Embed Size (px)
Citation preview
BORDERNETwork Training on
Hepatitis C Dr. med. Wolfgang Güthoff / Alexander Leff ers, M.A.
www.bordernet.eu
www.aidshilfe-potsdam.de
This presentation arises from the BORDERNETwork project which has received funding from the European Union, in the framework of the Health Program, and co-funding of the Ministry of Environment, Health and Consumer Protection of the Federal State of Brandenburg. The sole responsibility of any use that may be made of the information lies with the authors (SPI, AIDS-Hilfe Potsdam e.V.)
Table of Contents
Epidemiology
Genotypes
Natural Course
Diagnostic
Therapy
Treatment
Overview: Epidemiology
WORLD:
• Estimated 170 – 180 Million individuals infected with HCV
• Estimated 100 - 130 Million individuals with chronic HCV
• Highest prevalence in Asia, Africa and Eastern Europa
EUROPE:
• Estimated 3 – 5 Million individuals with a chronic HCV infection
GERMANY:
• 400.000 – 500.000 persons with chronic HCV
• ~ yearly 7.000 – 8.000 with acute, new diagnosed HCV
infection
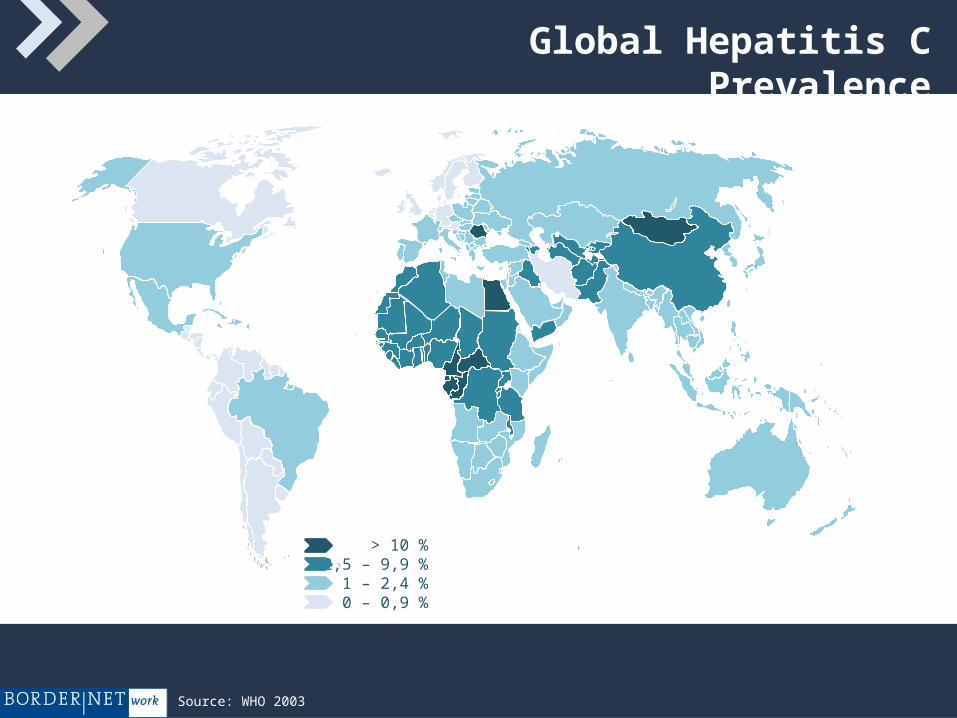
Global Hepatitis C Prevalence
> 10 %2,5 – 9,9 %
1 – 2,4 %0 – 0,9 %
Source: WHO 2003
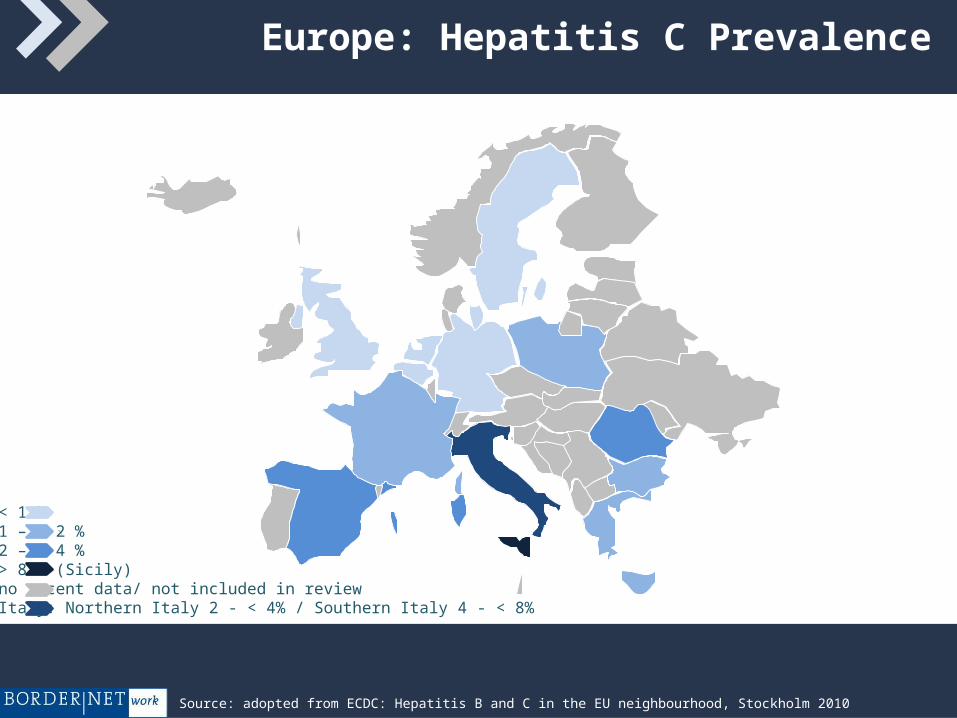
