Embed Size (px)
Citation preview
Board Review: Neurology
Matthew Volk6/11/2010
Question #1
Guillain-Barre Syndrome
Immune-mediated, demyelinating polyneuropathy Proximal and distal weakness – including
respiratory failure; Distal sensory loss Autonomic and cranial nerve
involvement Most cases triggered by infxn,
surgery, or immunization CMV, EBV, HIV, Hepatitis, Lyme,
campylobacter jejuni
Guillain-Barre Syndrome
Treatment Supportive care
Follow FVC and NIFs Mechanical ventilation as needed
IVIg – avoid in CKD, CHF, IgA deficiency Plasmapheresis – avoid in infxn, low BP No benefit to combination therapy Steroids not shown to help
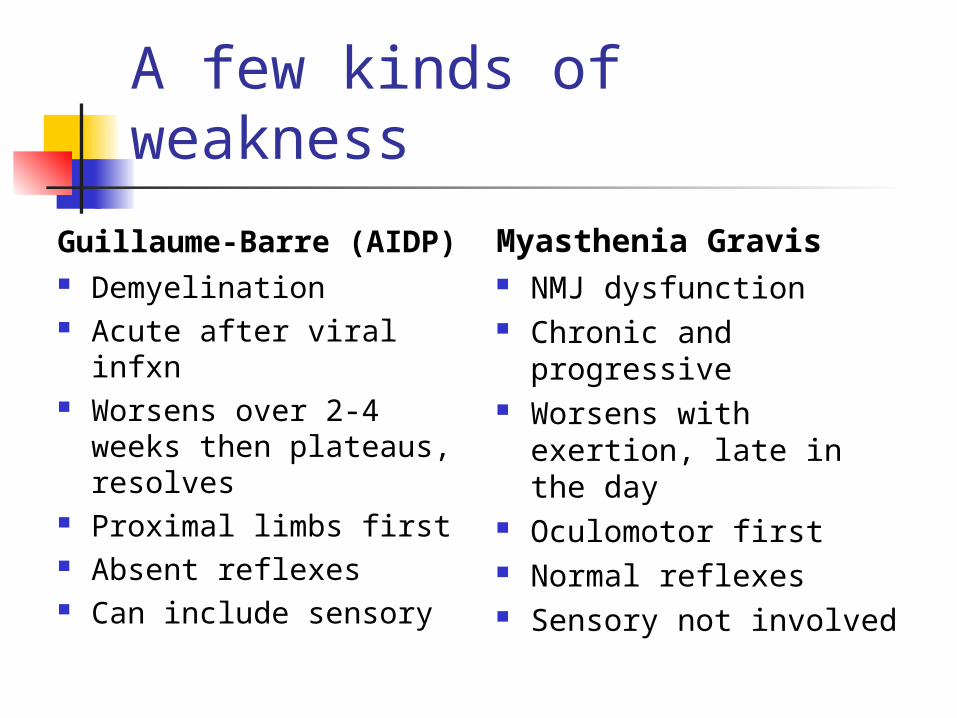
Guillaume-Barre (AIDP) Demyelination Acute after viral infxn Worsens over 2-4
weeks then plateaus, resolves
Proximal limbs first Absent reflexes Can include sensory
Myasthenia Gravis NMJ dysfunction Chronic and
progressive Worsens with exertion,
late in the day Oculomotor first Normal reflexes Sensory not involved
A few kinds of weakness
A few kinds of weakness
ALS – chronic progressive, ocular muscle sparing, hyperreflexia and spasticity (UMN disease)
Lambert Eaton – chronic but can resolve if malignancy-related, improves with exercise
What does this patient have?
HPI: 54 y/o F with worsening SOB and inability to swallow x 2 days. Has had fatigue, difficulty keeping eyelids open, intermittent double vision x 1 month.
PE: shows bilateral ptosis, mild proximal weakness, normal reflexes.
