Embed Size (px)
Citation preview

REVIEW ARTICLE
Body composition, metabolic syndrome and type 2 diabetes in KlinefeltersyndromeClaus H Gravholt ([email protected])1, Anne S Jensen1, Christian Høst1, Anders Bojesen2
1.Department of Endocrinology and Internal Medicine, Aarhus University Hospital, Aarhus Sygehus NBG, Aarhus C, Denmark2.Department of Clinical Genetics, Vejle Hospital, Sygehus Lillebaelt, Vejle, Denmark
KeywordsBody composition, Diabetes, Klinefelter syndrome,Metabolic syndrome, Testosterone
CorrespondenceClaus H Gravholt, Department of Endocrinology andInternal Medicine and Medical ResearchLaboratories, Aarhus University Hospital, AarhusHospital NBG, Noerrebrogade 44, DK-8000 AarhusC, Denmark.Tel: +4589492023 |Fax: +4589492010 |Email: [email protected]
Received6 September 2010; revised 15 February 2011;accepted 17 February 2011.
DOI:10.1111/j.1651-2227.2011.02233.x
ABSTRACTKlinefelter syndrome (KS) affects 1:660 men, making it the most common sex-chromo-
some disorder in man, and is a common cause of infertility, hypogonadism and learning
disability. Men with KS are described as tall, slim, narrow shouldered, broad hipped, with
hypergonadotropic hypogonadism and small testes, and recently the description has been
expanded to include increased risk of the metabolic syndrome, type 2 diabetes and an
unfavourable change in body composition, with accumulation of body fat and decreased
muscle mass and a concomitant decrease in insulin sensitivity, muscle strength and oxygen
consumption capacity. Here, we review the data on body composition, bone turnover, liver
function, insulin resistance and metabolic syndrome in relation to testosterone in both
patients with KS and normal men. Treatment with testosterone in hypogonadal men (other
than KS) improves body composition in both clinical and experimental studies. Despite the
lack of such studies in KS, we recommend testosterone treatment to patients with KS with
low serum testosterone or increased LH and change in body composition and thus possibly
prevent common diseases like type 2 diabetes, osteoporosis and heart disease.Conclusion: Preventable causes of the increased morbidity and mortality, such as
osteoporosis, chronic obstructive airway disease or type 2 diabetes, should be screened
for. Despite the lack of randomized controlled studies, we recommend testosterone treat-
ment in case of increased LH or low serum testosterone, and weight reduction pro-
grammes if overweight.
INTRODUCTIONSince the first description of Klinefelter syndrome (KS) in1942 (1), KS (47,XXY) has been known as a relatively com-mon cause of infertility, hypergonadotropic hypogonadism,gynaecomastia and learning disability in men. New epide-miological studies from England and Denmark have shownan increased morbidity and mortality owing to a variety ofdiseases and conditions (among them, type 2 diabetes) (2–5). Many have advocated for a new broader look at KS,where many patients do not fit the classical or typical ‘text-book’ image or phenotype of a patient with KS as a tall,slender man with small testes, gynaecomastia, narrowshoulders, long arms and legs and with sparse body hair.Most men with KS go through life without diagnosis, andonly 25% of the expected number of patients with KS arediagnosed in Denmark (5), a figure that may be even lowerin other countries where health care systems are not social-ized. This proportion of diagnosed versus undiagnosedcases is likely comparable with that of other countries,which challenges our current knowledge of the KS pheno-type and hampers the extrapolation hereof to the remaininggroup of undiagnosed men with KS. The only stigmata
seemingly shared by virtually all adult KS are small testes,increased LH and FSH, and azoospermia (6,7). Althoughbeing the most common sex-chromosome disorder, with aprevalence of 1:660 men (8), knowledge is still embarrass-ingly sparse.
Here, we will present data on the metabolic syndrome,type 2 diabetes and related risk factors, body composition inrelation to hypogonadism and the syndrome per se. Theeffect of testosterone therapy will be discussed.
THE RISK OF DIABETES OR METABOLIC SYNDROME IN KSEpidemiological studiesEpidemiological study concerning mortality in KS has beenperformed in Great Britain (9) and in Denmark (3) includ-ing more than 3500 patients and 780 patients, respectively.Both showed a generally increased mortality risk with ahazard rate (HR) of 1.4–1.5 and a specifically increased riskof dying from diabetes with a standardized mortality rate of5.8 and HR of 1.6, respectively. We also studied morbidity,based on hospital discharge diagnoses, and showed anincreased risk of being discharged from hospital with the
Acta Pædiatrica ISSN 0803–5253
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877 871
diagnosis of type 1 diabetes, type 2 diabetes or obesity, withHR for type 1 diabetes and type 2 diabetes being 2.21 and3.71, respectively, and HR for obesity of 3.41 (5).
Clinical studiesAn association between KS and diabetes has been reportedin a number of studies during the last 40 years. In 1966,Jackson et al. (10) examined eight men with KS and foundone with mild diabetes. Becker described in 1966 50patients with KS and among them five with diabetes (11).Zuppinger et al. (12) examined 24 patients with KS andfound frank diabetes in 2 and a diabetic glucose tolerancetest in 4 additional patients. In 1969, Nielsen et al. (13)described an increased prevalence (39%) of a diabetic oralglucose tolerance test in 31 patients with KS, while othersfound decreased insulin sensitivity and elevated fastinginsulin levels in seven patients with KS and seven hypogo-nadotropic hypogonadal patients compared to seven nor-mal controls (14). Furthermore, in a study on 13 patientswith KS, significantly increased fasting insulin levels werefound, but with no difference in insulin sensitivity (15).