Europe: Hepatitis C Prevalence
< 1 %1 – < 2 %2 – < 4 %> 8 % (Sicily) no recent data/ not included in reviewItaly: Northern Italy 2 - < 4% / Southern Italy 4 - < 8%
Source: adopted from ECDC: Hepatitis B and C in the EU neighbourhood, Stockholm 2010
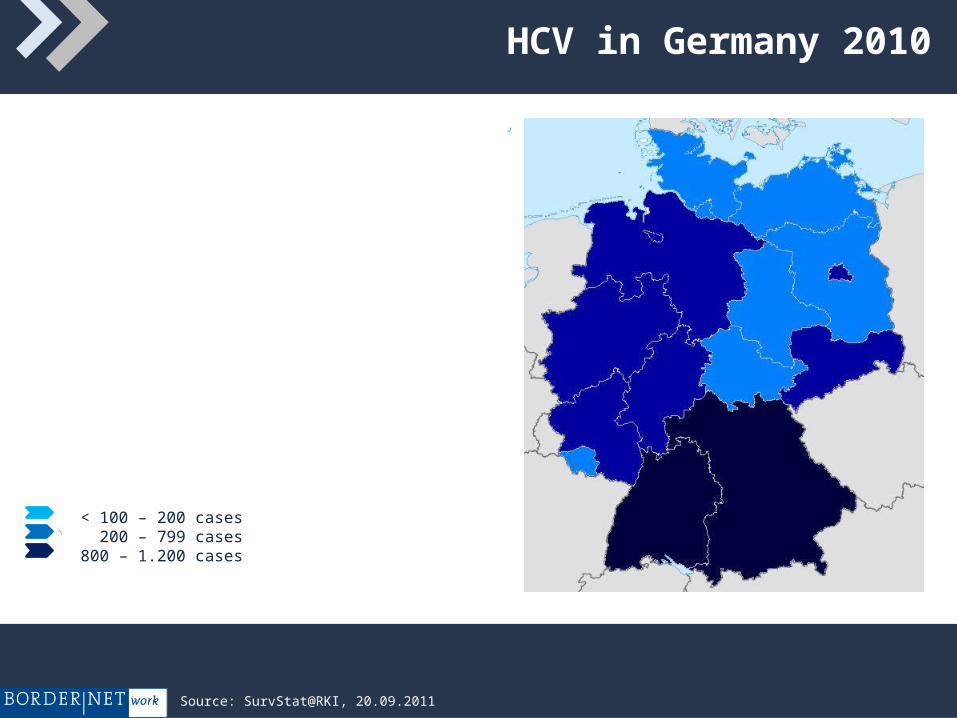
HCV in Germany 2010
< 100 – 200 cases200 – 799 cases
800 – 1.200 cases
Source: SurvStat@RKI, 20.09.2011
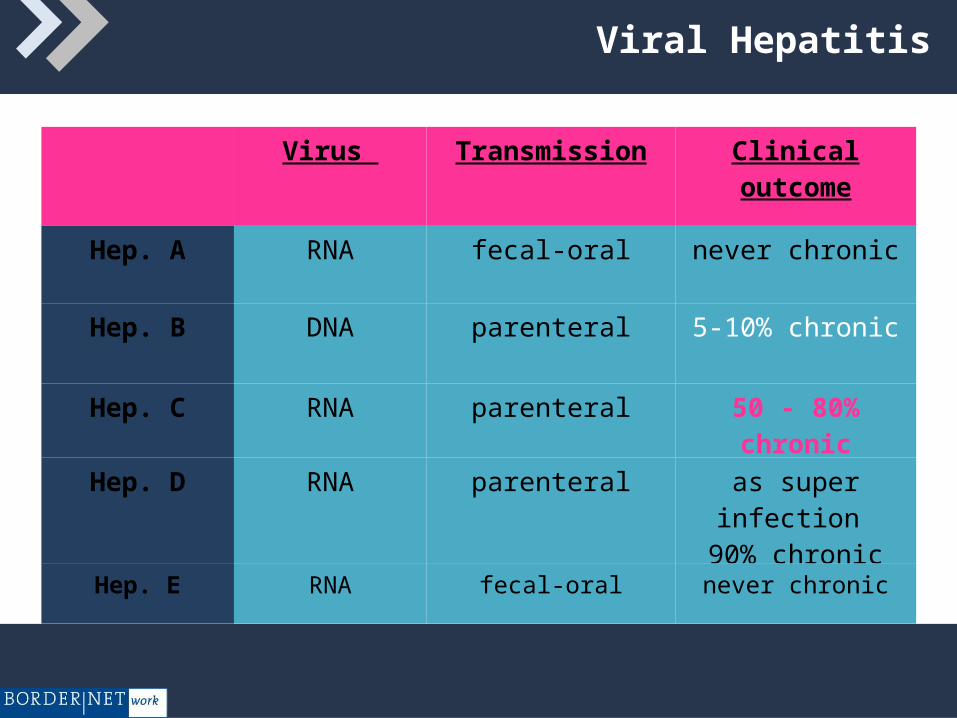
Viral Hepatitis
Virus Transmission Clinical outcome
Hep. A RNA fecal-oral never chronic
Hep. B DNA parenteral 5-10% chronic
Hep. C RNA parenteral 50 - 80% chronic
Hep. D RNA parenteral as super infection 90% chronic
Hep. E RNA fecal-oral never chronic
Cause: RNA-Virus
Incubation period: 4 month
Transmission: parenteral
Natural course: > 50 - 80% chronic
Treatment of acute and chronic Hepatitis C is possible
But until now:No vaccination –
prophylaxis of exposure !!
Virus C-Hepatitis
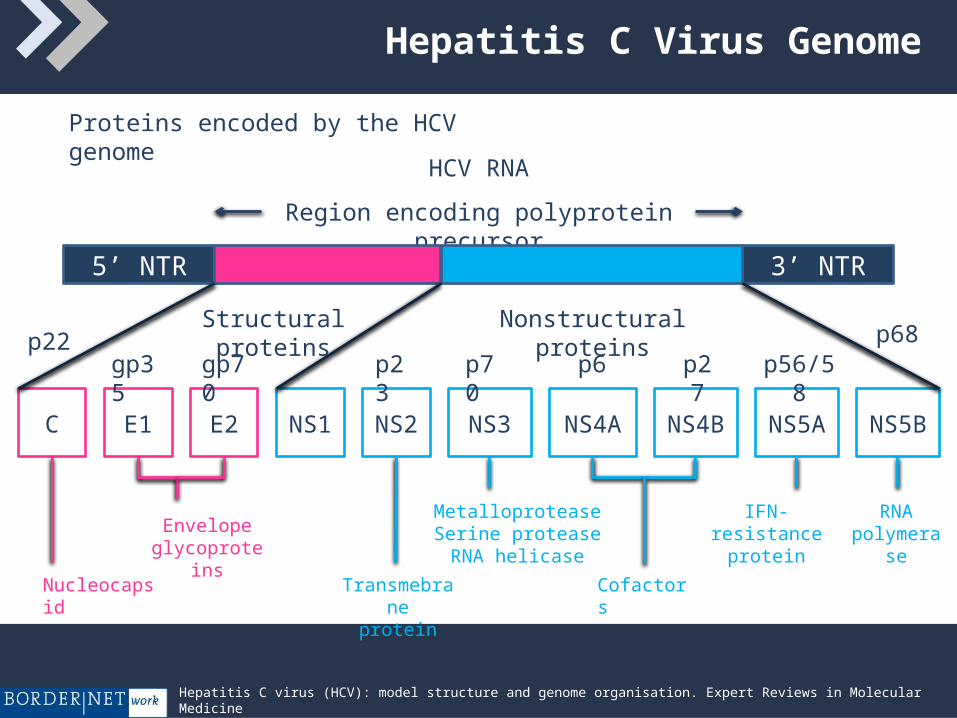
Hepatitis C Virus Genome
Proteins encoded by the HCV genome
HCV RNA
Region encoding polyprotein precursor
5’ NTR 3’ NTR
C E1 E2 NS1 NS2 NS3 NS4A NS4B NS5A NS5B
Nonstructural proteinsStructural proteins
p70 p6 p27 p56/58p23gp70gp35p68p22
Nucleocapsid
