Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1990;53:633-639
Botulinum toxin treatment of cranial-cervicaldystonia, spasmodic dysphonia, other focaldystonias and hemifacial spasm
Joseph Jankovic, Kenneth Schwartz, Donald T Donovan
AbstractIn the past five years, 477 patients withvarious focal dystonias and hemifacialspasm received 3 806 injections ofbotulinum A toxin for relief of involun-ary spasms. A definite improvementwith a global rating ) 2 on a 0-4 scale,was obtained in all 13 patients with spas-modic dysphonia, 94% of 70 patientswith blepharospasm, 92% of 13 patientswith hemifacial spasm, 90% of 195patients with cervical dystonia, 77% of 22patients with hand dystonia, 73% of 45patients with oromandibular dystonia,and in 90% of 21 patients with other focaldystonia who had adequate follow up.While the average duration ofmaximumimprovement lasted about 11 weeks afteran injection (range seven weeks inpatients with hand dystonia to 15 weeksin patients with hemifacial spasm), somepatients benefited for over a year. Only16% of the 941 treatment visits withfollow up were not successful. Except fortransient focal weakness, there were veryfew complications or systemic effectsattributed to the injections. This studysupports the conclusion that botulinumtoxin injections are a safe and effectivetherapy for patients with focal dystoniaand hemifacial spasm.
Department ofNeurology, BaylorCollege of Medicine,Houston, Texas,United StatesJ JankovicK SchwartzDepartment ofOtorhinolaryngology,Baylor College ofMedicine, Houston,Texas, United StatesD T DonovanCorrespondence to: JosephJankovic, Professor ofNeurology, Baylor College ofMedicine, Department ofNcurology, One BaylorPlaza, Houston, TX 77030,United States.
Received 24 April 1989and in revised form12 December 1989.Accepted 9 January 1990
Dystonia is a neurological disorder character-ised by involuntary, repetitive or sustainedmuscle contractions frequently causing twist-ing, squeezing or other movements, andabnormal postures.' In most patients, no
specific cause for the dystonia can be iden-tified, hence the term primary or idiopathictorsion dystonia. The neurochemical mechan-isms of dystonia are not well understood andpharmacological (and surgical) therapy, whilehelpful in some, is unsatisfactory in mostpatients. Recently, injections of botulinumtoxin into the contracting muscles have beenshown to provide effective relief for mostpatients with focal dystonia and other disor-ders characterised by involuntary musclespasms.Botulinum toxin, a protein with molecular
weight of 140,000 daltons, is produced by thebacterium Clostridium botulinum thatoccasionally contaminates certain foods andwounds.23 There are eight immunologicallydistinct types of C botulinum, but only typesA, B, and E have been linked to humanbotulism. Botulism, produced by the type A
toxin, the most potent biological toxin knownto humans, is a life-threatening illness. Thetoxin exerts its paralytic effect by rapidly andirreversibly binding to the presynaptic cholin-ergic nerve terminal where it is internalisedand disrupts calcium ion influx. This inter-feres with the release of acetylcholine from thepresynaptic terminal, causing weakness.When absorbed into the systemic circulation,the toxin may produce generalised weakness,but it has a primarily local effect when injec-ted directly into a muscle. In 1973, Dr AlanScott, from the Smith-Kettlewell EyeResearch Foundation in San Francisco, usedbotulinum toxin for treatment of strabismusin primates and eight years later he reportedthe results of botulinum toxin treatment inhumans.4 Botulinum toxin has since beentried in a variety of extraocular muscle andneurological problems."'5We previously demonstrated in a double-
blind, placebo controlled trial that botulinuimtoxin injections provide effective relief forpatients with blepharospasm and possiblyother focal dystonias."5 We report the resultsof a long-term, prospective trial of botulinumtoxin treatment in 477 patients with a varietyof focal dystonias and other involuntarymovements.
Materials and methodsPatients and assessmentsTo be included in the study, the patients musthave had a disabling dystonia or hemifacialspasm despite optimum pharmacologicaltherapy, surgery, or both. All patients gave awritten informed consent approved by theInstitutional Review Boards for HumanResearch of Baylor College of Medicine andThe Methodist Hospital. After a completeneurological evaluation, the patients werevideotaped according to a standard protocol.With the exception of nine patients with tar-dive dystonia and 18 patients with hemifacialspasm, all other patients had idiopathic dys-tonia. Patients with spasmodic dysphonia dueto laryngeal dystonia had flexible fibreopticvideo laryngoscopy to exclude vocal fold path-ology and tremor. When the contracting mus-cles in patients with cervical dystonia couldnot be identified by inspection and palpation,electromyography (EMG) of the neck muscleswas used to select the most appropriate mus-cles for injection.The severity of dystonia and hemifacial
spasm was rated on a 0 to 4 scale (0 = nospasm; 1 = mild, barely noticeable; 2 = mild,
633 on 25 M
ay 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.53.8.633 on 1 August 1990. D
ownloaded from

Jankovic, Schwartz, Donovan
without functional impairment; 3 = moderatespasm, moderate functional impairment; 4 =severe, incapacitating spasm). Furthermore,the patients were instructed to rate and recordthe degree of their spasm in a daily diary."3"Latency" was defined as the interval (indays) between the injection and the first signof improvement following the injection. "Peakeffect", the maximum benefit obtained fromthe injection, was determined after a carefulreview of the patient's diary, an interview of aspouse or friends, and by the patient's ownperception of response. The "peak effect" wasrated on a 0 to 4 scale (0 = no effect; 1 = mildimprovement; 2 = moderate improvement,but no change in function; 3 = moderateimprovement in severity and function; 4 =marked improvement in severity and func-tion). "Global rating" was used as a measureof overall response and was defined as thepeak effect score minus one point if the injec-tion was associated with mild or moderatecomplications and two points if associatedwith severe or disabling complications. The"maximum" duration of improvement wasthe number of weeks during which thepatients experienced "peak effect"; "total"duration was the entire period (in weeks) afterthe injection during which the patients notedany improvement. The patients returned fortheir repeat injections about every three to sixmonths. If patients returned before theprevious injection wore off, then the total ormaximum duration of benefit was consideredindeterminable.The data was entered and constantly
updated in a computer database.