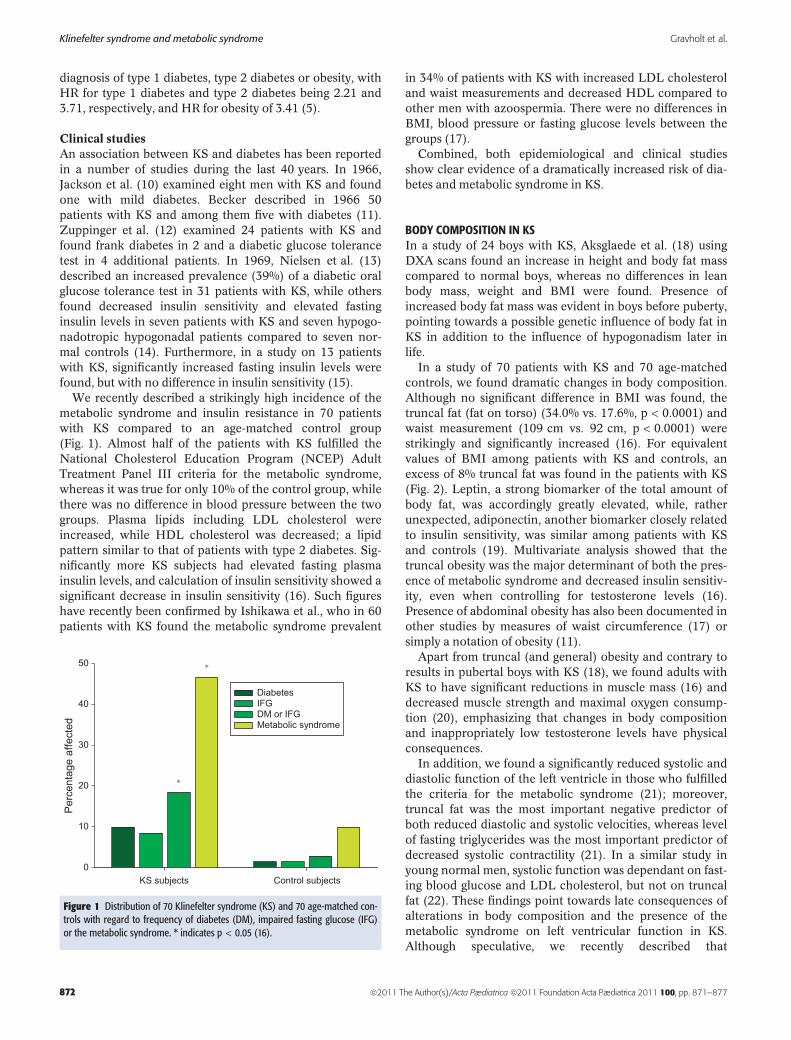
We recently described a strikingly high incidence of themetabolic syndrome and insulin resistance in 70 patientswith KS compared to an age-matched control group(Fig. 1). Almost half of the patients with KS fulfilled theNational Cholesterol Education Program (NCEP) AdultTreatment Panel III criteria for the metabolic syndrome,whereas it was true for only 10% of the control group, whilethere was no difference in blood pressure between the twogroups. Plasma lipids including LDL cholesterol wereincreased, while HDL cholesterol was decreased; a lipidpattern similar to that of patients with type 2 diabetes. Sig-nificantly more KS subjects had elevated fasting plasmainsulin levels, and calculation of insulin sensitivity showed asignificant decrease in insulin sensitivity (16). Such figureshave recently been confirmed by Ishikawa et al., who in 60patients with KS found the metabolic syndrome prevalent
in 34% of patients with KS with increased LDL cholesteroland waist measurements and decreased HDL compared toother men with azoospermia. There were no differences inBMI, blood pressure or fasting glucose levels between thegroups (17).
Combined, both epidemiological and clinical studiesshow clear evidence of a dramatically increased risk of dia-betes and metabolic syndrome in KS.
BODY COMPOSITION IN KSIn a study of 24 boys with KS, Aksglaede et al. (18) usingDXA scans found an increase in height and body fat masscompared to normal boys, whereas no differences in leanbody mass, weight and BMI were found. Presence ofincreased body fat mass was evident in boys before puberty,pointing towards a possible genetic influence of body fat inKS in addition to the influence of hypogonadism later inlife.
In a study of 70 patients with KS and 70 age-matchedcontrols, we found dramatic changes in body composition.Although no significant difference in BMI was found, thetruncal fat (fat on torso) (34.0% vs. 17.6%, p < 0.0001) andwaist measurement (109 cm vs. 92 cm, p < 0.0001) werestrikingly and significantly increased (16). For equivalentvalues of BMI among patients with KS and controls, anexcess of 8% truncal fat was found in the patients with KS(Fig. 2). Leptin, a strong biomarker of the total amount ofbody fat, was accordingly greatly elevated, while, ratherunexpected, adiponectin, another biomarker closely relatedto insulin sensitivity, was similar among patients with KSand controls (19). Multivariate analysis showed that thetruncal obesity was the major determinant of both the pres-ence of metabolic syndrome and decreased insulin sensitiv-ity, even when controlling for testosterone levels (16).Presence of abdominal obesity has also been documented inother studies by measures of waist circumference (17) orsimply a notation of obesity (11).