Envelope glycoproteins
Transmebraneprotein
Cofactors
RNA polymerase
IFN-resistance protein
MetalloproteaseSerine proteaseRNA helicase
Hepatitis C virus (HCV): model structure and genome organisation. Expert Reviews in Molecular Medicine ©2003 Cambridge University Press
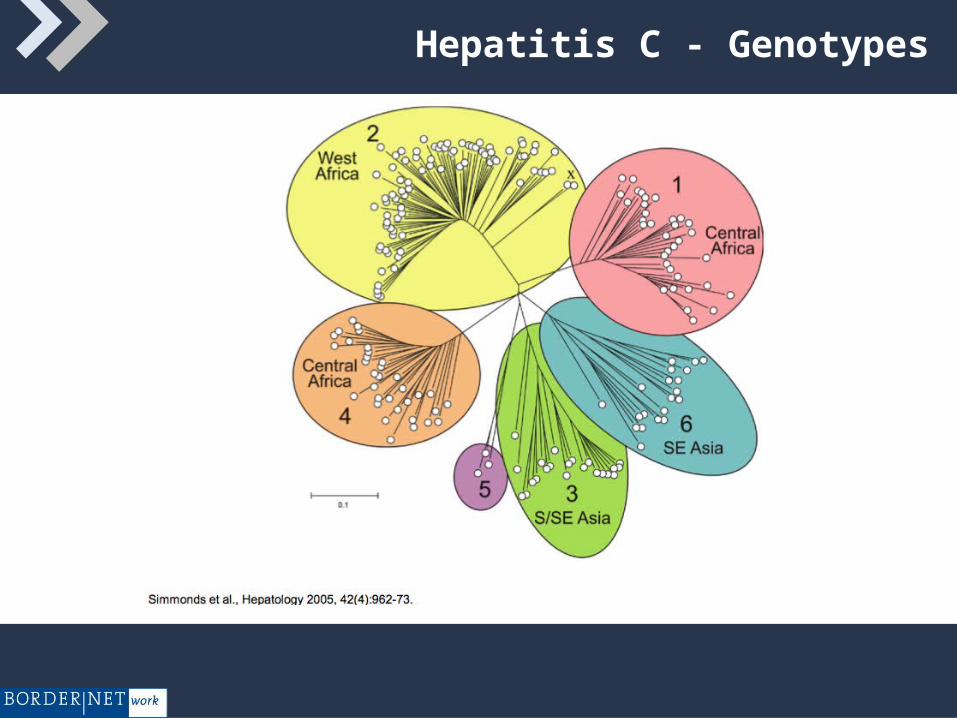
Hepatitis C - Genotypes
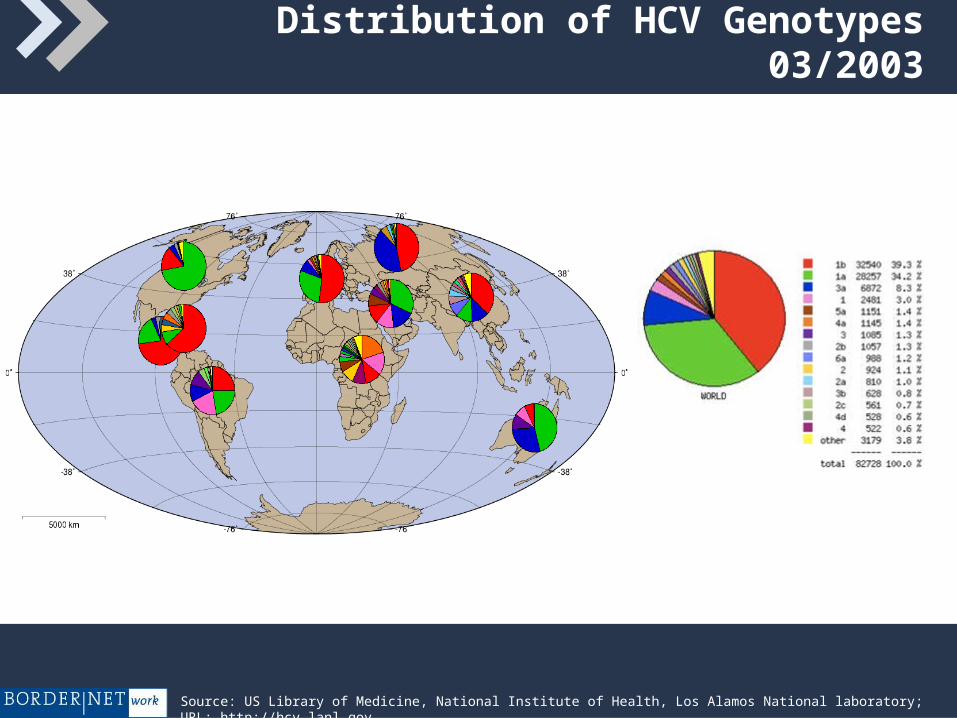
Distribution of HCV Genotypes 03/2003
Source: US Library of Medicine, National Institute of Health, Los Alamos National laboratory; URL: http://hcv.lanl.gov
Virus C – Hepatitis - Risk Situations
Parenteral transmission
Direct blood contact (professional
risk)
Hidden blood contact :
• Tattoo
• Piercing
• Needle sharing
Sexual intercourse
Vertical transmission
Decrease
of
infection
risk
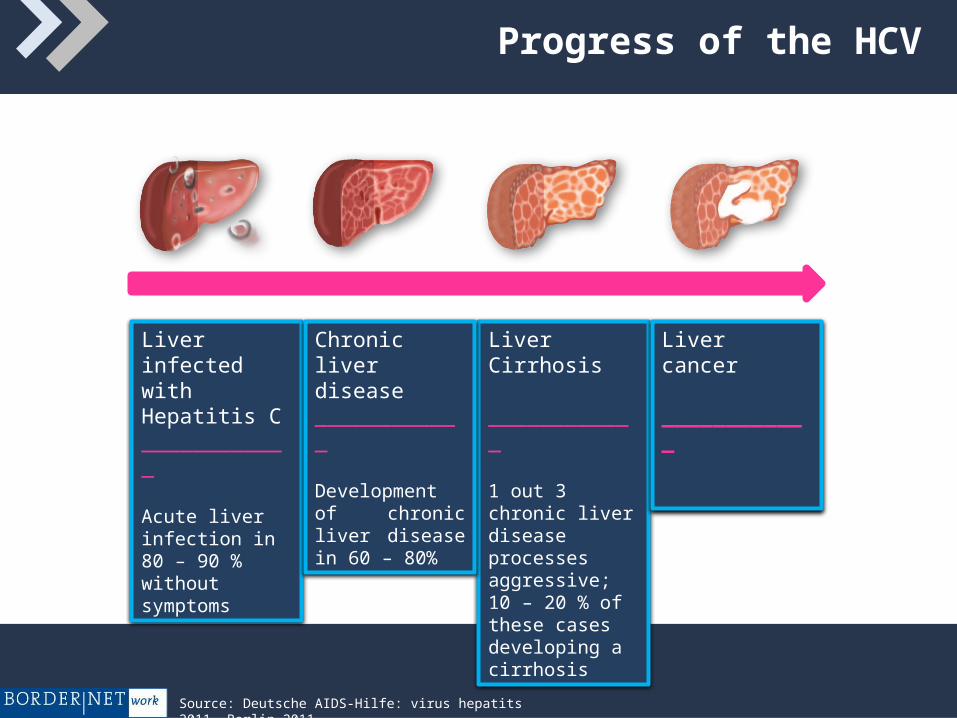
Liver infected with Hepatitis C____________
Acute liver infection in 80 – 90 % without symptoms
Liver Cirrhosis
____________
1 out 3 chronic liver disease processes aggressive; 10 – 20 % of these cases developing a cirrhosis
Chronic liver disease____________
Development of chronic liver disease in 60 – 80%
Liver cancer
____________
Progress of the HCV
Source: Deutsche AIDS-Hilfe: virus hepatits 2011. Berlin 2011.
