRP than HA 3-6 months (p=0.0008); 6-12 months (p=0.0062)
• 5 of 5 LP-PRP studies showed improvement!
• Filardo (LR-PRP) showed no improvement
Meheux, 2015
Meta-Analysis of PRP
Meta-Analyses
• Level IV systematic review
• Concluded that intra-articular PRP is a
viable treatment for knee OA
– Particularly with early degenerative changes
• Shown to be more effective than other strategies-
including HA or placebo treatments
Campbell, 2015
Putting it all together….
04/12/2016
16
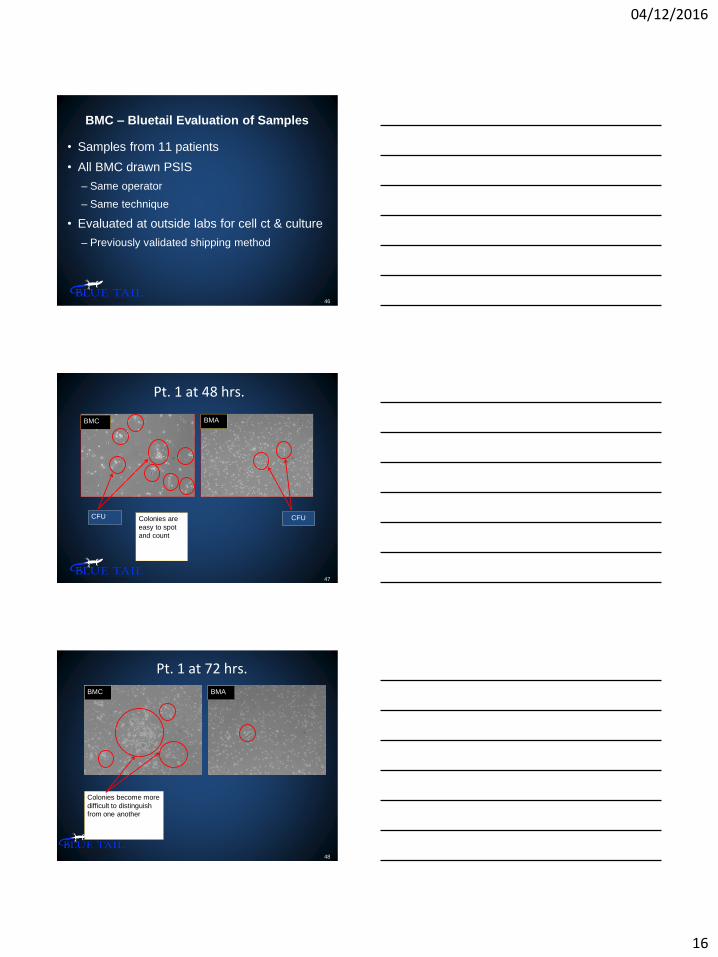
BMC – Bluetail Evaluation of Samples
• Samples from 11 patients
• All BMC drawn PSIS
– Same operator
– Same technique
• Evaluated at outside labs for cell ct & culture
– Previously validated shipping method
46
47
Pt. 1 at 48 hrs.
BMC BMA
CFU CFU Colonies are
easy to spot
and count
Pt. 1 at 72 hrs.
48
BMC BMA
Colonies become more
difficult to distinguish
from one another

04/12/2016
17
Pt. 1 at 96 hrs
49
BMC BMA
Colonies blend together
50
Bone Marrow Aspirate
Angel BMC
51
We found what we expected
Cellular
Concentrations2% BMC/PPP
Statistical
Difference?15% BMC/PPP
PLT (k/μL) 145 ± 193 Yes, p = 0.016 1030 ± 732
WBC (k/μL) 1.90 ± 3.54 Yes, p = 0.002 52.87 ± 28.34
NE (k/μL) 0.16 ± 0.23 Yes, p = 0.023 17.13 ± 15.43
LY (k/μL) 0.95 ± 2.06 Yes, p = 0.001 18.20 ± 9.32
MO (k/μL) 0.35 ± 0.69 Yes, p = 0.002 7.02 ± 3.87
RBC (M/μL) 0.04 ± 0.01 Yes, p = <0.001 1.51 ± 0.65
TNC (k/uL) 2.22 ± 4.10 Yes, p = 0.002 56.98 ± 30.23
HPC (k/μL) 2.00 ± 4.47x10-4 No, p = 0.198 2.92 ± 5.09x10-2

04/12/2016
18
52
IL-1ra Average ± StDev (pg/mL)Statistical
Difference?