Apart from truncal (and general) obesity and contrary toresults in pubertal boys with KS (18), we found adults withKS to have significant reductions in muscle mass (16) anddecreased muscle strength and maximal oxygen consump-tion (20), emphasizing that changes in body compositionand inappropriately low testosterone levels have physicalconsequences.
In addition, we found a significantly reduced systolic anddiastolic function of the left ventricle in those who fulfilledthe criteria for the metabolic syndrome (21); moreover,truncal fat was the most important negative predictor ofboth reduced diastolic and systolic velocities, whereas levelof fasting triglycerides was the most important predictor ofdecreased systolic contractility (21). In a similar study inyoung normal men, systolic function was dependant on fast-ing blood glucose and LDL cholesterol, but not on truncalfat (22). These findings point towards late consequences ofalterations in body composition and the presence of themetabolic syndrome on left ventricular function in KS.Although speculative, we recently described that
Control subjectsKS subjects
Per
cent
age
affe
cted
0
10
20
30
40
50
Diabetes IFG DM or IFG Metabolic syndrome
∗
∗
Figure 1 Distribution of 70 Klinefelter syndrome (KS) and 70 age-matched con-trols with regard to frequency of diabetes (DM), impaired fasting glucose (IFG)or the metabolic syndrome. * indicates p < 0.05 (16).
Klinefelter syndrome and metabolic syndrome Gravholt et al.
872 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877
hypothyroidism secondary to hypothalamic–pituitary dys-function may also be present in KS, which could contributeto slight alterations in body composition in addition to theabove-mentioned factors (23). Most recently, we have alsodocumented an increased risk of non-alcoholic fatty liverdisease, which is linked to the presence of the metabolicsyndrome and type 2 diabetes (24).
HYPOGONADISM AND CHANGE IN BODY COMPOSITIONProspective studies in populations of normal men indi-cate that low levels of testosterone (and SHBG) predictfuture abdominal adiposity (25), the metabolic syndrome(26) and type 2 diabetes (25–27). This effect is probablynot direct, because two studies independently showedthat measures of insulin sensitivity, hepatic glucose out-put and insulin secretion were independent of sex hor-mone levels after controlling for upper body obesity(28,29). Similarly, the significant correlations of testos-terone with insulin sensitivity, measures of body fat andmaximal oxygen consumption found in our patients withKS disappeared in multivariate analyses when control-ling for confounders (16).
In KS, it is intriguing to assume that hypogonadism pre-cedes obesity, but the findings of increased body fat masseven before puberty (18) make this assumption weaker.And data on the early mini-puberty during the first monthsof life are equivocal with two studies showing low circulat-ing testosterone (30,31) and one study normal levels (32).Thus, the temporal occurrences of events are unknown. For
instance, does the ensuing hypogonadism lead to abdominaladiposity and hence to the well-known side effects of adi-posity (the metabolic syndrome and insulin resistance), ordoes abdominal adiposity lead to decreased testosteroneproduction (as well as the aforementioned known effects ofadiposity)? – Indeed, both scenarios may be present and bepart of a self-perpetuating vicious circle. The Leydig cellsmay become insulin resistant as well as other cells in thebody. In vitro studies showed a stimulatory effect of insulinon testosterone production in both rat and mouse Leydigcells (33); moreover, young insulin-resistant men producedless testosterone when stimulated with human choriogona-dotropin (hCG) compared to non-obese men (34). In addi-tion, lower levels of testosterone, free testosterone andSHBG have been found in both obese (35) and diabeticmen (36). However, prospective studies have not been per-formed to confirm that abdominal adiposity leads todecreased testosterone production.
Taken together, these studies suggest the presenceof a vicious circle, whereby increased abdominaladiposity aggravates overall and Leydig cell insulinsensitivity, eventually leading to a further deterioration ofT production.