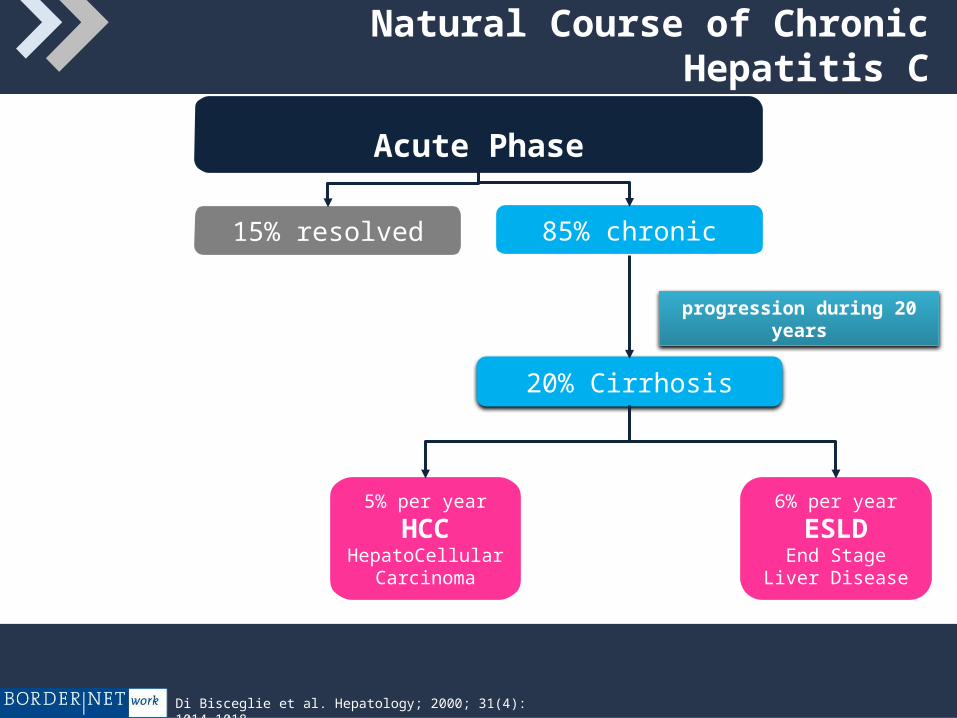
Natural Course of Chronic Hepatitis C
Acute Phase
15% resolved 85% chronic
5% per year
HCCHepatoCellular
Carcinoma
6% per year
ESLDEnd Stage Liver
Disease
20% Cirrhosis
progression during 20 years
Di Bisceglie et al. Hepatology; 2000; 31(4): 1014-1018
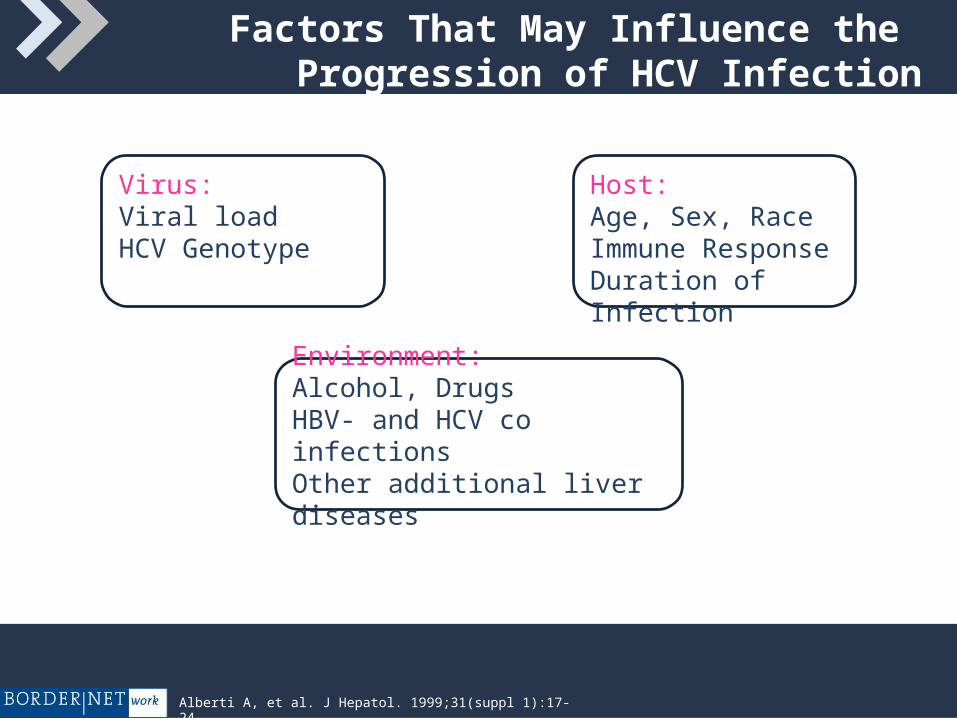
Factors That May Influence the Progression of HCV Infection
Virus:Viral loadHCV Genotype
Host:Age, Sex, RaceImmune ResponseDuration of Infection
Environment:Alcohol, DrugsHBV- and HCV co infectionsOther additional liver diseases
Alberti A, et al. J Hepatol. 1999;31(suppl 1):17-24.
Hepatitis C - Diagnostic possibilities
1. Blood Chemistry: Liver enzymes • ALAT (SGPT) • ASAT (SGOT) • Gamma GT
2. Serology: Detection of antibodies • anti-HCV (EIA, RIBA)
3. Viral Detection:• HCV qualitative (PCR)• HCH quantitative (PCR)• HCV genotype
(4.) Liver biopsy
I. Blood Chemistry - Diagnosis of HCV
Liver enzymes: ALAT (SGPT); ASAT (SGOT); Gamma GT
• in acute hepatitis higher levels
• in chronic hepatitis often mild or moderate elevations,
normal values are also possible
Other tests:
• Alkaline Phosphatase, Bilirubin
In progressive stages like Cirrhosis:
• Cholinesterase, Albumin;
• Prothrombin time
II. Serology of HCV - Detection of Antibodies
The HCV ELISA or EIA is a blood test that can detect HCV- antibodies. That means this person was infected with HCV at one time.
