-
8/4/2019 Bone Metastasis Presentation 3
1/23
Metastatic Bone
Disease
Aiman AwadDarlington Memorial Hospital
-
8/4/2019 Bone Metastasis Presentation 3
2/23
Pathophysiology How tumour cells migrate to bone?
How tumour cells grow in bone?
Diagnosis. Primary or secondary.
Solitary or multiple.
If secondary, where is the primary? The local extension of the
metastatic tumour.
Differential diagnosis.
-
8/4/2019 Bone Metastasis Presentation 3
3/23
Pathophysiology
How tumour cells migrate to bone?
By 3 main mechanisms:
(1) direct extension,
(2) retrograde venous flow, and(3) seeding with tumour emboli
via the blood
circulation
-
8/4/2019 Bone Metastasis Presentation 3
4/23
Sources of Bone Metastases
Breast
Prostate
Kidny
Lung
Thyroid
Bladder
Gastrointestinal Tract.
http://www.3dscience.com/3D_Images/Human_Anatomy/System_Composites/index.php
-
8/4/2019 Bone Metastasis Presentation 3
5/23
Bone metastasis
the most common locations include thefollowing:
Spine Pelvis Ribs Proximal limb girdles
Metastases distal to the knee and elbow are
extremely uncommon, but approximately 50% ofthese acral
metastases are secondary to primarylung tumors. Carcinomas, such as
those of thebreast and prostate, rarely exhibit such a
distinctpattern.
-
8/4/2019 Bone Metastasis Presentation 3
6/23
-
8/4/2019 Bone Metastasis Presentation 3
7/23
How tumour cells grow in bone?
There are two forms of bone Metastasis
Osteolytic bone disease.
Osteoblastic bone disease.
-
8/4/2019 Bone Metastasis Presentation 3
8/23
Osteolytic bone disease
(1) Metastatic tumour cells releasehumoral factors that
stimulateosteoclastic recruitment anddifferentiation.
(2)
Osteoclasts begin to break downbone.
(3) Bone resorption results in therelease of growth factors
thatstimulate tumour cell growth.
(4) As the tumour proliferates, itproduces substances
thatincrease osteoclast-mediatedbone resorption.
-
8/4/2019 Bone Metastasis Presentation 3
9/23
Osteoblastic bone disease
1- Metastatic tumour cells releasegrowth factors that stimulate
theactivity of osteoclasts.
2-Tumor cells also secrete growthfactors that stimulate the
activity
of osteoblasts.3-Excessive new bone formation
occurs around tumour-celldeposits.
4-Osteoclastic activity releases
growth factors that stimulatetumor cell growth.
5-Osteoblastic activation releasesunidentified osteoblastic
growthfactors that also stimulatetumour cell growth.
-
8/4/2019 Bone Metastasis Presentation 3
10/23
Clinical Presentation
Pain initially related to activity thenprogressive day and
night.
Pathological fracture.
Mass.
Abnormal radiographic finding detected
during the evaluation of an unrelatedproblem.
-
8/4/2019 Bone Metastasis Presentation 3
11/23
Diagnosis of bone Metastasis
History and Physical Examination
Laboratory Investigation
X Ray Bone Scan
CT
MRI Biopsy
-
8/4/2019 Bone Metastasis Presentation 3
12/23
METASTASES OF UNKNOWN ORIGIN
a patient over the age of 40 with a new, painfulbone lesion,
multiple myeloma and metastaticcarcinoma are the most likely
diagnoses
Prostate cancer and breast cancer are the twomost common primary
sources for bonemetastasis.
If a patient has no known primary tumour, themost likely sources
are lungcancer and renalcell carcinoma.
-
8/4/2019 Bone Metastasis Presentation 3
13/23
-
8/4/2019 Bone Metastasis Presentation 3
14/23
Biopsy should not be done until theevaluation is complete:
1. The lesion may be a primary sarcoma of bone that mayrequire a
biopsy technique that allows for future limbsalvage surgery;
2. Another more accessible lesion may be found3. If renal cell
carcinoma is considered likely, the surgeon may
wish to consider preoperative embolization to avoidexcessive
bleeding;
4. If the diagnosis of multiple myeloma is made by
laboratorystudies, an unnecessary biopsy will be avoided;
5. The pathological diagnosis will be more accurate if aided
byappropriate imaging studies; and
6. the pathologist and surgeon may be more assured of adiagnosis
of metastasis made on frozen section analysis ifsupported by the
preoperative evaluation. This is importantif stabilization of an
impending fracture is planned for thesame procedure.