Question #2
Question #2
Acute Ischemic Stroke
Inclusion criteria for tPA Age >18 years Clinical diagnosis of ischemic stroke Onset of symptoms within 3 hours of
rx CT without evidence of ICH
Key exclusion criteria Rapidly improving symptoms Persistent BP > 185/110
Acute Ischemic Stroke Aspirin to reduce rate of recurrent
stroke; effect within 2 weeks Subcutaneous heparin to prevent DVT Airway protection/dysphagia screening Blood pressure control in certain cases Maintainence of normothermia
Hypothermia not studied in acute stroke Aim for normoglycemia
Acute Ischemic Stroke
More on Blood Pressure control: Hypertension protective unless
extreme Many would not treat unless >220 systolic EXCEPT treat to goal 140-150 with MI,
aortic dissection, hemorrhagic conversion Recommended agents
Nicardipine, labetalol, nitroprusside
Question #3
Parkinsonism
Drug-induced Parkinsonism Antiemetics, Antipsychotics, CCBs Reversible with removal of offending
agent Neurodegenerative processes
Progressive Supranuclear Palsy Multiple System Atrophy Corticobasal Degeneration Huntington’s Disease
Parkinsonism
Essential Tremor Restless Leg Syndrome Focal/generalized dystonias
Cervical dystonia Blepharospasm Oromandibular dystonia Spasmotic dysphonia
Ideopathic Parkinson’s Disease
Parkinson’s Disease
Symptoms: resting tremor, rigidity, bradykinesia, postural instability
Treatments Levodopa/carbidopa – older patients Dopamine agonists – young patients Amantadine – mainly works with
tremor Anticholinergics – young patients MAO inhibitors – adjunctive therapy
Normal Pressure Hydrocephalus
Gait Impairment Cognitive Decline Urinary Incontinence
Some Dementias
Frontotemporal Dementia Impaired executive function Preserved visual-spatial function
Lewy Body Dementia Visual hallucinations Fluctuating cognition Parkinsonism
Question #4
Multiple Sclerosis
Signs and Symptoms – develop over hours to days to years Diplopia or Optic Neuritis Hemiparesis Hemisensory disturbance Band-like sensations around trunk Urinary retention Cognitive decline
Multiple Sclerosis
Treatment Solumedrol followed by prednisone
taper in acute exacerbations Disease-modifying therapy – for
relapsing-remitting disease Interferon beta (Betaseron, Avonex, Rebif) Glatiramer acetate (MHC interaction)
Combination therapy – for progressive dz
Combine with cyclophos or Mitoxantrone
Question #5
Migraine Headaches
Throbbing pain with photophobia and phonophobia.
Brainstem involvement results in nausea, pallor, flushing, tearing, rhinorrhea, and sinus congestion.
60-70% with prodrome 24 hr prior 15-25% with aura 1 hr prior
Migraine Headaches
Treatment NSAIDs – nonspecific; for mild headaches Triptans – direct trigeminal nerve binding;
for moderate to severe headaches Contraindicated in CAD
Ergot derivatives – hospitalized patients Rescue medications – Haldol, lidocaine,
magnesium, dilantin, tizanidine, zyprexa. Opioids can be used occasionally
Distinguishing Headaches
Migraine/Cluster versus Tension Cause disability versus able to work
through them Migraine versus Cluster
Stay still versus pace and even strike head
>4 hours versus <3 hours
Question #6
Question #7
Epilepsy
Two or more unprovoked seizures Etiologies: unknown (ideopathic) or
focal abn (symptomatic) Vascular malformation Tumor Restricted scar Focal cortical dysgenesis
Epilepsy Treatment
After first seizure – decision to start treatment is individualized
No driving for 6 months to 1 year Risk for recurrence is 30 to 60%.
Abnormal EEG indicates higher risk After second seizure recurrance rate
is 80 to 90%.
Epilepsy Treatment
Choice of medication Absence – Ethosuximide GTC – Phenytoin, Carbamazepine,
Phenobarbital, Valproate Partial – Gabapentin, Lamotrigine,
topiramate, oxcarbazepine Cognitive impairment – Phenobarb,
Phenytoin, Carbamazepine, Topiramate
Status Epilepticus
Secure ABCs – including intubation Ativan 0.1 mg/kg then Phenytoin/phos-phenytoin 18
mg/kg Phenobarbitol 15 mg/kg Pentobarbitol 5-15 mg/kg
Question #8
Question #8
Primary CNS Lymphoma Presentation: confusion, lethargy,
memory loss, focal neuro signs, and/or seizures
Solitary or multiple brain masses Diagnostic evaluation
Evaluation for uveitis, retinitis CSF EBV viral load brain biopsy
Treat with MTX and whole brain XRT
Toxoplasmic Encephalitis
Similar presentation to PCNSL Diagnostic criteria
Seropositive for Toxo IgG antibody CD4 < 100 and not getting prophy Multiple ring-enhancing lesions on MRI
If all three present 90% likelihood Presumptive
pyrimethamine/sulfadiazine Otherwise brain biopsy recommended.