A positive anti HCV-Test could be:
• a status after acute Hepatitis C with recovery and without
chronic course
• acute Hepatitis C (but think about the diagnostic window in
the very early phase of an acute Virus C Hepatitis, in
this stage only HCVRNA is positive)
• chronic Hepatitis C
II. Serology - Detection of Antibodies
A negative anti-HCV test does not exclude HCV infection in
patients with suspected hepatitis c in following settings:
• acute HCV infection
• HIV infection
• patients with immunosuppression like e.g. chronic
haemodialysis
In immunosuppressed patients always an HIVRNA test should be
carried out if there is suspicion of hepatitis c infection independent
from the result of anti-HCV
Who should get an HCV –Test?
individuals who received blood, blood products or organs before
screening for HCV was implemented or where screening was not
yet widespread
current or former injecting drug users (even those who injected
drugs once many years ago)
patients on long-term haemodialysis
health-care workers
people living with HIV
individuals with abnormal liver tests or liver disease
infants born to infected mothers
Source: WHO June 2011
III. Viral Detection – Diagnosis of HCV
Viral Load: It measures the amount of HCV circulating in the blood in copies per millilitre or as a standard unit (International Units)
• Viral Load detection confirms the HCV replication
• Measurement is necessary predicting the medical response before starting treatment
• Analysis of the genotype choosing procedure of therapy
IV. Liver Biopsy for determination of Grading (inflammation) and Staging (Fibrosis)
There are three primary reasons for performing a liver biopsy:
• determination of the liver injury,
• grading and staging for the decision to initiate
therapy,
• with the diagnosis of advanced fibrosis or cirrhosis a
special surveillance for hepatocellular carcinoma
(HCC) and esophageal varices is necessary
Therapy of Chronic Hepatitis C