Botulinum toxin injectionsBotulinum toxin (Oculinum), was obtainedfrom Dr A Scott, as a freeze-dried lyophilisedpreparation. The vials were stored frozen(-20 0C) until the toxin was reconstitutedwith 0-900 sterile saline (without preservative)
eLLMX
, Site I Mean Dose SD
3.22.5
23.126.235.812.531.427.16.2
(5-20)(5-25)
(10-150)(50-150)(10-200)(10-75)(25-200)(25-200)(15-50)
Figure I Botulinum toxin: location of injections and dose per muscle. B = eyebrow,L = eyelid (orbicularis oculi),M = masseter, SC = scalenus,SCM = sternocleidomastoid, SM = submental, SP = splenius capitis,T = trapezius, V = vocalis complex.
at the time of injection. The potency isexpressed in units, where one unit (U)represents the estimated LD50 for mice,approximately 0-4 ng of the protein toxin.The lethal dose in juvenile monkeys is about40 U/kg of body weight which, whenextrapolated, is approximately fifty times theaverage dose injected for the treatment offocal dystonia. The diluted solution wasdrawn into a tuberculin syringe and the toxinwas injected with a 0-5 inch 30 gauge needleinto superficial muscles and with a 1-5 inch 22gauge needle into deep muscles. The dilutionswere identified for each patient; 10 U/0 1 mlwas used for small muscles such as the eyelidsand vocal folds, and 20 U/0- 1 ml was used fordoses greater than 25 U per site.At the beginning of the study there were no
published guidelines; the dose therefore foreach muscle was determined empirically. Lowdoses were used initially, particularly forsmall muscles, and the dose was titrated atsubsequent visits depending on the patient'sresponse after the previous injection. As wegained more experience, we adopted the fol-lowing dose schedule for initial injection: 5 Ufor each eyebrow, 12 5 U for each eyelid, 50 Ufor each masseter, 20 U for other facial mus-cles, 100 U for neck or shoulder muscles, 30 Ufor one vocal fold (only one vocal fold wasinjected in a single visit), 25 U for forearmand 100 U for distal leg muscles.
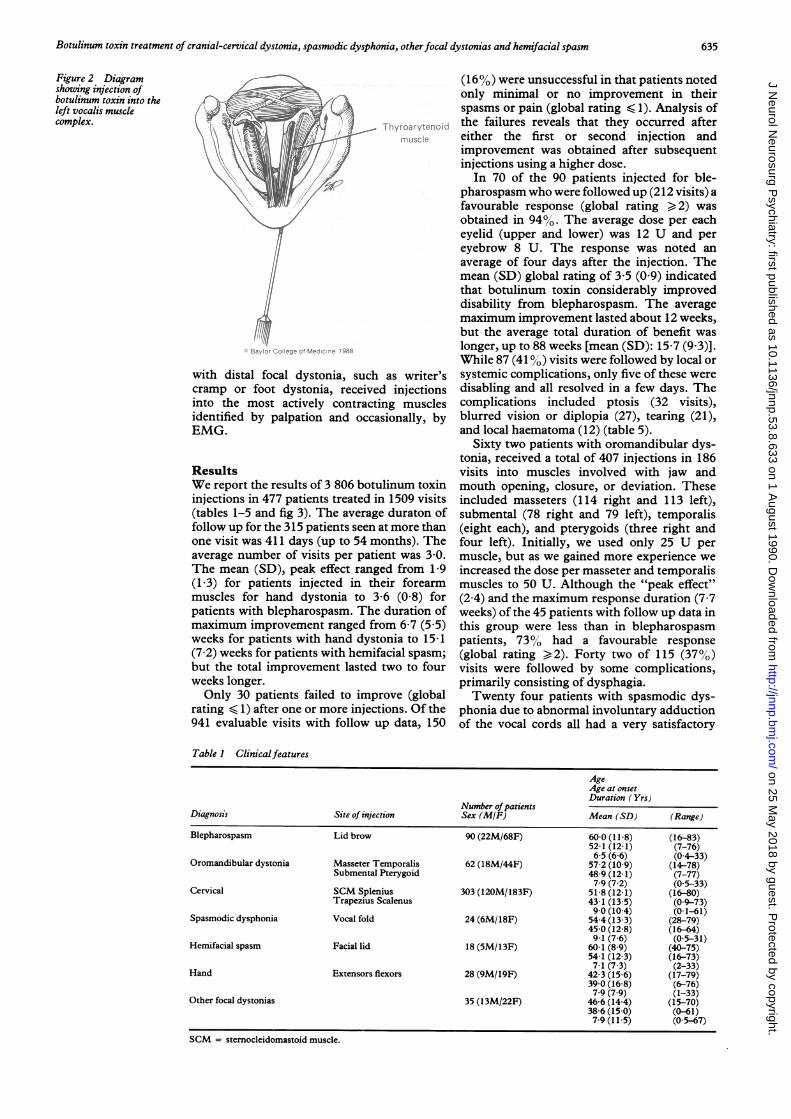
Injection techniqueWith the patient in a supine position, theeyelids and eyebrows were cleaned with alco-hol and the toxin was injected medially andlaterally into the pretarsal orbicularis oculi,avoiding the superior oblique and the levatorpalpebrae muscles to prevent diplopia andptosis respectively (fig 1). The masseter, tem-poralis and submental or suprahyoid (digas-tric, geniohyoid, and mylohyoid) muscleswere also injected when the patient was in asupine position. Other muscles were identifiedby palpation or by EMG and were injectedwith the patient in a sitting position. Patientswith torticollis usually required injections intothe sternocleidomastoid muscle (SCM) re-sponsible for turning the head to the oppositeside. This was usually combined with injec-tions to the contralateral trapezius. Patientswith retrocollis needed injections into bothsplenius capitum muscles, whereas laterocolliswas treated with injections into the ipsilateralsplenius capitis, trapezius, and occasionallyscalenus medius. Anterocollis usually resultedfrom contraction of both SCMs, but occasion-ally injections into the submental muscleswere also needed. The total dose was dis-tributed into the larger neck muscles in fourto six injections. The left thyroarytenoidvocalis muscle complex was identified byEMG and the toxin was injected through thesame teflon coated hollow monopolar needle(fig 2). The posterior pharyngeal andpterygoid muscles were approached orally."Hemifacial spasm was treated with local injec-tions into the muscles which contracted most,carefully avoiding perilabial regions. Patients
634
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from
Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, otherfocal dystonias and hemifacial spasm
Figure 2 Diagramshowing injection ofbotulinum toxin into theleft vocalis musclecomplex.