Findings of increased amounts of body fat in prepubertalboys with KS point out other causes than low testosterone.Genetic (over-expression of X-bound genes, skewedX-chromosome inactivation or CAG-repeat polymorphismin the androgen receptor) (37) and psycho-social causes areboth plausible, but no studies addressing these possible rela-tions are at hand. Apart from the association between low
SHBG
U-KS T-KS Controls
nmol/L
0
20
40
60
80
0.040. 38
Testosterone
U-KS T-KS Controls
nmol/L
0
10
20
30
40
<0.00010.15
17β−estradiol
U-KS T-KS Controls
pmol/L
0
50
100
150
200
250
0.820.04
LH
U-KS T-KS Controls
iU/L
0
5
10
15
20
25
30
<0.00010.0001
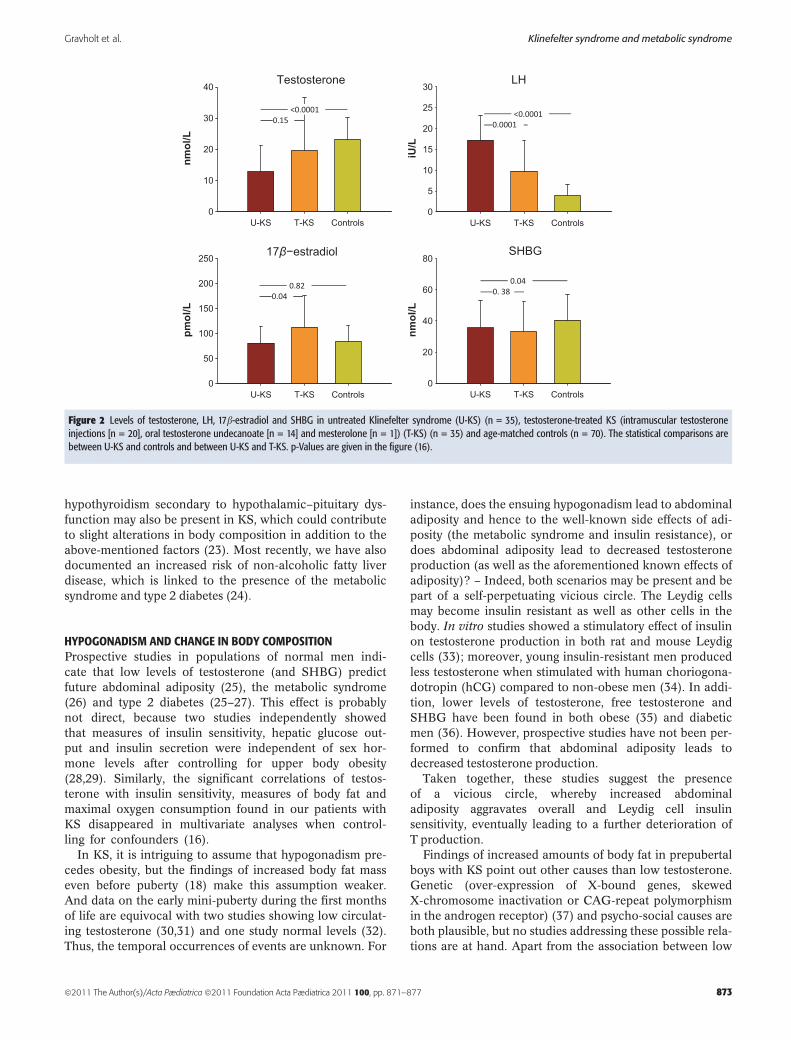
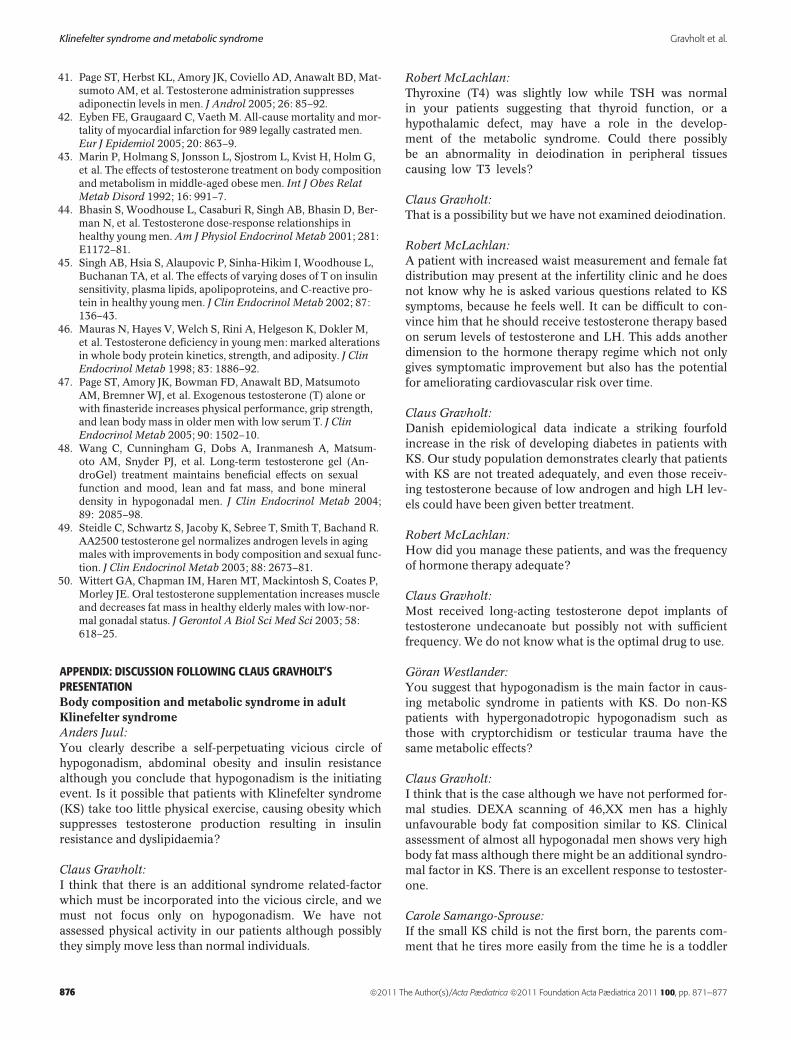
Figure 2 Levels of testosterone, LH, 17b-estradiol and SHBG in untreated Klinefelter syndrome (U-KS) (n = 35), testosterone-treated KS (intramuscular testosteroneinjections [n = 20], oral testosterone undecanoate [n = 14] and mesterolone [n = 1]) (T-KS) (n = 35) and age-matched controls (n = 70). The statistical comparisons arebetween U-KS and controls and between U-KS and T-KS. p-Values are given in the figure (16).