Pegylated Interferon alfa 2a or alfa 2b:
• 1 time per week subcutaneous
Ribavirin:
• daily 800 - 1200 mg, depending on HCV genotype and weight of the patient
Duration of therapy depends on HCV genotype, viral load,
viral kinetics!
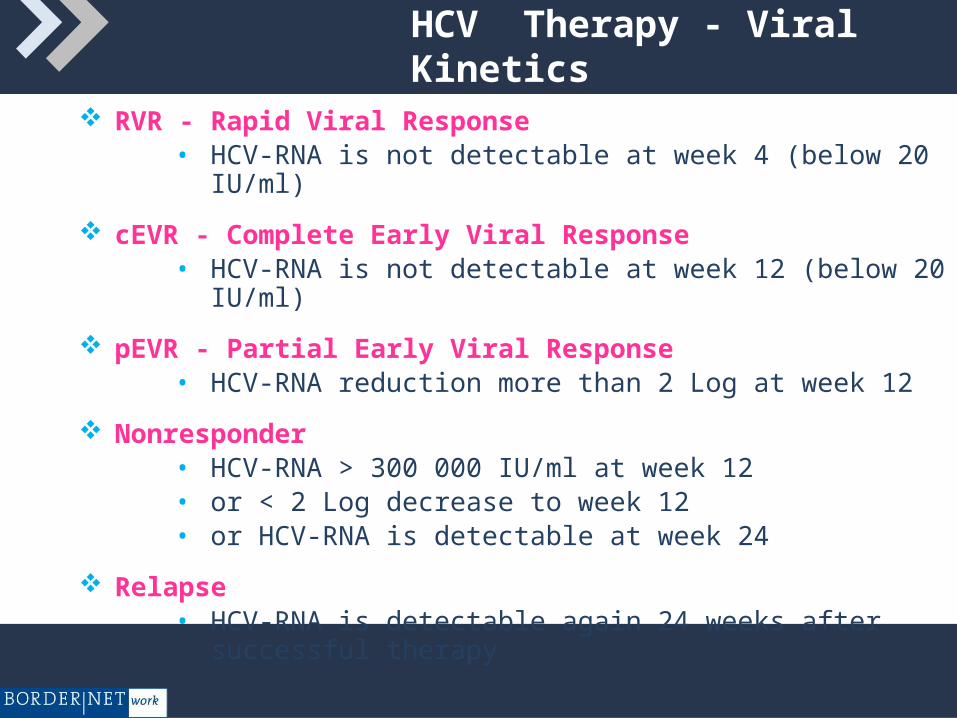
HCV Therapy - Viral Kinetics
RVR - Rapid Viral Response • HCV-RNA is not detectable at week 4 (below 20 IU/ml)
cEVR - Complete Early Viral Response • HCV-RNA is not detectable at week 12 (below 20 IU/ml)
pEVR - Partial Early Viral Response• HCV-RNA reduction more than 2 Log at week 12
Nonresponder• HCV-RNA > 300 000 IU/ml at week 12• or < 2 Log decrease to week 12• or HCV-RNA is detectable at week 24
Relapse• HCV-RNA is detectable again 24 weeks after successful
therapy
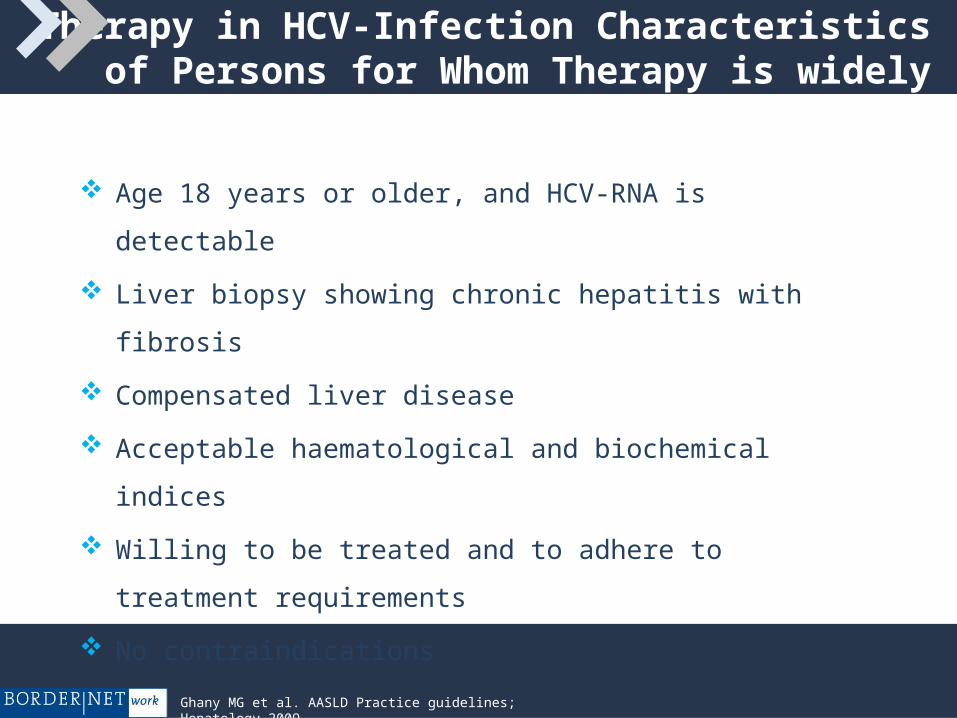
Therapy in HCV-Infection Characteristics of Persons for Whom Therapy is widely accepted
Age 18 years or older, and HCV-RNA is detectable
Liver biopsy showing chronic hepatitis with fibrosis
Compensated liver disease
Acceptable haematological and biochemical indices
Willing to be treated and to adhere to treatment requirements
No contraindications
Ghany MG et al. AASLD Practice guidelines; Hepatology 2009
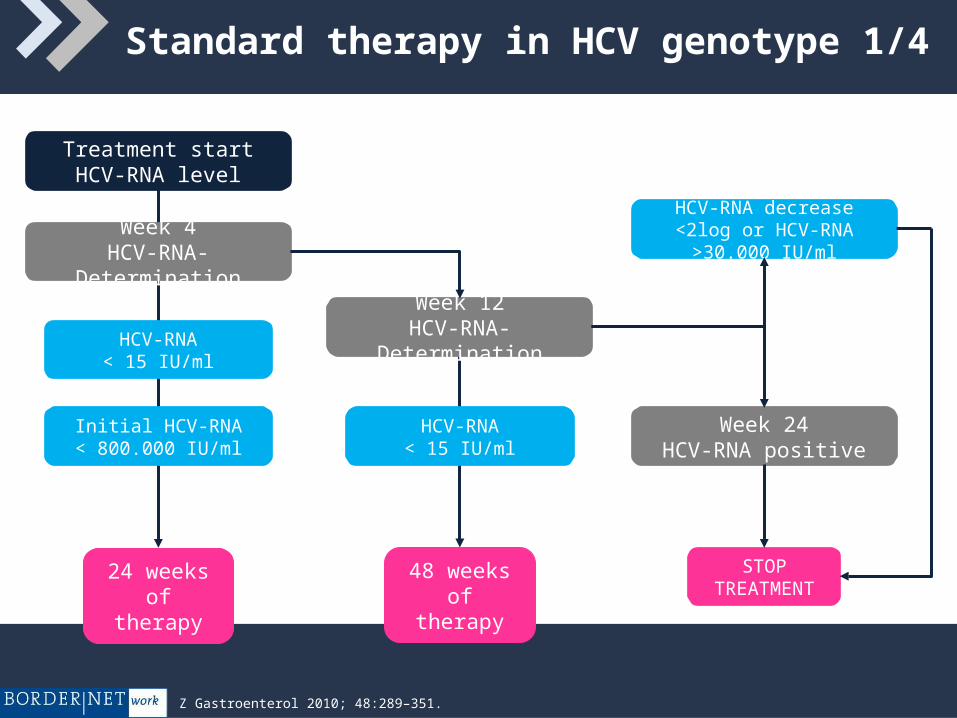
Standard therapy in HCV genotype 1/4
Treatment startHCV-RNA level
Week 4HCV-RNA-Determination
Week 12HCV-RNA-DeterminationHCV-RNA
< 15 IU/ml
Initial HCV-RNA< 800.000 IU/ml
HCV-RNA< 15 IU/ml
Week 24HCV-RNA positive
HCV-RNA decrease <2log or HCV-RNA >30.000 IU/ml
STOP TREATMENT
24 weeks of therapy
48 weeks of therapy
Z Gastroenterol 2010; 48:289–351.
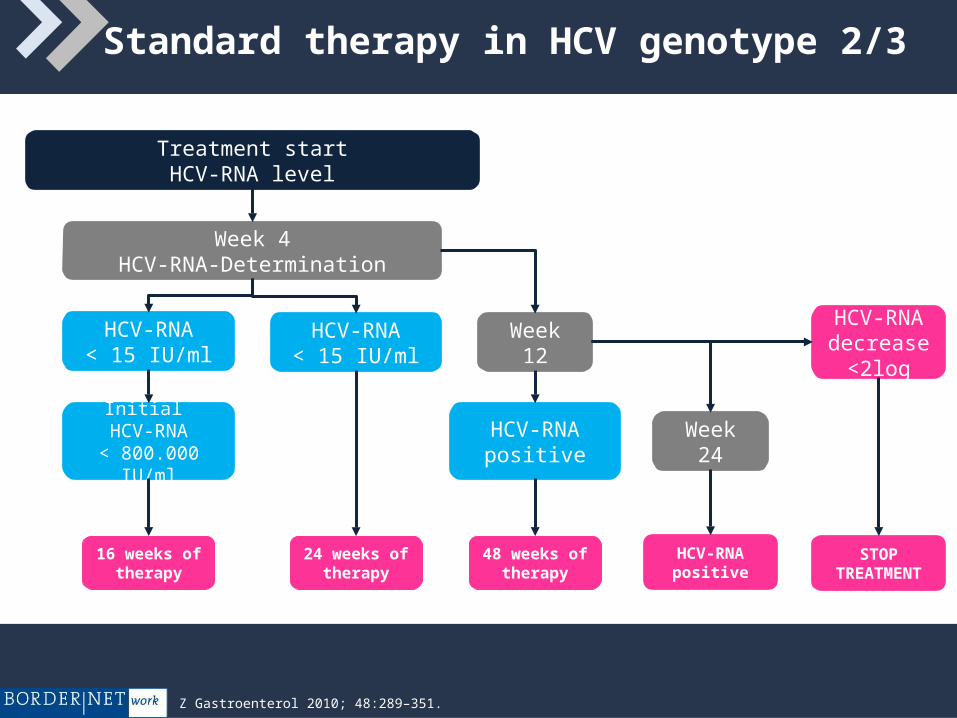
Standard therapy in HCV genotype 2/3
Treatment startHCV-RNA level
Week 4HCV-RNA-Determination
Week 12HCV-RNA< 15 IU/ml
Initial HCV-RNA
< 800.000 IU/ml
HCV-RNApositive
Week 24
HCV-RNA decrease
<2log
STOP TREATMENT
16 weeks of therapy
48 weeks of therapy
HCV-RNA< 15 IU/ml
24 weeks of therapy
HCV-RNApositive
Z Gastroenterol 2010; 48:289–351.