with distal focal dystonia, suchcramp or foot dystonia, receivesinto the most actively contractiidentified by palpation and occa
EMG.
ResultsWe report the results of 3 806 botuinjections in 477 patients treated ir(tables 1-5 and fig 3). The averagefollow up for the 315 patients seen a
one visit was 411 days (up to 54 mlaverage number of visits per paticThe mean (SD), peak effect rang((1 -3) for patients injected in thmuscles for hand dystonia to 3patients with blepharospasm. Themaximum improvement ranged fr(weeks for patients with hand dyst(7-2) weeks for patients with hemifbut the total improvement lastedweeks longer.Only 30 patients failed to impr
rating < 1) after one or more inject941 evaluable visits with follow u
(160%) were unsuccessful in that patients notedonly minimal or no improvement in theirspasms or pain (global rating < 1). Analysis ofthe failures reveals that they occurred aftereither the first or second injection andimprovement was obtained after subsequentinjections using a higher dose.
In 70 of the 90 patients injected for ble-pharospasm who were followed up (212 visits) afavourable response (global rating ) 2) wasobtained in 9400. The average dose per eacheyelid (upper and lower) was 12 U and pereyebrow 8 U. The response was noted anaverage of four days after the injection. Themean (SD) global rating of 3-5 (0 9) indicatedthat botulinum toxin considerably improveddisability from blepharospasm. The averagemaximum improvement lasted about 12 weeks,but the average total duration of benefit waslonger, up to 88 weeks [mean (SD): 15-7 (9 3)].While 87 (41 %) visits were followed by local or
as writer's systemic complications, only five of these wered injections disabling and all resolved in a few days. Theng muscles complications included ptosis (32 visits),sionally, by blurred vision or diplopia (27), tearing (21),
and local haematoma (12) (table 5).Sixty two patients with oromandibular dys-
tonia, received a total of 407 injections in 186visits into muscles involved with jaw and
linum toxin mouth opening, closure, or deviation. These1509 visits included masseters (114 right and 113 left),
. duraton of submental (78 right and 79 left), temporalisat more than (eight each), and pterygoids (three right andonths). The four left). Initially, we used only 25 U per
ent was 3 0. muscle, but as we gained more experience weed from 1 9 increased the dose per masseter and temporaliseir forearm muscles to 50 U. Although the "peak effect"*6 (08) for (2 4) and the maximum response duration (7.7duration of weeks) of the 45 patients with follow up data in)m 6-7 (5 5) this group were less than in blepharospasmonia to 15-1 patients, 73% had a favourable response
acial spasm; (global rating > 2). Forty two of 115 (37%o)two to four visits were followed by some complications,
primarily consisting of dysphagia.rove (global Twenty four patients with spasmodic dys--ions. Of the phonia due to abnormal involuntary adductionIp data, 150 of the vocal cords all had a very satisfactory
Table 1 Clinicalfeatures
AgeAge at onsetDuration (Yrs)
Number ofpatientsDiagnosis Site of injection Sex (MIF) Mean (SD) (Range)
Blepharospasm Lid brow 90 (22M/68F) 600 (11 8) (16-83)52-1 (12-1) (7-76)6-5 (6-6) (04-33)
Oromandibular dystonia Masseter Temporalis 62 (18M/44F) 57-2 (10-9) (14-78)Submental Pterygoid 48-9 (12-1) (7-77)
7-9 (7-2) (05-33)Cervical SCM Splenius 303 (120M/183F) 51-8 (12-1) (16-80)
Trapezius Scalenus 43-1 (13-5) (09-73)90 (10-4) (01-61)
Spasmodic dysphonia Vocal fold 24 (6M/18F) 54-4 (13 3) (28-79)45-0 (12-8) (16-64)91 (76) (05-31)
Hemifacial spasm Facial lid 18 (5M/13F) 601 (8-9) (40-75)54-1 (12 3) (16-73)7-1 (7-3) (2-33)
Hand Extensors flexors 28 (9M/19F) 42-3 (15 6) (17-79)39-0 (16 8) (6-76)7-9 (7-9) (1-33)
Other focal dystonias 35 (13M/22F) 46-6 (14-4) (15-70)38-6 (15-0) (0-61)7-9(115) (05-67)
SCM = stemocleidomastoid muscle.