Question #9
Compressive myelopathy Presentation:
Initial spinal or radicular pain Bilateral motor or sensory dysfxn No brain or brainstem findings
Evaluate with MRI spine Surgical decompression for
epidural abscess and spondylosis Steroids and XRT vs. surgery for
epidural tumors
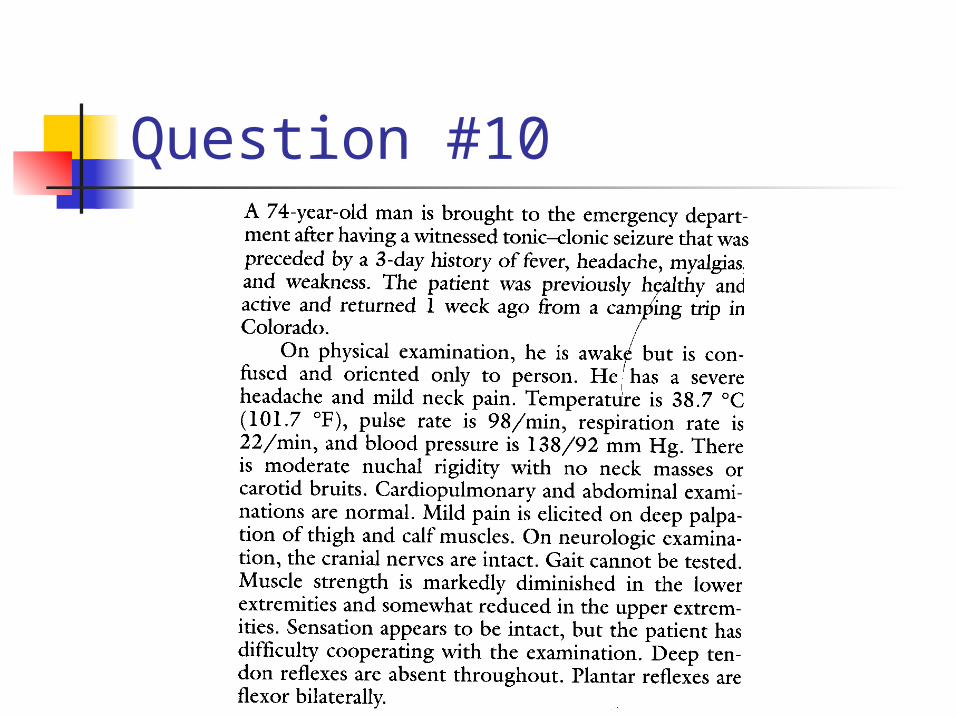
Question #10
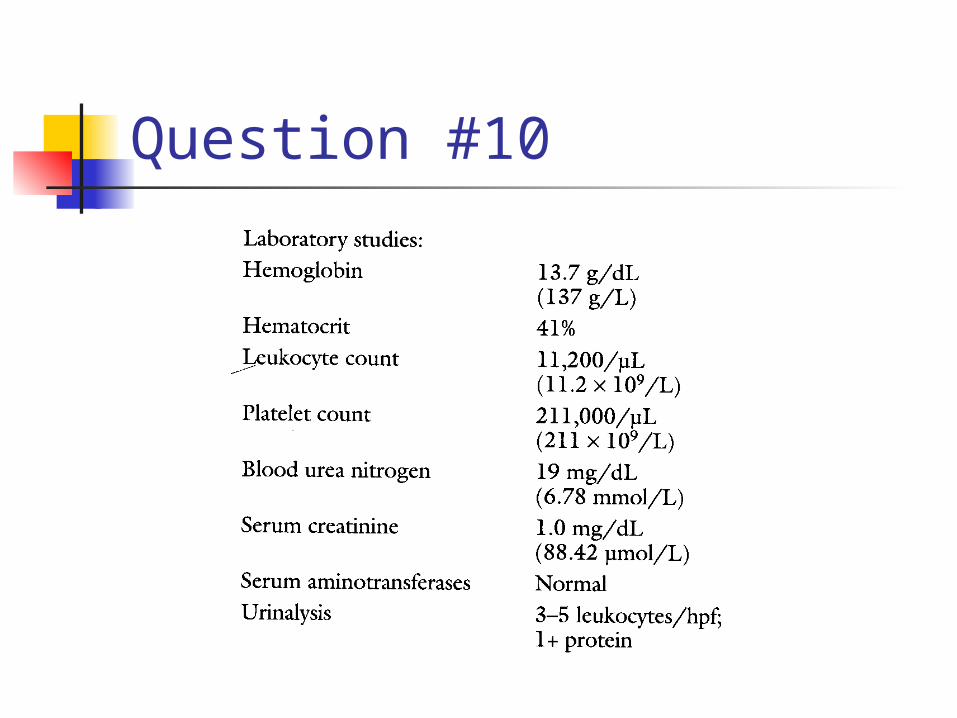
Question #10
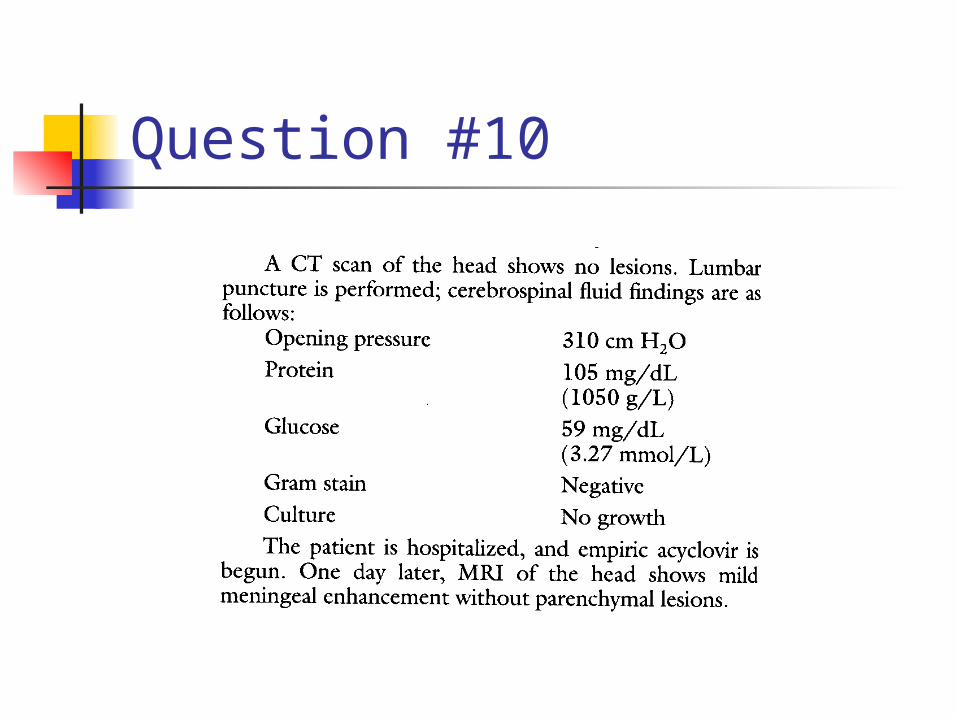
Question #10
Question #10
Viral Encephalitis Symptoms of encephalitis
AMS – subtle to unresponsive Usually no meningeal signs Seizures common Focal neurologic findings; abn reflexes
CT/MRI Findings VZV, HSV, HHV-6 – temporal lobe West Nile – temporal lobe, basal
ganglia, thalamus, brainstem, cerebellum
Viral Encephalitis
CSF Findings Elevated protein but <150 mg/dl Normal glucose Elevated WBC count but <250/mm3 No red cells except in HSV
References
MKSAP 14 – Neurology MKSAP 14 – Infectious Disease Uptodate Online