Treatment of Hepatitis C - Protease Inhibitors
Very potent antiviral activity (HCV-RNA decline 3-5 Log within 3 - 7 days
Developed against HCV genotype 1
Very rapid emergence of viral resistance when applied as mono-therapy
Cross-resistance between different protease inhibitors
PI improve the SVR in patients with chronic hepatitis genotype 1
Treatment naïve patients:
SVR rates increases from 38 - 44% to 63 – 75%
Treatment experienced patients:
SVR rates increase from 17 – 21% to 59 – 66%
Approval Studies for Protease Inhibitors
Telaprevir:
First therapy: ADVANCE / ILLUMINATE
Re – Therapy: REALIZE
Boceprevir:
First therapy: SPRINT 2
Re – Therapy: RESPOND 2
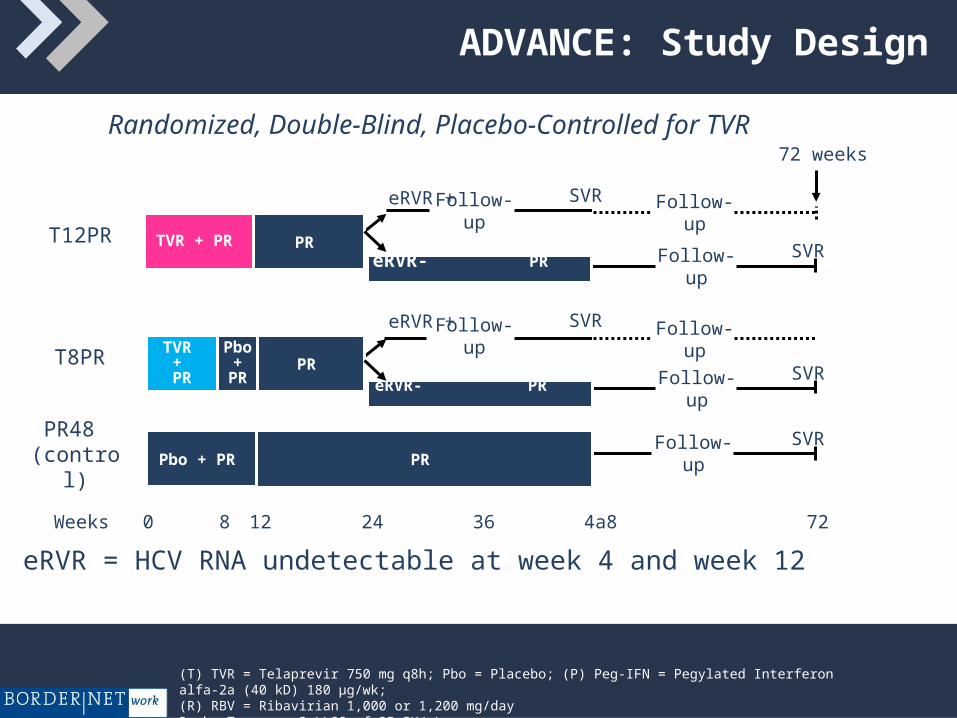
ADVANCE: Study Design
Randomized, Double-Blind, Placebo-Controlled for TVR
eRVR = HCV RNA undetectable at week 4 and week 12
240 4a8 72Weeks 128 36
Follow-upSVR
Pbo + PR PR
TVR + PR
Follow-upSVR
eRVR- PR .
eRVR +Follow-up
SVR
PR
Follow-upSVR
TVR + PR
eRVR- PR .
Pbo +
PR
Follow-upSVReRVR +
PR
72 weeks
Follow-up
Follow-up
PR48 (control)
T12PR
T8PR
(T) TVR = Telaprevir 750 mg q8h; Pbo = Placebo; (P) Peg-IFN = Pegylated Interferon alfa-2a (40 kD) 180 µg/wk; (R) RBV = Ribavirian 1,000 or 1,200 mg/dayRoche Taqman® v2 LLOQ of 25 IU/mL
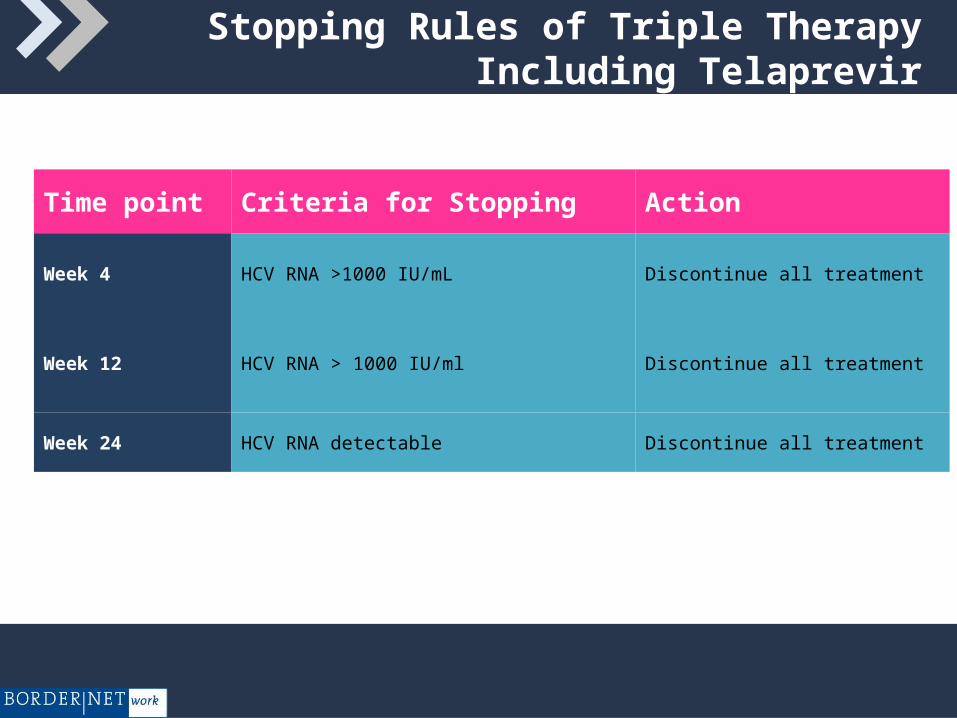
Stopping Rules of Triple Therapy Including Telaprevir
Time point Criteria for Stopping Action
Week 4 HCV RNA >1000 IU/mL Discontinue all treatment
Week 12 HCV RNA > 1000 IU/ml Discontinue all treatment
Week 24 HCV RNA detectable Discontinue all treatment
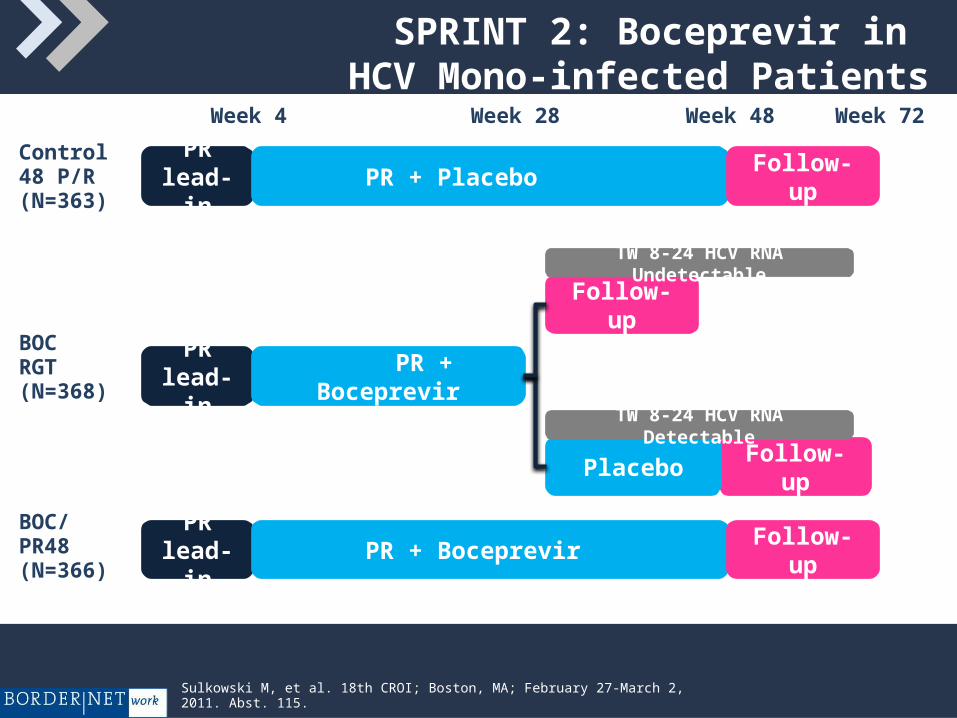
SPRINT 2: Boceprevir in HCV Mono-infected Patients
Sulkowski M, et al. 18th CROI; Boston, MA; February 27-March 2, 2011. Abst. 115.