635
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from

Jankovic, Schwartz, Donovan
Table 2 Botulinum toxin: site and dose of injections
Number of Muscle dose Cumulative dose/ptNumber of injections Number of
Site of injection patients (right/left) visits Mean (SD) (range) Units Mean (SD) (range) Units
Lid (upper) 89 1047 (287/278) 303 11-5 (2 5) (5-25) 135-1 (134-4) (6-745)(lower) (244/238)
Brow 40 234 (117/117) 118 7-9 (3 2) (5-20) 46-4 (35 8) (7-143)Masseter 42 227 (114/113) 117 51-9 (23-1) (10-150) 280-5 (279-0) (40-1350)Pterygoid 3 7 (3/4) 4 329(110) (25-50) 767 (20.5) (50-100)Submental 43 157 (78/79) 80 29-2 (12-5) (10-75) 106-7 (106-7) (20-630)Hemifacial 18 45 (24/21) 45 18-7 (10-6) (5-50) 46 7 (40 4) (5-150)SCM 249 635 (338/297) 554 93-5 (35.8) (10-200) 238-5 (192-7) (10-1000)Splenius 262 831 (432/399) 676 116-6 (31-4) (25-200) 369-8 (332-9) (25-1950)Trapezius 122 272 (144/128) 249 99 7 (27-1) (25-200) 222-3 (193-6) (50-1200)Scalenus 54 80 (44/36) 69 98-8 (26-2) (50-150) 146-3 (87-1) (50-550)Vocal fold 24 52 (2/50) 52 29-7 (6-2) (15-50) 64-3 (56 4) (20-287)Hand (flexor) 28 97 (60/18) 79 66-9 (44 4) (10-300) 231-6 (164-1) (50-675)
(extensor) (8/11)Other 35 102 67 90 7 (70 2) (10-250) 264-4 (298.8) (20-1100)
SCH= Sternocleidomastoid muscle.
Table 3 Response to botulinum toxin injections
Number of Duration of responseGlobal rating evaluable Latency to response(days) Peak effect (weeks) maximum Total
patients/Type of dystonia Mean (SD) (Range) visits Mean (SD) (Range) Mean (SD) (Range) Mean (SD) (Range) Mean (SD) (Range)
Blepharospasm 3-4 (09) (0-4) 70/212 4-2 (57) (0-42) 3-6 (08) (0-4) 12-4 (85) (0-88) 15-7 (93) (0-88)Oromandibular 2-2 (1-5) (0-4) 45/115 4-6 (5 6) (0-30) 2-4 (1-6) (0-4) 7-7 (6-4) (0-32) 10 3 (8-7) (0-54)Cervical 2-9 (1-2) (0-4) 195/500 7-2 (7 9) (0-80) 3-0 (1-2) (0-4) 11-7 (7-1) (0-88) 14-3 (7 6) (0-88)Spasmodic 3-3 (1-0) (0-4) 13/29 2-7 (3 8) (0-1-14) 3-4 (0 8) (0-4) 10.6 (6.3) (0-24) 14-9 (8-1) (0-28)dysphonia
Hemifacial 3 1 (1 3) (0-4) 13/29 4-8 (7-0) (0-28) 3-2 (1 4) (0-4) 15-1 (7 2) (0-28) 19-0 (17 5) (0-32)Hand 1-5 (1-2) (0-4) 22/50 5-1 (5-7) (0-28) 1-9 (1-3) (0-4) 6-7 (5-5>- (0-20) 8-6 (6-9) (0-28)Other 3-1 (1-3) (0-4) 21/39 6-3 (6-3) (0-23) 3-2 (1-3) (0-4) 9-4 (7-6) (0-24) 10-5 (8.4) (0-28)
response (global rating > 2) with average "peakeffect" of 3-4. In most patients theimprovement was noted within a few hours ordays after injection and lasted for up to 28weeks (average 15). The starting dose was 30 Uper one (left) vocal fold. Complications wereuncommon and consisted of hypophonia orhoarseness in seven patients and dysphagia inthree.
Three hundred and three patients withcervical dystonia received a total of 1818 injec-tions in 844 visits. The muscles injectedincluded SCM (338 right and 297 left),trapezius (144 right and 128 left), spleniuscapitus (432 right and 399 left), and scalenusmedius (44 right and 36 left). Ninety per cent ofthe 195 patients with adequate follow upimproved (global rating > 2). The mostdramatic improvement was noted by patientswho experienced pain with their cervical dys-tonia. Of the 123 patients who reported pain,114 (93%) noted improvement of their pain.The overall mean (SD) pain response in allpatients with cervical dystonia was 3 5 (1 1) (0-4 scale; from 0 = no response to 4 = completeresolution of pain). During the last three yearsthe average initial dose per- muscle hasincreased from 25 to 100 U. While most
patients have noted improvement within thefirst week after injection, a few have had alatency ofup to eleven weeks. In some patients,a previously hypertrophied muscle had shrunkwithout improvement in the head- position orrange of neck movement. This usuallyindicated that additional muscles wereinvolved or that the wrong muscle may havebeen selected. When other muscles were laterinjected the response usually was morefavourable. Only 78 patients in 119 visits (24%of all visits with follow up) had some complica-tions, consisting chiefly of dysphagia (45patients) and neck weakness (24 patients).These side effects lasted an average of 18 days.
In 18 patients with hemifacial spasm, twelveof 13 patients who had been followed up (92%),noted reduction in unilateral blepharospasmand annoying facial twitching. The averagemaximum and total duration of improvement,mean 15-1 and 19-0 weeks respectively, was
longer than for any of the focal dystonias (table3). Except for transient focal weakness, seen insix of 21 (21%) patients, there were no othercomplications.