-
8/4/2019 Bone Metastasis Presentation 3
15/23
physical examination
The evaluation begins with a historyfocusing on any previous
malignancies.
Examination includes not only the involvedextremity, but also
the thyroid, lungs,abdomen, prostate in men, and a
breastexamination in women
-
8/4/2019 Bone Metastasis Presentation 3
16/23
Laboratory analysis
should include a FBC, ESR , electrolytes, liverenzymes, alkaline
phosphatase, a serum proteinelectrophoresis, and possibly
prostate-specificantigen.
A FBC may be helpful to rule out infection andleukemia.
The ESR usually is elevated in infection,metastatic carcinoma,
and small "blue cell"
tumors such as Ewing sarcoma, lymphoma,leukemia, and
histiocytosis.
-
8/4/2019 Bone Metastasis Presentation 3
17/23
A serum protein electrophoresis should be orderedif multiple
myeloma is part of the differentialdiagnosis.
Hypercalcemia may be present with metastaticdisease, multiple
myeloma, andhyperparathyroidism.
Alkaline phosphatase may be elevated inmetabolic bone disease,
metastatic disease,osteosarcoma, Ewing sarcoma, or lymphoma.
Blood urea nitrogen and creatinine may beelevated with renal
tumors, and a urinalysis mayreveal hematuria in this setting.
A basic metabolic panel may be indicated to
evaluate the overall health of a patient.
-
8/4/2019 Bone Metastasis Presentation 3
18/23
plain roentgenograms
provides useful diagnosticinformation for evaluation ofbone
lesions.
Most vertebral lesions in
adult patients aremetastases, myelomas, orhemangiomas.
The aggressiveness of thelesion, and whether it is likely
to be benign or malignant,usually can be determined bycareful
evaluation of the plainfilms.
http://www.emedicine.com/radio/images/336139-387840-5173.jpg
-
8/4/2019 Bone Metastasis Presentation 3
19/23
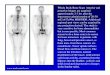
Technetium bone scans
With the exception ofmyeloma, all malignantneoplasms of
bonedemonstrate increased
uptake on technetium bonescans
A normal bone scan istherefore very reassuring;however, the
converse
statement is not true becausemost benign lesions of bonealso
demonstrate increaseduptake.
http://www.emedicine.com/radio/images/336139-387840-5191.jpg
-
8/4/2019 Bone Metastasis Presentation 3
20/23
Computed tomography (CT)
Helpful in assessingossification andcalcification and in
evaluating the integrityof the cortex
CT of the chest,abdomen, and pelvis
should be obtained forUnknown Metastasis.
Axial CT scan shows 2 rounded, mixedosteolytic-sclerotic lesions
in thethoracic vertebral body of a 44-year-old woman with lung
carcinoma.
http://www.emedicine.com/radio/images/336139-387840-5179.jpghttp://www.emedicine.com/radio/images/336139-387840-5179.jpghttp://www.emedicine.com/radio/images/336139-387840-5179.jpghttp://www.emedicine.com/radio/images/336139-387840-5179.jpghttp://www.emedicine.com/radio/images/336139-387840-5179.jpghttp://www.emedicine.com/radio/images/336139-387840-5179.jpg
-
8/4/2019 Bone Metastasis Presentation 3
21/23
Magnetic resonance imaging (MRI)
the most accurate technique fordetermining the limits of
diseaseboth within and outside bone.
not very useful in differentiatingbenign from malignant
lesions.
-
8/4/2019 Bone Metastasis Presentation 3
22/23
Biopsy
patient with a suspected primarymusculoskeletal malignancy
should be referredbefore biopsy to the institution where
definitivetreatment will take place
A biopsy should be planned as carefully as thedefinitive
procedure.
Regardless of whether a needle biopsy or anopen biopsy is done,
the biopsy track should be
considered contaminated with tumor cells The surgeon performing
the biopsy should be
familiar with incisions for limb salvage surgery
-
8/4/2019 Bone Metastasis Presentation 3
23/23
http://www.zwani.com/graphics/thank_you/images/1.gif