BOCRGT(N=368) PR + Boceprevir
PRlead-in
BOC/PR48(N=366)
PR + BoceprevirPR
lead-in
Week 4 Week 48
PRlead-in
Week 28 Week 72
Control48 P/R(N=363)
PR lead-in
PR lead-in
PR lead-in
PR + Placebo
PR + Boceprevir
PR + Boceprevir
Follow-up
Follow-up
Follow-up
Follow-upPlacebo
TW 8-24 HCV RNA Undetectable
TW 8-24 HCV RNA Detectable
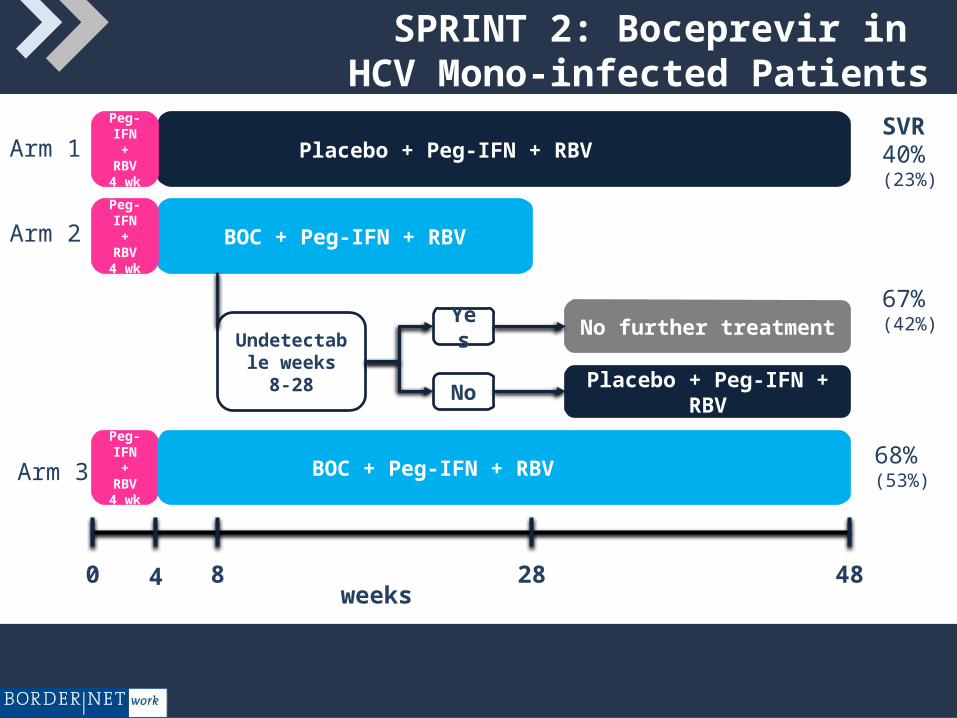
SPRINT 2: Boceprevir in HCV Mono-infected Patients
Peg-IFN + RBV4 wk
Placebo + Peg-IFN + RBV
BOC + Peg-IFN + RBV
BOC + Peg-IFN + RBV
No further treatment
Placebo + Peg-IFN + RBV
Yes
No
Undetectable weeks 8-28
Arm 1
Arm 2
Arm 3
0 4 8 28 48weeks
Peg-IFN + RBV4 wk
Peg-IFN + RBV4 wk
68%(53%)
40%(23%)
67%(42%)
SVR
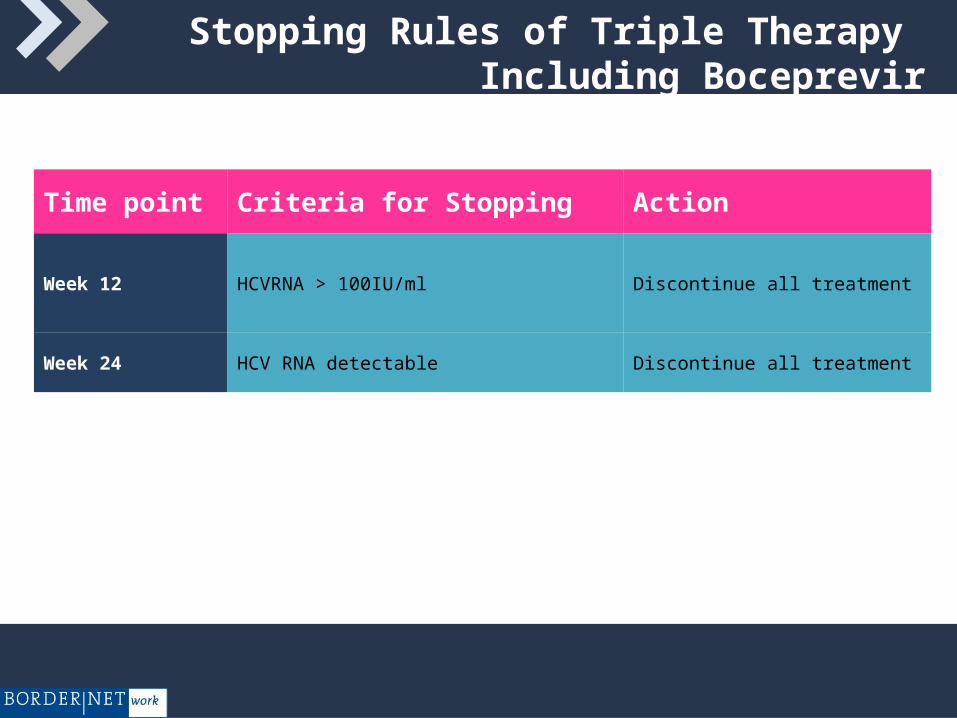
Stopping Rules of Triple Therapy Including Boceprevir
Time point Criteria for Stopping Action
Week 12 HCVRNA > 100IU/ml Discontinue all treatment
Week 24 HCV RNA detectable Discontinue all treatment
Possible Side Effects of Hepatitis C Therapy
56 55
7466
38
(SVR-12)
Flu-like symptoms (fever, arthralgia, myalgia) Gastrointestinal disorders Weight loss Haematological and immunologic effects (anaemia, leucopoenia,
thrombocytopenia) Skin disorders (dry skin, rash – especially in connection with Telaprevir) Psychiatric side effects (fatigue, irritability, depressive episodes, dysgeusia
– especially in connection with Boceprevir) Disorders of the thyroids Cough and dyspnoea
Challenges in HCV - Therapy with PI
IVD - Patients
Patients with HIV Co-infections
Prevention of Resistance
Drug Interactions
Compliance
Goals of a HCV - Therapy
Main Goal of HCV Therapy: Eradication of the virus
Additional effects of successful therapy:
• Disease progression will be stopped
• Histological liver changes recover
• Risk of hepatocellular carcinoma decreases
• Normalized quality of life
• Prevent transmission of virus






