Patients with hand dystonia (for example,writer's cramp) presented the most challengingproblem because the muscles responsible for
Table 4 Botulinum toxin injections:failures and complications
Number ofpatients withcomplications
Percent of Duration in dayspatients whofailed Percent of Patients Visits
Type of dystonia 1 or more visits failed visits (disabling) Mean (SD) (Range)
Blepharospasm 12-9 4-7 44 87 (5) 23 8 (17 5) (2-62)Oromandibular 55-6 33 0 28 42 (13) 28-0 (22-1) (2-90)Cervical 27-7 13-2 77 115 (15) 18 2 (14-4) (0-001-60)Spasmodic dysphonia 15-4 6-9 8 10 (1) 29-3 (18 7) (7-60)Hemifacial 30 8 13 8 6 6 (1) 31-8 (18-4) (14-62)Hand 68-2 48-0 14 22(5) 26 2 (21-7) (4-90)Other 26-3 14-7 8 8 (1) 22-2 (16-6) (3-42)
636
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from
Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, otherfocal dystonias and hemifacial spasm
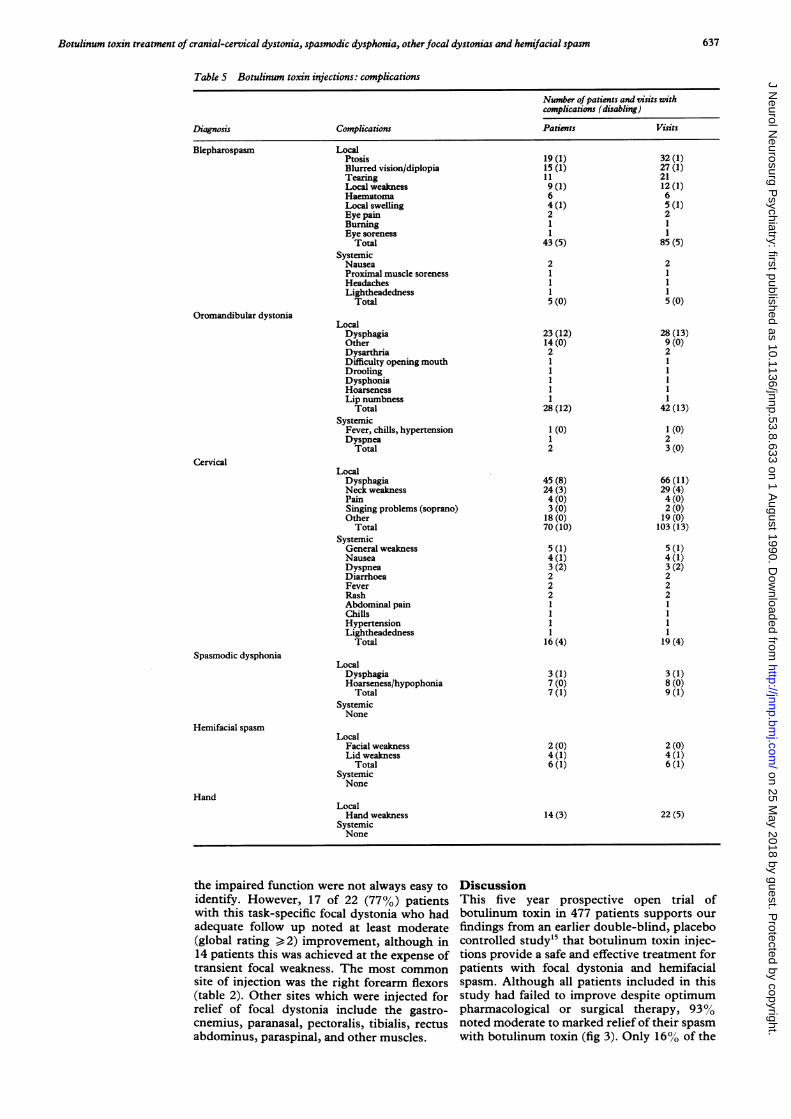
Table 5 Botulinum toxin injections: complications
Number ofpatients and visits withcomplications (disabling)
Diagnosis Complications Patients Visits
Blepharospasm Local
Oromandibular dystonia
Cervical
Spasmodic dysphonia
Hemifacial spasm
Hand
PtosisBlurred vision/diplopiaTearingLocal weaknessHaematomaLocal swellingEye painBurningEye soreness
TotalSystemicNauseaProximal muscle sorenessHeadachesLightheadedness
Total
LocalDysphagiaOtherDysarthriaDifficulty opening mouthDroolingDysphoniaHoarsenessLip numbness
TotalSystemic
Fever, chills, hypertensionDyspnea
Total
LocalDysphagiaNeck weaknessPainSinging problems (soprano)Other
TotalSystemicGeneral weaknessNauseaDyspneaDiarrhoeaFeverRashAbdominal painChillsHypertensionLightheadedness
Total
LocalDysphagiaHoarseness/hypophonia
TotalSystemicNone
LocalFacial weaknessLid weakness
TotalSystemicNone
LocalHand weakness
SystemicNone
the impaired function were not always easy toidentify. However, 17 of 22 (77%) patientswith this task-specific focal dystonia who hadadequate follow up noted at least moderate(global rating > 2) improvement, although in14 patients this was achieved at the expense oftransient focal weakness. The most common
site of injection was the right forearm flexors(table 2). Other sites which were injected forrelief of focal dystonia include the gastro-
cnemius, paranasal, pectoralis, tibialis, rectusabdominus, paraspinal, and other muscles.