Gravholt et al. Klinefelter syndrome and metabolic syndrome
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877 873

testosterone, body composition, the metabolic syndromeand insulin sensitivity, hypogonadism has been associatedwith an adverse cardiovascular risk profile, with increasedC-reactive protein and triglycerides but decreased HDLcholesterol (38). Opposingly, testosterone is negativelyassociated with adiponectin, a cardioprotective and anti-diabetic adipocytokine (39). Furthermore, testosteronetreatment has been shown to suppress (relatively elevated)adiponectin levels in both hypogonadal men and in cas-trated mice (40,41). Adiponectin is closely and inverselycorrelated with obesity. We found normal (non-suppressed)levels of total adiponectin and normal blood pressure in KS,albeit in the presence of a host of acknowledged cardiacrisk factors, and the high molecular weight (HMW) subformof adiponectin, mediating insulin-sensitizing effects onhepatocytes, was non-suppressed (19).
In KS, hypogonadism is relative rather than absolute,with testosterone typically in the low-normal or subnormalrange. The non-suppressed level of adiponectin may there-fore be the result of the opposing effects of (subnormal) tes-tosterone levels and obesity. Further, it seems plausible thatnon-suppressed adiponectin acts in concert with the non-elevated blood pressure to somehow counteract (and evenovercome) the unfavourable effects of hypogonadism onother cardiac risk factors. Although speculative, thishypothesis is supported by the finding of decreased mortal-ity risk from ischaemic heart disease in both patients withKS (9) and legally castrated men (42), despite a generallyincreased mortality in both groups. We also found thatdespite testosterone treatment, KS had low testosterone andelevated LH levels in comparison with controls and onlyslightly (significantly) lower LH levels than untreated KS,but similar testosterone levels (Fig. 2), while 17b-estradioland SHBG levels were similar. This would indicate that thetreatment regimen offered to many men with KS is insuffi-cient.
TESTOSTERONE TREATMENT AND BODY COMPOSITIONApart from case reports, no prospective randomized studieson the effect of testosterone treatment on insulin sensitivity,body composition or other surrogate markers of cardiovas-cular health in KS have been published, but other popula-tions have been studied. Middle-aged abdominal obese menhad a significant reduction in visceral adiposity andimprovement in insulin sensitivity after 8 months of testos-terone treatment compared to placebo (43). Experimentallyinduced hypogonadism in 61 younger men followed by sub-stitution with different doses of testosterone (five differentdose regimens from sub- to supra-physiological doses)showed a dose dependent increase in fat-free mass, whereasfat mass was negatively correlated with testosterone dose(44). Despite these changes in body composition, no differ-ence in insulin resistance was detected between the groups(45). In another study, induction of hypogonadism in sixhealthy young men for 10 weeks increased fat mass,whereas lean body mass, resting energy expenditure, proteinanabolism and muscle strength decreased (46).
Additionally, in much larger populations of elderly men,several placebo-controlled studies have concurrently showntestosterone treatment to increase lean body mass and todecrease fat mass (47–50). We found a trend (albeit non-sig-nificant) towards a reduction in truncal fat, total choles-terol, fasting plasma glucose and leptin among those ontestosterone treatment compared to those without treat-ment, perhaps indicative of insufficient testosterone supple-mentation in the treated group (16). These studies suggestthat testosterone treatment in hypogonadal men mayreverse the unfavourable body composition and (with lessevidence) improve insulin resistance, although this is notsupported by comparable trials in patients with KS.
CONCLUSIONThe metabolic syndrome, type 2 diabetes and an unfavour-able body composition are frequent in KS, and based onavailable evidence, we recommend hormone replacementtherapy in patients with low serum testosterone orincreased LH, and with other signs of hypogonadism,which, in our opinion, should also include increased fatmass and decreased muscle mass. The ultimate goal is areduction in morbidity and mortality and an improvementin quality of life of patients with KS. Currently, no studiesindicate such positive effects of testosterone treatment inKS, but future studies will address these important issues.When blood is submitted for karyotype examination for KS,the patient usually has symptoms that are being investi-gated. We plan to visit all the cytogenetic laboratories inDenmark to identify the underlying indications for karyo-typic analysis. Preventable causes of the increased morbidityand mortality, such as osteoporosis, chronic obstructive air-way disease or type 2 diabetes, should be screened for.Despite the lack of randomized controlled studies, we rec-ommend testosterone treatment in case of increased LH orlow serum testosterone, and weight reduction programmesif the patient is overweight.
References
1. Klinefelter HF, Reifenstein EC, Albright F. Syndrome charac-terized by gynecomastia,aspermatogenesis without a-leydigism,and increased excretion of follicle-stimulating hormone. J ClinEndocrinol 1942; 2: 615–27.
2. Swerdlow AJ, Hermon C, Jacobs PA, Alberman E, Beral V,Daker M, et al. Mortality and cancer incidence in persons withnumerical sex chromosome abnormalities: a cohort study. AnnHum Genet 2001; 65: 177–88.