2% BMC/PPP 1693 ± 1012
15% BMC/PPP 22654 ± 3877
IL-1beta Average ± StDev (pg/mL)Statistical
Difference?
2% BMC/PPP 8.8 ± 1.6
15% BMC/PPP 24.6 ± 35.0
Yes, p = <0.001
Yes, p = 0.041
But found something unexpected!
There is IL-ra in BMC!
IL-ra1 and BMC
• A ratio of IL-ra/IL-1β of 10-1000:1 is sufficient
to effect blockade of the IL-1 receptors,
thereby alleviating the degenerative effects of
IL-1
Wehling et al 2007
53
IL-1ra/IL-1beta Ratio AverageStatistical
Difference?
2% BMC/PPP 193.5
15% BMC/PPP 720.6Yes, p = 0.007
Clinical Outcome of Bone Marrow Concentrate in Knee
Osteoarthritis. Oliver, Bayes, Crane; J of Prolo: 2015
• Prospective Case Review using Arthrex SOS
– 70 pts with II-IV Knee OA
– BMC and MM Adipose
– VAS and KOOS at 3 and 6 months
• Stat. significant improvement
– Pain
– Function
– QOL
– ADL’s
04/12/2016
19
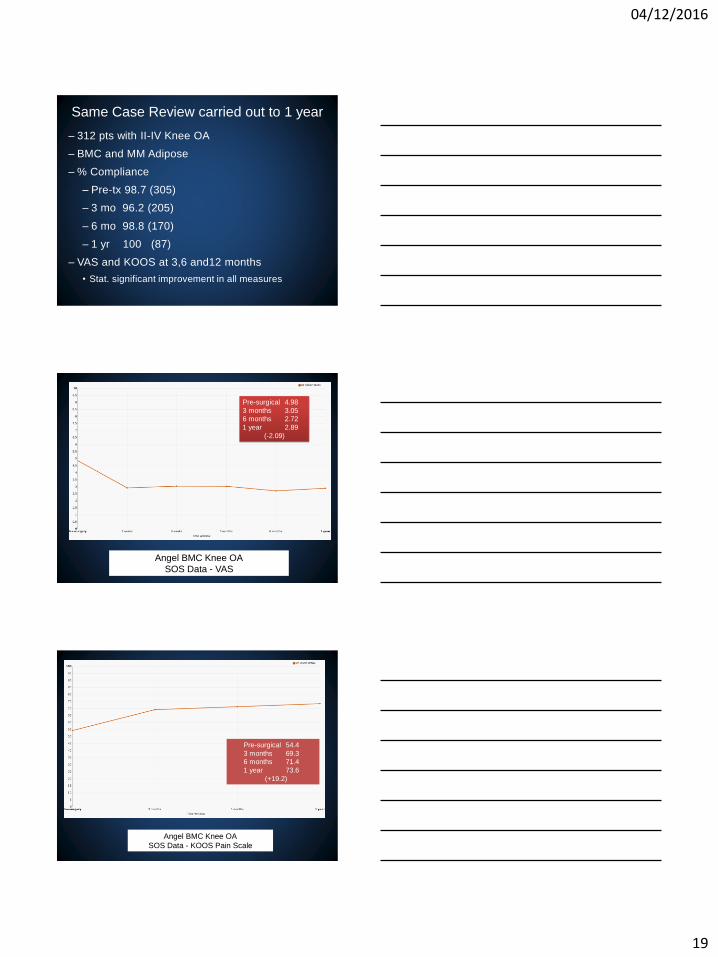
Same Case Review carried out to 1 year
– 312 pts with II-IV Knee OA
– BMC and MM Adipose
– % Compliance
– Pre-tx 98.7 (305)
– 3 mo 96.2 (205)
– 6 mo 98.8 (170)
– 1 yr 100 (87)
– VAS and KOOS at 3,6 and12 months
• Stat. significant improvement in all measures
Angel BMC Knee OA
SOS Data - VAS
Pre-surgical 4.98
3 months 3.05
6 months 2.72
1 year 2.89
(-2.09)
Angel BMC Knee OA
SOS Data - KOOS Pain Scale