DiscussionThis five year prospective open trial ofbotulinum toxin in 477 patients supports ourfindings from an earlier double-blind, placebocontrolled study'5 that botulinum toxin injec-tions provide a safe and effective treatment forpatients with focal dystonia and hemifacialspasm. Although all patients included in thisstudy had failed to improve despite optimumpharmacological or surgical therapy, 93%/Onoted moderate to marked relief of their spasmwith botulinum toxin (fig 3). Only 16% of the
19 (1)15 (1)119 (1)64 (1)21
43 (5)
2
11
5 (0)
32 (1)27 (1)2112 (1)65 (1)211
85 (5)
21115 (0)
28 (13)9 (0)2
l11
42 (13)
1 (0)23 (0)
66 (11)29 (4)4 (0)2 (0)19(0)
103 (13)
5 (1)4 (1)3 (2)222
111
19 (4)
23 (12)14 (0)2
128 (12)
1 (O)12
45 (8)24 (3)4 (0)3 (0)18 (0)70 (10)
5 (1)4 (1)3 (2)222
111
16 (4)
3(1)7 (0)7 (1)
3 (1)8 (0)9 (1)
2 (0)4 (1)6 (1)
2 (0)4 (1)6 (1)
14 (3) 22 (5)
637
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from
Jankovic, Schwartz, Donovan
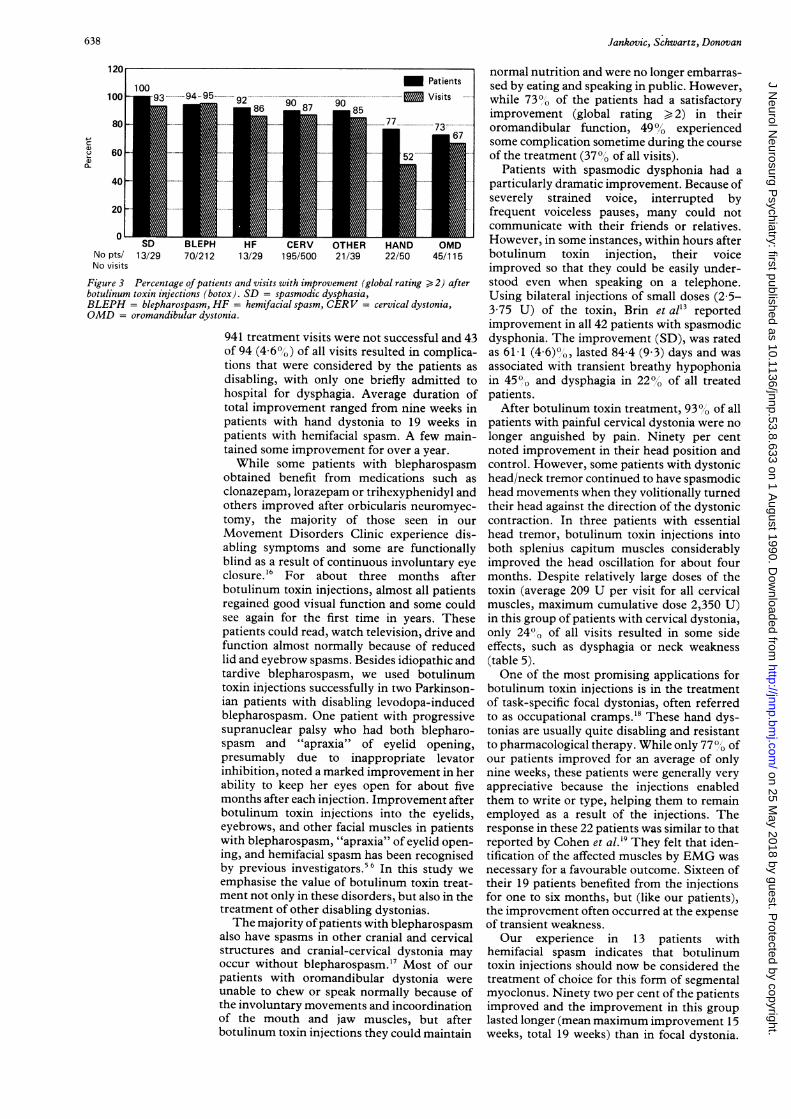
195/500 21/39 22/50 45/115
Figure 3 Percentage of patients and visits with improvement (global rating > 2) afterbotulinum toxin injections (botox). SD = spasmodic dysphasia,BLEPH = blepharospasm, HF = hemifacial spasm, CERV = cervical dystonia,OMD = oromandibular dystonia.
941 treatment visits were not successful and 43of 94 (4 6%) of all visits resulted in complica-tions that were considered by the patients asdisabling, with only one briefly admitted tohospital for dysphagia. Average duration oftotal improvement ranged from nine weeks inpatients with hand dystonia to 19 weeks inpatients with hemifacial spasm. A few main-tained some improvement for over a year.While some patients with blepharospasm
obtained benefit from medications such asclonazepam, lorazepam or trihexyphenidyl andothers improved after orbicularis neuromyec-tomy, the majority of those seen in ourMovement Disorders Clinic experience dis-abling symptoms and some are functionallyblind as a result of continuous involuntary eyeclosure."6 For about three months afterbotulinum toxin injections, almost all patientsregained good visual function and some couldsee again for the first time in years. Thesepatients could read, watch television, drive andfunction almost normally because of reducedlid and eyebrow spasms. Besides idiopathic andtardive blepharospasm, we used botulinumtoxin injections successfully in two Parkinson-ian patients with disabling levodopa-inducedblepharospasm. One patient with progressivesupranuclear palsy who had both blepharo-spasm and "apraxia" of eyelid opening,presumably due to inappropriate levatorinhibition, noted a marked improvement in herability to keep her eyes open for about fivemonths after each injection. Improvement afterbotulinum toxin injections into the eyelids,eyebrows, and other facial muscles in patientswith blepharospasm, "apraxia" of eyelid open-ing, and hemifacial spasm has been recognisedby previous investigators."6 In this study we
emphasise the value of botulinum toxin treat-ment not only in these disorders, but also in thetreatment of other disabling dystonias.The majority ofpatients with blepharospasm
also have spasms in other cranial and cervicalstructures and cranial-cervical dystonia mayoccur without blepharospasm.'7 Most of our
patients with oromandibular dystonia wereunable to chew or speak normally because ofthe involuntary movements and incoordinationof the mouth and jaw muscles, but afterbotulinum toxin injections they could maintain
normal nutrition and were no longer embarras-sed by eating and speaking in public. However,while 73%O of the patients had a satisfactoryimprovement (global rating > 2) in theiroromandibular function, 49% experiencedsome complication sometime during the courseof the treatment (37%' of all visits).