3. Bojesen A, Juul S, Birkebaek N, Gravholt CH. Increased mor-tality in Klinefelter syndrome. J Clin Endocrinol Metab 2004;89: 3830–4.
4. Swerdlow AJ, Schoemaker MJ, Higgins CD, Wright AF, JacobsPA. Cancer incidence and mortality in men with Klinefeltersyndrome: a cohort study. J Natl Cancer Inst 2005; 97: 1204–10.
5. Bojesen A, Juul S, Birkebaek NH, Gravholt CH. Morbidity inKlinefelter syndrome: a Danish register study based on hospitaldischarge diagnoses. J Clin Endocrinol Metab 2006; 91: 1254–60.
Klinefelter syndrome and metabolic syndrome Gravholt et al.
874 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877
6. Smyth CM, Bremner WJ. Klinefelter syndrome. Arch InternMed 1998; 158: 1309–14.
7. Bojesen A, Gravholt CH. Klinefelter syndrome in clinical prac-tice. Nat Clin Pract Urol 2007; 4: 192–204.
8. Handelsman DJ. Update in andrology. J Clin Endocrinol Metab2007; 92: 4505–11.
9. Swerdlow AJ, Higgins CD, Schoemaker MJ, Wright AF, JacobsPA. Mortality in patients with Klinefelter syndrome in Britain: acohort study. J Clin Endocrinol Metab 2005; 90: 6516–22.
10. Jackson IM, Buchanan KD, McKiddie MT, Prentice CR. Carbo-hydrate metabolism in Klinefelter’s syndrome. J Endocrinol1966; 35: 169–72.
11. Becker KL, Hoffman DL, Underdahl LO, Mason HL. Klinefel-ter’s syndrome. Clinical and laboratory findings in 50 patients.Arch Intern Med 1966; 118: 314–21.
12. Zuppinger K, Engel E, Forbes AP, Mantooth L, Claffey J. Kline-felter’s syndrome, a clinical and cytogenetic study in twenty-four cases. Acta Endocrinol (Copenh) 1967; 54 Suppl 113:5–48.
13. Nielsen J, Johansen K, Yde H. Frequency of diabetes mellitus inpatients with Klinefelter’s syndrome of different chromosomeconstitutions and the XYY syndrome. Plasma insulin andgrowth hormone level after a glucose load. J Clin EndocrinolMetab 1969; 29: 1062–73.
14. Pei D, Sheu WH, Jeng CY, Liao WK, Fuh MM. Insulin resis-tance in patients with Klinefelter’s syndrome and idiopathicgonadotropin deficiency. J Formos Med Assoc 1998; 97:534–40.
15. Yesilova Z, Oktenli C, Sanisoglu SY, Musabak U, Cakir E,Ozata M, et al. Evaluation of insulin sensitivity in patients withKlinefelter’s syndrome: a hyperinsulinemic euglycemic clampstudy. Endocrine 2005; 27: 11–6.
16. Bojesen A, Kristensen K, Birkebaek NH, Fedder J, Mosekilde L,Bennett P, et al. The metabolic syndrome is frequent in Kline-felter’s syndrome and is associated with abdominal obesity andhypogonadism. Diabetes Care 2006; 29: 1591–8.
17. Ishikawa T, Yamaguchi K, Kondo Y, Takenaka A, Fujisawa M.Metabolic syndrome in men with Klinefelter’s syndrome. Urol-ogy 2008; 71: 1109–13.
18. Aksglaede L, Molgaard C, Skakkebaek NE, Juul A. Normalbone mineral content but unfavourable muscle ⁄ fat ratio inKlinefelter syndrome. Arch Dis Child 2008; 93: 30–4.
19. Host C, Bojesen A, Frystyk J, Flyvbjerg A, Christiansen JS,Gravholt CH. Effect of sex hormone treatment on circulatingadiponectin and subforms in Turner and Klinefelter syndrome.Eur J Clin Invest 2010; 40: 211–9.
20. Bojesen A, Birkebaek N, Kristensen K, Heickendorff L, Mose-kilde L, Christiansen JS, et al. Bone mineral density in Klinefel-ter syndrome is reduced and primarily determined by musclestrength and resorptive markers, but not directly by testoster-one. Osteoporos Int 2010; Jul 24. [Epub ahead of print].
21. Andersen NH, Bojesen A, Kristensen K, Birkebaek NH, FedderJ, Bennett P, et al. Left ventricular dysfunction in Klinefeltersyndrome is associated to insulin resistance, abdominaladiposity and hypogonadism. Clin Endocrinol (Oxf) 2008; 69:785–91.
22. Andersen NH, Bojesen A, Christiansen JS, Gravholt CH. Gly-cemia, lipidemia and systolic left ventricular function evaluatedby myocardial strain rate: a tissue Doppler echocardiographicstudy. Ultrasound Med Biol 2008; 34: 151–4.
23. Bjorn AM, Bojesen A, Gravholt CH, Laurberg P. Hypothyroid-ism secondary to hypothalamic-pituitary dysfunction may bepart of the phenotype in klinefelter syndrome: a case-controlstudy. J Clin Endocrinol Metab 2009; 94: 2478–81.
24. Jensen AS, Bojesen A, Gravholt CH. Mild liver dysfunction inKlinefelter syndrome is associated with abdominal obesity and
elevated total cholesterol. Endocrine Society Meeting 2009; P2-768 (abstarct).