Pre-surgical 54.4
3 months 69.3
6 months 71.4
1 year 73.6
(+19.2)
04/12/2016
20
Angel BMC Knee OA
SOS Data – KOOS Symptoms Scale
Pre-surgical 53.2
3 months 69.7
6 months 69.9
1 year 70.7
(+17.5)
Angel BMC Knee OA
SOS Data - KOOS ADL’s
Pre-surgical 60.6
3 months 73.4
6 months 78.3
1 year 78.6
(+18)
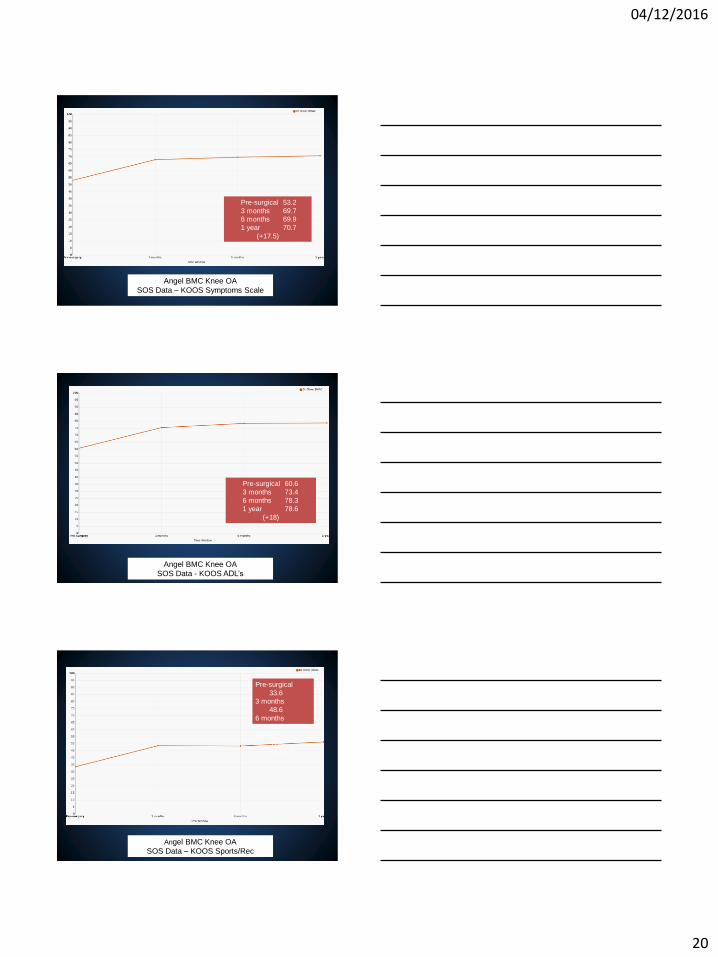
Angel BMC Knee OA
SOS Data – KOOS Sports/Rec
Pre-surgical
33.6
3 months
48.6
6 months
48.4
1 year
51.3
(+17.7)

04/12/2016
21
Angel BMC Knee OA
SOS Data – KOOS QOL
Pre-surgical 29.1
3 months 47.9
6 months 50.8
1 year 52.6
(+23.5)
• Biocellular grafts are showing continued
promise as a viable, safe, effective, and cost
effective way to treat mild to moderate and
possibly some cases of severe OA in some
cases.
• Choose your patients wisely
• “Go out and do good in the world”
Summary
Thank You!
David Crane MD
Bluetail Medical Group St. Louis, MO; Columbia, MO; Naples, FL











![IMG 2015 [Skrivebeskyttet] · • “Intratendinousinjections of platelet-poor or platelet rich plasma with or without leukocyte enrichment for ... (Angel system from Cytomedix/ Arthrex)](https://img.pdfslide.net/doc/110x75/5f50a037afc361566c318f31/img-2015-skrivebeskyttet-a-aoeintratendinousinjections-of-platelet-poor-or-platelet.jpg)

