Patients with spasmodic dysphonia had aparticularly dramatic improvement. Because ofseverely strained voice, interrupted byfrequent voiceless pauses, many could notcommunicate with their friends or relatives.However, in some instances, within hours afterbotulinum toxin injection, their voiceimproved so that they could be easily under-stood even when speaking on a telephone.Using bilateral injections of small doses (2 5-3 75 U) of the toxin, Brin et al'3 reportedimprovement in all 42 patients with spasmodicdysphonia. The improvement (SD), was ratedas 61 1 (4 6)0o, lasted 84 4 (9 3) days and wasassociated with transient breathy hypophoniain 4500 and dysphagia in 220, of all treatedpatients.
After botulinum toxin treatment, 930%1 of allpatients with painful cervical dystonia were nolonger anguished by pain. Ninety per centnoted improvement in their head position andcontrol. However, some patients with dystonichead/neck tremor continued to have spasmodichead movements when they volitionally turnedtheir head against the direction of the dystoniccontraction. In three patients with essentialhead tremor, botulinum toxin injections intoboth splenius capitum muscles considerablyimproved the head oscillation for about fourmonths. Despite relatively large doses of thetoxin (average 209 U per visit for all cervicalmuscles, maximum cumulative dose 2,350 U)in this group of patients with cervical dystonia,only 24% of all visits resulted in some sideeffects, such as dysphagia or neck weakness(table 5).One of the most promising applications for
botulinum toxin injections is in the treatmentof task-specific focal dystonias, often referredto as occupational cramps.18 These hand dys-tonias are usually quite disabling and resistantto pharmacological therapy. While only 77% ofour patients improved for an average of onlynine weeks, these patients were generally veryappreciative because the injections enabledthem to write or type, helping them to remainemployed as a result of the injections. Theresponse in these 22 patients was similar to thatreported by Cohen et al."9 They felt that iden-tification of the affected muscles by EMG wasnecessary for a favourable outcome. Sixteen oftheir 19 patients benefited from the injectionsfor one to six months, but (like our patients),the improvement often occurred at the expenseof transient weakness.Our experience in 13 patients with
hemifacial spasm indicates that botulinumtoxin injections should now be considered thetreatment of choice for this form of segmentalmyoclonus. Ninety two per cent of the patientsimproved and the improvement in this grouplasted longer (mean maximum improvement 15weeks, total 19 weeks) than in focal dystonia.
inn
CL
M Patients
Visits
o _- XSD
No pts/ 13/29No visits
70/212 13/29
638
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from

Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, otherfocal dystonias and hemifacial spasm
One possible reason for this long duration ofimprovement may be the presence of subclin-ical denervation, which may also account forthe lower than usual dose needed for thetreatment of unilateral blepharospasmassociated with the hemifacial spasm. Becauseof the marked benefit from botulinum toxininjections, we no longer recommend microvas-cular facial nerve decompression for thesepatients except in rare cases.A detailed analysis of 30 patients who failed
to improve even after several treatment visitsdid not reveal any clinical variables, such asage, duration of illness, previous history ofsurgical treatment or any other demographicdata that could reliably predict the poor out-come. One possible explanation for the failureto improve after botulinum toxin injections isthe presence of blocking antibodies, either as aresult of previous injections or because of aprevious history of botulism. While someinvestigators718 have found anti-botulinumtoxin antibodies, particularly in those patientswho have received large cumulative doses andwho failed to respond, another study20 found noantibodies by either bioassay or immunoassayin a large group of patients treated with thetoxin. Furthermore, the presence of blockingantibodies would not explain why, despitemarked weakness and atrophy of the injectedmuscle, some patients fail to improve. Wesuspect that, in such cases, the abnormal dys-tonic movement or posture is due to contrac-tions of muscles that were not injected or werenot readily accessible. Another possible reasonfor poor response to botulinum toxin injectionsis the presence of secondary contractures orskeletal deformities.
Besides the development ofantibodies, otherpotential concerns on the effects of repeatedbotulinum toxin injections include local spreadof injectate (which could account for some ofthe complications due to weakness of adjacentmuscles), retrograde transport ofthe toxin witheventual involvement of the spinal cord orbrainstem, and the possibility of denervationsupersensitivity.2122 To prevent effects of localdiffusion, some investigators have suggestedthat the toxin should be injected as close to themotor end-point as possible. In one study,patients with blepharospasm were injectedonly in motor end-points identified by per-cutaneous electrical stimulation (lateral perior-bital region of the upper eyelid and medialpreseptal region of the lower eyelid) [GBorodic, personal communication]. The res-ponse was not as good as when the toxin wasadministered by multiple injections over thelength of the muscle. One possible explanationis that motor end-point, as identified by acutaneous stimulus, may not be near the actualneuromuscular junction. We obtained goodresults by distributing the injections near themidpoint of the muscle, an area whichpresumably contains the innervation zone. Wedid not see the need to use EMG to identifymotor end-points. While some investigatorsusing single fibre EMG recordings have sug-gested that the toxin might have a systemicaction,23 24 there is so far no evidence that repeat
injections of the toxin produce any seriousadverse systemic effects.Although there are many unanswered ques-
tions about this new therapy, our results sug-gest that botulinum toxin injection should nowbe regarded as the treatment of choice fordisabling focal dystonia and hemifacial spasm.While the long-term effects of repeated injec-tions of botulinum toxin are unknown, ourexperience indicates that the treatment is safeand that the beneficial effects seem to bemaintained for at least five years.