25. Tsai EC, Boyko EJ, Leonetti DL, Fujimoto WY. Low serum tes-tosterone level as a predictor of increased visceral fat in Japa-nese-American men. Int J Obes Relat Metab Disord 2000; 24:485–91.
26. Laaksonen DE, Niskanen L, Punnonen K, Nyyssonen K,Tuomainen TP, Valkonen VP, et al. Testosterone and sexhormone-binding globulin predict the metabolic syndromeand diabetes in middle-aged men. Diabetes Care 2004; 27:1036–41.
27. Stellato RK, Feldman HA, Hamdy O, Horton ES, McKinlay JB.Testosterone, sex hormone-binding globulin, and the develop-ment of type 2 diabetes in middle-aged men: prospective resultsfrom the Massachusetts male aging study. Diabetes Care 2000;23: 490–4.
28. Abate N, Haffner SM, Garg A, Peshock RM, Grundy SM. Sexsteroid hormones, upper body obesity, and insulin resistance.J Clin Endocrinol Metab 2002; 87: 4522–7.
29. Tsai EC, Matsumoto AM, Fujimoto WY, Boyko EJ. Associationof bioavailable, free, and total testosterone with insulin resis-tance: influence of sex hormone-binding globulin and body fat.Diabetes Care 2004; 27: 861–8.
30. Lahlou N, Fennoy I, Carel JC, Roger M. Inhibin B and anti-mul-lerian hormone, but not testosterone levels, are normal ininfants with nonmosaic klinefelter syndrome. J Clin EndocrinolMetab 2004; 89: 1864–8.
31. Ross JL, Samango-Sprouse C, Lahlou N, Kowal K, Elder FF,Zinn A. Early androgen deficiency in infants and youngboys with 47,XXY Klinefelter syndrome. Horm Res 2005; 64:39–45.
32. Aksglaede L, Petersen JH, Main KM, Skakkebaek NE, Juul A.High normal testosterone levels in infants with non-mosaicKlinefelter’s syndrome. Eur J Endocrinol 2007; 157: 345–50.
33. Bebakar WM, Honour JW, Foster D, Liu YL, Jacobs HS. Regu-lation of testicular function by insulin and transforming growthfactor-beta. Steroids 1990; 55: 266–70.
34. Pitteloud N, Hardin M, Dwyer AA, Valassi E, Yialamas M,Elahi D, et al. Increasing insulin resistance is associated with adecrease in Leydig cell testosterone secretion in men. J ClinEndocrinol Metab 2005; 90: 2636–41.
35. Pasquali R, Casimirri F, Cantobelli S, Melchionda N, MorselliLabate AM, Fabbri R, et al. Effect of obesity and body fat distri-bution on sex hormones and insulin in men. Metabolism 1991;40: 101–4.
36. Dhindsa S, Prabhakar S, Sethi M, Bandyopadhyay A, Chaudh-uri A, Dandona P. Frequent occurrence of hypogonadotropichypogonadism in type 2 diabetes. J Clin Endocrinol Metab2004; 89: 5462–8.
37. Zitzmann M, Depenbusch M, Gromoll J, Nieschlag E. X-chro-mosome inactivation patterns and androgen receptor function-ality influence phenotype and social characteristics as well aspharmacogenetics of testosterone therapy in klinefelterpatients. J Clin Endocrinol Metab 2004; 89: 6208–17.
38. Laaksonen DE, Niskanen L, Punnonen K, Nyyssonen K, Tuo-mainen TP, Salonen R, et al. Sex hormones, inflammation andthe metabolic syndrome: a population-based study. Eur J Endo-crinol 2003; 149: 601–8.
39. Nishizawa H, Shimomura I, Kishida K, Maeda N, Kuriyama H,Nagaretani H, et al. Androgens decrease plasma adiponectin,an insulin-sensitizing adipocyte-derived protein. Diabetes2002; 51: 2734–41.
40. Lanfranco F, Zitzmann M, Simoni M, Nieschlag E. Serumadiponectin levels in hypogonadal males: influence of testoster-one replacement therapy. Clin Endocrinol (Oxf) 2004; 60: 500–7.
Gravholt et al. Klinefelter syndrome and metabolic syndrome
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877 875
41. Page ST, Herbst KL, Amory JK, Coviello AD, Anawalt BD, Mat-sumoto AM, et al. Testosterone administration suppressesadiponectin levels in men. J Androl 2005; 26: 85–92.
42. Eyben FE, Graugaard C, Vaeth M. All-cause mortality and mor-tality of myocardial infarction for 989 legally castrated men.Eur J Epidemiol 2005; 20: 863–9.
43. Marin P, Holmang S, Jonsson L, Sjostrom L, Kvist H, Holm G,et al. The effects of testosterone treatment on body compositionand metabolism in middle-aged obese men. Int J Obes RelatMetab Disord 1992; 16: 991–7.
44. Bhasin S, Woodhouse L, Casaburi R, Singh AB, Bhasin D, Ber-man N, et al. Testosterone dose-response relationships inhealthy young men. Am J Physiol Endocrinol Metab 2001; 281:E1172–81.
