Embed Size (px)
Citation preview
206
57
2a7
M!zDIASTINoscoPIc EVALUATIONOF STAGS IIIALUNG CANCER: DET'ININGAPOPULATICNFCRPRR~PEX?ATIVE
-TRIMS. ThanasLadfortheLungCancer StudyGroup. ChicagoIL, USA
To standardize anatanic eligibility for pre-op treatment trials in unresectable stage III non-small celllungcancer, theICSGdecided to try to identify patients with stage IIIAdiseasewhowereunresectable because of bulky mediastinal node disease (NZ+) but who had negative contralateral mediastinal nodes (N3-). N3+ patients were felt to have involvenent beyond the bounds of surgical treatment. Candidates for pre-op treatment trials were reguired to have surgical media- st_inal exploration to be eligible. The surgeon charted mediastinoscopy findings for each patient according to the ICSG/ATS lymph node map. Mediastinoscopies of 58 patients were analyzed. 66% had right-sided primaries. 48% had squamous histology. A total of 170 mediastinal node stations were biopsied (2.9 per patient). 78 bi- opsies were positive (mean 1.3) and 92 were negative (mean 1.6). Of the 92 negative node stations, 44 (48%) were contralateral to the primary (i.e. N3 nodes). 30 (68%) of these negative N3 nodes were paratracheal and 14 (32%) were hilar. 17 patients (29%) had mediastino- scopy limited to ipsilateral upper paratracheal nodes, which were judged unresectable. The remaining 71% had more complete mediastinal evaluation. This study con- cludes thatncdemapping canbe accoanlishedbymedia- stinoscopy, that N2 and N3 node stations can be dis- tinguished, and that specific anatanic populations can be defined for pre-op treatment trials in locally ad- vancedlung cancer. (Supported by NC1 Grant CA-36045)
208
The signification of coagulation and fibrinolytic parameters in patients with lung cancer.
Masaharu Nagayama, Mikio Toyoshima, Hideki Suganuma. Masaaki Ida, Takashi Yamada, Jun Hasegawa, Atuhiko Satoh. The 2nd department of internal medicine, Hamamatsu University, School of Medicine.
To clarify the signification of measurements of coagulation and fibrinolytic parameters in lung cancer, we studied the plasma levels of Ddimer(DD), thrombin- antithrombin III complex(TAT), plasmin-a2antiplasmin complex(PAP). together with conventional parameters, PT, APTT, FDP and fibrinogen and also the levels of tumor markers, CEA. WC and SLX. The subjects included 35 patients with lung cancer. In 13 patients out of 35, we investigated the changes of these parameters before and after chemotherapy simultaneously. The levels of DD, TAT and PAP were elevated even in early clinical stage and changed in parallel with the progression of clinical stage and the response to chemotherapy compared to other coagulation and fibriolytic parameters. There was no correlation between these three parameters and tumor markers. The data suggest that DD, TAT and PAP determinations are useful for evaluation of tumor progression and response to chemotherapy in patients with lung cancer.
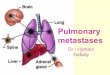
PRIMARY STAGING OF CARCINOMA OF THE BRONCHUS - IS COMPUTER TOMOGRAPHY OF THE BRAIN NECESSARY?
B. Wahlera, Lun enkllnik Hemw, 5870 Hemer F.R.G. From January 1 !3! 1 to December 1990,342 patients with brain metastases from carcinoma of the bronchus were reviewed to determine in which histologi+ groups.com- fxJt&~graphy of the brarn IS rndrcated In the pnmary
1. In small cell carcinoma, brain CT is recommended as brain metastases were detected in 51 % of patients. In those who develop brain metastases, 70 % manifest themselves within 6 months. 2. In adenocarcinoma, brain CT is recommended as even Ti tumours may metastasise to the brain. We detected 64 % of the brain me&stases during the primary staging and within 4 months, 60 % were detectable. 3. In contrast, in squamous carcinoma of the bronchus, brain metastases in patients with stage 1 or stage 2 disease without neurol
“B vanced disease, 54 % o ical symptoms are rare. In ad- the metastases were detected
during primary staging and within 4 months, 60 % were detectable. In tumours of the lung that are otherwise operable, a brain metastasis that can be surgically removed should be confirmed by magnetic resonance imaging as this method is more sensitive n detecting diise smaller meta&ases. We recommend that the brarn metastases be first removed followed by lung resection.
209
m B (HI) METASTASSS IN PATImS wITBSHAr&cELLLIJmcuK?ml(BcLc) DETECTSDBX~ICALANDIHlDHD- UWICAL mTmD8.
Aamdal, S., Myklabust, A., Beiske, K., Jakobsen, E., Langholm, R., Bmt, H.. Fodstad, 0. Dept. of Oncology and Institute for Cancer Research, The Norwegian Radium Hospital, 0310 Oslo 3, Norway.
1x1 a group of 81 previously untreated patients with SCLC, 50(62%) had extensive disease and 31(38%) limited disease as detected by X-ray of thorax, acintigraphic bone scan, ultrasound of liver and in most camea MR of the brain. SM aspirates and biopsies were taken from the-iliacal crest. Five Mabs (MCC-1, MCC-31, NrLulO, 81A6, MLuC-1) were selected and used for immuno- staining. Morphological examination of BM biopsies identified 8/81 patients (10%) with tumor infiltration, and examination of BM aspirates identified 12/81 (15%) whereas -kunostaining of aspirates, identified BM metaataees in 24/81 (30%). Less than 9% tumor infiltration was only detected by inxaunostaining. 23/24 patiente with SM metaetasee had exteneive disease and in only one (4%) was SM the sole location of metakakee. CoaolumLon: The diagnostic sensitivity of Famunostainina of AM aeniratee was twice is high aa each of-the two m&ho- logical methods-detecting very low numbers of tumor cells. Aa follow un of this study the possible usefulness of -k%unobeads and immunotoxina in ax viva removal of SCLC cells from SM is now ufiae?Tiivestigation.






![MAYA KOTAN CATÁLOGO [SCLC CHIAPAS MEXICO]](https://img.pdfslide.net/doc/110x75/568bf4a21a28ab89339ec8ae/maya-kotan-catalogo-sclc-chiapas-mexico.jpg)