We thank Compaq Computer Corporation for donating thecomputer equipment used in the analysis of the data presented.
1 Jankovic J, Fahn S: Dystonic syndromes. In: Jankovic J,Tolosa E, eds. Parkinson's disease and movement disorders,Baltimore, MD: Urban and Schwarzenberg, 1988:283-314.
2 Sellin LC. The action of botulinum toxin at the neuromus-cular junction. Med Biol 198 1;59:11-20.
3 Dolly JO, Black J, Williams RS, Melling J. Acceptors forbotulinum neurotoxin reside on motor nerve terminalsand mediate its internalization, Nature 1984;307:457-60.
4 Scott AB. Botulinum toxin injection of eye muscles tocorrect strabismus. Trans Am Ophthalmol Soc
. 1981;79:734-70.5 Scott AB, Kennedy RA, Stubbs HA. Botulinum A Toxin
injection as a treatment for blepharospasm. Arch Ophthal-mol 1985;103:347-50.
6 Katz B, Rosenberg JH. Botulinum therapy for apraxia ofeyelid opening. Am J Ophthalm 1987;103:718-9.
7 Brin MF, Fahn S, Moskowitz CB, et al. Localized injectionsof botulinum toxin for the treatrnent of focal dystonia andhemifacial spasm. Movement Disorders 1987;2:237-54.
8 Tsui JKC, Calne DB. Botulinum toxin in cervical dystonia.In: Jankovic J, Tolosa E (eds), Facial Dyskinesias, AdvNeurol, Vol 49, New York, NY: Raven Press, 1988:479-92.
9 Stell R, Thompson PD, Marsden CD. Botulinum toxin inspasmodic torticollis. J Neurol Neurosurg Psychiatry1988;51:920-3.
10 Jankovic J, Schwartz K. Botulinum toxin injection forcervical dystonia. Neurology 1990;40:277-80.
11 Miller RH, Woodson GE, Jankovic J. Botulinum toxininjection of the vocal fold for spasmodic dysphonia. Apreliminary report. Arch Otolaryngol Head Neck Surg1987;1 13:603-5.
12 Ludlow CL, Naunton RF, Sedory SE, Schulz GM, HallettM. Effects of botulinum toxin injections on speech inadductor spasmodic dysphonia. Neurology 1988;38:1220-5.
13 Brin MF, Blitzer A, Fahn S, et al. Adductor laryngealdystonia (spastic dysphonia): Treatment with local injec-tions of botulinum toxin (botox). Movement Disorders1989;4:287-96.
14 Cohen LG, Hallett M, Geller B, Hochberg F. Treatment offocal dystonias of the hand with botulinum toxin injec-tions. J Neurol Neurosurg Psychiatry 1989;52:355-63.
15 Jankovic J, Oriman J. Botulinum A toxin for cranial-cervicaldystonia: A double-blind, placebo-controlled study.Neurology 1987;37:616-23.
16 Jankovic J, Ford J. Blepharospasm and orofacial-cervicaldystonia: Clinical and pharmacologic findings in 100patients. Ann Neurol 1983;13:402-1 1.
17 Jankovic J. Etiology and differential diagnosis of blepharo-spasm and oromandibular dystonia. In: Jankovic J,Tolosa E, eds. Facial Dyskinesias, Adv Neurol, Vol 49.New York, NY: Raven Press, 1988:103-16.
18 Rosenbaum F, Jankovic J. Task-specific focal dystonia andtremor: Categorization of occupational movement disor-ders. Neurology 1988;38:522-7.
19 Tsui JK, Wong NLM, Wong E, Calne DB. Production ofcirculating antibodies to botulinum-A toxin in patientsreceiving repeated injections for dystonia. Ann Neurol1988;23:181 (abstract).
20 Biglan AW, Gonnering R, Lockhart LB, Rabin B, FuersteFH. Absence of antibody production in patients treatedwith botulinum A toxin. Am J Ophthalmol 1986;101:232-5.
21 Wiegand H, Erdmann G, Wellhoner HH. '25I-labelledbotulinum A neurotoxin: pharmacokinetics in cats afterintramuscular injection. Naunyn-Schmiedebergs ArchPharmacol 1976;292:161-5.
22 Black JD, Dolly JO. Interaction of 1'2I-labelled botulinumneurotoxins with nerve terminals. I: Ultrastructuralautoradiographic localization and quantitation of distinctmembrane receptors for typesAand B onmotorneurons. JCell Biol 1986;103:521-34.
23 Lange DJ, Brin MF, Warner CL, Fahn S, Lovelace RE.Distant effects of local injections of botulinum toxin.Muscle and Nerve 1987;10:552-5.
24 Sanders DB, Massey EW, Buckley EC. Botulinum toxin forblepharospasm: Single-fiber EMG studies. Neurology1986;36:545-7.
639
on 25 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.8.633 on 1 A
ugust 1990. Dow
nloaded from





