45. Singh AB, Hsia S, Alaupovic P, Sinha-Hikim I, Woodhouse L,Buchanan TA, et al. The effects of varying doses of T on insulinsensitivity, plasma lipids, apolipoproteins, and C-reactive pro-tein in healthy young men. J Clin Endocrinol Metab 2002; 87:136–43.
46. Mauras N, Hayes V, Welch S, Rini A, Helgeson K, Dokler M,et al. Testosterone deficiency in young men: marked alterationsin whole body protein kinetics, strength, and adiposity. J ClinEndocrinol Metab 1998; 83: 1886–92.
47. Page ST, Amory JK, Bowman FD, Anawalt BD, MatsumotoAM, Bremner WJ, et al. Exogenous testosterone (T) alone orwith finasteride increases physical performance, grip strength,and lean body mass in older men with low serum T. J ClinEndocrinol Metab 2005; 90: 1502–10.
48. Wang C, Cunningham G, Dobs A, Iranmanesh A, Matsum-oto AM, Snyder PJ, et al. Long-term testosterone gel (An-droGel) treatment maintains beneficial effects on sexualfunction and mood, lean and fat mass, and bone mineraldensity in hypogonadal men. J Clin Endocrinol Metab 2004;89: 2085–98.
49. Steidle C, Schwartz S, Jacoby K, Sebree T, Smith T, Bachand R.AA2500 testosterone gel normalizes androgen levels in agingmales with improvements in body composition and sexual func-tion. J Clin Endocrinol Metab 2003; 88: 2673–81.
50. Wittert GA, Chapman IM, Haren MT, Mackintosh S, Coates P,Morley JE. Oral testosterone supplementation increases muscleand decreases fat mass in healthy elderly males with low-nor-mal gonadal status. J Gerontol A Biol Sci Med Sci 2003; 58:618–25.
APPENDIX: DISCUSSION FOLLOWING CLAUS GRAVHOLT’SPRESENTATIONBody composition and metabolic syndrome in adultKlinefelter syndromeAnders Juul:You clearly describe a self-perpetuating vicious circle ofhypogonadism, abdominal obesity and insulin resistancealthough you conclude that hypogonadism is the initiatingevent. Is it possible that patients with Klinefelter syndrome(KS) take too little physical exercise, causing obesity whichsuppresses testosterone production resulting in insulinresistance and dyslipidaemia?
Claus Gravholt:I think that there is an additional syndrome related-factorwhich must be incorporated into the vicious circle, and wemust not focus only on hypogonadism. We have notassessed physical activity in our patients although possiblythey simply move less than normal individuals.
Robert McLachlan:Thyroxine (T4) was slightly low while TSH was normalin your patients suggesting that thyroid function, or ahypothalamic defect, may have a role in the develop-ment of the metabolic syndrome. Could there possiblybe an abnormality in deiodination in peripheral tissuescausing low T3 levels?
Claus Gravholt:That is a possibility but we have not examined deiodination.
Robert McLachlan:A patient with increased waist measurement and female fatdistribution may present at the infertility clinic and he doesnot know why he is asked various questions related to KSsymptoms, because he feels well. It can be difficult to con-vince him that he should receive testosterone therapy basedon serum levels of testosterone and LH. This adds anotherdimension to the hormone therapy regime which not onlygives symptomatic improvement but also has the potentialfor ameliorating cardiovascular risk over time.
Claus Gravholt:Danish epidemiological data indicate a striking fourfoldincrease in the risk of developing diabetes in patients withKS. Our study population demonstrates clearly that patientswith KS are not treated adequately, and even those receiv-ing testosterone because of low androgen and high LH lev-els could have been given better treatment.
Robert McLachlan:How did you manage these patients, and was the frequencyof hormone therapy adequate?
Claus Gravholt:Most received long-acting testosterone depot implants oftestosterone undecanoate but possibly not with sufficientfrequency. We do not know what is the optimal drug to use.
Goran Westlander:You suggest that hypogonadism is the main factor in caus-ing metabolic syndrome in patients with KS. Do non-KSpatients with hypergonadotropic hypogonadism such asthose with cryptorchidism or testicular trauma have thesame metabolic effects?
Claus Gravholt:I think that is the case although we have not performed for-mal studies. DEXA scanning of 46,XX men has a highlyunfavourable body fat composition similar to KS. Clinicalassessment of almost all hypogonadal men shows very highbody fat mass although there might be an additional syndro-mal factor in KS. There is an excellent response to testoster-one.
Carole Samango-Sprouse:If the small KS child is not the first born, the parents com-ment that he tires more easily from the time he is a toddler
Klinefelter syndrome and metabolic syndrome Gravholt et al.
876 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877

and walking, which is related to muscle tone and strength.Our adolescent boys who are started on appropriate andro-gen dosage feel better, and for the first time, they understandhow bad they were previously with a feeling of inadequacyand being under the weather. This is an important feature ofhow much the obesity is factored into being fatigued all ofthe time. We start our small children on a training pro-gramme at an early stage in order to build up their endur-ance, and this reduces their fat disposition.
Claus Gravholt:That is why we should give testosterone to a man of35 years old who is newly diagnosed as KS as a result ofattending the infertility clinic. He felt fine but is much betteronce he has been on androgen therapy for 6 months.
Robert McLachlan:These men do not realize what they have been missing untiltherapy starts.
Gravholt et al. Klinefelter syndrome and metabolic syndrome
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 871–877 877